
⚠️ Disclaimer: The information provided in this article is for educational purposes only and does not constitute medical advice. RevisionTown does not provide diagnosis, treatment, or medical recommendations. Always consult a qualified healthcare professional regarding any medical condition, symptoms, or concerns.
Read More – 🏥 Medical Disclaimer
Comprehensive Report on Rheumatoid Arthritis
1. Overview
What is Rheumatoid Arthritis?
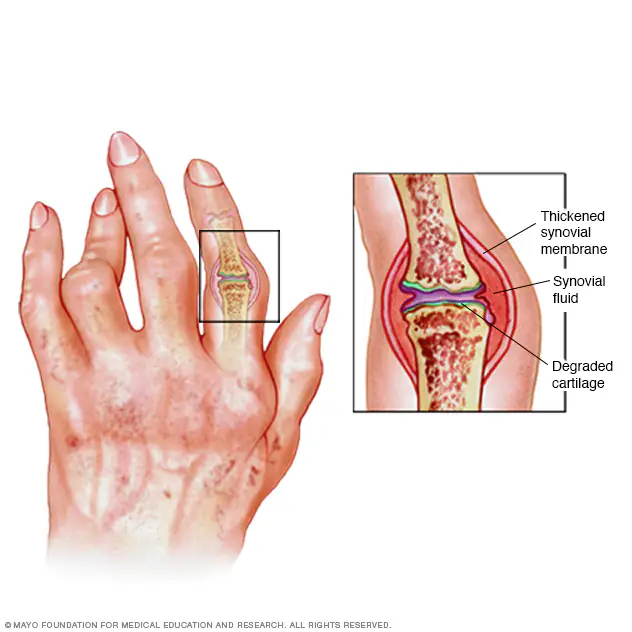
Rheumatoid arthritis (RA) is a chronic, progressive, systemic autoimmune disease characterized primarily by symmetric inflammation of the synovial joints. It is distinguished from other forms of arthritis by its autoimmune nature, where the body’s immune system mistakenly attacks its own tissues, particularly the synovial membrane lining the joint capsules. This inflammatory process leads to pain, swelling, and eventually joint destruction if left untreated.
Unlike degenerative joint conditions such as osteoarthritis, RA is marked by periods of increased disease activity (flares) alternating with periods of relative remission. As a systemic disease, RA can affect multiple organ systems beyond the joints, making it far more than simply a joint disorder.
Affected Body Parts/Organs
While RA is primarily known for its impact on joints, it can affect numerous body systems:
Joint Involvement:
- Small joints: Characteristically affects small joints symmetrically, particularly:
- Metacarpophalangeal (MCP) joints (knuckles)
- Proximal interphalangeal (PIP) joints (middle finger joints)
- Metatarsophalangeal (MTP) joints (base of toes)
- Wrist joints
- Larger joints: Can also involve:
- Elbows
- Shoulders
- Knees
- Ankles
- Hips
- Cervical spine: Particularly the atlantoaxial joint (C1-C2)
Extra-articular Manifestations:
- Skin: Rheumatoid nodules, vasculitis, palmar erythema
- Eyes: Scleritis, episcleritis, keratoconjunctivitis sicca (dry eyes)
- Lungs: Interstitial lung disease, pleural effusions, rheumatoid nodules
- Heart: Pericarditis, myocarditis, increased risk of cardiovascular disease
- Blood vessels: Rheumatoid vasculitis
- Nervous system: Peripheral neuropathy, mononeuritis multiplex
- Blood: Anemia of chronic disease, Felty’s syndrome (neutropenia and splenomegaly)
- Salivary glands: Sjögren’s syndrome (dry eyes and mouth)
- Bone: Osteoporosis, localized bone erosions
- Muscles: Myositis, muscle atrophy
Prevalence and Significance
Rheumatoid arthritis represents a significant global health burden:
Prevalence:
- Global prevalence: Approximately 0.5-1% of the adult population
- Estimated 14-16 million affected individuals worldwide
- Higher prevalence in developed countries (0.5-1.5%) than in developing nations (0.1-0.5%)
- North American and European prevalence: 0.5-1.1%
- Regional variations exist, with lowest rates in rural Africa and Asia (0.1-0.3%)
Demographic Patterns:
- Gender distribution: 2-3 times more common in women than men
- Age of onset: Can occur at any age, but peak onset is typically between 40-60 years
- Juvenile onset: Juvenile idiopathic arthritis (JIA) affects approximately 1 in 1,000 children
Economic and Social Impact:
- Direct medical costs estimated at $12,000-$18,000 per patient annually in the US
- Indirect costs (work disability, lost productivity) often exceed direct medical costs
- Work disability rates of 35-50% after 10 years of disease (in the absence of modern treatments)
- Significant impact on quality of life, comparable to serious cardiovascular or neurological diseases
- Ranks among the top causes of disability worldwide according to the World Health Organization
- Economic burden in the US estimated at $19-39 billion annually
Medical Significance:
- Serves as a prototype autoimmune disease, providing insights into immune dysregulation
- Has transformed from an inevitably disabling condition to a manageable disease with modern therapies
- Remains incurable but increasingly controllable with advanced treatments
- Represents one of the most common autoimmune diseases worldwide
- Associated with reduced life expectancy (3-10 years) if inadequately treated
The significance of RA extends beyond its prevalence, as its chronic, progressive nature creates substantial cumulative disability, economic costs, and reduced quality of life. However, dramatic improvements in treatment over the past two decades have transformed outcomes for many patients, highlighting the importance of early diagnosis and aggressive treatment.
2. History & Discoveries
First Identification and Early Descriptions
Rheumatoid arthritis has a rich and complex historical background:
Ancient Observations:
- Skeletal remains dating back to 4500 BCE show evidence of polyarthritis consistent with RA
- Hippocrates (460-370 BCE) described conditions potentially representing RA
- Unclear historical record due to potential confusion with other forms of arthritis
First Formal Descriptions:
- 1800: Augustin Jacob Landré-Beauvais, a French medical student, published the first recognized clinical description, calling it “primary asthenic gout”
- 1809: William Heberden distinguished it from gout in his work “Commentaries on the History and Cure of Diseases”
- 1858: Sir Alfred Baring Garrod coined the term “rheumatoid arthritis” in his treatise “The Nature and Treatment of Gout and Rheumatic Gout”
Early Clinical Characterization:
- 1876: Jean-Martin Charcot provided detailed descriptions of joint deformities
- 1890s: Recognition of the chronic, progressive nature of the disease
- Early 1900s: Distinction from osteoarthritis became clearer
Major Discoveries and Breakthroughs
Immunological Discoveries:
- 1940: Erik Waaler discovered the rheumatoid factor (RF), the first autoantibody associated with RA
- 1948: Rose and colleagues developed the sheep cell agglutination test for rheumatoid factor
- 1964: American Rheumatism Association (now American College of Rheumatology) established the first diagnostic criteria
- 1970s-1980s: Recognition of the role of T-cells and antigen-presenting cells
- 1987: Revised ACR criteria for RA classification
- 1997-1998: Anti-citrullinated protein antibodies (ACPA) identified
- 2010: ACR/EULAR developed new classification criteria emphasizing early disease
Treatment Evolution:
- Early remedies (1500s-1800s): Willow bark (containing salicylates), bloodletting, gold salts
- 1897: Aspirin (acetylsalicylic acid) synthesized
- 1929: Gold compounds introduced for RA treatment
- 1930s-1940s: Sulfasalazine developed
- 1950s: Corticosteroids introduced, dramatically altering short-term outcomes
- 1960s: Recognition of the disease-modifying potential of antimalarials
- 1962: Methotrexate first used for RA (became mainstream in 1980s)
- 1980s: Emergence of combination DMARD therapy
- 1998: FDA approval of first TNF inhibitor (etanercept)
- 1999-2001: Additional TNF inhibitors (infliximab, adalimumab) approved
- 2005-2010: Approval of biologics targeting other pathways (B-cells, T-cells, IL-6)
- 2012: First JAK inhibitor (tofacitinib) approved
- 2018-2023: Next-generation JAK inhibitors with improved selectivity
Pathophysiological Insights:
- 1970s: HLA-DR4 association established, indicating genetic predisposition
- 1980s: Recognition of cytokines (particularly TNF-α) in disease pathogenesis
- 1990s: Identification of synovial fibroblasts as key effector cells
- 2000s: Genome-wide association studies identifying multiple risk loci
- 2010s: Recognition of citrullination in breaking immune tolerance
- 2015-present: Role of microbiome in disease pathogenesis
Evolution of Medical Understanding
Conceptual Shifts:
- From a mysterious “wasting disease” to a defined clinical entity (19th century)
- From a primary joint disease to a systemic autoimmune disorder (mid-20th century)
- From a single disease to a syndrome with multiple subtypes (late 20th century)
- From focusing on symptom management to disease modification (1960s-1990s)
- From accepting progressive disability to expecting remission (2000s-present)
Diagnostic Evolution:
- From purely clinical diagnosis to incorporation of laboratory markers (1940s-1950s)
- From late diagnosis of established disease to emphasis on early detection (1990s-present)
- From rigid classification criteria to more fluid, probability-based approaches
- From binary “RA/not RA” thinking to spectrum concepts including “pre-RA”
Treatment Philosophy Changes:
- From “go low, go slow” to “hit hard, hit early” approach (1990s)
- From sequential monotherapy to combination therapy (1980s-1990s)
- From symptom control to treatment-to-target approaches (2000s)
- From empirical treatment selection to biomarker-guided precision medicine (emerging)
- From accepting treatment toxicity to emphasizing safety and quality of life
Research Focus Shifts:
- From clinical description to pathophysiological understanding
- From broad immunosuppression to targeted immune modulation
- From palliative care to disease remission and prevention
- From managing established disease to identifying pre-clinical phases
- From drug discovery to prediction, prevention, and cure
The evolution of our understanding of rheumatoid arthritis represents one of medicine’s great success stories, transforming from a poorly understood, inevitably disabling condition to a prime example of how molecular understanding can lead to targeted therapies and dramatically improved outcomes. This evolution continues today, with increasing focus on personalized approaches, prediction, and ultimately prevention.
