
⚠️ Disclaimer: The information provided in this article is for educational purposes only and does not constitute medical advice. RevisionTown does not provide diagnosis, treatment, or medical recommendations. Always consult a qualified healthcare professional regarding any medical condition, symptoms, or concerns.
Read More – 🏥 Medical Disclaimer
Comprehensive Report on Ulcerative Colitis
1. Overview
What is ulcerative colitis?
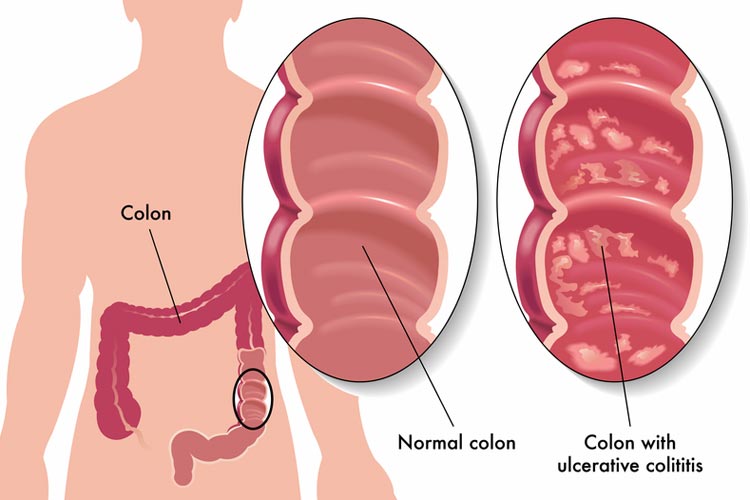
Ulcerative colitis (UC) is a chronic, relapsing-remitting inflammatory bowel disease characterized by continuous inflammation and ulceration of the colonic mucosa. It begins in the rectum and extends proximally in a continuous manner to involve variable lengths of the colon, with inflammation limited to the mucosal and submucosal layers of the intestinal wall. This distinguishes it from Crohn’s disease, which can affect any part of the gastrointestinal tract with discontinuous lesions and transmural inflammation.
Affected body parts/organs
Ulcerative colitis primarily affects the large intestine (colon) and rectum, with distinct distribution patterns:
- Proctitis: Limited to the rectum (30-40% of patients)
- Left-sided colitis: Extends from the rectum up to the splenic flexure (30-40%)
- Extensive colitis: Extends beyond the splenic flexure but not to the cecum (10-20%)
- Pancolitis: Involves the entire colon, from rectum to cecum (20-30%)
While UC is primarily a disease of the colon and rectum, it can also present with extraintestinal manifestations affecting:
- Joints: Arthritis, sacroiliitis, ankylosing spondylitis
- Skin: Erythema nodosum, pyoderma gangrenosum
- Eyes: Episcleritis, uveitis
- Liver and biliary tract: Primary sclerosing cholangitis, autoimmune hepatitis
- Vascular system: Thromboembolism
- Bones: Decreased bone mineral density
Prevalence and significance
Ulcerative colitis is a global disease with significant regional variations in prevalence:
Epidemiology:
- Global prevalence: 7.6-245 cases per 100,000 persons
- Incidence: 1.2-20.3 cases per 100,000 person-years
- Age distribution: Bimodal, with peaks between 15-30 years and 50-70 years
- Gender distribution: Slightly more common in males in some regions, equal in others
Significance:
- Economic burden: Annual direct medical costs of $8,000-$14,000 per patient in developed countries
- Quality of life impact: Significant reduction in health-related quality of life during active disease
- Work productivity: 35-50% reduction during active disease phases
- Hospitalization: Approximately 20-30% of patients require hospitalization for severe flares
- Surgery: 15-30% of patients will require colectomy during their lifetime
- Colorectal cancer risk: Increased 2.4-fold compared to the general population
- Social impact: Affects education, career choices, relationships, and family planning
Ulcerative colitis represents a substantial burden on healthcare systems worldwide, with increasing incidence in newly industrialized countries, highlighting its importance as a global health challenge.
2. History & Discoveries
Early descriptions and identification
The history of ulcerative colitis as a recognized medical condition spans several centuries:
- Early references: Possible descriptions in ancient Greek and Roman medical texts
- 1859: First clear clinical description by British physician Sir Samuel Wilks
- 1875: Detailed characterization by Wilks and Walter Moxon, distinguishing UC from infectious colitis
- 1909: First comprehensive monograph on ulcerative colitis by Sir Arthur Hurst in England
- 1913: J.Y. Brown published the first American account of ulcerative colitis
Key historical figures and discoveries
Several physicians and scientists have made significant contributions to understanding ulcerative colitis:
- Sir Samuel Wilks (1859): First described “idiopathic colitis” as a distinct clinical entity
- Sir Arthur Hurst (1909-1931): Pioneered the use of sigmoidoscopy for diagnosis and described the clinical course
- Burrill Crohn, Leon Ginzburg, and Gordon Oppenheimer (1932): Distinguished Crohn’s disease from ulcerative colitis
- Sidney Truelove and Leslie Witts (1955): Developed the first systematic classification of disease severity and introduced corticosteroid therapy
- Joseph Kirsner (1950s-1980s): Advanced understanding of disease pathophysiology and treatment
- Marvin Sleisenger (1960s-1970s): Contributed to the knowledge of extraintestinal manifestations
- Daniel Present and Burton Korelitz (1960s-1980s): Pioneered immunomodulator therapy
Major breakthroughs in research and treatment
The understanding and management of ulcerative colitis has evolved significantly:
- 1930s: Introduction of sulfasalazine by Nanna Svartz
- 1950s: First successful use of corticosteroids by Truelove and Witts
- 1950s-1960s: Improved surgical techniques with the development of ileal pouch-anal anastomosis (IPAA)
- 1960s-1970s: Recognition of genetic predisposition and familial clustering
- 1970s-1980s: Introduction of immunomodulators (azathioprine, 6-mercaptopurine)
- 1980s-1990s: Development of mesalamine formulations
- 1990s-2000s: Identification of the role of cytokines, leading to biologic therapies
- 1998: First anti-TNF therapy (infliximab) approved for Crohn’s disease, later for UC
- 2000s-2010s: Genome-wide association studies identifying genetic risk loci
- 2010s-2020s: Development of gut-selective anti-integrin therapies and small molecule inhibitors
- 2020s: Increasing focus on precision medicine and a treat-to-target approach
Evolution of medical understanding
The conceptual framework for ulcerative colitis has transformed dramatically:
- Early theories (pre-1900s): Considered primarily infectious or dietary in origin
- Early 20th century: Recognized as a distinct non-infectious inflammatory condition
- Mid-20th century: Psychological factors emphasized (psychosomatic theory)
- 1960s-1970s: Recognition of immune system involvement
- 1980s-1990s: Appreciation of mucosal barrier dysfunction and bacterial interactions
- 1990s-2000s: Understanding of cytokine networks in pathogenesis
- 2000s-2010s: Genetic associations and environmental influences characterized
- 2010s-present: Integration of microbiome science, immunology, genetics, and environmental factors
- Current paradigm: Complex gene-environment interaction causing dysregulated immune response to intestinal microbiota in genetically susceptible individuals
This historical progression reflects the transition from considering ulcerative colitis as a mysterious disorder to understanding it as a multifactorial disease with complex interactions between genetics, environment, immune function, and gut microbiota.
3. Symptoms
Early symptoms
The initial presentation of ulcerative colitis can be variable in severity and may develop gradually over weeks to months:
Cardinal early symptoms:
- Bloody diarrhea: Most characteristic feature, present in 90% of patients
- Rectal urgency: Sudden, intense need to have a bowel movement
- Tenesmus: Painful sensation of incomplete bowel evacuation
- Rectal bleeding: From small amounts to significant bleeding
- Abdominal discomfort: Typically left-sided, relieved with defecation
- Increased stool frequency: Usually 4-8 bowel movements per day
Systemic early symptoms:
- Fatigue: Common but often overlooked
- Low-grade fever: Present in 30-40% of patients
- Weight loss: Usually modest (2-5 kg) in early disease
- Anorexia: Decreased appetite
- Malaise: General feeling of discomfort or illness
Symptom patterns by disease extent:
- Proctitis: Primarily rectal symptoms (bleeding, urgency, tenesmus) with normal stool frequency
- Left-sided colitis: More prominent diarrhea with abdominal discomfort and urgency
- Extensive/pancolitis: More severe symptoms with systemic features more common
Advanced-stage symptoms
As the disease progresses or during severe flares, symptoms become more pronounced:
Severe intestinal symptoms:
- Severe bloody diarrhea: 10+ bowel movements daily
- Nocturnal diarrhea: Awakening for bowel movements
- Significant rectal bleeding: Sometimes passing pure blood
- Severe abdominal pain: More prominent than in mild disease
- Abdominal distension: May indicate toxic megacolon
- Severe urgency and incontinence: Significantly impacting quality of life
- Perianal complications: Less common than in Crohn’s disease but can occur
Systemic manifestations:
- High fever: > 38.5°C (101.3°F)
- Tachycardia: Rapid heart rate
- Significant weight loss: Sometimes >10% of body weight
- Dehydration: Due to fluid losses
- Anemia: Due to chronic blood loss and inflammation
- Hypoalbuminemia: Due to protein loss and malnutrition
- Electrolyte abnormalities: Particularly hypokalemia
Extraintestinal manifestations: These can occur at any disease stage but are more common in advanced or longstanding disease:
- Musculoskeletal: Peripheral arthritis, axial spondyloarthritis
- Dermatological: Erythema nodosum, pyoderma gangrenosum
- Ocular: Episcleritis, uveitis, iritis
- Hepatobiliary: Primary sclerosing cholangitis, fatty liver disease
- Hematologic: Anemia, thromboembolism, hypercoagulable state
- Metabolic: Decreased bone mineral density, growth failure in children
Symptom progression and patterns
Ulcerative colitis typically follows a relapsing and remitting course:
Disease patterns:
Relapsing-remitting: Most common pattern (70-80% of patients)
- Alternating periods of active disease and remission
- Remission periods can last months to years
- Flares can be triggered by specific factors or occur spontaneously
Chronically active: Persistent symptoms despite standard therapy (10-15%)
- Continuous disease activity of varying severity
- Often requires escalation to advanced therapies
Fulminant colitis: Severe, rapidly progressive form (<5%)
- Medical emergency requiring hospitalization
- Risk of toxic megacolon and perforation
Quiescent disease: Extended periods of remission (10-20%)
- Minimal or no symptoms for years
- May still have low-grade inflammation on endoscopy
Factors affecting progression:
- Disease extent: Pancolitis associated with more severe course
- Disease severity at diagnosis: Severe initial presentation predicts more aggressive disease
- Age at onset: Earlier onset often associated with more severe disease
- Response to initial therapy: Poor response predicts more difficult disease course
- Healing of mucosa: Complete mucosal healing associated with sustained remission
Long-term progression:
- Disease extension: About 20-30% of patients with limited disease will progress to more extensive involvement over 10 years
- Risk of colorectal cancer: Increases with disease duration, particularly after 8-10 years
- Medication effects: Long-term steroid exposure can lead to additional complications
- Surgical outcomes: Approximately 30% of patients will ultimately require colectomy, although this rate has been decreasing with modern therapies
Understanding the variable presentation and progression of symptoms is crucial for timely diagnosis, appropriate management, and monitoring of disease activity in ulcerative colitis patients.
