
⚠️ Disclaimer: The information provided in this article is for educational purposes only and does not constitute medical advice. RevisionTown does not provide diagnosis, treatment, or medical recommendations. Always consult a qualified healthcare professional regarding any medical condition, symptoms, or concerns.
Read More – 🏥 Medical Disclaimer
Hypertrophic Cardiomyopathy (HCM): A Comprehensive Report
1. Overview
What is HCM?
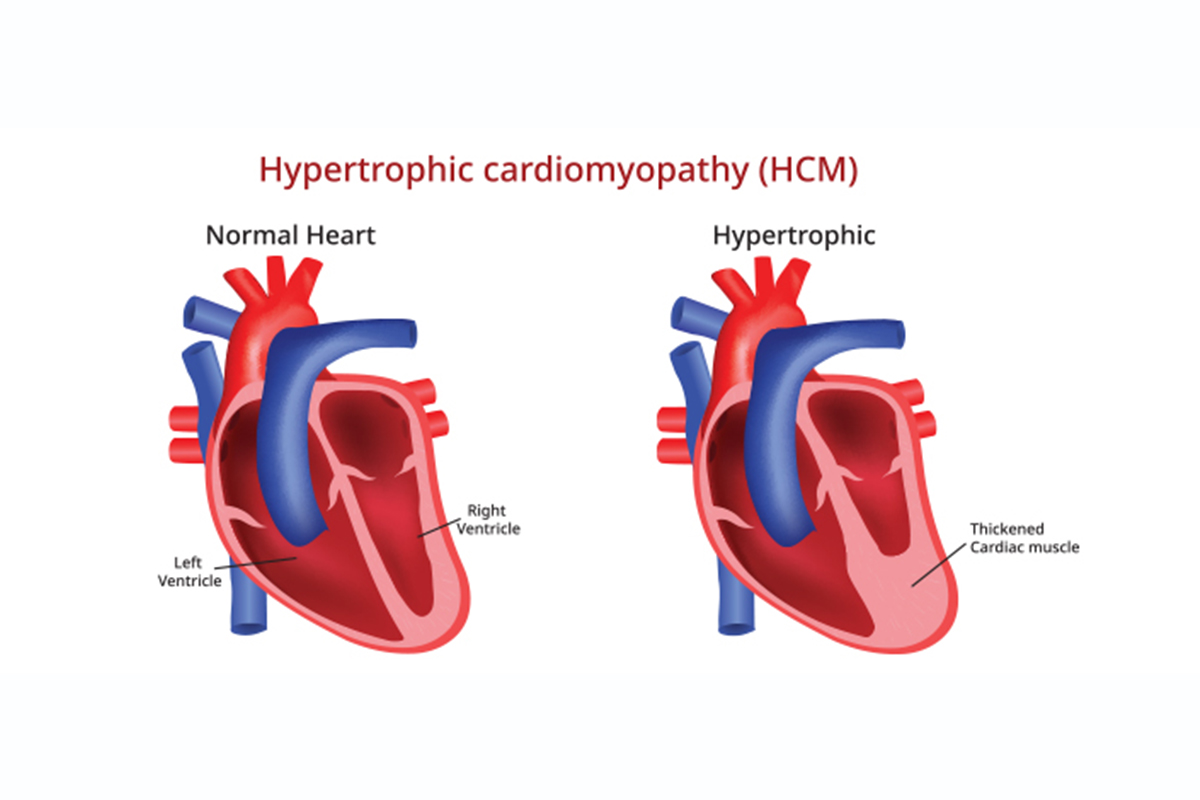
Hypertrophic Cardiomyopathy (HCM) is a complex genetic cardiovascular disease primarily characterized by an abnormal thickening (hypertrophy) of the heart muscle, specifically the left ventricle. This thickening occurs without an obvious cause, such as high blood pressure or valve disease, and develops due to genetic mutations that affect cardiac muscle proteins. The disease often involves asymmetric septal hypertrophy, where the interventricular septum becomes disproportionately thickened compared to other parts of the heart. This can potentially obstruct blood flow from the left ventricle to the aorta, a condition known as obstructive hypertrophic cardiomyopathy (HOCM).
A concise yet detailed definition
Hypertrophic Cardiomyopathy is an inherited primary myocardial disorder defined by left ventricular hypertrophy (wall thickness ≥15 mm in adults or the equivalent relative to body surface area in children) that occurs in the absence of abnormal loading conditions sufficient to explain the observed degree of hypertrophy. It is characterized by myocyte hypertrophy, disarray, and interstitial fibrosis, which create an arrhythmogenic substrate and impaired cardiac function. HCM has variable clinical expression, complex pathophysiology, and diverse outcomes ranging from asymptomatic longevity to progressive heart failure, stroke, and sudden cardiac death.
The affected body parts/organs
HCM primarily affects the heart, with several specific structures and functions being impacted:
Left Ventricle:
- Ventricular wall thickening (most commonly the septum)
- Reduced chamber size (cavity dimensions)
- Impaired filling (diastolic dysfunction)
- Potential dynamic outflow tract obstruction
Myocardium (Heart Muscle):
- Myocyte enlargement and disarray
- Interstitial and replacement fibrosis
- Microvascular dysfunction and ischemia
- Altered energy metabolism
Mitral Valve Apparatus:
- Systolic anterior motion (SAM) of the mitral valve
- Secondary mitral regurgitation
- Elongated mitral valve leaflets (in some cases)
- Abnormal papillary muscle architecture
Coronary Arteries:
- Intramural coronary arteriole remodeling
- Microvascular dysfunction
- Reduced coronary flow reserve
- Myocardial perfusion abnormalities
Conduction System:
- Disruption of normal electrical pathways
- Substrate for ventricular and atrial arrhythmias
- Potential for heart block or conduction delays
- Enhanced arrhythmogenic potential
Secondary Involvement:
- Right ventricle (in some cases)
- Atrial enlargement (particularly left atrium)
- Pulmonary vasculature (secondary pulmonary hypertension)
- Systemic effects from heart failure
Prevalence and significance of the disease
Hypertrophic Cardiomyopathy is the most common inherited cardiac disease, with significant global impact:
Prevalence:
- General population prevalence: 1 in 200 to 1 in 500 individuals (0.2-0.5%)
- Approximately 20 million people affected worldwide
- Present across all racial and ethnic groups
- Often underdiagnosed, particularly in certain populations and regions
- Higher recognition in developed countries with advanced cardiac imaging
Age and Gender Distribution:
- Can manifest at any age, from infancy to late adulthood
- Classical presentation often in young adulthood (teens to 40s)
- Male predominance in clinical diagnosis (3:2 ratio)
- Delayed diagnosis in women (often misdiagnosed with anxiety or other conditions)
- Age-related penetrance of genetic variants
Clinical Significance:
- Leading cause of sudden cardiac death in young people and athletes
- Accounts for approximately 5-15% of sudden cardiac deaths in young athletes
- Major cause of heart failure with preserved ejection fraction
- Significant contributor to stroke and atrial fibrillation in younger patients
- Source of substantial healthcare utilization and economic burden
- Psychological impact due to exercise limitations and sudden death risk
- Hereditary implications affecting multiple family members
- Important consideration in pre-participation sports screening
Mortality and Morbidity:
- Annual mortality rate: 0.5-1% in contemporary treated cohorts
- Sudden cardiac death risk: 0.2-0.8% per year in adults with HCM
- 5-year survival rate with modern management: >95%
- Substantial morbidity from symptoms, arrhythmias, and heart failure
- Reduced quality of life in symptomatic patients
- Progressive disease course in approximately 10-15% of patients
2. History & Discoveries
When and how was HCM first identified?
The identification and understanding of Hypertrophic Cardiomyopathy evolved gradually over time:
Early Observations (19th Century):
- 1869: Henri Liouville published the first documented case of asymmetric septal hypertrophy in a young woman who died suddenly
- 1895: Henri Huchard noted association between left ventricular hypertrophy and sudden death in young adults
- 1907: Schmincke described myocardial disarray (a hallmark microscopic finding) in autopsy specimens
Mid-20th Century Recognition:
- 1949: T.J. Evans described the combination of massive ventricular hypertrophy and sudden death
- 1957: Sir Russell Brock identified “functional obstruction of the left ventricle” as a distinct entity
- 1958: Donald Teare published his landmark paper describing asymmetrical hypertrophy in young adults who died suddenly
- 1959: Coining of the term “Idiopathic Hypertrophic Subaortic Stenosis” (IHSS)
Comprehensive Clinical Description:
- 1960-1965: Braunwald, Morrow, and colleagues at the NIH defined the hemodynamic, clinical, and pathological features
- 1961: First hemodynamic characterization of the obstruction with provocative maneuvers
- 1964: First formal echocardiographic descriptions
- 1969: Recognition as a disease of the sarcomere following familial studies
Modern Era:
- 1975: Adoption of the term “Hypertrophic Cardiomyopathy” by the World Health Organization
- 1978: First documentation of non-obstructive forms having clinical significance
- 1980s: Recognition of the disease as a primary disorder of the myocardium
- 1990: First genetic mutation identified as causative for HCM
Who discovered it?
While many clinicians and scientists contributed to the understanding of HCM, several key figures played pivotal roles:
Donald Teare (1911-1979):
- British forensic pathologist widely credited with the first modern description of HCM
- Published the landmark paper in 1958 in the British Heart Journal titled “Asymmetrical Hypertrophy of the Heart in Young Adults”
- His observations came from autopsy findings in eight patients who had died suddenly
- Recognized the characteristic asymmetric septal hypertrophy and myocardial fiber disarray
Eugene Braunwald, Andrew Glenn Morrow, and colleagues:
- Led groundbreaking research at the National Institutes of Health (NIH) in the late 1950s and 1960s
- Established the hemodynamic, clinical, and therapeutic foundations of HCM
- Morrow developed the first surgical treatment (myectomy) for obstruction
- Braunwald documented the dynamic nature of the obstruction and its response to various interventions
John Goodwin and colleagues (UK):
- Characterized the diverse clinical and hemodynamic manifestations
- Proposed the term “hypertrophic cardiomyopathy” to replace earlier terms like IHSS
- Demonstrated the familial nature of the disease
- Established the concept of primary cardiomyopathies as distinct clinical entities
French School:
- Pierre Soulie and colleagues described similar cases in the 1950s
- Used cardiac catheterization to document the pressure gradient
- Made important early observations about left ventricular outflow tract obstruction
Major discoveries and breakthroughs in its research and treatment
Genetic Discoveries:
- 1989-1990: First causative gene mutation (MYH7 encoding beta-myosin heavy chain) identified by Seidman and colleagues
- 1991-1995: Discovery of multiple sarcomere protein gene mutations
- 2000s: Recognition of non-sarcomere genes associated with HCM phenocopies
- 2010s: Development of comprehensive genetic testing panels
- 2015-present: Advances in genotype-phenotype correlations and modifier genes
Pathophysiological Understandings:
- 1970s: Characterization of myocardial disarray at microscopic level
- 1980s: Recognition of diastolic dysfunction as a key mechanism
- 1990s: Understanding of mitral valve dynamics and systolic anterior motion
- 2000s: Identification of microvascular dysfunction and myocardial fibrosis
- 2010s: Energy depletion hypothesis; recognition of metabolic abnormalities
Diagnostic Advances:
- 1970s: M-mode echocardiography for septal thickness measurement
- 1980s: 2D echocardiography for comprehensive assessment
- 1990s: Doppler echocardiography for outflow gradients and diastolic function
- 2000s: Cardiac MRI for tissue characterization and fibrosis detection
- 2010s: Strain imaging, 3D echocardiography, and multimodality approaches
Treatment Milestones:
- 1960s: First septal myectomy surgery by Morrow
- 1970s: Propranolol (beta-blocker) shown to reduce symptoms and obstruction
- 1980s: Dual-chamber pacing attempted for gradient reduction
- 1994: First alcohol septal ablation procedure (non-surgical septal reduction)
- 1996: First use of implantable defibrillators specifically for HCM
- 2000s: Refined risk stratification for sudden death
- 2020s: First targeted pharmacologic therapy (mavacamten) approved
Management Paradigms:
- 1980s: Recognition of exercise limitations for HCM patients
- 1990s: Development of specialized HCM centers of excellence
- 2000s: Family screening protocols established
- 2010s: Shared decision-making approach to ICD implantation
- 2020s: Precision medicine approaches based on genotype and phenotype
Evolution of medical understanding over time
Terminology and Definition:
- 1950s-1960s: Various terms including “Idiopathic Hypertrophic Subaortic Stenosis” (IHSS), “Asymmetric Septal Hypertrophy” (ASH), “Muscular Subaortic Stenosis”
- 1975: World Health Organization adopts “Hypertrophic Cardiomyopathy”
- 1980s: Focus on obstruction as the defining feature
- 1990s: Recognition as a genetic disease of the sarcomere
- 2000s: Emphasis on myocardial disorder beyond obstruction
- 2010s: Integration of genetics into definition and classification
- Present: Multimodality approach to diagnosis incorporating imaging and genetics
Pathophysiological Understanding:
- 1960s: Primary focus on left ventricular outflow tract obstruction
- 1970s: Recognition of myocardial disarray as a hallmark feature
- 1980s: Appreciation of diastolic dysfunction independent of obstruction
- 1990s: Understanding of mitral valve dynamics and contribution to obstruction
- 2000s: Recognition of microvascular dysfunction and ischemia
- 2010s: Emphasis on myocardial fibrosis as an arrhythmogenic substrate
- Present: Integrative model incorporating genetic, structural, functional, and metabolic abnormalities
Risk Stratification:
- 1960s-1970s: Limited to observed high-risk features like family history of sudden death
- 1980s: Identification of high-risk activities and environments
- 1990s: First formal risk factors identified (wall thickness, family history, syncope, non-sustained VT)
- 2000s: Development of algorithm-based approaches
- 2010s: Statistical models (HCM Risk-SCD) for individualizing risk prediction
- Present: Integration of advanced imaging markers and genetic information
Treatment Approach:
- 1960s: Primarily surgical with high morbidity and mortality
- 1970s-1980s: Introduction of medical therapy (beta-blockers, calcium channel blockers)
- 1990s: Development of less invasive interventions (alcohol septal ablation)
- 2000s: Preventive approach with ICDs and family screening
- 2010s: Refinement of selection criteria for various interventions
- Present: Targeted molecular therapies addressing specific disease mechanisms
Prognosis Perspective:
- 1960s: Viewed as a highly lethal condition with poor prognosis
- 1970s: Recognition of variable clinical course and outcomes
- 1980s: Documentation of patients with normal life expectancy
- 1990s: Appreciation of diverse phenotypic expressions and outcomes
- 2000s: Significant improvement in overall prognosis with contemporary management
- 2010s: Identification of specific high-risk and low-risk subgroups
- Present: Personalized prognostication based on phenotype, genotype, and biomarkers
3. Symptoms
Early symptoms vs. advanced-stage symptoms
Early Symptoms (Mild to Moderate Disease):
Cardiac-Related Symptoms:
- Exertional dyspnea (shortness of breath with activity): Often the earliest symptom, due to diastolic dysfunction and elevated filling pressures
- Decreased exercise tolerance: Inability to maintain previous exercise capacity without unusual fatigue
- Chest discomfort: Typically non-anginal, described as a pressure or heaviness, often related to exertion
- Palpitations: Awareness of irregular or forceful heartbeats, may indicate atrial or ventricular arrhythmias
- Pre-syncope: Lightheadedness or dizziness, particularly with exertion or postural changes
- Fatigue: Disproportionate to activity level, may be present even at rest
Subclinical Manifestations:
- Asymptomatic murmurs detected during routine examinations
- Abnormal ECG findings incidentally discovered
- Mild HCM detected during family screening
- Exercise intolerance attributed to poor conditioning
- Subtle arrhythmias detected during monitoring
- Mild hypotension during exercise testing
Advanced-Stage Symptoms (Severe Disease):
Progressive Heart Failure Symptoms:
- Orthopnea: Shortness of breath when lying flat
- Paroxysmal nocturnal dyspnea: Awakening at night gasping for breath
- Peripheral edema: Swelling of the legs and ankles
- Ascites: Fluid accumulation in the abdomen (in right-sided heart failure)
- Exercise intolerance: Severe limitation of physical activity
- Profound fatigue: Even with minimal exertion or at rest
Advanced Cardiac Sequelae:
- Frank syncope: Complete loss of consciousness, often with minimal or no warning
- Angina at rest: Chest pain occurring without exertion
- Persistent atrial fibrillation: Causing worsening heart failure and stroke risk
- Ventricular arrhythmias: Sustained ventricular tachycardia episodes
- Pulmonary hypertension symptoms: Right ventricular failure, hepatic congestion
- End-stage (“burnt-out”) phase: Dilated LV with systolic dysfunction and heart failure
Complications-Related Symptoms:
- Embolic events: Stroke or transient ischemic attack symptoms
- Pulmonary edema: Acute respiratory distress with frothy sputum
- Sudden cardiac death: Fatal arrhythmia (may be the first and only symptom in some cases)
- Cardiogenic shock: In severe obstruction or end-stage disease
- Infective endocarditis symptoms: Fever, malaise, new murmurs in susceptible patients
- Renal dysfunction symptoms: Due to cardiorenal syndrome
Common vs. rare symptoms
Common Symptoms (>20% of patients):
Exertional Limitations:
- Dyspnea on exertion (50-70%): The most frequent complaint
- Exercise intolerance (50-60%): Inability to perform usual activities
- Easy fatigability (40-50%): Disproportionate to level of exertion
- Post-exertional exhaustion (30-40%): Prolonged recovery after activity
Cardiac Awareness:
- Palpitations (30-40%): Awareness of forceful, rapid, or irregular heartbeats
- Chest discomfort (25-30%): Typically atypical, not classic angina
- Postural lightheadedness (20-30%): Particularly upon standing quickly
Non-Specific Symptoms:
- General fatigue (40-50%): Independent of physical exertion
- Anxiety related to cardiac awareness (25-35%)
- Sleep disturbances (20-30%): Including orthopnea or nocturnal dyspnea
Rare Symptoms (<10% of patients):
Neurological Manifestations:
- Syncope at rest (5-10%): Complete loss of consciousness without exertion
- Stroke as presenting symptom (3-5%): Due to atrial fibrillation or emboli
- Transient global amnesia (1-2%): Temporary memory loss episodes
- Seizure-like activity (1-3%): Due to cerebral hypoperfusion during arrhythmias
Gastrointestinal and Systemic Symptoms:
- Significant weight loss (3-5%): In advanced heart failure
- Ascites as initial presentation (2-4%): In right heart failure
- Hemoptysis (1-2%): Rare complication of severe pulmonary congestion
- Hoarseness (1-2%): Due to left atrial enlargement affecting the recurrent laryngeal nerve
- Platypnea-orthodeoxia (<1%): Breathlessness and oxygen desaturation when upright
Unusual Cardiac Presentations:
- Acute pulmonary edema without apparent trigger (3-5%)
- Sudden cardiac death as first manifestation (3-8%)
- Silent myocardial infarction pattern (2-4%): ECG changes without coronary disease
- Infective endocarditis (1-2%): Particularly affecting the mitral valve
- Systemic embolization (1-3%): To kidney, spleen, or extremities
- Right ventricular outflow tract obstruction (<1%)
How symptoms progress over time
Natural History of Symptom Progression:
Early Phase (Initial Diagnosis to 5 Years):
- Often stable symptoms with predictable triggers
- Episodic worsening with dehydration, excessive exertion, or environmental heat
- Gradual adaptation and limitation of activities to avoid symptoms
- Development of compensatory mechanisms and lifestyle modifications
- Symptoms often responsive to initial medical therapy
- Possible periods of symptom improvement with appropriate management
Mid-Term Evolution (5-15 Years):
- Gradual increase in symptom frequency and severity in approximately 25-30% of patients
- Development of new symptoms (e.g., palpitations from atrial fibrillation)
- Decreasing effectiveness of medications over time in some patients
- Need for increased dosages or additional medications
- Emergence of more consistent symptoms with lighter degrees of exertion
- Progressive exercise limitation affecting quality of life
Advanced Disease (15+ Years or End-Stage):
- Significant limitation of daily activities in progressive cases
- Development of heart failure symptoms even at rest
- Transition from episodic to persistent symptoms
- Refractory symptoms despite optimal medical therapy
- Possible transition to the dilated “burnt-out” phase in 5-10% of patients
- Development of multiple symptom types simultaneously
Trajectory Patterns:
Stable Pattern (60-70% of patients):
- Minimal symptom progression over decades
- Consistent symptom profile with predictable triggers
- Good response to medical therapy
- Preserved quality of life and life expectancy
- May have excellent prognosis with appropriate management
Progressive Pattern (20-30% of patients):
- Gradual worsening of symptom frequency and intensity
- Development of additional symptom types over time
- Initially episodic symptoms become more constant
- Increasing limitation of activities
- May require interventional procedures (myectomy or alcohol ablation)
- Increased risk for complications like atrial fibrillation
Arrhythmic Pattern (10-15% of patients):
- Primary progression is development of arrhythmias
- Transition from occasional to frequent palpitations
- Development of sustained arrhythmias (atrial fibrillation, ventricular tachycardia)
- Symptoms of hemodynamic compromise during arrhythmias
- Increased risk of thromboembolic events
End-Stage/Dilated Pattern (5-10% of patients):
- Transition from preserved to reduced ejection fraction
- Development of systolic heart failure symptoms
- Decreasing response to standard HCM therapies
- Progressive heart failure symptoms despite maximal medical therapy
- May require advanced heart failure therapies or transplantation
Factors Affecting Symptom Progression:
Disease-Related Factors:
- Severity and distribution of hypertrophy
- Degree of outflow tract obstruction
- Extent of myocardial fibrosis
- Presence of microvascular dysfunction
- Genetic substrate (specific mutations)
- Development of atrial fibrillation
Patient-Related Factors:
- Age at diagnosis (earlier onset often predicts more progression)
- Comorbidities (hypertension, diabetes, obesity)
- Adherence to medications and lifestyle recommendations
- Physical activity levels (extremes of inactivity or overexertion)
- Body weight changes and fluid status management
- Development of coronary artery disease
Management-Related Factors:
- Timeliness of appropriate therapy initiation
- Optimization of medical therapy
- Appropriate timing of septal reduction therapy
- Management of atrial fibrillation and anticoagulation
- ICD implantation in high-risk patients
- Regular follow-up and monitoring
4. Causes
What are the biological and environmental causes?
