⚠️ Disclaimer: The information provided in this article is for educational purposes only and does not constitute medical advice. RevisionTown does not provide diagnosis, treatment, or medical recommendations. Always consult a qualified healthcare professional regarding any medical condition, symptoms, or concerns.
Read More – 🏥 Medical Disclaimer
Comprehensive Report on Congestive Heart Failure
1. Overview
What is congestive heart failure?
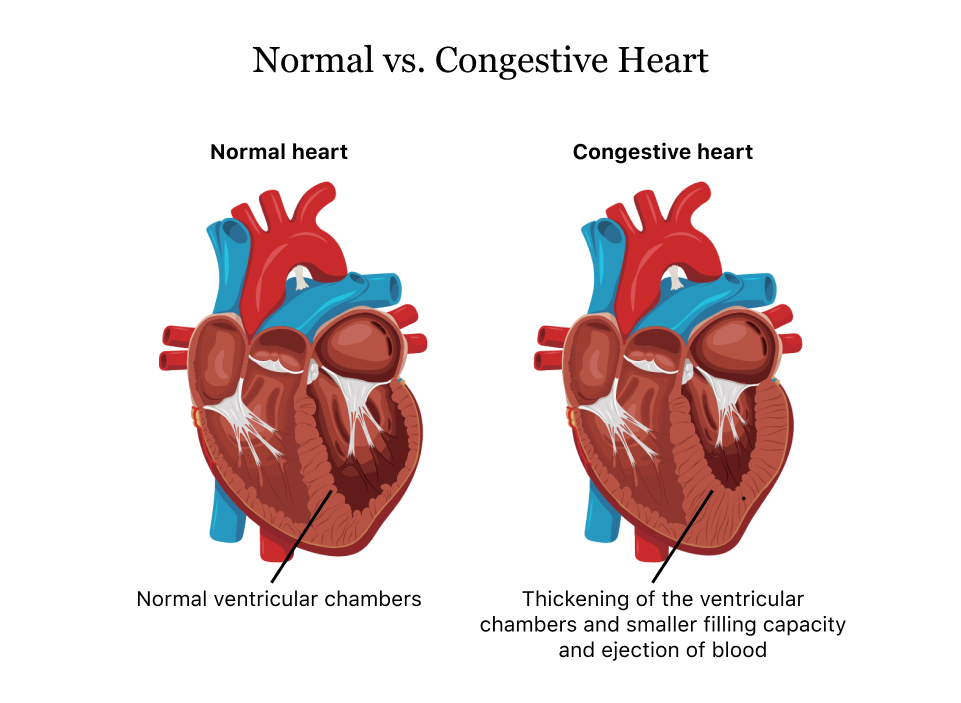
Congestive heart failure (CHF), often simply called heart failure, is a complex clinical syndrome resulting from any structural or functional cardiac disorder that impairs the ability of the heart to fill with or eject blood. It represents the final common pathway of numerous cardiac diseases. Despite its name, heart failure does not mean the heart has “failed” completely, but rather that it is failing to pump efficiently enough to meet the body’s needs. The term “congestive” specifically refers to the accumulation of fluid in body tissues that often accompanies the condition.
Heart failure can be categorized based on:
- Ejection fraction: Heart failure with reduced ejection fraction (HFrEF, <40%), heart failure with mildly reduced ejection fraction (HFmrEF, 40-49%), and heart failure with preserved ejection fraction (HFpEF, ≥50%)
- Side of heart affected: Left-sided, right-sided, or biventricular failure
- Onset: Acute or chronic
- Functional capacity: New York Heart Association (NYHA) Class I-IV
Affected body parts/organs
Heart failure affects multiple body systems through complex pathophysiological mechanisms:
Primary cardiac effects:
- Ventricles: Impaired contractility, remodeling, dilation
- Atria: Enlargement, increased filling pressures
- Heart valves: Functional regurgitation due to chamber dilation
- Coronary circulation: Reduced perfusion pressure
- Cardiac conduction system: Arrhythmias
Secondary systemic effects:
- Lungs: Pulmonary congestion, edema, pleural effusions
- Kidneys: Reduced perfusion, sodium and water retention, cardiorenal syndrome
- Liver: Congestion, impaired function, potential cirrhosis in chronic right heart failure
- Brain: Hypoperfusion, cognitive changes, depression
- Skeletal muscle: Reduced perfusion, deconditioning, sarcopenia
- Gastrointestinal system: Congestion, malabsorption, reduced appetite
- Peripheral circulation: Edema, venous stasis
- Endocrine system: Neurohormonal activation, metabolic abnormalities
Prevalence and significance
Heart failure represents a global health challenge of growing magnitude:
Epidemiology:
- Global prevalence: Estimated 64 million people worldwide
- Lifetime risk: Approximately 20% for persons aged 40 and older
- Age distribution: Prevalence increases dramatically with age (1% in 40s, 10% in 80s)
- Gender differences: Higher incidence in men, but women constitute nearly half of cases due to longer life expectancy
Public health impact:
- Hospitalizations: Leading cause of hospitalization in people over 65
- Economic burden: Annual global cost estimated at $108 billion
- Mortality: 30-40% of patients die within 1 year of diagnosis for advanced heart failure
- Quality of life: Significant impact on functional capacity and independence
- Healthcare utilization: High rate of readmissions (25% within 30 days)
- Societal impact: Growing burden due to aging populations worldwide
Heart failure thus represents a critical challenge for healthcare systems worldwide, demanding comprehensive strategies for prevention, early diagnosis, effective management, and coordinated care.
2. History & Discoveries
Early recognition and descriptions
The understanding of heart failure has evolved significantly throughout medical history:
Ancient civilizations (3000-1000 BCE):
- Egyptian papyri contain descriptions of heart disorders and fluid retention
- Ayurvedic texts from India described a condition resembling heart failure
- Traditional Chinese medicine recognized patterns similar to heart failure symptoms
Greco-Roman medicine (400 BCE-400 CE):
- Hippocrates described dropsy (edema) and linked it to the heart
- Galen theorized that the heart was the center of innate heat and vital spirits
- Early recognition of fluid accumulation as a medical problem
Middle Ages and Renaissance (500-1500 CE):
- Limited advancement in cardiac understanding
- Persistence of humoral theories of disease
- Initial anatomical studies by vesalius and others
Key historical figures and discoveries
The modern understanding of heart failure emerged through the work of numerous physicians:
- William Harvey (1628): Discovered circulatory system function, providing the basis for understanding heart failure
- Giovanni Morgagni (18th century): Conducted early pathological studies linking cardiac enlargement to symptoms
- René Laennec (1819): Invented the stethoscope, enabling better diagnosis of cardiac conditions
- James Hope (1832): Published comprehensive work on heart diseases, describing heart failure patterns
- James Mackenzie (early 1900s): Advanced clinical understanding of heart failure
- Ernst Starling (1918): Described the relationship between cardiac filling pressure and cardiac output (Starling’s law)
- Willem Einthoven (1924): Nobel Prize for the electrocardiogram, revolutionizing cardiac diagnosis
- Helen Taussig and Alfred Blalock (1944): Pioneered surgical procedures for congenital heart defects
- André Cournand, Werner Forssmann, and Dickinson Richards (1956): Nobel Prize for cardiac catheterization development
- Eugene Braunwald (1960s-present): Transformed understanding of heart failure pathophysiology
Major breakthroughs in research and treatment
The management of heart failure has seen remarkable advances over the past century:
- 1785-1850s: Foxglove plant (digitalis) recognized for treating dropsy by William Withering
- 1950s: Introduction of thiazide diuretics
- 1960s: First heart transplant by Christiaan Barnard (1967)
- 1970s-1980s: Development of vasodilator therapy
- 1980s-1990s:
- ACE inhibitors demonstrated to improve survival
- Beta-blockers, initially contraindicated, shown to provide mortality benefit
- Initial development of left ventricular assist devices (LVADs)
- 1990s-2000s:
- Angiotensin receptor blockers (ARBs) introduced
- Cardiac resynchronization therapy developed
- Implantable cardioverter-defibrillators (ICDs) for prevention of sudden cardiac death
- 2000s-2010s:
- Aldosterone antagonists shown to improve outcomes
- Continuous flow LVADs developed
- Natriuretic peptides recognized as diagnostic markers
- 2010s-present:
- SGLT2 inhibitors discovered to reduce heart failure events
- Angiotensin receptor-neprilysin inhibitors (ARNIs) demonstrated superiority over ACE inhibitors
- Advances in minimally invasive structural heart interventions
- Remote monitoring technologies
Evolution of medical understanding
The conceptual framework for heart failure has transformed dramatically:
- Pre-20th century: Focus on symptoms (dropsy) rather than cardiac function
- Early 20th century: Cardiorenal model emphasizing fluid retention
- Mid-20th century: Cardiocirculatory model focusing on hemodynamics
- 1970s-1980s: Neurohormonal model recognizing compensatory mechanisms that become maladaptive
- 1990s-2000s: Ventricular remodeling concept and recognition of inflammation and oxidative stress
- 2000s-2010s: Differentiation of HFrEF vs. HFpEF as distinct syndromes
- Current paradigm: Multi-system disorder involving complex interactions between:
- Cardiac dysfunction
- Neurohormonal activation
- Inflammation
- Renal impairment
- Metabolic abnormalities
- Genetic factors
- Comorbidities
- Aging biology
This evolution reflects a shift from viewing heart failure as primarily a hemodynamic disorder to understanding it as a complex syndrome with multiple pathophysiological mechanisms, requiring comprehensive approaches to management.
