
⚠️ Disclaimer: The information provided in this article is for educational purposes only and does not constitute medical advice. RevisionTown does not provide diagnosis, treatment, or medical recommendations. Always consult a qualified healthcare professional regarding any medical condition, symptoms, or concerns.
Read More – 🏥 Medical Disclaimer
Comprehensive Report on Sarcoidosis
1. Overview
What is sarcoidosis?
Sarcoidosis is a multisystem inflammatory disorder characterized by the formation of tiny clusters of inflammatory cells called granulomas. These granulomas can develop in virtually any organ of the body, though they most frequently affect the lungs and lymph nodes. When these granulomas accumulate in tissues, they can disrupt normal organ function and lead to various symptoms. Sarcoidosis is considered a rare disease, with fewer than 200,000 cases in the United States at any given time.
The term “sarcoidosis” comes from the Greek words “sark” meaning flesh and “oid” meaning like – essentially describing flesh-like tumors. It’s also known as Besnier-Boeck-Schaumann disease, named after the physicians who made significant early contributions to its understanding.
Affected body parts/organs
While sarcoidosis can potentially affect any organ system in the body, certain sites are more commonly involved than others:
Lungs: The respiratory system is involved in approximately 90% of sarcoidosis cases, making pulmonary manifestations the most common. Granulomas can form in the lung tissue and lymph nodes within the chest.
Lymph nodes: Lymph nodes, particularly those in the chest (hilar and mediastinal), are affected in up to 90% of cases. Lymph nodes in other areas such as the neck, armpits, and groin may also become enlarged.
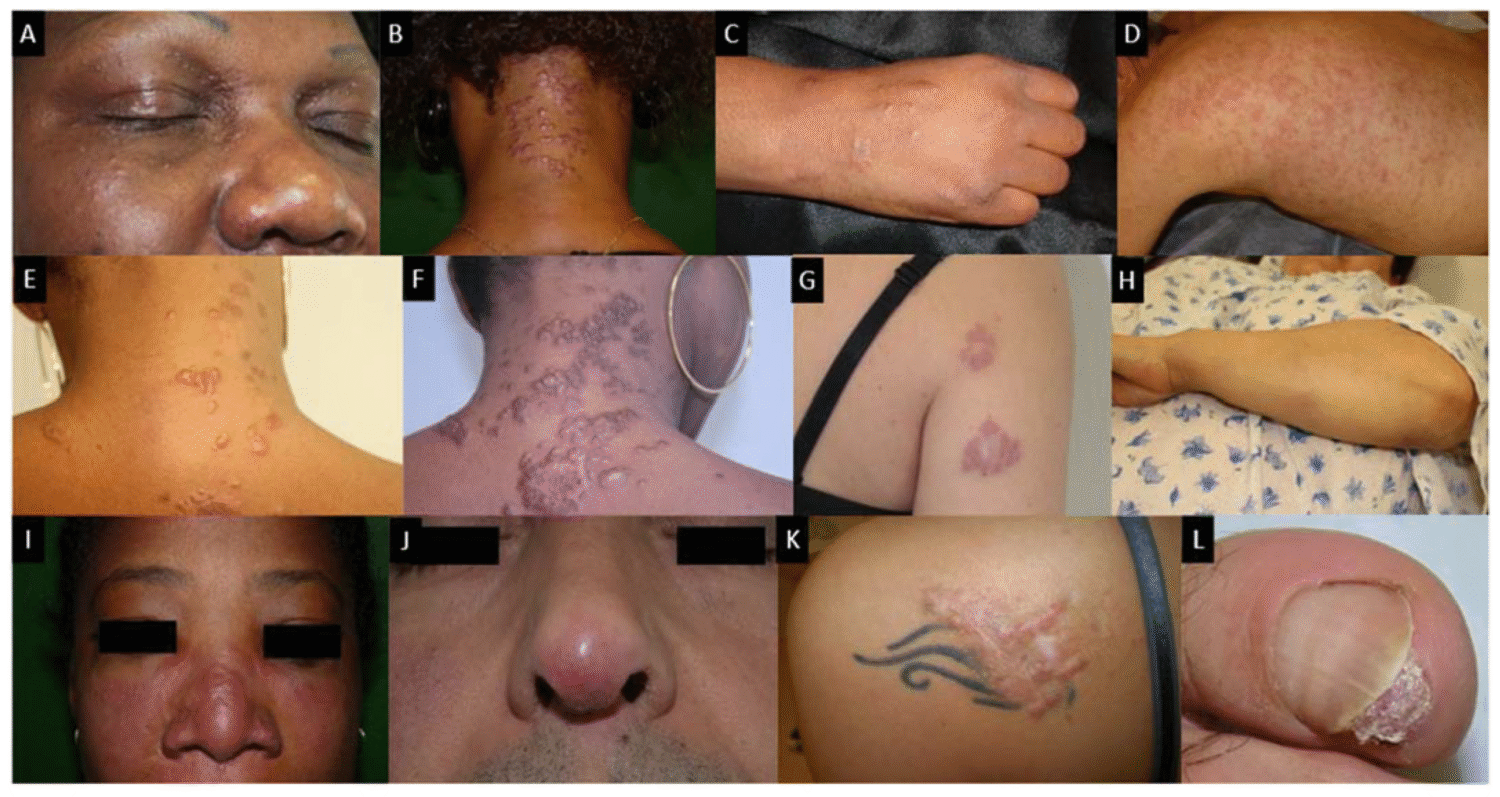
Skin: Cutaneous involvement occurs in 25-35% of patients, presenting as various types of lesions including erythema nodosum (painful, red nodules usually on the shins), plaques, maculopapular eruptions, and lupus pernio (chronic, violaceous lesions typically on the nose, cheeks, and ears).
Eyes: Ocular sarcoidosis affects approximately 25-50% of patients and can involve any part of the eye. Uveitis (inflammation of the uvea) is the most common ocular manifestation.
Heart: Cardiac sarcoidosis, though only clinically apparent in about 5% of patients, is a serious manifestation that can lead to arrhythmias, heart block, heart failure, and sudden death. Autopsy studies suggest it may be present in up to 25% of cases but remain undetected during life.
Nervous system: Neurosarcoidosis occurs in approximately 5-10% of patients and can affect any part of the nervous system, including the brain, spinal cord, and peripheral nerves.
Liver and spleen: These organs are commonly affected but usually without causing symptoms. Granulomas in the liver are found in up to 80% of patients in autopsy studies.
Bones and joints: Arthritic symptoms and bone lesions can occur in approximately 5-15% of cases.
Kidneys: Renal involvement may lead to kidney stones or impaired kidney function in some patients.
Salivary and parotid glands: Enlargement of these glands occurs in a small percentage of patients.
The distribution and severity of organ involvement vary widely among individuals, contributing to the highly variable clinical presentation and course of the disease.
Prevalence and significance of the disease
Sarcoidosis is a relatively uncommon disease, but its prevalence varies significantly by geographic region and ethnic group. Global statistics indicate:
- The annual incidence ranges from approximately 1-35 cases per 100,000 people, depending on the population studied.
- In the United States, the estimated annual incidence is around 10-35 cases per 100,000 population.
- The prevalence is highest in Nordic countries, particularly Sweden, with an estimated incidence of 11.5-15 per 100,000 per year.
- In African Americans, particularly women, the incidence is notably high at approximately 35-80 per 100,000.
- East Asian countries report much lower rates, with South Korea reporting an incidence of only 0.5-1.3 per 100,000.
The significance of sarcoidosis extends beyond its prevalence numbers for several reasons:
Diagnostic challenges: The disease can mimic many other conditions, leading to misdiagnosis or delayed diagnosis.
Variable disease course: While many cases resolve spontaneously within 2-5 years, approximately 30% of patients develop chronic disease that may progressively worsen and cause permanent organ damage.
Quality of life impact: Even non-life-threatening manifestations can significantly impact quality of life through chronic fatigue, pain, and psychological distress.
Mortality risk: Though uncommon, sarcoidosis can be fatal, particularly when it affects the heart, central nervous system, or leads to severe pulmonary fibrosis. The overall mortality rate is estimated at approximately 7% over a 5-year follow-up period.
Economic burden: The disease often affects young adults in their productive years, leading to work disability and healthcare costs.
Healthcare disparities: The disproportionate impact on certain ethnic groups, particularly African Americans, highlights potential healthcare disparities in diagnosis, treatment, and outcomes.
Sarcoidosis represents a significant healthcare challenge due to its complexity, variability, and the lack of a clear understanding of its causes, which limits targeted treatment approaches.
2. History & Discoveries
When and how was sarcoidosis first identified?
Sarcoidosis was first recognized as a distinct clinical entity in the late 19th century, though the full understanding of the disease as we know it today evolved gradually over several decades. The earliest documented case that is now recognized as sarcoidosis dates back to 1869, when the English dermatologist Jonathan Hutchinson described a patient with purplish skin lesions affecting the hands and feet. At that time, Hutchinson attributed these lesions to a manifestation of gout.
In 1889, Ernest Besnier, a French dermatologist, described a condition he called “lupus pernio,” which is now recognized as a manifestation of cutaneous sarcoidosis. This condition presented as violaceous lesions on the nose, cheeks, and ears.
The pathological hallmark of sarcoidosis – the granuloma – was first identified by the Norwegian dermatologist Caesar Boeck in 1899. Boeck obtained skin biopsies from patients with what he termed “multiple benign sarkoid of the skin” and described the characteristic histological pattern. He used the term “sarkoid” because the lesions resembled sarcomas (cancerous tumors) but were benign in nature.
During these early years, sarcoidosis was primarily considered a dermatological condition. The recognition of sarcoidosis as a multisystem disorder evolved gradually as more cases were documented with involvement of internal organs.
Who discovered it?
Rather than having a single discoverer, sarcoidosis was characterized through the contributions of multiple physicians over several decades. The key historical figures include:
Jonathan Hutchinson (1828-1913): The English surgeon and pathologist who first described what is now recognized as sarcoidosis in 1869. He later documented a second case in 1898, in a patient named Mrs. Mortimer.
Ernest Besnier (1831-1909): The French dermatologist who described “lupus pernio” in 1889, a distinctive form of cutaneous sarcoidosis.
Caesar Boeck (1845-1917): The Norwegian dermatologist who in 1899 first identified the histological hallmark of sarcoidosis – the granuloma – and coined the term “sarkoid” to describe the condition.
Jörgen Schaumann (1879-1953): A Swedish dermatologist who made significant contributions to understanding sarcoidosis as a systemic disease. In 1914, he wrote a prize-winning essay that synthesized the various manifestations of sarcoidosis into a unified concept of a single disease.
David Kreibich: In 1904, he described the characteristic bone lesions associated with sarcoidosis.
Christian Heerfordt (1871-1953): A Danish ophthalmologist who in 1909 described uveoparotid fever (fever, parotid enlargement, anterior uveitis, and facial nerve palsy), now known as Heerfordt’s syndrome, a manifestation of sarcoidosis.
Major discoveries and breakthroughs in its research and treatment
Several key discoveries and breakthroughs have advanced our understanding and management of sarcoidosis:
Kveim Test (1941): Ansgar Kveim developed a diagnostic test for sarcoidosis by injecting an extract of sarcoid tissue into the skin and observing the formation of granulomas. This test was later refined by Louis Siltzbach and became known as the Kveim-Siltzbach test. Though now rarely used due to standardization issues and the advent of better diagnostic techniques, it represented a major advance in diagnosis.
Löfgren’s Syndrome (1946): Sven Löfgren described a characteristic constellation of symptoms (erythema nodosum, bilateral hilar lymphadenopathy, fever, and polyarthritis) that often occurs at the onset of sarcoidosis in Caucasians. Recognition of this syndrome has helped in early diagnosis.
Immunologic Basis (1954): Harold Israel and Max Sones helped establish sarcoidosis as an immunologic disorder, paving the way for understanding its pathophysiology.
International Kveim Test Trial (1966): Siltzbach conducted an international trial validating the Kveim test, which represented a major collaborative research effort in sarcoidosis.
Corticosteroid Treatment (1951): The first use of corticosteroids to treat sarcoidosis marked a significant therapeutic advance. Anecdotal successes with this approach led to corticosteroids becoming the mainstay of sarcoidosis treatment.
Recognition of Cardiac Sarcoidosis: The identification and characterization of cardiac involvement in sarcoidosis represented a crucial advance, as it is one of the most serious manifestations of the disease.
TNF-Alpha Inhibitors (Early 2000s): The introduction of biologic therapies, particularly tumor necrosis factor (TNF) inhibitors like infliximab, provided new treatment options for refractory cases.
Genetic Studies: Multiple studies have identified genetic factors associated with sarcoidosis susceptibility and disease course, though no definitive causative gene has been identified.
Advanced Imaging Techniques: The development of high-resolution CT scanning, PET scanning, and cardiac MRI has greatly improved the diagnosis and monitoring of various forms of sarcoidosis.
Evolution of medical understanding over time
The medical understanding of sarcoidosis has evolved significantly over time:
From Skin Disease to Systemic Disorder: Initially regarded as a purely dermatological condition, sarcoidosis was gradually recognized as a multisystem disorder that can affect virtually any organ system.
Histopathological Understanding: The identification of non-caseating granulomas as the histopathological hallmark of sarcoidosis distinguished it from other granulomatous diseases like tuberculosis.
Etiological Theories: The understanding of potential causes has shifted from various infectious theories to a more complex model involving genetic susceptibility, environmental exposures, and immunological responses.
Classification Systems: Various staging systems have been developed for pulmonary sarcoidosis, such as the Scadding stages, which categorize disease based on chest radiographic findings.
Treatment Approaches: Treatment has evolved from purely symptomatic management to more targeted immunosuppressive and immunomodulatory approaches.
Recognition of Disease Phenotypes: Research has increasingly recognized distinct clinical phenotypes of sarcoidosis, which may have different prognoses and treatment responses.
Refinement of Diagnostic Criteria: The diagnostic approach has been refined from relying heavily on clinical features and the Kveim test to using a combination of compatible clinical and radiological findings, histological confirmation of granulomas, and exclusion of other causes.
From Acute to Chronic Disease Management: There has been increased recognition of sarcoidosis as a potentially chronic disease requiring long-term management rather than just treatment of acute phases.
Patient-Centered Outcomes: Modern research has placed greater emphasis on patient-reported outcomes and quality of life issues, including fatigue, which affects up to 85% of patients.
Despite significant advances in our understanding of sarcoidosis over the past century, many aspects of the disease remain enigmatic, including its exact cause, the factors determining disease progression, and the optimal treatment approach for various manifestations. This ongoing uncertainty continues to drive research efforts worldwide.
3. Symptoms
Early symptoms vs. advanced-stage symptoms
Sarcoidosis presents with a wide spectrum of symptoms that can vary significantly based on the organs involved and the stage of the disease. The distinction between early and advanced symptoms is not always clear-cut, as the disease follows different patterns in different individuals.