Biological Causes:
Primary Genetic Mechanisms:
- Sarcomere Protein Mutations: Account for 50-60% of HCM cases
- Dominant inheritance pattern, variable penetrance
- Lead to abnormal contractile properties
- Result in inefficient energy utilization
- Cause compensatory hypertrophy and disarray
- Trigger maladaptive cellular signaling cascades
- Primarily affect force generation and transmission
Sarcomere-Related Pathophysiology:
Myocardial Disarray: Hallmark histopathological finding
- Myocytes arranged at oblique and perpendicular angles
- Disruption of normal force transmission
- Creation of arrhythmogenic substrate
- Impaired contractile efficiency
- Associated with increased risk of sudden death
Interstitial Fibrosis: Progressive scarring between myocytes
- Results from repeated microscopic injury
- Exacerbated by microvascular dysfunction
- Creates regions of electrical heterogeneity
- Contributes to diastolic dysfunction
- Forms substrate for reentrant arrhythmias
Microvascular Dysfunction: Small vessel disease
- Reduced coronary flow reserve
- Arteriolar wall thickening and lumen narrowing
- Inadequate vasodilation during stress
- Contributes to myocardial ischemia
- Creates supply-demand mismatch
Biomechanical Consequences:
Diastolic Dysfunction: Impaired relaxation and filling
- Increased chamber stiffness
- Elevated filling pressures
- Reduced early diastolic filling
- Increased reliance on atrial contraction
- Contributes to exercise intolerance and symptoms
Left Ventricular Outflow Tract Obstruction: Dynamic blockage
- Occurs in approximately 70% of patients at rest or with provocation
- Results from septal hypertrophy and SAM of mitral valve
- Creates pressure gradient and increased afterload
- Worsens mitral regurgitation
- Contributes to symptoms and long-term complications
Environmental Modifiers (not primary causes but influence expression):
Physiological Factors:
Physical Activity and Exercise:
- Extremes of athletic training can exacerbate hypertrophy
- Isometric/resistance exercise increases afterload and wall stress
- Dehydration can worsen obstruction and symptoms
- Intense competitive sports increase risk of sudden death in susceptible individuals
Hemodynamic State:
- Dehydration worsens obstruction by reducing preload
- Vasodilation (heat, alcohol, medications) can worsen obstruction
- Sympathetic stimulation increases obstruction
- Blood pressure changes affect symptomatology
Medical and Pharmacological Factors:
Medications:
- Positive inotropes worsen obstruction (digoxin, dobutamine)
- Vasodilators can exacerbate gradients (nitrates, nifedipine)
- Diuretics may worsen symptoms if excessive
- Some antiarrhythmics affect cardiac function
Comorbidities:
- Hypertension increases afterload and may accelerate remodeling
- Obstructive sleep apnea increases sympathetic tone and arrhythmia risk
- Coronary artery disease compounds ischemia from microvascular dysfunction
- Metabolic syndrome may accelerate fibrosis and progression
Developmental and Age-Related Factors:
Growth and Development:
- Pubertal growth spurt may unmask or worsen HCM
- Increased body size requires greater cardiac output
- Hormonal changes affect cardiac remodeling
- Sports participation may reveal previously asymptomatic disease
Aging Effects:
- Age-related fibrosis compounds genetic predisposition
- Comorbid conditions more common with aging
- Diastolic function worsens naturally with age
- Atrial enlargement and fibrillation risk increases with time
Genetic and hereditary factors
Genetic Basis of HCM:
Inheritance Patterns:
Autosomal Dominant Transmission: Most common pattern
- 50% chance of inheriting mutation from affected parent
- Variable expression even within families
- Incomplete penetrance (not all mutation carriers develop disease)
- Age-dependent penetrance (increasing with age)
- Sex-influenced penetrance (males express earlier/more severely)
De Novo Mutations: New mutations without affected parents
- Account for 10-15% of cases
- May be transmissible to offspring
- Important consideration in genetic counseling
- Often identified in isolated cases without family history
Compound Heterozygosity: Multiple mutations in different genes
- Present in 5-7% of genotyped patients
- Associated with earlier onset and more severe disease
- More complex inheritance risk assessment
- May explain severe phenotypes in some families
Causative Genes:
Sarcomere Protein Genes (Most Common):
MYH7 (β-myosin heavy chain):
- Accounts for 30-40% of genetic cases
- Often associated with early-onset, severe hypertrophy
- Significant variability between specific mutations
- First HCM gene identified (1990)
MYBPC3 (Myosin binding protein C):
- Accounts for 30-40% of genetic cases
- Often associated with later onset, more variable penetrance
- Founder mutations in specific populations
- May have better prognosis than MYH7 on average
TNNT2 (Cardiac troponin T):
- Accounts for 5-10% of genetic cases
- Often less hypertrophy but high arrhythmic risk
- “Thin filament” gene with distinct phenotype
- Associated with sudden death in some families
TNNI3 (Cardiac troponin I):
- Accounts for 5% of genetic cases
- Variable phenotype, some associated with restrictive physiology
- Another “thin filament” gene
- Some mutations cause restrictive cardiomyopathy
TPM1 (α-tropomyosin):
- Accounts for <5% of genetic cases
- Variable penetrance and expression
- Third “thin filament” gene
- Some mutations associated with apical hypertrophy
MYL2 and MYL3 (Regulatory and essential light chains):
- Account for <5% of genetic cases
- Sometimes associated with mid-ventricular obstruction
- Variable phenotypes reported
- Essential light chain mutations often affect papillary muscles
ACTC1 (Cardiac actin):
- Rare cause of HCM (<1% of cases)
- Also associated with other cardiomyopathies
- Critical sarcomere structural protein
- Variable phenotypic expression
Other Genetic Causes:
Z-disc Protein Genes:
- CSRP3 (Muscle LIM protein)
- TCAP (Telethonin)
- ACTN2 (α-actinin-2)
- Associated with later onset and variable penetrance
Calcium-Handling Protein Genes:
- JPH2 (Junctophilin-2)
- PLN (Phospholamban)
- Often associated with arrhythmic risk
Metabolic Phenocopies:
- PRKAG2: AMP-kinase defect causing glycogen storage and HCM phenotype
- LAMP2: Danon disease, X-linked lysosomal storage disorder
- GLA: Fabry disease, X-linked α-galactosidase A deficiency
- Clinically important to recognize as treatment differs from sarcomeric HCM
Genotype-Phenotype Correlations:
Specific Mutation Effects:
- MYH7 R403Q: Early onset, high penetrance, significant arrhythmic risk
- MYBPC3 founder mutations: Common in Dutch, Finnish, and Japanese populations
- TNNT2 mutations: Often minimal hypertrophy but high sudden death risk
- Multiple mutation cases: Earlier onset, more severe phenotype
Genetic Testing Implications:
- Overall yield of genetic testing: 30-60% of clinically affected patients
- Higher yield in those with family history and earlier onset
- Negative genetic test does not rule out HCM (clinical diagnosis prevails)
- Allows cascade family screening when mutation identified
- Potential prognostic implications for specific genes/mutations
- Important for distinguishing phenocopies requiring different treatment
Any known triggers or exposure risks
Physiological and Environmental Triggers:
Hemodynamic Triggers:
Dehydration: Reduces preload, worsening obstruction
- Hot environments causing fluid loss
- Gastrointestinal illness with fluid loss
- Inadequate fluid intake during exercise
- Excessive diuretic use
- May precipitate symptoms or hemodynamic collapse
Vasodilation States:
- Hot environments (saunas, hot tubs)
- Alcohol consumption (peripheral vasodilation)
- Vasodilating medications (nitrates, nifedipine)
- Post-prandial state (food-induced splanchnic vasodilation)
- Can worsen outflow obstruction and symptoms
Volume Shifts:
- Rapid position changes (standing quickly)
- Post-hemorrhage or blood donation
- Hemodialysis-associated volume removal
- Large-volume paracentesis without albumin replacement
- May precipitate syncope or pre-syncope
Autonomic Nervous System Triggers:
Adrenergic Stimulation:
- Intense emotional stress
- Competitive athletic participation
- Public speaking or performance
- Unexpected loud noises or startling
- Increases contractility and outflow obstruction
Valsalva-Like Maneuvers:
- Heavy lifting or straining
- Forceful coughing or vomiting
- Straining during bowel movements
- Wind instrument playing
- Reduces venous return and increases obstruction
Specific Activity Triggers:
Sports and Exercise:
- Burst activities (sprinting, basketball)
- Isometric/resistance exercise (weightlifting)
- Exercise in extreme environmental conditions
- Inadequate warm-up periods
- Association with sudden death in young athletes
Daily Activities:
- Rapid standing from squatting position
- Heavy meals followed by activity
- Sexual activity (combines adrenergic stimulation with vasodilation)
- Rapid stair climbing
- Can provoke symptoms in susceptible individuals
Medical and Pharmacological Exposures:
Medication-Related Triggers:
Positive Inotropic Agents:
- Digoxin
- Dobutamine and other sympathomimetics
- Theophylline
- Increase contractility and worsen outflow obstruction
Vasodilators:
- Nitroglycerin and nitrates
- Hydralazine
- Minoxidil
- Phosphodiesterase inhibitors (sildenafil)
- Reduce afterload and exacerbate dynamic gradients
Rate/Rhythm-Altering Medications:
- Some antiarrhythmics
- Abrupt discontinuation of beta-blockers
- Medications prolonging QT interval
- May precipitate arrhythmias or worsen hemodynamics
Medical Procedures/Conditions:
Perioperative Period:
- Anesthesia-induced vasodilation
- Hypovolemia during surgery
- Positive pressure ventilation reducing venous return
- Post-operative pain and catecholamine surge
- Requires specialized anesthesia management
Acute Medical Conditions:
- Atrial fibrillation onset
- Systemic infections with fever/tachycardia
- Acute blood loss
- Thyrotoxicosis (increases contractility and heart rate)
- May precipitate heart failure or hemodynamic decompensation
Physiological States:
Pregnancy:
- Hemodynamic changes (increased blood volume, heart rate)
- Third trimester positioning (compression of vena cava)
- Labor and delivery (Valsalva, pain, exertion)
- Postpartum hemorrhage
- Generally well-tolerated but requires specialized management
Adolescent Growth Spurt:
- Rapid increase in body size and cardiac demands
- Hormonal changes affecting remodeling
- Often coincides with disease expression
- Particularly impactful in male adolescents
Aging-Related Changes:
- Increased vascular stiffness
- Hypertension development
- Diastolic function deterioration
- Coronary atherosclerosis development
- May lead to symptomatic progression in previously stable patients
5. Risk Factors
Who is most at risk (age, gender, occupation, lifestyle, etc.)?
Demographic Risk Factors:
Age-Related Risk:
Adolescents and Young Adults (14-35 years):
- Peak period for initial HCM diagnosis
- Highest risk period for sudden cardiac death
- Coincides with maximum physical activity levels
- Disease often becomes apparent during growth spurt
- Athletic participation may reveal previously undiagnosed disease
Middle-Aged Adults (36-60 years):
- Second peak for HCM diagnosis (often from screening or incidental findings)
- Increasing prevalence of symptoms and complications
- Development of atrial fibrillation becomes more common
- Heart failure symptoms often emerge in this age group
- Comorbidities begin to influence disease expression
Older Adults (>60 years):
- Later-onset disease expression common with some genetics (especially MYBPC3)
- Increased prevalence of heart failure symptoms
- Higher risk of thromboembolic complications
- Burning out to end-stage more likely
- Cumulative effects of lifelong disease burden
Gender-Related Risk:
Male Predominance:
- Diagnosed 1.5-3 times more frequently in men
- Earlier disease expression in males
- More pronounced hypertrophy on average
- Higher sudden death risk across age groups
- Potential hormonal influence on disease expression
Female-Specific Considerations:
- Often diagnosed later in disease course
- More likely to be symptomatic at diagnosis
- Higher prevalence of outflow tract obstruction
- More frequent progression to heart failure symptoms
- Pregnancy introduces specific management challenges
Racial and Ethnic Factors:
- Similar prevalence across racial groups but differences in:
- Access to diagnosis and care
- Specific founder mutations in certain populations
- Age at diagnosis (later in some minority populations)
- Comorbidity profiles affecting disease
- Healthcare disparities affecting outcomes
Occupational and Lifestyle Risk Factors:
Athletic Participation:
Competitive/Elite Athletes:
- Increased risk of sudden cardiac death with undiagnosed HCM
- Sports with high dynamic and static components carry highest risk
- Physiologic remodeling may mask or mimic HCM
- Pre-participation screening may identify disease
- Restrictions often recommended after diagnosis
Physically Demanding Occupations:
- Military service (especially special forces training)
- Firefighting, law enforcement with intense physical requirements
- Construction and manual labor (particularly in heat)
- Commercial diving and high-altitude work
- May experience symptoms sooner or more severely
Specific Occupational Considerations:
Pilots and Air Traffic Controllers:
- Licensing restrictions with HCM diagnosis
- Syncope risk presents safety concern
- Arrhythmia potential during critical operations
- Regular medical certification requirements
- Career implications of diagnosis
Professional Athletes:
- Diagnosis often career-ending in many countries/leagues
- Regular cardiac screening may detect disease
- High-profile cases have increased awareness
- Risk-benefit assessment increasingly individualized
- Legal and ethical issues around disqualification
Environmental and Lifestyle Factors:
Extreme Environments:
- High altitude exposure
- Very hot climates increasing dehydration risk
- Very cold environments (vasoconstriction/increased afterload)
- Exposure to sudden temperature changes
- May exacerbate symptoms or trigger events
Substance Use:
- Cocaine and stimulants (increase arrhythmia risk)
- Alcohol (acute vasodilation; chronic myocardial effects)
- Anabolic steroids (may worsen hypertrophy)
- Energy drinks with high caffeine content
- Increased risk with underlying HCM
Environmental, occupational, and genetic factors
Environmental Factors Affecting HCM:
Physical Environment:
Climate Considerations:
- Heat exposure increases vasodilation and dehydration risk
- Humidity impairs thermoregulation and increases cardiovascular stress
- Altitude exposure increases pulmonary pressure and hypoxic stress
- Environmental pollutants may increase cardiovascular strain
- Seasonal variation in symptoms reported by many patients
Exercise Environment:
- Indoor vs. outdoor activity differences in temperature regulation
- Swimming (horizontal position and water pressure effects)
- High-altitude exercise with reduced oxygen availability
- Exercise in extreme temperatures (hot or cold)
- Supervised vs. unsupervised settings for safety
Social and Lifestyle Environment:
Socioeconomic Factors:
- Access to specialized HCM care
- Ability to adhere to medication regimens
- Financial resources for genetic testing
- Occupation flexibility for symptom management
- Education level affecting disease understanding
Psychological Environment:
- Chronic stress effects on sympathetic tone
- Anxiety about disease prognosis
- Depression affecting self-care
- Social support network availability
- Mental health comorbidities affecting management
Occupational Factors:
Physical Demands:
Strenuous Occupations:
- Heavy manual labor increasing cardiac workload
- Occupations requiring bursts of intense activity
- Jobs with significant isometric components
- Physically demanding emergency responses
- May accelerate symptom development or limit career longevity
Environmental Workplace Conditions:
- Hot work environments (foundries, kitchens, outdoor labor)
- High-altitude work sites
- Confined spaces with limited climate control
- Exposure to cardiotoxic chemicals
- May exacerbate underlying disease
Occupational Restrictions and Accommodations:
Safety-Sensitive Positions:
- Commercial transportation (pilots, train operators, bus drivers)
- Critical infrastructure operations
- Military service limitations
- First responder fitness requirements
- May have regulatory restrictions for those with HCM
Workplace Adjustments:
- Modified duty accommodations
- Temperature-controlled environments
- Flexible scheduling to manage fatigue
- Access to hydration and rest periods
- Employment protections under disability legislation
Genetic Factors (Expanded):
Genetic Testing Complexities:
Variable Penetrance:
- Not all mutation carriers develop clinical HCM
- Age-dependent expression
- Sex-influenced penetrance
- Environmental modifier effects
- Implications for family screening and counseling
Variable Expressivity:
- Same mutation causes different phenotypes
- Intrafamilial diversity in disease severity
- Range from asymptomatic to severe disease
- Modifier genes influencing expression
- Prediction challenges for individual mutation carriers
Genetic Modifiers:
Compound Mutations:
- Multiple pathogenic variants worsen prognosis
- Earlier onset and more severe phenotype
- Higher risk of adverse events
- Complexity in genetic counseling
- Importance of comprehensive genetic testing
Background Genetic Variation:
- Polymorphisms affecting protein expression
- Renin-angiotensin system variants
- Variants in signaling pathway genes
- Mitochondrial DNA variations
- Explains some variation within families
Population-Specific Genetic Factors:
Founder Mutations:
- MYBPC3 c.2373_2374insG in Dutch population
- MYBPC3 p.Gln1061X in South Asian populations
- TPM1 p.Glu62Gln in Japanese cohorts
- Higher prevalence in certain geographic regions
- Different phenotypic expressions between populations
Genetic Architecture Differences:
- Varying mutation frequencies between ethnic groups
- Different genetic backgrounds affecting expression
- Population-specific modifier genes
- Importance in genetic testing strategy
- Implications for global HCM management
Impact of pre-existing conditions
Cardiovascular Comorbidities:
Hypertension:
- Prevalence: Affects 30-40% of adults with HCM
- Impact:
- Increases afterload and wall stress
- Exacerbates hypertrophy and remodeling
- Accelerates fibrosis development
- Complicates assessment of true HCM-related hypertrophy
- Contributes to diastolic dysfunction
- Management Challenges:
- Balancing blood pressure control with preload needs
- Avoiding vasodilators in obstructive HCM
- Medication selection overlap with HCM therapy
- Differentiating primary vs. secondary hypertrophy
Coronary Artery Disease:
- Prevalence: Increases with age; 20-30% of HCM patients >50 years
- Impact:
- Compounds ischemia from microvascular dysfunction
- Increases arrhythmia substrate
- Worsens systolic function in advanced disease
- Adds complexity to chest pain evaluation
- May accelerate progression to end-stage disease
- Management Considerations:
- Symptom overlap challenges
- Stress testing limitations in HCM
- Coronary intervention risks in obstructive disease
- Beta-blocker therapy beneficial for both conditions
- Antiplatelet/anticoagulant balance challenges
Atrial Fibrillation:
- Prevalence: Lifetime risk of 20-25% in HCM patients
- Impact:
- Substantial symptom worsening
- Loss of atrial contribution to filling
- Increased stroke risk
- Heart failure exacerbation
- Reduced exercise capacity
- Management Implications:
- Anticoagulation generally indicated regardless of CHA₂DS₂-VASc score
- Rate control challenges with beta-blockers/calcium channel blockers
- Rhythm control often prioritized
- Catheter ablation more complex and less successful
- Increased monitoring requirements
Non-Cardiovascular Comorbidities:
Obstructive Sleep Apnea:
- Prevalence: 40-70% in HCM patients (often undiagnosed)
- Impact:
- Increases sympathetic activation
- Exacerbates atrial fibrillation risk
- Contributes to systemic hypertension
- Worsens oxygen delivery/demand imbalance
- Independent risk factor for heart failure progression
- Management Importance:
- Screening recommended in symptomatic patients
- CPAP therapy improves overall outcomes
- Weight management component essential
- Positional sleep strategies may help obstruction
- Addresses potentially reversible contributor to symptoms
Diabetes Mellitus:
- Prevalence: Similar to general population but worse impact
- Effects:
- Accelerates microvascular dysfunction
- Increases fibrosis development
- Exacerbates diastolic dysfunction
- Adds complexity to medication choices
- May accelerate disease progression
- Special Considerations:
- Avoidance of hypoglycemia (arrhythmia trigger)
- Beta-blocker effects on glucose regulation
- Increased heart failure risk with some diabetes medications
- Enhanced risk of coronary disease
- Importance of tight glucose control
Chronic Kidney Disease:
- Prevalence: Increases with age and heart failure progression
- Impact:
- Limits medication options and dosing
- Increases complications from contrast procedures
- Fluid management challenges
- Electrolyte disturbances affecting arrhythmia risk
- Worsens anemia in advanced disease
- Management Adaptations:
- Medication dose adjustments
- Careful contrast use with imaging
- Enhanced monitoring of renal function
- Avoidance of NSAIDs
- Coordination with nephrology
Age-Related Conditions:
Frailty and Deconditioning:
- Prevalence: Increases with age, especially with longstanding HCM
- Impact:
- Limits exercise tolerance independent of cardiac status
- Increases fall risk with certain medications
- Complicates surgical intervention decisions
- Affects quality of life beyond cardiac symptoms
- May lead to unnecessary activity restriction
- Approaches:
- Structured, supervised exercise programs
- Physical therapy involvement
- Balanced activity recommendations
- Fall prevention strategies
- Nutritional support
Cognitive Impairment:
- Prevalence: Higher in older HCM patients, especially with atrial fibrillation
- Impact:
- Medication adherence challenges
- Reduced self-monitoring capability
- Communication barriers with healthcare team
- Missed symptoms or warning signs
- Decision-making capacity for interventions
- Adaptations:
- Simplified medication regimens
- Caregiver involvement in care plan
- Written instructions and reminders
- Cognitive screening in older patients
- Advanced care planning while capacity intact
Special Populations:
Pregnancy with HCM:
- Prevalence: Many women with HCM have successful pregnancies
- Considerations:
- Increased cardiac output requirements
- Physiologic volume expansion
- Arrhythmia risk changes
- Labor and delivery hemodynamic challenges
- Medication safety concerns
- Management Approach:
- Preconception counseling and risk assessment
- Multidisciplinary team management
- Careful monitoring throughout pregnancy
- Delivery planning with cardiac anesthesia input
- Close postpartum monitoring
Athletic Training Background:
- Impact:
- Physiologic hypertrophy complicating diagnosis
- Enhanced cardiovascular reserve
- Better tolerance of heart failure symptoms
- Psychological adjustment to activity restrictions
- Detraining effects on cardiovascular health
- Management Considerations:
- Careful differentiation of physiologic vs. pathologic hypertrophy
- Appropriate activity recommendation balancing risk and benefits
- Psychological support for identity changes
- Individualized rather than blanket exercise restrictions
- Supervised cardiac rehabilitation approaches
6. Complications
What complications can arise from HCM?