3. Symptoms
Early symptoms
The initial presentation of heart failure often includes subtle manifestations that may be overlooked or attributed to aging or deconditioning:
Cardiovascular symptoms:
- Exertional dyspnea: Initially occurs during moderate activity, the earliest and most common symptom
- Reduced exercise tolerance: Difficulty completing previously routine activities
- Fatigue: Persistent tiredness disproportionate to activity level
- Mild ankle swelling: Often noticed at the end of the day
- Orthopnea: Need to use more pillows to breathe comfortably when lying flat
- Nocturnal cough: Dry, non-productive cough when recumbent
- Heart palpitations: Awareness of irregular or rapid heartbeat
Non-specific symptoms:
- Nocturia: Increased urination at night
- Mild cognitive changes: Difficulty concentrating, mild memory issues
- Sleep disturbances: Trouble sleeping, frequent awakening
- Reduced appetite: Gradual decrease in food intake
- Subtle weight changes: May gain weight (fluid retention) or lose weight (cardiac cachexia)
These early symptoms often develop insidiously and may be interpreted as normal aging, stress, or deconditioning, contributing to delayed diagnosis.
Advanced-stage symptoms
As heart failure progresses, symptoms become more pronounced and debilitating:
Severe cardiac symptoms:
- Dyspnea at rest: Difficulty breathing even without exertion
- Paroxysmal nocturnal dyspnea: Sudden awakening with severe breathlessness
- Orthopnea requiring multiple pillows or sleeping upright
- Severe peripheral edema: Swelling of legs, ankles, sometimes extending to thighs and genitalia
- Ascites: Abdominal swelling due to fluid accumulation
- Angina: Chest pain, particularly in heart failure due to coronary artery disease
- Severe fatigue and weakness: Profound limitation of daily activities
- Syncope or presyncope: Fainting or near-fainting episodes
Systemic manifestations:
- Pulmonary crackles/rales: Audible with breathing
- Persistent cough with pink, frothy sputum: Sign of pulmonary edema
- Anorexia and nausea: Due to gastrointestinal congestion and reduced perfusion
- Abdominal pain: From liver congestion and bowel edema
- Cheyne-Stokes respiration: Periodic breathing pattern with apneic periods
- Cyanosis: Bluish discoloration of lips, fingers
- Significant weight loss and muscle wasting: Cardiac cachexia
- Confusion and altered mental status: From cerebral hypoperfusion
End-stage manifestations:
- Cardiogenic shock: Hypotension, poor peripheral perfusion, organ dysfunction
- Severe liver dysfunction: Jaundice from congestive hepatopathy
- Renal failure: Oliguria, anuria
- Severe respiratory distress and pulmonary edema
Symptom progression and patterns
Heart failure symptoms typically evolve in patterns that reflect the underlying pathophysiology:
Progression timeline:
- Stage A (Pre-heart failure): Asymptomatic with risk factors but no structural heart disease
- Stage B (Pre-clinical): Structural heart disease without symptoms
- Stage C (Symptomatic): Structural heart disease with current or previous symptoms
- Stage D (Advanced): Refractory symptoms requiring specialized interventions
Progression patterns:
- Gradual deterioration: Slow, progressive worsening over years
- Stepwise decline: Periods of stability interrupted by acute decompensations
- Plateau with acute exacerbations: Relatively stable baseline with periodic severe episodes
- Rapid progression: Quick deterioration over months (e.g., in some inflammatory cardiomyopathies)
Symptom variations by heart failure type:
- Left-sided heart failure: Predominantly respiratory symptoms (dyspnea, orthopnea)
- Right-sided heart failure: Predominantly congestive symptoms (edema, ascites, hepatomegaly)
- HFrEF vs. HFpEF: Similar symptoms but potentially different triggers and progression
- Acute vs. chronic: Acute heart failure presents more dramatically with severe, sudden-onset symptoms
Functional classification (NYHA):
- Class I: No limitation of physical activity
- Class II: Slight limitation; comfortable at rest but ordinary activity causes symptoms
- Class III: Marked limitation; comfortable at rest but less than ordinary activity causes symptoms
- Class IV: Unable to carry out any physical activity without discomfort; symptoms at rest
Understanding symptom patterns helps guide treatment strategies and predict prognosis, with symptom progression often correlating with underlying pathophysiological changes and disease severity.
4. Causes
Biological mechanisms
Heart failure develops through complex pathophysiological processes that initially attempt to compensate for reduced cardiac performance but ultimately become maladaptive:
Primary cardiac pathophysiology:
- Impaired contractility: Reduced force generation by cardiac myocytes
- Increased afterload: Greater resistance to ventricular emptying (e.g., hypertension, aortic stenosis)
- Increased preload: Excessive ventricular filling pressures
- Impaired relaxation/compliance: Stiff ventricle unable to fill properly
- Rhythm disturbances: Arrhythmias affecting cardiac output
- Valve dysfunction: Stenosis or regurgitation affecting blood flow
- Ventricular remodeling: Progressive changes in ventricular size, shape, and function
- Myocyte hypertrophy
- Myocyte loss through apoptosis and necrosis
- Fibroblast proliferation and fibrosis
- Extracellular matrix alteration
Compensatory mechanisms that become detrimental:
Neurohormonal activation:
- Sympathetic nervous system activation → tachycardia, vasoconstriction
- Renin-angiotensin-aldosterone system → sodium/water retention, vasoconstriction, fibrosis
- Vasopressin release → water retention
- Natriuretic peptides (compensatory but insufficient)
Inflammatory and oxidative processes:
- Pro-inflammatory cytokine production
- Oxidative stress damaging cellular components
- Nitric oxide dysregulation
- Endothelial dysfunction
Metabolic abnormalities:
- Impaired myocardial energetics
- Insulin resistance
- Mitochondrial dysfunction
- Calcium handling defects
Etiological causes
Heart failure has numerous potential underlying causes:
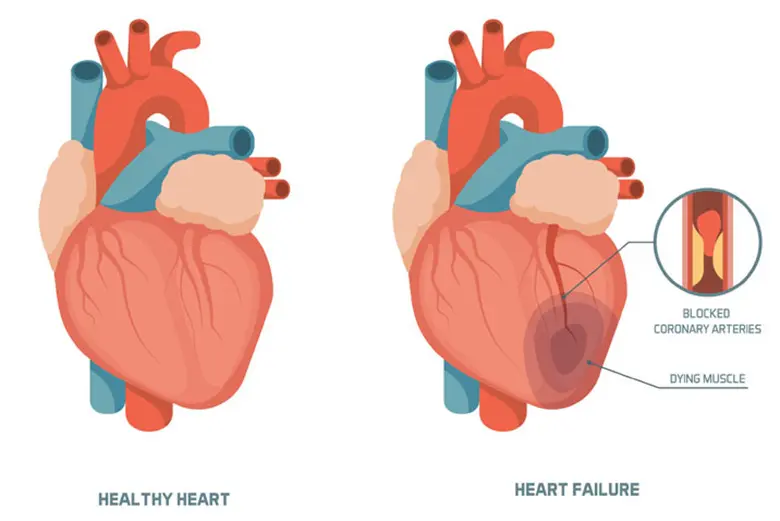
Ischemic causes:
- Coronary artery disease and myocardial infarction
- Chronic myocardial ischemia
- Hibernating or stunned myocardium
Non-ischemic causes:
- Hypertension: Leading cause globally
- Valvular heart disease: Stenosis or regurgitation of any valve
- Cardiomyopathies:
- Dilated cardiomyopathy
- Hypertrophic cardiomyopathy
- Restrictive cardiomyopathy
- Arrhythmogenic cardiomyopathy
- Left ventricular non-compaction
- Congenital heart disease: Both repaired and unrepaired
- Arrhythmias: Particularly atrial fibrillation and prolonged tachycardias
- Toxic/drug-induced: Alcohol, cocaine, certain chemotherapies (anthracyclines)
- Infectious: Viral myocarditis, Chagas disease, HIV-associated
- Inflammatory: Sarcoidosis, autoimmune conditions
- Infiltrative diseases: Amyloidosis, hemochromatosis, sarcoidosis
- Peripartum cardiomyopathy: Occurs in late pregnancy or postpartum
- High-output states: Anemia, thyrotoxicosis, arteriovenous fistulas, Paget’s disease
- Right ventricular failure causes: Pulmonary hypertension, pulmonary embolism
Genetic and hereditary factors
Genetic contributions to heart failure are increasingly recognized:
Monogenic cardiomyopathies:
- Hypertrophic cardiomyopathy: Mutations in sarcomeric proteins
- β-myosin heavy chain (MYH7)
- Cardiac myosin-binding protein C (MYBPC3)
- Troponin T (TNNT2)
- Multiple others
- Dilated cardiomyopathy: Over 40 genes identified
- Titin (TTN) – most common, 15-25% of familial cases
- Lamin A/C (LMNA)
- RNA-binding motif protein 20 (RBM20)
- Multiple others
- Arrhythmogenic cardiomyopathy: Desmosomal protein genes
- Plakophilin-2 (PKP2)
- Desmoplakin (DSP)
- Desmoglein-2 (DSG2)
- Restrictive cardiomyopathy: Various genes
- Troponin I (TNNI3)
- Desmin (DES)
- Left ventricular non-compaction: Multiple genes
- Primarily sarcomeric genes (overlap with HCM and DCM)
Inherited metabolic disorders:
- Fabry disease (GLA gene)
- Danon disease (LAMP2 gene)
- Mitochondrial cardiomyopathies (multiple genes)
- Hemochromatosis (HFE gene)
- Transthyretin amyloidosis (TTR gene)
Genetic risk factors for common heart failure:
- Polymorphisms affecting:
- Natriuretic peptide pathways
- Adrenergic receptors
- Renin-angiotensin-aldosterone system
- Inflammatory pathways
Inheritance patterns:
- Autosomal dominant (most common in familial cardiomyopathies)
- Autosomal recessive
- X-linked
- Matrilineal (mitochondrial)
- Complex polygenic inheritance
Genetic testing implications:
- Cascade screening for family members
- Prognostic information
- Potential therapeutic implications
- Reproductive counseling
Environmental triggers and exacerbating factors
Environmental factors can trigger or worsen heart failure:
Direct cardiotoxins:
- Alcohol (dose-dependent effects)
- Cocaine and amphetamines
- Certain chemotherapeutic agents
- Heavy metals (lead, cobalt)
- Industrial chemicals (carbon monoxide)
Medications that may precipitate heart failure:
- NSAIDs (fluid retention, hypertension)
- Thiazolidinediones (fluid retention)
- Some anti-cancer agents (anthracyclines, trastuzumab)
- Some antiarrhythmics (flecainide, propafenone in structural heart disease)
- Some calcium channel blockers (verapamil, diltiazem in systolic dysfunction)
- Corticosteroids and hormonal therapies
Acute precipitants of heart failure decompensation:
- Medication non-adherence
- Dietary indiscretion (excessive sodium intake)
- Acute infection or sepsis
- Arrhythmias (especially atrial fibrillation)
- Myocardial ischemia or infarction
- Uncontrolled hypertension
- Pulmonary embolism
- Pregnancy
- Progression of underlying heart disease
- Anemia
- Thyroid disorders (hyper- or hypothyroidism)
- Renal dysfunction
- Environmental temperature extremes
- Physical or emotional stress
- Alcohol or drug abuse
Understanding the complex interplay between biological mechanisms, underlying causes, genetic predisposition, and environmental factors is essential for comprehensive management and prevention strategies tailored to individual patients.
