Ovulation Calculator
Track Your Ovulation & Maximize Your Chances of Conception
Ovulation & Fertility Calculator
Enter Your Cycle Information
Fertility by Cycle Day
| Days Before Ovulation | Pregnancy Chance | Fertility Level |
|---|---|---|
| 5 days before | ~10% | Low fertility |
| 3-4 days before | ~15% | Moderate fertility |
| 1-2 days before | ~25-30% | High fertility (best days) |
| Ovulation day | ~20% | High fertility |
What is Ovulation?
Ovulation is the release of a mature egg from one of the ovaries, occurring approximately once per menstrual cycle. The egg travels down the fallopian tube where it can be fertilized by sperm for 12-24 hours. If fertilization occurs, the resulting embryo implants in the uterine lining, beginning pregnancy. If unfertilized, the egg dissolves and the uterine lining sheds during menstruation approximately 14 days later.
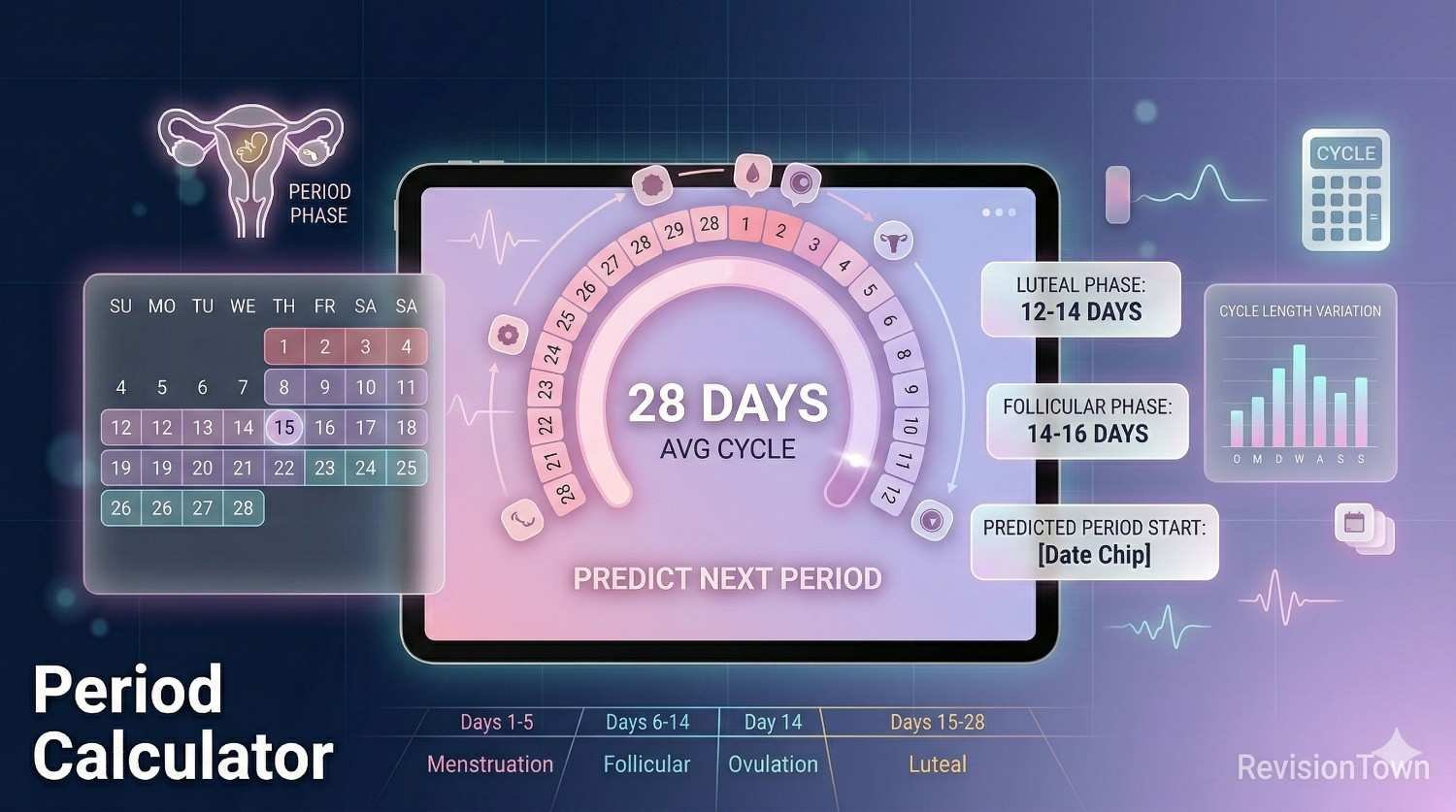
Ovulation is triggered by a luteinizing hormone (LH) surge approximately 24-36 hours before the egg releases. This surge can be detected using ovulation predictor kits (OPKs). For women with regular 28-day cycles, ovulation typically occurs around day 14 (counting from the first day of the period). However, ovulation timing varies: for a 21-day cycle, it occurs around day 7; for a 35-day cycle, around day 21. The general rule: ovulation happens approximately 12-14 days before the next period starts.
Understanding ovulation is crucial for both achieving and preventing pregnancy. The fertile window—the days when pregnancy is possible—includes the 5 days before ovulation plus ovulation day itself, totaling 6 days. This is because sperm can survive in the female reproductive tract for up to 5 days when fertile-quality cervical mucus is present, while the egg survives only 12-24 hours. The 2-3 days immediately before ovulation offer the highest conception probability (~25-30% per cycle for healthy couples).
Signs & Symptoms of Ovulation
Cervical Mucus Changes (Primary Sign)