4. Causes
Biological mechanisms
Ulcerative colitis results from complex interactions between genetic susceptibility, environmental factors, intestinal microbiota, and immune system dysfunction:
Mucosal immune dysregulation:
- Barrier dysfunction:
- Defective intestinal epithelial tight junctions
- Increased intestinal permeability
- Impaired mucus production (defective MUC2 expression)
- Reduced antimicrobial peptide production
- Innate immune responses:
- Altered pattern recognition receptor function (TLRs, NOD-like receptors)
- Impaired epithelial cell autophagy
- Dysregulated inflammasome activation
- Enhanced innate lymphoid cell activation, particularly ILC2s
- Adaptive immunity:
- Polarization toward Th2 cytokine profile (IL-4, IL-5, IL-13)
- Increased IL-17-producing T cells
- Defective regulatory T cell function
- Altered B cell responses with auto-antibody production
- Cytokine networks:
- Increased pro-inflammatory cytokines (TNF-α, IL-6, IL-1β)
- Elevated IL-13 production by non-classical natural killer T cells
- Dysregulated IL-10 signaling (important anti-inflammatory cytokine)
- JAK-STAT signaling pathway activation
- Tissue damage mechanisms:
- Enhanced production of matrix metalloproteinases
- Increased reactive oxygen species
- Neutrophil extracellular trap formation
- Aberrant epithelial cell death (apoptosis, necroptosis)
Microbiome alterations:
- Reduced microbial diversity (dysbiosis)
- Decreased abundance of anti-inflammatory commensal bacteria (e.g., Faecalibacterium prausnitzii)
- Increased pathobionts (bacteria with inflammatory potential)
- Altered short-chain fatty acid production
- Disrupted bile acid metabolism
- Impaired intestinal barrier-microbiome interactions
Genetic and hereditary factors
Ulcerative colitis has a significant genetic component:
Heritability:
- 10-25% of patients have a family history of IBD
- Monozygotic twin concordance: 10-15% (compared to 4% in dizygotic twins)
- First-degree relatives have a 10-15 fold increased risk
- Overall genetic contribution estimated at 40-60%
Genetic associations:
- Over 200 genetic risk loci identified through genome-wide association studies (GWAS)
- Many loci are shared with Crohn’s disease, but some are UC-specific
Key genetic pathways:
Epithelial barrier function:
- HNF4A (transcription factor regulating colonic epithelial cells)
- CDH1 (E-cadherin, involved in cell-cell adhesion)
- LAMB1 (laminin beta 1, basement membrane component)
- GNA12 (involved in tight junction regulation)
Immune regulation:
- IL23R (interleukin-23 receptor pathway)
- IL10 (anti-inflammatory cytokine)
- TNFRSF14, TNFRSF9 (TNF receptor superfamily members)
- JAK2, STAT3 (signaling pathway components)
Autophagy: Less prominently involved in UC compared to Crohn’s disease
HLA associations:
- HLA-DRB1*0103 (strongest association in Caucasians)
- HLA-DR2 (DRB1*1502) in East Asian populations
Genetic differences from Crohn’s disease:
- NOD2/CARD15 mutations (strongly associated with Crohn’s) are not associated with UC
- UC shares more genetic risk loci with other autoimmune diseases
- UC has stronger associations with HLA loci than Crohn’s disease
Environmental triggers and risk factors
Multiple environmental factors influence ulcerative colitis risk and disease course:
Protective factors:
- Appendectomy: 69% reduced risk, particularly when performed for appendicitis before age 20
- Cigarette smoking: Uniquely protective in UC (unlike in Crohn’s disease)
- Breastfeeding: Both as recipient in infancy and providing as a mother
- Regular physical activity: Moderate exercise appears protective
Risk-increasing factors:
- Former smoking: Risk increases upon smoking cessation
- Air pollution: Particularly nitrogen dioxide and particulate matter
- Oral contraceptive use: Modest association in some studies
- Antibiotic exposure: Particularly in childhood
- Non-steroidal anti-inflammatory drugs (NSAIDs): Can trigger flares and possibly increase risk
- Diet: Western diet high in refined sugars, fats, and low in fiber
Infectious triggers:
- No consistent specific pathogen identified
- Acute gastroenteritis may trigger initial presentation in susceptible individuals
- Clostridium difficile infection can trigger flares in established disease
Stress and psychological factors:
- Psychological stress may trigger flares in established disease
- Bidirectional brain-gut interaction with inflammation affecting mood and stress affecting inflammation
- Early life stress may increase risk in susceptible individuals
Dietary components:
- Emulsifiers and food additives: May disrupt mucus barrier and alter microbiome
- High-fat diet: Associated with pro-inflammatory changes in gut microbiota
- Low fiber intake: Leads to reduced production of beneficial short-chain fatty acids
- Artificial sweeteners: May alter microbiome composition and function
- Sulfur-containing foods: May promote growth of sulfate-reducing bacteria in susceptible individuals
The development of ulcerative colitis likely requires a complex interplay between multiple genetic and environmental factors, with different combinations of factors relevant in different individuals. This heterogeneity underlies the variable disease presentation, course, and treatment response observed in clinical practice.