5. Risk Factors
Demographic risk factors
Certain demographic characteristics significantly influence heart failure risk:
Age:
- Most powerful risk factor for heart failure
- Incidence doubles each decade after age 45
- Prevalence rises from <1% in under-50s to >10% in over-80s
- Aging-associated changes (vascular stiffening, fibrosis, reduced regenerative capacity)
- Different heart failure phenotypes by age (HFpEF more common in elderly)
Sex/gender:
- Men have higher incidence of heart failure at younger ages
- Women develop heart failure later but have higher lifetime risk due to longevity
- Women more likely to develop HFpEF than HFrEF
- Different underlying etiologies (men more ischemic, women more hypertensive)
- Potential hormonal influences (estrogen effects on cardiac remodeling)
Race/ethnicity:
- African Americans have higher incidence and prevalence
- 20% higher risk of heart failure than whites
- Earlier onset (average 5-10 years younger)
- Higher rates of hypertensive heart failure
- Potentially different response to certain medications
- Hispanic populations show geographical variations in risk
- South Asians at elevated risk, particularly at younger ages
- Differences reflect complex interactions between genetics, healthcare access, socioeconomic factors, and prevalence of risk factors
Socioeconomic factors:
- Lower socioeconomic status associated with:
- Higher heart failure incidence
- Poorer outcomes after diagnosis
- Less access to preventive care
- Higher rates of risk factors
- Educational level inversely associated with heart failure risk
- Healthcare access disparities influence disease management
Medical and lifestyle risk factors
Established medical risk factors:
- Coronary artery disease: 2-3 fold increased risk
- Prior myocardial infarction confers 5-10 fold increased risk
- Ischemic heart disease accounts for approximately 60-70% of HFrEF cases
- Hypertension: Major contributor to heart failure
- Doubles risk in men, triples risk in women
- Strongest population-attributable risk due to high prevalence
- Long duration and poor control increase risk substantially
- Particularly important for HFpEF development
- Diabetes mellitus: 2-5 fold increased risk
- Independent risk factor beyond associated coronary disease
- Direct diabetic cardiomyopathy from metabolic derangements
- Risk increases with duration and severity of diabetes
- Synergistic effects with other risk factors
- Obesity: Independent dose-dependent relationship
- 5-7% increased risk per BMI unit above normal
- Both direct effects (cardiac adiposity, inflammation)
- Indirect effects through associated conditions
- Obesity cardiomyopathy in severe cases
- Metabolic syndrome: Cluster of risk factors
- Greater than additive risk from individual components
- Central obesity particularly significant
- Valvular heart disease: Progressive burden on cardiac function
- Aortic stenosis or regurgitation
- Mitral regurgitation or stenosis
- Risk proportional to severity and duration
- Arrhythmias:
- Atrial fibrillation associated with 3-fold increased risk
- Prolonged tachyarrhythmias can lead to tachycardia-induced cardiomyopathy
Lifestyle risk factors:
- Smoking: 40-50% increased risk
- Dose-dependent relationship (pack-years)
- Both direct cardiotoxic effects and indirect through vascular disease
- Partial reversibility with cessation
- Alcohol consumption:
- J-shaped curve relationship
- Moderate intake may be neutral or slightly protective
- Heavy consumption (>90g/day) increases risk significantly
- Alcoholic cardiomyopathy with prolonged heavy use
- Physical inactivity: Independent risk factor
- Sedentary lifestyle associated with 30-50% increased risk
- Regular activity provides substantial protection
- Dietary factors:
- High sodium intake: Associated with hypertension and direct myocardial effects
- Poor quality diet: Low in fruits, vegetables, whole grains
- Processed food consumption
- Excessive calories leading to obesity
- Sleep disorders:
- Obstructive sleep apnea: 2-3 fold increased risk
- Insomnia and poor sleep quality
- Shift work disrupting normal patterns
Impact of pre-existing conditions
Cardiovascular conditions:
- Left ventricular hypertrophy: Strong precursor to heart failure
- 2-3 fold increased risk independent of blood pressure
- Asymptomatic left ventricular dysfunction:
- 5-fold increased risk of symptomatic heart failure
- Annual progression rate of 5-10%
- Peripheral arterial disease:
- Marker for systemic atherosclerosis
- Associated with 30% increased heart failure risk
- Cerebrovascular disease:
- Shared risk factors and pathophysiology
- 25-30% increased heart failure risk after stroke
Non-cardiovascular conditions:
- Chronic kidney disease:
- Bidirectional relationship with heart failure
- Each 10 mL/min reduction in GFR increases risk by 25%
- Cardiorenal syndrome mechanisms
- Chronic lung disease:
- COPD associated with 30% increased risk
- Diagnostic challenges due to symptom overlap
- Shared inflammatory pathways
- Thyroid disorders:
- Both hyper- and hypothyroidism increase risk
- Direct effects on cardiac contractility and loading conditions
- Anemia:
- Associated with progression and worsening outcomes
- Both cause and consequence of heart failure
- Depression and psychological stress:
- 40-60% increased risk with chronic depression
- Potential neuroendocrine and behavioral mechanisms
- Autoimmune disorders:
- Rheumatoid arthritis: 70% increased risk
- Systemic lupus erythematosus: 2-fold increased risk
- Both direct inflammatory effects and medication side effects
- HIV infection:
- 50-100% increased risk
- Combination of direct viral effects, inflammation, and antiretroviral toxicities
- Cancer therapies:
- Anthracyclines: Dose-dependent risk (1-5% at standard doses)
- Trastuzumab: 2-4% risk as monotherapy, higher in combination
- Radiation therapy to chest: Long-term risk proportional to dose
- Emerging risks with newer targeted therapies and immunotherapies
Risk factor clustering:
- Multiple risk factors show synergistic rather than merely additive effects
- Risk prediction models (e.g., ARIC HF Risk Score, Health ABC HF Risk Score) incorporate multiple factors
- Risk factor modification more effective when addressing multiple factors simultaneously
Understanding these complex and interacting risk factors enables targeted prevention strategies, early intervention in high-risk individuals, and comprehensive management approaches for those with established heart failure.