Cervical mucus changes dramatically throughout the cycle due to estrogen fluctuations. After period ends, mucus is minimal, thick, and sticky—hostile to sperm. As ovulation approaches (rising estrogen), mucus becomes increasingly watery, then clear, stretchy, and slippery—resembling raw egg white. This "fertile-quality" mucus facilitates sperm transport and survival, creating the fertile window. Peak fertile mucus appears 1-2 days before ovulation. After ovulation (progesterone dominance), mucus quickly becomes thick, cloudy, and sticky again or disappears. Tracking mucus daily (check toilet paper or cervical opening) is one of the most reliable free ovulation detection methods.
Basal Body Temperature (BBT) Shift
Basal body temperature is your lowest resting temperature, measured immediately upon waking before any activity. BBT remains relatively low (97.0-97.5°F) during the follicular phase (pre-ovulation). After ovulation, progesterone causes a sustained temperature rise of 0.5-1.0°F (97.6-98.6°F) that persists until the next period or throughout pregnancy if conception occurs. BBT tracking confirms ovulation occurred but doesn't predict it in advance—temperature rises after the egg has already released. Chart BBT daily for 3+ cycles to identify patterns. Use a basal thermometer (more precise than standard fever thermometers) and measure at the same time each morning.
Ovulation Pain (Mittelschmerz)
Mittelschmerz ("middle pain" in German) is one-sided lower abdominal or pelvic pain occurring during ovulation, experienced by approximately 20% of women. The pain is typically a sharp twinge, cramp, or dull ache lasting minutes to hours, occasionally up to 1-2 days. It occurs on the side where the egg releases (alternating sides month-to-month as ovaries take turns). The cause is likely follicle swelling before rupture or slight irritation from fluid/blood released during ovulation. While mittelschmerz can help pinpoint ovulation, it's not reliable alone since similar pain can result from other causes (gas, digestion, cysts).