3. Symptoms
Early Symptoms
The initial manifestations of rheumatoid arthritis often develop gradually over weeks to months and may be subtle:
Joint Symptoms:
- Morning stiffness: Lasting >30 minutes (often 1-3 hours), a key distinguishing feature
- Joint pain (arthralgia): Typically worse after periods of inactivity
- Joint swelling: Soft tissue swelling due to synovitis
- Joint tenderness: Disproportionate to the degree of visible swelling
- Symmetrical involvement: Typically affecting the same joints on both sides of the body
- Small joint predominance: Especially MCP, PIP joints of hands, and MTP joints of feet
Characteristic Early Joint Patterns:
- Wrists, MCPs, and PIPs of hands
- MTPs of feet (may be overlooked by patients)
- Often sparing distal interphalangeal (DIP) joints
- Gradual addition of joints over weeks to months
Systemic Symptoms:
- Fatigue: Often profound and not proportional to inflammation or anemia
- Low-grade fever: Typically 99-100°F (37.2-37.8°C)
- General malaise: Feeling unwell without specific complaints
- Weight loss: Mild to moderate, often unintentional
- Depression and anxiety: May precede other symptoms
Early Extra-articular Manifestations (less common initially):
- Mild anemia of chronic disease
- Low-grade elevations in inflammatory markers
- Subtle peripheral sensory neuropathy
- Early signs of carpal tunnel syndrome
- Dry eyes or dry mouth (early Sjögren’s syndrome)
Advanced-Stage Symptoms
As the disease progresses without adequate treatment, symptoms become more severe and permanent joint damage occurs:
Advanced Joint Manifestations:
- Joint deformities:
- Ulnar deviation of fingers
- Boutonnière deformity (flexion of PIP, extension of DIP)
- Swan-neck deformity (hyperextension of PIP, flexion of DIP)
- Z-thumb deformity
- Hallux valgus (bunion) and hammer toes
- Ankylosis (joint fusion)
- Joint instability: From ligament and tendon damage
- Muscle atrophy: Around affected joints
- Limited range of motion: Due to structural damage
- Joint contractures: Fixed position due to soft tissue changes
- Crepitus: Grating sensation with joint movement
- Subluxation: Partial dislocation of joints
- Larger joint involvement: Progressive involvement of knees, hips, shoulders, elbows
Advanced Extra-articular Manifestations:
- Rheumatoid nodules: Firm subcutaneous lumps, typically over pressure points
- Pulmonary involvement:
- Interstitial lung disease
- Pleural effusions
- Pulmonary nodules
- Bronchiolitis
- Cardiovascular complications:
- Pericarditis
- Accelerated atherosclerosis
- Increased risk of myocardial infarction
- Valve abnormalities
- Ocular manifestations:
- Scleritis
- Episcleritis
- Keratoconjunctivitis sicca
- Neurological involvement:
- Mononeuritis multiplex
- Peripheral neuropathy
- Cervical spine instability with potential cord compression
- Hematologic abnormalities:
- Significant anemia
- Thrombocytosis
- Felty’s syndrome (splenomegaly and neutropenia)
- Vasculitis:
- Skin ulcerations
- Digital infarcts
- Multiple organ system involvement
- Amyloidosis: Protein deposition in organs (rarer with modern treatments)
Functional Consequences:
- Difficulty with fine motor tasks (buttoning, writing)
- Impaired mobility and ambulation
- Reduced grip strength
- Inability to perform activities of daily living
- Work disability
- Psychological impact (depression, anxiety, body image issues)
Common vs. Rare Symptoms
Very Common Symptoms (>50% of patients):
- Symmetric polyarthritis
- Morning stiffness
- Fatigue
- Metacarpophalangeal and wrist involvement
- Elevated inflammatory markers
- Elevated autoantibodies (RF and/or ACPA)
Common Symptoms (10-50% of patients):
- Rheumatoid nodules
- Low-grade fever
- Weight loss
- Carpal tunnel syndrome
- Dry eyes and mouth
- Mild anemia
- Depression and anxiety
Less Common Symptoms (5-10% of patients):
- Interstitial lung disease
- Pericarditis
- Episcleritis or scleritis
- Sjögren’s syndrome
- Lymphadenopathy
Rare Symptoms (<5% of patients):
- Felty’s syndrome
- Rheumatoid vasculitis
- Mononeuritis multiplex
- Amyloidosis
- Atlantoaxial subluxation
- Cricoarytenoid arthritis (hoarseness, stridor)
- Sclerosing cholangitis
- AA amyloidosis
Symptom Progression Over Time
The natural history of RA without effective treatment typically follows a pattern:
Pre-clinical Phase:
- Autoantibodies (RF, ACPA) may be present years before symptoms
- Subtle inflammatory marker elevations
- Occasional joint symptoms without clear pattern
- Nonspecific fatigue or malaise
Early Clinical Phase (first 1-2 years):
- Initial onset often insidious, with morning stiffness and fatigue
- Gradual addition of involved joints
- Periods of flare and partial remission
- Responsive to simple interventions initially
- Subtle signs of systemic inflammation
Established Disease Phase (2-10 years):
- More persistent joint symptoms
- Development of early deformities
- Onset of extra-articular manifestations
- Decreasing functional capacity
- More refractory to simple treatments
Advanced Disease Phase (>10 years):
- Established joint deformities
- Significant functional limitation
- More prevalent extra-articular disease
- Secondary degenerative changes
- Complications from long-term inflammation
Pattern Variants:
- Monocyclic: Single episode with remission (10-20% of patients)
- Polycyclic: Periods of flare and remission (70% of patients)
- Progressive: Unremitting active disease (10-20% of patients)
- Palindromic rheumatism: Recurrent acute attacks with complete resolution between episodes
- Rheumatoid arthritis with secondary fibromyalgia: Persistent pain despite controlled inflammation
It’s crucial to note that modern treatment approaches have dramatically altered this natural history, particularly with the “treat-to-target” strategy and early aggressive intervention. Today, many patients achieve low disease activity or remission, preventing the progression to advanced stages of joint destruction.
The recognition of a “window of opportunity” early in the disease course has emphasized the importance of prompt diagnosis and treatment initiation before irreversible joint damage occurs.
4. Causes
Biological Causes
Rheumatoid arthritis results from a complex interplay of immune system dysregulation, with multiple cellular and molecular mechanisms contributing to the inflammatory process:
Immune System Abnormalities:
Autoantibody production:
- Rheumatoid factor (RF): Antibodies against the Fc portion of IgG
- Anti-citrullinated protein antibodies (ACPA): Target proteins that have undergone citrullination (conversion of arginine to citrulline)
- Other autoantibodies: Anti-carbamylated protein, anti-PAD4, anti-RA33
Cellular immune responses:
- T-cell abnormalities: CD4+ T cells (particularly Th1 and Th17 subtypes) contribute to inflammation
- B-cell hyperactivity: Autoantibody production and antigen presentation
- Innate immune cells: Macrophages, dendritic cells, mast cells, and neutrophils all play roles
- Altered T-regulatory cell function: Impaired immunomodulatory function
Cytokine imbalance:
- Pro-inflammatory cytokines: Tumor necrosis factor-alpha (TNF-α), interleukin-1 (IL-1), interleukin-6 (IL-6), GM-CSF
- Chemokines: Attracting inflammatory cells to joints
- Reduced anti-inflammatory cytokines: IL-10, TGF-β
Synovial Pathology:
- Synovial hyperplasia: Thickening of normally thin synovial lining
- Neoangiogenesis: Formation of new blood vessels
- Infiltration of inflammatory cells: Creating lymphoid-like structures in some cases
- Pannus formation: Invasive synovial tissue that degrades cartilage and bone
- Fibroblast-like synoviocytes: Become hyperplastic and invasive with tumor-like properties
Joint Destruction Mechanisms:
- Cartilage degradation: Matrix metalloproteinases and other enzymes
- Bone erosion: Mediated by osteoclast activation via RANKL pathway
- Altered osteoblast function: Reduced bone formation and repair
- Ligament and tendon weakening: Leading to joint instability and deformity
Systemic Inflammation:
- Acute phase reactants: Elevated C-reactive protein (CRP), erythrocyte sedimentation rate (ESR)
- Complement activation: Contributing to tissue damage
- Endothelial activation: Promoting cardiovascular disease
- Anemia of chronic disease: Mediated by hepcidin and altered iron metabolism
Genetic and Hereditary Factors
Genetic predisposition plays a crucial role in RA susceptibility:
Heritability:
- Twin studies show 15-30% concordance in monozygotic twins vs. 5% in dizygotic twins
- Overall heritability estimated at 60%
- First-degree relatives have 2-4 times increased risk
Major Genetic Associations:
HLA-DR genes (strongest genetic risk factor):
- Shared epitope hypothesis: Specific amino acid sequences in HLA-DRB1 (positions 70-74)
- HLA-DRB1*01 and *04 alleles particularly associated with RA
- Stronger association with ACPA-positive RA than ACPA-negative RA
Non-HLA genes:
- PTPN22: Tyrosine phosphatase involved in T-cell receptor signaling
- PADI4: Peptidyl arginine deiminase type 4, involved in citrullination
- STAT4: Signal transducer and activator of transcription 4, involved in cytokine signaling
- TRAF1-C5: Tumor necrosis factor receptor-associated factor 1
- IL6R: Interleukin-6 receptor
- TNFAIP3: Tumor necrosis factor alpha-induced protein 3 (A20)
- Many others: >100 risk loci identified by genome-wide association studies
Genetic Contributions to Disease Subtypes:
- Different genetic associations with ACPA-positive vs. ACPA-negative RA
- Specific genetic markers associated with treatment response
- Genetic factors influencing extra-articular manifestations
Epigenetic Factors:
- DNA methylation patterns altered in RA
- Histone modifications affecting gene expression
- MicroRNAs regulating immune cell function
- Long non-coding RNAs influencing inflammatory pathways
Environmental Triggers and Exposure Risks
Various environmental factors may trigger disease onset in genetically susceptible individuals:
Infectious Agents (potential roles):
Bacterial infections:
- Porphyromonas gingivalis (periodontal disease): Can cause protein citrullination
- Proteus mirabilis: Molecular mimicry with HLA-DR4
- Mycoplasma: Found in synovial fluid of some patients
- Mycobacteria: Potential triggers through heat shock proteins
Viral infections:
- Epstein-Barr virus (EBV): Molecular mimicry, altered immune regulation
- Parvovirus B19: Can cause an RA-like arthritis
- Retroviruses: Theoretical associations
- SARS-CoV-2: Emerging data on post-COVID autoimmunity
Lifestyle and Environmental Exposures:
Smoking: Most well-established environmental risk factor
- 1.5-2 times increased risk in current smokers
- Particularly strong interaction with shared epitope alleles
- Promotes protein citrullination in lung tissue
Air pollution: Exposure to particulate matter associated with increased risk
Occupational exposures:
- Silica dust (mining, sandblasting, construction)
- Mineral oils and solvents
- Textile dust
Dietary factors:
- High sodium intake may increase risk
- Mediterranean diet may be protective
- Fish oil consumption potentially protective
- Insufficient vitamin D associated with increased risk
Microbiome Dysbiosis:
- Altered gut microbiota composition in RA patients
- Reduced microbial diversity
- Increased abundance of Prevotella copri in some patients
- Depletion of beneficial anti-inflammatory species
- Potential “gut-joint axis” involvement
Hormonal Factors:
- Female predominance suggests hormonal influence
- Pregnancy often improves symptoms (temporary remission)
- Postpartum flares common
- Oral contraceptive use may have modest protective effect
- Breastfeeding may be protective
- Abnormal estrogen metabolism in some patients
Physical and Psychological Stressors:
- Physical trauma occasionally reported as a trigger (“gateway theory”)
- Major life stressors may precede onset in some cases
- Chronic stress affects immune regulation
The development of rheumatoid arthritis likely requires a combination of genetic susceptibility and environmental exposures, with different factors predominating in different individuals. The concept of “multiple hits” suggests that several factors must converge to break immune tolerance and initiate disease.