5. Risk Factors
Demographic risk factors
Ulcerative colitis affects specific demographic groups with distinct patterns:
Age:
- Peak incidence: Bimodal distribution
- First peak: 15-30 years of age
- Second peak: 50-70 years of age
- Pediatric UC: Accounts for 15-20% of all cases
- Often more extensive disease
- Higher risk of colectomy
- Elderly-onset UC: After age 60
- Often milder course
- More responsive to therapy
- Lower surgery risk
Sex/Gender:
- Overall ratio: Slight male predominance (1.1-1.5:1) in developed countries
- Age-specific variations:
- Female predominance in adolescence
- Male predominance in early adulthood
- More equal distribution in older adults
- Course differences:
- Females more likely to experience extraintestinal manifestations
- Pregnancy and hormonal factors affect disease course in women
Race/Ethnicity:
- Highest incidence: Historically in Caucasians, particularly Ashkenazi Jews
- Rapidly increasing: In Asian populations, Hispanic populations
- Lowest incidence: Traditionally in African and Asian populations
- Clinical differences:
- More extensive disease in African Americans
- Higher rate of primary sclerosing cholangitis in Northern Europeans
- Lower surgery rates in Asian populations
Geographic variations:
- North-South gradient: Higher rates in northern latitudes in both hemispheres
- East-West gradient: Historically higher in Western countries
- Urbanization effect: Higher in urban vs. rural areas
- Migration effect: Migrants adopt risk of host country within 1-2 generations
Socioeconomic status:
- Higher incidence: In higher socioeconomic groups
- Education level: Positive correlation with UC risk
- “Hygiene hypothesis”: Cleaner environments may predispose to immune dysregulation
- Healthcare access: Affects diagnosis rates and treatment outcomes
Lifestyle and environmental risk factors
Smoking:
- Current smoking: Protective effect (50-70% reduced risk)
- Former smoking: Increased risk compared to never-smokers
- Dose effect: Greater protection with heavier smoking
- Mechanisms: Nicotine effects on mucus, nitric oxide, cytokines
- Clinical relevance: Smoking cessation can trigger disease onset or worsen established UC
Diet:
- Western diet pattern:
- High in refined carbohydrates, saturated fats, and ultra-processed foods
- Low in fruits, vegetables, and fiber
- Associated with 2-3 fold increased risk
- Specific dietary components:
- Red meat (particularly processed): Modest risk increase
- Sulfur-containing foods: May increase risk in susceptible individuals
- Low fiber intake: Associated with increased risk
- High sugar consumption: Associated with increased risk
- Protective dietary factors:
- Mediterranean diet pattern
- High omega-3 fatty acids
- High fruit and vegetable intake
Medication exposure:
- Antibiotics: Early-life exposure associated with 40-80% increased risk
- NSAIDs: Can trigger flares and possibly increase initial risk
- Oral contraceptives: Modest risk increase in some studies
- Isotretinoin: Controversial association, data inconsistent
- Proton pump inhibitors: Possible association through microbiome effects
Early-life factors:
- Breastfeeding: Protective effect when received in infancy
- Cesarean delivery: Modest increase in risk
- Early-life infections: Mixed evidence, may influence risk
- Urban upbringing: Associated with higher risk
- Childhood hygiene: “Too clean” environments may increase risk
Environmental exposures:
- Air pollution: Nitrogen dioxide and particulate matter exposure increases risk
- Water pollution: Potential risk from microplastics and chemical contaminants
- Shift work: Disrupted circadian rhythms associated with increased risk
- Stress: Psychological stress may influence disease onset and flares
- Sleep disruption: Poor sleep quality associated with increased inflammation
Genetic and pre-existing condition risk factors
Genetic risk factors:
- Family history: 10-25% of patients have a relative with IBD
- First-degree relative risk: 10-15 fold increased risk
- Specific genetic loci: Over 200 identified through GWAS
- Highest genetic risk: Individuals with multiple risk variants
- Ethnic variation: Different genetic risk profiles across populations
- Polygenic risk scores: Emerging tool for risk stratification
Pre-existing conditions:
- Autoimmune diseases:
- Primary sclerosing cholangitis: Strong association, affects 2-10% of UC patients
- Ankylosing spondylitis: Increased risk of UC
- Psoriasis: Associated with increased UC risk
- Autoimmune thyroid disease: More common in UC patients
- Intestinal conditions:
- History of appendectomy: Protective if performed for appendicitis before age 20
- Prior gastrointestinal infections: May trigger disease onset
- Irritable bowel syndrome: May precede diagnosis or coexist
- Other conditions:
- Depression and anxiety: Bidirectional relationship with UC
- Atopic conditions (asthma, eczema): Modest association
- Obstructive sleep apnea: Associated with increased inflammation
The microbiome as a risk factor:
- Dysbiosis: Altered microbiome composition precedes and predicts disease
- Reduced diversity: Associated with increased risk
- Decreased beneficial bacteria: Particularly Faecalibacterium prausnitzii
- Pathobiont expansion: Increased adherent-invasive E. coli and other species
- Functional changes: Altered short-chain fatty acid production
- Viral and fungal components: Altered virome and mycobiome also implicated
Protective factors and risk modification:
- Regular exercise: 30-40% risk reduction with regular physical activity
- Vitamin D sufficiency: May reduce risk and improve disease course
- Adequate sleep: 7-8 hours associated with lower risk
- Stress management: Mindfulness and stress reduction may be beneficial
- Dietary approaches: Mediterranean diet pattern may reduce risk
The constellation of risk factors varies between individuals, supporting the concept of ulcerative colitis as a heterogeneous disorder with multiple subtypes defined by different combinations of genetic and environmental influences. This heterogeneity has important implications for personalized approaches to prevention, diagnosis, and management.
6. Complications
Intestinal complications
Acute severe ulcerative colitis:
- Prevalence: Affects 10-15% of patients during their disease course
- Definition: ≥6 bloody stools/day with systemic symptoms
- Systemic features: Fever, tachycardia, anemia, elevated inflammatory markers
- Mortality: 1-2% despite modern management
- Predictors: Extensive disease, hypoalbuminemia, elevated CRP, deep ulceration
Toxic megacolon:
- Incidence: Complicates 1-5% of acute severe colitis
- Pathophysiology: Transmural inflammation with colonic dilatation
- Diagnostic criteria: Colonic dilatation >6cm with systemic toxicity
- Mortality rate: 3-8% with modern management
- Risk factors: Hypokalemia, opioid use, anticholinergics, barium enema
Perforation:
- Incidence: 1-3% of hospitalized patients with severe colitis
- Mortality: Up to 40% despite surgical intervention
- Warning signs: Abdominal rigidity, severe pain, pneumoperitoneum
- Risk factors: Toxic megacolon, severe ulceration, corticosteroid therapy
Hemorrhage:
- Significant bleeding: Occurs in 3-5% of patients
- Massive hemorrhage: Rare (1-2%) but potentially life-threatening
- Management: Usually medical, rarely requires colectomy
- Predictors: Severe pancolitis, deep ulceration
Strictures:
- Prevalence: 3-10% of long-standing UC
- Locations: Most commonly in rectosigmoid region
- Malignant potential: Must be distinguished from malignant strictures
- Management: Endoscopic dilation, surveillance, or surgery
Colorectal cancer:
- Overall risk: 2-4 fold increase compared to general population
- Cumulative incidence: 2% at 10 years, 8% at 20 years, 18% at 30 years
- Risk factors:
- Disease duration (particularly >8 years)
- Extensive colitis
- Persistent inflammation
- Primary sclerosing cholangitis (5-fold additional risk)
- Family history of colorectal cancer
- Prevention: Surveillance colonoscopy, anti-inflammatory therapy
- Prognosis: Improved with surveillance detection
Pseudopolyps:
- Prevalence: 10-20% of patients
- Pathophysiology: Islands of intact mucosa surrounded by ulceration
- Clinical significance: Marker of severe inflammation, can complicate cancer surveillance
- Malignant potential: Not pre-malignant themselves but indicate higher risk
Extraintestinal complications
Musculoskeletal:
- Peripheral arthritis:
- Type 1 (pauciarticular): Affects 5-10%, parallels intestinal activity
- Type 2 (polyarticular): Affects 3-5%, independent of intestinal activity
- Axial arthropathies:
- Ankylosing spondylitis: 2-6%
- Sacroiliitis: 10-15%
- Osteoporosis and osteopenia:
- Affects 20-50% of patients
- Multifactorial: inflammation, steroid use, malnutrition, vitamin D deficiency
Dermatological:
- Erythema nodosum:
- Prevalence: 3-10%
- Painful, raised, red lesions typically on extensor surfaces
- Usually parallels intestinal disease activity
- Pyoderma gangrenosum:
- Prevalence: 0.5-2%
- Severe, painful ulcerating lesions
- Often independent of intestinal disease activity
- Sweet’s syndrome: Rare neutrophilic dermatosis
- Psoriasis: 3-fold increased risk in UC patients
Ocular:
- Episcleritis: 1-5%, parallels disease activity
- Uveitis: 0.5-3%, can be independent of disease activity
- Scleritis: Less common but more serious
- Conjunctivitis: Most common but non-specific
Hepatobiliary:
- Primary sclerosing cholangitis (PSC):
- Affects 2-10% of UC patients
- Progressive bile duct inflammation and fibrosis
- Often asymptomatic until advanced
- Increases cholangiocarcinoma and colorectal cancer risk
- May persist or develop after colectomy
- Fatty liver disease: Common, multifactorial
- Autoimmune hepatitis: Increased prevalence
- Cholelithiasis: Increased risk due to altered bile salt metabolism
Hematologic:
- Anemia:
- Iron deficiency: Most common (30-50% of patients)
- Anemia of chronic disease: Common in active disease
- Vitamin B12/folate deficiency: Less common
- Hypercoagulable state:
- 3-fold increased risk of venous thromboembolism
- Higher risk during flares and hospitalization
- Risk factors: Inflammation, immobility, dehydration, corticosteroids
Metabolic and nutritional:
- Malnutrition: 20-85% depending on disease severity
- Weight loss: Common during active disease
- Growth failure in children: 10-15% of pediatric patients
- Vitamin deficiencies: D, K, B12, folate
- Mineral deficiencies: Iron, zinc, magnesium, selenium
Renal and urological:
- Nephrolithiasis: Increased risk, particularly with ileal involvement
- Urinary tract obstruction: Rare complication of severe inflammation
- Drug-induced nephrotoxicity: From aminosalicylates or other medications
Psychosocial complications and mortality
Psychological impact:
- Depression: Affects 20-30% of patients
- Anxiety: Affects 30-50% of patients
- Stress-related symptoms: Common, can worsen disease course
- Sleep disorders: Affect 60-80% during active disease
- Impaired quality of life: Particularly during active disease
Social and economic complications:
- Work productivity: 35-50% reduction during flares
- Employment challenges: Higher unemployment rates
- Educational impact: Increased absenteeism, academic underachievement
- Sexual dysfunction: 45-60% report impact on sexual health
- Relationship stress: Higher divorce rates in some studies
- Financial burden: Both direct medical costs and lost productivity
Treatment-related complications:
- Corticosteroid-related: Osteoporosis, diabetes, hypertension, cataracts
- Immunomodulator-related: Increased infection risk, bone marrow suppression
- Biologic therapy-related: Infection risk, infusion reactions, skin manifestations
- Surgical complications: Pouchitis, anastomotic leakage, small bowel obstruction
Mortality:
- Overall mortality: Slight increase compared to general population (SMR 1.1-1.4)
- Causes of excess mortality:
- Colorectal cancer
- Complications of surgery
- Thromboembolic events
- Adverse effects of medications
- Primary sclerosing cholangitis and related complications
- Age-specific mortality:
- Higher relative mortality in younger patients
- Nearly normal life expectancy with modern management
- Time trends: Declining mortality rates in recent decades
The broad spectrum of complications associated with ulcerative colitis highlights the importance of a comprehensive, multidisciplinary approach to patient care that addresses not only intestinal manifestations but also extraintestinal, psychological, and social dimensions of the disease.