Secondary Physical Signs
Additional ovulation symptoms include: Breast tenderness from rising progesterone post-ovulation; Increased libido (evolutionary mechanism to encourage intercourse during fertile window); Light spotting (ovulation bleeding) from the sudden estrogen drop at ovulation in some women; Bloating and water retention; Heightened sense of smell; Increased energy and mood (estrogen peak); Cervical position changes (cervix becomes higher, softer, and more open during fertile window, then drops and firms after ovulation). These secondary signs are less reliable than mucus and BBT but can support ovulation timing when tracked together.
Ovulation Predictor Kits (OPKs)
OPKs detect the LH surge that precedes ovulation by 24-36 hours, providing advance warning of your most fertile days. Test daily starting 2-3 days before expected ovulation (cycle length - 17 days). Use second morning urine (first morning may be too concentrated, causing false positives). A positive OPK (test line as dark or darker than control) indicates ovulation within 12-48 hours—have intercourse that day and the following 2 days. Digital OPKs display "yes/no" or smiley face results (easier to read but more expensive). Advanced monitors (Clearblue Fertility Monitor) track both estrogen and LH for wider fertile window detection. OPKs are highly effective for regular cycles but may give false readings with PCOS (persistently elevated LH).
Methods for Tracking Ovulation
Calendar Method (Least Accurate)
The calendar method estimates ovulation by tracking cycle length over several months and assuming ovulation occurs 12-14 days before the next period. For a 28-day cycle, predict ovulation around day 14. This method works reasonably well for perfectly regular cycles but fails for irregular cycles, stress-related variations, or anovulatory cycles. It's best used as a starting point for identifying when to begin more precise tracking methods (OPKs, mucus monitoring) rather than relying on it alone for conception or contraception.
Symptothermal Method (Most Comprehensive)
The symptothermal method combines multiple fertility indicators: daily BBT charting, cervical mucus observation, and cervical position checking. This comprehensive approach is 95-99% effective (with perfect use) for both achieving and preventing pregnancy. The method requires consistent daily tracking, chart interpretation training, and partner cooperation. Fertile window is identified when cervical mucus becomes slippery/stretchy; infertile phase is confirmed when BBT has remained elevated for 3+ consecutive days AND cervical mucus has dried up. While time-intensive, this method provides deep understanding of personal fertility patterns without cost or side effects.
Fertility Awareness Apps
Fertility tracking apps (Flo, Clue, Kindara, Ovia) use algorithms to predict fertile windows based on cycle data, BBT, mucus observations, OPK results, and symptoms. Apps simplify data entry and visualization but accuracy depends on input quality and algorithm sophistication. Calendar-only apps (predicting from cycle length alone) are less reliable than apps incorporating BBT and mucus data. FDA-cleared apps like Natural Cycles use temperature data and advanced algorithms for contraception with 93% typical-use effectiveness. Apps are tools to assist tracking but don't replace understanding personal fertility signs.
Clinical Ovulation Monitoring
Medical ovulation tracking includes: Transvaginal ultrasound monitoring (visualizes follicle growth and confirms ovulation through corpus luteum presence); Blood tests measuring LH, FSH, estradiol, and progesterone levels throughout cycle; Endometrial biopsy (rarely used—checks uterine lining response to hormones). These clinical methods are used when investigating fertility issues, irregular cycles, or during fertility treatments (IVF, IUI). They provide definitive ovulation confirmation but require multiple doctor visits and aren't necessary for women with regular cycles trying to conceive naturally.
Maximizing Conception Chances
Optimal Timing for Intercourse
Pregnancy probability is highest with intercourse 1-2 days before ovulation (~25-30% per cycle). Having sex the day of ovulation yields ~20% chance; 3 days before drops to ~15%; 5 days before is ~10%. Intercourse after ovulation has minimal pregnancy potential since the egg rapidly degrades within 12-24 hours. For maximum conception chances: have intercourse every 1-2 days during the 6-day fertile window (5 days before ovulation through ovulation day). Daily sex slightly increases odds but isn't necessary—sperm count remains adequate with every-other-day frequency, and some men's sperm quality actually improves with 1-2 day abstinence.