Current research focuses on understanding these interactions, particularly the interface between genetic predisposition, environmental exposures, and the mechanisms by which tolerance to self-proteins is broken.
5. Risk Factors
Demographic Risk Factors
Age:
- Peak onset typically between ages 40-60
- Can occur at any age, including childhood
- Average age of onset decreasing in recent decades
- Elderly-onset RA (>60 years) often has more acute onset and greater systemic symptoms
- Juvenile idiopathic arthritis (JIA) represents a distinct entity in children
Sex/Gender:
- 2-3 times more common in women than men
- Female-to-male ratio highest during reproductive years (4:1)
- Ratio decreases in older age groups (closer to 1:1 after age 60)
- Males often have more erosive disease when affected
- Different clinical patterns sometimes observed between sexes:
- Women: More often seropositive, more extra-articular manifestations
- Men: More likely to have large joint involvement initially
Ethnicity and Geographic Factors:
- Native American populations: Particularly high prevalence (5-7% in some tribes)
- Northern European ancestry: Higher rates than Southern European
- African and African-American populations: Often have more aggressive disease but lower prevalence
- East Asian populations: Generally lower prevalence but can have severe disease
- Geographic gradient: Higher prevalence in northern latitudes generally
- Urban vs. rural: Often higher prevalence in urban settings
Genetic Risk Factors
HLA Associations:
- HLA-DRB1 shared epitope: Key genetic risk factor
- Confers 4-5 fold increased risk with one copy
- Up to 13-fold increased risk with two copies
- Present in approximately 70% of RA patients
- Specific risk alleles: HLA-DRB1*04:01, *04:04, *01:01, *10:01
- Protective alleles: HLA-DRB1*13:01, *04:02
Non-HLA Genetic Factors:
- PTPN22 polymorphism: 1.5-2 fold increased risk
- PADI4 variants: Particularly important in Asian populations
- STAT4 polymorphisms: 1.3-1.5 fold increased risk
- Other gene variants: TRAF1/C5, TNFAIP3, CD40, CCR6, IL6R, etc.
Family History:
- First-degree relatives: 2-4 times increased risk
- Concordance in monozygotic twins: 15-30%
- Concordance in dizygotic twins: approximately 5%
- Multicase families show stronger genetic component
Genetic Risk Score:
- Combination of multiple risk alleles substantially increases risk
- Potential for risk stratification in future preventive approaches
- Different genetic profiles for ACPA-positive vs. ACPA-negative disease
Environmental and Lifestyle Risk Factors
Tobacco Smoking:
- Strongest environmental risk factor
- Dose-dependent effect (pack-years)
- Primarily increases risk for ACPA-positive RA
- Multiplicative interaction with HLA-DRB1 shared epitope
- Mechanism involves promoting protein citrullination in lung tissue
- Continued smoking associated with worse treatment response
Other Inhalants:
- Silica dust exposure: 1.5-3 fold increased risk
- Mining, stone cutting, sandblasting, construction work
- Air pollution exposure
- Textile dust
- Asbestos exposure
- Industrial emissions
Obesity and Metabolic Factors:
- Body mass index >30: 1.2-1.5 fold increased risk
- Central obesity particularly associated
- Adipose tissue produces pro-inflammatory adipokines
- Associated with poorer treatment response
- May accelerate progression of early arthritis to RA
Dietary Factors:
- High-salt diet: Potential risk factor
- Low antioxidant intake: Possible increased risk
- Red meat consumption: Modest association in some studies
- Alcohol: Moderate consumption may be protective
- Coffee: High consumption possibly associated with increased risk (controversial)
- Sugar-sweetened beverages: Associated with increased risk in some studies
Reproductive and Hormonal Factors:
- Pregnancy history:
- Nulliparity associated with slightly increased risk
- Pregnancy provides temporary protection
- Postpartum period is high-risk time for onset
- Breastfeeding: Longer duration associated with reduced risk
- Menstrual factors: Early menarche may increase risk
- Hormone replacement therapy: Mixed evidence
- Oral contraceptive use: May modestly decrease risk
Oral and Periodontal Health:
- Periodontitis associated with increased RA risk
- Porphyromonas gingivalis infection: Promotes citrullination
- Poor dental hygiene: General association with risk
Physical and Psychological Stressors:
- Major life stressors preceding onset in some cases
- Physical trauma occasionally reported as triggering event
- Chronic psychological stress may increase risk
- Sleep disturbances: Potential modifier of risk
Impact of Pre-existing Conditions
Autoimmune Disorders:
- Autoimmune thyroid disease: Increased co-occurrence
- Primary Sjögren’s syndrome: May evolve into RA
- Systemic lupus erythematosus: Increased risk of developing RA
- Type 1 diabetes: Modest association
Infectious Diseases:
- Recent GI or urogenital infections may trigger reactive arthritis that evolves into RA
- Epstein-Barr virus (EBV) seropositivity: Associated with increased risk
- Chronic hepatitis C: Can present with RA-like manifestations
- HIV: Paradoxically may protect against RA development
Other Medical Conditions:
- Chronic obstructive pulmonary disease: Associated with increased risk
- Bronchiectasis: Associated with higher prevalence
- Gout: Negative association (potentially protective)
- Inflammatory bowel disease: Modest association
- Psoriasis: May present as psoriatic arthritis (distinct from RA)
Medication Exposures:
- Some medications associated with drug-induced lupus may trigger RA-like syndrome
- Immune checkpoint inhibitors can cause inflammatory arthritis
Risk Factor Interactions: The complex interplay between multiple risk factors dramatically impacts overall risk:
Gene-environment interactions:
- Smoking + HLA-DRB1 shared epitope = up to 40-fold increased risk
- Silica exposure + smoking = synergistic effect
- Periodontal disease + shared epitope = enhanced risk
Risk factor accumulation:
- Multiple risk factors exponentially increase risk
- Different combinations may lead to different disease phenotypes
- May explain earlier onset in certain populations
Protective factor modulation:
- Mediterranean diet may mitigate genetic risk
- Regular physical activity potentially protective
- Maintaining healthy weight may reduce risk in genetically susceptible individuals
Understanding these risk factors is crucial for identifying high-risk individuals who might benefit from preventive strategies or early intervention, and for developing targeted approaches to modify risk factors. Research increasingly focuses on developing personalized risk profiles combining genetic and environmental factors to predict individual risk.
6. Complications
Joint Complications
Without adequate treatment, rheumatoid arthritis leads to significant joint destruction and deformity:
Structural Joint Damage:
- Cartilage destruction: Progressive loss of joint space
- Bone erosions: Localized bone loss at joint margins
- Joint space narrowing: Resulting from cartilage loss
- Subchondral cysts: Fluid-filled spaces in bone near joints
- Osteophytes: Less common than in osteoarthritis, but can occur in later stages
- Periarticular osteopenia: Loss of bone density around joints
- Ankylosis: Complete joint fusion (less common with modern treatments)
Joint Deformities:
Hands and wrists:
- Ulnar deviation of fingers
- Boutonnière deformity (flexion of PIP, extension of DIP)
- Swan-neck deformity (hyperextension of PIP, flexion of DIP)
- Z-thumb (zigzag) deformity
- Piano key deformity of the wrist (displaced ulnar styloid)
- Carpal collapse
Feet:
- Hallux valgus (bunion)
- Cock-up toes / hammer toes
- Pes planovalgus (flattening of longitudinal arch)
- Subluxation of metatarsal heads
Larger joints:
- Baker’s cysts at the knee
- Hip protrusio acetabuli
- Knee valgus deformity
- Elbow contractures
- Shoulder rotator cuff tears and impingement
Tendon and Ligament Complications:
- Tendon rupture: Particularly extensor tendons of fingers
- Tenosynovitis: Inflammation of tendon sheaths
- Ligament laxity: Leading to joint instability
- Trigger finger/thumb: Due to tendon nodules or tenosynovitis
- De Quervain’s tenosynovitis: Affects thumb abductors
Functional Consequences:
- Loss of fine motor skills
- Reduced grip strength
- Inability to perform activities of daily living
- Impaired ambulation
- Work disability
Systemic Complications
Cardiovascular Complications:
- Accelerated atherosclerosis: Leading cause of excess mortality
- Increased risk of myocardial infarction: 1.5-2 times general population
- Heart failure: Both systolic and diastolic dysfunction
- Pericarditis: Inflammation of the pericardium
- Myocarditis: Less common but reported
- Valvular heart disease: Particularly mitral regurgitation
- Conduction abnormalities: Various arrhythmias
- Coronary vasculitis: Rare but serious complication
Pulmonary Complications:
- Interstitial lung disease: Occurs in 10-30% of patients
- Various patterns (UIP, NSIP, OP, etc.)