7. Diagnosis & Testing
Clinical evaluation
The diagnostic approach to ulcerative colitis begins with thorough clinical assessment:
History taking:
- Symptoms: Duration, severity, pattern of bowel movements, presence of blood
- Associated symptoms: Abdominal pain, weight loss, fever, extraintestinal manifestations
- Family history: IBD, colorectal cancer, autoimmune diseases
- Medication history: Antibiotics, NSAIDs, oral contraceptives
- Smoking history: Current, former, or never smoker
- Recent travel: Infectious etiology consideration
- Diet history: Food intolerances, dietary patterns
- Previous treatments: Response to antibiotics, anti-diarrheals
- Impact on quality of life: Sleep, work, social activities
Physical examination:
- Vital signs: Temperature, heart rate, blood pressure, weight
- Abdominal examination: Tenderness (typically left-sided), distension, bowel sounds
- Digital rectal examination: Assess for perianal disease, rectal tenderness, blood
- Extraintestinal manifestations:
- Skin: Erythema nodosum, pyoderma gangrenosum
- Joints: Arthritis, limited spinal mobility
- Eyes: Episcleritis, uveitis
- Oral: Aphthous ulcers
- Nutritional status: Weight loss, muscle wasting, edema
Symptom assessment tools:
- Mayo Score: Combines stool frequency, rectal bleeding, endoscopic findings, physician assessment
- Ulcerative Colitis Activity Index (UCAI): Quantifies symptoms and signs
- Simple Clinical Colitis Activity Index (SCCAI): Patient-reported outcome measure
- Patient-Reported Outcomes Measurement Information System (PROMIS): Quality of life assessment
Laboratory testing
Blood tests:
- Complete blood count:
- Anemia: Present in 60-80% of patients with active disease
- Thrombocytosis: Marker of inflammation
- Leukocytosis: Indicates inflammation or infection
- Inflammatory markers:
- Erythrocyte sedimentation rate (ESR): Elevated in 60-80%
- C-reactive protein (CRP): Elevated in 50-70%, less consistently than in Crohn’s
- Fecal calprotectin: Highly sensitive marker of intestinal inflammation
- Fecal lactoferrin: Alternative marker of neutrophilic inflammation
- Biochemical profile:
- Albumin: Decreased in severe disease
- Electrolytes: Abnormalities common in severe colitis
- Liver function tests: May be abnormal with PSC or drug effects
- Renal function: Baseline and monitoring
Serological markers:
- pANCA (perinuclear anti-neutrophil cytoplasmic antibody):
- Positive in 60-70% of UC patients
- Specificity 84-95%
- Not routinely used for diagnosis but can help differentiate from Crohn’s
- Anti-Saccharomyces cerevisiae antibodies (ASCA):
- Usually negative in UC (vs. positive in Crohn’s)
- May help differentiate indeterminate colitis
- Newer antibody panels:
- Anti-CBir1 (anti-flagellin)
- Anti-OmpC (outer membrane porin C)
- Limited utility in routine clinical practice
Stool tests:
- Fecal calprotectin:
- Sensitivity 80-90% for intestinal inflammation
- Useful for diagnosis, monitoring, and predicting relapse
- Levels correlate with endoscopic activity
- Microbiological studies:
- Bacterial culture: Rule out infectious colitis
- C. difficile toxin: Essential to exclude infection
- Ova and parasites: Particularly with travel history
- Cytomegalovirus (CMV): Consider in severe or refractory cases
- Occult blood testing: Usually positive but nonspecific
Endoscopy and imaging
Endoscopic procedures:
- Flexible sigmoidoscopy:
- Often sufficient for initial diagnosis
- Safer in acute severe colitis
- Allows visualization of rectosigmoid region
- Colonoscopy:
- Gold standard for diagnosis and assessment of extent
- Contraindicated in severe acute colitis due to perforation risk
- Classic findings:
- Continuous inflammation from rectum extending proximally
- Erythema, granularity, friability, spontaneous bleeding
- Loss of vascular pattern
- Ulcerations (typically superficial)
- Clear demarcation between involved and uninvolved mucosa
- Chromoendoscopy:
- Dye-spray technique (indigo carmine or methylene blue)
- Enhances detection of dysplasia in surveillance
- Recommended for cancer surveillance in longstanding colitis
- Narrow-band imaging:
- Advanced endoscopic technique
- Enhances mucosal and vascular patterns
- May improve dysplasia detection
Histopathology:
- Key features:
- Chronic inflammation confined to mucosa and submucosa
- Crypt architectural distortion
- Crypt abscesses
- Goblet cell depletion
- Basal plasmacytosis
- Lamina propria infiltration with neutrophils, lymphocytes, plasma cells
- Biopsy protocol:
- Multiple biopsies from inflamed and non-inflamed areas
- Step biopsies every 10cm for surveillance
- Targeted biopsies of suspicious lesions
- Dysplasia classification:
- Negative for dysplasia
- Indefinite for dysplasia
- Low-grade dysplasia
- High-grade dysplasia
Imaging studies:
- Plain abdominal radiography:
- Useful in acute severe colitis
- Evaluates for toxic megacolon (colonic dilatation >6cm)
- May detect perforation
- CT scan:
- Not primary diagnostic tool
- Useful in acute complications
- Findings: Bowel wall thickening, pericolic fat stranding
- MRI:
- Limited role in UC compared to Crohn’s disease
- Useful for extraintestinal manifestations
- MR enterography not routinely needed
- Transabdominal ultrasound:
- Increasing use in some centers
- Can detect bowel wall thickening
- Limited by operator experience and patient factors
Novel diagnostic techniques:
- Confocal laser endomicroscopy:
- Real-time microscopic imaging of mucosa
- May improve dysplasia detection
- Endocytoscopy:
- Ultra-high magnification of mucosal surfaces
- Research tool, not widely available
- Molecular imaging:
- Fluorescent probes targeting specific molecules
- Under research development
Differential diagnosis
Several conditions can mimic ulcerative colitis and must be excluded:
Infectious colitis:
- Bacterial: Salmonella, Shigella, Campylobacter, E. coli, C. difficile
- Parasitic: Entamoeba histolytica, Schistosomiasis
- Viral: Cytomegalovirus, Herpes simplex virus
- Mycobacterial: Tuberculosis
Other inflammatory bowel diseases:
- Crohn’s colitis
- Indeterminate colitis (10-15% of IBD cases)
- Microscopic colitis (lymphocytic, collagenous)
- Diversion colitis
Vascular disorders:
- Ischemic colitis
- Radiation colitis
- Vasculitis
Medication-induced colitis:
- NSAID-associated colitis
- Immune checkpoint inhibitor colitis
- Mycophenolate-associated colitis
Other conditions:
- Irritable bowel syndrome
- Diverticular disease-associated colitis
- Solitary rectal ulcer syndrome
- Segmental colitis associated with diverticulosis
- Behçet’s disease
Distinguishing UC from Crohn’s colitis:
| Feature | Ulcerative Colitis | Crohn’s Colitis |
|---|---|---|
| Distribution | Continuous, rectum to proximal | Skip lesions, rectal sparing common |
| Depth | Mucosa/submucosa only | Transmural |
| Strictures | Rare | Common |
| Fistulas | Very rare | Common |
| Perianal disease | Uncommon | Common (40-50%) |
| Granulomas | Absent | Present in 30-60% |
| Endoscopy | Diffuse erythema, friability | Aphthous ulcers, cobblestoning |
| Serology | pANCA positive | ASCA positive |
The diagnostic process for ulcerative colitis requires integration of clinical, laboratory, endoscopic, and histological findings, with particular attention to excluding infectious etiologies before initiating immunosuppressive therapy.