6. Complications
Cardiovascular complications
Arrhythmias:
- Atrial fibrillation/flutter: 30-40% of heart failure patients
- Both cause and consequence of heart failure
- Associated with increased mortality and hospitalization
- Thromboembolic risk
- Reduced exercise capacity
- Ventricular arrhythmias:
- Premature ventricular contractions
- Ventricular tachycardia (15-20% of advanced heart failure)
- Ventricular fibrillation
- Leading cause of sudden cardiac death in heart failure
- Bradyarrhythmias:
- Sinus node dysfunction
- Atrioventricular blocks
- May be exacerbated by necessary medications
Thromboembolic complications:
- Stroke: 1.5-3 fold increased risk
- Higher with atrial fibrillation
- Embolic strokes more common
- Venous thromboembolism:
- Deep vein thrombosis (increased risk due to venous stasis)
- Pulmonary embolism (can precipitate acute decompensation)
- Peripheral arterial thromboembolism: Less common but serious
Structural cardiovascular complications:
- Functional mitral regurgitation:
- Secondary to ventricular dilation and remodeling
- Creates vicious cycle worsening heart failure
- Tricuspid regurgitation:
- Common in right heart failure
- Associated with worse outcomes
- Progressive ventricular dilation:
- Self-perpetuating cycle of remodeling
- Increasingly spherical ventricle with less efficient contraction
- Ventricular aneurysm formation:
- Following large myocardial infarctions
- Risk of thrombus formation
- Ventricular rupture: Rare but catastrophic complication
Hemodynamic complications:
- Cardiogenic shock:
- Profound systemic hypoperfusion
- Multi-organ dysfunction
- 30-50% in-hospital mortality
- Pulmonary hypertension:
- Initially reactive/reversible
- Can become fixed with chronic elevation
- Associated with right ventricular failure
- Right ventricular failure:
- Often follows left heart failure
- Associated with worse prognosis
- Systemic venous congestion
Systemic complications
Pulmonary complications:
- Pulmonary edema:
- Acute: Medical emergency with respiratory distress
- Chronic: Persistent lung congestion and impaired gas exchange
- Pleural effusions:
- Present in 30-50% of hospitalized patients
- Contribute to dyspnea
- Usually bilateral but may be right-predominant
- Pulmonary fibrosis:
- Long-term consequence of recurrent pulmonary edema
- Reduced lung compliance and diffusion capacity
- Pulmonary infections:
- Increased susceptibility due to congestion
- Higher complication rates from respiratory infections
Renal complications:
- Cardiorenal syndrome:
- Bidirectional heart-kidney dysfunction
- Progressive decline in GFR
- Resistance to diuretics
- Heightened mortality risk
- Acute kidney injury:
- During decompensations or from treatments
- Predictor of poor outcomes
- Chronic kidney disease progression:
- Shared risk factors and pathophysiology
- Challenging medical management
Hepatobiliary complications:
- Congestive hepatopathy:
- Elevated liver enzymes in 20-30%
- Right upper quadrant discomfort
- Impaired synthetic function in advanced cases
- Cardiac cirrhosis:
- Long-term consequence of hepatic congestion
- Portal hypertension
- May be irreversible
- Cholestasis and gallstone formation:
- Altered bile composition
- Reduced gallbladder motility
Gastrointestinal complications:
- Gut congestion:
- Malabsorption
- Protein-losing enteropathy (severe cases)
- Reduced appetite and early satiety
- Mesenteric ischemia:
- Chronic or acute
- Abdominal pain, altered bowel habits
- Drug-related complications:
- Anticoagulant-related bleeding
- NSAID-induced worsening
Hematologic complications:
- Anemia:
- Present in 30-50% of patients
- Multifactorial etiology
- Associated with worse functional capacity and outcomes
- Iron deficiency:
- Common even without anemia
- Impairs cellular energetics and exercise capacity
- Thrombocytopenia:
- Due to congestion, medications, or comorbidities
Metabolic and endocrine complications:
- Cardiac cachexia:
- Involuntary weight loss >6% over 6-12 months
- Associated with 2-3 fold increased mortality
- Multifactorial: inflammation, catabolism, malnutrition
- Insulin resistance and diabetes:
- Bidirectional relationship
- Impaired glucose handling
- Micronutrient deficiencies:
- Vitamin D, thiamine, selenium, zinc
- May exacerbate cardiac dysfunction
Neuropsychiatric complications:
- Cognitive impairment:
- Present in 25-50% of heart failure patients
- Ranges from mild deficits to dementia
- Associated with poor self-care and outcomes
- Depression:
- Affects 20-40% of patients
- Associated with increased hospitalization and mortality
- Bidirectional relationship with heart failure
- Anxiety disorders:
- Acute anxiety during decompensations
- Chronic anxiety affecting quality of life
- Sleep disorders:
- Insomnia, sleep-disordered breathing
- Cheyne-Stokes respiration
- Central sleep apnea in 30-50%
Mortality and disability
Mortality patterns:
- Overall mortality: 50% at 5 years from diagnosis
- Annual mortality:
- NYHA Class I: 5-10%
- NYHA Class II: 10-15%
- NYHA Class III: 15-20%
- NYHA Class IV: 30-50%
- Mode of death:
- Progressive heart failure (pump failure): 40-50%
- Sudden cardiac death: 30-40%
- Non-cardiovascular causes: 10-15%
- Predictors of mortality:
- NYHA functional class
- Ejection fraction
- Natriuretic peptide levels
- Renal function
- Systolic blood pressure
- Comorbidity burden
- Frailty
Hospitalization burden:
- Leading cause of hospitalization in those >65 years
- 25% readmission rate within 30 days
- Average 1-2 hospitalizations annually in symptomatic patients
- Each hospitalization associated with increased mortality risk
Functional disability:
- Progressive limitation of activities of daily living
- Loss of independence
- Reduced quality of life scores comparable to end-stage cancer
- High caregiver burden
- Significant work disability and productivity loss
Economic and societal impact:
- Direct medical costs averaging $30,000-40,000 per patient annually
- Indirect costs through lost productivity
- Informal caregiving burden
- Reduced contribution to workforce and society
These complications highlight why heart failure requires comprehensive management beyond cardiac function alone, addressing the multi-system nature of the syndrome and its profound impact on patients’ lives.
7. Diagnosis & Testing
Clinical evaluation
The diagnostic approach to heart failure begins with thorough clinical assessment:
History taking:
- Detailed symptom assessment (dyspnea, fatigue, edema, orthopnea)
- Symptom progression and timeline
- Prior cardiovascular events or procedures
- Risk factor evaluation
- Medication review (both cardiac and non-cardiac)
- Family history of cardiac disease
- Impact on functional capacity and quality of life
- Dietary habits, especially sodium intake
- Alcohol consumption pattern
Physical examination:
- Vital signs: Blood pressure, heart rate, respiratory rate, temperature
- General appearance: Cachexia, distress, positioning for breathing
- Jugular venous pressure: Height and waveform
- Cardiac examination:
- Heart sounds (S3 gallop, S4, murmurs)
- Apical displacement
- Precordial heave
- Pulmonary examination:
- Crackles/rales
- Pleural effusions
- Wheezing
- Abdominal examination:
- Hepatomegaly and tenderness
- Ascites
- Hepatojugular reflux
- Extremities:
- Peripheral edema (grading and distribution)
- Peripheral pulses and perfusion
- Temperature
- Skin: Color, turgor, evidence of scratching (pruritus in severe cases)
Functional assessment:
- New York Heart Association (NYHA) classification (I-IV)
- 6-minute walk test
- Cardiopulmonary exercise testing for selected patients
- Activities of daily living evaluation
Laboratory testing
Routine laboratory tests:
- Complete blood count: Anemia, infection, polycythemia
- Comprehensive metabolic panel:
- Electrolytes (sodium, potassium, calcium, magnesium)
- Renal function (BUN, creatinine, estimated GFR)
- Liver function tests
- Glucose
- Lipid profile: Assess cardiovascular risk
- Thyroid function tests: Hyper- or hypothyroidism can cause or exacerbate heart failure
- Iron studies: Ferritin, transferrin saturation
- Urinalysis: Protein, specific gravity
Cardiac biomarkers:
- Natriuretic peptides:
- B-type natriuretic peptide (BNP)
- N-terminal pro-B-type natriuretic peptide (NT-proBNP)
- Key diagnostic markers
- Prognostic value
- Treatment monitoring
- Different cutoffs based on clinical context
- Cardiac troponins:
- May be elevated in acute decompensation without infarction
- Prognostic significance
- High-sensitivity assays detect subclinical myocardial injury
- Novel biomarkers:
- ST2 (member of interleukin-1 receptor family)
- Galectin-3 (marker of fibrosis)
- Growth differentiation factor-15
- Mid-regional pro-ANP
- High-sensitivity C-reactive protein
Specialized laboratory testing:
- Genetic testing:
- For suspected familial cardiomyopathies
- When genetic etiology suspected based on age, family history
- Specific etiological testing:
- Hemochromatosis: Ferritin, transferrin saturation
- Amyloidosis: Serum free light chains, immunofixation
- Sarcoidosis: ACE levels, calcium
- HIV testing when risk factors present
- Autoimmune markers in appropriate clinical context
- Drug level monitoring:
- Therapeutic drug monitoring for certain medications
- Digoxin levels when toxicity suspected
Imaging studies
Echocardiography:
- Cornerstone of heart failure diagnosis
- Provides assessment of:
- Left ventricular systolic function (ejection fraction)
- Left ventricular diastolic function
- Chamber sizes and wall thickness
- Regional wall motion abnormalities
- Valvular function
- Right ventricular function
- Pulmonary pressures (estimated)
- Pericardial disease
- Multiple modalities:
- Transthoracic echocardiography (TTE): First-line
- Transesophageal echocardiography (TEE): Better visualization of certain structures
- Stress echocardiography: Assesses ischemia and contractile reserve
- 3D echocardiography: More accurate volumetric assessment
Chest X-ray:
- Evaluates:
- Cardiac size and contour
- Pulmonary congestion
- Pleural effusions
- Alternative pulmonary diagnoses