Mechanical and Hemodynamic Complications:
Obstruction-Related:
Dynamic Left Ventricular Outflow Tract Obstruction (LVOTO):
- Present in ~70% of patients at rest or with provocation
- Causes pressure overload and increased myocardial work
- Leads to dyspnea, syncope, and chest pain
- Contributes to progressive heart failure
- Associated with worse long-term outcomes
Mitral Regurgitation:
- Secondary to systolic anterior motion of mitral valve
- Can be dynamic, varying with obstruction
- Reduces forward cardiac output
- Contributes to pulmonary congestion
- May require intervention with persistent severe regurgitation
Diastolic Dysfunction:
- Present in virtually all HCM patients
- Impaired ventricular relaxation and increased stiffness
- Elevates filling pressures
- Leads to exercise intolerance and dyspnea
- Precedes systolic dysfunction in disease progression
Heart Failure Syndromes:
Heart Failure with Preserved Ejection Fraction (HFpEF):
- Most common heart failure presentation in HCM
- Symptoms disproportionate to systolic function
- Often refractory to standard heart failure therapies
- Exercise intolerance and fatigue predominate
- Requires specialized management approach
End-Stage/Burnt-Out Phase:
- Develops in 5-10% of patients
- Progressive wall thinning and cavity dilation
- Systolic dysfunction (ejection fraction <50%)
- Fibrosis replacing muscle tissue
- Poor prognosis once established
Pulmonary Hypertension:
- Secondary to chronic elevated left atrial pressure
- Develops in 10-20% of patients
- Exacerbates exercise intolerance
- Right ventricular dysfunction may develop
- Associated with worse outcomes
Arrhythmic Complications:
Ventricular Arrhythmias:
Ventricular Tachycardia:
- Non-sustained VT common (25-30% of patients)
- Sustained VT less common but more serious
- Substrate includes fibrosis and myocardial disarray
- May cause syncope or presyncope
- Risk factor for sudden cardiac death
Sudden Cardiac Death (SCD):
- Most devastating complication
- Annual risk 0.2-1% in adult HCM patients
- Higher risk in younger patients
- First manifestation of disease in some cases
- Prevention primarily through ICDs in high-risk patients
Ventricular Fibrillation:
- Terminal rhythm in most SCD cases
- May occur without warning
- Often triggered by VT, exercise, or ischemia
- Requires immediate defibrillation
- Survivor management critically important
Atrial Arrhythmias:
Atrial Fibrillation:
- Occurs in 20-25% of patients lifetime
- Often poorly tolerated hemodynamically
- Increases stroke and heart failure risk
- May be paroxysmal initially, becoming persistent
- Management challenging due to structural abnormalities
Atrial Flutter:
- Less common than atrial fibrillation
- Often precedes or coexists with atrial fibrillation
- Rapid ventricular rates can worsen obstruction
- May respond to catheter ablation
- Anticoagulation considerations similar to atrial fibrillation
Thromboembolic Complications:
Stroke and Systemic Embolism:
Cardioembolic Stroke:
- 5-fold increased risk in HCM patients
- Particularly high with atrial fibrillation
- Can occur even with preserved systolic function
- Often results in significant disability
- Preventable with appropriate anticoagulation
Peripheral Arterial Embolism:
- Less common than stroke
- May affect any arterial territory
- Acute limb ischemia requires urgent intervention
- Visceral embolism can be difficult to diagnose
- Often accompanies cerebral embolism
Left Atrial Thrombus:
- Develops in enlarged, poorly contractile left atria
- Can form even in sinus rhythm in advanced disease
- Detectable on transesophageal echocardiography
- May be first indication for anticoagulation
- Requires extended anticoagulation for resolution
Long-term impact on organs and overall health
Cardiac Structural and Functional Changes:
Progressive Myocardial Remodeling:
Increasing Fibrosis:
- Progressive replacement of myocytes with collagen
- Detectable on cardiac MRI as late gadolinium enhancement
- Increases over time (3-5% per year in some patients)
- Creates substrate for arrhythmias
- Contributes to progressive diastolic and systolic dysfunction
Left Atrial Enlargement:
- Nearly universal in longstanding disease
- Reflects chronic elevation of filling pressures
- Predisposes to atrial fibrillation
- Increases thromboembolic risk
- Marker of disease progression and prognosis
Transition to Dilated Phenotype:
- “Burnt-out” or end-stage progression
- Wall thinning and ventricular dilation
- Systolic dysfunction (ejection fraction <50%)
- Heart failure with reduced ejection fraction
- Occurs in 5-10% of patients over decades
Coronary and Microvascular Effects:
Progressive Small Vessel Disease:
- Thickening of intramural arterioles
- Reduced coronary flow reserve
- Contributes to myocardial ischemia
- Accelerates fibrosis development
- May worsen even with stable hypertrophy
Myocardial Bridging Complications:
- Symptomatic ischemia with deep bridges
- Potential trigger for malignant arrhythmias
- Progressive symptoms over time in some cases
- Management increasingly invasive with progression
- Long-term effects on regional wall function
Non-Cardiac Organ System Effects:
Cerebrovascular System:
Chronic Cerebral Hypoperfusion:
- Fluctuating cardiac output with obstruction
- Episodes of hypotension or near-syncope
- Concerns for cumulative cognitive effects
- White matter changes on brain imaging
- Potential contribution to vascular cognitive impairment
Stroke Sequelae:
- Long-term disability from embolic events
- Cognitive impairment post-stroke
- Physical limitations affecting independence
- Impact on employability and quality of life
- Psychological consequences of disability
Pulmonary System:
Secondary Pulmonary Hypertension:
- Develops in 15-20% of patients long-term
- Results from chronic elevated left atrial pressure
- Contributes to dyspnea and exercise intolerance
- May lead to right ventricular dysfunction
- Associated with worse long-term outcomes
Pulmonary Congestion Effects:
- Recurrent pulmonary edema in some patients
- Chronic interstitial edema affecting gas exchange
- Increased susceptibility to respiratory infections
- Long-term impact on pulmonary function
- Contribution to exercise limitation
Renal System:
Cardiorenal Syndrome:
- Reduced renal perfusion in advanced disease
- Diuretic resistance in heart failure
- Neurohormonal activation affecting kidney function
- Progressive renal function decline with disease advancement
- Limitations on medical therapy options
Contrast Nephropathy Risk:
- Multiple imaging studies throughout disease course
- Cumulative contrast exposure concerns
- Particular risk with coexisting diabetes or hypertension
- May limit diagnostic and therapeutic options
- Potential for accelerated renal function decline
Systemic Effects and Quality of Life:
Exercise Capacity and Functional Status:
Progressive Exercise Limitation:
- Declining peak oxygen consumption over time
- Reduced daily activity levels
- Impact on occupational capabilities
- Limitations on recreational activities
- Dependency for activities of daily living in advanced cases
Deconditioning Cycle:
- Symptom-limited exercise capacity
- Progressive deconditioning from activity restriction
- Further reduction in functional capacity
- Skeletal muscle changes from inactivity
- Challenging to reverse once established
Psychological and Cognitive Effects:
Anxiety and Depression:
- Reported in 30-50% of HCM patients
- Related to unpredictability of disease course
- Concerns about sudden death risk
- Impact of activity restrictions
- Worry about genetic transmission to children
Cognitive Function:
- Concerns about effects of chronic heart failure
- Impact of microemboli in atrial fibrillation
- Effects of medications on cognition
- Sleep disruption affecting cognitive performance
- Emerging research area in HCM
Social and Economic Impact:
Employment Limitations:
- Restrictions in physically demanding occupations
- Limitations in safety-sensitive positions
- Absenteeism due to symptoms and medical care
- Potential income reduction and financial stress
- Early retirement in progressive cases
Insurance Challenges:
- Difficulty obtaining life insurance
- Higher premiums for health insurance
- Disability insurance limitations
- Financial burden of uncovered medical expenses
- Long-term financial planning complications
Potential disability or fatality rates
Mortality Statistics and Risk:
Overall Mortality Risk:
Contemporary Annual Mortality Rate: 0.5-1%
- Significant improvement from historical rates (3-6%)
- Varies by age, risk factors, and access to care
- Lower in specialized HCM centers
- Higher in developing regions with limited resources
- Still elevated compared to age-matched general population
Cause-Specific Mortality:
- Sudden cardiac death: 35-40% of deaths
- Heart failure progression: 30-40% of deaths
- Stroke and thromboembolism: 10-15% of deaths
- Non-cardiac causes: 15-20% of deaths
- Post-procedural complications: <5% of deaths
Temporal Trends:
- Progressive decline in mortality over past 50 years
- Reduction in sudden death with risk stratification and ICDs
- Extended survival with contemporary heart failure management
- Reduced stroke mortality with anticoagulation
- Continuing improvements with specialized care models
Sudden Cardiac Death Risk:
Overall Rates:
- Annual SCD risk: 0.2-0.8% in general HCM population
- Age-related variations:
- Highest in adolescents/young adults: 2-4% annual risk in highest-risk subgroups
- Lower in middle age: 0.5-1% annual risk in intermediate-risk patients
- Lowest in elderly: 0.2-0.3% annual risk except with multiple risk factors
- Children: variable but concerning in symptomatic cases
Risk Stratification Models:
European Society of Cardiology HCM Risk-SCD calculator:
- 5-year SCD risk prediction model
- Low risk (<4%): ICD generally not indicated
- Intermediate risk (4-6%): Individualized decision
- High risk (>6%): ICD generally recommended
- Clinical use has reduced inappropriate ICD implantation
American College of Cardiology/American Heart Association approach:
- Major risk factors (massive hypertrophy, family history of SCD, syncope, NSVT)
- Modifier factors (age, obstruction, LGE on MRI)
- More individualized approach than strict statistical model
- Emphasis on shared decision-making
Heart Failure Progression:
End-Stage Progression Risk:
- Lifetime risk of progression to end-stage: 5-10%
- Annual risk of developing systolic dysfunction: 0.5-1%
- Annual mortality once systolic dysfunction develops: 5-10% without advanced therapies
- Median survival with end-stage disease: 3-5 years without transplantation
- Risk factors for progression:
- Extensive fibrosis on MRI
- Multiple genetic mutations
- Early age of onset
- Atrial fibrillation
- Uncontrolled hypertension
Heart Failure Hospitalization Risk:
- Annual heart failure hospitalization rate: 2-5%
- Readmission rate after HF hospitalization: 25-30% within 30 days
- Impact of septal reduction therapy: Reduces HF hospitalizations by 70-80% in obstructive cases
- Hospitalization risk factors:
- NYHA class III-IV symptoms
- Severe outflow obstruction
- Atrial fibrillation
- Pulmonary hypertension
- Renal dysfunction
Disability Patterns and Rates:
Functional Disability:
NYHA Functional Classification Distribution:
- Class I (no limitation): 25-30% of patients
- Class II (mild limitation): 40-45% of patients
- Class III (marked limitation): 20-25% of patients
- Class IV (symptoms at rest): 5-10% of patients
- Progression to higher class: 5-10% of patients per year without intervention
Work Disability:
- Proportion requiring disability benefits: 10-15% overall
- Early retirement due to HCM: 15-20% of patients
- Occupational restrictions affecting livelihood: 25-30%
- Partial work accommodations needed: 30-40%
- Complete work disability in end-stage disease: >75%
Activity and Lifestyle Disability:
Sports participation restrictions:
- Complete competitive sports prohibition: historically most patients, now individualized
- Recreational sport limitations: 50-70% of patients
- Impact on quality of life from activity restrictions: significant in 40-50%
- Psychological impact of sports disqualification: substantial in young athletes
Daily Activity Limitations:
- Difficulty with stairs: 30-40% of symptomatic patients
- Limited walking distance (<2 blocks): 15-25% of symptomatic patients
- Need for assistance with activities of daily living: 5-10% overall, 30-40% in advanced disease
- Driving restrictions due to syncope risk: 10-15% at some point during disease course
Special Population Considerations:
Pediatric HCM Patients:
- Annual mortality rate: 1-2% (higher than adults)
- Sudden death risk: Particularly elevated in symptomatic children
- Progressive disease course: More common with syndromic/metabolic causes
- Transplantation requirement: 2-3 times more likely than adult-onset disease
- Educational accommodations needed: 30-40% of symptomatic children
- Limitations on development and peer activities: Significant psychosocial impact
Elderly HCM Patients (>75 years):
- Competing mortality risks: Non-cardiac causes predominate
- Disability from combined cardiac and non-cardiac conditions: 40-50%
- Symptom burden typically higher: Despite lower sudden death risk
- Heart failure predominates as cause of death: 50-60% of cardiac deaths
- Quality of life impact: Often severe due to limited physiologic reserve
Pregnancy-Related Risks:
- Maternal mortality: 0.5-1% per pregnancy (concentrated in high-risk cases)
- Heart failure development: 15-20% of pregnancies
- Arrhythmia exacerbation: 20-25% of pregnancies
- Persistent symptom worsening post-partum: 10-15% of cases
- Generally favorable outcomes with proper care: >95% successful pregnancies
7. Diagnosis & Testing
Common diagnostic procedures
Initial Diagnostic Evaluation:
Clinical Assessment:
Comprehensive Medical History:
- Symptom assessment (dyspnea, chest pain, syncope, palpitations)
- Age of symptom onset and progression pattern
- Exercise tolerance and limitations
- Family history of HCM, sudden death, or unexplained cardiac events
- Previous cardiac evaluations and findings
- Response to medications if previously prescribed
Physical Examination:
- Cardiac auscultation for murmurs (systolic ejection murmur that increases with Valsalva)
- Assessment for displaced apical impulse
- Evaluation for signs of heart failure
- Examination for extra-cardiac manifestations of syndromic HCM
- Evaluation of blood pressure response to postural changes
- Detection of abnormal jugular venous pulse
Electrocardiographic Assessment:
12-lead Electrocardiogram (ECG):
- Abnormal in 90-95% of HCM patients
- LV hypertrophy voltage criteria
- ST segment and T wave abnormalities
- Pathological Q waves (septal hypertrophy)
- Left atrial enlargement
- Conduction abnormalities
- Sensitivity: 90-95%
- Specificity: 60-70%
- Primary screening test in family evaluation
Ambulatory ECG Monitoring:
- 24-48 hour Holter monitoring
- Extended monitoring (1-2 weeks) in selected cases
- Evaluation for:
- Ventricular arrhythmias (risk stratification)
- Atrial fibrillation or flutter
- Conduction abnormalities
- Correlation of symptoms with arrhythmias
- Recommended in initial evaluation and periodically thereafter
- Frequency determined by risk profile and symptoms
Imaging Studies:
Transthoracic Echocardiography (TTE):
- Cornerstone of diagnosis
- Measures:
- Left ventricular wall thickness (diagnostic ≥15mm)
- Distribution of hypertrophy
- Left ventricular outflow tract gradient
- Systolic anterior motion of mitral valve
- Mitral regurgitation
- Left atrial size
- Systolic and diastolic function
- Enhanced with provocative maneuvers (Valsalva, standing)
- Sensitivity: 80-95% (operator-dependent)
- Limitations: acoustic windows, apical hypertrophy detection
Stress Echocardiography:
- Exercise or dobutamine stress
- Assesses:
- Dynamic obstruction with exertion
- Exercise-induced wall motion abnormalities
- Blood pressure response to exercise
- Provocable gradients not evident at rest
- Exercise capacity objectively
- Provides functional and hemodynamic information
- Useful in symptomatic patients without resting obstruction
- Helps guide management decisions
Functional Testing:
Cardiopulmonary Exercise Testing (CPET):
- Objective assessment of functional capacity
- Measures:
- Peak oxygen consumption (pVO₂)
- Ventilatory efficiency (VE/VCO₂ slope)
- Chronotropic response
- Blood pressure response to exercise
- Exercise-induced arrhythmias
- Prognostic value (pVO₂ strongly correlates with outcomes)
- Useful for serial assessment of disease progression
- Guides activity recommendations and rehabilitation
6-Minute Walk Test:
- Simpler alternative to CPET
- Measures submaximal exercise capacity
- Correlates with quality of life and symptoms
- Useful for serial assessments
- Particularly valuable in elderly or deconditioned patients
- Limited prognostic information compared to CPET
Medical tests (e.g., blood tests, imaging, biopsies)
Advanced Imaging Techniques:
Cardiac Magnetic Resonance Imaging (MRI):
Morphological Assessment:
- Gold standard for ventricular mass and volumes
- Superior detection of apical and anterolateral hypertrophy
- Precise wall thickness measurements
- Right ventricular involvement assessment
- Identification of anatomical variants (papillary muscle abnormalities)
- Not limited by acoustic windows unlike echocardiography
Tissue Characterization:
- Late gadolinium enhancement (LGE) for fibrosis detection
- T1 mapping for diffuse fibrosis assessment
- T2 mapping for edema evaluation
- Extent of LGE correlates with:
- Ventricular arrhythmia risk
- Sudden cardiac death risk
- Heart failure progression
- Overall prognosis
- Increasingly important for risk stratification
Functional Assessment:
- Precise ejection fraction measurement
- Regional wall motion analysis
- Mitral valve function evaluation