8. Treatment Options
Treatment principles and goals
The management of ulcerative colitis follows several key principles:
Treatment goals:
- Symptom control: Resolution of diarrhea, bleeding, urgency, and pain
- Mucosal healing: Endoscopic resolution of inflammation
- Quality of life improvement: Return to normal activities
- Nutritional restoration: Weight gain, correction of deficiencies
- Prevention of complications: Reducing hospitalizations, surgery, cancer risk
- Steroid-free remission: Minimizing corticosteroid exposure
- Maintenance of remission: Preventing disease flares
Treat-to-target approach:
- Specific, measurable treatment targets
- Regular assessment of disease activity
- Treatment escalation if targets not met
- Commonly used targets:
- Clinical remission: Normal bowel habits, no blood
- Biochemical remission: Normalized CRP, fecal calprotectin
- Endoscopic remission: Healing of mucosa
- Histologic remission: Resolution of microscopic inflammation
Treatment selection factors:
- Disease severity (mild, moderate, severe)
- Disease extent (proctitis, left-sided, extensive)
- Previous treatment response
- Comorbidities
- Patient preferences and concerns
- Pregnancy considerations
- Cost and access issues
Treatment phases:
- Induction: Achieving remission during active disease
- Maintenance: Sustaining remission once achieved
- Rescue: Managing severe or refractory disease
Pharmacological treatments
5-Aminosalicylates (5-ASA):
- Mechanism: Anti-inflammatory, antioxidant, PPAR-γ activation
- Formulations:
- Oral: pH-dependent release, time-dependent release, MMX technology
- Topical: Suppositories, enemas, foams
- Indications:
- First-line for mild-moderate UC
- Most effective for distal and left-sided disease
- Maintenance therapy
- Efficacy:
- Induction of remission: 40-60%
- Maintenance of remission: 60-75%
- Examples: Mesalamine, sulfasalazine, balsalazide, olsalazine
- Side effects: Generally well-tolerated; headache, nausea, rarely nephrotoxicity
Corticosteroids:
- Mechanism: Broad anti-inflammatory effects
- Formulations:
- Systemic: Prednisone, prednisolone, methylprednisolone
- Topical: Hydrocortisone enemas, foams
- Second-generation: Budesonide MMX
- Indications:
- Moderate-severe flares
- Not for maintenance therapy
- Efficacy:
- Induction of remission: 60-80%
- High relapse rate after discontinuation
- Side effects: Weight gain, mood disturbances, hyperglycemia, osteoporosis, adrenal suppression
Immunomodulators:
- Thiopurines (azathioprine, 6-mercaptopurine):
- Mechanism: Inhibit purine synthesis
- Indications: Steroid-dependent disease, maintenance
- Efficacy: 60-70% for maintenance
- Onset: 2-3 months
- Side effects: Myelosuppression, hepatotoxicity, pancreatitis, infection risk
- Calcineurin inhibitors (cyclosporine, tacrolimus):
- Mechanism: Inhibit T-cell activation
- Indications: Severe, steroid-refractory UC
- Efficacy: 60-85% short-term response in severe UC
- Onset: Rapid (within days)
- Side effects: Nephrotoxicity, hypertension, neurotoxicity, infection risk
- Methotrexate:
- Limited evidence in UC compared to Crohn’s disease
- Occasionally used in patients intolerant to thiopurines
Biologic therapies:
- Anti-TNF agents:
- Mechanism: Neutralize tumor necrosis factor-α
- Examples: Infliximab, adalimumab, golimumab
- Indications: Moderate-severe UC
- Efficacy: Induction remission 30-40%, maintenance 40-60%
- Side effects: Injection/infusion reactions, infection risk, rare demyelination
- Anti-integrin therapy:
- Mechanism: Block gut-specific lymphocyte trafficking
- Example: Vedolizumab
- Indications: Moderate-severe UC
- Efficacy: Similar to anti-TNF with better safety profile
- Side effects: Generally well-tolerated, rare PML risk
- Anti-IL-12/23 therapy:
- Mechanism: Block interleukin-12 and interleukin-23
- Example: Ustekinumab
- Indications: Moderate-severe UC
- Efficacy: Comparable to other biologics
- Side effects: Generally well-tolerated, infection risk
- Anti-IL-23 specific therapy:
- Mechanism: Selectively blocks IL-23
- Examples: Risankizumab, mirikizumab, guselkumab
- Status: Recently approved or in late-stage trials
- Promising efficacy with favorable safety profile
Small molecule inhibitors:
- JAK inhibitors:
- Mechanism: Block Janus kinase signaling pathway
- Examples: Tofacitinib, upadacitinib
- Indications: Moderate-severe UC
- Efficacy: Comparable to biologics
- Advantages: Oral administration, rapid onset
- Side effects: Infection risk, thromboembolic events, lipid elevations
- S1P receptor modulators:
- Mechanism: Prevent lymphocyte egress from lymph nodes
- Example: Ozanimod
- Recently approved for moderate-severe UC
- Side effects: Bradycardia, AV block, liver enzyme elevations
Other medications:
- Antibiotics: Limited role, used for complications
- Probiotics: VSL#3 has evidence for pouchitis
- Fecal microbiota transplantation: Emerging data, not standard care
- Antidiarrheals: Used cautiously in stable disease
- Pain management: Non-NSAID approaches
Surgical interventions
Indications for surgery:
- Emergency indications:
- Massive hemorrhage
- Perforation
- Toxic megacolon unresponsive to medical therapy
- Fulminant colitis with deterioration
- Elective indications:
- Medically refractory disease
- Intolerable medication side effects
- Dysplasia or colorectal cancer
- Growth retardation in children
- Quality of life considerations
Surgical options:
- Total proctocolectomy with end ileostomy:
- Complete removal of colon and rectum
- Permanent ileostomy
- Lowest complication rate
- Often used in emergency settings or older patients
- Total proctocolectomy with ileal pouch-anal anastomosis (IPAA):
- Standard elective procedure
- Creation of internal pouch from terminal ileum
- Preserves transanal defecation
- Usually performed in 2-3 stages
- Complication rate 30-50%
- Total colectomy with ileorectal anastomosis:
- Rarely performed in UC
- Preserves rectum
- Risk of ongoing proctitis or cancer in retained rectum
- Subtotal colectomy with temporary ileostomy:
- Bridge procedure in acute severe colitis
- Allows patient stabilization and nutrition optimization
- Definitive surgery performed later
Surgical outcomes:
- IPAA functional outcomes:
- Stool frequency: 4-8 bowel movements per day
- Nocturnal incontinence: 5-10%
- Sexual dysfunction: 3-17%
- Fertility reduction in females (though laparoscopic approach reduces this)
- IPAA complications:
- Pouchitis: 20-50% lifetime risk
- Small bowel obstruction: 13-25%
- Anastomotic stricture: 8-14%
- Pouch failure: 5-10% at 10 years
- Quality of life:
- 90-95% patient satisfaction
- Significant improvement in quality of life
- Most return to full employment
- Long-term outcomes:
- Cuff inflammation: 10-20%
- Pouch dysplasia: Rare but possible
- Most maintain satisfactory function long-term
Minimally invasive approaches:
- Laparoscopic surgery:
- Reduced adhesions
- Faster recovery
- Better cosmetic results
- Preserved fertility in women
- Robotic surgery:
- Improved visualization
- Enhanced precision
- Outcomes similar to laparoscopic
- Single-incision laparoscopic surgery (SILS):
- Further improved cosmesis
- Comparable outcomes to traditional laparoscopy
Diet, nutrition, and lifestyle approaches
Dietary interventions:
- No universal diet for UC, but individualized approaches:
- Low FODMAP diet: May help with IBS-like symptoms
- Specific Carbohydrate Diet (SCD): Limited evidence, some patient-reported benefit
- Mediterranean diet: Anti-inflammatory properties
- Exclusion diets: Based on individual intolerances
- Low-fiber during flares: Reduces mechanical irritation
- High-fiber in remission: May support beneficial microbiota
Nutritional support:
- Nutritional assessment: Regular screening for deficiencies
- Specific deficiencies to address:
- Iron: IV iron often better tolerated than oral
- Vitamin D: Supplementation for bone health
- Calcium: Particularly with steroid use
- Zinc, magnesium, selenium: As needed
- Vitamin B12, folate: Particularly with extensive disease
- Enteral nutrition: For malnutrition, rarely primary therapy
- Parenteral nutrition: For severe disease with intolerance to enteral feeding
Complementary and alternative approaches:
- Probiotics: VSL#3/Visbiome shows benefit in pouchitis and mild UC
- Prebiotics: Potential microbiome benefits
- Curcumin: Anti-inflammatory properties, some evidence as adjunctive therapy
- Omega-3 fatty acids: Mixed evidence
- Acupuncture: Limited evidence
- Mind-body interventions:
- Stress reduction techniques
- Cognitive behavioral therapy
- Mindfulness-based stress reduction
- Hypnotherapy: Some positive studies
Lifestyle modifications:
- Exercise:
- Regular moderate exercise beneficial
- May reduce inflammation and improve well-being
- Adaptation during flares
- Smoking cessation:
- Despite protective effect, cessation recommended
- Managed carefully with monitoring for disease worsening
- Stress management:
- Stress reduction techniques
- Adequate sleep
- Work-life balance
- Psychological support:
- Support groups
- Patient advocacy organizations
- Mental health services when needed
Emerging treatments and clinical trials
The therapeutic landscape for ulcerative colitis continues to evolve rapidly:
Novel biologics in development:
- Anti-IL-23 agents:
- Mirikizumab (Phase 3)
- Risankizumab (Phase 3)
- Guselkumab (Phase 2/3)
- Potentially better safety profile than broader spectrum agents
- TL1A inhibitors:
- PF-06480605 (Phase 2)
- Target a key inflammatory pathway
- Anti-integrin therapies:
- Etrolizumab (β7 integrin inhibitor)
- AJM300 (oral α4 integrin inhibitor)
- Anti-MAdCAM-1 antibodies:
- Ontamalimab: Blocks gut-specific homing
Small molecules in pipeline:
- Selective JAK inhibitors:
- Filgotinib (JAK1 selective)
- TD-1473 (gut-selective JAK inhibitor)
- Izencitinib (gut-restricted pan-JAK inhibitor)
- S1P receptor modulators:
- Etrasimod (Phase 3)
- Selective S1P1 modulation
- PDE4 inhibitors:
- Apremilast (Phase 2)
- Oral anti-inflammatory
- DHODH inhibitors:
- Vidofludimus calcium (Phase 3)
- Novel mechanism targeting lymphocyte proliferation
Cell-based therapies:
- Stem cell therapy:
- Mesenchymal stem cells
- Alofisel (darvadstrocel): Approved for Crohn’s perianal fistulas
- Regulatory T-cell therapies:
- Ex vivo expanded Tregs
- Enhance immune regulation
- Fecal microbiota transplantation:
- Multiple ongoing trials
- Mixed results to date
- Refinement of donor selection and processing
Novel delivery technologies:
Microbiota-triggered drug release systems
Engineered bacteria:
- Modified to produce anti-inflammatory mediators
- SYNB1020, ActoBio therapeutics platforms
Nanoparticle drug delivery:
- Enhanced colonic targeting
- Reduced systemic exposure
Precision medicine approaches:
- Biomarker-driven therapy selection:
- Genetic markers
- Microbial signatures
- Immune cell phenotyping
- Transcriptomic profiles
- Combination therapy optimization:
- Identifying synergistic combinations
- Sequential therapy approaches
- Prediction models:
- Artificial intelligence for treatment response
- Risk stratification algorithms
The treatment of ulcerative colitis has transformed from limited options to a rich array of targeted therapies, with many more in development. This expansion offers hope for more personalized and effective management, potentially changing the natural history of this challenging disease.