- May be normal in compensated or early heart failure
Cardiac magnetic resonance imaging (CMR):
- Gold standard for ventricular volumes and ejection fraction
- Superior tissue characterization:
- Myocardial fibrosis (late gadolinium enhancement)
- Edema
- Infiltration
- Inflammation
- Particularly valuable for:
- Cardiomyopathy etiology determination
- Right ventricular assessment
- Congenital heart disease
- Viability assessment
Cardiac computed tomography (CT):
- Coronary artery disease assessment
- Structural evaluation
- Pericardial assessment
- Alternative to CMR when contraindicated
- Radiation exposure consideration
Nuclear imaging:
- Multigated acquisition scan (MUGA):
- Accurate ejection fraction assessment
- Used when echocardiography suboptimal
- Myocardial perfusion imaging:
- Assesses ischemia and viability
- Helps determine ischemic etiology
- PET imaging:
- Metabolic assessment
- Inflammation detection (e.g., cardiac sarcoidosis)
- Amyloid detection with specific tracers
Other diagnostic procedures
Electrocardiogram (ECG):
- Standard 12-lead ECG evaluates:
- Rhythm abnormalities
- Conduction disturbances
- Chamber enlargement
- Prior myocardial infarction
- Acute ischemia
- Electrolyte imbalances
- Rarely normal in heart failure
Ambulatory monitoring:
- Holter monitoring (24-48 hours)
- Extended event monitoring (up to 30 days)
- Implantable loop recorders
- Useful for:
- Arrhythmia detection
- Correlation of symptoms with rhythm
- Risk stratification
Cardiopulmonary exercise testing (CPET):
- Provides objective assessment of:
- Functional capacity (peak VO2)
- Ventilatory efficiency (VE/VCO2 slope)
- Chronotropic response
- Blood pressure response
- Valuable for:
- Prognosis determination
- Transplant evaluation
- Differentiating cardiac vs. pulmonary limitation
Cardiac catheterization:
- Left heart catheterization:
- Coronary angiography to assess ischemic etiology
- Left ventricular end-diastolic pressure
- Ventriculography for function and regional wall motion
- Right heart catheterization:
- Pulmonary artery pressures
- Cardiac output/index
- Pulmonary capillary wedge pressure
- Pulmonary vascular resistance
- Systemic vascular resistance
- Response to vasodilator challenge
Endomyocardial biopsy:
- Limited role in routine diagnosis
- Indications:
- Suspected myocarditis
- Infiltrative diseases
- Unexplained new-onset heart failure
- Suspected transplant rejection
Sleep studies:
- Polysomnography to assess for:
- Obstructive sleep apnea
- Central sleep apnea
- Cheyne-Stokes respiration
- Increasingly recognized contribution to heart failure
Diagnostic algorithms and classification
Diagnostic pathway:
- Clinical suspicion based on symptoms and risk factors
- Initial evaluation with history, physical examination, ECG, chest X-ray
- Natriuretic peptide testing
- Echocardiography for confirmation and phenotyping
- Additional testing based on clinical context
Heart failure classification by ejection fraction:
- HFrEF: Heart failure with reduced ejection fraction (EF <40%)
- HFmrEF: Heart failure with mildly reduced ejection fraction (EF 40-49%)
- HFpEF: Heart failure with preserved ejection fraction (EF ≥50%)
Heart failure stages (ACC/AHA):
- Stage A: Risk factors but no structural heart disease or symptoms
- Stage B: Structural heart disease but no symptoms
- Stage C: Structural heart disease with current or prior symptoms
- Stage D: Refractory heart failure requiring specialized interventions
New York Heart Association (NYHA) functional classification:
- Class I: No limitation of physical activity
- Class II: Slight limitation of physical activity
- Class III: Marked limitation of physical activity
- Class IV: Unable to carry on any physical activity without discomfort
Diagnostic challenges:
- Distinguishing heart failure from other causes of dyspnea
- Diagnosing HFpEF (often a diagnosis of exclusion)
- Determining specific etiology
- Identifying heart failure in patients with comorbidities (COPD, obesity)
- Early diagnosis before significant structural changes
Comprehensive diagnosis involves integrating clinical assessment with appropriate testing to confirm the presence of heart failure, determine its type and severity, identify underlying causes, and guide treatment strategies.
8. Treatment Options
General management principles
The approach to heart failure management is multifaceted:
Treatment goals:
- Improve survival
- Reduce hospitalizations
- Alleviate symptoms
- Improve functional capacity
- Enhance quality of life
- Slow or reverse cardiac remodeling
- Address underlying causes
- Manage comorbidities
Team-based approach:
- Cardiologists
- Primary care physicians
- Heart failure specialist nurses
- Pharmacists
- Dietitians
- Exercise physiologists
- Physical/occupational therapists
- Social workers
- Palliative care specialists
- Mental health professionals
Disease management programs:
- Multidisciplinary heart failure clinics
- Home-based care programs
- Telemonitoring
- Structured follow-up
- Patient education
- Care coordination
- Early intervention for decompensation
Individualized care:
- Consideration of:
- Heart failure phenotype (HFrEF, HFmrEF, HFpEF)
- Etiology
- Comorbidities
- Age and frailty
- Patient preferences and goals
- Socioeconomic factors
Pharmacological therapies
Core medications for HFrEF:
Renin-angiotensin system inhibitors:
- Angiotensin-converting enzyme (ACE) inhibitors:
- First-line therapy
- Mortality benefit (20-25% reduction)
- Examples: enalapril, lisinopril, ramipril
- Monitor for cough, angioedema, hyperkalemia, renal dysfunction
- Angiotensin receptor blockers (ARBs):
- Alternative in ACE inhibitor-intolerant patients
- Examples: candesartan, valsartan, losartan
- Similar monitoring as ACE inhibitors
- Angiotensin receptor-neprilysin inhibitor (ARNI):
- Sacubitril/valsartan
- Superior to ACE inhibitors in reducing cardiovascular death and hospitalization
- Preferred over ACE inhibitors/ARBs in appropriate patients
- Monitor for hypotension, hyperkalemia, renal dysfunction
- Angiotensin-converting enzyme (ACE) inhibitors:
Beta-blockers:
- Mortality benefit (30-35% reduction)
- Evidence-based options: carvedilol, metoprolol succinate, bisoprolol
- Start at low dose and titrate gradually
- Continue during mild to moderate exacerbations
- Monitor for bradycardia, hypotension, bronchospasm, fatigue
Mineralocorticoid receptor antagonists (MRAs):
- Spironolactone, eplerenone
- Mortality benefit (15-30% reduction)
- Monitor for hyperkalemia, worsening renal function, gynecomastia (spironolactone)
Sodium-glucose cotransporter-2 (SGLT2) inhibitors:
- Dapagliflozin, empagliflozin
- Reduce heart failure hospitalizations and cardiovascular death
- Benefits independent of diabetes status
- Monitor for urinary tract infections, genital infections, volume depletion
Additional medications for HFrEF:
Ivabradine:
- Indication: Sinus rhythm with heart rate ≥70 despite maximally tolerated beta-blocker
- Reduces hospitalization
- Monitor for bradycardia, visual disturbances
Hydralazine/isosorbide dinitrate:
- Particularly beneficial in African American patients
- Alternative in patients unable to tolerate RAAS inhibitors
- Monitor for hypotension, headache, lupus-like syndrome
Digoxin:
- Reduces hospitalizations but not mortality
- Consider in patients remaining symptomatic despite other therapies
- Narrow therapeutic window
- Monitor levels and for toxicity
Diuretics:
- Loop diuretics (furosemide, torsemide, bumetanide)
- Thiazide diuretics (often as add-on therapy)
- For symptom relief and volume management
- Not shown to reduce mortality
- Monitor electrolytes, renal function, volume status
Medications for HFpEF:
- More limited evidence-based options
- Focus on symptom management and comorbidities
- SGLT2 inhibitors showing benefit in recent trials
- Diuretics for congestion
- Aggressive blood pressure control
- Rate/rhythm control for atrial fibrillation
- Spironolactone in selected patients
Medications for specific etiologies:
- Ischemic heart disease:
- Antiplatelet therapy
- Statins
- Antianginal medications as needed
- Amyloidosis:
- Tafamidis for transthyretin amyloidosis
- Chemotherapy for light chain amyloidosis
- Inflammatory cardiomyopathies:
- Immunosuppressive therapy in selected cases
- Tachycardia-induced cardiomyopathy:
- Antiarrhythmic therapy
- Cardioversion
- Ablation
Devices and surgical interventions
Implantable devices:
- Implantable cardioverter-defibrillator (ICD):
- Primary prevention: EF ≤35% despite optimal medical therapy
- Secondary prevention: Survived cardiac arrest or sustained ventricular arrhythmias
- Reduces sudden cardiac death
- Considerations: life expectancy, comorbidities, patient preferences
- Cardiac resynchronization therapy (CRT):
- Indication: EF ≤35%, QRS duration ≥130ms (especially LBBB)
- Improves symptoms, reduces hospitalizations, improves survival
- Can be combined with defibrillator (CRT-D)
- Remote monitoring devices:
- Implantable hemodynamic monitors
- Provides early warning of decompensation
- Allows proactive management
Interventional procedures:
- Coronary revascularization:
- Percutaneous coronary intervention (PCI)
- Coronary artery bypass grafting (CABG)
- Consider when ischemia contributes to heart failure
- Valve interventions:
- Transcatheter aortic valve replacement (TAVR)
- MitraClip for functional mitral regurgitation
- Surgical valve repair or replacement
- Left atrial appendage occlusion:
- Stroke prevention alternative in atrial fibrillation
- Option when anticoagulation contraindicated
- Atrial fibrillation ablation:
- Rhythm control strategy
- May improve outcomes in selected patients
Advanced surgical options:
- Left ventricular assist devices (LVADs):
- Mechanical circulatory support
- Bridge to transplant
- Destination therapy (lifetime support)
- Significant improvement in survival and quality of life
- Complications: infection, bleeding, stroke, device malfunction
- Heart transplantation:
- Gold standard for end-stage heart failure
- Limited by donor availability
- Excellent outcomes in selected patients
- 1-year survival >90%, 10-year survival >60%