- Flow quantification for obstruction and regurgitation
- Myocardial strain analysis
- First-pass perfusion for microvascular function (research)
Cardiac Computed Tomography (CT):
Anatomical Evaluation:
- Alternative when MRI contraindicated
- Coronary artery assessment (rule out coronary disease)
- Calcification assessment
- 3D reconstruction for interventional planning
- Useful for pre-procedural septal reduction planning
- Limited functional information compared to MRI
CT Angiography Applications:
- Coronary anatomy before myectomy
- Septal perforator anatomy for alcohol ablation planning
- Mitral valve and papillary muscle relationships
- Concomitant coronary anomalies detection
- Lower radiation with modern protocols
Positron Emission Tomography (PET):
Metabolic Assessment:
- Myocardial efficiency evaluation
- Used primarily in research setting
- May identify pre-clinical disease
- Differentiates HCM from phenocopies in selected cases
- Evaluates therapeutic response at molecular level
Perfusion Assessment:
- Quantifies coronary flow reserve
- Detects microvascular dysfunction
- Identifies regional perfusion abnormalities
- Correlates with symptoms and outcomes
- More sensitive than SPECT for balanced ischemia
Laboratory and Genetic Testing:
Blood Biomarkers:
Cardiac Biomarkers:
- Natriuretic peptides (BNP, NT-proBNP):
- Correlate with symptom severity
- Predict heart failure and adverse outcomes
- Useful for monitoring disease progression
- Elevated in 25-50% of HCM patients
- Higher in obstructive forms
- Cardiac troponins:
- Chronically elevated in 25-50% of patients
- Marker of ongoing myocardial damage
- Associated with adverse outcomes
- Different cutoffs from acute coronary syndromes
- Useful in serial monitoring
- Natriuretic peptides (BNP, NT-proBNP):
Other Blood Tests:
- Complete blood count (anemia worsens symptoms)
- Renal function (impacts medication choices)
- Thyroid function (hyperthyroidism worsens obstruction)
- Iron studies (hemochromatosis phenocopy)
- Alpha-galactosidase A (Fabry disease screening in selected cases)
Genetic Testing:
Comprehensive Sarcomere Gene Panels:
- Tests for 8-16 genes depending on panel
- Core genes: MYH7, MYBPC3, TNNT2, TNNI3, TPM1, MYL2, MYL3, ACTC1
- Expanded panels include additional genes
- Identifies causative mutation in 30-60% of cases
- Higher yield with family history of HCM
Testing Strategy:
- Cascade testing based on identified family mutation
- Most cost-effective approach for families
- Negative test doesn’t rule out HCM if clinically present
- Positive test in absence of phenotype requires surveillance
- Results may influence management and risk stratification
Invasive Testing:
Cardiac Catheterization:
Hemodynamic Assessment:
- Direct measurement of pressure gradients
- Response to provocative maneuvers
- Left ventricular end-diastolic pressure evaluation
- Simultaneous pressure recordings
- Gold standard for obstruction quantification
- Reserved for cases with equivocal non-invasive testing
Coronary Angiography:
- Assessment of coronary anatomy
- Rule out coronary artery disease in symptomatic patients
- Identification of myocardial bridges
- Planning for septal alcohol ablation
- Generally performed before surgical myectomy
- Increasingly replaced by CT angiography in selected cases
Electrophysiological Studies:
- Limited role in standard evaluation
- Specific indications:
- Evaluation of conduction abnormalities
- Investigation of unexplained syncope
- Risk stratification in selected cases
- Pre-ablation assessment for ventricular arrhythmias
- Diagnostic approach to wide-complex tachycardias
Myocardial Biopsy:
- Limited role in routine diagnosis
- Specific indications:
- Differentiation of HCM from phenocopies
- Infiltrative disease suspicion
- Evaluation of inflammatory processes
- Research purposes
- Risk of complications limits routine use
- Generally obtained during surgical procedures rather than percutaneously
Early detection methods and their effectiveness
Family Screening Approaches:
Clinical Screening Protocol:
First-degree relatives screening:
- Initial evaluation with ECG and echocardiography
- Periodic reevaluation even if initial screening negative
- Frequency based on age and genetic status
- Children: evaluation every 1-2 years until puberty, then annually during adolescence
- Adults: every 3-5 years if initial screening negative
- Effectiveness: Detects clinical HCM in 25-30% of first-degree relatives
Extended Family Screening:
- Recommended when mutation identified
- Cascade genetic testing most efficient
- Clinical screening for those without genetic testing
- Identifies at-risk individuals before clinical expression
- Cost-effective approach for early detection
- Effectiveness: Extends detection to 10-15% of second-degree relatives
Genetic Testing in Family Screening:
Predictive genetic testing:
- Testing relatives for known family mutation
- Allows release from screening if gene-negative
- Focuses clinical surveillance on gene-positive individuals
- Most useful approach when mutation identified in proband
- Psychological implications require genetic counseling
- Effectiveness: Near 100% for future risk prediction when family mutation known
Limitations of genetic screening:
- Causative mutation identified in only 30-60% of HCM cases
- Variable penetrance means gene-positive may never develop disease
- Cannot predict severity or onset timing
- Potential for variants of uncertain significance
- Psychological impact of positive result
- Cost and insurance concerns
Pre-Clinical Detection Methods:
Electrocardiographic Abnormalities:
ECG changes preceding hypertrophy:
- Abnormal in 60-70% of genotype-positive, phenotype-negative individuals
- Q waves and repolarization abnormalities most common
- May be present years before echocardiographic changes
- Easily obtained, low-cost screening tool
- Effectiveness: Sensitivity 60-70%, specificity 60-70% for pre-clinical disease
Advanced ECG analysis:
- Signal-averaged ECG
- Electrocardiographic imaging
- Fragmented QRS assessment
- Digital ECG biomarkers
- Research applications evolving to clinical use
- Effectiveness: Improving with machine learning approaches
Early Imaging Markers:
Subclinical abnormalities on echocardiography:
- Diastolic dysfunction preceding hypertrophy
- Subtle segmental wall thickening
- Abnormal longitudinal strain patterns
- Elongated mitral valve leaflets
- Crypts in inferior septum
- Effectiveness: Speckle tracking detects abnormalities in 25-30% of gene-positive without hypertrophy
Cardiac MRI preclinical markers:
- Myocardial crypts (especially inferior septum)
- Abnormal mitral valve morphology
- Subtle non-diagnostic hypertrophy
- Early fibrosis detection with T1 mapping
- Abnormal trabeculation patterns
- Effectiveness: Detects structural abnormalities in 50-65% of gene-positive individuals before clinical diagnosis
Biomarkers for Early Detection:
Natriuretic peptides:
- Modest elevations before clinical disease
- Correlate with future disease development
- Serial measurements more valuable than single readings
- Effectiveness: Sensitivity 30-40%, specificity 70-80% for pre-clinical disease
Emerging biomarkers:
- Galectin-3 (fibrosis marker)
- Soluble ST2 (remodeling marker)
- MicroRNAs specific to cardiomyopathy
- Proteomic signatures
- Metabolomic profiles
- Effectiveness: Research stage, not yet validated for clinical use
Athletic Screening Programs:
Pre-participation Screening Approaches:
History and physical examination alone:
- Recommended minimum in US guidelines
- Questionable sensitivity for HCM detection
- Relies heavily on symptoms and family history
- Cost-effective but limited effectiveness
- Effectiveness: Detects only 10-20% of HCM cases in athletes
ECG-inclusive screening:
- European standard includes routine ECG
- Significantly improved detection rates
- Cost-effectiveness debated in different healthcare systems
- Implementation requires trained interpreters
- Effectiveness: Increases detection to 70-80% of HCM cases in athletes
Advanced screening approaches:
- Limited echocardiography (focused protocol)
- Biomarker-enhanced screening
- Risk-stratified intensity based on initial findings
- Not standard but increasingly studied
- Effectiveness: Comprehensive screening detects >90% of cases but cost and false positives are concerns
Effectiveness of Early Detection:
Impact on Outcomes:
Sudden cardiac death prevention:
- Early detection allows risk stratification
- Appropriate activity guidance reduces event risk
- ICD implantation in high-risk individuals
- Family studies suggest 70-80% reduction in mortality with screening programs
- Number needed to screen to prevent one death: approximately 1,000-2,000
Disease progression modification:
- Early medical therapy may delay progression
- Lifestyle modifications before symptoms
- Regular monitoring detects complications earlier
- Impact on long-term outcomes still being studied
- Emerging evidence suggests benefit of pre-symptomatic intervention
Limitations and Challenges:
Variable penetrance and expressivity:
- Not all gene-positive individuals develop disease
- Unpredictable timing and severity of expression
- Risk of unnecessary anxiety and restrictions
- Challenge of managing gene-positive, phenotype-negative individuals
- Lifetime surveillance requirement
False positives and negatives:
- Athletic heart mimicking mild HCM
- Other causes of LVH confounding diagnosis
- Normal variants in certain populations
- Technical limitations of imaging
- Resource utilization for follow-up testing
Cost and resource considerations:
- Genetic testing expenses
- Serial imaging requirements
- Specialist involvement
- Psychological support resources
- Varies widely between healthcare systems
8. Treatment Options
Standard treatment protocols
Medical Management:
Symptom Management and Obstruction Relief:
Beta-Blockers:
- First-line therapy for most symptomatic patients
- Mechanism: Reduces heart rate, contractility, and outflow gradient
- Options: Metoprolol, bisoprolol, atenolol, propranolol
- Dosing: Titrated to heart rate 55-65 bpm at rest
- Efficacy: Improves symptoms in 60-70% of patients
- Side effects: Fatigue, bronchospasm, hypotension, depression
- Contraindications: Severe asthma, high-grade AV block
Calcium Channel Blockers (Non-Dihydropyridines):
- Alternative or additive to beta-blockers
- Mechanism: Reduces contractility and improves diastolic function
- Options: Verapamil, diltiazem
- Most effective in non-obstructive or mildly obstructive HCM
- Caution in severe obstruction (can worsen with vasodilation)
- Efficacy: Improves symptoms in 50-60% of patients
- Side effects: Constipation, edema, bradycardia, AV block
Disopyramide:
- Added for persistent symptoms despite beta-blockers
- Mechanism: Negative inotrope reducing obstruction
- Typically combined with beta-blockers
- Efficacy: Reduces obstruction in 60-70% of patients
- Side effects: Anticholinergic effects, QT prolongation
- Requires monitoring for QT prolongation and proarrhythmia
Mavacamten:
- First-in-class cardiac myosin inhibitor
- Mechanism: Reduces hypercontractility and obstruction
- FDA approved for obstructive HCM
- Efficacy: Reduces gradients and improves symptoms in >70% of patients
- Side effects: Potential for reduced ejection fraction
- Requires regular monitoring of cardiac function
Heart Failure Management:
Loop Diuretics:
- For fluid overload and congestion symptoms
- Cautious use to avoid excessive preload reduction
- Options: Furosemide, torsemide, bumetanide
- Efficacy: Effective for edema and dyspnea in 70-80% of congested patients
- Side effects: Electrolyte disturbances, hypotension, renal dysfunction
Mineralocorticoid Receptor Antagonists:
- For advanced heart failure symptoms
- Options: Spironolactone, eplerenone
- Additional benefit for fibrosis attenuation
- Efficacy: Modest improvement in symptoms and biomarkers
- Side effects: Hyperkalemia, gynecomastia (spironolactone)
Angiotensin Receptor-Neprilysin Inhibitors (ARNI):
- Consider in end-stage/dilated phase with reduced EF
- Limited evidence specifically in HCM population
- Efficacy: Benefit demonstrated in general HFrEF population
- Monitoring: Blood pressure, renal function, potassium
Arrhythmia Management:
Atrial Fibrillation Management:
- Anticoagulation: Recommended regardless of CHA₂DS₂-VASc score
- Rate control: Beta-blockers, calcium channel blockers
- Rhythm control: Amiodarone, sotalol, dofetilide
- Catheter ablation for refractory cases
- Efficacy of rhythm control: 40-60% maintenance of sinus rhythm at 1 year
Ventricular Arrhythmia Management:
- Beta-blockers as foundation
- Amiodarone for recurrent ventricular arrhythmias
- ICD for high-risk patients and secondary prevention
- Catheter ablation for refractory ventricular tachycardia
- Efficacy of amiodarone: Reduces arrhythmia burden by 60-80%
Invasive Treatment Options:
Septal Reduction Therapy:
Surgical Myectomy:
- Gold standard for drug-refractory obstruction
- Extended myectomy with mitral valve repair if needed
- Performed at experienced centers (>50 procedures/year)
- Mortality: <1% at experienced centers
- Efficacy: >90% achieve significant gradient reduction
- Durability: Excellent long-term results (>20 years)
- Complications: Heart block (5-10%), ventricular septal defect (<1%)
Alcohol Septal Ablation:
- Catheter-based alternative to surgery
- Selective infarction of basal septum with alcohol
- Best suited for older patients or surgical high-risk
- Efficacy: 80-90% achieve significant gradient reduction
- Mortality: 1-2%
- Complications: Heart block requiring pacemaker (10-20%)
- Less predictable than surgery for certain anatomies
Implantable Devices:
Implantable Cardioverter-Defibrillator (ICD):
- Primary prevention: For high-risk patients
- Secondary prevention: After cardiac arrest or sustained VT
- Risk stratification essential for primary prevention
- Transvenous or subcutaneous systems
- Efficacy: Terminates life-threatening arrhythmias in >98% of cases
- Complications: Inappropriate shocks (5-25%), lead failure, infection
- Psychological impact significant for some patients
Pacemaker Therapy:
- Limited role in modern management
- May help selected patients with conduction disease
- Right ventricular pacing can reduce obstruction in some cases
- Generally not recommended as primary therapy for obstruction
- Efficacy for obstruction: Modest (30-50%) and unpredictable
Advanced Heart Failure Therapies:
Cardiac Resynchronization Therapy:
- Consider in end-stage HCM with reduced EF and bundle branch block
- Limited evidence specifically in HCM population
- Efficacy variable and less predictable than in primary dilated cardiomyopathy
Mechanical Circulatory Support:
- Ventricular assist devices as bridge to transplantation
- Technical challenges due to small LV cavity
- Higher complication rates than in dilated cardiomyopathy
- Limited as destination therapy
Heart Transplantation:
- For end-stage disease refractory to other therapies
- Indications:
- Progressive heart failure despite optimal therapy
- Refractory ventricular arrhythmias
- Severe functional limitation (NYHA III-IV)
- Excellent outcomes post-transplant (similar to other cardiomyopathies)
- Limited by organ availability
Treatment Protocol Based on Disease Stage:
Asymptomatic Patients:
- Regular risk assessment and monitoring
- Exercise recommendations and restrictions
- Generally no medications unless high-risk features
- ICD if high-risk criteria met
- Genetic counseling and family screening
- Annual or biennial follow-up based on risk profile
Mildly Symptomatic (NYHA II):
- Beta-blockers first-line therapy
- Calcium channel blockers alternative
- Lifestyle modifications and exercise guidance
- Consider mavacamten if obstructive with persistent symptoms
- Regular monitoring with echocardiography and Holter
- Follow-up every 6-12 months
Moderately to Severely Symptomatic (NYHA III-IV):
- Optimized medical therapy (beta-blockers, disopyramide)
- Consider mavacamten for obstructive disease
- Septal reduction therapy if resting/provoked gradient >50 mmHg and refractory symptoms
- Diuretics for congestive symptoms
- Arrhythmia management as needed
- ICD if high-risk features
- Follow-up every 3-6 months
End-Stage Disease:
- Heart failure therapy (diuretics, MRAs, ARNI if reduced EF)
- Arrhythmia management
- Advanced heart failure evaluation
- Consider cardiac transplantation
- Palliative care involvement
- Follow-up every 1-3 months
Medications, surgeries, and therapies
Pharmacological Therapies in Detail:
Negative Inotropic Agents:
Beta-Adrenergic Blockers:
- Metoprolol succinate (extended-release):
- Dose: 25-200 mg daily
- Advantages: Once-daily dosing, cardioselective
- Considerations: Less potent obstruction reduction than propranolol
- Propranolol:
- Dose: 10-80 mg three to four times daily
- Advantages: Potent gradient reduction, long track record
- Considerations: Multiple daily dosing, non-selective effects
- Bisoprolol:
- Dose: 2.5-10 mg daily
- Advantages: High cardioselectivity, once-daily dosing
- Considerations: Less experience in HCM than other beta-blockers
- Atenolol:
- Dose: 25-100 mg daily or divided twice daily
- Advantages: Cardioselective, well-studied in HCM
- Considerations: Twice-daily dosing may be needed for optimal effect
- Metoprolol succinate (extended-release):
Non-Dihydropyridine Calcium Channel Blockers:
- Verapamil:
- Dose: 120-480 mg daily in divided doses
- Mechanism: Improves diastolic function, reduces contractility
- Advantages: Beneficial effects on relaxation and filling
- Cautions: Can worsen obstruction in severe cases, interaction with beta-blockers
- Diltiazem:
- Dose: 120-360 mg daily in divided doses
- Advantages: Better tolerated than verapamil in some patients
- Considerations: Less evidence specifically in HCM
- Verapamil:
Antiarrhythmic Agents with Negative Inotropic Properties:
- Disopyramide:
- Dose: 400-800 mg daily in divided doses