9. Prevention & Precautionary Measures
Primary prevention
While ulcerative colitis cannot be completely prevented due to its complex pathogenesis involving genetic susceptibility, several strategies may reduce risk or delay onset:
Modifiable risk factor management:
- Smoking considerations:
- Despite protective effect, smoking initiation not recommended
- For high-risk individuals who already smoke, abrupt cessation may trigger disease
- Gradual cessation with monitoring might be considered
- Appendectomy:
- Early appendectomy for appendicitis is associated with lower UC risk
- Prophylactic appendectomy not recommended
- Diet and nutrition:
- Mediterranean diet pattern associated with reduced risk
- Adequate vitamin D levels may be protective
- Balanced omega-3/omega-6 fatty acid intake
- Limiting processed foods and additives
- Moderate alcohol consumption
- Breastfeeding:
- Both receiving as an infant and providing as a mother appears protective
- Promotes healthy microbiome development
- May program appropriate immune responses
Environmental modifications:
- Antibiotic stewardship:
- Judicious use, especially in childhood
- Particularly first year of life
- Pollution exposure:
- Reducing exposure to air pollutants where possible
- Consideration of air quality in living location
- Stress management:
- Stress reduction techniques
- Adequate sleep
- Work-life balance
- Physical activity:
- Regular moderate exercise
- Associated with reduced inflammation
Microbiome considerations:
- Probiotics:
- Role in primary prevention unclear
- May have role in high-risk individuals
- Prebiotic foods:
- Support beneficial microbiome
- Fermented foods, high-fiber diet
- Avoiding unnecessary microbial disruption:
- Limiting unnecessary antibiotics
- Avoidance of harsh antimicrobial cleaning products
Disease management and complication prevention
For individuals with established ulcerative colitis, preventing flares and complications is essential:
Maintenance of remission:
- Medication adherence:
- Critical for sustained remission
- Addressing barriers to adherence
- Regular monitoring
- Patient education on importance
- Regular monitoring:
- Clinical assessment
- Biomarkers (calprotectin, CRP)
- Endoscopic evaluation when indicated
- Trigger avoidance:
- Individual dietary triggers
- NSAIDs
- Stress management
- Infection prevention
Specific complication prevention:
- Colorectal cancer surveillance:
- Start 8 years after diagnosis
- Every 1-3 years based on risk factors
- Chromoendoscopy preferred
- Consideration of chemoprevention (5-ASA, possibly statins)
- Nutritional monitoring:
- Regular assessment of nutritional status
- Iron studies
- Vitamin D levels
- Bone density screening
- Venous thromboembolism prevention:
- Thromboprophylaxis during hospitalization
- Maintaining hydration
- Early mobilization after surgery
- Consideration of prophylaxis during severe flares
Strategies during disease flares:
- Early intervention:
- Prompt treatment at first signs of flare
- Patient education on early symptoms
- Self-management plans
- Access to healthcare team
- Nutritional support during flares:
- Lower fiber intake temporarily
- Adequate protein intake
- Fluid and electrolyte maintenance
- Nutritional supplements if needed
- Psychological support:
- Managing disease-related anxiety
- Access to mental health services
- Support groups
Extraintestinal manifestation prevention:
- Joint complications:
- Physical therapy
- Maintenance of muscular strength
- Proper body mechanics
- Bone health:
- Vitamin D and calcium supplementation
- Weight-bearing exercise
- Minimizing steroid exposure
- Regular bone density monitoring
- Ocular complications:
- Regular eye examinations
- Prompt evaluation of eye symptoms
Lifestyle and environmental precautions
Dietary considerations:
- Individualized approach:
- Food diary to identify triggers
- Structured elimination and reintroduction
- Working with dietitian specializing in IBD
- General recommendations:
- Well-balanced, anti-inflammatory diet
- Adequate protein intake
- Limited processed foods
- Appropriate fiber based on disease state
- Small, frequent meals during active disease
- Hydration:
- Maintaining adequate fluid intake
- Electrolyte replacement when indicated
- Limiting caffeine and alcohol
Physical activity guidelines:
- Regular exercise:
- Moderate intensity
- 30 minutes most days
- Low-impact activities during flares
- Gradual return after surgery
- Adaptations during flares:
- Reduced intensity
- Shorter duration
- Focus on gentle movement
- Swimming and aquatic exercise well-tolerated
Stress management:
- Mind-body techniques:
- Mindfulness meditation
- Progressive muscle relaxation
- Guided imagery
- Yoga and tai chi
- Psychological approaches:
- Cognitive behavioral therapy
- Acceptance and commitment therapy
- Stress management training
- Sleep hygiene:
- Regular sleep schedule
- Sleep environment optimization
- Management of nocturnal symptoms
Travel and everyday precautions:
- Travel planning:
- Medication supply and storage
- Healthcare access at destination
- Travel insurance
- Restroom mapping
- Food and water safety
- Workplace accommodations:
- Restroom access
- Flexible scheduling
- Remote work options when needed
- FMLA and disability awareness
- Vaccination guidelines:
- Annual influenza vaccination
- Pneumococcal vaccination
- Hepatitis A and B
- Special considerations on immunosuppressive therapy
- COVID-19 vaccination
- Avoiding live vaccines on certain medications
Social support systems:
- Patient organizations:
- Crohn’s and Colitis Foundation
- European Federation of Crohn’s & Ulcerative Colitis Associations
- National and regional support groups
- Family education:
- Involving family in management
- Education about disease nature
- Communication strategies
- Peer support:
- Buddy systems
- Online communities
- In-person support groups
Reproductive planning:
- Fertility considerations:
- Disease control before conception
- Medication review for pregnancy compatibility
- Surgical considerations (particularly IPAA in women)
- Pregnancy management:
- Maintaining remission during pregnancy
- Multidisciplinary care
- Medication adjustments
- Delivery planning
- Genetic counseling:
- Risk discussion for offspring
- Family planning
While ulcerative colitis cannot be prevented entirely, these strategies may reduce risk, minimize complications, and optimize quality of life for those affected. Individualized approaches tailored to each person’s specific disease characteristics, risk factors, and life circumstances are essential for effective prevention and management.
10. Global & Regional Statistics
Global prevalence and incidence
Overall global burden:
- Worldwide prevalence: Estimated 5.8 million people with ulcerative colitis
- Global incidence range: 1.2-20.3 per 100,000 person-years
- Global prevalence range: 7.6-245 per 100,000 population
- Time trends: Increasing incidence in newly industrialized countries
- Economic impact: Estimated $7.5-10 billion in direct costs annually worldwide
Geographic variations in prevalence:
- Highest: Northern Europe and North America (10-20 per 100,000 person-years)
- Intermediate: Southern Europe, Australia, South America (5-10 per 100,000 person-years)
- Lowest historically: Asia, Africa (1-5 per 100,000 person-years), though rapidly increasing
Epidemiological transition:
- Historical pattern: Higher in developed, Western nations
- Current trend: Rising rapidly in newly industrialized countries
- Stabilizing: Plateauing incidence in long-industrialized regions
- Global convergence: Narrowing of differences between regions
Key epidemiological observations:
- North-South gradient: Higher rates in northern latitudes in both hemispheres
- Urban-rural differences: Higher prevalence in urban areas
- Western lifestylization effect: Increases with adoption of Western lifestyle
- Migration effect: Migrants adopt risk of host country within 1-2 generations
Regional epidemiology
North America:
- United States:
- Prevalence: 200-240 per 100,000 (approximately 800,000 patients)
- Incidence: 10-12 per 100,000 person-years
- Higher rates in northern states
- Racial variations: Historically higher in Caucasians, increasing in other groups
- Annual cost: $8,000-15,000 per patient
- Canada:
- Prevalence: 180-225 per 100,000
- Incidence: 10-15 per 100,000 person-years
- Among highest rates globally
- Provincial variations: Higher in Alberta, Manitoba
Europe:
- Northern Europe:
- Prevalence: 160-300 per 100,000
- Incidence: 10-15 per 100,000 person-years
- Highest rates in Scandinavia, particularly Denmark and Iceland
- Western Europe:
- Prevalence: 150-230 per 100,000
- Incidence: 8-11 per 100,000 person-years
- Well-established registries providing reliable data
- Southern Europe:
- Prevalence: 80-150 per 100,000
- Incidence: 5-8 per 100,000 person-years
- Eastern Europe:
- Prevalence: 50-150 per 100,000
- Incidence: 4-6 per 100,000 person-years
- Rapidly increasing
Asia:
- East Asia:
- Japan:
- Prevalence: 30-100 per 100,000
- Incidence: 1.5-5 per 100,000 person-years
- Dramatic increase since 1960s
- South Korea:
- Prevalence: 30-75 per 100,000
- Incidence: 3-5 per 100,000 person-years
- Nearly 3-fold increase in last decade
- China:
- Prevalence: 10-40 per 100,000
- Incidence: 1-3 per 100,000 person-years
- Urban areas much higher than rural
- Rapid increase with industrialization
- Japan:
- South Asia:
- India:
- Prevalence: 7-20 per 100,000
- Incidence: 1-2 per 100,000 person-years
- Higher in northern and western regions
- Rising significantly in urban centers
- India:
Middle East:
- Prevalence: 20-80 per 100,000
- Incidence: 2-5 per 100,000 person-years
- Israel: Higher rates, similar to European patterns
- Saudi Arabia, Turkey: Intermediate rates
- Regional challenge: Limited epidemiological studies
Africa:
- North Africa:
- Prevalence: 10-40 per 100,000
- Better documented than sub-Saharan regions
- Sub-Saharan Africa:
- Prevalence: 3-15 per 100,000 (limited data)
- Likely underestimated due to diagnostic limitations
- Urban centers showing increasing rates
- South Africa:
- Higher rates in Caucasian population
- Increasing in urban Black African populations
Australia and New Zealand:
- Prevalence: 140-200 per 100,000
- Incidence: 7-10 per 100,000 person-years
- Population variations: Higher in European-descended populations
- Geographic pattern: Southern regions higher than northern (reverse of Northern Hemisphere)
Latin America:
- Prevalence: 20-80 per 100,000
- Incidence: 2-4 per 100,000 person-years
- Country variations:
- Brazil and Argentina: Higher rates
- Central American countries: Lower rates
- Limited epidemiological studies: Likely underestimation
Time trends and projections
Historical trends:
- 1940s-1960s: Initial recognition of increasing cases in Western world