Early Symptoms:
Constitutional Symptoms:
- Fatigue (occurs in up to 85% of cases)
- Low-grade fever
- Unexplained weight loss
- Night sweats
- General malaise
Respiratory Symptoms:
- Persistent dry cough
- Shortness of breath, especially with exertion
- Chest discomfort or pain
Skin Manifestations:
- Erythema nodosum (painful, red nodules usually on the shins)
- Rashes or lesions
- Small bumps (papules) on the face or extremities
Lymph Node Involvement:
- Painless swelling of lymph nodes, particularly in the chest, neck, and armpits
Löfgren’s Syndrome:
- A specific presentation consisting of erythema nodosum, bilateral hilar lymphadenopathy, and often joint pain
- Generally associated with a good prognosis and often resolves spontaneously
Advanced-Stage Symptoms:
Progressive Pulmonary Symptoms:
- Worsening shortness of breath
- Decreased exercise tolerance
- Persistent cough, sometimes productive
- Signs of pulmonary fibrosis (scarring) including decreased lung volumes and impaired gas exchange
Cardiac Manifestations:
- Arrhythmias (irregular heartbeats)
- Heart block (disruption of electrical signals in the heart)
- Cardiomyopathy leading to heart failure
- Pericarditis (inflammation of the sac surrounding the heart)
Neurological Complications:
- Cranial nerve palsies (particularly facial nerve)
- Seizures
- Cognitive dysfunction
- Peripheral neuropathy (numbness, tingling, weakness)
- Meningitis
Advanced Ocular Disease:
- Progressive vision loss
- Glaucoma
- Cataracts
- Blindness if left untreated
Renal Complications:
- Kidney stones due to hypercalciuria
- Granulomatous nephritis
- Renal dysfunction
Hepatic and Splenic Involvement:
- Hepatomegaly (enlarged liver)
- Splenomegaly (enlarged spleen)
- Portal hypertension
- Impaired liver function
Bone and Joint Manifestations:
- Chronic arthritis
- Bone cysts
- Bone pain
- Joint deformities
Endocrine Abnormalities:
- Hypercalcemia (elevated calcium levels in the blood)
- Dysfunction of pituitary, thyroid, or adrenal glands
- Diabetes insipidus
Common vs. rare symptoms
Common Symptoms (occurring in more than 10% of patients):
Pulmonary Symptoms:
- Shortness of breath
- Persistent dry cough
- Chest discomfort
Constitutional Symptoms:
- Fatigue (extremely common, affecting up to 85% of patients)
- Malaise
- Low-grade fever
Lymphadenopathy:
- Swollen lymph nodes, particularly hilar and mediastinal lymph nodes in the chest
Skin Manifestations:
- Various types of skin lesions, including papules, nodules, and plaques
- Erythema nodosum, particularly in acute presentations
Ocular Symptoms:
- Eye redness
- Pain
- Photophobia (light sensitivity)
- Blurred vision
Musculoskeletal Symptoms:
- Joint pain and stiffness
- Muscle aches
Rare Symptoms (occurring in less than 10% of patients):
Neurological Manifestations:
- Seizures
- Hydrocephalus
- Psychiatric symptoms
- Aseptic meningitis
- Spinal cord involvement
Gastrointestinal Involvement:
- Pancreatitis
- Gastric sarcoidosis
- Symptoms mimicking Crohn’s disease
Genitourinary Symptoms:
- Testicular or epididymal masses
- Reproductive organ involvement
Bone Marrow Involvement:
- Anemia
- Leukopenia
- Thrombocytopenia
Salivary and Lacrimal Gland Symptoms:
- Sicca syndrome (dry eyes and mouth)
- Parotid gland enlargement (can be part of Heerfordt’s syndrome)
Cardiac Symptoms:
- While cardiac involvement may occur in up to 25% of patients (based on autopsy studies), symptomatic cardiac sarcoidosis is relatively rare
- Sudden cardiac arrest may be the first manifestation in some cases
Ear, Nose, and Throat Manifestations:
- Sinusitis
- Nasal obstruction
- Hearing loss
- Vertigo
Metabolic Abnormalities:
- Hypercalcemia (elevated calcium levels in the blood)
- Abnormalities in vitamin D metabolism
How symptoms progress over time
The progression of sarcoidosis symptoms over time follows several distinct patterns, which contribute to the unpredictable nature of the disease:
Acute Presentation with Spontaneous Resolution:
- Approximately 50-70% of patients, particularly those with Löfgren’s syndrome, experience an acute onset of symptoms
- These symptoms often resolve spontaneously within 6 months to 2 years without significant treatment
- This pattern is more common in Caucasians, especially those of Scandinavian descent
Persistent Stable Disease:
- Some patients develop chronic symptoms that neither improve nor worsen significantly over time
- These individuals may require maintenance therapy to control symptoms
- Organ function remains relatively preserved despite ongoing inflammation
Progressive Disease:
- Approximately 10-30% of patients experience a progressive course
- Initial symptoms gradually worsen over time
- New organ systems may become involved years after initial diagnosis
- This pattern may lead to significant organ dysfunction and fibrosis, particularly in the lungs
Relapsing-Remitting Pattern:
- Some patients experience periods of symptom exacerbation alternating with periods of remission
- Relapses may be triggered by medication tapering or environmental factors
- This pattern may require intermittent intensification of therapy
Organ-Specific Progression:
- In some cases, sarcoidosis may improve in one organ system while simultaneously worsening in another
- For example, lung manifestations may improve while cardiac or neurological involvement progresses
The timeline of progression varies widely:
- In acute presentations that resolve spontaneously, the entire course of the disease may be limited to 6-24 months.
- Chronic persistent sarcoidosis may last for many years or even decades with relatively stable symptoms.
- Progressive disease typically develops over a period of 2-5 years, with gradual worsening of symptoms and organ function.
- Mortality typically occurs in patients with severe fibrotic lung disease, cardiac involvement, or neurosarcoidosis, usually after several years of disease progression.
Factors that may influence disease progression include:
- Ethnicity (African Americans tend to have more severe, chronic disease)
- Age at onset (older individuals often have a more chronic course)
- Specific organ involvement (cardiac and neurological involvement tend to indicate a worse prognosis)
- Initial disease severity
- Response to initial treatment
- Genetic factors
Regular monitoring by healthcare providers is essential for tracking disease progression and adjusting treatment plans accordingly. Pulmonary function tests, imaging studies, and organ-specific assessments are typically used to monitor disease activity and progression over time.
4. Causes
Biological and environmental causes
The exact cause of sarcoidosis remains unknown, but current evidence suggests that it results from a complex interaction between genetic predisposition and environmental triggers. The biological and environmental factors implicated in the development of sarcoidosis include:
Biological Factors:
Immunological Dysregulation:
- Sarcoidosis involves an exaggerated immune response characterized by increased activity of T-helper cells (particularly Th1 cells)
- There is enhanced production of inflammatory cytokines such as interferon-gamma, interleukin-2, and tumor necrosis factor-alpha (TNF-α)
- This leads to the formation of granulomas, which are organized clusters of activated macrophages and lymphocytes
Infectious Agents:
- Various microorganisms have been proposed as potential triggers for sarcoidosis in genetically susceptible individuals
- These include mycobacteria (with some studies detecting mycobacterial DNA in approximately 26% of sarcoidosis tissues)
- Other implicated organisms include Propionibacterium acnes, fungi, and certain viruses
- The hypothesis is that these agents may trigger an immune response that persists even after the infectious agent is cleared
Altered Vitamin D Metabolism:
- Activated macrophages in sarcoidosis can convert vitamin D to its active form (1,25-dihydroxyvitamin D) outside the kidneys
- This can lead to hypercalcemia and hypercalciuria in some patients
- This dysregulation may play a role in the immune abnormalities seen in sarcoidosis
Environmental Factors:
Occupational and Environmental Exposures:
- Certain occupations have been associated with higher rates of sarcoidosis, suggesting environmental triggers
- These include firefighters, healthcare workers, and those exposed to:
- Insecticides and pesticides
- Metal dusts (particularly beryllium, which causes a similar condition called berylliosis)
- Silica dust
- Moldy or dusty environments
- Wood-burning stoves
Geographic Variations:
- The significant geographic variations in sarcoidosis prevalence (high in Scandinavian countries and among African Americans in the United States, low in South America and most parts of Asia) suggest environmental factors
- These variations may reflect differences in both genetic susceptibility and environmental exposures
Seasonal Patterns:
- Some studies have noted seasonal variations in the onset of sarcoidosis
- For example, Löfgren’s syndrome shows a peak incidence in spring in some populations
- This seasonality hints at potential environmental triggers that vary throughout the year, such as specific pollens or infectious agents
Climate and Sunlight Exposure:
- The north-south gradient in sarcoidosis prevalence in Europe (higher in northern countries) has led to theories about sunlight exposure and vitamin D status as potential modifying factors
Genetic and hereditary factors
Genetic factors play a significant role in determining both susceptibility to sarcoidosis and the pattern of disease expression. Evidence for genetic involvement includes:
Familial Clustering:
- The disease occurs more frequently in first-degree relatives of sarcoidosis patients
- Approximately 5-16% of patients report having affected family members
- This familial association is particularly strong in African Americans, where 20% of patients report an affected family member compared to 5% in European Americans
Racial and Ethnic Differences:
- The marked differences in prevalence between racial and ethnic groups suggest genetic factors
- African Americans have a 3-4 times higher incidence than Caucasians in the United States
- Certain populations, such as those of Japanese descent, have distinctive patterns of organ involvement (e.g., higher rates of cardiac sarcoidosis)
Twin Studies:
- Studies in twins have shown higher concordance rates in monozygotic (identical) twins compared to dizygotic (fraternal) twins
Specific Genetic Associations:
- Human Leukocyte Antigen (HLA) genes: Various HLA alleles have been associated with sarcoidosis risk and phenotype
- HLA-DRB1*03 is associated with Löfgren’s syndrome and good prognosis
- HLA-DRB1*15 is associated with chronic disease
- Non-HLA genes: Several other genes involved in immune function have been implicated, including:
- BTNL2 (butyrophilin-like 2): A regulator of T-cell activation
- TNF-α: Involved in granuloma formation
- Various cytokine and chemokine genes
- Human Leukocyte Antigen (HLA) genes: Various HLA alleles have been associated with sarcoidosis risk and phenotype
Heritability Estimates:
- Heritability (the proportion of disease risk attributed to genetic factors) has been estimated at around 39% in Swedish populations
- If a first-degree family member is affected, the risk increases approximately 4-fold
The genetic basis of sarcoidosis is complex and likely involves multiple genes interacting with environmental factors. No single gene has been identified as the “sarcoidosis gene,” and the genetic architecture appears to involve numerous variants, each contributing a small effect to overall risk.
Known triggers or exposure risks
Several potential triggers and exposure risks have been identified that may initiate or exacerbate sarcoidosis in genetically predisposed individuals:
Infectious Agents:
- Mycobacteria: Including atypical mycobacteria and possibly cell wall deficient forms of Mycobacterium tuberculosis
- Propionibacterium acnes: Found in increased numbers in sarcoidosis tissues
- Fungi: Such as Cryptococcus and Histoplasma
- Viruses: Including Epstein-Barr virus and herpesvirus
Inorganic Particulates:
- Metal dusts and fumes, particularly aluminum, zirconium, and titanium
- Silica (silicon dioxide)
- Talc and talc-containing drugs (in cases of drug-induced granulomatosis)
Organic Dusts:
- Mold and mildew from water-damaged buildings
- Pine tree pollen
- Clay soil
- Bioaerosols from various sources
Occupational Exposures:
- Firefighting: Exposure to smoke and combustion products
- Healthcare work: Particularly nursing, which has been associated with higher risk in several studies
- Agriculture: Exposure to various organic and inorganic dusts
- Military service: Particularly exposure to burn pits and airborne particulates in deployment settings
Medication-Induced Sarcoidosis-Like Reactions:
- Tumor necrosis factor (TNF) inhibitors (paradoxically, these are also used to treat sarcoidosis)
- Interferon therapy
- Immune checkpoint inhibitors used in cancer treatment
Physical Factors:
- Foreign bodies
- Tattoo ink (particularly black ink)
- Surgical implants or suture material
Other Associated Conditions:
- Lymphoma: There is a bidirectional association between lymphoma and sarcoidosis
- Other autoimmune diseases: Sarcoidosis occurs more frequently in people with other autoimmune conditions
It’s important to note that while these triggers and exposures have been associated with sarcoidosis, a direct causal relationship has not been definitively established for many of them. The evidence for specific triggers varies in strength, and it’s likely that different triggers may be relevant in different individuals.
The complex interplay between genetic susceptibility and environmental exposures means that a particular trigger may cause sarcoidosis in one genetically predisposed individual but not in another. This complexity has made it challenging to identify a single causative agent, leading to the current understanding of sarcoidosis as a heterogeneous disorder with multiple potential causes rather than a single disease entity.
5. Risk Factors
Who is most at risk (age, gender, occupation, lifestyle, etc.)?
Several demographic, occupational, and lifestyle factors appear to influence the risk of developing sarcoidosis. Understanding these risk factors helps identify higher-risk populations for targeted screening and early intervention.