- Mechanism: Class IA antiarrhythmic with negative inotropic effect
- Efficacy: Reduces outflow gradient by 30-70%
- Limitations: Anticholinergic side effects (dry mouth, urinary retention, constipation)
- Must be combined with beta-blocker to prevent reflex tachycardia
- Amiodarone:
- Dose: 200 mg daily for maintenance
- Primary use for arrhythmia control
- Secondary benefit of modest negative inotropic effect
- Significant long-term toxicity concerns
- Disopyramide:
Cardiac Myosin Inhibitors:
- Mavacamten:
- Dose: 2.5-15 mg daily (titrated based on LVEF and gradient)
- Mechanism: Reduces actin-myosin cross-bridge formation
- Efficacy: 70-80% of patients achieve significant gradient reduction
- Benefits: Improves exercise capacity, symptoms, and quality of life
- Monitoring: Regular echocardiograms for LVEF assessment
- Contraindications: LVEF <55%, severe heart failure
- Mavacamten:
Other Cardiac Medications:
Anticoagulants:
- Direct Oral Anticoagulants (DOACs):
- Preferred for most HCM patients with atrial fibrillation
- Options: Apixaban, rivaroxaban, dabigatran, edoxaban
- Advantages: No monitoring, fewer interactions, reduced intracranial bleeding risk
- Vitamin K Antagonists:
- Traditional option (warfarin)
- Target INR 2.0-3.0
- Considerations: Monitoring requirements, food/drug interactions
- Anticoagulation indications:
- Atrial fibrillation (regardless of CHA₂DS₂-VASc score)
- Prior thromboembolism
- Left atrial thrombus
- Significantly enlarged left atrium with spontaneous contrast
- Direct Oral Anticoagulants (DOACs):
Antiarrhythmics for Rhythm Control:
- Sotalol:
- Dose: 80-160 mg twice daily
- Combined beta-blocker and Class III antiarrhythmic effects
- QT monitoring required
- Dofetilide:
- Dose: Based on renal function, 125-500 mcg twice daily
- Initiated in-hospital with monitoring
- Effective for atrial fibrillation in HCM
- Dronedarone:
- Generally avoided in HCM with significant structural abnormalities
- Limited evidence in HCM population
- Sotalol:
Surgical and Interventional Procedures:
Surgical Septal Reduction:
Transaortic Septal Myectomy:
- Morrow Procedure:
- Traditional approach through aortotomy
- Resection of basal septal muscle
- Depth: 1-1.5 cm, length: 3-4 cm, width: 1.0-1.5 cm
- Success rate: >90% for symptom relief
- Extended Myectomy:
- Resection extended more distally into mid-ventricle
- Addresses mid-ventricular obstruction
- May include papillary muscle mobilization/realignment
- Better addresses complex anatomical variants
- Advantages:
- Comprehensive approach allowing direct visualization
- Concomitant mitral valve repair when needed
- Additional abnormalities addressed simultaneously
- Durable results (>20 years follow-up data)
- Recovery:
- Hospital stay: 5-7 days
- Return to full activities: 6-8 weeks
- Success rate: >90% for gradient reduction
- Morrow Procedure:
Mitral Valve Procedures in HCM:
- Mitral Valve Repair:
- Anterior leaflet shortening/plication
- Posterior leaflet support
- Annuloplasty for dilation
- Addresses intrinsic valve abnormalities common in HCM
- Mitral Valve Replacement:
- Reserved for intrinsic valve disease not amenable to repair
- Mechanical vs. tissue valve based on age and anticoagulation considerations
- Subvalvular apparatus preservation important
- Mitral Valve Repair:
Percutaneous Interventions:
Alcohol Septal Ablation (ASA):
- Technique:
- Selective coronary angiography to identify septal perforators
- Balloon occlusion of target vessel
- Contrast echocardiography to confirm target area
- Injection of 1-3 mL absolute alcohol
- Controlled infarction of basal septum
- Selection criteria:
- Appropriate septal anatomy
- Suitable septal perforator vessels
- Generally older patients (>65 years)
- Surgical contraindications
- Technique:
Alcohol Septal Ablation (ASA):
- Technique:
- Selective coronary angiography to identify septal perforators
- Balloon occlusion of target vessel
- Contrast echocardiography to confirm target area
- Injection of 1-3 mL absolute alcohol
- Controlled infarction of basal septum
- Selection criteria:
- Appropriate septal anatomy
- Suitable septal perforator vessels
- Generally older patients (>65 years)
- Surgical contraindications
- Outcomes:
- Gradient reduction: 60-80% immediately, 70-90% at follow-up
- Symptom improvement: 70-80% of patients
- Mortality: 1-2% (higher than surgery)
- Permanent pacemaker: 10-20% of patients
- Repeat procedures: 7-10% of patients
- Technique:
Percutaneous Mitral Edge-to-Edge Repair:
- MitraClip in HCM:
- Emerging option for selected patients
- Primarily for significant mitral regurgitation
- May help reduce SAM and outflow gradients
- Limited experience specifically in HCM
- Anatomical challenges in HCM patients
- Patient selection:
- Prohibitive surgical risk
- Significant mitral regurgitation
- Suitable valve anatomy
- Typically elderly patients with comorbidities
- MitraClip in HCM:
Device Therapies:
Implantable Cardioverter-Defibrillator (ICD):
- Device Types:
- Transvenous systems (single or dual chamber)
- Subcutaneous ICD (S-ICD)
- Leadless systems with external defibrillation capability
- Primary prevention indications (for patients without prior events):
- Extreme LV hypertrophy (≥30 mm)
- Family history of sudden death
- Unexplained syncope
- Non-sustained ventricular tachycardia
- Abnormal blood pressure response to exercise
- Extensive LGE on cardiac MRI
- High-risk genetic mutations
- Risk calculators guide selection (ESC HCM Risk-SCD)
- Secondary prevention (after cardiac arrest or sustained VT):
- Class I indication for ICD
- Higher rate of appropriate interventions
- Aggressive programming to reduce shocks
- Considerations:
- Programming to minimize inappropriate shocks
- Balance of protection vs. device complications
- Psychological impact assessment
- Sports participation guidance
- Replacement considerations (battery life 5-10 years)
- Device Types:
Pacemaker Therapy:
- Conventional indications:
- Symptomatic bradycardia
- High-grade AV block
- Sinus node dysfunction
- Post-procedural heart block after myectomy/ablation
- Reduction of obstruction:
- RV apical pacing alters septal activation
- Modest efficacy (30-50% gradient reduction)
- Limited role as primary therapy
- May consider in elderly/frail patients unsuitable for other interventions
- AV sequential pacing with short AV delay
- Conventional indications:
Non-Pharmacological and Supportive Therapies:
Exercise and Rehabilitation:
Cardiac Rehabilitation Programs:
- Supervised exercise training
- Individualized protocols based on risk
- Aerobic exercise at moderate intensity
- Heart rate monitoring and limits
- Symptom monitoring during exercise
- Demonstrated improvements in functional capacity
- Helps counteract deconditioning
Exercise Recommendations:
- Low to moderate intensity (typically <70% max heart rate)
- Aerobic activity preferred over isometric/resistance
- Adequate warm-up and cool-down periods
- Avoidance of extreme environments (heat, humidity)
- Hydration emphasizing pre-hydration and maintenance
- Monitoring parameters (symptoms, heart rate, BP)
- Recreational rather than competitive activities
Lifestyle and Supportive Care:
Psychological Support:
- Anxiety and depression screening
- Coping strategies for chronic illness
- Support groups (in-person and online)
- Counseling for specific concerns (sports disqualification, genetic transmission)
- Mental health professional involvement when needed
Vocational and Insurance Counseling:
- Workplace accommodations
- Disability application assistance if needed
- Insurance options counseling
- Legal protections awareness
- Career planning with disease considerations
Nutritional Guidance:
- Sodium intake recommendations
- Regular meal patterns (avoiding large meals)
- Caffeine moderation
- Alcohol limitation (vasodilator effect can worsen symptoms)
- Weight management for symptom control
- Hydration strategies for obstruction management
Emerging treatments and clinical trials
Novel Pharmacologic Approaches:
Cardiac Myosin Modulators:
Mavacamten (Omecamtiv):
- First-in-class cardiac myosin inhibitor
- FDA-approved in 2022 for obstructive HCM
- Mechanism: Reduces excessive actin-myosin cross-bridge formation
- Clinical trials:
- EXPLORER-HCM: Positive Phase 3 results
- VALOR-HCM: Reduced need for septal reduction procedures
- PIONEER-OLE: Long-term safety and efficacy
- Future directions:
- Potential for non-obstructive HCM
- Earlier intervention studies
- Combination therapies
- Prevention of disease progression
Aficamten (CK-3773274):
- Next-generation cardiac myosin inhibitor
- Mechanism similar to mavacamten
- Potentially improved pharmacokinetics
- Clinical trials:
- REDWOOD-HCM: Phase 2 dose-finding study
- SEQUOIA-HCM: Ongoing Phase 3 trial
- MAPLE-HCM: Non-obstructive HCM study
- Preliminary results suggest:
- Significant reduction in LVOT gradients
- Improvement in NYHA functional class
- Favorable safety profile to date
Other Myosin Modulators:
- CK-3872646: Early development stage
- Additional compounds in preclinical development
- Varying selectivity profiles
- Potential for tailored approaches based on specific genetic subtypes
Anti-Fibrotic Therapies:
Pirfenidone:
- Approved for idiopathic pulmonary fibrosis
- Mechanism: Inhibits TGF-β-mediated fibrosis
- PIROUETTE trial in HCM:
- Phase 2 study examining effect on cardiac fibrosis
- Primary endpoint: Change in extracellular volume on MRI
- Potential to modify disease progression
- Challenges:
- Tolerability (GI side effects)
- Long treatment duration needed for fibrosis effects
Galectin-3 Inhibitors:
- GM-CT-01 and other compounds
- Target galectin-3-mediated fibrosis pathway
- Preclinical data shows reduced fibrosis in HCM models
- Early Phase 1/2 studies underway
- Potential biomarker-guided approach
Spironolactone and Eplerenone:
- Mineralocorticoid receptor antagonists
- Well-established safety profile
- Potential anti-fibrotic effects beyond diuretic action
- SPHERE-HCM trial evaluating effect on fibrosis
- May be particularly beneficial in genotype-positive, phenotype-negative individuals
Gene-Targeted Approaches:
RNA-Based Therapies:
Antisense Oligonucleotides (ASOs):
- Mechanism: Target specific mRNA to reduce mutant protein
- Advantage: Allele-specific targeting potential
- Programs in development for specific mutations:
- MYBPC3 frameshift mutations
- MYH7 missense mutations
- Challenges:
- Delivery to cardiac tissue
- Long-term safety with chronic administration
- Mutation specificity limiting broad application
Small Interfering RNA (siRNA):
- Mechanism: RNA interference to silence specific genes
- Preclinical development for common HCM mutations
- Delivery systems including lipid nanoparticles
- Potential for broader mutation coverage than ASOs
- Early preclinical data showing reduced hypertrophy in models
Gene Editing and Replacement:
CRISPR-Based Approaches:
- In vitro correction of HCM mutations demonstrated
- iPSC models showing phenotype rescue
- Base editing technology for point mutations
- Challenges:
- In vivo cardiac delivery
- Off-target effects
- Regulatory pathway
- Limited to specific mutations
Gene Therapy:
- AAV-Mediated Gene Delivery:
- Cardiotropic serotypes (AAV9, AAV6)
- Potential for MYBPC3 haploinsufficiency
- Preclinical models show prevention of phenotype
- Safety in large animal models being assessed
- mRNA Therapeutics:
- Transient expression of functional protein
- Potential for repeat administration
- Lipid nanoparticle delivery systems
- Preclinical development stage
- AAV-Mediated Gene Delivery:
Novel Device and Interventional Approaches:
Emerging Septal Reduction Techniques:
Radiofrequency Septal Ablation:
- Alternative to alcohol septal ablation
- Direct application of radiofrequency energy to septum
- Early studies show promising gradient reduction
- Potentially reduced risk of heart block
- Under investigation in multiple centers
Magnetic Resonance-Guided Focused Ultrasound:
- Non-invasive septal ablation technique
- Uses high-intensity focused ultrasound
- Real-time MRI guidance for precise targeting
- Preclinical and early clinical studies underway
- Potential for reduced procedural risk
Septal Coil Embolization:
- Alternative to alcohol for septal artery occlusion
- May offer more controlled infarct size
- Potentially reduced conduction system effects
- Limited early experience with case series
- Under evaluation compared to standard alcohol ablation
Advanced Device Technologies:
Leadless Pacing Systems:
- Reduced complications compared to transvenous leads
- Options expanding to dual-chamber capability
- Combining with subcutaneous ICDs
- Potential advantages in young HCM patients
- Long-term performance data accumulating
Subcutaneous ICD Advancements:
- Newer generation devices with reduced size
- Improved discrimination algorithms
- ATP capability development
- Hybrid systems with leadless pacing
- Particularly valuable in young HCM patients
Cell-Based Therapies:
Stem Cell Approaches:
- Mesenchymal stem cells to modulate fibrosis
- Cardiac progenitor cells for regenerative potential
- Early-phase clinical trials in cardiomyopathies
- Challenges in cell engraftment and differentiation
- Mechanism likely paracrine rather than direct replacement
Exosome and Vesicle Therapies:
- Cell-derived vesicles containing microRNAs and proteins
- Anti-fibrotic and anti-hypertrophic effects in models
- Advantages over cell therapy (stability, manufacturing)
- Preclinical development for HCM
- Potential for targeted delivery to cardiac tissue
Clinical Trials of Note:
Active Major Trials:
- LIBERTY-HCM: Long-term extension study of mavacamten
- REDWOOD-HCM OLE: Long-term safety of aficamten
- SEQUOIA-HCM: Phase 3 trial of aficamten
- VALOR-HCM: Mavacamten to reduce need for septal reduction therapy
- EXPLORER-HCM OLE: Long-term safety of mavacamten
- MAPLE-HCM: Aficamten in non-obstructive HCM
- FABHCM: Spironolactone for fibrosis in HCM
- VANISH: Valsartan in genotype-positive, phenotype-negative HCM
Early-Phase and Emerging Studies:
- ENDEAVOR: Mavacamten in non-obstructive HCM
- FRONTIER-HCM: Novel myosin modulator trial
- PROACT HCM: Pirfenidone for fibrosis reduction
- EARLY-HCM: Treatment of preclinical disease
- SILICOFCM: Metabolic modulator therapy
- TRED-HCM: Exercise training safety and efficacy
- RELAXED: Ranolazine in non-obstructive HCM
- HALO-HCM: Lifestyle intervention impacts
9. Prevention & Precautionary Measures
How can HCM be prevented?
Genetic Prevention Strategies:
Family Screening and Cascade Testing:
Identification of At-Risk Family Members:
- First-degree relatives of HCM patients have 50% risk of carrying mutation
- Cascade screening starting with closest relatives
- Clinical screening (ECG, echocardiography) for all first-degree relatives
- Genetic testing for known family mutation when available
- Cost-effective approach for prevention of complications
- Implementation:
- Ideally coordinated through specialized HCM centers
- Family-based approach rather than individual
- Genetic counseling prior to testing
- Psychological support throughout process
Surveillance of Genotype-Positive Individuals:
- Regular clinical evaluation to detect phenotype development
- Frequency based on age and risk:
- Children/adolescents: Annual
- Adults: Every 3-5 years if phenotype-negative
- More frequently with concerning features
- Early intervention when phenotype develops
- Activity guidance based on risk assessment
- Early use of beta-blockers in selected cases
- Demonstrated benefit in early detection and management
Pre-Pregnancy and Reproductive Counseling:
Genetic Counseling for HCM Patients:
- Information on autosomal dominant transmission (50% risk)
- Discussion of reproductive options
- Psychological support for decision-making
- Coordination with specialists in reproductive medicine
- Importance of early involvement before pregnancy planning
Reproductive Options:
- Natural conception with prenatal testing:
- Chorionic villus sampling or amniocentesis
- Ethical considerations regarding termination
- Limited clinical utility given variable expressivity
- Preimplantation genetic diagnosis (PGD):
- IVF with genetic testing of embryos
- Selection of embryos without known mutation
- High success rates for mutation exclusion
- Considerations:
- Cost and insurance coverage
- Emotional/physical burden of IVF
- Availability and access
- Religious or ethical concerns for some families
- Natural conception with prenatal testing:
Pregnancy Management:
- Pre-conception risk assessment
- Multidisciplinary approach during pregnancy
- Medication adjustments for fetal safety
- Careful hemodynamic monitoring during delivery
- Post-partum monitoring for decompensation
- Generally well-tolerated with proper management
Emerging Preventive Approaches:
Therapies for Mutation Carriers:
Pharmacological Prevention:
Beta-blockers in genotype-positive/phenotype-negative individuals:
- Limited evidence but theoretical benefit
- May reduce hypertrophic stimulus
- Generally well-tolerated
- Individualized approach based on genetic variant
VANISH Trial:
- Valsartan in early-stage disease
- Target: Prevent/delay development of hypertrophy
- Rationale: Angiotensin II contributes to hypertrophic signaling
- Status: Ongoing clinical trial
Metabolic modulators:
- Address energy depletion hypothesis
- Improve cardiac energetics
- Examples: Perhexiline, trimetazidine
- Early investigational stage for prevention
Potential Gene Therapy Prevention:
- Theoretical application before phenotype development
- Correction of genetic defect in carriers
- Highest potential benefit early in life
- Technical and ethical challenges
- Currently experimental with animal models only
Note: True primary prevention of genetic HCM is currently limited, as the genetic mutation is present from conception. Strategies focus on preventing disease manifestation and complications rather than preventing the underlying genetic condition itself.