- Requires lifelong immunosuppression
- Ventricular restoration procedures:
- Surgical ventricular reconstruction
- Limited role in contemporary practice
- Experimental surgical approaches:
- Myoblast transplantation
- Bioengineered tissues
- Stem cell implantation
- Dynamic cardiomyoplasty
Lifestyle modifications and rehabilitation
Dietary recommendations:
- Sodium restriction: 2-3g daily for most patients
- Fluid restriction in select patients (severe or hyponatremia)
- Weight monitoring
- Alcohol limitation or abstinence
- Adequate protein intake to prevent cachexia
- Mediterranean diet pattern
- Avoidance of very large meals
Physical activity:
- Regular, structured exercise
- Cardiac rehabilitation programs
- Benefits:
- Improved exercise capacity
- Enhanced quality of life
- Reduced hospitalizations
- Possible mortality benefit
- Initially supervised for safety
- Progressive increase in duration and intensity
- Resistance training as tolerated
Self-care education:
- Symptom recognition and management
- Medication adherence strategies
- Daily weight monitoring
- When to contact healthcare providers
- Dietary adherence
- Activity pacing
Psychosocial support:
- Depression screening and treatment
- Anxiety management
- Support groups
- Caregiver support
- Stress reduction techniques
- Cognitive behavioral therapy
Other lifestyle factors:
- Smoking cessation
- Sleep hygiene
- Vaccination (influenza, pneumococcal, COVID-19)
- Avoidance of extreme temperatures
- Travel planning and precautions
Emerging therapies and clinical trials
Novel pharmacological approaches:
- Cardiac myosin activators:
- Omecamtiv mecarbil: Increases cardiac contractility
- Shown to reduce heart failure events
- Soluble guanylate cyclase stimulators:
- Vericiguat: Enhances nitric oxide signaling
- Reduces cardiovascular death and heart failure hospitalization
- SGLT1/2 dual inhibitors:
- Sotagliflozin and others under development
- Potential advantages over SGLT2-selective inhibitors
- Novel anti-inflammatory agents:
- Targeting specific inflammatory pathways
- IL-1β inhibitors being studied
Cellular and gene therapies:
- Stem cell therapy:
- Mesenchymal stem cells
- Cardiac progenitor cells
- Bone marrow-derived cells
- Multiple delivery methods under investigation
- Gene therapy approaches:
- SERCA2a gene transfer
- Adenylyl cyclase type 6
- MicroRNA modulators
- AAV vector delivery systems
- RNA-based therapies:
- siRNA and antisense oligonucleotides
- Targeting specific pathways in heart failure
Advanced device innovations:
- Next-generation LVADs:
- Smaller, fully implantable designs
- Reduced complication rates
- Partial support devices
- Pulsatile support devices:
- Counterpulsation devices
- Aortic wave energy converters
- Novel monitoring approaches:
- Implantable multiparameter sensors
- Wearable monitoring technologies
- Artificial intelligence integration for predictive analytics
Innovative procedural approaches:
- Cardiac contractility modulation:
- Electrical stimulation to enhance contractility
- Approved for selected patients
- Baroreflex activation therapy:
- Modulation of autonomic nervous system
- Improves symptoms in selected patients
- Renal denervation:
- Targets sympathetic overactivation
- Being evaluated in heart failure
- Intramyocardial injection therapies:
- Growth factors
- Gene constructs
- Stem cells
- Biomaterials for structural support
Personalized medicine approaches:
- Pharmacogenomics to guide medication selection
- Biomarker-guided therapy
- Precision phenotyping for targeted interventions
- Molecular profiling of heart failure subgroups
The treatment landscape for heart failure continues to evolve rapidly, with novel approaches targeting different aspects of the complex pathophysiology. Integration of these advances with established therapies offers increasing hope for improved outcomes in this challenging syndrome.
9. Prevention & Precautionary Measures
Primary prevention
Strategies to prevent initial development of heart failure focus on risk factor management:
Hypertension management:
- Most important modifiable risk factor
- Target BP <130/80 mmHg for most patients
- Regular screening
- Lifestyle measures and pharmacotherapy
- Regular monitoring and medication adjustment
- Population-based strategies for detection and control
Coronary artery disease prevention:
- Lipid management:
- Appropriate statin therapy
- Target LDL based on risk category
- Consider additional lipid-lowering agents in high-risk patients
- Antiplatelet therapy in appropriate patients
- Smoking cessation
- Diabetes management
- Regular physical activity
Valvular heart disease management:
- Timely intervention for significant valvular disease
- Appropriate antibiotic prophylaxis when indicated
- Regular follow-up of moderate valve disease
- Early surgical referral when progression noted
Diabetes management:
- Tight glycemic control
- SGLT2 inhibitors for high-risk patients even without heart failure
- Regular screening for cardiac dysfunction
- Aggressive management of other cardiovascular risk factors
Lifestyle and behavioral interventions:
- Regular physical activity (150+ minutes/week moderate or 75+ minutes/week vigorous)
- Maintenance of healthy weight (BMI 18.5-24.9)
- Heart-healthy diet (Mediterranean or DASH pattern)
- Moderate or no alcohol consumption
- Smoking avoidance/cessation
- Stress management
- Adequate sleep
Specific high-risk group management:
- Cancer patients undergoing cardiotoxic therapy:
- Baseline cardiac assessment
- Monitoring during treatment
- Cardioprotective strategies
- Early intervention for dysfunction
- Genetic risk:
- Screening of family members in heritable cardiomyopathies
- Genetic counseling
- Early preventive measures
- Pregnancy-related risk:
- Pre-conception counseling in high-risk women
- Close monitoring during pregnancy and postpartum
- Team-based care with high-risk obstetrics and cardiology
Secondary prevention
These strategies aim to prevent progression to symptomatic heart failure in those with structural heart disease:
Asymptomatic left ventricular dysfunction management:
- ACE inhibitors or ARBs
- Beta-blockers
- Regular monitoring of ventricular function
- Aggressive risk factor management
- Exercise prescription
- Early intervention for symptoms
Post-myocardial infarction care:
- Comprehensive cardiac rehabilitation
- Optimal medical therapy
- Implantable defibrillator when indicated
- Regular follow-up and reassessment
- Depression screening and management
- Secondary prevention medications
Management of arrhythmias:
- Rhythm control strategies when appropriate
- Rate control for persistent atrial fibrillation
- Anticoagulation for stroke prevention
- Treatment of underlying causes
- Catheter ablation in selected cases
Structural interventions:
- Timely repair of significant valvular disease
- Closure of significant shunts
- Coronary revascularization when appropriate
- Early intervention for congenital defects
Disease management for established heart failure
Optimization of medical therapy:
- Guideline-directed medical therapy at target doses
- Regular review and adjustment
- Medication reconciliation
- Adherence support strategies
- Minimization of potentially harmful medications
Self-care management:
- Daily weight monitoring
- Symptom monitoring
- Flexible diuretic protocols
- Dietary adherence
- Activity prescription
- Action plans for decompensation
- Electronic tools and apps for self-management
Heart failure disease management programs:
- Multidisciplinary team approach
- Regular scheduled follow-up
- Telephone monitoring
- Home visits for selected patients
- Education reinforcement
- Caregiver inclusion
Monitoring strategies:
- Remote monitoring systems
- Telemonitoring
- Implantable hemodynamic monitors in selected cases
- Laboratory monitoring (electrolytes, renal function, natriuretic peptides)
- Regular functional assessment
Comorbidity management:
- Systematic screening for common comorbidities
- Coordinated care plans
- Medication optimization for multiple conditions
- Prevention of iatrogenic complications
- Prioritization of interventions
Environmental and situational precautions
Environmental considerations:
- Extreme temperature avoidance
- Air conditioning during heat waves
- Appropriate heating in cold weather
- Adjusted activity during extreme weather
- Air quality awareness
- Air pollution monitoring
- Indoor air quality
- Masks when air quality poor
- Altitude considerations
- Gradual acclimatization to high altitude
- Oxygen supplementation when needed
- Avoidance of extremely high altitudes
Travel precautions:
- Consultation before extended travel
- Medication planning and adequate supply
- Medical records availability
- Knowledge of medical facilities at destination
- Compression stockings for long flights
- Adequate hydration while avoiding excessive fluid
- Activity during long journeys
- Travel insurance with cardiac condition coverage
Infection prevention:
- Regular vaccinations:
- Annual influenza
- Pneumococcal (PCV13 and PPSV23)
- COVID-19
- Shingles
- Hand hygiene
- Avoidance of sick contacts
- Prompt treatment of infections
- Dental hygiene and regular check-ups
Special situations:
- Surgery:
- Preoperative optimization
- Perioperative medication management
- Appropriate monitoring
- Volume management
- Early mobilization
- Pregnancy:
- Preconception counseling
- Medication adjustments
- Multidisciplinary management
- Close monitoring
- Planned delivery
- Acute illness:
- Medication adjustments during intercurrent illness
- Volume status monitoring
- Temporary intensification of follow-up
End-of-life planning:
- Advance directives
- Device deactivation planning
- Palliative care integration
- Healthcare proxy designation
- Goals of care discussions
- Hospice referral when appropriate
Comprehensive prevention strategies span the entire spectrum from primordial prevention in the general population to specialized interventions for those with advanced disease, emphasizing the importance of both system-level and individual approaches to reducing the burden of heart failure.