Age:
- Sarcoidosis most commonly develops between ages 25 and 40 years
- A second peak of incidence occurs in women over 50 years (particularly in Scandinavian populations)
- Pediatric sarcoidosis is rare, although it can occur in children of all ages
- Very elderly onset (>70 years) is uncommon
Gender:
- Slight female predominance overall with a female-to-male ratio of approximately 1.3:1
- The gender distribution varies by ethnicity and age:
- In Scandinavian populations, the female predominance is more pronounced
- The second peak of incidence in older adults primarily affects women
- Males tend to develop sarcoidosis at a younger age than females (median age at diagnosis approximately 45 for men versus 54 for women in some studies)
- Female patients may have higher rates of certain extrapulmonary manifestations
Race and Ethnicity:
- African Americans have the highest risk, with an incidence 3-4 times higher than Caucasians in the United States
- The estimated lifetime risk of sarcoidosis is:
- 2.1% in African American males
- 2.7% in African American females
- 0.7% in Caucasian males
- 1.0% in Caucasian females
- Northern European populations, particularly Scandinavians, have higher rates than other Caucasian groups
- Japanese populations have a distinctive pattern with higher rates of cardiac involvement
- The disease is relatively rare in South American, Central American, and most Asian populations
Occupation:
- Healthcare workers: Several studies have shown an increased risk, particularly among nurses
- Firefighters and first responders: Possibly related to exposure to various inhaled particles
- Agricultural workers: Exposure to various organic dusts may increase risk
- Military personnel: Particularly those deployed to environments with high particulate exposure
- Industries with exposure to:
- Metal dusts and fumes
- Silica
- Organic dusts
- Insecticides and pesticides
Lifestyle Factors:
- Living in environments with:
- Mold and moisture damage
- Wood-burning stoves
- Poor indoor air quality
- Tobacco smoking: Interestingly, smoking appears to be associated with a lower risk of sarcoidosis, although smoking can worsen symptoms in those who already have the disease
Geographic Location:
- Higher prevalence in:
- Northern European countries (especially Sweden, Denmark, and Finland)
- Northern United States
- Lower prevalence in:
- Southern Europe
- Central and South America
- Most parts of Asia (with the exception of Japan)
Environmental, occupational, and genetic factors
Environmental Factors:
- Exposure to various environmental antigens has been implicated:
- Microorganisms: Mycobacteria, Propionibacterium acnes, fungi
- Inorganic materials: Silica, metals, talc
- Organic dusts: Mold, pollen, bioaerosols
- Seasonal variation: Some studies report higher incidence in spring and early summer
- Climate: The north-south gradient in disease prevalence suggests potential influences of:
- UV radiation exposure
- Vitamin D levels
- Temperature-related changes in behavior or exposure patterns
- Built environment:
- Water-damaged buildings
- Indoor air quality
- Use of wood-burning stoves
Occupational Factors:
- Specific occupational exposures associated with increased risk:
- Healthcare work: Possibly related to increased exposure to infectious agents or chemicals
- Firefighting: Smoke and particulate exposure
- Agriculture: Various organic and inorganic dusts
- Manufacturing with exposure to:
- Metal dusts and fumes
- Silica
- Industrial chemicals
- Work-related activities involving:
- Handling moldy materials
- Insecticide application
- Exposure to bioaerosols
Genetic Factors:
Heritability estimates range from approximately 39% in Swedish populations to higher rates in African American populations
Familial clustering is well-documented:
- 5-16% of patients report affected family members
- First-degree relatives have a 4-fold increased risk
Specific genetic associations:
- HLA genes: Various HLA types influence both susceptibility and disease phenotype
- HLA-DRB1*03 is associated with acute disease and good prognosis
- HLA-DRB1*15 is associated with chronic disease
- Non-HLA genes:
- BTNL2 (butyrophilin-like 2): A negative regulator of T-cell activation
- TNF-α polymorphisms: Influence inflammation and granuloma formation
- Various cytokine and chemokine genes
- Immunoregulatory genes
- HLA genes: Various HLA types influence both susceptibility and disease phenotype
Genetic-environmental interactions:
- Current evidence suggests that sarcoidosis arises from environmental triggers acting on a genetically susceptible host
- Different genetic variants may predispose to different disease phenotypes and organ manifestations
- The same environmental exposure may trigger disease in genetically susceptible individuals but not in others
Impact of pre-existing conditions
Several pre-existing conditions may influence the risk of developing sarcoidosis or affect its clinical course once established:
Autoimmune Disorders:
- There is an observed association between sarcoidosis and other autoimmune conditions:
- Sjögren’s syndrome
- Systemic lupus erythematosus
- Rheumatoid arthritis
- Multiple sclerosis
- The co-occurrence of these conditions suggests shared immunological mechanisms or genetic predisposition
Lymphoma and Other Malignancies:
- There is a bidirectional association between sarcoidosis and lymphoma:
- Patients with sarcoidosis have an increased risk of developing lymphoma
- Sarcoidosis-like reactions can occur in patients with lymphoma and other malignancies
- This association may reflect shared immunologic dysregulation or potential misdiagnosis
Chronic Infections:
- History of certain infections may predispose to sarcoidosis development:
- Tuberculosis: Some studies suggest prior tuberculosis infection may be associated with increased sarcoidosis risk
- Chronic fungal infections
- Certain viral infections
Immune Deficiency States:
- Paradoxically, some immune deficiency states have been associated with sarcoidosis or sarcoidosis-like granulomatous reactions
- Sarcoidosis has been reported in patients with:
- HIV infection (particularly during immune reconstitution)
- Common variable immunodeficiency
- Following organ transplantation
Pre-existing Lung Disease:
- Prior pulmonary conditions may affect the presentation and course of pulmonary sarcoidosis:
- Chronic obstructive pulmonary disease (COPD)
- Asthma
- Interstitial lung diseases
- These conditions may complicate the diagnosis and management of sarcoidosis
Metabolic Disorders:
- Obesity: Some studies suggest an association between obesity and sarcoidosis risk
- Diabetes: May affect disease course and treatment options (particularly given the side effects of corticosteroids)
- Hyperlipidemia: May influence cardiovascular risk in sarcoidosis patients
Cardiovascular Disease:
- Pre-existing cardiac conditions may complicate the diagnosis and management of cardiac sarcoidosis
- Cardiovascular risk factors may influence the overall prognosis
Psychological Conditions:
- Depression and anxiety are common in sarcoidosis patients
- Pre-existing psychological conditions may:
- Affect symptom perception and reporting
- Influence quality of life and functional status
- Complicate treatment adherence
Understanding these risk factors and pre-existing conditions helps clinicians identify at-risk populations, facilitate earlier diagnosis, and tailor management approaches to individual patient circumstances. However, it’s important to note that many individuals develop sarcoidosis without any identifiable risk factors, highlighting the complex and multifactorial nature of this disease.
6. Complications
What complications can arise from sarcoidosis?
Sarcoidosis can lead to a wide range of complications, varying in severity from mild and self-limiting to severe and life-threatening. These complications typically result from persistent inflammation, granuloma formation, and eventual fibrosis (scarring) in affected organs. The most significant complications include:
Pulmonary Complications:
- Pulmonary fibrosis: Permanent scarring of lung tissue, which can lead to restrictive lung disease and impaired gas exchange
- Bronchiectasis: Abnormal widening of the airways, which can lead to recurrent infections
- Pulmonary hypertension: Increased pressure in the pulmonary arteries, which can strain the right side of the heart
- Aspergilloma: Fungal infection (aspergillus) that can colonize pre-existing cavities in the lungs
- Pneumothorax: Collapsed lung, which can occur due to rupture of subpleural cysts
- Respiratory failure: In advanced cases of pulmonary fibrosis
Cardiac Complications:
- Arrhythmias: Abnormal heart rhythms, which can range from benign to life-threatening
- Conduction blocks: Disruption of electrical signals in the heart, including atrioventricular blocks
- Cardiomyopathy: Weakening of the heart muscle, which can lead to heart failure
- Sudden cardiac death: Can occur due to severe arrhythmias or conduction abnormalities
- Valvular dysfunction: Caused by granulomatous inflammation affecting heart valves
- Pericarditis: Inflammation of the sac surrounding the heart
Neurological Complications:
- Cranial neuropathies: Particularly facial nerve palsy
- Seizures: Due to involvement of brain tissue
- Hydrocephalus: Buildup of fluid in the brain
- Aseptic meningitis: Inflammation of the meninges (coverings of the brain and spinal cord)
- Myelopathy: Spinal cord involvement leading to weakness, sensory changes, or bladder/bowel dysfunction
- Peripheral neuropathy: Damage to peripheral nerves causing numbness, tingling, or weakness
- Cognitive dysfunction: Memory problems, confusion, or other cognitive impairments
Ocular Complications:
- Uveitis: Inflammation of the uvea (middle layer of the eye), which can lead to vision loss if untreated
- Glaucoma: Increased pressure in the eye, which can damage the optic nerve
- Cataracts: Clouding of the lens, which can be accelerated by corticosteroid treatment
- Retinal detachment: Separation of the retina from the back of the eye
- Blindness: Can result from severe or untreated ocular sarcoidosis
Renal Complications:
- Nephrocalcinosis: Calcium deposits in the kidneys due to abnormal calcium metabolism
- Kidney stones: Related to hypercalciuria (excessive calcium in urine)
- Granulomatous nephritis: Inflammation and granuloma formation in the kidneys
- Renal failure: In severe cases of renal sarcoidosis
Hepatic and Splenic Complications:
- Portal hypertension: Increased pressure in the portal vein, which can lead to varices and bleeding
- Cirrhosis: Scarring of the liver in advanced cases of hepatic sarcoidosis
- Cholestasis: Impaired bile flow, which can cause jaundice and itching
- Splenomegaly: Enlarged spleen, which can cause discomfort and may increase risk of splenic rupture
Metabolic Complications:
- Hypercalcemia: Elevated calcium levels in the blood, which can cause various symptoms including confusion, weakness, and kidney problems
- Hypercalciuria: Excessive calcium in urine, which can lead to kidney stones and kidney damage
- Vitamin D dysregulation: Abnormal metabolism of vitamin D due to granuloma activity
Long-term impact on organs and overall health
The long-term impact of sarcoidosis on organs and overall health varies greatly depending on the extent of organ involvement, treatment response, and individual factors. Here’s an overview of potential long-term impacts:
Pulmonary System:
- Permanent reduction in lung function: Even after inflammation resolves, fibrotic changes may persist
- Reduced exercise capacity and physical functioning
- Increased susceptibility to respiratory infections
- Long-term oxygen dependency in severe cases
- Chronic cough and dyspnea affecting quality of life
- Development of bronchiectasis with recurrent infections
Cardiovascular System:
- Permanent conduction abnormalities requiring pacemaker implantation
- Chronic heart failure requiring ongoing management
- Increased risk of sudden cardiac death (even years after initial diagnosis)
- Vascular complications secondary to granulomatous vasculitis
- Exercise intolerance due to compromised cardiac function
Nervous System:
- Permanent neurological deficits from granulomatous inflammation
- Chronic seizure disorders requiring long-term anticonvulsant therapy
- Persistent headaches
- Cognitive impairment and memory problems
- Depression and anxiety related to chronic neurological symptoms
- Sleep disorders
Visual System:
- Permanent vision loss in cases of severe or untreated ocular involvement
- Chronic uveitis requiring ongoing treatment
- Increased risk of glaucoma and cataracts (both from the disease itself and from corticosteroid treatment)
- Need for regular ophthalmological monitoring
Renal System:
- Chronic kidney disease due to granulomatous nephritis or calcium-related kidney damage
- Recurrent kidney stones
- Hypertension secondary to renal involvement
Hepatic System:
- Chronic liver disease in cases of severe hepatic sarcoidosis
- Portal hypertension with potential complications like varices
- Need for liver transplantation in rare, severe cases
Musculoskeletal System:
- Chronic joint pain and arthritis
- Bone cysts and other osseous lesions
- Muscle weakness and atrophy
- Limitations in physical functioning and activities of daily living
Overall Health Impact:
- Chronic fatigue: Affects up to 85% of patients and can persist even when other symptoms are controlled
- Reduced quality of life: Both from physical symptoms and psychological impact
- Sleep disturbances: Common and contribute to fatigue and reduced quality of life
- Psychological effects: Depression, anxiety, and adjustment difficulties are common
- Treatment-related complications: Long-term steroid use can lead to osteoporosis, diabetes, weight gain, and other side effects
- Occupational limitations: May affect employment status and career progression
- Financial burden: From direct healthcare costs and potential loss of income
- Increased mortality risk: Particularly in cases with cardiac involvement, advanced pulmonary fibrosis, or neurological complications
Potential disability or fatality rates
Sarcoidosis can lead to varying degrees of disability and, in some cases, premature death. While many patients experience mild disease with complete resolution, others face severe, progressive disease with significant morbidity and mortality.
Disability Rates and Patterns:
Overall Disability: Approximately 10-30% of sarcoidosis patients experience some form of disability related to their disease.
Functional Limitations:
- Reduced exercise capacity and physical functioning
- Limitations in activities of daily living
- Reduced ability to work or maintain employment
Work Disability:
- Studies from various countries report work disability rates of 6-25% among sarcoidosis patients
- Factors associated with work disability include:
- Pulmonary function impairment
- Fatigue
- Pain
- Neurological involvement
- Multiple organ involvement
Predictors of Disability:
- African American race (higher rates of chronic, severe disease)
- Older age at diagnosis
- Extrapulmonary organ involvement, particularly cardiac and neurological
- Pulmonary fibrosis on imaging
- Lower socioeconomic status and educational level
- Delayed diagnosis and treatment
Quality of Life Impact:
- Significant reductions in health-related quality of life are reported
- Both physical and mental health components are affected
- Fatigue is often the most disabling symptom, reported by up to 85% of patients
- Social functioning is frequently impaired
Fatality Rates:
Overall Mortality:
- The mortality rate for sarcoidosis over a 5-year follow-up period is approximately 7%
- African Americans have a higher mortality rate compared to Caucasians
- The age-adjusted mortality rate in the United States has increased over recent decades
Causes of Death in Sarcoidosis:
- Respiratory failure due to advanced pulmonary fibrosis (accounts for >60% of sarcoidosis-related deaths)
- Cardiac complications, including sudden cardiac death and heart failure
- Neurological complications
- Infections (sometimes related to immunosuppressive therapy)
- Pulmonary hypertension
- Treatment-related complications
Prognostic Factors for Mortality:
- Advanced age at diagnosis
- African American race
- Cardiac involvement
- Neurological involvement
- Severe pulmonary fibrosis (radiographic stage IV)
- Pulmonary hypertension
- Treatment resistance
- Presence of co-morbidities
Specific Mortality Risks:
- Cardiac sarcoidosis: Associated with a 5-year mortality rate of approximately 25-40% if left untreated
- Advanced pulmonary fibrosis: 5-year mortality rates of 30-50% in those with severe fibrotic disease
- Pulmonary hypertension: Significantly increases mortality risk
- Neurosarcoidosis affecting the brain stem or spinal cord: Associated with higher mortality
Long-term Survival:
- Overall 10-year survival rates range from 70-95%, depending on the population studied
- Survival rates are lower for patients with:
- African American ethnicity
- Advanced age at diagnosis
- Multiple organ involvement
- Cardiac or advanced pulmonary disease
It’s important to note that while these statistics provide general information, individual outcomes vary widely. Early diagnosis, appropriate treatment, close monitoring, and comprehensive management of complications can significantly improve outcomes and reduce both disability and mortality in sarcoidosis patients.