- 1960s-1980s: Steady increase in Europe and North America
- 1980s-2000s: Stabilization in highly industrialized countries
- 1990s-present: Dramatic increases in newly industrialized Asian countries
- 2000s-present: Beginning of increases in Africa and less developed regions
Current trends (2010s-2020s):
- Western regions: Stable or slightly increasing incidence
- Asian regions: Rapidly increasing (10-15% annually in some areas)
- Pediatric UC: Increasing faster than adult-onset
- Elderly-onset UC: Increasing due to aging populations
- Extended family effect: Increasing in immigrant families over generations
Future projections:
- Global burden: Expected to affect 8-10 million people by 2030
- Fastest growth regions: Asia, Middle East, Latin America
- Developed regions: Expected stable rates with aging affected population
- Economic impact: Projected to increase by 30-40% by 2030
- Healthcare system challenges:
- Increasing need for specialized IBD care in developing regions
- Access to biologics and advanced therapies
- Colorectal cancer surveillance programs
Factors affecting future trends:
- Economic development: Continued industrialization driving increases
- Environmental changes: Air pollution, dietary shifts
- Diagnostic access: Improved healthcare access revealing true prevalence
- Treatment advances: May alter natural history and complication rates
- Preventive strategies: Emerging microbiome interventions
Mortality and quality of life statistics
Mortality:
- Overall mortality: Slight increase compared to general population (SMR 1.1-1.3)
- Cause-specific mortality:
- Colorectal cancer (SMR 1.5-2.0)
- Surgical complications
- Venous thromboembolism
- Infections on immunosuppressive therapy
- Age-specific mortality:
- Higher relative mortality in younger patients
- Nearly normal in elderly patients
- Time trends:
- Declining mortality over past decades
- Earlier diagnosis and improved treatments contributing
Health-related quality of life:
- During remission: Comparable to general population
- During flares: Significantly reduced (30-50% reduction)
- Overall impact:
- Sleep disturbance: 70-80% during flares
- Fatigue: 60-80% even in remission
- Sexual dysfunction: 45-60%
- Anxiety/depression: 20-30%
- Work productivity:
- Absenteeism: 3-6 times higher than general population
- Presenteeism: 15-20% reduced productivity while at work
- Work disability: 10-25% at 10 years from diagnosis
- Educational impact:
- Missed school days: 3-5 times general population
- Educational attainment: Minimally affected with proper support
Healthcare utilization:
- Hospitalization rates:
- Annual risk: 20-25% in active disease
- Declining trend with newer therapies
- Surgery rates:
- Colectomy at 10 years: 10-15%
- Lifetime colectomy risk: 20-30%
- Declining trend over recent decades
- Emergency department utilization:
- 30-40% annual use during active disease
- Often for pain, bleeding, or dehydration
The global epidemiology of ulcerative colitis reflects complex interactions between genetic susceptibility and environmental factors associated with industrialization and Western lifestyle. The disease burden is shifting, with rapid increases in newly industrialized nations causing significant healthcare challenges in regions that may have limited resources for managing this complex, chronic condition.
11. Recent Research & Future Prospects
Latest research advances
Disease mechanisms:
- Microbiome insights:
- Reduced microbial diversity precedes flares
- Specific bacterial signatures associated with treatment response
- Functional metabolite changes more consistent than taxonomic changes
- Microbial transplant shows variable efficacy, suggesting importance of specific donor signatures
- Epithelial barrier function:
- New understanding of tight junction regulation
- Barrier-healing compounds under development
- Role of mucus layer defects as primary rather than secondary phenomenon
- Claudin-directed therapeutics in development
- Immune pathways:
- Specific IL-23-responsive pathogenic T cell populations identified
- Novel immune regulatory mechanisms in the intestinal mucosa
- Trained immunity and epigenetic effects in innate immune cells
- Identification of tissue-resident immune cells maintaining inflammation
- Molecular classification:
- Transcriptomic signatures defining patient subgroups
- Predictive biomarkers of therapeutic response
- Epigenetic modifications in UC pathogenesis
- Integration of multi-omics data (genome, transcriptome, proteome, metabolome)
Clinical advancements:
- Mucosal healing as therapeutic target:
- Superior long-term outcomes with complete healing
- Development of standardized endoscopic scoring systems
- Non-invasive biomarkers correlating with mucosal status
- Histologic healing emerging as deeper goal beyond endoscopic healing
- Therapeutic drug monitoring:
- Optimization of biologic therapy through drug levels
- Proactive versus reactive monitoring
- Development of point-of-care assays
- Algorithms incorporating antidrug antibodies
- Precision medicine approaches:
- Biomarker-guided therapy selection
- Genetic predictors of drug response and toxicity
- Machine learning models integrating clinical and molecular data
- Patient stratification based on disease behavior
Technological innovations:
- Advanced endoscopic techniques:
- Confocal laser endomicroscopy for real-time histology
- Artificial intelligence for polyp detection and characterization
- Enhanced imaging techniques (NBI, i-scan, chromoendoscopy)
- Motorized spiral enteroscopy for complete small bowel assessment
- Digital health solutions:
- Remote monitoring platforms
- Predictive algorithms for flare detection
- Patient-reported outcome electronic systems
- Teleconsultation models
- Novel diagnostic tools:
- Capsule endoscopy for panenteric assessment
- Ultrasensitive inflammatory biomarkers
- Noninvasive intestinal permeability tests
- Bowel ultrasound for monitoring
Ongoing research and clinical trials
Novel therapeutic targets:
- Epithelial barrier enhancement:
- Peroxisome proliferator-activated receptor-γ (PPAR-γ) agonists
- Rho kinase inhibitors
- Intestinal alkaline phosphatase
- E-cadherin stabilizers
- Microbiome modulation:
- Defined microbial consortia
- Designer probiotics producing anti-inflammatory molecules
- Phage therapy targeting pathobionts
- Microbial metabolite supplementation
- Mucosal healing accelerators:
- Growth factors (GLP-2 analogues)
- Mesenchymal stem cell therapies
- Interleukin-22 based approaches
- Specialized pro-resolving mediators
- Novel anti-inflammatory pathways:
- NLRP3 inflammasome inhibitors
- Targeted phosphodiesterase inhibitors
- Sphingosine-1-phosphate lyase inhibitors
- Selective A3 adenosine receptor agonists
Emerging treatment strategies:
- Combination therapy approaches:
- Combination biologics with complementary mechanisms
- Small molecule and biologic combinations
- Sequential therapy protocols
- Top-down versus step-up comparisons
- Treatment de-escalation:
- Predictors of successful withdrawal
- Sequential versus complete withdrawal
- Drug-level guided de-escalation
- Maintenance of remission with minimal therapy
- Advanced delivery technologies:
- Colon-specific delivery systems
- Nanoparticle drug carriers
- Hydrogel-based release systems
- Oral biologic delivery technologies
- Regenerative medicine:
- Intestinal organoids for personalized drug testing
- Bioengineered intestinal tissue
- Ex vivo expanded regulatory T cells
- Genetically modified cell therapies
Major ongoing clinical trials:
- Novel biologics:
- Mirikizumab (IL-23p19 inhibitor) Phase 3
- Etrolizumab (anti-β7 integrin) Phase 3
- Spesolimab (IL-36 receptor antagonist) Phase 2
- Brazikumab (IL-23 inhibitor) Phase 2/3
- Small molecules:
- Etrasimod (S1P receptor modulator) Phase 3
- Izencitinib (gut-selective JAK inhibitor) Phase 2/3
- Filgotinib (selective JAK1 inhibitor) Phase 3
- Vidofludimus calcium (DHODH inhibitor) Phase 3
- Microbiome-directed therapies:
- FIN-524 (defined microbial consortium) Phase 1
- SER-287 (microbiome therapeutic) Phase 2
- Multiple fecal microbiota transplantation trials
- Bacteriophage preparations targeting adherent-invasive E. coli
- Novel therapeutic strategies:
- QBECO SSI (innate immune modulator) Phase 2
- ABX464 (miRNA modulator) Phase 2b
- Obefazimod (miR-124 upregulator) Phase 2b/3
- GS-5745 (MMP9 inhibitor) Phase 2/3
Future directions and paradigm shifts
Preventive strategies:
- Early intervention in high-risk individuals:
- Genetically susceptible family members
- Pre-clinical biomarker-positive individuals
- Post-infectious high-risk patients
- Microbiome-based prevention:
- Targeted probiotics for at-risk individuals
- Dietary interventions shaping microbiome
- Next-generation prebiotics
- Prevention of dysbiosis after antibiotic exposure
- Environmental modification:
- Air pollution mitigation strategies
- Food additive and emulsifier regulation
- Early-life exposures optimization
- Stress reduction programs
Cure-directed research:
- Immunological reset:
- Induction of immune tolerance
- Regulatory T-cell expansion therapies
- Autologous hematopoietic stem cell transplantation
- Targeted depletion of pathogenic memory cells
- Genetic approaches:
- Gene editing of disease-associated variants
- RNA-based therapies targeting disease pathways
- Epigenetic modification therapies
- MicroRNA-targeted approaches
- Radical microbiome intervention:
- Designer microbial communities
- Engineered bacteriophage therapies
- Genetic modification of resident microbiota
- Comprehensive depletion and repopulation
Paradigm shifts in management:
- Disease interception:
- Identifying and treating pre-clinical disease
- Biomarker-defined high-risk states
- Preventive rather than reactive approach
- Comprehensive disease control:
- Beyond symptom control to deep remission
- Histologic and molecular remission as goals
- Prevention of long-term complications
- Restoration of normal quality of life
- Personalized medicine implementation:
- Molecular profiling guiding therapy
- Risk stratification for treatment intensity
- Pharmacogenomic-guided drug selection
- Integration of multi-omics data in clinical decisions
- Digital transformation of care:
- Continuous remote monitoring
- Predictive analytics for disease course
- Virtual specialized care delivery
- Patient-driven disease management
The future of ulcerative colitis research and treatment is rapidly evolving toward more personalized, precise, and potentially curative approaches. The integration of advanced molecular techniques, microbiome science, immunology, and digital health technologies promises to transform management from the current symptom-control paradigm to one focused on disease modification, prevention, and potentially cure in the coming decades.