10. Global & Regional Statistics
Global epidemiology
Prevalence and incidence:
- Global prevalence: Estimated 64 million people worldwide
- Lifetime risk: Approximately 20% for those reaching age 40
- Annual incidence:
- Developed nations: 5-10 new cases per 1,000 person-years in those >65 years
- Developing nations: Limited data but increasing burden
- Prevalence by age:
- <50 years: <1%
- 50-59 years: 2-3%
- 60-69 years: 4-6%
- 70-79 years: 10-12%
80 years: 15-20%
Global burden of disease metrics:
- Responsible for 1-2% of disability-adjusted life years (DALYs) globally
- Leading cause of hospitalization in older adults worldwide
- Contributes to approximately 1 million hospitalizations annually in the US alone
- Economic burden estimated at $108 billion annually worldwide
- Accounts for 1-3% of healthcare expenditure in developed nations
Heart failure phenotypes globally:
- HFrEF more common in low- and middle-income countries
- HFpEF increasingly prevalent in high-income countries
- Ischemic etiology predominant globally but with regional variations
- Hypertensive heart failure more common in Africa and parts of Asia
- Valvular heart disease significant in many developing regions
- Chagas cardiomyopathy important in Latin America
Regional variations
North America:
- United States:
- Prevalence: 6.2 million adults (2.2% of population)
- Annual incidence: 550,000-900,000 new cases
- Lifetime risk at age 40: 20% for men, 20% for women
- Leading cause of hospitalization in those >65 years
- Annual cost: $30-40 billion
- Racial disparities: Higher incidence and earlier onset in African Americans
- Canada:
- Prevalence: 600,000 (1.6% of population)
- Similar patterns to US with universal healthcare impact
Europe:
- Overall:
- Prevalence: 15 million (2-3% of population)
- Annual direct cost: €35 billion
- East-West gradient in outcomes corresponding to healthcare resources
- Western Europe:
- Well-established heart failure programs
- Higher proportion of HFpEF
- Earlier diagnosis
- Better outcomes
- Eastern Europe:
- Higher cardiovascular mortality
- More limited access to advanced therapies
- Higher proportion of valvular etiologies in some regions
Asia:
- Developed regions (Japan, South Korea, Singapore):
- Prevalence: 1-2% of adult population
- Rapidly aging populations driving increasing burden
- High proportion of HFpEF (40-50%)
- Excellent access to advanced therapies
- China:
- Estimated 10 million patients
- Rapidly increasing prevalence with urbanization
- Significant regional disparities in care
- Hypertension as major contributor
- South Asia:
- Limited epidemiological data
- Younger age of onset
- Higher proportion of rheumatic heart disease
- Significant barriers to care
- Limited access to advanced therapies
Africa:
- Limited population-based data
- Estimated prevalence: 1-2% of adult population
- Distinct etiological profile:
- Hypertensive heart disease (30-40%)
- Cardiomyopathies (20-30%)
- Rheumatic heart disease (15-20%)
- Ischemic heart disease (10-15%)
- Younger age of presentation (mean age 52 years)
- Limited access to diagnostics and treatments
- Very high in-hospital mortality (15-20%)
Latin America:
- Prevalence: 1-2% of population, with limited data
- Mixed etiological profile:
- Ischemic (30-40%)
- Hypertensive (20-30%)
- Chagas disease (regionally important, up to 20%)
- Rheumatic (5-10%)
- Significant urban-rural disparities in care
- Variable access to advanced therapies
Australia/New Zealand:
- Prevalence similar to Western Europe and North America
- Indigenous populations with higher rates and earlier onset
- Excellent data collection through national registries
- Well-developed heart failure programs
Mortality and survival statistics
Global mortality:
- Contributes to approximately 9-10% of all deaths globally
- Annual heart failure-related deaths: Estimated 3-5 million worldwide
- Mortality higher in low- and middle-income countries
Survival rates by region:
- High-income countries:
- 1-year mortality: 15-20%
- 5-year mortality: 45-60%
- Improving over time with medical advances
- Middle-income countries:
- 1-year mortality: 20-30%
- 5-year mortality: 60-70%
- Significant urban-rural disparities
- Low-income countries:
- 1-year mortality: 25-40%
- 5-year mortality: 70-80%
- Limited data available
Hospital mortality variations:
- United States: 2-7% in-hospital mortality
- Europe: 3-9% in-hospital mortality with North-South gradient
- Africa: 15-25% in-hospital mortality
- Asia: Variable (3-20%) depending on healthcare system development
Causes of death by region:
- Developed regions:
- Progressive heart failure: 40-50%
- Sudden cardiac death: 30-40%
- Non-cardiovascular causes: 10-20%
- Developing regions:
- Progressive heart failure: 50-60%
- Sudden cardiac death: 20-30%
- Infectious complications: 10-20%
Trends and projections
Historical trends:
- Increasing prevalence in most regions due to:
- Aging populations
- Improved survival from acute cardiac events
- Better detection
- Growing prevalence of risk factors
- Declining age-adjusted mortality in developed nations
- Shifting from HFrEF toward HFpEF in developed nations
Current trends:
- Stabilizing incidence in some developed regions
- Increasing incidence in developing regions
- Decreasing in-hospital mortality
- Persistent high readmission rates (20-25% at 30 days)
- Growing burden of HFpEF (now 50% of cases in developed nations)
Future projections:
- Global projections:
- 46% increase in heart failure prevalence by 2030
- Particularly steep increases in Asia and Africa
- Economic burden expected to double in next 20 years
- United States:
- Projected 25% increase in prevalence by 2030
- Growing racial and geographic disparities
- Europe:
- Aging population driving 25-30% increase by 2030
- East-West convergence in outcomes with EU integration
- Asia:
- Most dramatic increases projected (50-75% by 2030)
- Rapid transition to chronic disease burden
- Growing economic impact
- Africa:
- Double burden of communicable and non-communicable disease
- Limited healthcare infrastructure for chronic disease
- Projected 75-100% increase by 2030
Healthcare system impact:
- Growing percentage of hospital beds occupied by heart failure patients
- Increasing demand for specialized heart failure services
- Economic pressure for cost-effective management strategies
- Push toward home-based care models
- Integration of digital health solutions
These statistics highlight the global nature of the heart failure epidemic, with important regional variations in epidemiology, etiology, management, and outcomes. They emphasize the need for region-specific strategies while learning from successful approaches across different healthcare systems.