7. Diagnosis & Testing
Common diagnostic procedures
Diagnosing sarcoidosis can be challenging due to its variable presentation and the lack of a single definitive test. The diagnosis typically relies on a combination of compatible clinical and radiological findings, histological confirmation of non-caseating granulomas, and the exclusion of other causes of granulomatous inflammation. The common diagnostic procedures include:
Clinical Evaluation:
- Comprehensive medical history: Assessing symptoms, onset, progression, and risk factors
- Complete physical examination: Checking for characteristic manifestations across multiple organ systems
- Review of occupational and environmental exposures
- Family history assessment
Laboratory Tests:
- Complete blood count (CBC): May show anemia, leukopenia, or thrombocytopenia
- Comprehensive metabolic panel: To assess kidney and liver function
- Serum calcium and phosphorus: May be elevated in some patients
- Erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP): Non-specific markers of inflammation
- Angiotensin-converting enzyme (ACE) levels: Often elevated in active sarcoidosis, but has limited sensitivity and specificity
- Soluble interleukin-2 receptor (sIL-2R): A more sensitive marker of disease activity
- Vitamin D levels: To assess for dysregulation of vitamin D metabolism
- Urinalysis: To detect calcium in urine (hypercalciuria)
- Tuberculin skin test or interferon-gamma release assay: To help exclude tuberculosis
Pulmonary Function Tests (PFTs):
- Spirometry: Often shows a restrictive pattern with reduced forced vital capacity (FVC)
- Lung volumes: Total lung capacity (TLC) is typically reduced
- Diffusion capacity for carbon monoxide (DLCO): Often reduced, reflecting impaired gas exchange
- Exercise testing: May reveal exercise limitation and oxygen desaturation
Imaging Studies:
- Chest X-ray: Often the initial imaging study, which can reveal characteristic findings like bilateral hilar lymphadenopathy
- High-resolution computed tomography (HRCT): Provides detailed images of lung parenchyma and mediastinal structures
- Magnetic resonance imaging (MRI): Particularly useful for assessing cardiac and neurological involvement
- 18F-fluorodeoxyglucose positron emission tomography (FDG-PET): Can identify areas of active inflammation and guide biopsy
- Gallium-67 scintigraphy: May show characteristic uptake patterns, though less commonly used now
- Cardiac imaging:
- Echocardiography
- Cardiac MRI with gadolinium enhancement
- Cardiac PET scanning
Biopsy Procedures:
- Lymph node biopsy: Often accessible and less invasive
- Transbronchial lung biopsy: Performed during bronchoscopy
- Endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA): For sampling hilar and mediastinal lymph nodes
- Skin biopsy: For cutaneous lesions
- Surgical lung biopsy: May be necessary if less invasive methods are non-diagnostic
- Biopsy of other affected organs: Including liver, kidney, myocardium, or nervous system tissue when clinically indicated
Bronchoscopic Procedures:
- Bronchoscopy with bronchoalveolar lavage (BAL): Typically shows lymphocytosis with an elevated CD4/CD8 ratio
- Transbronchial biopsy: To obtain lung tissue for histological examination
- Endobronchial biopsy: When endobronchial lesions are present
Medical tests (e.g., blood tests, imaging, biopsies)
Blood Tests:
Angiotensin-Converting Enzyme (ACE):
- Produced by epithelioid cells within granulomas
- Elevated in about 60-70% of patients with active sarcoidosis
- Limitations: Lacks sensitivity and specificity; can be elevated in other conditions; genetic variations affect baseline levels
Soluble Interleukin-2 Receptor (sIL-2R):
- Released by activated T cells
- More sensitive than ACE for detecting active sarcoidosis
- Can be useful for monitoring disease activity
Calcium Metabolism:
- Serum calcium: Elevated in 10-20% of patients due to increased vitamin D conversion
- 1,25-dihydroxyvitamin D: Often elevated due to conversion outside the kidneys
- 25-hydroxyvitamin D: May be low, normal, or high
Inflammatory Markers:
- ESR and CRP: Often elevated but non-specific
- Neopterin: Produced by activated macrophages; can be elevated
Liver Function Tests:
- Alkaline phosphatase and gamma-glutamyl transferase (GGT): May be elevated with hepatic involvement
- Transaminases (ALT, AST): Usually normal or mildly elevated
Complete Blood Count:
- May show anemia, leukopenia, or thrombocytopenia in some cases
- Lymphopenia is relatively common
Immunoglobulins:
- Polyclonal hypergammaglobulinemia is common
- Specific immunoglobulin subtypes may be elevated
Imaging Tests:
Chest Radiography:
- Traditionally classified using the Scadding staging system:
- Stage 0: Normal chest radiograph
- Stage I: Bilateral hilar lymphadenopathy (BHL)
- Stage II: BHL plus pulmonary infiltrates
- Stage III: Pulmonary infiltrates without BHL
- Stage IV: Pulmonary fibrosis
- Sensitivity limitations: May miss subtle disease
- Traditionally classified using the Scadding staging system:
High-Resolution Computed Tomography (HRCT):
- Superior to chest X-ray for detecting parenchymal abnormalities
- Characteristic findings: Nodules along bronchovascular bundles, perilymphatic distribution, upper and middle lung predominance
- Can identify complications like fibrosis, architectural distortion, and traction bronchiectasis
Magnetic Resonance Imaging (MRI):
- Cardiac MRI: Gold standard for diagnosing cardiac sarcoidosis; can detect myocardial inflammation and fibrosis
- Neurological MRI: Essential for diagnosing neurosarcoidosis
- Musculoskeletal MRI: For evaluating bone and joint involvement
Nuclear Medicine Studies:
- FDG-PET: Detects areas of active inflammation; useful for assessing disease activity and guiding biopsy
- Gallium-67 scintigraphy: Can show characteristic “panda” (uptake in lacrimal and parotid glands) and “lambda” (hilar and right paratracheal uptake) signs
- Thallium-201 or technetium-99m sestamibi: For assessing cardiac involvement
Ultrasonography:
- Abdominal ultrasound: For evaluating hepatic and splenic involvement
- Echocardiography: Initial screening test for cardiac sarcoidosis
- Endobronchial ultrasound (EBUS): Guides transbronchial needle aspiration of lymph nodes
Biopsy Procedures:
Transbronchial Lung Biopsy (TBLB):
- Most common biopsy procedure for diagnosing pulmonary sarcoidosis
- Diagnostic yield: 40-90% depending on disease stage
- Complications include pneumothorax and bleeding
Endobronchial Biopsy:
- High yield when endobronchial lesions are present
- Can be performed during the same bronchoscopy procedure as TBLB
EBUS-guided Transbronchial Needle Aspiration:
- Minimally invasive method for sampling mediastinal and hilar lymph nodes
- High diagnostic yield (80-90%) for stage I and II disease
- Lower complication rate than TBLB
Mediastinoscopy:
- Surgical procedure for sampling mediastinal lymph nodes
- Higher diagnostic yield but more invasive than bronchoscopic techniques
- Usually reserved for cases where less invasive methods are non-diagnostic
Surgical Lung Biopsy:
- Video-assisted thoracoscopic surgery (VATS) or open lung biopsy
- Highest diagnostic yield but most invasive pulmonary sampling method
- Reserved for cases where less invasive methods fail
Peripheral Lymph Node Biopsy:
- Simple procedure when accessible lymph nodes are present
- High diagnostic yield with minimal complications
Skin Biopsy:
- Easily accessible when cutaneous lesions are present
- Simple procedure with high diagnostic yield for cutaneous sarcoidosis
Other Organ Biopsies:
- Liver biopsy: When liver involvement is suspected
- Myocardial biopsy: For suspected cardiac sarcoidosis (low sensitivity due to patchy distribution)
- Nerve and muscle biopsy: For neuromuscular involvement
- Kidney biopsy: For suspected renal sarcoidosis
- Brain or meningeal biopsy: Rarely performed for neurosarcoidosis
Other Specialized Tests:
Pulmonary Function Tests:
- Patterns: Restrictive, obstructive, or mixed
- DLCO: Often reduced due to impaired gas exchange
- Six-minute walk test: Assesses functional capacity and exercise-induced oxygen desaturation
Bronchoalveolar Lavage (BAL):
- Typically shows lymphocytosis (>15% lymphocytes)
- Elevated CD4/CD8 ratio (>3.5) is suggestive but not specific
- Helps exclude infections
Electrocardiogram (ECG) and Holter Monitoring:
- Screening for cardiac conduction abnormalities
- May detect arrhythmias or conduction blocks
Ophthalmological Examination:
- Slit-lamp examination
- Fundoscopy
- Optical coherence tomography
Neurological Testing:
- Cerebrospinal fluid analysis
- Nerve conduction studies
- Electroencephalography (EEG)
Early detection methods and their effectiveness
Early detection of sarcoidosis is challenging due to its variable presentation, the non-specific nature of many symptoms, and the lack of a single definitive screening test. However, several approaches can contribute to earlier diagnosis, particularly in high-risk populations:
Screening in High-Risk Populations:
First-Degree Relatives:
- Periodic clinical evaluation and possibly chest X-rays
- Effectiveness: Limited data, but may identify early asymptomatic disease
- Limitations: No standardized screening protocols established; cost-effectiveness uncertain
Occupational Screening:
- Regular health assessments for workers in high-risk occupations (e.g., healthcare workers, firefighters)
- Chest X-rays or HRCT in symptomatic individuals or those with concerning exposures
- Effectiveness: May identify early pulmonary involvement
- Limitations: Radiation exposure; low yield in asymptomatic individuals
Screening After Environmental Exposures:
- Evaluation of individuals exposed to potential triggers
- Effectiveness: Limited data; may identify clusters of cases
- Limitations: Unclear which exposures warrant screening
Symptom-Based Early Detection:
Recognition of Löfgren’s Syndrome:
- Characteristic constellation of erythema nodosum, bilateral hilar lymphadenopathy, and arthritis
- Effectiveness: High; allows for prompt diagnosis without invasive procedures
- Limitations: Present in only a minority of cases, primarily in European populations
Early Evaluation of Constitutional Symptoms:
- Fatigue, unexplained weight loss, low-grade fever
- Effectiveness: Low specificity; many potential causes
- Limitations: Often attributed to other conditions or dismissed as non-specific
Prompt Investigation of Persistent Respiratory Symptoms:
- Chronic cough, dyspnea, chest discomfort
- Effectiveness: Variable; can lead to earlier diagnosis through chest imaging
- Limitations: Low specificity; many respiratory conditions present similarly
Imaging-Based Early Detection:
Chest X-ray:
- Traditional first-line imaging study
- Effectiveness: Can detect bilateral hilar lymphadenopathy in asymptomatic individuals
- Limitations: Limited sensitivity for early parenchymal disease; radiation exposure
HRCT:
- Superior sensitivity for detecting subtle parenchymal changes
- Effectiveness: Can identify disease not visible on chest X-ray
- Limitations: Higher radiation dose; cost; incidental findings requiring further evaluation
FDG-PET:
- Detects areas of active inflammation
- Effectiveness: Can identify occult areas of inflammation
- Limitations: Expensive; limited availability; non-specific (many conditions cause increased FDG uptake)
Laboratory-Based Early Detection:
Serum ACE:
- Traditionally used biomarker
- Effectiveness: Limited; low sensitivity and specificity for early disease
- Limitations: Affected by genetic variations; elevated in many other conditions
Soluble IL-2 Receptor:
- More sensitive marker of T-cell activation
- Effectiveness: Better than ACE for early detection
- Limitations: Not widely available; elevated in many inflammatory conditions
Novel Biomarkers:
- Research is ongoing for more specific biomarkers
- Potential candidates include chitotriosidase, neopterin, and various cytokines
- Effectiveness: Promising in research settings but not yet validated for clinical use
Effectiveness of Early Detection:
The effectiveness of early detection strategies varies depending on the population and methods used:
Benefits of early detection include:
- Potential to initiate treatment before permanent organ damage occurs
- Avoidance of complications related to advanced disease
- Reduction in diagnostic uncertainty and patient anxiety
- Opportunity to identify triggering exposures and implement preventive measures
Limitations of early detection include:
- Absence of validated screening protocols
- Risk of overdiagnosis and unnecessary procedures
- Cost and resource implications
- Uncertain impact on long-term outcomes (given that many cases resolve spontaneously)
The most effective approach to early detection involves increased awareness among healthcare providers, prompt investigation of suggestive symptoms, and targeted evaluation of high-risk individuals. Continued research into more sensitive and specific biomarkers and predictive models will likely improve early detection strategies in the future.
8. Treatment Options
Standard treatment protocols
Treatment for sarcoidosis is highly individualized based on organ involvement, disease severity, and patient factors. Not all patients require treatment, as spontaneous remission occurs in approximately 30-70% of cases, particularly those with Löfgren’s syndrome or stage I pulmonary disease. Current standard treatment protocols include:
Observation Without Pharmacological Treatment:
- Appropriate for:
- Asymptomatic patients
- Mild symptoms that do not affect quality of life
- Stage I pulmonary disease without progression
- Mild, stable extrapulmonary involvement
- Protocol:
- Regular clinical monitoring
- Periodic pulmonary function tests and imaging
- Organ-specific assessments based on involvement
- Patient education regarding disease symptoms and when to seek medical attention
First-Line Therapy: Corticosteroids:
- Indications:
- Symptomatic pulmonary disease with significant functional impairment
- Progressive pulmonary disease
- Significant extrapulmonary involvement (cardiac, neurological, ocular, renal)
- Hypercalcemia
- Severe cutaneous disease
- Protocol for Pulmonary Sarcoidosis:
- Initial dose: Prednisone 20-40 mg daily for 4-6 weeks
- Gradual taper over 6-12 months based on clinical and functional response
- Typical maintenance dose: 5-10 mg daily if needed
- Total treatment duration: Usually 6-12 months, but may be longer in chronic disease
- Monitoring:
- Clinical assessment
- Pulmonary function tests
- Chest imaging
- Side effect monitoring (glucose, blood pressure, bone density, ocular pressure)
Second-Line Therapy: Steroid-Sparing Agents:
- Indications:
- Failure to respond adequately to corticosteroids
- Inability to taper corticosteroids without disease relapse
- Contraindications to corticosteroids
- Significant side effects from corticosteroids
- Common Agents:
- Methotrexate:
- Protocol: 5-15 mg once weekly, oral or subcutaneous
- Monitoring: Complete blood count, liver function, renal function
- Azathioprine:
- Protocol: 50-200 mg daily
- Monitoring: Complete blood count, liver function
- Leflunomide:
- Protocol: 10-20 mg daily
- Monitoring: Complete blood count, liver function, blood pressure
- Mycophenolate mofetil:
- Protocol: 1000-3000 mg daily in divided doses
- Monitoring: Complete blood count, liver function, renal function
- Hydroxychloroquine (particularly for cutaneous and hypercalcemic manifestations):
- Protocol: 200-400 mg daily
- Monitoring: Ophthalmological examinations, complete blood count
- Methotrexate:
Third-Line Therapy: Biologics and Cytotoxic Agents:
- Indications:
- Refractory disease despite conventional immunosuppressives
- Severe organ-threatening disease requiring rapid control
- Contraindications to or intolerance of first and second-line therapies
- TNF-α Inhibitors:
- Infliximab:
- Protocol: 3-5 mg/kg IV at weeks 0, 2, and 6, then every 4-8 weeks
- Particularly effective for refractory pulmonary, cutaneous, and neurological sarcoidosis
- Adalimumab:
- Protocol: 40 mg subcutaneously every 1-2 weeks
- Alternative when infliximab cannot be used or causes reactions
- Infliximab:
- Cytotoxic Agents:
- Cyclophosphamide:
- Protocol: Oral (50-150 mg daily) or IV pulse therapy (500-1000 mg/m² monthly)
- Reserved for severe, life-threatening disease, particularly neurosarcoidosis
- Chlorambucil:
- Protocol: 2-6 mg daily
- Rarely used due to toxicity concerns
- Cyclophosphamide:
Organ-Specific Treatment Protocols:
Cardiac Sarcoidosis:
- Corticosteroids (higher doses than for pulmonary disease): Prednisone 30-60 mg daily initially
- Early introduction of steroid-sparing agents
- TNF-α inhibitors for refractory cases
- Antiarrhythmic medications as needed
- Device therapy (pacemaker, implantable cardioverter-defibrillator) for conduction abnormalities or high risk of arrhythmias
- Heart transplantation in end-stage disease
Neurosarcoidosis:
- Higher-dose corticosteroids: Prednisone 40-80 mg daily initially, sometimes preceded by IV methylprednisolone pulses
- Early introduction of immunosuppressants (often methotrexate or mycophenolate)
- TNF-α inhibitors or cyclophosphamide for severe or refractory cases
- Anticonvulsants for seizures
- Ventriculoperitoneal shunt for hydrocephalus
Ocular Sarcoidosis:
- Topical corticosteroids for anterior uveitis
- Systemic therapy for posterior uveitis or refractory anterior disease
- Local steroid injections for specific lesions
- Methotrexate or mycophenolate as steroid-sparing agents
- TNF-α inhibitors for severe or refractory cases
Cutaneous Sarcoidosis:
- Topical or intralesional corticosteroids for limited disease
- Hydroxychloroquine or chloroquine as first-line systemic therapy
- Methotrexate for more extensive or refractory disease
- TNF-α inhibitors for severe, disfiguring, or refractory cases
- Thalidomide or JAK inhibitors as alternative options
Hypercalcemia and Hypercalciuria:
- Corticosteroids for symptomatic hypercalcemia
- Hydroxychloroquine as an alternative
- Dietary calcium restriction and adequate hydration
- Avoidance of vitamin D supplements
- Bisphosphonates for persistent hypercalcemia
These treatment protocols continue to evolve as new evidence emerges. Treatment decisions should be individualized based on disease severity, organ involvement, comorbidities, and patient preferences, with a focus on minimizing both disease damage and treatment-related side effects.
Medications, surgeries, and therapies
The management of sarcoidosis encompasses a range of medications, procedures, and supportive therapies tailored to the specific manifestations and severity of the disease.