- Can precede joint symptoms in some cases
- May be exacerbated by certain RA medications
- Pleural disease: Effusions, pleuritis
- Rheumatoid nodules: Can occur in lung parenchyma
- Bronchiectasis: Bidirectional association with RA
- Pulmonary hypertension: Primary or secondary
- Cricoarytenoid arthritis: Affecting voice and airway
- Caplan’s syndrome: RA with pneumoconiosis in coal miners
Hematologic Complications:
- Anemia of chronic disease: Most common hematologic abnormality
- Felty’s syndrome: Triad of RA, splenomegaly, and neutropenia
- Large granular lymphocyte (LGL) syndrome: Expanded T-cell populations
- Thrombocytosis: Due to chronic inflammation
- Thrombocytopenia: Can occur in Felty’s syndrome or with medications
- Lymphoma: 2-4 fold increased risk, particularly diffuse large B-cell lymphoma
- Leukopenia: Due to medications or autoimmune neutropenia
Neurological Complications:
- Peripheral neuropathy: Sensory or sensorimotor
- Mononeuritis multiplex: Due to vasculitis
- Carpal tunnel syndrome: Due to tenosynovitis at the wrist
- Cervical myelopathy: From atlantoaxial subluxation or other cervical spine instability
- Entrapment neuropathies: At various sites
- Central nervous system vasculitis: Rare but serious
- Cognitive impairment: Associated with chronic inflammation
Ocular Complications:
- Keratoconjunctivitis sicca (dry eyes): Often part of secondary Sjögren’s syndrome
- Episcleritis: Inflammation of the episclera
- Scleritis: More serious than episcleritis, can threaten vision
- Peripheral ulcerative keratitis: Can lead to corneal perforation
- Retinal vasculitis: Rare but vision-threatening
- Cataracts: Often related to corticosteroid treatment
Gastrointestinal Complications:
- Medication-related GI issues: Peptic ulcers, GI bleeding with NSAIDs
- Liver abnormalities: Often medication-related (methotrexate, leflunomide)
- Vasculitis: Can affect mesenteric vessels
- Secondary amyloidosis: Deposition of amyloid A in GI tract (rare with modern treatments)
- Dry mouth: From secondary Sjögren’s syndrome
Renal Complications:
- Medication-induced nephropathy: NSAIDs, disease-modifying agents
- Amyloidosis: Renal involvement most common (historical)
- Membranous nephropathy: Associated autoimmune phenomenon
- Glomerulonephritis: Associated with vasculitis
- Renal vasculitis: Part of systemic vasculitis
Dermatological Complications:
- Rheumatoid nodules: Firm subcutaneous nodules, typically over pressure points
- Vasculitic skin lesions: Nail fold infarcts, purpura, ulcers
- Palmar erythema: Nonspecific finding
- Pyoderma gangrenosum: Neutrophilic dermatosis
- Medication-related skin reactions: Various patterns
Bone Complications:
- Osteoporosis: Multifactorial, from inflammation, immobility, and medications
- Increased fracture risk: 1.5-2 times general population
- Osteonecrosis: Often related to corticosteroid use
Psychosocial Complications
Psychological Impact:
- Depression: Affects 15-40% of patients
- Anxiety disorders: Common comorbidity
- Body image issues: Related to deformities
- Reduced self-efficacy: Feeling unable to control disease
- Sleep disturbances: Both from pain and independent sleep disorders
- Cognitive effects: “Brain fog” reported by many patients
Social Consequences:
- Work disability: 35-50% after 10 years (less with modern treatments)
- Financial burden: Direct and indirect costs
- Relationship strain: Changed roles within families
- Reduced social participation: Isolation due to disability
- Sexual dysfunction: From both physical limitations and psychological factors
- Reduced educational attainment: In juvenile-onset cases
Treatment-Related Complications
NSAID Complications:
- Gastrointestinal bleeding and ulceration
- Cardiovascular risks (myocardial infarction, stroke)
- Renal impairment
- Hypertension
- Hepatotoxicity
Corticosteroid Complications:
- Osteoporosis and fractures
- Weight gain and redistribution
- Diabetes and glucose intolerance
- Hypertension
- Cataracts and glaucoma
- Avascular necrosis
- Skin thinning and bruising
- Increased infection risk
- Adrenal suppression
DMARD Complications:
- Methotrexate: Hepatotoxicity, pneumonitis, cytopenia, oral ulcers
- Leflunomide: Hepatotoxicity, hypertension, peripheral neuropathy
- Sulfasalazine: GI intolerance, cytopenia, hypersensitivity reactions
- Hydroxychloroquine: Retinopathy, cardiomyopathy (rare)
- Biologic agents: Infections, injection site reactions, allergic reactions
- JAK inhibitors: Infections, herpes zoster, lipid abnormalities, thromboembolic events
Mortality Impact
Overall Mortality:
- Standardized mortality ratio: 1.5-2.0 (improved with modern treatments)
- Life expectancy reduced by 3-10 years historically
- Mortality gap narrowing with modern treatment approaches
- Cardiovascular disease accounts for approximately 40% of excess mortality
- Infections account for approximately 25% of excess mortality
- Respiratory complications account for approximately 15% of excess mortality
Prognostic Factors for Mortality:
- High disease activity
- Extra-articular manifestations
- Seropositivity (RF, ACPA)
- Delayed treatment
- Comorbidities (particularly cardiovascular)
- Older age at onset
- Male sex
- Lower socioeconomic status
- Corticosteroid use (especially chronic, high-dose)
Preventable Mortality: Advances in treatment have significantly reduced many complications, particularly with:
- Early diagnosis and treatment
- Treat-to-target approaches
- Decreased reliance on long-term corticosteroids
- Aggressive cardiovascular risk management
- Infection prevention strategies
- Regular monitoring for complications
The comprehensive understanding of these complications underscores the importance of early, effective treatment to prevent or minimize long-term damage. Modern management strategies aim to address not only the primary joint disease but also the systemic inflammatory state and associated comorbidities that contribute to excess morbidity and mortality in rheumatoid arthritis.
7. Diagnosis & Testing
Clinical Assessment
Medical History:
- Detailed joint symptom history (onset, pattern, duration)
- Morning stiffness duration (>60 minutes suggestive of inflammatory arthritis)
- Constitutional symptoms (fatigue, fever, weight loss)
- Prior episodes of joint swelling or inflammation
- Family history of RA or other autoimmune diseases
- Response to anti-inflammatory medications
- Impact on daily activities and function
- Presence of extra-articular symptoms
- Review of systems to identify systemic involvement
Physical Examination:
Joint examination:
- Systematic assessment of all peripheral joints
- Documentation of tender and swollen joint counts
- Assessment of joint range of motion
- Evaluation for deformities, subluxations, and contractures
- Symmetry of joint involvement
- Distribution pattern (small vs. large joints)
Extra-articular assessment:
- Skin examination for rheumatoid nodules, vasculitis
- Eye examination for signs of scleritis or sicca symptoms
- Cardiopulmonary examination
- Neurological assessment
- Lymph node examination
- Abdominal examination for hepatosplenomegaly
Functional assessment:
- Grip strength
- Fine motor skills
- Mobility and gait
- Activities of daily living capability
Laboratory Tests
Autoantibody Testing:
Rheumatoid Factor (RF):
- Historically first biomarker for RA
- Sensitivity: 60-80% (can be negative early in disease)
- Specificity: 80-90% (can be positive in other conditions)
- Higher titers associated with more severe disease
- IgA RF may have higher specificity than IgM RF
Anti-Citrullinated Protein Antibodies (ACPA):
- Also known as anti-CCP (cyclic citrullinated peptide) antibodies
- Sensitivity: 50-75% (potentially positive before clinical disease)
- Specificity: 95-98% (more specific than RF)
- Strongly associated with erosive disease
- May help identify patients at risk for developing RA
- Different generations of tests (CCP2, CCP3) with improving performance
Other Autoantibodies:
- Anti-mutated citrullinated vimentin (anti-MCV)
- Anti-carbamylated protein antibodies (anti-CarP)
- Anti-PAD4 antibodies
- Anti-RA33 (anti-heterogeneous nuclear ribonucleoprotein A2)
- Anti-nuclear antibodies (present in 15-30% of RA patients)
Inflammatory Markers:
Erythrocyte Sedimentation Rate (ESR):
- Nonspecific marker of inflammation
- Often elevated in active RA
- Used to calculate disease activity scores
- May be normal in some patients despite active disease
C-Reactive Protein (CRP):
- Acute phase reactant produced by the liver
- More responsive to short-term changes than ESR
- Better correlation with disease activity than ESR
- Used in multiple disease activity indices
- Important prognostic marker
Hematologic Tests:
Complete Blood Count (CBC):
- Anemia of chronic disease common
- Thrombocytosis in active disease
- Leukocytosis or leukopenia (medication-related or Felty’s syndrome)
- Lymphopenia may be present
Comprehensive Metabolic Panel:
- Baseline liver and renal function before treatment
- Albumin often decreased in active disease
- Elevated alkaline phosphatase possible
Synovial Fluid Analysis:
Cell count and differential:
- Inflammatory pattern: >2,000 WBC/mm³, predominantly neutrophils
- Distinguishes inflammatory from non-inflammatory arthritis
- Less specific for RA vs. other inflammatory arthritides
Crystal examination: To exclude gout or pseudogout
Culture: To exclude infectious arthritis
Protein and glucose: Typically abnormal in inflammatory conditions
Complement levels: Often decreased in synovial fluid
Genetic Testing:
- HLA-DRB1 typing: Not routinely performed but may help in uncertain cases
- Not currently recommended for routine diagnosis
Imaging Studies
Conventional Radiography (X-rays):
- Traditional first-line imaging
- Findings in established RA:
- Periarticular osteopenia (early)
- Uniform joint space narrowing
- Marginal erosions
- Subluxations and deformities
- Alignment abnormalities
- Often normal in early disease (limited sensitivity)
- Used for baseline assessment and monitoring progression
- Specific scoring systems (Sharp-van der Heijde, Larsen) for quantification
Ultrasound:
- Increasing role in early diagnosis and monitoring
- Advantages: No radiation, dynamic assessment, relatively inexpensive
- Can detect:
- Synovitis (gray-scale and power Doppler)
- Tenosynovitis
- Early erosions before radiographic visibility
- Enthesitis
- Joint effusions
- More sensitive than clinical examination for synovitis
- Operator-dependent (requires training and experience)
- Standardized scoring systems available (EULAR-OMERACT)
Magnetic Resonance Imaging (MRI):
- Most sensitive imaging modality for early changes
- Can detect:
- Synovitis
- Bone marrow edema (osteitis) – predictor of erosive progression
- Early erosions (3-6 months before radiographic visibility)
- Tenosynovitis
- Cartilage damage
- Ligament and tendon pathology
- Excellent for assessing difficult-to-evaluate joints (e.g., temporomandibular, cricoarytenoid)
- Whole-body MRI protocols available for comprehensive assessment
- Expensive and less widely available than X-ray or ultrasound
- RAMRIS (RA MRI Scoring) system for standardized assessment
Computed Tomography (CT):
- Superior to radiographs for detecting erosions
- Useful for assessing complex joints (wrist, midfoot)
- Limited by radiation exposure and inability to detect synovitis
- Particularly valuable for cervical spine evaluation
Nuclear Medicine Studies:
- Bone scintigraphy: Shows areas of increased bone turnover
- PET scans: Can demonstrate metabolically active synovitis
- PET-CT: Combining metabolic and anatomic information
- Generally used for research or specific clinical scenarios rather than routine diagnosis
Classification Criteria and Diagnostic Approach
ACR/EULAR 2010 Classification Criteria:
Joint involvement (0-5 points):
- 1 large joint (0 points)
- 2-10 large joints (1 point)
- 1-3 small joints (2 points)
- 4-10 small joints (3 points)
10 joints including at least 1 small joint (5 points)
Serology (0-3 points):
- Negative RF and ACPA (0 points)
- Low-positive RF or ACPA (2 points)
- High-positive RF or ACPA (3 points)
Acute phase reactants (0-1 point):
- Normal CRP and ESR (0 points)
- Abnormal CRP or ESR (1 point)
Duration of symptoms (0-1 point):
- <6 weeks (0 points)
- ≥6 weeks (1 point)
Score ≥6 points classifies as RA. These criteria are primarily for research classification but guide clinical diagnosis.