12. Interesting Facts & Lesser-Known Insights
Historical perspectives
Notable historical figures with ulcerative colitis:
- John F. Kennedy: Struggled with UC throughout his presidency, was on corticosteroids
- Dwight D. Eisenhower: Developed UC during his presidency
- Shinzo Abe: Former Japanese Prime Minister resigned due to UC flare
- Sir Steve Redgrave: Five-time Olympic gold medalist, competed while managing UC
- Anastacia: Singer diagnosed at age 13, advocated for awareness
- Theo Walcott: Professional footballer who has spoken about managing UC as an athlete
- Ken Baumann: Actor and author who has written about his experience with UC
Historical treatments:
- Mercury compounds: Used in the early 1900s
- Arsenic preparations: Applied before the antibiotic era
- Charcoal filters: External filtration of blood to remove “toxins”
- Tobacco enemas: Used historically, ironically foreshadowing the protective effect of smoking
- Diathermy: Application of electrical current to inflamed areas
- Worm therapy: Helminth treatment explored in the early 2000s
- Exclusive meat diets: Advocated in the 1920s-1930s
Evolution of surgical approaches:
- Three-stage procedure was standard in the 1950s-1970s
- The J-pouch was developed in the late 1970s
- Initial pouches were S-shaped, later K, W, and finally J configuration
- First laparoscopic colectomy for UC performed in 1992
- Early mortality from surgery was 30-40% in the 1930s, now <1%
Milestone discoveries:
- 1909: First detailed description by Sir Arthur Hurst
- 1935: First use of sulfasalazine by Nanna Svartz
- 1955: First controlled trial of corticosteroids by Truelove and Witts
- 1974: Discovery of the association between smoking cessation and UC
- 1982: First description of pouchitis after IPAA
- 1998: First use of infliximab for UC
- 2006: First genome-wide association study in UC
Unusual facts and phenomena
Unique aspects of ulcerative colitis:
- The smoking paradox: One of few diseases where smoking is protective
- Appendectomy protection: Appendix removal before age 20 reduces risk by ~70%
- Gradient-based distribution: Always begins in rectum and extends proximally
- Northern gradient: More common in northern latitudes in both hemispheres
- Urban predominance: Higher prevalence in urban vs. rural areas worldwide
- Post-infectious onset: 10-15% of cases follow documented gastroenteritis
- Sleep effect: Relapse risk increased 2-fold with poor sleep quality
Biological curiosities:
- Microbial composition: The colonic mucosa normally contains 10^14 bacteria
- Colonocyte metabolism: 70% of energy comes from bacterial fermentation products
- Mucus layer thickness: Normally 800μm, reduced to <150μm in active UC
- Sulfation deficiency: UC patients show reduced ability to detoxify sulfur compounds
- Cellular turnover: Colon epithelium renews completely every 5-7 days
- Colon capacities: Can absorb up to 4-5 liters of water daily
- Biological clock: Colonic function regulated by circadian rhythms
Unique clinical phenomena:
- Backwash ileitis: Inflammation extending into terminal ileum in pancolitis
- Cecal patch: Isolated cecal inflammation in left-sided colitis
- Reverse gradient colitis: Rare proximal-to-distal gradient of inflammation
- Post-infectious dominant pattern: Higher risk of colectomy in those with infectious onset
- Fulminant first presentation: 5-10% present with severe disease as first manifestation
- Refractory proctitis syndrome: Isolated proctitis more difficult to treat than extensive disease
- Rectal sparing with treatment: Can mimic Crohn’s disease after topical therapy
Myths vs. facts
Myth: Ulcerative colitis is caused by psychological stress. Fact: While stress can trigger flares, UC is an immune-mediated condition with genetic and environmental factors.
Myth: Diet alone causes ulcerative colitis. Fact: No single diet causes UC, though dietary factors may influence risk and symptoms.
Myth: Ulcerative colitis is contagious. Fact: UC is not infectious or contagious; it cannot be transmitted from person to person.
Myth: Ulcerative colitis and Crohn’s disease are the same condition. Fact: They are distinct conditions with different patterns, locations, complications, and treatment responses.
Myth: Ulcerative colitis only affects the intestines. Fact: UC can cause extraintestinal manifestations affecting joints, skin, eyes, and liver.
Myth: Ulcerative colitis requires a permanent ostomy bag. Fact: Most patients never need surgery, and when surgery is required, ileal pouch-anal anastomosis allows stool to pass through the anus without a permanent bag.
Myth: Patients with ulcerative colitis cannot live normal lives. Fact: With proper treatment, most patients achieve remission and maintain normal activities.
Myth: Pregnancy is dangerous for women with ulcerative colitis. Fact: With disease under control, pregnancy outcomes are generally good.
Myth: Children with ulcerative colitis can’t grow normally. Fact: With proper treatment and nutrition, most achieve normal growth.
Myth: Ulcerative colitis inevitably leads to colorectal cancer. Fact: While risk is increased, regular surveillance and anti-inflammatory therapy reduces this risk significantly.
Impact on specific populations
Children and adolescents:
- Educational impact: Average 20-25 missed school days annually during active disease
- Growth effects: 15-40% experience growth delays without proper treatment
- Social development: Challenges with body image and peer relationships
- Transition challenges: Critical period moving from pediatric to adult care
- Career planning: Often influences educational and vocational choices
- Treatment differences: More aggressive approach often needed
- Family dynamics: Significant impact on parents and siblings
Elderly patients:
- Presentation differences: Often less typical, with constipation sometimes predominating
- Diagnosis challenges: Often delayed due to consideration of other causes
- Comorbidity interactions: Management complicated by other medical conditions
- Medication considerations: Altered pharmacokinetics and higher risk of side effects
- Higher hospitalization rates: More frequent admissions
- Lower surgery rates: More conservative approach to colectomy
- Cognitive impact: Higher risk of delirium during flares
Athletes and physically active individuals:
- Performance considerations: Potential for dehydration and electrolyte disturbances
- Special nutritional needs: Higher caloric requirements to support training
- Competition strategies: Managing bathroom access, nutrition, and medication timing
- Disclosure challenges: Decisions about informing coaches and teammates
- Beneficial aspects: Regular exercise associated with reduced inflammation
- Professional sports examples: Several Olympic and professional athletes compete successfully
- Sport-specific considerations: Water sports and running particularly challenging
Pregnant women:
- Fertility impacts: Generally normal when in remission
- Disease activity patterns: 1/3 improve, 1/3 worsen, 1/3 remain stable
- Medication adjustments: Most IBD medications considered low risk
- Flare management: More challenging during pregnancy
- Delivery considerations: Most can have vaginal delivery
- Breastfeeding compatibility: Most medications compatible with breastfeeding
- Postpartum flare risk: Increased in first 3-6 months after delivery
Occupational considerations:
- High-stress professions: Additional challenges in managing stress triggers
- Bathroom access occupations: Transportation, teaching, field work particularly challenging
- Military service: Often requires waivers, limitations on deployment
- Healthcare workers: Rotating shifts and long procedures problematic
- Workplace accommodations: Legal protections under disability legislation
- Disclosure decisions: Complex considerations regarding telling employers
- Career impact: 25-35% report significant career limitations due to UC
These interesting perspectives and lesser-known aspects of ulcerative colitis illustrate the condition’s complexity and far-reaching impacts beyond the basic medical understanding. They highlight the importance of a holistic, individualized approach to patient care that considers the many facets of this challenging chronic disease.