Medications:
Corticosteroids:
- Mechanism: Potent anti-inflammatory and immunosuppressive effects; inhibit granuloma formation
- Formulations:
- Systemic: Prednisone, prednisolone, methylprednisolone
- Inhaled: Budesonide, fluticasone (for endobronchial disease)
- Topical: Various preparations for cutaneous and ocular disease
- Injectable: Triamcinolone for intralesional treatment
- Side effects: Weight gain, diabetes, hypertension, osteoporosis, cataracts, mood changes, adrenal suppression, increased infection risk
Antimalarials:
- Hydroxychloroquine and chloroquine
- Mechanism: Interfere with antigen presentation and cytokine production
- Particularly effective for cutaneous lesions and hypercalcemia
- Side effects: Retinopathy (requiring regular ophthalmological monitoring), gastrointestinal disturbances, rare cardiac toxicity
Conventional Immunosuppressants:
- Methotrexate:
- Most commonly used steroid-sparing agent
- Mechanism: Inhibits folate metabolism and adenosine signaling
- Side effects: Hepatotoxicity, pneumonitis, bone marrow suppression, teratogenicity
- Azathioprine:
- Prodrug converted to 6-mercaptopurine
- Mechanism: Inhibits purine synthesis and lymphocyte proliferation
- Side effects: Bone marrow suppression, hepatotoxicity, increased infection risk
- Leflunomide:
- Mechanism: Inhibits pyrimidine synthesis
- Side effects: Hepatotoxicity, peripheral neuropathy, hypertension
- Mycophenolate mofetil:
- Mechanism: Inhibits inosine monophosphate dehydrogenase, affecting lymphocyte proliferation
- Side effects: Gastrointestinal disturbances, bone marrow suppression, increased infection risk
- Methotrexate:
Biologic Agents:
- TNF-α inhibitors:
- Infliximab: Chimeric monoclonal antibody
- Adalimumab: Fully human monoclonal antibody
- Certolizumab: PEGylated Fab fragment
- Golimumab: Human monoclonal antibody
- Mechanism: Block TNF-α, a key cytokine in granuloma formation
- Side effects: Increased infection risk (particularly tuberculosis), infusion reactions, autoimmune phenomena
- Other biologics under investigation:
- Rituximab: Anti-CD20 monoclonal antibody targeting B cells
- Ustekinumab: IL-12/IL-23 inhibitor
- Abatacept: CTLA-4 fusion protein
- TNF-α inhibitors:
Cytotoxic Agents:
- Cyclophosphamide:
- Mechanism: Alkylating agent that cross-links DNA
- Side effects: Bone marrow suppression, hemorrhagic cystitis, infertility, secondary malignancies
- Chlorambucil:
- Mechanism: Alkylating agent
- Side effects: Bone marrow suppression, increased malignancy risk
- Cyclophosphamide:
Other Medications:
- Pentoxifylline: Phosphodiesterase inhibitor with anti-TNF properties
- Thalidomide and lenalidomide: Immunomodulatory agents effective for cutaneous disease
- JAK inhibitors (tofacitinib, baricitinib): Emerging options for refractory disease
- Repository corticotropin injection (ACTH gel): FDA-approved for sarcoidosis but with limited contemporary data
- Tetracycline antibiotics: May have anti-inflammatory effects beneficial in some cases
Surgical and Procedural Interventions:
Diagnostic Procedures:
- Bronchoscopy with transbronchial biopsy
- Surgical lung biopsy (VATS or open)
- Mediastinoscopy
- Lymph node biopsy
- Organ-specific biopsies (liver, kidney, heart, brain, etc.)
Therapeutic Procedures:
- Cardiac Interventions:
- Pacemaker implantation for heart block
- Implantable cardioverter-defibrillator (ICD) for arrhythmias or primary prevention
- Catheter ablation for refractory arrhythmias
- Heart transplantation for end-stage cardiac sarcoidosis
- Neurological Procedures:
- Ventriculoperitoneal shunt for hydrocephalus
- Surgical decompression for space-occupying lesions
- Ophthalmological Procedures:
- Cataract surgery
- Procedures for glaucoma management
- Vitrectomy for complications of uveitis
- Pulmonary Procedures:
- Lung transplantation for end-stage fibrotic disease
- Bronchial artery embolization for hemoptysis
- Pleurodesis for recurrent pneumothorax
- Cutaneous Procedures:
- Surgical excision of disfiguring lesions
- Laser therapy for cosmetically significant lesions
- Cardiac Interventions:
Supportive Therapies:
Pulmonary Rehabilitation:
- Structured exercise programs
- Breathing techniques
- Energy conservation strategies
- Education about disease management
- Improvement of functional capacity
Oxygen Therapy:
- Supplemental oxygen for hypoxemia
- May be required only with exertion or continuously depending on severity
Physical Therapy:
- Targeted exercise programs
- Management of musculoskeletal symptoms
- Maintenance of functional capacity
Occupational Therapy:
- Adaptive strategies for activities of daily living
- Energy conservation techniques
- Workplace accommodations
Psychological Support:
- Counseling for adjustment to chronic illness
- Management of anxiety and depression
- Cognitive-behavioral therapy for coping with chronic symptoms
Nutritional Support:
- Calcium-restricted diet for hypercalcemia/hypercalciuria
- Weight management if on corticosteroids
- General healthy eating guidance
Complementary Approaches:
- Mindfulness and meditation for symptom management
- Yoga and tai chi for gentle exercise and stress reduction
- Acupuncture for pain management
- Note: These should complement, not replace, medical treatment
The comprehensive management of sarcoidosis often requires a multidisciplinary approach involving pulmonologists, cardiologists, neurologists, ophthalmologists, dermatologists, rheumatologists, and other specialists based on organ involvement. Treatment plans should be regularly reassessed and adjusted based on disease activity, treatment response, and side effects.
Emerging treatments and clinical trials
The treatment landscape for sarcoidosis continues to evolve, with numerous emerging therapies and ongoing clinical trials aimed at improving efficacy, reducing side effects, and addressing refractory disease. Here’s an overview of the most promising developments:
Novel Biologic Therapies:
JAK Inhibitors:
- Mechanism: Inhibit Janus kinases, which are involved in cytokine signaling
- Examples: Tofacitinib, baricitinib, ruxolitinib
- Status: Case reports and small series showing promise, particularly for cutaneous disease; formal trials underway
- Potential advantages: Oral administration, targeted mechanism
IL-6 Inhibitors:
- Mechanism: Block interleukin-6, which is elevated in active sarcoidosis
- Examples: Tocilizumab, sarilumab
- Status: Case reports and early-phase trials
- Potential applications: Refractory pulmonary and multisystem disease
IL-17 Inhibitors:
- Mechanism: Target the Th17 inflammatory pathway
- Examples: Secukinumab, ixekizumab
- Status: Limited data in sarcoidosis; potential application in cutaneous disease
- Rationale: Th17 cells are present in sarcoidosis granulomas
B-Cell Targeted Therapies:
- Mechanism: Deplete B cells or inhibit B-cell activity
- Examples: Rituximab (anti-CD20), belimumab (anti-BAFF)
- Status: Small studies and case reports for rituximab; increasing interest in B-cell role
- Potential applications: Refractory neurosarcoidosis, multisystem disease
Efzofitimod (ATYR1923):
- Mechanism: Novel immunomodulator targeting neuropilin-2
- Status: Phase 1/2 trial showed promising results with good safety profile
- Potential advantages: Novel mechanism, potentially fewer side effects than current options
Small Molecule Approaches:
CFI-801 (CMK389):
- Mechanism: Anti-inflammatory agent targeting specific inflammatory pathways
- Status: Phase 2 trials for pulmonary sarcoidosis
- Focus: Reducing granulomatous inflammation with fewer side effects
PDE4 Inhibitors:
- Mechanism: Inhibit phosphodiesterase-4, reducing inflammatory cytokine production
- Examples: Apremilast, roflumilast
- Status: Limited data in sarcoidosis; approved for other inflammatory conditions
- Potential applications: Pulmonary and cutaneous disease
Antifibrotic Agents:
- Mechanism: Target fibrotic pathways to prevent scarring
- Examples: Pirfenidone, nintedanib
- Status: Being evaluated for fibrotic sarcoidosis based on success in idiopathic pulmonary fibrosis
- Potential applications: Stage IV fibrotic pulmonary sarcoidosis
Alternative Treatment Approaches:
Antimicrobial Therapy:
- Rationale: Potential microbial triggers of sarcoidosis
- Examples: The CLEAR regimen (Concomitant Levofloxacin, Ethambutol, Azithromycin, and Rifampin)
- Status: Phase 2 trial completed with some positive results
- Controversy: Mixed evidence for infectious etiology
Repository Corticotropin Injection (ACTH Gel):
- Mechanism: Stimulates endogenous cortisol production and has direct anti-inflammatory effects
- Status: FDA-approved but undergoing contemporary reevaluation
- Potential applications: Alternative to exogenous corticosteroids
Stem Cell Approaches:
- Mechanism: Mesenchymal stem cells with immunomodulatory properties
- Status: Early-stage investigations
- Potential applications: Regenerative approach for fibrotic disease
Novel Treatment Strategies:
“Hit Hard and Early” Approach:
- Concept: Aggressive early treatment to induce remission and prevent chronic disease
- Status: Clinical trials comparing this to conventional stepwise approach
- Rationale: May prevent irreversible fibrosis and organ damage
Steroid-Free Treatment Protocols:
- Concept: Using alternative agents as first-line therapy to avoid steroid side effects
- Examples: Methotrexate or hydroxychloroquine as initial treatment
- Status: Being evaluated in clinical trials
- Potential benefits: Reduced long-term complications of steroid therapy
Combination Therapy Approaches:
- Concept: Using agents with complementary mechanisms simultaneously
- Examples: Corticosteroids plus methotrexate plus TNF inhibitor
- Status: Being explored in refractory disease
- Rationale: May provide synergistic effects with lower doses of individual agents
Ongoing Notable Clinical Trials:
EFZO-FIT Study:
- Agent: Efzofitimod
- Phase: Phase 3
- Focus: Pulmonary sarcoidosis
- Primary outcome: Steroid-sparing effect while maintaining disease control
- Status: Actively recruiting
Ustekinumab and Golimumab Trial:
- Agents: IL-12/IL-23 inhibitor and TNF inhibitor
- Phase: Multinational clinical trial
- Focus: Pulmonary and skin sarcoidosis
- Status: Completed, results pending
Novel Biomarkers for Treatment Personalization:
- Concept: Identifying biomarkers to predict treatment response
- Status: Multiple ongoing studies
- Goal: Personalized medicine approach to sarcoidosis treatment
Antifibrotic Therapy in Fibrotic Pulmonary Sarcoidosis:
- Agents: Pirfenidone or nintedanib
- Focus: Stage IV fibrotic disease
- Status: Early clinical evaluation
- Goal: Address the current therapeutic gap for fibrotic disease
Patient-Centered Outcomes Research:
- Focus: Evaluating treatments based on patient-reported outcomes
- Status: Increasing emphasis in clinical trials
- Goal: Ensure treatments address symptoms most important to patients
Challenges in Clinical Trial Development:
Disease Heterogeneity:
- Variable organ involvement and disease phenotypes
- Different genetic and environmental factors
- Challenge in defining homogeneous study populations
Outcome Measures:
- Lack of validated, responsive endpoints specific to sarcoidosis
- Need for organ-specific and patient-centered outcomes
- Challenge in defining “treatment success”
Natural History Variability:
- Spontaneous remission in many patients
- Variable disease course
- Difficulty in attributing improvement to therapy versus natural history
Rare Disease Challenges:
- Limited patient populations for trials
- Funding constraints for a relatively rare disease
- Need for multinational collaboration
Despite these challenges, the field of sarcoidosis treatment is experiencing unprecedented activity in clinical trials and therapeutic development. These emerging approaches offer hope for improved outcomes, particularly for patients with refractory disease or those who cannot tolerate current therapies. As our understanding of the pathophysiology continues to advance, more targeted and effective treatments are likely to emerge.
9. Prevention & Precautionary Measures
How can sarcoidosis be prevented?
The prevention of sarcoidosis is challenging because the exact cause remains unknown. Currently, there is no proven method to prevent the initial development of sarcoidosis. However, certain strategies may reduce the risk of developing the disease or help prevent disease progression and complications in those already diagnosed:
Primary Prevention (Preventing Initial Development):
Avoidance of Potential Environmental Triggers:
- While definitive triggering agents have not been established, prudent avoidance of suspected environmental exposures may be reasonable:
- Occupational exposures: Proper protective equipment when working with metals, silica, or in dusty environments
- Reducing exposure to mold and water-damaged buildings
- Appropriate protection during firefighting activities or exposure to combustion products
- Limitations: The specific environmental triggers remain largely speculative, making targeted prevention difficult
- While definitive triggering agents have not been established, prudent avoidance of suspected environmental exposures may be reasonable:
Smoking Cessation:
- Though smoking is not a direct cause of sarcoidosis (and has actually been associated with lower incidence in some studies), smoking can worsen pulmonary symptoms and outcomes
- Smoking cessation is advisable for general lung health and to reduce complications if sarcoidosis develops
Regular Health Monitoring for High-Risk Individuals:
- First-degree relatives of sarcoidosis patients
- Individuals in high-risk occupations
- People of ethnicities with higher prevalence (African Americans, Northern Europeans)
- Limitations: No established screening protocols exist; cost-effectiveness unproven
Secondary Prevention (Preventing Progression in Diagnosed Patients):
Early Diagnosis and Treatment:
- Prompt recognition and appropriate treatment may prevent progression to chronic or fibrotic disease
- Regular monitoring for asymptomatic organ involvement
- Timely initiation of therapy when indicated by disease progression
Optimal Management of Active Disease:
- Appropriate immunosuppressive therapy to control inflammation
- Regular monitoring of disease activity
- Adjustment of treatment based on response
- Goal: Prevent granuloma formation and subsequent fibrosis
Prevention of Treatment-Related Complications:
- Appropriate prophylaxis for long-term corticosteroid users:
- Calcium and vitamin D supplementation (with monitoring in sarcoidosis)
- Bone density monitoring and bisphosphonates when indicated
- Pneumocystis jirovecii pneumonia prophylaxis for patients on significant immunosuppression
- Tuberculosis screening before biologic therapy
- Appropriate prophylaxis for long-term corticosteroid users:
Tertiary Prevention (Limiting Impact in Established Disease):
Vigilant Monitoring for Organ Involvement:
- Regular cardiac screening for sarcoidosis patients (ECG, echocardiography)
- Ophthalmological examinations to detect and treat ocular involvement
- Pulmonary function testing to monitor for deterioration
- Neurological evaluation when symptoms suggest CNS involvement
Management of Comorbidities:
- Aggressive management of conditions that may worsen sarcoidosis outcomes:
- Hypertension
- Diabetes
- Obesity
- Other respiratory conditions
- Aggressive management of conditions that may worsen sarcoidosis outcomes:
Rehabilitation and Supportive Care:
- Pulmonary rehabilitation for respiratory impairment
- Exercise programs to maintain cardiorespiratory fitness
- Psychological support for coping with chronic illness
- Occupational therapy to maintain function despite limitations
General Preventive Measures:
Lifestyle Factors:
- Balanced nutrition
- Regular physical activity appropriate to condition
- Stress management
- Adequate sleep
- Maintenance of healthy weight
Infection Prevention:
- Proper vaccinations (particularly important for immunosuppressed patients)
- Hand hygiene and general infection prevention measures
- Avoiding exposure to individuals with active infections
Environmental Controls:
- Air filtration systems for those with significant respiratory involvement
- Avoidance of air pollution and respiratory irritants
- Humidity control to reduce mold exposure
Regular Healthcare Surveillance:
- Established relationship with healthcare providers familiar with sarcoidosis
- Regular follow-up even during apparent remission
- Low threshold for evaluation of new symptoms
It’s important to note that the effectiveness of these preventive measures remains largely theoretical, as there have been few studies specifically examining prevention strategies for sarcoidosis. The complex and multifactorial nature of the disease, involving both genetic predisposition and environmental triggers, makes developing definitive prevention strategies challenging.