Lifestyle Factors Affecting Fertility
Maintain healthy weight: Both underweight (BMI <18.5) and overweight (BMI >30) disrupt ovulation and reduce fertility. Women with PCOS often don't ovulate regularly—even 5-10% weight loss can restore ovulation. Limit alcohol and caffeine: Heavy drinking disrupts hormones; limit to <1 drink/day when trying to conceive. High caffeine (>300mg/day) may reduce fertility. Don't smoke: Smoking accelerates egg loss and brings menopause 1-4 years earlier. Manage stress: Chronic stress can delay or prevent ovulation through cortisol-reproductive hormone interactions. Exercise moderately: Regular moderate exercise supports fertility, but excessive training (>7 hours/week intense exercise) can suppress ovulation.
Supplements & Nutrients
Preconception nutrition: Take prenatal vitamins with 400-800 mcg folic acid at least 3 months before trying to conceive—prevents neural tube defects. Include CoQ10 (may improve egg quality), vitamin D (linked to fertility and pregnancy success), omega-3 fatty acids (support reproductive health), and iron (prevent anemia). Ensure adequate protein, healthy fats, and complex carbohydrates. Avoid trans fats (reduce ovulatory fertility). Men should take zinc, vitamin C, and antioxidants to optimize sperm quality. However, supplements don't replace healthy diet—food sources provide better nutrient absorption and additional beneficial compounds.
When to Seek Fertility Help
Consult a reproductive endocrinologist if: Under 35 and trying for 12+ months without pregnancy; Over 35 and trying for 6+ months; Irregular or absent periods; Known reproductive conditions (PCOS, endometriosis, fibroids); History of pelvic inflammatory disease; Multiple miscarriages; Male partner has known fertility issues. Women over 35 have declining egg quantity and quality—don't wait full year before seeking evaluation. Fertility testing for both partners includes: semen analysis, ovulation confirmation (blood progesterone test), ovarian reserve testing (AMH, FSH, antral follicle count), and hysterosalpingography (tubal patency check). Early intervention improves success rates with treatments like ovulation induction, IUI, or IVF.
Tips for Successful Ovulation Tracking
- Track for 3+ cycles before relying on patterns: Cycles vary month-to-month. Establish your personal patterns before using data for conception or contraception.
- Use multiple methods: Combine calendar tracking, cervical mucus observation, and OPKs for highest accuracy. Single-method tracking is less reliable.
- Check cervical mucus consistently: Observe daily—check toilet paper after urination or insert fingers to cervix. Track texture, color, amount.
- Chart BBT immediately upon waking: Keep thermometer at bedside. Measure before any activity, talking, or drinking. Chart at same time daily.
- Start OPK testing at the right time: Begin 2-3 days before expected ovulation (cycle length - 17 days). Test daily until positive, then have intercourse that day and next 2 days.
- Don't stress about "perfect" timing: Intercourse every 2-3 days throughout cycle ensures sperm is present whenever ovulation occurs without pressure.
- Account for cycle variations: Stress, illness, travel, weight changes, and medications can delay ovulation. Track actual signs rather than assuming regular timing.
- Avoid lubricants that harm sperm: Most commercial lubricants reduce sperm motility. Use "fertility-friendly" lubricants (Pre-Seed) or none at all.
- Both partners should optimize health: Male fertility matters equally. Partner should avoid excessive heat (hot tubs), wear loose underwear, maintain healthy weight, and limit alcohol/smoking.
- Stay patient and positive: Healthy couples under 35 have ~20-25% pregnancy chance per cycle. 85% conceive within one year—most pregnancies take multiple months.