Lifestyle changes and environmental precautions
Exercise and Physical Activity Recommendations:
General Activity Guidelines:
Aerobic Exercise Recommendations:
- Low to moderate intensity aerobic activity encouraged
- Target heart rate typically 50-70% of maximum
- Duration: 30-60 minutes, 3-5 times weekly
- Adequate warm-up and cool-down periods
- Gradual progression in intensity and duration
- Monitoring parameters:
- Symptoms (chest pain, dizziness, palpitations)
- Heart rate response
- Perceived exertion (moderate level recommended)
- Recovery time after exertion
Activities Generally Considered Safe:
- Walking at comfortable pace
- Light jogging in low-risk patients
- Stationary cycling with moderate resistance
- Swimming (non-competitive)
- Leisure hiking on gentle terrain
- Golf (walking course, avoiding extreme heat)
- Doubles tennis in selected low-risk patients
- Low-impact aerobics or dance classes
Activities to Approach with Caution:
- Moderate-intensity group fitness classes
- Recreational sports with intermittent exertion
- Downhill skiing (moderate slopes)
- Cycling on varied terrain
- Requires individual risk assessment
- Consider supervised introduction
Activities Generally Not Recommended:
- High-intensity interval training
- Heavy weight lifting or power lifting
- Burst exertion sports (basketball, soccer, hockey)
- Sprint running or swimming
- Activities with potential for collision/trauma
- Exertion in extreme environmental conditions
- Competitive sports (individualized exceptions possible)
Special Populations and Considerations:
Children and Adolescents:
- Balance protection with normal development
- Emphasis on enjoyable activities
- Physical education modifications rather than exemption
- Sports participation decisions involve:
- Degree of phenotypic expression
- Presence of high-risk features
- Psychological impact of restrictions
- Educational approach with schools and coaches
Low-Risk Adult Patients:
- More liberal approach in contemporary management
- Consideration of:
- Absence of high-risk markers
- Minimal or no symptoms
- Normal blood pressure response to exercise
- Minimal or no obstruction
- Patient preference and quality of life
- Shared decision-making approach to activity
- Possible participation in recreational competitive sports
Athletes with HCM:
- Individualized approach replacing blanket disqualification
- Comprehensive risk stratification
- Consideration of specific sport and position
- Level of competition and training requirements
- Psychological readiness for modified participation
- Structured return-to-play protocols
- Regular reassessment of risk-benefit balance
Daily Living and Environmental Considerations:
Hydration and Nutrition:
Hydration Guidelines:
- Maintain adequate hydration at all times
- Particular importance before and during exercise
- Increased needs in hot environments
- Strategic hydration before predictable exertion
- Signs of adequate hydration (urine color, volume)
- Electrolyte replacement during prolonged activity or excessive sweating
Meal Planning Considerations:
- Avoid large, heavy meals (increased splanchnic blood flow)
- Smaller, more frequent meals if postprandial symptoms
- Moderate alcohol consumption (vasodilatory effect)
- Caffeine limitation or monitoring response
- Sodium awareness if heart failure symptoms present
- Overall heart-healthy diet for general cardiovascular health
Environmental Adaptations:
Temperature Extremes:
- Heat precautions:
- Increased vasodilation worsens obstruction
- Heightened dehydration risk
- Activity modification during hot weather
- Cooling strategies (appropriate clothing, shade, fans)
- Air conditioning importance in extreme climates
- Cold weather considerations:
- Vasoconstriction can increase afterload
- Proper layering of clothing
- Extended warm-up in cold conditions
- Face covering to warm inhaled air
- Avoidance of sudden exertion in extreme cold
- Heat precautions:
Altitude Considerations:
- Lower oxygen availability stresses cardiovascular system
- Gradual acclimatization if traveling to high altitude
- Supplemental oxygen consideration above 8,000 feet
- Medication adjustments may be needed
- Initial activity limitation until adaptation
- Lower threshold to seek medical attention for symptoms
Occupational Considerations:
Workplace Accommodations:
Physical Demand Adaptations:
- Modification of heavy lifting requirements
- Pacing of physically demanding tasks
- Adequate rest breaks during extended activity
- Environmental controls (temperature, humidity)
- Assistive devices for strenuous tasks
- Job restructuring when appropriate
Safety-Sensitive Occupations:
- Individual assessment for:
- Commercial driving
- Pilot certification
- Emergency response roles
- Military service
- Industrial equipment operation
- Considerations include:
- Syncope risk assessment
- Arrhythmia burden
- Symptom profile
- Treatment stability
- Risk to public safety
- Relevant regulatory requirements
- Individual assessment for:
Legal Framework:
- Americans with Disabilities Act (US) protections
- Equivalent protections in other countries
- Reasonable accommodation requirements
- Medical certification processes
- Disclosure considerations and privacy
- Resources for workplace advocacy
Behavioral and Psychological Considerations:
Stress Management:
Importance in HCM:
- Sympathetic activation can worsen obstruction
- Stress as potential arrhythmia trigger
- Anxiety about condition can create cycle of symptoms
- Sleep disruption from stress worsens cardiovascular strain
Effective Techniques:
- Mindfulness and meditation practices
- Progressive muscle relaxation
- Guided imagery
- Cognitive behavioral approaches
- Regular exercise within guidelines
- Adequate sleep hygiene
- Professional counseling when needed
Medication and Substance Precautions:
Medications to Use with Caution:
- Vasodilators (can worsen obstruction)
- Diuretics (excessive preload reduction)
- Positive inotropes (digoxin, dobutamine)
- Many antiarrhythmics (QT prolongation)
- Medication lists provided to all care providers
Substances to Avoid:
- Cocaine and stimulants (severe risk)
- Excessive alcohol (vasodilation, arrhythmia risk)
- Anabolic steroids (worsen hypertrophy)
- Energy drinks with high caffeine content
- Herbal supplements affecting heart rate or blood pressure
Vaccines and preventive screenings
Preventive Health Measures:
Cardiovascular Preventive Care:
Regular Cardiovascular Assessment:
- Frequency based on disease severity and risk profile
- Typically every 6-12 months for stable patients
- Elements include:
- Symptom assessment and functional capacity
- Physical examination
- ECG to assess for changes
- Echocardiography to monitor structure and function
- Periodic Holter monitoring for arrhythmia surveillance
- Exercise testing to assess functional capacity and symptoms
- Risk stratification updated at regular intervals
- ICD need reassessment (for those without devices)
Comorbidity Screening and Management:
- Hypertension screening and management
- Target: Lower than general population (<130/80 mmHg)
- Medication selection considering HCM physiology
- Home blood pressure monitoring for optimization
- Lipid screening and management
- Standard guidelines for general population
- Statin benefit beyond lipid lowering (pleiotropic effects)
- Diabetes screening and management
- Standard guidelines with attention to medication interactions
- Glycemic control important for myocardial health
- Obstructive sleep apnea screening
- High prevalence in HCM population (30-40%)
- Low threshold for sleep study
- CPAP therapy when indicated
- Positive impact on arrhythmia risk and symptoms
- Hypertension screening and management
General Preventive Health:
Standard Age-Appropriate Screenings:
- Cancer screenings per guidelines
- Bone density assessment, especially with risk factors
- Mental health screenings (depression, anxiety)
- Vision and hearing assessments
- Comprehensive approach to overall health maintenance
- Coordination between cardiology and primary care
Immunizations:
- Annual influenza vaccination
- COVID-19 vaccination and appropriate boosters
- Pneumococcal vaccination as indicated
- Up-to-date adult immunization schedule
- Particular importance for ICD patients (avoid infectiou complications)
- Generally safe with no specific contraindications
Special Preventive Considerations in HCM:
Endocarditis Prevention:
- Current Guidelines:
- Routine antibiotic prophylaxis NOT recommended for most HCM patients
- Exceptions:
- Previous history of endocarditis
- Prosthetic heart valves
- Unrepaired cyanotic congenital heart disease
- Repaired congenital heart disease with prosthetic material
- Dental hygiene emphasis more important than prophylaxis
- Patient education about endocarditis signs and symptoms
Thromboembolism Prevention:
Atrial Fibrillation Screening:
- Lower threshold for extended monitoring
- Consider implantable loop recorder in high-risk patients
- Surveillance frequency increases with:
- Left atrial enlargement
- Age over b0
- Previous paroxysmal atrial fibrillation
- Heart failure symptoms
Anticoagulation Approach:
- Initiated promptly when atrial fibrillation detected
- Generally indicated regardless of CHA₂DS₂-VASc score
- Direct oral anticoagulants (DOACs) preferred in most cases
- Warfarin if DOACs contraindicated
- Antiplatelet therapy not adequate substitute
- Bleeding risk assessment but rarely outweighs benefit
Family Screening Protocols:
Clinical Screening Recommendations:
First-Degree Relatives:
- Initial evaluation including:
- Detailed history and examination
- 12-lead ECG
- Transthoracic echocardiography
- Consideration of cardiac MRI in selected cases
- Genetic testing if mutation identified in proband
- Frequency of follow-up:
- Children (age 12-18): Annual
- Adults (age 18-21): Every 1-2 years
- Adults (>21 years): Every 3-5 years if normal
- Genotype-positive: More frequent monitoring
- Any symptoms: Immediate re-evaluation
- Initial evaluation including:
Second-Degree Relatives:
- Screening if:
- First-degree relative unavailable for screening
- Family history of early sudden death or severe disease
- Symptoms suggesting cardiac disease
- Otherwise, individualized approach based on family history
- Genetic testing available if family mutation known
- Screening if:
Athletic Pre-Participation Screening:
Standard Recommendations:
- Pre-participation history and physical examination
- Addition of ECG improves sensitivity significantly
- Echocardiography for abnormal findings
- Follow-up with specialty evaluation when HCM suspected
- Varying protocols by country and organization
- Most effective when performed by experienced providers
Implementation Challenges:
- Cost-effectiveness debates
- Resource availability in different settings
- False positive concerns with athlete’s heart
- Psychological impact of screening process
- Provider training in athlete-specific interpretation
- Variable policy adoption internationally
Digital Health and Remote Monitoring:
- Emerging Preventive Applications:
- Wearable ECG technology
- Single or multi-lead recording capability
- Atrial fibrillation detection algorithms
- Potential for early rhythm diagnosis
- Integration with healthcare systems
- Activity and exercise tracking
- Objective measurement of functional capacity
- Trends over time with interventions
- Safe exercise zone guidance
- Medication adherence technologies
- Smart pill bottles or apps
- Reminder systems
- Documentation of compliance
- Remote physiological monitoring
- Blood pressure tracking
- Weight monitoring for fluid status
- Symptoms logging with alerts
- Advancing technologies under evaluation
- Wearable ECG technology
10. Global & Regional Statistics
Incidence and prevalence rates globally
Global Epidemiology:
Overall Prevalence:
Global Estimate: 1 in 200 to 1 in 500
- Represents 0.2-0.5% of the general population
- Approximately 20 million people affected worldwide
- One of the most common inherited cardiac disorders
- Consistent across different racial and ethnic groups
- Previously underestimated (historical estimates: 1 in 500-1,000)
Detection Rate Variations:
- Higher in regions with advanced cardiac imaging
- Increased with systematic screening programs
- Genetic testing availability affects confirmed diagnoses
- Healthcare access disparities influence diagnosis rates
- Detection improving with widespread use of echocardiography
Regional Prevalence Patterns:
North America:
United States:
- Estimated prevalence: 1 in 200-250 (0.4-0.5%)
- Approximately 750,000-1 million affected individuals
- Similar rates across racial and ethnic groups
- Higher detection rates in urban areas with specialized centers
- Specialized HCM centers concentrated in major academic centers
Canada:
- Estimated prevalence: 1 in 250-300 (0.33-0.4%)
- Approximately 120,000-150,000 affected individuals
- Provincial variations in diagnosis rates
- Centralized care through regional referral centers
- Universal healthcare facilitates access to diagnosis
Europe:
Western Europe:
- Estimated prevalence: 1 in 200-300 (0.33-0.5%)
- Population screening studies in Italy, Spain show consistent rates
- Strong registry data from multiple countries
- National healthcare systems facilitate comprehensive tracking
- Specialized centers of excellence in most countries
United Kingdom:
- Prevalence approximately 1 in 250 (0.4%)
- Centralized care through inherited cardiac conditions clinics
- NHS tracking provides comprehensive data
- Strong family screening implementation
- Established national guidelines and care pathways
Eastern Europe:
- Estimated prevalence: 1 in 250-500 (0.2-0.4%)
- Less robust epidemiological data
- Increasing recognition with improved healthcare resources
- Growing network of specialized centers
- Diagnosis rates improving with international collaboration
Asia-Pacific:
Japan:
- Prevalence: 1 in 250-300 (0.33-0.4%)
- Approximately 400,000-500,000 affected individuals
- Extensive research focus and registry data
- Higher proportion of apical variant (15-25% of HCM)
- Strong genetic research programs
China:
- Estimated prevalence: 1 in 250-500 (0.2-0.4%)
- Potentially 3-5 million affected individuals
- Urban-rural disparities in diagnosis
- Rapidly improving detection with healthcare advancement
- Increasing genetic testing availability
Australia and New Zealand:
- Prevalence: 1 in 200-300 (0.33-0.5%)
- Well-established registry programs
- National coordination of inherited cardiac disease clinics
- Strong emphasis on family screening
- Sports cardiology programs improving detection
Other Regions:
Latin America:
- Estimated prevalence: 1 in 300-500 (0.2-0.33%)
- Limited systematic epidemiological data
- Diagnosis concentrated in urban centers
- Growing awareness and specialized care
- Collaborative international programs improving detection
Middle East:
- Prevalence: 1 in 250-400 (0.25-0.4%)
- Higher rates of consanguinity increasing homozygous cases
- Growing recognition in specialized centers
- Regional variations in healthcare access
- Some countries with national screening programs
Africa:
- Limited epidemiological data available
- Estimated prevalence: 1 in 300-500 (0.2-0.33%)
- Diagnosis primarily in urban medical centers
- Likely significant underdiagnosis in rural areas
- Growing research interest and international collaboration
Incidence (New Diagnosis Rates):
Age-Specific Incidence:
Children (0-10 years):
- 0.3-0.5 per 100,000 per year
- Often detected through family screening
- Occasionally presents with symptoms or murmur
- Metabolic phenocopies more common in this age group
Adolescents (11-20 years):
- 0.8-1.5 per 100,000 per year
- Peak age for initial diagnosis in some regions
- Often detected through sports screening
- Symptomatic presentation more common
Young Adults (21-40 years):
- 1.0-2.0 per 100,000 per year
- Second peak for diagnosis
- Combination of symptomatic presentation and screening
- Diagnosis often prompted by workplace exams or insurance requirements
Middle Age (41-60 years):
- 1.2-2.5 per 100,000 per year
- Increasing diagnosis with routine healthcare
- Incidental findings on imaging for other indications
- Later-onset genetic variants become apparent
Older Adults (>60 years):
- 1.0-2.0 per 100,000 per year
- Challenge distinguishing from hypertensive heart disease
- Later-onset genetic variants (especially MYBPC3)
- Diagnosis often with heart failure presentation
Temporal Trends:
Historical Underdiagnosis:
- Pre-1990s: Estimated at 1 in 1,000-2,000
- 1990-2000s: Revised to 1 in 500
- Post-2010: Current estimates of 1 in 200-500
- Reflects improved detection rather than increasing incidence
Factors Increasing Diagnosis Rates:
- Widespread availability of echocardiography
- Advanced imaging (cardiac MRI)
- Genetic testing access
- Increased awareness among physicians
- Implementation of family screening programs
- Athletic screening programs
- Improved definition and diagnostic criteria
Mortality and survival rates
Mortality Statistics:
Overall Mortality:
Contemporary Annual Mortality Rate: 0.5-1.0%
- Significant improvement from historical rates (3-6% annual mortality)
- Largely attributed to:
- Earlier diagnosis
- ICD use in high-risk patients
- Improved management strategies
- Advanced surgical techniques
- Specialized care centers
- Varies by risk profile and access to care
- Higher in non-specialized centers
Historical Trends:
- 1960-1970s: 3-6% annual mortality
- 1980-1990s: 2-3% annual mortality
- 2000-2010s: 1-2% annual mortality
- 2010-present: 0.5-1.0% annual mortality
- Represents one of the most significant improvements in cardiovascular outcome
Age-Specific Mortality:
Children and Adolescents (≤18 years):
- Annual mortality: 2-6% historically, 1-2% in contemporary cohorts
- Highest risk in symptomatic children
- Challenging risk stratification
- Significant reduction with primary prevention ICDs
- Family history particularly important in risk assessment
Young Adults (19-35 years):
- Annual mortality: 1-3% historically, 0.5-1% in contemporary cohorts
- Primary risk is sudden cardiac death
- Athletic participation as risk modifier
- Period of transition from pediatric to adult care
- Effective risk stratification tools available
Middle-Aged Adults (36-60 years):
- Annual mortality: 1-2% historically, 0.5-1% in contemporary cohorts
- Mix of sudden death and heart failure mortality
- Atrial fibrillation contribution to morbidity and mortality
- Risk profile often changes during this period
- Benefits from comprehensive management approach
Older Adults (>60 years):
- Annual mortality: 1-3% historically, 1-2% in contemporary cohorts
- Heart failure deaths predominate over sudden death
- End-stage progression more common
- Comorbidities significantly affect outcomes
- Lower sudden death risk than younger patients
Cause-Specific Mortality:
Sudden Cardiac Death:
- Historically: 60-70% of HCM-related deaths
- Contemporary cohorts: 30-40% of HCM-related deaths
- Significant reduction with ICD use
- Mechanisms:
- Ventricular tachycardia/fibrillation
- Primary conduction system disease
- Acute hemodynamic collapse with obstruction
- Age-related risk highest in adolescents and young adults
Heart Failure-Related Death:
- Accounts for 40-50% of contemporary HCM-related deaths
- Increasing proportion as sudden death decreases
- Mechanisms:
- Progressive diastolic dysfunction
- Development of systolic dysfunction (end-stage)
- Atrial fibrillation with hemodynamic deterioration
- Refractory symptoms despite optimal therapy
- More common in older patients and advanced disease
Stroke and Thromboembolism:
- Accounts for 10-15% of HCM-related deaths
- Associated with atrial fibrillation
- Reduced with appropriate anticoagulation
- Risk persists despite rhythm control
- Atrial myopathy contribution beyond rhythm
Other Causes:
- Infective endocarditis (1-2%)
- Post-procedural complications (1-2%)
- Comorbidity-related deaths
- Non-cardiac causes increasingly predominant with aging
Survival Statistics:
Long-Term Survival Rates:
5-Year Survival Rate:
- Overall: 95-98% in contemporary cohorts
- Varies by risk profile:
- Low risk: >98%
- Intermediate risk: 95-97%
- High risk: 90-95%
- Specialized center care associated with improved outcomes
- Significantly better than historical cohorts (80-85% in 1980s)
10-Year Survival Rate:
- Overall: 90-95% in contemporary cohorts
- Risk-stratified outcomes:
- Low risk: >95%
- Intermediate risk: 90-94%
- High risk: 85-90%
- Approaches general population in low-risk patients
- Significant improvement from historical rates (70-75% in 1980s)
Lifetime Survival Impact:
- Life expectancy approaching normal in well-managed patients
- Estimated reduction of 2-5 years in moderate-risk patients
- Greater reduction (5-10+ years) in high-risk or advanced disease
- Significantly better than historical perceptions of the disease
Subgroup Survival Differences:
Genetic Substrate Impact:
MYBPC3 mutations:
- Generally later onset
- Often milder phenotype
- Better overall survival compared to MYH7
- 10-year survival approximately 92-97%
MYH7 mutations:
- Earlier disease onset
- More severe hypertrophy on average
- Higher adverse event rates
- 10-year survival approximately 88-94%
Multiple mutation carriers:
- Compound or double heterozygotes
- More severe phenotype
- Earlier onset of symptoms
- Worse survival (10-year survival 80-90%)
- Higher treatment requirements
Phenotypic Expression Variations:
Obstructive HCM:
- Without treatment: Worse prognosis
- With optimal management including septal reduction: Similar to non-obstructive
- Successful gradient reduction improves survival
- Symptom improvement correlates with outcome
Non-obstructive HCM:
- Heterogeneous outcomes
- Better than obstructive if minimal symptoms
- Worse if restrictive physiology or extensive fibrosis
- Limited specific therapeutic options
End-stage/Dilated phase:
- 5-year survival without transplant: 60-70%
- Significant improvement with transplantation
- Progressive heart failure primary cause of death
- Limited response to standard heart failure therapy
Intervention Impact on Survival:
ICD implantation:
- Reduces sudden death by >90% in appropriate candidates
- Translates to 1-2% absolute annual mortality reduction in high-risk patients
- Number needed to treat: 4-5 high-risk patients to save one life over 5 years
- Improving patient selection reduces unnecessary implants
Septal reduction therapy:
- Surgical myectomy: Restores near-normal life expectancy in appropriate candidates
- Alcohol septal ablation: Similar survival benefit in carefully selected patients
- Most benefit in severely symptomatic obstructive patients
- Long-term survival data strongest for surgical approach
Medical therapy impact:
- Limited direct mortality benefit in most studies
- Symptom improvement correlates with better outcomes
- Newer agents (mavacamten) impact on survival not yet established
- Appropriate medication selection based on phenotype important
Country-wise comparison and trends
North America:
United States:
- Prevalence: Approximately 1 in 200-250 (750,000-1 million affected)
- Mortality trends: Declined from approximately 2% annually in 1990s to 0.5-1% currently
- Healthcare delivery:
- Network of ~40 specialized HCM centers of excellence
- Concentrated in academic medical centers
- Significant regional disparities in access
- Variable insurance coverage for genetic testing
- Established patient advocacy organizations
- Distinctive elements:
- Strong emphasis on ICD use for primary prevention
- Surgical myectomy preferred over alcohol ablation
- Comprehensive athletic participation guidelines
- Direct-to-consumer genetic testing increasing
- Significant investment in research and clinical trials
Canada:
- Prevalence: Approximately 1 in 250-300 (120,000-150,000 affected)
- Healthcare approach:
- Universal healthcare system facilitating access
- Centralized inherited heart disease clinics in provinces
- More conservative approach to ICD implantation than US