Research into the exact causes and mechanisms of sarcoidosis is ongoing, and as our understanding improves, more targeted prevention strategies may emerge. For now, the focus remains on risk factor modification where possible, early detection, and appropriate management to prevent complications and disease progression.
Lifestyle changes and environmental precautions
While there is no proven way to prevent sarcoidosis, certain lifestyle modifications and environmental precautions may help manage the condition, potentially reduce flares, and improve overall quality of life for those with the disease:
Lifestyle Modifications:
Diet and Nutrition:
- Anti-inflammatory diet: Emphasis on fruits, vegetables, whole grains, and omega-3 fatty acids
- Calcium management:
- Moderate calcium intake for patients with hypercalcemia or hypercalciuria
- Careful monitoring of vitamin D supplementation (due to altered metabolism in sarcoidosis)
- Adequate hydration: Particularly important for those with hypercalciuria to reduce kidney stone risk
- Weight management: Helps reduce inflammatory burden and improves respiratory symptoms
- Limited alcohol consumption: Particularly important for those on hepatotoxic medications
Physical Activity:
- Regular, moderate exercise appropriate to condition
- Pulmonary rehabilitation programs for those with significant respiratory involvement
- Breathing exercises to improve lung function
- Balance between activity and rest for those with fatigue
- Avoidance of extreme exertion that may worsen symptoms
Stress Management:
- Stress reduction techniques: Meditation, mindfulness, yoga
- Adequate sleep and sleep hygiene
- Psychological support and counseling when needed
- Support groups for emotional well-being and shared experiences
- Pacing of activities to avoid exhaustion
Smoking Cessation:
- Critical for those with pulmonary involvement
- Avoidance of secondhand smoke
- Resources and support for quitting
Alcohol and Substance Use:
- Moderation or avoidance of alcohol, particularly for those with liver involvement or on hepatotoxic medications
- Avoidance of recreational drugs that may impact respiratory function
- Careful medication management to avoid interactions
Environmental Precautions:
Occupational Considerations:
- Assessment of workplace exposures that might trigger or exacerbate symptoms
- Use of personal protective equipment when exposed to:
- Dusts and particulates
- Industrial chemicals
- Metal fumes
- Insecticides or pesticides
- Workplace accommodations when needed
- Consideration of occupational change in severe cases with ongoing exposures
Home Environment:
- Indoor air quality management:
- HEPA air filtration systems
- Regular HVAC maintenance
- Removal of visible mold
- Repair of water damage
- Reduced use of irritating cleaning chemicals or air fresheners
- Dust control measures
- Proper ventilation
- Humidity control (40-50% ideal) to prevent mold growth
- Indoor air quality management:
Outdoor Environment:
- Monitoring air quality indices and limiting outdoor activities during poor air quality days
- Wearing masks (N95 or better) when air quality is poor or during high pollen or dust conditions
- Awareness of seasonal variations that may affect symptoms
- Limiting exposure to extreme temperatures, which can trigger respiratory symptoms
Infection Prevention:
- Regular hand washing
- Avoiding crowds during peak infectious seasons
- Appropriate vaccinations (including annual influenza vaccine)
- Special precautions for those on immunosuppressive therapy
- Prompt treatment of infections to prevent exacerbations
Travel Considerations:
- Pre-travel consultations for those on immunosuppression
- Oxygen needs assessment for air travel
- Medication management plans for different time zones
- Awareness of air quality at destination
- Healthcare access planning for potential flares while traveling
Medication and Treatment Adherence:
Medication Management:
- Strict adherence to prescribed regimens
- Understanding of potential side effects and when to report them
- Regular monitoring of drug levels and potential toxicities when applicable
- Medication organization systems to improve adherence
- Communication with healthcare providers about effectiveness and side effects
Medical Monitoring:
- Keeping regular follow-up appointments
- Compliance with recommended screening and monitoring tests
- Maintaining a symptom diary to identify patterns and triggers
- Developing an action plan for flares or worsening symptoms
Integrated Healthcare Approach:
- Coordination among specialists involved in care
- Consideration of complementary approaches (acupuncture, massage) as adjuncts to medical therapy
- Rehabilitation services when appropriate (physical therapy, occupational therapy)
- Psychological support for coping with chronic illness
Practical Implementation Strategies:
Gradual Implementation:
- Focus on one or two changes at a time
- Build sustainable habits rather than making drastic temporary changes
- Regular reassessment of what’s working and what isn’t
Personalized Approach:
- Recognize that triggers and effective lifestyle changes vary between individuals
- Self-monitoring to identify personal patterns and triggers
- Adaptability as disease status changes
Support Systems:
- Engage family members and close friends in understanding the condition
- Connect with support groups (online or in-person)
- Utilize resources from organizations like the Foundation for Sarcoidosis Research
These lifestyle changes and environmental precautions should be viewed as complementary to medical treatment rather than replacements for appropriate medical care. The effectiveness of specific measures may vary between individuals, and any significant changes should be discussed with healthcare providers, particularly for those on medications that may interact with dietary supplements or significant lifestyle modifications.
Vaccines (if applicable) or preventive screenings
While there are no vaccines specifically designed to prevent sarcoidosis, immunizations and preventive screenings play important roles in the care of individuals with or at risk for sarcoidosis:
Immunization Recommendations:
Standard Adult Vaccines:
- All sarcoidosis patients should receive age-appropriate vaccinations according to national guidelines
- Particularly important for those on immunosuppressive therapy
- Include:
- Influenza vaccine (annually)
- Pneumococcal vaccines (PPSV23 and PCV13/PCV20/PCV15 per current guidelines)
- Tetanus, diphtheria, and pertussis (Tdap) boosters
- Hepatitis B (if not previously immunized)
- Herpes zoster vaccine (for appropriate age groups)
- COVID-19 vaccination and boosters
Special Considerations for Immunosuppressed Patients:
- Live vaccines (e.g., live zoster vaccine, live MMR) are generally contraindicated for patients on significant immunosuppression
- Inactivated or recombinant vaccines are preferred
- Timing of vaccinations ideally before initiating immunosuppressive therapy when possible
- Potentially reduced vaccine response in those on immunosuppression
- Additional doses or booster vaccines may be recommended
Travel Vaccines:
- Pre-travel consultation recommended
- Assessment of specific travel-related risks
- Consideration of disease activity and immunosuppression when planning travel
- Avoidance of live vaccines for those on significant immunosuppression
Preventive Screenings for Those with Established Sarcoidosis:
Pulmonary Monitoring:
- Pulmonary function tests (PFTs): Initially and at regular intervals based on disease activity
- Chest imaging: Frequency determined by disease activity and treatment
- Six-minute walk test: To assess functional capacity
- Oxygen saturation monitoring: At rest and with activity
Cardiac Screening:
- Electrocardiogram (ECG): Baseline and periodic monitoring
- Echocardiography: Baseline for most patients, more frequent monitoring for those with cardiac involvement
- Advanced cardiac imaging (cardiac MRI, PET): For suspected cardiac involvement
- Holter monitoring: For those with arrhythmias or suspected conduction abnormalities
Ophthalmological Screening:
- Comprehensive eye examination: Baseline and periodic monitoring (every 6-12 months)
- Slit-lamp examination: For anterior uveitis
- Fundoscopic examination: For posterior segment involvement
- Regular screening for corticosteroid-induced complications (glaucoma, cataracts)
Metabolic Monitoring:
- Calcium levels: Serum calcium and urinary calcium excretion
- Renal function: Particularly important for those with hypercalciuria or on nephrotoxic medications
- Liver function: Baseline and periodic monitoring, especially for those on hepatotoxic medications
- Glucose monitoring: For those on corticosteroids
- Bone density screening: For patients on long-term corticosteroids
Neurological Assessment:
- Baseline evaluation when neurosarcoidosis is suspected
- Periodic monitoring of established neurological manifestations
- Cognitive assessment when indicated
- CSF analysis, MRI, and other studies as appropriate for suspected or established neurosarcoidosis
Preventive Screenings for High-Risk Individuals Without Diagnosed Sarcoidosis:
While there are no established screening protocols for detecting early or asymptomatic sarcoidosis in high-risk individuals, the following may be considered:
First-Degree Relatives of Sarcoidosis Patients:
- Increased awareness of symptoms
- Lower threshold for evaluation of suggestive symptoms
- No evidence currently supports routine screening of asymptomatic relatives
High-Risk Occupational Groups:
- Regular occupational health assessments
- Respiratory symptom questionnaires
- Consideration of baseline and periodic chest imaging and PFTs
- Proper use of protective equipment to minimize exposures
High-Risk Ethnic Groups:
- African Americans and those of Scandinavian descent
- Increased awareness of symptoms
- Prompt evaluation of suggestive symptoms
- No evidence currently supports population-based screening
Monitoring for Treatment-Related Complications:
Corticosteroid-Related Monitoring:
- Bone density testing (DEXA scan): Baseline and follow-up
- Blood pressure monitoring
- Blood glucose monitoring
- Eye examinations for cataracts and glaucoma
- Regular weight monitoring
Immunosuppressant Monitoring:
- Methotrexate: CBC, liver function, renal function
- Azathioprine: CBC, liver function
- Mycophenolate: CBC, renal function
- TNF inhibitors: Tuberculosis screening before initiation, monitoring for infections
Antimalarial Monitoring:
- Regular ophthalmological examinations for retinal toxicity
- ECG for QT interval monitoring with chloroquine
Implementation of Preventive Measures:
Coordinated Care Approach:
- Multidisciplinary team involvement when multiple organ systems are affected
- Clear communication among providers
- Comprehensive care plan addressing all aspects of disease management
Patient Education:
- Understanding of disease manifestations and when to seek care
- Recognition of potential complications
- Importance of adherence to screening recommendations
- Self-monitoring techniques
Systematic Follow-up:
- Structured follow-up schedules based on disease activity and organ involvement
- Systems to ensure patients don’t fall through cracks in care
- Reminder systems for screenings and vaccinations
While there is no specific vaccine or screening test for sarcoidosis itself, these preventive measures aim to reduce complications from the disease and improve overall outcomes for affected individuals.
10. Global & Regional Statistics
Incidence and prevalence rates globally
Sarcoidosis demonstrates significant geographic and ethnic variations in both incidence and prevalence. Understanding these patterns provides important epidemiological insights and may help identify environmental or genetic factors contributing to the disease.
Global Incidence Rates:
The annual incidence of sarcoidosis varies widely across different regions:
North America:
- United States: 5-10 cases per 100,000 population annually
- Higher rates among African Americans (35-80 per 100,000) compared to Caucasians (10-14 per 100,000)
- Canada: Approximately 6.8 cases per 100,000 population annually
Europe:
- Northern European countries (particularly Scandinavia): 11-15 cases per 100,000 annually
- Sweden: Estimated at 11.5 per 100,000 per year
- Southern European countries: Lower rates than in Northern Europe, demonstrating a north-south gradient
- United Kingdom: Intermediate rates between Northern and Southern Europe
Asia:
- Japan: 1-2 cases per 100,000 population annually
- South Korea: 0.5-1.3 per 100,000 population annually
- Other parts of Asia: Generally lower incidence than Western countries
Africa:
- Limited data from most African countries
- Higher rates reported in studies of specific populations, but comprehensive epidemiological data are lacking
Australia/Oceania:
- Intermediate rates similar to North America
- Limited population-based studies
South America:
- Generally lower rates compared to North America and Europe
- Limited epidemiological data available
Global Prevalence Rates:
Prevalence figures (the total number of cases in a population at a given time) also show significant variation:
North America:
- United States: Overall prevalence of 10-20 per 100,000
- African Americans: Higher prevalence of approximately 50-60 per 100,000
- Native Americans: Low prevalence compared to other U.S. populations
Europe:
- Sweden: Prevalence of approximately 160 per 100,000 (0.16% of the population)
- Denmark: Similar to Sweden
- Southern European countries: Lower prevalence compared to Northern Europe
Asia:
- Japan: Prevalence of approximately 1-10 per 100,000
- Other Asian countries: Generally lower prevalence compared to Western countries
The variation in incidence and prevalence rates may reflect true differences in disease occurrence due to genetic and environmental factors, but may also be influenced by:
- Differences in diagnostic approaches and healthcare access
- Variation in awareness and recognition of the disease
- Competing diseases (like tuberculosis) that may mask sarcoidosis in some regions
- Differences in study methodologies and case definitions
- Variable healthcare documentation and reporting systems
It’s important to note that sarcoidosis is likely underdiagnosed in many parts of the world, particularly in regions with limited healthcare resources or where other granulomatous diseases like tuberculosis are common.
Mortality and survival rates
Mortality and survival rates for sarcoidosis vary based on factors including disease severity, organ involvement, demographic characteristics, and access to healthcare:
Overall Mortality:
- The mortality rate attributable to sarcoidosis is approximately 1-6% of all diagnosed cases
- Five-year mortality after diagnosis is estimated at approximately 7%
- Most deaths occur in patients with severe pulmonary, cardiac, or neurological involvement
- In the United States, mortality appears to be increasing over time, possibly due to better recognition of the disease as a cause of death
Mortality by Demographics:
- Age: Higher mortality in older patients at diagnosis
- Gender: Some studies show higher mortality in females, though results are inconsistent
- Race/Ethnicity:
- African Americans have a higher mortality rate compared to Caucasians in the United States
- Age-adjusted sarcoidosis-related mortality is 12 times higher in African Americans compared to Caucasians in some studies
- In the United States, mortality rates are highest among African American females
Cause-Specific Mortality:
- Respiratory Failure: The most common cause of sarcoidosis-related death, accounting for more than 60% of sarcoidosis-related mortality
- Cardiac Complications: Including arrhythmias, conduction blocks, and heart failure
- Neurological Complications: Particularly those affecting vital functions
- Infections: Sometimes related to immunosuppressive therapy
- Treatment Complications: Related to long-term immunosuppression
Survival Rates:
Overall Survival:
- 10-year survival rates range from 70-95%, depending on the population studied
- Survival has improved over time with advances in detection and treatment
Prognostic Factors Affecting Survival:
- Pulmonary fibrosis (stage IV disease) is associated with increased mortality
- Cardiac involvement significantly reduces survival rates
- Pulmonary hypertension is associated with poor outcomes
- Neurosarcoidosis affecting critical areas has higher mortality
Cardiac Sarcoidosis:
- Five-year survival rates of 60-75% with treatment
- Untreated cardiac sarcoidosis has a much worse prognosis, with five-year survival rates possibly as low as 40%
Fibrotic Pulmonary Sarcoidosis:
- Five-year survival rates of 50-70% for those with extensive fibrotic changes
- Progressive fibrotic phenotype associated with worse outcomes
It’s important to note that mortality figures may underestimate the true impact of sarcoidosis, as the disease is not always recognized as the cause of death, particularly in cases of cardiac involvement where sudden death may be attributed to other causes. Additionally, treatment-related complications may contribute to mortality without being directly attributed to sarcoidosis.