Differential Diagnosis:
Other inflammatory arthritides:
- Psoriatic arthritis
- Systemic lupus erythematosus
- Sjögren’s syndrome
- Polymyalgia rheumatica
- Adult-onset Still’s disease
- Reactive arthritis
- Crystalline arthropathies (gout, pseudogout)
- Spondyloarthritides
Non-inflammatory conditions:
- Osteoarthritis
- Fibromyalgia
- Paraneoplastic syndromes
- Hypothyroidism
- Sarcoidosis
- Hemochromatosis
Infectious causes:
- Viral arthritis (parvovirus, hepatitis, HIV)
- Bacterial arthritis
- Lyme disease
- Tuberculosis
Early Detection and Screening
Early RA Detection Strategies:
- Recognition of early symptoms by primary care providers
- Referral guidelines for early inflammatory arthritis
- Early arthritis clinics in specialized centers
- Screening high-risk individuals (first-degree relatives)
- Public awareness campaigns about early symptoms
Screening Biomarkers Under Investigation:
- Autoantibody profiles before clinical disease
- Cytokine patterns
- MicroRNA signatures
- Proteomic markers
- Metabolomic profiles
- Multi-biomarker disease activity scores
Pre-clinical RA:
Increasing recognition of phases preceding clinical disease:
- Genetic risk phase
- Environmental risk factors phase
- Systemic autoimmunity (autoantibodies present)
- Symptoms without clinical arthritis
- Unclassified arthritis
- Classified RA
Research initiatives focusing on identifying individuals in pre-clinical phases
Potential for preventive interventions in high-risk individuals
Effectiveness of Early Detection:
- “Window of opportunity” concept: better outcomes with earlier treatment
- Treatment within 3-6 months of symptom onset associated with higher remission rates
- Reduced radiographic progression with early intervention
- Better functional outcomes with prompt diagnosis and treatment
- Challenge: balancing early intervention against potential overtreatment
Modern diagnostic approaches emphasize the importance of early detection before irreversible joint damage occurs. The combination of clinical assessment, laboratory biomarkers, and sensitive imaging modalities allows for increasingly earlier diagnosis and treatment initiation, which is crucial for optimizing long-term outcomes in rheumatoid arthritis.
8. Treatment Options
Treatment Principles and Goals
Modern RA treatment follows several key principles:
Treat-to-Target Approach:
- Clearly defined treatment target (remission or low disease activity)
- Regular assessment of disease activity using validated measures
- Systematic therapy adjustments until target achieved
- Maintenance strategy once target is reached
- Consideration of patient factors in target selection
Early Aggressive Intervention:
- Recognition of “window of opportunity” early in disease
- Prompt initiation of disease-modifying therapy
- Combination therapy often used from the start
- Goal of preventing irreversible joint damage
Individualized Treatment:
- Consideration of disease characteristics (serostatus, erosions, etc.)
- Patient-specific factors (age, comorbidities, pregnancy plans)
- Shared decision-making incorporating patient preferences
- Balance of efficacy and safety for each individual
Comprehensive Management:
- Addressing inflammation and pain
- Preventing joint damage
- Maintaining function
- Managing comorbidities
- Supporting psychological well-being
- Considering social and occupational needs
Non-Pharmacological Approaches
Physical Therapy and Exercise:
- Range-of-motion exercises to maintain flexibility
- Strengthening exercises for periarticular muscles
- Low-impact aerobic conditioning
- Joint protection techniques
- Aquatic therapy
- Balance and proprioception training
Occupational Therapy:
- Assistive devices for daily activities
- Splinting for pain relief and deformity prevention
- Energy conservation techniques
- Home and workplace modifications
- Hand therapy for fine motor skills
Psychological Support:
- Cognitive-behavioral therapy for pain management
- Stress reduction techniques
- Depression and anxiety management
- Support groups
- Self-management education programs
Other Non-Pharmacological Approaches:
- Heat and cold therapy
- Transcutaneous electrical nerve stimulation (TENS)
- Acupuncture
- Massage therapy
- Nutrition counseling
- Weight management
Pharmacological Treatments
Analgesics and Anti-inflammatory Drugs:
NSAIDs (Non-Steroidal Anti-Inflammatory Drugs):
- Provide symptomatic relief
- Do not alter disease course
- Multiple options: ibuprofen, naproxen, diclofenac, celecoxib
- Caution with GI, renal, and cardiovascular risks
- Best used as bridging therapy or for residual symptoms
Corticosteroids:
- Rapid anti-inflammatory effect
- Various routes: oral, intramuscular, intravenous, intra-articular
- Low-dose oral (prednisone ≤10 mg/day) commonly used
- “Bridge therapy” until DMARDs take effect
- Long-term use limited by significant adverse effects
- Intra-articular injections for persistent monoarthritis
Conventional Synthetic DMARDs (csDMARDs):
Methotrexate:
- Cornerstone of RA treatment
- Typical dose: 15-25 mg weekly (oral or subcutaneous)
- Mechanism: Antiproliferative, immunomodulatory, anti-inflammatory
- Folate supplementation reduces side effects
- Efficacy: 30-40% achieve low disease activity as monotherapy
- Onset of action: 6-12 weeks
- Key adverse effects: Hepatotoxicity, pneumonitis, cytopenias, stomatitis
Leflunomide:
- Alternative to methotrexate
- Dose: 20 mg daily
- Mechanism: Inhibits pyrimidine synthesis
- Efficacy similar to methotrexate
- Long half-life requiring washout procedures if needed
- Main adverse effects: Diarrhea, hair loss, hepatotoxicity, teratogenicity
Sulfasalazine:
- Dose: 2-3 g daily
- Less effective than methotrexate overall
- Useful in mild disease or combination therapy
- Better tolerated in pregnancy than most DMARDs
- Common side effects: GI intolerance, rash, cytopenias
Hydroxychloroquine:
- Dose: 200-400 mg daily
- Mildest DMARD with excellent safety profile
- Often used in combinations
- Limited efficacy as monotherapy for established RA
- Requires ophthalmologic monitoring for retinopathy
- Potential cardiovascular benefits
Combination csDMARD Therapy:
- Various combinations possible
- “Triple therapy”: Methotrexate + sulfasalazine + hydroxychloroquine
- Methotrexate + leflunomide
- Shown to be effective and cost-efficient
Biological DMARDs (bDMARDs):
TNF Inhibitors:
- First class of biologics approved for RA
- Options:
- Adalimumab: Fully human monoclonal antibody, 40 mg every 2 weeks
- Etanercept: Soluble TNF receptor fusion protein, 50 mg weekly
- Infliximab: Chimeric monoclonal antibody, 3-10 mg/kg IV every 8 weeks
- Golimumab: Fully human monoclonal antibody, 50 mg monthly
- Certolizumab pegol: PEGylated Fab fragment, 200 mg every 2 weeks
- Efficacy: 60-70% response rates
- Rapid onset (2-4 weeks)
- Combined with methotrexate for optimal effect
- Key concerns: Infections, reactivation of tuberculosis, injection reactions
IL-6 Receptor Inhibitors:
- Tocilizumab: IV (4-8 mg/kg monthly) or SC (162 mg weekly)
- Sarilumab: 150-200 mg SC every 2 weeks
- Particularly effective for systemic symptoms
- Can be used as monotherapy (unique among biologics)
- Effect on acute phase reactants particularly pronounced
- Adverse effects: Neutropenia, elevated liver enzymes, lipid abnormalities
T-Cell Co-stimulation Modulator:
- Abatacept: Fusion protein blocking T-cell activation
- Dosing: Weight-based IV (500-1000 mg every 4 weeks) or SC (125 mg weekly)
- Slower onset of action (2-3 months)
- Excellent safety profile, particularly for infection risk
- Good option for elderly patients or those with recurrent infections
B-Cell Depleting Therapy:
- Rituximab: Anti-CD20 monoclonal antibody
- Dosing: 1000 mg IV × 2 doses, repeated every 6-12 months
- Particularly effective in seropositive (RF/ACPA+) patients
- Used after TNF inhibitor failure or in specific situations (e.g., history of lymphoma)
- Screening for hepatitis B essential
- Ofatumumab: Newer anti-CD20 antibody (subcutaneous)
IL-1 Receptor Antagonist:
- Anakinra: 100 mg SC daily
- Less widely used due to modest efficacy compared to other biologics
- Daily injection requirement
- May have role in specific RA subtypes
Targeted Synthetic DMARDs (tsDMARDs):
JAK Inhibitors:
- Oral small molecules targeting Janus kinase pathways
- Rapid onset of action (1-2 weeks)
- Options:
- Tofacitinib: JAK1/3 inhibitor, 5 mg twice daily or 11 mg XR once daily
- Baricitinib: JAK1/2 inhibitor, 2-4 mg once daily
- Upadacitinib: Selective JAK1 inhibitor, 15 mg once daily
- Filgotinib: Selective JAK1 inhibitor, 200 mg once daily
- Can be used as monotherapy
- Adverse effects: Herpes zoster, cytopenias, elevated lipids, venous thromboembolism
- Convenient oral administration
BTK Inhibitors:
- In late-stage development
- Target B-cell signaling pathways
- Examples: Evobrutinib, fenebrutinib
Biosimilars:
- Lower-cost alternatives to original biologic agents
- Available for most TNF inhibitors, rituximab
- Similar efficacy and safety to reference products
- Important for improving access and reducing costs
Treatment Strategies
Initial Treatment Approaches:
- Monotherapy: Usually methotrexate as first-line
- Step-up combination: Adding medications if response inadequate
- Initial combination: Starting with multiple DMARDs for high-risk patients
- Induction-maintenance: Intensive early therapy with step-down after response
Treatment Algorithms (based on ACR and EULAR guidelines):
- Methotrexate monotherapy (with short-term low-dose glucocorticoids)
- If inadequate response after 3-6 months:
- Add second csDMARD (triple therapy), OR
- Add bDMARD (typically TNF inhibitor), OR
- Add JAK inhibitor
- If inadequate response to first targeted therapy:
- Switch mechanism of action (different class of bDMARD or tsDMARD)
- Consider IL-6 inhibitor or JAK inhibitor if TNF-IR
Special Considerations:
- Elderly patients: Greater emphasis on safety profile
- Pregnancy planning: Hydroxychloroquine, sulfasalazine, certolizumab safest
- Comorbidities: Guide treatment selection
- Heart failure: Avoid TNF inhibitors
- Interstitial lung disease: Caution with methotrexate
- History of cancer: Consider abatacept or rituximab
- Recurrent infections: Abatacept may be preferred
- Demyelinating disorders: Avoid TNF inhibitors
- Prior tuberculosis: Rituximab or abatacept safer than TNF inhibitors
Glucocorticoid Use:
- Short-term bridging while waiting for DMARD effect
- Intra-articular for persistent synovitis in a few joints
- Lowest effective dose for shortest time possible
- Bone protection if prolonged use necessary
- Careful tapering to avoid flares
Surgical Interventions
Joint Preservation Procedures:
- Synovectomy (removal of inflamed synovium)
- Tenosynovectomy for tendon inflammation
- Tendon repairs or transfers
- Removal of rheumatoid nodules
- Joint debridement
Reconstructive Procedures:
- Joint replacements (arthroplasty): Most commonly hip, knee, shoulder, elbow
- Wrist fusion or replacement
- Metacarpophalangeal joint replacement
- Small joint fusions of hands and feet
- Cervical spine fusion for instability
Preventive Orthopedic Interventions:
- Carpal tunnel release
- Tendon realignment
- Boutonnière and swan-neck deformity correction
- Forefoot reconstruction
Emerging Treatments and Clinical Trials
Novel Targeted Therapies:
- Dual JAK1/TYK2 inhibitors: Potentially improved safety profile
- Anti-GM-CSF antibodies: Mavrilimumab, otilimab
- Novel IL-6 pathway inhibitors: Direct IL-6 targeting
- Proteasome inhibitors: Ixazomib
- Newer B-cell targeting: Anti-BAFF, anti-BCMA
Immunomodulatory Approaches:
- Regulatory T-cell expansion: Low-dose IL-2 therapy
- Tolerogenic dendritic cell therapy: Restoring immunological tolerance
- Cellular therapies: Mesenchymal stem cells, CAR-Treg cells
- Vagus nerve stimulation: Neuroimmune modulation
- Microbiome-based interventions: FMT, bacterial consortia
Combination Approaches:
- Combining biologics targeting different pathways
- Biologics combined with JAK inhibitors
- “Induction-maintenance” strategies with drug tapering
- Precision medicine approaches based on biomarkers
Treatment Reduction Strategies:
- Drug tapering in sustained remission
- Spacing biologic intervals
- Predicting successful drug reduction
- Defining optimal reduction protocols
The treatment landscape for RA has been transformed over the past two decades, with an expanding array of therapeutic options allowing more personalized approaches. The paradigm has shifted from accepting moderate disease control to expecting remission or low disease activity for most patients. Research continues to focus on developing therapies with improved efficacy, safety, and convenience, as well as on strategies for treatment de-escalation and ultimately disease prevention.
9. Prevention & Precautionary Measures
Primary Prevention
Complete prevention of rheumatoid arthritis remains challenging due to its complex, multifactorial nature. However, several approaches may reduce risk in susceptible individuals:
Modifiable Risk Factor Intervention:
Smoking cessation: Strongest modifiable risk factor
- 35-50% of RA risk attributable to smoking in seropositive disease
- Benefits seen with smoking reduction even if unable to quit completely
- Public health campaigns targeting smoking may reduce population RA burden
Maintaining healthy weight:
- Obesity increases risk by 1.2-1.5 times
- Weight reduction may lower risk in obese individuals
- Particularly important for those with other risk factors
Dietary interventions:
- Mediterranean diet associated with reduced risk
- Higher omega-3 fatty acid intake potentially protective
- Moderate alcohol consumption may reduce risk slightly
- Antioxidant-rich diet possibly beneficial
Oral hygiene:
- Regular dental care to prevent periodontitis
- Treatment of established periodontal disease
- Particularly important in those with genetic risk factors
Pharmaceutical Prevention (experimental approaches):
- Hydroxychloroquine: Being studied for prevention in high-risk individuals
- Statins: Observational data suggest possible risk reduction
- Vitamin D supplementation: For deficient individuals, controversial benefit
- Probiotics: Microbiome modulation, still experimental
Environmental Exposure Reduction:
- Occupational safety measures for silica dust exposure
- Reducing exposure to industrial pollutants
- Avoiding textile dust exposure
- Minimizing exposure to airborne particulates
Secondary Prevention (Early Intervention)
Identifying and treating individuals in the earliest phases of disease:
Pre-clinical RA Detection:
- Screening high-risk individuals (first-degree relatives)
- Autoantibody testing in those with joint symptoms
- Genetic testing in research settings
- Biomarker panels under development
- Emerging role of ultrasound and MRI for subclinical synovitis
Intervention in “Pre-RA” States:
Undifferentiated arthritis:
- Brief methotrexate course may prevent progression to RA
- Short-term corticosteroids in some cases
- Close monitoring with treat-to-target approach if RA develops
ACPA-positive arthralgia:
- Emerging area of research
- Clinical trials evaluating rituximab, abatacept, hydroxychloroquine
- Lifestyle modifications (smoking cessation, weight management)
- Regular monitoring for development of clinical arthritis
Early Intervention Strategies:
- “Window of opportunity” concept
- Treatment within 12 weeks of symptom onset ideal
- Early referral pathways from primary care
- Early arthritis clinics for rapid assessment
- Early, aggressive therapy to prevent joint damage
Precautionary Measures for Diagnosed RA
Once RA is diagnosed, preventing complications becomes crucial:
Infection Prevention:
Vaccination recommendations:
- Pneumococcal vaccines (PCV13 and PPSV23)
- Annual influenza vaccination
- Hepatitis B for at-risk individuals
- Herpes zoster vaccine (recombinant) particularly for those on JAK inhibitors
- COVID-19 vaccination
- Timing vaccinations before starting immunosuppressive therapy when possible
General infection prevention measures:
- Hand hygiene
- Avoiding high-risk exposures
- Prompt treatment of infections
- Tuberculosis screening before biologic therapy
- Temporary treatment interruption during serious infections
Cardiovascular Risk Management:
- Regular cardiovascular risk assessment
- Aggressive management of traditional risk factors:
- Hypertension
- Dyslipidemia
- Diabetes
- Smoking cessation
- Regular exercise within capabilities
- Consider statin therapy at lower thresholds than general population
- Effective RA treatment may itself reduce cardiovascular risk
Bone Health Protection:
- Bone density screening
- Adequate calcium and vitamin D intake
- Weight-bearing exercise when possible
- Minimizing corticosteroid exposure
- Bisphosphonates or other osteoporosis therapies when indicated
- Fall prevention strategies
Cancer Screening:
- Age-appropriate cancer screening
- Heightened vigilance for lymphoma signs
- Skin examinations for patients on biologics
- Potential role for lung cancer screening in long-standing RA
Lifestyle Measures
Exercise Recommendations:
- Regular, moderate exercise tailored to capabilities
- Combination of:
- Range-of-motion exercises
- Strengthening exercises
- Low-impact aerobic activity
- Aquatic exercise often well-tolerated
- Balance exercises to prevent falls
- Working with physical therapist to develop appropriate program
Dietary Considerations:
- Mediterranean diet pattern (fruits, vegetables, whole grains, fish, olive oil)
- Adequate protein intake to prevent muscle loss
- Omega-3 fatty acids (fish oil) may have modest benefits
- Maintain healthy weight
- Limited evidence for elimination diets
- Alcohol moderation
- Adequate hydration
Joint Protection Strategies:
- Ergonomic principles at home and work
- Using largest joints for heavy tasks
- Balancing activity and rest
- Assistive devices when needed
- Proper body mechanics
- Splinting acutely inflamed joints
Stress Management:
- Mindfulness-based stress reduction
- Regular relaxation techniques
- Adequate sleep hygiene
- Cognitive behavioral therapy
- Appropriate pacing of activities
Functional Optimization:
- Workplace accommodations
- Home modifications
- Energy conservation techniques
- Assistive technology
- Maintaining social engagement
- Regular reassessment of functional needs
Future Directions in Prevention
Precision Prevention:
- Genetic risk profiling
- Biomarker-guided preventive strategies
- Targeted interventions based on RA subtype
- Personalized risk assessment tools
Novel Preventive Approaches in Development:
- Tolerization therapies targeting specific autoantigens
- Microbiome modification approaches
- Mucosal tolerance induction
- Antigen-specific regulatory T-cell induction
- Targeted anti-citrullination strategies
Research Initiatives:
- PRAIRI study (Prevention of RA by Rituximab)
- STAPRA study (Statins to Prevent RA)
- TREAT EARLIER study (abatacept in at-risk individuals)
- APIPPRA trial (abatacept in pre-clinical RA)
- Stop-RA study (hydroxychloroquine for prevention)
While complete primary prevention of RA remains elusive, the combination of risk factor modification, early detection, and prompt intervention offers the best current approach to preventing disease development and progression. The evolution from treating established disease to intervening in pre-clinical phases represents a paradigm shift toward potentially preventing RA before irreversible damage occurs.