Medical Disclaimer
This ovulation calculator provides estimates based on average cycle patterns and cannot account for individual variations, irregular cycles, anovulatory cycles, or medical conditions affecting ovulation. Calculated ovulation dates and fertile windows are approximations—actual ovulation timing varies individually and monthly. This calculator is NOT a reliable contraception method; do not use for pregnancy prevention. Women with irregular cycles, PCOS, thyroid disorders, perimenopause, recent childbirth/breastfeeding, or hormonal contraception may have unpredictable or absent ovulation not captured by standard calculations. This tool cannot diagnose fertility issues, confirm ovulation occurrence, or predict pregnancy success. If experiencing irregular periods, absence of ovulation signs, or difficulty conceiving after appropriate trying periods (12 months under age 35, 6 months over age 35), consult reproductive endocrinologists or fertility specialists for proper evaluation including ovulation confirmation tests (ultrasound, blood hormone levels), ovarian reserve assessment, and comprehensive fertility workup. This calculator is for educational and tracking purposes only, not medical advice, diagnosis, or treatment. Always consult healthcare providers for personalized reproductive health guidance.
About the Author
Adam
Co-Founder @ RevisionTown
Math Expert specializing in various curricula including IB, AP, GCSE, IGCSE, and more
Ovulation and Conception
Ovulation in humans is the process by which ovarian follicles rupture and release one or more mature eggs from the ovaries. On average, ovulation occurs within the 4 days before or after the midpoint of a woman’s menstrual cycle (14 days before the start of a woman’s next menstrual period).
Day 10-18 of the menstrual cycle (on average) is the most fertile phase of the menstrual cycle. This is important when trying to conceive because fertilization of the egg can only occur for 12-24 hours after release during part of the luteal phase, when a mature egg travels through the fallopian tubes towards the uterus. Since sperm can survive inside a woman’s body for up to five days, regular sex five days before and on the day of ovulation can improve the likelihood of conception. If fertilized, the egg will implant in the uterus 6-12 days later. Otherwise, menstruation occurs, and blood and mucosal tissue from the inner lining of the uterus is expelled.
Ovulation Prediction
Many people would like to predict their ovulation date, mostly to increase their chances of getting pregnant. The following are a few common methods for doing so.
Tracking Menstrual Cycles
This ovulation calculator uses the method of tracking menstrual cycles in order to predict when ovulation occurs. Since day 10-18 of the menstrual cycle is typically the most fertile phase of the menstrual cycle, women with regular cycles can fairly easily determine when they are ovulating and most likely to conceive. Menstrual cycles vary between women however, and a person without a 28-day menstrual cycle may need to track their menstrual cycle to more accurately determine when ovulation might occur.
The first day of the menstrual cycle is the day that bleeding starts, and it ends the day that bleeding starts again. It can be helpful to maintain a menstrual calendar to determine how regular your periods are. If they are irregular, other methods may be more accurate for estimating when ovulation will occur.
Tracking Basal Body Temperatures
Basal body temperature (BBT) is measured using a special thermometer. This is your temperature when you first wake up in the morning. BBT is generally at the lowest level right before ovulation occurs. It starts rising by about ½ a degree a day during ovulation. Tracking BBT over a few months can help you determine when you are ovulating and most likely to be able to conceive. However, there are other factors involved that can affect your BBT, such as having a cold or infection. In these cases, measuring BBT would likely not be a good indicator of ovulation.
Ovulation Kits
It is also possible to use an over-the-counter ovulation test that tests for a surge in some specific hormones that precede ovulation by 24-48 hours. While these tests are 99% accurate in detecting the specific hormones, they cannot guarantee when exactly ovulation will occur within the two-day period. These tests typically measure the level of luteinizing hormone (LH), which, when released in high quantities (and under other conditions), triggers ovulation.
There are also ovulation predictor kits that can test changes in the estrogen level in saliva or salts in the sweat, which change during the month and can be related to the menstrual cycle. These changes generally occur earlier than the hormonal changes (LH increase), and can therefore predict ovulation earlier. Unlike LH tests, this does require more preparation in terms of tracking the levels of these markers to determine a baseline level.