Country-wise comparison and trends
Sarcoidosis shows significant variation across different countries and regions, with notable trends in incidence, prevalence, and clinical presentation:
North America:
United States:
- Clear racial disparities with higher incidence and prevalence in African Americans
- Estimated lifetime risk: 2.1% for African American males, 2.7% for African American females, 0.7% for Caucasian males, and 1.0% for Caucasian females
- Geographic variation with higher rates in northern and northeastern states
- African Americans tend to have more severe, chronic, and extrapulmonary disease
- Rising incidence in recent decades, particularly in women and older adults
- Higher mortality rates in African Americans, especially women
Canada:
- Patterns similar to the United States but with less pronounced racial differences
- Incidence of approximately 6.8 per 100,000 per year
- Higher rates in eastern provinces
Europe:
Scandinavian Countries (Sweden, Denmark, Finland, Norway):
- Highest incidence and prevalence in Europe
- Sweden: Incidence of 11.5 per 100,000 per year and prevalence of 0.16%
- Higher rates in northern regions compared to southern regions within these countries
- Löfgren’s syndrome (acute presentation with erythema nodosum, bilateral hilar lymphadenopathy, and often arthritis) is particularly common
United Kingdom and Ireland:
- Intermediate rates between Northern and Southern Europe
- Significant ethnic variations within the UK, with higher rates in ethnic minorities
Southern Europe (Spain, Italy, Greece):
- Lower incidence and prevalence compared to Northern Europe
- Less frequent Löfgren’s syndrome presentations
Eastern Europe:
- Limited epidemiological data
- Generally lower reported rates, but this may reflect underdiagnosis
Asia:
Japan:
- Most well-studied Asian country for sarcoidosis
- Lower incidence (1-2 per 100,000) compared to Western countries
- Distinctive clinical features with higher rates of cardiac and ocular involvement
- Higher rates of disease in females and older adults
China, India, and Southeast Asia:
- Very low reported incidence and prevalence
- Potential underdiagnosis due to high tuberculosis prevalence
- Limited epidemiological studies
Middle East:
- Limited data but appears to have intermediate prevalence
- Higher rates reported in some countries (e.g., Saudi Arabia, Turkey) compared to East Asia
Africa:
Sub-Saharan Africa:
- Limited epidemiological data
- Likely underdiagnosed due to high prevalence of tuberculosis and other granulomatous diseases
- High rates of sarcoidosis in African Americans suggest genetic susceptibility in populations of African descent
North Africa:
- Limited data, with rates appearing lower than in Europe
- Possible underdiagnosis due to tuberculosis prevalence
Australia and New Zealand:
- Intermediate incidence and prevalence similar to North America
- Higher rates in indigenous populations in some studies
- Limited population-based epidemiological data
South and Central America:
- Generally lower reported incidence and prevalence compared to North America and Europe
- Higher rates in populations of African descent
- Limited epidemiological studies
- In Brazil, sarcoidosis is often initially misdiagnosed as tuberculosis
Temporal Trends:
Increasing Incidence: Many countries report increasing incidence over recent decades, which may reflect:
- Improved diagnostic capabilities
- Increased awareness among clinicians
- Environmental changes
- Aging populations
- Reduced competing diagnoses (e.g., tuberculosis)
Age Shifts: Many regions are reporting later age at onset compared to historical data
- Mean age at diagnosis has increased in many countries
- Bimodal distribution in some populations with peaks in young adults and older adults
Gender Trends: Increasing female predominance in many countries
- Particularly notable in older age groups
- May reflect both biological factors and healthcare-seeking behaviors
Phenotypic Changes: Some evidence suggests changing clinical presentations
- Possible decrease in frequency of Löfgren’s syndrome in some regions
- Increasing recognition of extrapulmonary manifestations
These country-wise comparisons and trends provide valuable epidemiological insights, though interpretation must consider differences in healthcare systems, diagnostic approaches, and study methodologies. The variations observed suggest complex interactions between genetic predisposition and environmental exposures that may vary across different geographic regions.
11. Recent Research & Future Prospects
Latest advancements in treatment and research
Sarcoidosis research has seen significant progress in recent years, with advancements in understanding disease mechanisms, diagnostic approaches, and treatment strategies:
Treatment Advancements:
Biologic Therapies:
- TNF-α inhibitors: Expanded use beyond refractory cases, with growing evidence supporting efficacy
- Novel biologics targeting other pathways:
- JAK inhibitors (tofacitinib, baricitinib): Showing promise in early studies, particularly for cutaneous disease
- IL-6 inhibitors (tocilizumab): Case reports suggesting efficacy in refractory disease
- Rituximab (anti-CD20): Emerging data for neurosarcoidosis and other refractory manifestations
Novel Small Molecules:
- Efzofitimod (ATYR1923): A promising immunomodulator targeting neuropilin-2, showing positive results in phase 1/2 trials for pulmonary sarcoidosis
- Antimalarial derivatives: Refined use strategies for cutaneous and systemic disease
- Antifibrotic agents: Being investigated for fibrotic pulmonary sarcoidosis
Treatment Strategy Innovations:
- Steroid-sparing approaches: Earlier introduction of steroid-sparing agents to reduce corticosteroid exposure
- “Hit early and hard” protocols: More aggressive initial treatment to potentially prevent chronic disease
- Combination therapy approaches: Using multiple agents with complementary mechanisms
- Personalized treatment algorithms based on disease phenotype and biomarkers
Diagnostic Advancements:
Imaging Technologies:
- Advanced PET techniques: Novel tracers and improved protocols for detecting active granulomatous inflammation
- Cardiac MRI: Improved sequences for detecting subtle cardiac involvement
- Quantitative chest CT analysis: Artificial intelligence and machine learning to better characterize pulmonary disease
Biomarker Development:
- Soluble interleukin-2 receptor (sIL-2R): Increasingly recognized as superior to ACE for disease activity monitoring
- Chitotriosidase: Promising marker for disease activity
- Multi-biomarker panels: Combining markers for improved sensitivity and specificity
- Exhaled breath analysis: Preliminary studies identifying volatile organic compounds associated with active disease
Genetic and Molecular Diagnostics:
- Genome-wide association studies identifying new genetic variants associated with disease susceptibility and phenotype
- Transcriptomic profiling to identify disease subtypes and predict treatment response
- Epigenetic markers associated with disease activity and progression
Research Advancements:
Pathophysiology Insights:
- Improved understanding of granuloma formation and maintenance
- Recognition of dysregulated immune pathways beyond traditional Th1 responses
- Identification of potential antigenic triggers
- Better characterization of the role of specific cell populations (Th17 cells, B cells, macrophage subtypes)
Environmental Factors:
- Increased recognition of specific occupational and environmental exposures
- Microbiome studies examining potential influences on disease development and progression
- Investigation of gene-environment interactions
Clinical Phenotyping:
- Identification of distinct disease phenotypes with different prognoses and treatment responses
- Development of clinical prediction tools
- Recognition of organ-specific disease patterns
Patient-Centered Research:
- Increased focus on patient-reported outcomes
- Quality of life assessment tools specific to sarcoidosis
- Greater emphasis on fatigue and other commonly underrecognized symptoms
- Development of sarcoidosis-specific questionnaires and functional assessments
These recent advancements reflect a growing research interest in sarcoidosis and a shift toward more personalized and targeted approaches to diagnosis and treatment. While significant challenges remain, the pace of discovery has accelerated, offering hope for improved outcomes in the future.
Ongoing studies and future medical possibilities
The field of sarcoidosis research is active with numerous ongoing studies and promising future directions that may transform our understanding and management of this complex disease:
Ongoing Clinical Trials:
Novel Therapeutics:
- EFZO-FIT Study: Phase 3 trial of efzofitimod (ATYR1923) for pulmonary sarcoidosis, evaluating its steroid-sparing effects
- JAK Inhibitor Trials: Multiple studies evaluating tofacitinib, baricitinib, and other JAK inhibitors
- Anti-IL-6 Studies: Investigating tocilizumab for refractory sarcoidosis
- Antifibrotic Agents: Trials of pirfenidone and nintedanib in fibrotic pulmonary sarcoidosis
- Combination Therapy Approaches: Studies of various combinations of conventional and biologic agents
Treatment Strategy Studies:
- Corticosteroid-Free Protocols: Evaluating methotrexate and other agents as initial therapy without steroids
- Early Intensive Treatment: Testing whether aggressive early therapy alters long-term outcomes
- Drug Withdrawal Studies: Investigating optimal duration of therapy and protocols for medication tapering
Diagnostic Studies:
- Biomarker Validation: Large-scale studies to validate promising biomarkers
- PET-CT Protocols: Standardization and validation of imaging approaches
- Machine Learning Applications: Using artificial intelligence to improve diagnostic accuracy and phenotyping
Future Medical Possibilities:
Targeted Therapies:
- Precision Medicine Approaches: Treatments tailored to specific pathophysiological pathways
- Gene Therapy: Potential approaches for genetic variants strongly associated with disease
- Nanotechnology-Based Drug Delivery: Targeted delivery of anti-inflammatory agents to affected organs
- Novel Biologics: Agents targeting newly identified inflammatory pathways
Preventive Strategies:
- Risk Prediction Models: Tools to identify high-risk individuals for preventive interventions
- Environmental Modification: Interventions to reduce exposure to potential triggering agents
- Prophylactic Therapies: For high-risk individuals, such as first-degree relatives
Diagnostic Innovations:
- Liquid Biopsy: Detection of cell-free DNA or other biomarkers in blood or other body fluids
- Molecular Imaging: Novel tracers for more specific identification of sarcoidosis activity
- Point-of-Care Testing: Rapid diagnostic tools for primary care settings
- Home Monitoring Devices: For ongoing assessment of disease activity
Technological Advances:
- Telemedicine Applications: Remote monitoring and management of sarcoidosis
- Wearable Devices: Continuous monitoring of relevant physiological parameters
- Digital Therapeutics: Applications to support symptom management and treatment adherence
- 3D Bioprinting: Potential for creating tissue models for research and personalized drug testing
Emerging Research Fields:
Microbiome Studies:
- Investigating the role of the lung and gut microbiome in disease development and progression
- Potential for microbiome-based therapeutics
Immunometabolism:
- Exploring the relationship between cellular metabolism and immune function in granuloma formation
- Metabolic pathway targeting as a therapeutic approach
Systems Biology Approaches:
- Integrative analysis of genomic, transcriptomic, proteomic, and metabolomic data
- Network-based models of disease pathogenesis
Regenerative Medicine:
- Stem cell therapies for organ repair after fibrotic damage
- Tissue engineering approaches for severely damaged organs
Challenges and Future Directions:
Clinical Trial Design:
- Development of more sensitive and responsive outcome measures
- Strategies for studying a heterogeneous disease with variable natural history
- Methods to account for spontaneous remission in efficacy assessment
Collaborative Networks:
- International registries and biobanks
- Multi-center trials to achieve adequate sample sizes
- Standardized protocols for sample collection and data sharing
Translational Research:
- Improved animal models that better recapitulate human disease
- Organoid and tissue culture systems for studying granuloma formation
- Rapid translation of laboratory findings to clinical applications
Health Disparities Research:
- Understanding and addressing race-based outcome differences
- Improving access to care for underserved populations
- Culturally tailored interventions and education
These ongoing studies and future possibilities reflect a vibrant research landscape with potential to significantly improve outcomes for sarcoidosis patients. While many challenges remain, the convergence of advanced technologies, improved understanding of disease mechanisms, and increased research funding offers promise for meaningful advances in the coming years.
Potential cures or innovative therapies under development
While a definitive cure for sarcoidosis remains elusive, several innovative approaches under investigation show potential for dramatically improving outcomes or possibly leading to curative therapies in the future:
Targeted Immune Modulation:
Precision Pathway Targeting:
- JAK-STAT Pathway Inhibitors: More selective JAK inhibitors targeting specific JAK subtypes involved in sarcoidosis
- Specific Cytokine Blockade: Beyond TNF-α, targeted inhibition of IL-17, IL-23, and other key cytokines
- Costimulatory Molecule Targeting: Agents affecting T-cell activation and interaction with antigen-presenting cells
- Potential Impact: More effective suppression of granulomatous inflammation with fewer side effects than current approaches
Cell-Specific Therapies:
- Macrophage-Targeted Therapies: Agents specifically affecting macrophage function in granulomas
- T-Cell Modulation: Selective targeting of pathogenic T-cell subsets while preserving protective immunity
- Regulatory T-Cell Enhancement: Approaches to boost natural immunoregulatory mechanisms
- Potential Impact: Interruption of granuloma formation and maintenance without broad immunosuppression
Etiology-Based Approaches:
Antimicrobial Therapies:
- Targeted Antimicrobial Regimens: Based on evidence of microbial triggers, such as the CLEAR regimen (Concomitant Levofloxacin, Ethambutol, Azithromycin, and Rifampin)
- Microbiome Modulation: Interventions to restore beneficial microbiota and reduce harmful organisms
- Potential Impact: If specific infectious triggers are confirmed, targeted antimicrobial approaches could potentially cure certain forms of sarcoidosis
Antigen-Specific Immunotherapy:
- Tolerization Approaches: Inducing immune tolerance to specific antigens involved in sarcoidosis
- Peptide Vaccines: Designed to redirect immune responses away from granuloma formation
- Potential Impact: Could fundamentally alter the disease process rather than simply suppressing inflammation
Advanced Biological Therapies:
Cell-Based Therapies:
- Regulatory T-Cell Therapy: Infusion of expanded autologous regulatory T cells to restore immune balance
- Mesenchymal Stem Cells: For their immunomodulatory and tissue-repair properties
- CAR-T Cell Approaches: Highly experimental but potentially targeting specific granuloma-forming cells
- Potential Impact: Restoration of immune homeostasis and potential regeneration of damaged tissue
Gene Therapy and Editing:
- Gene Correction: For specific genetic variants strongly associated with sarcoidosis
- RNA Therapeutics: Including siRNA and antisense oligonucleotides targeting disease-related gene expression
- CRISPR-Based Approaches: Precise editing of genetic elements contributing to dysregulated immunity
- Potential Impact: Could address underlying genetic susceptibility in certain patients
Regenerative Medicine:
Tissue Engineering:
- Bioengineered Lung Tissue: To replace areas damaged by fibrosis
- 3D-Printed Scaffolds: Seeded with patient-derived cells for organ repair
- Extracellular Matrix Modulators: To reverse or prevent fibrotic changes
- Potential Impact: Restoration of organ function after permanent damage has occurred
Stem Cell Therapies for Tissue Repair:
- Induced Pluripotent Stem Cells (iPSCs): Differentiated into specific cell types needed for tissue repair
- Tissue-Specific Progenitor Cells: To repopulate damaged areas
- Growth Factor Delivery: To stimulate endogenous repair mechanisms
- Potential Impact: Could address end-organ damage currently considered irreversible
Novel Drug Delivery Systems:
Targeted Delivery Technologies:
- Nanoparticle Formulations: Delivering drugs specifically to sites of granulomatous inflammation
- Inhalational Delivery: For direct lung targeting in pulmonary disease
- Organ-Specific Delivery Systems: For cardiac, neurological, or other organ involvement
- Potential Impact: Higher local drug concentrations with fewer systemic side effects
Long-Acting Formulations:
- Depot Injections: Providing sustained release over weeks to months
- Implantable Drug Reservoirs: For continuous delivery
- Smart Delivery Systems: Responsive to disease activity
- Potential Impact: Improved adherence, more stable drug levels, and potentially better outcomes
Combination Approaches:
Multi-Target Therapy:
- Rational Drug Combinations: Simultaneously targeting multiple pathways involved in disease
- Sequential Therapy Protocols: Different agents at different disease stages
- Individualized Combination Regimens: Based on disease phenotype and biomarkers
- Potential Impact: More complete disease control through complementary mechanisms
Integrated Treatment Strategies:
- Combined Pharmacological and Non-Pharmacological Approaches
- Drug Therapy with Rehabilitation: To address both inflammation and functional impairment
- Medical and Psychological Interventions: Addressing both physiological and psychological aspects
- Potential Impact: Comprehensive management of all disease manifestations
While true cures remain aspirational at present, these innovative approaches represent potential paradigm shifts in sarcoidosis treatment. Many are in early stages of development, and translation to clinical practice will require years of research and clinical trials. However, the diversity of approaches and increasing pace of discovery offer hope that transformative therapies may emerge in the coming decades.