10. Global & Regional Statistics
Global Incidence and Prevalence
Worldwide Prevalence:
- Global prevalence estimate: 0.5-1% of adult population
- Approximately 14-16 million people affected worldwide
- Higher prevalence in developed countries
- Variation by region, ethnicity, and urbanization
- Increasing prevalence with aging global population
Incidence Rates:
- Global annual incidence: 20-50 new cases per 100,000 population
- Women: 24-60 per 100,000 person-years
- Men: 12-30 per 100,000 person-years
- Peaks in women aged 55-64 years
- Stabilizing or slightly declining in some developed regions
- Rising in some developing countries with urbanization
Demographic Patterns:
- Female-to-male ratio: 2-3:1 overall
- Narrower sex difference in elderly-onset RA (closer to 1:1)
- Juvenile idiopathic arthritis: approximately 1 in 1,000 children
- Mean age of onset decreasing in some regions
- Lifetime risk: approximately 3.6% for women, 1.7% for men
Regional Variations and Comparisons
North America:
United States:
- Prevalence: 0.5-1.0% (1.3-2.6 million people)
- Annual incidence: 40-50 per 100,000
- Higher rates in Native American populations (5-7%)
- Navajo, Pima, and Chippewa tribes have highest documented prevalence globally
- Annual direct costs: $12,000-$18,000 per patient
- Total economic burden: $19-39 billion annually
Canada:
- Prevalence: 0.4-0.9%
- Higher rates in Indigenous populations
- Increasing prevalence in northern territories
- Universal healthcare provides more equitable access to biologics
Europe:
Northern Europe:
- Prevalence: 0.5-1.0%
- Highest rates in Scandinavian countries
- Finland: 0.8% prevalence
- Sweden: 0.7% prevalence
- Strong research infrastructure and registries
Southern Europe:
- Lower prevalence: 0.3-0.7%
- Italy: 0.4% prevalence
- Spain: 0.5% prevalence
- Mediterranean diet potentially protective
Eastern Europe:
- Intermediate prevalence: 0.4-0.8%
- Less access to biologic therapies
- Higher disability rates due to treatment disparities
- Growing efforts to improve early diagnosis
Asia:
East Asia:
- Generally lower prevalence: 0.2-0.3%
- Japan: 0.3% prevalence
- China: 0.2-0.4% prevalence, with urban-rural gradient
- South Korea: 0.2-0.3% prevalence
- Increasing rates with westernization and urbanization
South Asia:
- India: 0.2-0.4% prevalence
- Pakistan: 0.1-0.3% prevalence
- Bangladesh: 0.2-0.3% prevalence
- Significant urban-rural disparities in diagnosis and treatment
- Limited access to advanced therapies
Middle East:
- Turkey: 0.5% prevalence
- Iran: 0.3-0.4% prevalence
- Saudi Arabia: 0.2-0.3% prevalence
- Emerging data showing similar rates to Western countries when adjusted for age
Latin America:
- Brazil: 0.4-0.5% prevalence
- Mexico: 0.3-0.4% prevalence
- Argentina: 0.4-0.6% prevalence
- Significant socioeconomic disparities in treatment access
- Growing recognition of disease burden
Africa:
- Limited epidemiological data
- South Africa: 0.1-0.3% prevalence
- Nigeria: 0.1-0.2% prevalence
- Rural areas: 0.1% or lower
- Urban areas showing increasing prevalence
- Substantially underdiagnosed
- Very limited access to biologic therapies
- Competing health priorities (infectious diseases, malnutrition)
Australia and New Zealand:
- Australia: 0.5-0.7% prevalence
- New Zealand: 0.5-0.8% prevalence
- Higher rates in Māori population
- Excellent access to advanced therapies
- Strong patient registries
Mortality and Survival Rates
Overall Mortality Impact:
- Standardized mortality ratio: 1.5-2.0 (improved with modern treatments)
- Life expectancy reduction: 3-10 years historically
- Now closer to 3-5 years with modern treatment
- Mortality gap narrowing in countries with early access to biologics
- Cardiovascular disease accounts for 30-50% of excess mortality
- Infections account for 20-25% of excess mortality
- Treatment advances improving survival rates over past 20 years
Regional Mortality Variations:
High-income countries:
- Declining excess mortality
- SMR approaching 1.2-1.5 with optimal treatment
- Mortality primarily from cardiovascular complications
- Early diagnosis and treatment significantly improving outcomes
Middle-income countries:
- SMR typically 1.5-2.5
- More deaths from infections and untreated complications
- Improving with greater treatment access
- Significant disparities based on healthcare access
Low-income countries:
- Limited survival data
- Estimated SMR 2.0-3.0
- Higher rates of work disability and complications
- Minimal access to biologic therapies
- Lower life expectancy overall compounds impact
Temporal Trends:
- Improving survival rates since 1990s
- Greatest mortality improvements coinciding with biologic era (post-2000)
- Early aggressive treatment strategies reducing long-term complications
- Cardiovascular risk management improving outcomes
- Infection prevention strategies reducing mortality
- Comorbidity management increasingly recognized as important
Economic Impact and Healthcare Burden
Direct Medical Costs:
United States: $12,000-$18,000 per patient annually
- Biologic therapies account for 30-50% of costs
- Hospitalization costs declining with better outpatient management
- Total direct medical costs: $8-10 billion annually
European Union: €4,000-€12,000 per patient annually
- National healthcare systems providing broader access to therapies
- Significant variations between Eastern and Western Europe
- Total EU direct costs: €6-8 billion annually
Asia: Highly variable
- Japan: $5,000-$8,000 per patient annually
- China: $2,000-$5,000 per patient annually in urban centers
- India: $500-$2,000 per patient annually
- Limited access to biologics in many regions
Indirect Costs:
- Often exceed direct medical costs
- Work disability costs: $6,000-$25,000 per patient annually
- Productivity loss from presenteeism (working while ill)
- Early retirement costs
- Caregiver burden and costs
- Globally estimated at $25-35 billion annually
Work Disability Impact:
- Historical data: 50% work disability at 10 years
- Current rates with modern treatment: 20-35% at 10 years
- Regional variations:
- Lowest in Scandinavian countries with early biologic access
- Highest in regions with delayed diagnosis and limited treatment
- Significant socioeconomic disparities within countries
- Early aggressive treatment significantly reduces work disability
Healthcare Utilization:
- Specialist visits: 4-8 annually in well-managed healthcare systems
- Primary care visits: 6-12 annually
- Hospitalizations decreasing with modern outpatient management
- Emergency department visits: Higher in regions with poor access to ongoing care
- Annual monitoring tests: Blood work, radiographs, occasionally ultrasound/MRI
Treatment Accessibility:
- Biologic therapy access:
- North America, Western Europe, Australia: 30-40% of patients
- Eastern Europe, Latin America: 10-30% of patients
- Asia (variable): 5-25% of patients
- Africa: <5% of patients
- Biosimilar impact:
- Increasing access in middle-income countries
- Cost reductions of 25-70% compared to originators
- Expanded eligibility criteria in some healthcare systems
- Treatment delays:
- High-income: 6-12 month average diagnostic delay
- Middle-income: 1-2 year diagnostic delay
- Low-income: 2-5 year diagnostic delay
These global and regional statistics highlight the significant worldwide burden of rheumatoid arthritis, with pronounced disparities in prevalence, outcomes, and treatment access. Encouraging trends include narrowing mortality gaps with modern treatments and expanding access to advanced therapies through biosimilars and evolving healthcare policies. However, substantial work remains to address inequities in diagnosis and treatment, particularly in resource-limited settings.
11. Recent Research & Future Prospects
Latest Advances in Understanding RA Pathogenesis
Genetic and Genomic Insights:
- Single-cell RNA sequencing: Identifying specific cellular subsets driving disease
- Multi-omics approaches: Integrating genomics, proteomics, metabolomics
- Epigenetic modifications: DNA methylation, histone modifications, and microRNAs
- Genetic risk score development: Combining multiple risk alleles for prediction
- Pharmacogenomics: Genetic predictors of treatment response
- Trans-ancestry genetic studies: Understanding ethnic variations in disease
Immunological Advances:
- Citrullination mechanisms: Better understanding of protein modification and autoimmunity
- Innate immune system role: Beyond adaptive immunity focus
- IL-23/IL-17 axis: Potential therapeutic target
- Tissue-resident memory T cells: Persistence in synovium driving chronicity
- Stromal cell biology: Fibroblast heterogeneity and pathogenic subsets
- B-cell autoimmunity: Beyond antibody production to antigen presentation
- Myeloid cell plasticity: Macrophage polarization and dendritic cell subsets
- Trained immunity concepts: Innate immune memory contributing to chronicity
Microbiome Research:
- Gut-joint axis: Communication between intestinal and synovial inflammation
- Specific microbial signatures: Prevotella copri and other species associations
- Periodontal microbiome: Porphyromonas gingivalis and protein citrullination
- Lung microbiome alterations: Particularly in smokers at risk for RA
- Microbial metabolites: Short-chain fatty acids and immune regulation
- Fecal microbiota transplant studies: Emerging experimental approaches
Tissue Biology Insights:
- Synovial tissue analysis: Technology advances enabling detailed characterization
- Synovial biopsy standardization: Enabling broader research applications
- Fibroblast heterogeneity: Identification of pathogenic NOTCH3+ fibroblasts
- Neuro-immune interactions: Neural regulation of joint inflammation
- Vascular changes: Angiogenesis and lymphangiogenesis in synovium
- Pain mechanisms: Beyond inflammatory pain to central sensitization
Current Cutting-Edge Treatment Research
Novel Biologic Approaches:
- Dual cytokine inhibition: Bispecific antibodies targeting multiple pathways
- IL-23 pathway targeting: Successful in psoriatic arthritis, being evaluated in RA
- GM-CSF inhibition: Mavrilimumab, otilimab, and namilumab in development
- Anti-CD19 therapy: Alternative to CD20-targeted B-cell depletion
- Anti-BAFF/APRIL targeted therapy: Atacicept and other agents
- Anti-interferons: Anifrolumab and other type I interferon blocking agents
- IL-17 pathway inhibitors: Reassessment in specific RA subsets
Small Molecule Advances:
- JAK inhibitor refinement:
- Selective JAK1 inhibitors: Filgotinib, upadacitinib
- JAK3 selective approaches
- Novel dosing strategies
- Extended release formulations
- Non-systemic JAK inhibitors
- BTK inhibitors: Targeting B-cell receptor signaling pathway
- PI3K inhibitors: Cell signaling modulators
- TYK2 inhibitors: Potential improved safety profile
- RORγt inhibitors: Blocking Th17 cell development
- IRAK4 inhibitors: Targeting innate immune signaling
Cellular Therapies:
- CAR-T regulatory cells: Engineered cells targeting inflammation
- Mesenchymal stem cells: Anti-inflammatory and tissue repair properties
- Tolerogenic dendritic cells: Restoring immune tolerance
- Regulatory T-cell expansion: Low-dose IL-2 therapy
- Hematopoietic stem cell transplantation: For refractory cases
- Extracellular vesicles: Cell-free approach to cellular therapy
Precision Medicine Approaches:
- Biomarker-guided therapy selection:
- Synovial tissue biopsies to guide mechanism selection
- Blood-based biomarker panels
- Genetic predictors of response
- Multi-omics prediction models
- Pharmacomicrobiomics: Microbiome influence on drug metabolism
- Digital biomarkers: Wearable technology and remote monitoring
- Imaging to guide therapy: Ultrasound and MRI-directed treatment
- Artificial intelligence applications: Treatment selection algorithms
Future Research Directions
Preventive Approaches:
- Pre-RA intervention: Trials in high-risk ACPA-positive individuals
- Mucosal tolerance induction: Nasal, oral, or respiratory antigen exposure
- Antigen-specific tolerization: Targeted immune regulation
- Microbiome manipulation: Probiotics, prebiotics, or fecal transplantation
- Primary prevention strategies: Risk factor modification in high-risk groups
- Lifestyle intervention programs: Diet, exercise, smoking cessation
Drug Development Approaches:
- Disease phenotype-specific therapies: Treatments for RA subtypes
- Organ-specific delivery systems: Joint-targeted therapies
- Novel formulations: Extended release, implantable devices
- Combination approaches: Rational combinations of targeted therapies
- Sequential therapy protocols: Induction and maintenance strategies
- Biosimilar expansion: Increasing access to biologic therapies
- Nanotechnology applications: Enhanced drug delivery
Remission and Cure Research:
- Drug-free remission: Identifying patients who can discontinue therapy
- Induction of immunological tolerance: Fundamental disease modification
- Predictive models for sustained remission: Biomarkers of deep remission
- Tapering strategies: Systematic approaches to treatment reduction
- Maintenance of remission approaches: Low-dose or intermittent therapy
- Defining “cure” in RA: Biological vs. symptomatic remission
Addressing Challenges and Unmet Needs:
- Refractory RA management: Options for treatment-resistant patients
- Pain mechanisms beyond inflammation: Central sensitization approaches
- Fatigue management: Addressing persistent fatigue despite inflammation control
- Comorbidity management: Integrative approaches to RA and associated conditions
- Extra-articular manifestations: Targeted approaches for systemic features
- Health disparities: Improving access to advanced therapies globally
- Treatment simplification: Reducing burden of complex regimens
Potential Breakthrough Therapies in Development
Disease-Modifying Potential:
- Proteasome inhibitors: Borrowed from oncology, showing immunomodulatory effects
- Plasma cell targeting agents: Depleting long-lived antibody-producing cells
- Tissue-resident memory T-cell modulators: Addressing persistence of autoimmunity
- Synovial fibroblast-targeted therapies: Addressing invasive behavior
- Epigenetic modifiers: Altering gene expression patterns
- Microbiome-based therapeutics: Defined bacterial consortia
- Nanoparticle-based antigen-specific immunotherapy: Targeting specific autoreactive cells
Technological Innovations:
- Gene therapy approaches: Targeted genetic modifications
- CRISPR-based therapies: Gene editing for autoimmunity
- RNA therapeutics: siRNA and antisense oligonucleotides
- 3D bioprinting: For joint tissue engineering and replacement
- Closed-loop drug delivery systems: Responsive to inflammatory markers
- Digital therapeutics: App-based behavioral interventions
- Virtual reality applications: For pain management and rehabilitation
Near-Term Clinical Advances:
- Dual JAK1/TYK2 inhibitors: Potentially improved safety profile
- IL-6 trans-signaling inhibitors: More specific IL-6 pathway blockade
- Subcutaneous formulations: Of previously intravenous-only drugs
- Oral TNF inhibitors: Early development stages
- Extended-interval dosing: Reducing treatment burden
- Combination biologic therapy protocols: Currently in trials
- Predictive biomarkers of response: Entering clinical practice
The landscape of rheumatoid arthritis research is evolving rapidly, with significant advances in understanding disease pathogenesis translating into novel therapeutic approaches. The paradigm is shifting from symptom control to disease modification, with emerging focus on prevention, precision medicine, and potentially cure. While challenges remain, particularly in addressing disease heterogeneity and treatment resistance, the future holds promise for continued improvements in outcomes for patients with rheumatoid arthritis.
12. Interesting Facts & Lesser-Known Insights
Historical and Cultural Perspectives
Ancient Evidence and Descriptions:
- Skeletal remains showing RA-like changes date back to 4500 BCE in North America
- Certain Native American tribes have dramatically higher rates (5-7%) compared to global averages
- Emperor Constantine the Great (272-337 CE) may have had RA based on descriptions of his hands
- RA appears in European art from the 1400s onwards in paintings depicting joint deformities
- “The Three Graces” by Peter Paul Rubens (1639) potentially shows RA hand deformities
- Historical treatments included bloodletting, gold injections, and even bee venom therapy
Linguistic and Cultural Aspects:
- The term “rheumatoid arthritis” was coined by Sir Alfred Baring Garrod in 1858
- Previously called “primary asthenic gout” by Landré-Beauvais in 1800
- Descriptions matching RA exist in ancient Indian Ayurvedic texts as “Aamavata”
- Traditional Chinese medicine described a similar condition called “Bi syndrome”
- Many indigenous cultures attributed inflammatory arthritis to spiritual causes
Famous Individuals with RA:
- Pierre-Auguste Renoir continued painting despite severe RA, adapting his technique with brushes strapped to his hands
- Raoul Dufy, another French painter, was one of the first patients treated with cortisone for RA in 1950
- Lucille Ball struggled with RA that began in her teenage years
- Kathleen Turner’s acting career was significantly impacted by RA
- Glenn Frey of the Eagles died from complications of RA and its treatments
- Billy Bowden, cricket umpire, developed his distinctive signaling style due to RA limitations
Scientific Curiosities
Unusual Disease Patterns:
- “Palindromic rheumatism”: Recurrent, acute episodes of arthritis that resolve completely between attacks; 30-50% eventually develop classical RA
- “Rheumatoid nodulosis”: Development of rheumatoid nodules with minimal joint involvement
- “Lipstick sign”: Inability to apply lipstick due to hand deformities was historically used as a functional assessment
- “Bamboo spine”: Occasionally seen in RA despite being more characteristic of ankylosing spondylitis
- “Jaccoud’s arthropathy”: Deformities resembling RA but without erosions, historically associated with rheumatic fever
Biological Curiosities:
- RA virtually disappeared in famine conditions during World War II in European countries, only to return afterward
- Women often experience dramatic improvement during pregnancy, with 75% experiencing remission by the third trimester
- Postpartum flares occur in 90% of women who improve during pregnancy
- Smokers with RA have poorer response to treatments, particularly biologics
- Left-handed individuals may display different joint involvement patterns than right-handed people
- Identical twins have only 15-30% concordance for RA despite identical genetics
Geographic and Environmental Oddities:
- Prevalence decreases closer to the equator and increases with distance north or south
- The Yakima Indians of North America have the highest documented prevalence globally (~7%)
- RA is rare in rural Africa but increases with urbanization
- Higher altitude living is associated with lower RA prevalence in some studies
- Some evidence suggests RA was rare or nonexistent in the Americas before European contact
- RA rates increase in countries adopting Western lifestyles and diets
Lesser-Known Clinical Insights
Diagnostic Pearls:
- “Squeeze test”: Pain on squeezing across the MCP joints is a simple, sensitive early sign
- Morning stiffness duration correlates with inflammatory activity better than pain levels
- The 2nd and 3rd MCP joints are most commonly involved first
- Anti-CCP antibodies can precede clinical symptoms by up to 10-14 years
- “Hidden” rheumatoid nodules in unusual locations (vocal cords, heart valves, vertebrae)
- Pulmonary involvement can sometimes precede joint symptoms by months or years
Treatment Nuances:
- Low-dose methotrexate works through anti-inflammatory mechanisms, not as a cytotoxic agent
- Weekly, not daily, methotrexate dosing is crucial for safety (medication errors are common)
- Folic acid supplementation prevents methotrexate side effects without reducing efficacy
- Conventional DMARDs take 2-3 months to show full effect, not weeks
- Subcutaneous methotrexate has 20-30% higher bioavailability than oral tablets
- Specific antibodies against biologics (anti-drug antibodies) can develop, reducing efficacy
Prognostic Indicators:
- Smokers have worse prognosis regardless of treatment
- Early erosions in the feet often occur before hand erosions but may be asymptomatic
- High-positive RF/anti-CCP, erosions at onset, and many swollen joints predict aggressive disease
- The first 2 years of disease represent a “window of opportunity” for best long-term outcomes
- “Serological remission” (normalization of antibody levels) rarely occurs despite clinical remission
- Women have higher disease activity scores but potentially better long-term outcomes
Myths and Misconceptions
Common Misunderstandings:
Myth: RA is just “wear and tear” arthritis Fact: RA is an autoimmune disease fundamentally different from osteoarthritis
Myth: RA only affects the joints Fact: RA is a systemic disease affecting multiple organ systems
Myth: RA is a disease of the elderly Fact: RA can occur at any age, with peak onset between 30-60 years
Myth: RA is caused by poor diet or “acidic foods” Fact: RA has complex genetic and environmental causes, not directly related to diet
Myth: Exercise worsens RA and joints need rest Fact: Appropriate exercise is beneficial and recommended for RA
Myth: Cold, damp weather causes RA Fact: Weather doesn’t cause RA but may affect symptoms in established disease
Myth: All RA patients eventually end up in wheelchairs Fact: Modern treatments have dramatically improved outcomes
Myth: RA medications are more dangerous than the disease Fact: Untreated RA carries greater risks than the side effects of most medications
Myth: Pregnancy causes RA Fact: Pregnancy typically improves RA symptoms; postpartum period increases risk
Myth: RA can be cured with special diets or supplements Fact: While diet may influence symptoms, no diet has been proven to cure RA
Practical Insights for Daily Living
Adaptive Techniques:
- “Joint protection” techniques can reduce pain and preserve function
- Specially designed assistive devices can maintain independence
- Fatigue management often requires scheduled rest periods (“energy banking”)
- Hand exercises in warm water can reduce morning stiffness
- Preparation for “flare days” with pre-cooked meals and simplified routines
- Compression gloves worn at night may reduce morning symptoms
- Voice recognition software for those with hand limitations
- Lever door handles instead of knobs require less grip strength
- Electric can openers, jar openers, and button hooks preserve independence
- Sitting to perform tasks when possible conserves energy