- National coordination of genetic testing
- Strong family screening implementation
- Regional considerations:
- Geographic challenges in rural and remote areas
- Telemedicine initiatives improving access
- Provincial variations in specialized care access
- Referral patterns favor regional specialty centers
- French Canadian founder mutations in Quebec
Europe:
United Kingdom:
- Prevalence: Approximately 1 in 250 (200,000-250,000 affected)
- Healthcare model:
- National Health Service framework
- Network of specialized inherited cardiac conditions clinics
- Structured referral pathways
- National service framework for cardiac care
- Centralized genetic testing services
- Distinctive features:
- Strong cardiac genetics programs
- Pioneer in systematic family cascade screening
- Early adoption of risk stratification models
- Balanced approach to septal reduction techniques
- Strong patient support organizations
Italy:
- Prevalence: Approximately 1 in 250-300 (200,000-240,000 affected)
- Contributions and approach:
- Long research tradition in cardiomyopathies
- Leading center for athletic heart distinction
- National pre-participation screening model
- Regional centers of excellence
- Strong focus on exercise-related risk
- Trends:
- Decreasing sudden death in athletes following screening
- Growing genetic testing programs
- National registry data contributing to knowledge
- Balanced approach to sports participation
- Significant research contributions to field
Germany:
- Prevalence: Approximately 1 in 250-300 (270,000-320,000 affected)
- Healthcare approach:
- Well-structured specialized cardiac care centers
- Universal healthcare access
- Strong emphasis on guideline-directed care
- Robust certification process for specialty centers
- Comprehensive insurance coverage
- Trends:
- Leading alcohol septal ablation experience
- Strong cardiac MRI expertise and implementation
- Substantial involvement in clinical trials
- Emphasis on objective exercise capacity measurement
- Significant basic science research contributions
Netherlands:
- Prevalence: Approximately 1 in 200-250 (70,000-85,000 affected)
- Distinctive elements:
- Pioneer in family screening programs
- Founder mutations in MYBPC3 (2373insG)
- National registry with excellent follow-up
- Centralized approach to inherited cardiac disease
- Strong genetic counseling model
- Contributions:
- Development of risk models
- Significant publications on natural history
- Research on gene-specific outcomes
- Alcohol septal ablation techniques
- Leader in carrier detection strategies
Asia-Pacific:
Japan:
- Prevalence: Approximately 1 in 250-300 (400,000-500,000 affected)
- Distinctive features:
- Higher proportion of apical variant (15-25% vs. 3-10% elsewhere)
- Pioneering research in imaging and genetics
- National health insurance coverage
- Strong emphasis on family evaluation
- Unique founder mutations identified
- Trends:
- Growing genetic testing implementation
- Preference for percutaneous interventions
- Strong cardiac MRI research
- Aging HCM population demographic
- Significant contributions to pathophysiology research
China:
- Prevalence: Approximately 1 in 250-500 (3-5 million affected)
- Healthcare considerations:
- Rapidly evolving healthcare system
- Urban concentration of specialized care
- Growing access to advanced diagnostics
- Variable insurance coverage
- Developing specialized HCM centers
- Trends:
- Improved recognition and diagnosis
- Increasing genetic testing availability
- Growing research contributions
- Development of regional registries
- Unique genetic variants being identified
Australia:
- Prevalence: Approximately 1 in 200-300 (80,000-120,000 affected)
- Healthcare approach:
- Universal healthcare system
- Well-established inherited heart disease clinics
- National coordination of specialty services
- Strong genetic counseling implementation
- Comprehensive family screening
- Distinctive elements:
- Leadership in sports cardiology
- Innovative approaches to rural healthcare delivery
- Strong participation in international trials
- Regional differences in Aboriginal populations
- National registry contributions
Other Regions:
Brazil:
- Prevalence: Approximately 1 in 300-400 (500,000-700,000 affected)
- Characteristics:
- Developing network of specialized centers
- Regional disparities in healthcare access
- Growing expertise in septal reduction
- Active research participation
- Mixed public and private healthcare system
- Trends:
- Increasing diagnostic capacity
- Growing genetic testing availability
- Regional centers of excellence emerging
- Indigenous population considerations
- Collaborative international programs
South Africa:
- Prevalence: Limited data, estimated 1 in 300-500
- Unique aspects:
- Founder effect in Afrikaner population
- Mixed healthcare delivery system
- Limited specialized center availability
- Growing research presence
- Challenges in rural healthcare delivery
- Trends:
- Improving diagnostic capabilities
- International collaborations increasing
- Telemedicine initiatives
- Genetic testing becoming more accessible
- Regional disparities in care quality
Global Trends and Comparisons:
Management Approach Differences:
Septal Reduction Preferences:
- North America: Strong preference for surgical myectomy
- Europe: More balanced between surgery and alcohol ablation
- Asia: Greater utilization of alcohol ablation
- Influenced by:
- Training traditions
- Technology availability
- Reimbursement structures
- Patient preferences
- Healthcare system organization
ICD Utilization Patterns:
- United States: Most aggressive approach
- Europe: More conservative, risk model-driven
- Asia: Generally most conservative
- Disparities reflect:
- Different risk tolerance
- Resource availability
- Cultural attitudes toward interventions
- Economic considerations
- Historical experience
Genetic Testing Implementation:
- Highest in: Netherlands, UK, France, Canada, Australia
- Moderate in: US, Germany, Japan, Italy
- Variable in: China, Brazil, Middle East
- Limited in: Africa, South Asia, parts of Latin America
- Driven by:
- Healthcare system funding
- Insurance coverage
- Specialized center availability
- Cultural attitudes
- Return on investment perceptions
Athletic Participation Approaches:
- North America: Moving toward shared decision-making from previous restriction
- Italy: Strict disqualification based on screening programs
- UK/Australia: Risk-stratified approach
- Japan: Conservative approach with restriction
- Other regions: Variable implementation of guidelines
Resource Allocation and Access:
High-income countries:
- Specialized centers widely available
- Advanced imaging accessible
- Genetic testing routinely available
- Comprehensive family screening
- Novel therapies in clinical use
Middle-income countries:
- Growing specialized center network
- Basic imaging widely available, advanced imaging limited
- Genetic testing available but cost-prohibitive for many
- Variable family screening implementation
- Access to novel therapies limited
Low-income countries:
- Limited specialized expertise
- Basic echocardiography as primary tool
- Genetic testing rarely available
- Minimal family screening
- Focus on basic treatments with limited access to advanced options
Research and Innovation Distribution:
Leading research centers:
- USA: Mayo Clinic, Cleveland Clinic, NIH, Stanford, Boston
- UK: London centers, Oxford
- Italy: Florence, Pavia
- Netherlands: Amsterdam, Utrecht
- Japan: Tokyo, Kobe
- Canada: Toronto, Montreal
- Australia: Sydney
Clinical trial participation:
- Concentrated in North America, Western Europe
- Growing participation from Eastern Europe, Asia, Australia
- Limited participation from Africa, South America
- Expanding global representation in recent years
- Implications for generalizability of findings
11. Recent Research & Future Prospects
Latest advancements in treatment and research
Pharmacological Innovations:
Cardiac Myosin Inhibitors:
Mavacamten (Camzyos):
- First-in-class cardiac myosin inhibitor
- FDA approved in 2022 for obstructive HCM
- Mechanism: Reduces hypercontractility and outflow obstruction
- Clinical trial results:
- EXPLORER-HCM: 37% absolute improvement in NYHA class and exercise capacity
- VALOR-HCM: 74% reduction in eligibility for invasive procedures
- Significant quality of life improvements
- Real-world implementation:
- REMS program requirement
- Regular monitoring of left ventricular function
- Serial echocardiography requirements
- Specialized center certification
- Ongoing research:
- PIONEER-OLE: Long-term safety data
- EXPLORER-LTE: Extended follow-up
- Non-obstructive HCM trials
Aficamten (CK-3773274):
- Second cardiac myosin inhibitor in development
- Potential improvements in pharmacokinetics
- Phase 2 results (REDWOOD-HCM):
- Significant reduction in LVOT gradients
- Improvement in NYHA class
- Favorable safety profile
- Phase 3 (SEQUOIA-HCM) ongoing
- Potential expanded indications under investigation
Additional myosin inhibitors in pipeline:
- Multiple compounds in preclinical and early clinical phases
- Varying selectivity for cardiac vs. skeletal muscle
- Optimized pharmacokinetic profiles
- Different binding characteristics to cardiac myosin
- Potential for precision medicine approaches based on specific mutations
Anti-Fibrotic Approaches:
Pirfenidone in HCM:
- Antifibrotic agent approved for idiopathic pulmonary fibrosis
- PIROUETTE trial results:
- Slowed progression of myocardial fibrosis on MRI
- Favorable ventricular remodeling
- Well-tolerated in HCM population
- Potential to modify disease progression
- Under investigation for genotype-positive, phenotype-negative individuals
Spironolactone/Eplerenone:
- Mineralocorticoid receptor antagonists
- Anti-fibrotic effects beyond diuretic actions
- SPHERE-HCM trial evaluating effect on fibrosis
- Preliminary data suggesting fibrosis attenuation
- Well-established safety profile advantage
Novel anti-fibrotic targets:
- Galectin-3 inhibitors
- TGF-β pathway modulators
- Matrix metalloproteinase modulators
- Preclinical data showing promise
- Moving toward early clinical trials
Metabolic Modulators:
Energy Metabolism Enhancers:
- Perhexiline: Shifts metabolism from fatty acid to glucose utilization
- Trimetazidine: Partial fatty acid oxidation inhibitor
- Early studies showing improved energetics
- Addressed fundamental energy deficiency hypothesis
- Challenges with side effect profiles
Ranolazine:
- Late sodium current inhibitor
- Improves calcium handling and diastolic function
- RESTYLE-HCM trial:
- Mixed results on primary endpoints
- Some patients with significant benefit
- Subgroup identification ongoing
- Potential adjunctive therapy role
Advanced Diagnostic Approaches:
Imaging Innovations:
4D Flow MRI:
- Dynamic visualization of intraventricular flow patterns
- Quantification of turbulence and energy loss
- Better characterization of obstruction mechanisms
- Research applications moving to clinical implementation
- Potential for prediction of progressive remodeling
T1/T2 Mapping and ECV:
- Quantitative assessment of diffuse fibrosis
- Earlier detection of structural changes
- Prognostic value demonstrated in multiple studies
- Identification of at-risk genotype-positive individuals
- Potential therapeutic target identification
Positron Emission Tomography (PET):
- Assessment of myocardial blood flow and coronary flow reserve
- Metabolic imaging of substrate utilization
- Emerging molecular imaging probes for fibrosis
- Research applications moving toward clinical utility
- Potential for early therapeutic response assessment
Genetic and Molecular Diagnostics:
Expanded Gene Panels:
- Comprehensive testing for >80 cardiomyopathy-associated genes
- Improved detection of complex phenotypes
- Better distinction of phenocopies
- More precise genetic counseling
- Discovery of novel disease-causing variants
Variant Classification Improvements:
- Functional assays for variants of uncertain significance
- International databases improving interpretation
- Artificial intelligence algorithms for prediction
- Improved genotype-phenotype correlations
- Greater precision in family risk assessment
Multi-Omics Approaches:
- Integration of genomics, transcriptomics, proteomics
- Metabolomic profiling identifying biomarkers
- Epigenetic modifications in disease expression
- Systems biology approaches to complex interactions
- Moving toward personalized risk prediction
Interventional Advances:
Septal Reduction Innovations:
Minimally Invasive Myectomy:
- Robotically-assisted approaches
- Video-assisted techniques
- Smaller incisions and faster recovery
- Increasing availability at specialized centers
- Outcomes approaching conventional surgery
Alternative Septal Ablation Techniques:
- Radiofrequency ablation of septum
- Cryoablation approaches
- Targeted microwave ablation
- Preliminary results showing promise
- Potential for reduced conduction system effects
Structural Interventions for Mitral Valve:
- Transcatheter edge-to-edge repair (MitraClip) for HCM
- Artificial chordae implantation
- Combined approaches with septal reduction
- Growing experience in complex anatomies
- Expanding options for high-risk surgical patients
Implantable Device Advances:
Subcutaneous ICD Improvements:
- Smaller devices with improved comfort
- Better discrimination algorithms reducing inappropriate shocks
- Potential for pacing capability without transvenous leads
- Particularly valuable for young patients
- Integration with remote monitoring systems
Leadless Pacing Systems:
- Micra AV for AV sequential pacing
- Potential for dual-chamber communication
- Hybrid systems with subcutaneous ICDs
- Reduced long-term complications
- Particular benefit in active populations
Ongoing studies and future medical possibilities
Major Clinical Trials Underway:
Myosin Inhibitor Trials:
SEQUOIA-HCM:
- Phase 3 study of aficamten in obstructive HCM
- Primary completion expected 2024
- Comparing to placebo with background standard therapy
- Endpoints: Exercise capacity, symptoms, and gradients
- Potential for second FDA-approved myosin inhibitor
MAPLE-HCM:
- Aficamten in non-obstructive HCM
- Addressing unmet need in this population
- Evaluation of symptoms, exercise capacity, biomarkers
- Potential to expand treatment options beyond obstructive disease
- Results expected 2025
ENDEAVOR:
- Mavacamten in non-obstructive HCM
- Phase 3 study following promising Phase 2 data
- Focus on diastolic function and symptoms
- Potential to address fundamental mechanism beyond obstruction
- Results expected 2024-2025
Disease-Modifying Approaches:
LIBERTY-HCM:
- Long-term extension study of mavacamten
- Evaluating sustained effects and safety
- Assessing potential for ventricular remodeling
- Data on progression of disease with treatment
- Ongoing with periodic analyses
VANISH:
- Valsartan in genotype-positive, phenotype-negative subjects
- Prevention of disease development
- Targeting early intervention before hypertrophy
- Based on angiotensin II role in hypertrophic signaling
- Results expected 2025-2026
PROACT HCM:
- Pirfenidone for fibrosis reduction
- Building on PIROUETTE results
- Longer-term outcomes assessment
- Potential disease modification
- Focus on clinical outcomes beyond fibrosis
Novel Therapeutic Targets:
COURAGE-HCM:
- Cardiac-directed gene therapy
- MYBPC3 augmentation for haploinsufficiency
- First-in-human study for genetic cardiomyopathy
- Potentially transformative approach
- Initial safety results expected 2024-2025
RELIEVE-HCM:
- Targeting calcium handling abnormalities
- Novel agent affecting SERCA2a function
- Improving energetics and relaxation
- Addressing fundamental disease mechanisms
- Phase 2 study ongoing
Lifestyle and Supportive Care:
LIVE-HCM:
- Structured exercise program in HCM
- Safety and efficacy of supervised training
- Challenging traditional activity restrictions
- Quality of life and functional outcomes
- Potentially paradigm-shifting for activity recommendations
IMPROVE-HCM:
- Comprehensive lifestyle intervention
- Weight management, exercise, stress reduction
- Effect on symptoms and progression
- Patient-reported outcomes emphasis
- Potential for non-pharmacologic management strategies
Emerging Research Directions:
Genetic Manipulation Approaches:
CRISPR-Based Therapies:
- Gene editing technology for mutation correction
- Demonstrated in iPSC-derived cardiomyocytes
- Moving toward larger animal models
- Technical challenges:
- Delivery to cardiac tissue
- Editing efficiency
- Off-target effects
- Regulatory pathway
- Timeline: 5-10 years to early clinical trials
RNA Therapeutics:
- Antisense oligonucleotides (ASOs)
- Small interfering RNA (siRNA)
- Allele-specific silencing of mutant proteins
- Potential for precision approach to specific mutations
- Several programs in preclinical development
- Timeline: 3-7 years to clinical implementation
Gene Therapy Approaches:
- Adeno-associated virus (AAV) delivery
- Replacement of functional protein in haploinsufficiency
- Challenges in cardiotropic delivery
- Dosing and immunity considerations
- Most advanced for MYBPC3 mutations
- Timeline: Early clinical trials beginning now
Cellular and Regenerative Approaches:
iPSC-Derived Cardiomyocytes:
- Disease modeling for drug discovery
- Patient-specific therapy response prediction
- Potential regenerative applications
- Tissue engineering of cardiac patches
- Timeline: Current use in research, 10+ years for therapeutic applications
Exosome and Vesicle Therapeutics:
- Cell-derived vesicles with regenerative properties
- Anti-fibrotic and remodeling effects
- Advantages over direct cell therapy
- Targeted delivery potential
- Timeline: Early clinical trials within 5 years
Artificial Intelligence Applications:
Predictive Algorithms:
- Risk stratification refinement
- Personalized treatment response prediction
- Early disease detection in carriers
- Integration of multimodal data (imaging, genetics, biomarkers)
- Some applications beginning clinical implementation
Imaging Analysis:
- Automated quantification of hypertrophy
- Fibrosis assessment and quantification
- Standardization of measurements
- Improved reproducibility and precision
- Currently entering clinical practice
Digital Phenotyping:
- Wearable technology data integration
- Activity patterns and limitations
- Arrhythmia detection and characterization
- Symptom correlation with physiologic changes
- Growing implementation in clinical care
Precision Medicine Implementation:
Genotype-Directed Therapies:
Mutation-Specific Approaches:
- Different treatment strategies based on specific gene/mutation
- Example: MYH7 vs. MYBPC3 targeted therapies
- Rational drug selection based on molecular mechanism
- Clinical trials beginning to stratify by genetic subtype
- Timeline: Beginning implementation now, expanding over 5-10 years
Modifier Gene Consideration:
- Identification of genetic factors affecting expression
- Polygenic risk scores for disease severity
- Pharmacogenomic approach to medication selection
- Personalized risk prediction
- Timeline: Early implementation in 3-5 years
Phenotype-Specific Management:
Obstructive vs. Non-obstructive Pathways:
- Tailored approach beyond presence of obstruction
- Consideration of:
- Fibrosis burden
- Diastolic function pattern
- Mitral valve morphology
- Left atrial function
- Cellular energetics
- Growing clinical implementation currently
Multi-Parameter Risk Assessment:
- Integration of:
- Traditional risk factors
- Genetic profile
- Fibrosis assessment
- Biomarkers
- Functional capacity
- More precise sudden death risk prediction
- Reduced unnecessary ICDs
- Better identification of high-risk individuals
- Currently evolving in clinical practice
- Integration of:
Potential cures or innovative therapies under development
Transformative Therapeutic Approaches:
Genetic Correction Strategies:
Allele-Specific Silencing:
- Targeted suppression of mutant allele expression
- Preservation of wild-type allele function
- Approaches:
- Antisense oligonucleotides
- RNA interference
- CRISPR interference
- Potential applications:
- MYH7 missense mutations
- TNNT2 mutations with dominant negative effect
- Early intervention before phenotype development
- Current status:
- Preclinical demonstration in cellular and animal models
- Moving toward first-in-human studies
- Delivery methods being optimized
- Target selection and validation ongoing
Gene Replacement/Augmentation:
- Addition of functional gene copies
- Most applicable to haploinsufficiency mechanisms
- Delivery via adeno-associated virus (AAV) vectors
- Primary targets:
- MYBPC3 mutations (most common haploinsufficiency mechanism)
- Genes with reduced expression
- Current status:
- Large animal models demonstrating efficacy
- First human trials in planning stages
- Addressing manufacturing and delivery challenges
- Determining optimal timing of intervention
CRISPR Gene Editing:
- Permanent correction of genetic defect
- Approaches:
- Homology-directed repair
- Base editing
- Prime editing
- Potential for definitive treatment
- Challenges:
- Cardiac delivery methods
- Editing efficiency
- Off-target effects
- Regulatory pathway
- Current status:
- Proof-of-concept in cellular models
- Moving to animal testing
- Delivery methods under development
- 5-10 year timeline to clinical application
Disease-Modifying Pharmacological Approaches:
Targeting Fundamental Disease Mechanisms:
Myofilament Energy Utilization:
- Cardiac myosin inhibitors (mavacamten, aficamten)
- Optimize sarcomere function
- Reduce hypercontractility
- Address core functional abnormality
- Current status:
- First agent FDA approved
- Second in Phase 3 trials
- Long-term effects on remodeling being studied
- Potential for disease modification beyond symptom relief
Anti-Fibrotic Therapies:
- Target progressive fibrosis development
- Approaches:
- TGF-β pathway inhibition
- Galectin-3 inhibition
- Matrix metalloproteinase modulation
- Inflammation pathway targeting
- Potential to slow or halt disease progression
- Current status:
- Pirfenidone showing promise in clinical trials
- Several novel compounds in preclinical development
- Biomarkers being developed for response assessment
- Combination approaches with other therapies
Calcium Handling Normalization:
- Address diastolic dysfunction
- Targets:
- SERCA2a function enhancement
- Ryanodine receptor stabilization
- Late sodium current inhibition
- Calcium sensitivity modulators
- Improve energetics and relaxation
- Current status:
- Several compounds in early clinical trials
- Preclinical data showing improved function
- Challenges with specificity and side effects
- Potential adjunct to other approaches
Regenerative Medicine Approaches:
Cell-Based Therapies:
Cardiomyocyte Replacement:
- Stem cell-derived cardiomyocyte transplantation
- Replace damaged or disarrayed myocardium
- Potential applications:
- Focal scar replacement
- End-stage disease
- Post-myectomy regeneration
- Challenges:
- Cell engraftment and survival
- Electrical coupling with host tissue
- Immune rejection concerns
- Arrhythmia potential
- Current status:
- Preclinical proof-of-concept
- Manufacturing scalability issues
- Safety studies underway
- First human trials in planning stages
Paracrine Effect Approaches:
- Stem cells providing growth factors and signaling molecules
- Anti-fibrotic and regenerative effects
- Improved local environment
- Potential delivered via:
- Direct cell injection
- Engineered tissue patches
- Cell-derived vesicles
- Current status:
- Early clinical trials in cardiomyopathy
- Mixed results with first-generation approaches
- Improved targeting and delivery methods
- Growing evidence for mechanism of action
Tissue Engineering:
- Engineered Heart Tissue:
- Laboratory-grown cardiac tissue
- Organized architecture unlike native HCM
- Applications:
- Replacement of severely disarrayed regions
- Augmentation of thinned end-stage myocardium
- Delivery vehicle for therapeutic cells
- Current status:
- Successful small animal implantation