11. Recent Research & Future Prospects
Recent breakthroughs
Pharmacological advances:
- SGLT2 inhibitors:
- Landmark trials (DAPA-HF, EMPEROR-Reduced) showing benefit in HFrEF
- EMPEROR-Preserved demonstrating first convincing mortality benefit in HFpEF
- Mechanism of action in heart failure still under investigation
- Now considered fourth pillar of guideline-directed medical therapy
- ARNI (Sacubitril/Valsartan):
- PARADIGM-HF established superiority over ACE inhibitors
- PARAGON-HF showed suggestive benefit in HFpEF (particularly in women)
- Mechanistic studies clarifying dual action
- Position in treatment algorithms continuing to evolve
- Novel therapies:
- Vericiguat (soluble guanylate cyclase stimulator) showing modest benefit
- Omecamtiv mecarbil (cardiac myosin activator) reducing heart failure events
- Finerenone (non-steroidal MRA) with improved selectivity
Device and procedural innovations:
- Remote hemodynamic monitoring:
- CardioMEMS device demonstrating reduced hospitalizations
- Integration into clinical workflows improving outcomes
- Development of predictive algorithms for early intervention
- Transcatheter interventions:
- MitraClip for functional mitral regurgitation (COAPT trial)
- Transcatheter tricuspid valve interventions
- Interatrial shunt devices for HFpEF in trials
- Mechanical circulatory support:
- Fully magnetically levitated LVADs reducing complications
- Temporary percutaneous support devices for cardiogenic shock
- Development of partial support systems for less advanced disease
Diagnostic and monitoring advances:
- Biomarkers:
- Multi-marker panels for improved risk stratification
- Point-of-care testing for rapid assessment
- Novel biomarkers of fibrosis and inflammation
- Imaging:
- Machine learning applications in echocardiography
- Myocardial strain imaging for subclinical dysfunction
- T1 mapping in CMR for fibrosis quantification
- Wearable and implantable sensors:
- Continuous monitoring of multiple physiologic parameters
- Integration with electronic health records
- Early warning systems for decompensation
Basic and translational research:
- Genetic and molecular insights:
- Expanded understanding of genetic contributions
- Identification of novel therapeutic targets
- Precision medicine approaches
- Mechanisms of HFpEF:
- Recognition of multiple phenotypes
- Role of comorbidities and systemic inflammation
- Microvascular dysfunction pathways
- Cellular regeneration:
- Refinement of stem cell approaches
- Understanding of paracrine effects
- Tissue engineering advances
Current research focus areas
Precision medicine initiatives:
- Genetic profile-based therapy selection
- Biomarker-guided treatment strategies
- Phenotype-specific intervention approaches
- Integration of multi-omics data for personalized care
- Predictive models for treatment response
Novel therapeutic targets:
- Inflammation and immune modulation:
- Targeted anti-inflammatory approaches
- Immunomodulatory therapies
- Resolution of inflammation pathways
- Metabolic modulation:
- Cardiac energetics optimization
- Mitochondrial function enhancement
- Substrate utilization modification
- Fibrosis and remodeling:
- Anti-fibrotic agents
- Matrix metalloproteinase modulators
- Galectin-3 pathway inhibition
- Autonomic nervous system:
- Vagal nerve stimulation
- Sympathetic modulation
- Renal denervation refinement
Heart failure with preserved ejection fraction:
- Phenotype-specific interventions
- Exercise training and rehabilitation
- Novel pharmacological approaches
- Device-based approaches (interatrial shunts, pacing)
- Comorbidity management strategies
Advanced heart failure and end-of-life:
- Optimization of LVAD therapy and minimizing complications
- Total artificial heart development
- Xenotransplantation advances
- Palliative care integration
- Shared decision-making tools
Implementation and health services research:
- Optimal disease management program components
- Digital health interventions
- Telehealth optimization
- Reducing readmissions
- Healthcare disparities
- Cost-effectiveness of new interventions
Future directions and emerging technologies
Gene and RNA-based therapies:
- Gene therapy approaches:
- AAV-based vector delivery systems
- CRISPR-Cas9 gene editing for inherited cardiomyopathies
- Targeted delivery to cardiac tissue
- RNA therapeutics:
- microRNA modulators
- Antisense oligonucleotides
- mRNA therapeutics
Regenerative medicine:
- Next-generation cell therapies:
- Induced pluripotent stem cells (iPSCs)
- Cardiac progenitor cells
- Engineered cell products
- Combinatorial approaches with biomaterials
- Tissue engineering:
- 3D bioprinting of cardiac tissues
- Decellularized scaffolds
- Injectable hydrogels for structural support
Advanced implantable technologies:
- Miniaturized circulatory support:
- Fully implantable LVADs with transcutaneous power
- Minimally invasive implantation techniques
- Physiologic flow patterns
- Multi-modality devices:
- Combined pacing, defibrillation, and hemodynamic monitoring
- Responsive systems adapting to physiologic needs
- Energy harvesting technologies
- Smart materials and interfaces:
- Self-healing components
- Biologically integrated interfaces
- Infection-resistant materials
Digital health revolution:
- Artificial intelligence applications:
- Predictive analytics for early intervention
- Automated image analysis
- Clinical decision support systems
- Virtual care assistants
- Remote monitoring ecosystems:
- Integration of multiple data streams
- Patient-generated health data incorporation
- Seamless communication platforms
- Virtual and augmented reality:
- Patient education tools
- Rehabilitation applications
- Therapeutic adherence support
Barriers and challenges:
- Regulatory pathways for novel therapies
- Reimbursement for innovative approaches
- Technology adoption in diverse healthcare settings
- Ethics of advanced technologies
- Cost-effectiveness demonstration
- Healthcare workforce training
- Equitable access to innovations
The future of heart failure management lies at the intersection of basic science discoveries, technological innovation, and implementation science. Progress will require collaboration across disciplines, continued investment in research, and creative approaches to delivering these advances to the diverse population affected by this condition worldwide.
12. Interesting Facts & Lesser-Known Insights
Historical perspectives
Ancient understandings:
- Ancient Egyptians recognized “water in the chest” as a medical condition
- Traditional Chinese Medicine described a syndrome similar to heart failure as “water overflowing the heart”
- Hippocrates described “dropsy” (edema) and noted its poor prognosis
- The Romans recommended foxglove (source of digitalis) for “dropsical” conditions
Notable historical figures with heart failure:
- Ludwig van Beethoven likely suffered from cardiomyopathy and heart failure
- President Franklin D. Roosevelt had hypertensive heart disease and heart failure
- Queen Victoria experienced heart failure in her later years
- Pope John Paul II lived with heart failure for years before his death
Treatment evolution curiosities:
- Early treatments included bloodletting, leeches, and purgatives
- William Withering’s 1785 publication on foxglove (digitalis) revolutionized treatment
- Mechanical approaches included the “Southey’s tubes” inserted into edematous legs to drain fluid
- Until the 1950s, strict bed rest was a mainstay of treatment (now known to be harmful)
- Salt restriction has been recommended since the early 1900s
- Mercurial diuretics were the first effective diuretics but had significant toxicity
Terminology evolution:
- Term “heart failure” replaced older terms like “dropsy” and “cardiac decompensation”
- “Congestive” heart failure terminology being gradually replaced by simply “heart failure”
- Classification systems have evolved from hemodynamic (forward/backward failure) to functional (NYHA) to structural (ACC/AHA stages)
Unusual facts and phenomena
Cardiac adaptations:
- The heart’s energy consumption equals that of a car engine in a compact space
- A failing heart may consume up to 30% of the body’s oxygen at rest
- The heart pumps about 5 liters of blood per minute at rest (7,200 liters daily)
- Cardiac tissue can hibernate (reduce function to preserve viability) when blood flow is compromised
Reverse remodeling:
- Heart failure can sometimes be reversed with appropriate therapy
- LVAD support can lead to “bridge to recovery” in select patients
- Peripartum cardiomyopathy has higher recovery rates than other forms
- Tachycardia-induced cardiomyopathy often shows dramatic improvement with rate control
Circadian rhythms and heart failure:
- Heart failure symptoms often worsen at night due to fluid redistribution
- Neurohormonal cycles influence heart failure physiology
- Timing of medication administration can affect efficacy
- Morning hours associated with highest risk of heart failure decompensation
Environmental effects:
- High altitude exposure worsens heart failure due to hypoxia and pulmonary vasoconstriction
- Heart failure hospitalizations increase during extreme temperature events
- Air pollution exposure associated with acute exacerbations
- Seasonal variations affect hospitalization rates (higher in winter months)
The obesity paradox:
- Overweight and mildly obese heart failure patients show better survival than normal-weight patients
- Possible explanations include:
- Metabolic reserve during catabolic stress
- Earlier presentation due to symptoms
- Different underlying pathophysiology
- Cardioprotective effects of some adipokines
- The paradox disappears in severe obesity or cachexia
Myths vs. facts
Myth: Heart failure means the heart has stopped working. Fact: Heart failure indicates the heart isn’t pumping efficiently, not that it has stopped.
Myth: Heart failure only affects the elderly. Fact: While prevalence increases with age, heart failure can affect people of all ages, including children and young adults.
Myth: Heart failure always causes obvious swelling. Fact: Early heart failure may have subtle symptoms or manifestations primarily of fatigue and exertional dyspnea without obvious edema.
Myth: Heart failure is always due to coronary artery disease. Fact: Many conditions can cause heart failure, including hypertension, valve disease, genetic factors, infections, and toxins.
Myth: Heart failure patients should avoid all exercise. Fact: Appropriate exercise is beneficial and recommended for stable heart failure patients.
Myth: Salt restriction means using no salt. Fact: Moderate sodium restriction (2-3g daily) is recommended, not complete elimination.
Myth: Heart failure with preserved ejection fraction is milder than reduced ejection fraction. Fact: Both types carry significant symptom burden and mortality risk.
Myth: Beta-blockers worsen heart failure. Fact: While beta-blockers may transiently worsen symptoms when initiated, they improve outcomes long-term.
Myth: Once diagnosed with heart failure, quality of life is always poor. Fact: With optimal treatment, many patients maintain good quality of life and functional capacity.
Myth: A diagnosis of heart failure means you’ll need a heart transplant. Fact: Most heart failure patients never require transplantation or mechanical support.
Impact on specific populations
Athletes:
- Endurance athletes may develop “athlete’s heart” with cardiac enlargement
- Difficult to distinguish physiologic from pathologic remodeling
- High-performance athletes may mask early symptoms
- Performance-enhancing substances can cause cardiomyopathy
- Return to competition guidelines exist for athletes with heart failure
Pregnant women:
- Hemodynamic changes of pregnancy can unmask or worsen heart failure
- Peripartum cardiomyopathy affects 1 in 1,000-4,000 pregnancies
- Medication adjustments needed during pregnancy
- Multidisciplinary approach required
- Counseling about future pregnancies essential
- Risk of recurrence with subsequent pregnancies
Children:
- Different etiological profile than adults:
- Congenital heart disease
- Cardiomyopathies
- Myocarditis
- Arrhythmias
- Unique challenges in diagnosis and management
- Developmental impacts of the disease and treatments
- Long-term considerations into adulthood
- Family-centered approach to care
Occupational impacts:
- Commercial drivers: Regulatory restrictions based on symptoms and ejection fraction
- Pilots: Strict aviation medical certification requirements
- Military personnel: May be disqualified from certain duties
- First responders: Functional capacity limitations affect duty status
- Manual laborers: May require job modification or retraining
Professional musicians:
- Wind and brass players face unique challenges
- Beta-blockers may affect performance (timing, tremor)
- High-catecholamine performance situations can trigger symptoms
- Device implantation may affect certain instruments (violin)
Economic disparities:
- Lower socioeconomic status associated with:
- Higher incidence
- More severe presentation
- Limited access to advanced therapies
- Higher readmission rates
- Lower medication adherence due to cost
- Barriers to lifestyle modifications
- Poorer outcomes across metrics
These interesting perspectives highlight the complex, multifaceted nature of heart failure beyond the medical textbook descriptions, emphasizing its far-reaching impact on individuals and society throughout history and across diverse populations.