The path to potential cures will likely require better understanding of disease subtypes, identification of specific causes or triggers, and personalized approaches based on individual disease mechanisms. Advances in related fields such as cancer immunotherapy, autoimmune disease treatment, and regenerative medicine will continue to inform and accelerate progress in sarcoidosis research.
12. Interesting Facts & Lesser-Known Insights
Uncommon knowledge about sarcoidosis
Sarcoidosis has several intriguing aspects that are not widely known, even among healthcare professionals:
Historical and Etymological Facts:
Name Origin: The term “sarcoidosis” derives from the Greek words “sark” (flesh) and “oid” (like), referring to the flesh-like appearance of the skin lesions initially described.
Celebrity Cases: Several notable figures have been affected by sarcoidosis, including comedian Bernie Mac (who died from complications of sarcoidosis), NFL star Reggie White, and basketball player Sean Elliott.
World Trade Center Connection: Following the 9/11 attacks, an increased incidence of sarcoidosis was observed among first responders and recovery workers, suggesting potential environmental triggers from the dust and debris.
Unusual Clinical Presentations:
Reverse Racial Disparity in Survival: Despite higher incidence and severity in African Americans, some studies suggest that among patients with advanced disease, African Americans may have better survival rates than Caucasians when receiving equivalent treatment.
Heerfordt’s Syndrome: This rare manifestation combines uveitis, parotid gland enlargement, facial nerve palsy, and fever—a constellation originally thought to be a separate disease until recognized as a presentation of sarcoidosis.
Neurosarcoidosis Mimicry: Neurosarcoidosis can mimic almost any neurological disease, including multiple sclerosis, brain tumors, and psychiatric conditions, earning it the nickname “the great imitator” among neurologists.
Paradoxical Presentations:
- Some patients with extensive radiographic abnormalities have minimal symptoms (“radiologic-clinical dissociation”)
- Others with severe symptoms may have relatively normal imaging
- This disconnect between subjective symptoms and objective findings can lead to delayed diagnosis or inappropriate treatment
Biological Peculiarities:
Smoking Paradox: Unlike most respiratory diseases, smoking appears to be protective against developing sarcoidosis and is associated with less severe disease. However, smoking can worsen symptoms in those who already have the condition.
Vitamin D Dysregulation: Sarcoidosis is one of the few conditions where vitamin D supplementation can be harmful, as activated macrophages in granulomas can convert vitamin D to its active form outside normal regulatory controls, potentially causing hypercalcemia.
Seasonal Variation: Some forms of sarcoidosis, particularly Löfgren’s syndrome, show seasonal patterns with higher incidence in spring, suggesting potential seasonal environmental triggers.
Transplantation-Associated Sarcoidosis: Sarcoidosis can occur in organ transplant recipients, either as recurrence in the recipient or as transmission from donors who had undiagnosed sarcoidosis.
Diagnostic Challenges:
The Kveim Test: This historical diagnostic test involved injecting extracts of sarcoidosis-affected tissues into the skin and observing for granuloma formation. Though rarely used today, it remains one of the few disease-specific tests ever developed for sarcoidosis.
Tattoo Sarcoidosis: Sarcoidosis granulomas can develop within tattoos, sometimes decades after tattoo placement, typically appearing as raised areas corresponding to specific ink colors (particularly black).
FDG-PET “Panda” and “Lambda” Signs: These distinctive patterns of inflammation on PET scans—the “panda sign” (symmetric uptake in the lacrimal and parotid glands resembling a panda’s face) and the “lambda sign” (uptake in hilar and right paratracheal lymph nodes resembling the Greek letter)—are highly suggestive of sarcoidosis.
Spontaneous Remission: Approximately 30-70% of sarcoidosis cases resolve spontaneously without treatment, making it difficult to assess treatment efficacy and potentially resulting in overtreatment of self-limiting disease.
Treatment Peculiarities:
Hydroxychloroquine for Hypercalcemia: Unlike most causes of hypercalcemia, sarcoidosis-associated hypercalcemia often responds to hydroxychloroquine, which inhibits the conversion of vitamin D to its active form.
Paradoxical Responses to TNF Inhibitors: While TNF inhibitors are used to treat sarcoidosis, they can paradoxically cause sarcoidosis-like reactions when used for other conditions.
Thalidomide Resurgence: Thalidomide, infamous for causing birth defects when used for morning sickness in the 1950s-60s, has found new application in treating refractory cutaneous sarcoidosis due to its immunomodulatory properties.
These uncommon insights highlight the complex and sometimes contradictory nature of sarcoidosis, underscoring the challenges in understanding and managing this enigmatic disease.
Myths and misconceptions vs. medical facts
Several myths and misconceptions about sarcoidosis persist among both the general public and healthcare professionals. Addressing these with medical facts is important for improving understanding and care:
Myth 1: Sarcoidosis is a rare disease that primarily affects the lungs. Fact: While sarcoidosis is classified as a rare disease in many regions, it is actually relatively common in certain populations, with lifetime risks as high as 2-3% in African American women. Although the lungs are involved in about 90% of cases, sarcoidosis is a multisystem disorder that can affect virtually any organ system, and some patients have no pulmonary involvement at all.
Myth 2: Sarcoidosis is a form of cancer. Fact: Despite forming granulomas that can sometimes be mistaken for tumors on imaging, sarcoidosis is not cancerous. It is an inflammatory disease characterized by non-caseating granulomas. However, there is a complex relationship between sarcoidosis and malignancy, with some studies suggesting a slightly increased risk of certain cancers in sarcoidosis patients, and others showing sarcoidosis-like reactions can occur in response to malignancies.
Myth 3: Sarcoidosis is contagious. Fact: Sarcoidosis is not contagious and cannot be transmitted from person to person. While clusters of cases sometimes occur in families or workplaces, these likely reflect shared genetic susceptibility or environmental exposures rather than person-to-person transmission.
Myth 4: Sarcoidosis is a form of tuberculosis. Fact: Although sarcoidosis and tuberculosis can appear similar clinically and radiographically (both forming granulomas), they are distinct conditions. Tuberculosis is caused by Mycobacterium tuberculosis infection, while sarcoidosis has no definitively established cause. The granulomas in tuberculosis typically contain caseous (cheese-like) necrosis, whereas those in sarcoidosis are “non-caseating.”
Myth 5: Sarcoidosis always requires treatment with corticosteroids. Fact: Many cases of sarcoidosis (30-70%) resolve spontaneously without any treatment. Treatment decisions should be individualized based on organ involvement, symptom severity, and disease progression. While corticosteroids are often used when treatment is needed, alternative agents may be more appropriate in certain cases, particularly for long-term management.
Myth 6: Sarcoidosis is always a chronic, progressive disease. Fact: The disease course in sarcoidosis is highly variable. Many patients experience acute presentations with complete resolution within 2 years. Others have persistent disease that neither progresses nor resolves. Only about 10-30% develop progressive disease with organ damage. Prognosis varies significantly based on presentation, organ involvement, and demographic factors.
Myth 7: Fatigue in sarcoidosis patients is primarily due to lung involvement. Fact: Fatigue in sarcoidosis is a complex, multifactorial symptom that often occurs independently of lung function or other objective measures of disease activity. It may result from various factors including inflammation, altered sleep patterns, small fiber neuropathy, medication side effects, and comorbid conditions like depression. Fatigue can be one of the most debilitating aspects of sarcoidosis, affecting up to 85% of patients.
Myth 8: Vitamin D supplements are always beneficial for bone health in sarcoidosis patients. Fact: Unlike most conditions, vitamin D supplementation in sarcoidosis can be harmful due to dysregulated vitamin D metabolism. The granulomas in sarcoidosis can convert vitamin D to its active form outside normal regulatory controls, potentially leading to hypercalcemia and hypercalciuria. Vitamin D levels and calcium metabolism should be monitored carefully in sarcoidosis patients.
Myth 9: If chest X-rays and pulmonary function tests normalize, the disease is inactive. Fact: Sarcoidosis activity cannot be reliably determined by chest imaging and pulmonary function tests alone. The disease may be active in other organs or at a microscopic level not detectable by conventional testing. Additionally, some patients have persistent symptoms despite normalization of objective measures, possibly due to irreversible damage or ongoing subtle inflammation.
Myth 10: Sarcoidosis only affects adults. Fact: While sarcoidosis predominantly affects adults between 20-40 years of age, it can occur at any age, including in children and the elderly. Pediatric sarcoidosis, though rare, can present differently from adult disease, often with more prominent extrapulmonary manifestations. Very early-onset sarcoidosis (in children under 4 years) is now recognized as the same genetic disorder as Blau syndrome.
Myth 11: Sarcoidosis is an autoimmune disease. Fact: Despite some similarities to autoimmune conditions, sarcoidosis is better classified as a granulomatous inflammatory disorder. Unlike classic autoimmune diseases, a specific self-antigen has not been identified in sarcoidosis. The immune response in sarcoidosis appears to be directed against yet-unidentified antigens (possibly environmental), rather than self-antigens. However, the distinction is not absolute, and some overlap exists in the immune mechanisms involved.
Myth 12: All sarcoidosis patients should avoid sun exposure. Fact: While sun exposure can worsen certain cutaneous manifestations of sarcoidosis, blanket recommendations to avoid sun exposure are not appropriate for all patients. Individualized advice should consider the specific type of skin involvement, disease activity, medications (some of which cause photosensitivity), and the potential benefits of appropriate sun exposure for general health and vitamin D production.
Addressing these myths and misconceptions is essential for improving patient care, reducing stigma, and advancing public understanding of this complex disorder.
Impact on specific populations or professions
Sarcoidosis affects different populations in distinctive ways and can have unique impacts on certain professions and groups:
Impact on Specific Ethnic and Demographic Groups:
African Americans:
- Higher incidence, prevalence, and severity compared to other ethnic groups in the United States
- More likely to have chronic and extrapulmonary disease
- Often diagnosed at a younger age
- Higher rates of hospitalization and emergency department visits
- Increased mortality rates, with African American females particularly affected
- May face longer delays in diagnosis and treatment due to healthcare disparities
- Higher economic burden due to both direct medical costs and work disability
Northern Europeans (particularly Scandinavians):
- Higher prevalence compared to Southern Europeans
- More likely to present with Löfgren’s syndrome, which typically has a better prognosis
- Often have more acute presentations with higher rates of spontaneous resolution
- Different genetic associations compared to other populations
Japanese Populations:
- Lower overall prevalence but higher rates of cardiac and ocular involvement
- Distinctive genetic associations
- Often diagnosed at older ages compared to Western populations
- Higher proportion of cases in females
Women:
- Slightly higher incidence overall compared to men
- Often diagnosed at later ages than men
- May have different organ involvement patterns
- Potential impacts on reproductive health and pregnancy
- Special considerations for medications during pregnancy and breastfeeding
- May face gender-based disparities in diagnosis and treatment
Elderly Patients:
- Increasing recognition of late-onset sarcoidosis (>65 years)
- Often have atypical presentations with less obvious symptoms
- Higher risk of medication side effects
- Increased challenges in diagnosis due to comorbidities
- May have more severe disease but less aggressive treatment due to age-related concerns
Impact on Specific Professions:
Healthcare Workers:
- Multiple studies have shown higher rates of sarcoidosis among healthcare workers
- Particularly noted in nurses and those working in hospitals
- Potential occupational exposures to infectious agents or other environmental triggers
- May have earlier diagnosis due to medical knowledge and access to healthcare
- Professional impact may include difficulty performing physically demanding aspects of care
Firefighters and First Responders:
- Increased incidence noted in multiple studies, particularly following the World Trade Center attacks
- Exposure to smoke, combustion products, and other respiratory irritants
- May develop disease while still needing to perform physically demanding duties
- Potential implications for occupational health screening and monitoring
- May qualify for specific compensation programs in some regions
Military Personnel:
- Higher rates observed in certain military populations
- Potential exposures to various environmental agents during deployment
- Physical fitness requirements may be challenging with pulmonary involvement
- Access to care through military health systems may differ from civilian healthcare
- Potential eligibility for service-connected disability benefits
Industrial Workers:
- Those exposed to specific industrial materials (metals, silica, etc.) may have increased risk
- Workplace accommodations often needed for those with respiratory or physical limitations
- Challenges in distinguishing occupational lung diseases from sarcoidosis
- Potential workers’ compensation implications
Performing Artists:
- Singers, wind instrument musicians, and actors may face particular challenges with pulmonary sarcoidosis
- Vocal cord involvement can significantly impact professional capabilities
- Performance-related physical demands may be difficult with fatigue and respiratory limitations
- Career adaptations often necessary for those with significant disease
Special Populations with Unique Considerations:
Pregnant Women with Sarcoidosis:
- Disease often improves during pregnancy but may flare postpartum
- Medication considerations are complex during pregnancy and breastfeeding
- Higher risk of adverse pregnancy outcomes in women with active disease
- Need for coordinated care between rheumatologists/pulmonologists and obstetricians
Organ Transplant Recipients:
- Can develop sarcoidosis de novo after transplantation
- May experience recurrence of pre-existing sarcoidosis in the transplanted organ
- Complex interactions between immunosuppressive regimens for transplantation and sarcoidosis
- Diagnostic challenges in distinguishing rejection from sarcoidosis involvement
Patients with Concurrent Autoimmune Diseases:
- Higher than expected co-occurrence of sarcoidosis with conditions like Sjögren’s syndrome
- Treatment considerations for managing multiple immune-mediated conditions
- Diagnostic challenges when symptoms overlap
- Potential for medication interactions or cumulative toxicities
Athletes:
- Pulmonary involvement may significantly impact performance
- Cardiac sarcoidosis poses particular risks during intense physical activity
- May face difficult decisions regarding competition and career longevity
- Medication effects (e.g., corticosteroids) may impact athletic performance
Rural and Underserved Populations:
- Reduced access to specialists familiar with sarcoidosis
- Delays in diagnosis and appropriate treatment
- Challenges in maintaining complex medication regimens
- Limited access to clinical trials and newer therapies
- Telemedicine emerging as a potential solution for improving access to expertise
Understanding these population and profession-specific impacts is essential for tailoring screening, diagnosis, and management approaches to meet the needs of diverse affected groups. It also highlights the importance of considering occupational and environmental factors in disease development and management.