- Scaling to human-relevant size
- Vascularization challenges
- 7-10 years from clinical application
Prevention Strategies for At-Risk Individuals:
Pre-Phenotype Interventions:
Early Pharmacological Intervention:
- Treatment before hypertrophy develops
- Targeting gene carriers
- Approaches:
- ARB therapy (valsartan in VANISH trial)
- Beta-blockade
- Energy metabolism enhancement
- Anti-fibrotic therapy
- Potential to delay or prevent phenotype expression
- Current status:
- First major clinical trials underway
- Surrogate endpoint validation
- Biomarker development for early disease
- Challenges in risk-benefit for asymptomatic individuals
Lifestyle Optimization:
- Exercise prescription for gene carriers
- Potential protective effect of aerobic conditioning
- Avoidance of environmental triggers
- Stress management and sleep optimization
- Current status:
- Observational data supporting benefit
- Intervention studies in progress
- Replacing older restrictive approaches
- Individualized programs being developed
Innovative Delivery Systems:
Targeted Cardiac Delivery:
Nanoparticle Platforms:
- Cardiac-specific targeting moieties
- Enhanced drug or gene therapy delivery
- Controlled release formulations
- Reduced systemic effects
- Current status:
- Preclinical proof-of-concept
- Moving to large animal studies
- Manufacturing standardization
- 5-7 years from clinical application
Minimally Invasive Local Delivery:
- Catheter-based intramyocardial injection
- Coronary venous access for retrograde delivery
- Pericardial delivery platforms
- Targeted to areas of fibrosis or hypertrophy
- Current status:
- Delivery systems in clinical testing
- Applications for gene and cell therapy
- Combined with imaging guidance
- Some systems entering clinical trials
Integration of Multiple Approaches:
Comprehensive Treatment Platforms:
Combination Therapies:
- Simultaneous targeting of multiple pathways:
- Sarcomere function normalization
- Fibrosis prevention
- Energy metabolism enhancement
- Calcium handling improvement
- Personalized combinations based on phenotype
- Potential synergistic effects
- Current status:
- Preclinical studies showing promise
- First combination trials in planning
- Biomarker-guided selection
- Regulatory pathway challenges
- Simultaneous targeting of multiple pathways:
Staged Interventional Approach:
- Sequential implementation of therapies:
- Genetic modification as foundation
- Pharmacological optimization
- Targeted interventions for residual abnormalities
- Regenerative approaches as needed
- Comprehensive management of all disease aspects
- Tailored to individual disease characteristics
- Current status:
- Conceptual framework being developed
- Component therapies in various stages
- Implementation likely 10+ years away
- Potential for transformative outcomes
- Sequential implementation of therapies:
Timeline to Potential “Cure”:
Near-Term (1-5 Years):
- Expanded use of myosin inhibitors
- Refinement of risk stratification
- Anti-fibrotic therapies implementation
- Improved genotype-phenotype guidance
- Enhanced quality of life and symptoms
- Not curative but substantial improvement
Medium-Term (5-10 Years):
- Gene therapy for specific mutations
- RNA therapeutics for broader application
- Comprehensive prevention strategies
- Multi-modality treatment platforms
- Substantial disease modification
- Potential functional cure for some subtypes
Long-Term (10-15+ Years):
- CRISPR-based genetic correction
- Regenerative approaches for tissue replacement
- Prevention of disease development in carriers
- Personalized multi-modal cure strategies
- Potential for definitive genetic cure
- Technology-dependent timeline with uncertain acceleration
12. Interesting Facts & Lesser-Known Insights
Uncommon knowledge about HCM
Historical and Scientific Curiosities:
Evolution of Understanding:
“The Disease of Contradictions”:
- Initially considered rapidly fatal, now known many have normal lifespan
- Once thought rare, now recognized as most common genetic heart disease
- Previously believed untreatable, now multiple effective therapies
- Historical name changes reflect evolving understanding:
- Idiopathic Hypertrophic Subaortic Stenosis (IHSS)
- Asymmetric Septal Hypertrophy (ASH)
- Hypertrophic Obstructive Cardiomyopathy (HOCM)
- Now simply HCM (acknowledging not all are obstructive)
Landmark Cases:
- The “Teare Eight”: Eight young patients whose autopsies led to first modern description
- Several high-profile athletes whose sudden deaths raised awareness
- Identification of familial nature preceded genetic testing by decades
- Historical resistance to accepting genetic basis in medical community
Unique Biological Features:
Myocardial Disarray:
- Chaotic arrangement of cardiac muscle cells at microscopic level
- Can exceed 30% of myocardium (normal <1%)
- Create “whorled” pattern visible on histology
- Contributes to both mechanical dysfunction and electrical instability
- Most prominent in areas of hypertrophy but can exist without hypertrophy
- Can be found in small amounts in normal hearts at specific locations
Microvascular Abnormalities:
- Intramural coronary arterioles show medial and intimal thickening
- Reduced lumen size by up to 80%
- Occurs throughout myocardium, even in non-hypertrophied areas
- Contributes to ischemia despite normal epicardial coronary arteries
- May precede development of hypertrophy in gene carriers
- Not reversed by current treatments
Mitral Valve Differences:
- Elongated mitral valve leaflets in many patients independent of flow effects
- Increased leaflet area by 30-40% compared to normal
- Primary abnormality rather than secondary adaptation
- May represent developmental effect of sarcomere mutations
- Contributes to obstruction mechanism
- Influences surgical approach
Unusual Clinical Features:
Geographic and Ethnic Variations:
Apical Variant Predominance in East Asia:
- Represents 15-25% of HCM in Japan and Korea
- Only 3-10% in Western populations
- Different genetic basis suspected
- Often presents with giant T-wave inversions on ECG
- Ace of spades configuration on imaging
- Generally better prognosis than other variants
MYBPC3 c.2373_2374insG Mutation:
- Founder effect in Dutch population
- Present in approximately 1 in 200 individuals in Netherlands
- Accounts for >25% of all HCM in Dutch population
- Later onset phenotype
- Incomplete penetrance allowing survival to reproductive age
- Similar founder mutations in other populations
Dynamic Nature of Obstruction:
“Brockenbrough-Braunwald-Morrow Sign”:
- Paradoxical decrease in pulse pressure after PVC
- Opposite of normal response
- Diagnostic of dynamic outflow obstruction
- Reflects worsened obstruction from increased contractility
- Historical significance in diagnosis before imaging
- Still useful in cardiac catheterization laboratory
Provocative Factors Influence:
- Standing from squatting can precipitate near-syncope
- Post-prandial symptoms due to splanchnic vasodilation
- Hot environments worsen symptoms
- Dehydration dramatically increases gradients
- Alcohol produces biphasic response (initial worsening, then improvement)
- Morning dehydration explains common symptom pattern
Lesser-Known Manifestations:
Autonomic Dysfunction:
- Impaired heart rate recovery after exercise
- Abnormal blood pressure responses
- Baroreceptor sensitivity changes
- May contribute to syncope beyond hemodynamic effects
- Potential target for therapeutic intervention
- Correlates with symptoms independent of obstruction
Speech-Induced Symptoms:
- Public speaking can trigger symptoms
- Valsalva effect during projected speech
- Autonomic activation compounds effect
- Historical reports of clergymen with syncope during sermons
- Can be mitigated with proper breathing techniques
- Beta-blockers particularly helpful for this scenario
Reverse Split Second Heart Sound:
- P2 occurs before A2 (opposite of normal split)
- Due to prolonged left ventricular ejection time
- Useful bedside diagnostic clue
- Correlates with severity of obstruction
- Changes with interventions that reduce gradient
- Teaches important cardiac physiology concept
Myths and misconceptions vs. medical facts
Myth 1: HCM is uniformly a high-risk condition with poor prognosis. Fact: Contemporary management has dramatically improved outcomes, with overall annual mortality rates of 0.5-1%, approaching the general population in many subgroups. The vast majority of properly managed HCM patients can expect normal or near-normal life expectancy. Risk varies significantly between individuals, with many having excellent prognosis and others requiring more intensive management. The critical factor is accurate risk stratification and appropriate preventive measures for those at higher risk.
Myth 2: All HCM patients should avoid exercise and competitive sports. Fact: While historical recommendations included blanket exercise restrictions, contemporary guidelines recognize the heterogeneity of risk and the importance of physical activity for overall health. Current approaches favor individualized exercise recommendations based on specific risk profile, phenotype, genetic substrate, and patient preferences. Many HCM patients can safely participate in moderate-intensity exercise, and selected low-risk patients may even engage in competitive sports following comprehensive evaluation. Shared decision-making has replaced universal prohibition.
Myth 3: All HCM patients have significant outflow tract obstruction. Fact: While approximately 70% of HCM patients may develop obstruction at rest or with provocation, about 30% have non-obstructive disease throughout their lives. The pathophysiology of symptoms in non-obstructive HCM involves diastolic dysfunction, microvascular ischemia, and in some cases, midventricular obstruction or apical aneurysms. These patients require different management approaches, as septal reduction therapies are not appropriate without obstruction. Careful phenotyping is essential for proper management decisions.
Myth 4: HCM is always easily diagnosed by echocardiography. Fact: While echocardiography is the first-line imaging modality, it has limitations in certain scenarios. Apical hypertrophy may be missed due to near-field artifacts and limited apical visualization. Athletes with physiologic remodeling can be difficult to distinguish from mild HCM. Early disease may show borderline wall thickness. Other conditions can mimic HCM, including hypertensive heart disease, cardiac amyloidosis, and storage diseases. Cardiac MRI, genetic testing, and comprehensive clinical assessment are often necessary for accurate diagnosis in complex cases.
Myth 5: A positive genetic test is required to confirm HCM diagnosis. Fact: While genetic testing is valuable for family screening and prognostication, it is not required for clinical diagnosis. Current genetic testing identifies a causative mutation in only 30-60% of clinically diagnosed HCM patients. The diagnosis remains primarily clinical, based on imaging demonstration of unexplained left ventricular hypertrophy (≥15mm), typically with supporting features such as ECG abnormalities, family history, or characteristic functional findings. A negative genetic test does not rule out HCM.
Myth 6: Beta-blockers are the only effective medical therapy for HCM. Fact: While beta-blockers remain first-line therapy for symptom management, several other medication classes have established efficacy in HCM. Non-dihydropyridine calcium channel blockers (verapamil, diltiazem) are effective alternatives, particularly in non-obstructive disease. Disopyramide provides additional benefit for obstruction when combined with beta-blockers. Most recently, cardiac myosin inhibitors (mavacamten) have shown significant efficacy for obstructive HCM. Treatment selection should be individualized based on phenotype, comorbidities, and symptom pattern.
Myth 7: All HCM patients need an implantable cardioverter-defibrillator (ICD). Fact: ICDs are indicated only for patients identified as high-risk for sudden cardiac death, representing approximately 15-20% of the HCM population. Risk stratification involves assessment of multiple factors including family history of sudden death, unexplained syncope, extreme hypertrophy, abnormal blood pressure response to exercise, and non-sustained ventricular tachycardia. Contemporary risk calculators (e.g., HCM Risk-SCD) provide more precise risk estimation. Unnecessary ICD implantation exposes patients to device complications without benefit.
Myth 8: HCM is always caused by intense athletic training or hypertension. Fact: While athletic remodeling (“athlete’s heart”) and hypertensive heart disease can cause left ventricular hypertrophy that may mimic HCM, true HCM is a genetic disorder caused by mutations in cardiac sarcomere proteins. Key differentiating features include family history, ECG abnormalities, diastolic dysfunction, regional distribution of hypertrophy, and lack of regression with detraining or blood pressure control. Misattribution of HCM to these acquired causes can lead to missed diagnosis and failure to screen family members.
Myth 9: Septal reduction therapy (surgical myectomy or alcohol ablation) cures HCM. Fact: While septal reduction therapy effectively relieves obstruction and improves symptoms in appropriate candidates, it does not correct the underlying genetic abnormality or cure the disease. Patients require ongoing care and monitoring for potential progression of other disease aspects including diastolic dysfunction, arrhythmias, and non-outflow related complications. The primary benefit is hemodynamic and symptomatic improvement rather than modification of the underlying disease process, though long-term outcomes are excellent with appropriate patient selection.
Myth 10: HCM cannot be treated during pregnancy and poses prohibitive risk to mother and baby. Fact: The majority of women with HCM tolerate pregnancy well with appropriate management. While pregnancy does involve hemodynamic changes that can exacerbate HCM symptoms (increased blood volume, heart rate, cardiac output), these can generally be managed with careful monitoring and medication adjustments. Beta-blockers are considered safe during pregnancy and can be continued or initiated if needed. High-risk features requiring special attention include severe obstruction, heart failure symptoms pre-pregnancy, and significant arrhythmias. Multidisciplinary care involving cardiology and high-risk obstetrics is recommended.
Impact on specific populations or professions
Athletes and Sports Participants:
Elite Athletes with HCM:
Diagnostic Challenges:
- Overlap between athlete’s heart and mild HCM
- Gray zone of wall thickness (13-15mm)
- Similar ECG patterns in some cases
- Differentiation strategies:
- Family history assessment
- Genetic testing
- Detraining effects
- Diastolic function evaluation
- Pattern of hypertrophy
- CMR tissue characterization
- Importance of specialized sports cardiology expertise
Career Impact:
- Historically mandatory disqualification from competitive sports
- Evolution toward shared decision-making approach
- High-profile cases of athletes playing with known HCM
- Specific considerations:
- Sport and position (static vs. dynamic components)
- Phenotype severity
- Risk factor profile
- Psychological impact of restriction
- Legal and insurance implications
- Advanced monitoring options
Risk Mitigation Strategies:
- Customized emergency action plans
- Courtside/fieldside AED availability
- Specific hydration protocols
- Environmental adaptation strategies
- External defibrillator vests
- Targeted medication timing
- Symptom recognition education
Recreational Sports Participants:
Activity Guidelines Evolution:
- Historical strict limitations
- Current individualized approach based on:
- Obstruction severity
- Arrhythmia burden
- Fibrosis extent
- Functional capacity
- Risk factor profile
- Patient preference after informed discussion
- Benefits of appropriate exercise now recognized
- Focus on type rather than prohibition
Specific Recommendations:
- Adequate warm-up and cool-down periods
- Avoidance of peak-and-trough exertion patterns
- Hydration emphasis before, during, and after
- Environmental modifications (temperature, altitude)
- Heart rate monitoring guidelines
- Recognition of warning symptoms
- Companion awareness and preparation
Children and Adolescents with HCM:
School-Age Considerations:
Educational Accommodations:
- Physical education modifications:
- Activity type rather than exclusion
- Self-monitoring education
- Rest breaks as needed
- Alternative activities during high-exertion units
- Heat accommodation during outdoor activities
- Hydration access throughout day
- Medical emergency action plans
- Staff training in AED use
- Balance of safety with normal development
- Avoiding unnecessary restrictions
- Physical education modifications:
Psychosocial Impact:
- Identity development challenges
- Peer relationship effects
- Risk of overprotection
- Anxiety about condition
- Sport participation limitations
- Educational approaches:
- Age-appropriate disease education
- Peer education when appropriate
- Support groups with age peers
- Gradual transition to self-management
- Focus on capabilities rather than limitations
Transition to Adulthood:
Healthcare Transition:
- Planned transition from pediatric to adult care
- Overlap period with both providers
- Self-management skill development
- Medical decision-making participation
- Medication management responsibility
- Recognition of changing risk with age
- Adult team introduction before transfer
Life Development Considerations:
- Career counseling considering condition
- College selection and planning
- Independent living preparation
- Driving considerations and guidance
- Risk-taking behavior education
- Substance use counseling
- Reproductive planning discussions
- Insurance and healthcare navigation
Women with HCM:
Gender-Specific Considerations:
Diagnosis and Recognition:
- Often diagnosed later than men
- Symptoms sometimes attributed to anxiety
- Higher symptom burden at diagnosis
- More frequent misdiagnosis
- Higher prevalence of obstructive physiology
- Different remodeling patterns
- Often smaller absolute wall thickness but greater relative to body size
Treatment Response Differences:
- Often better response to septal reduction therapy
- More symptomatic benefit from beta-blockers
- Higher heart rate targets may be needed
- Calcium channel blocker effects more pronounced
- Medication dose adjustments often required
- Different side effect profiles
Reproductive Health:
Contraception Considerations:
- Estrogen-containing contraceptives generally safe
- Progestin-only options if risk factors for thrombosis
- IUD options well-tolerated
- Barrier methods without restrictions
- Coordinated decision-making between cardiology and gynecology
- Individual assessment rather than blanket restrictions
Pregnancy Management:
- Preconception counseling recommended
- Most women tolerate pregnancy well
- Multidisciplinary approach:
- High-risk obstetrics
- Cardiology
- Anesthesiology
- Genetics (for inheritance counseling)
- Medication adjustments (beta-blockers generally safe)
- Monitoring schedule typically:
- Each trimester if stable
- More frequent with symptoms or high-risk features
- Echo assessment of gradient in third trimester
- Delivery planning:
- Vaginal delivery generally preferred
- Adequate pain management to reduce stress
- Management of fluid shifts
- Monitoring during immediate postpartum period
- Special considerations for specific phenotypes:
- Severe obstruction may require more intervention
- Heart failure symptoms need closer monitoring
- Arrhythmia history requires enhanced vigilance
Occupation-Specific Impacts:
High-Risk or Safety-Sensitive Occupations:
Commercial Transportation:
- Commercial pilots: Regulatory restrictions vary by country
- Commercial drivers: Individual assessment, syncope risk key consideration
- Train operators: Similar concerns as commercial drivers
- Considerations:
- Risk of sudden incapacitation
- Third-party risk
- Regulatory requirements
- Individual phenotype and risk assessment
- Monitoring options
- Treatment optimization
- Decisions highly individualized based on specific duties and risk profile
Military Service:
- General exclusion from combat roles in most countries
- Possible non-combat positions based on:
- Phenotype severity
- Symptom profile
- Special skill sets
- Branch-specific policies
- Challenges with extreme environments (heat, altitude)
- Medication access during deployment
- Each country has specific policies
Emergency Response Roles:
- Firefighting: Heat, dehydration, and physical demands create challenges
- Law enforcement: Variable depending on specific role and requirements
- Paramedics/EMTs: Often compatible with diagnosis
- Individualized fitness for duty evaluations
- Adaptive equipment or position modifications sometimes possible
- Focus on specific job requirements rather than diagnosis alone
Physically Demanding Occupations:
Manual Labor:
- Construction: Heat exposure and isometric activity present challenges
- Agriculture: Environmental exposure and remote locations
- Mining: Heat, confined spaces, and remote medical access
- Warehouse/Logistics: Lifting and environmental considerations
- Adaptations:
- Work-rest cycles
- Enhanced hydration protocols
- Temperature-controlled environments when possible
- Mechanical assistance for heaviest tasks
- Buddy systems in high-risk settings
- Activity monitoring technology
Outdoor Work:
- Forestry/Conservation: Remote locations and physical demands
- Landscaping/Grounds: Heat exposure and exertion
- Road construction: Environmental challenges
- Adaptations:
- Scheduling around weather conditions
- Enhanced heat precautions
- Communication devices for remote settings
- Modified work duties during extreme conditions
- Regular access to hydration and cooling
Social and Economic Factors:
Insurance and Financial Impacts:
Life Insurance:
- Often denied or highly rated
- Improved with comprehensive medical documentation
- Specialty insurers for substandard risks
- Group policies through employers may be better option
- Impact of genetic testing results
- Variation in practices by country and insurer
Health Insurance:
- Pre-existing condition issues in some countries
- High-risk pool placement
- Premium increases common
- Coverage limitations for specialty care
- Genetic discrimination protections vary by country
- Medication coverage challenges, especially newer therapies
Disability Insurance:
- Occupation-specific considerations
- Often available with exclusions or limitations
- Important for those in physically demanding roles
- Benefit period and definition considerations
- Best obtained before diagnosis when possible
- Employer-provided options often more accessible
Social and Relationship Effects:
Family Planning:
- Genetic counseling importance
- Reproductive options including:
- Natural conception with prenatal testing
- Preimplantation genetic diagnosis
- Donor gametes
- Adoption
- Complex decision-making process
- Impact of parent’s disease severity on perspective
- Psychological support during decision process
- Genetic test results significantly impact options
Relationship Dynamics:
- Explaining condition to partners
- Impact of activity limitations on shared experiences
- Caregiver burden in advanced cases
- Hereditary implications for future children
- Sexual activity considerations
- Balancing protection with independence
- Support resources for partners and families
This comprehensive report on Hypertrophic Cardiomyopathy (HCM) provides an evidence-based overview of this complex cardiovascular condition, covering epidemiology, genetics, clinical manifestations, diagnosis, and management. While every effort has been made to include the most current information, medical understanding continues to evolve, and consultation with healthcare providers is essential for individual patient care decisions.