
⚠️ Disclaimer: The information provided in this article is for educational purposes only and does not constitute medical advice. RevisionTown does not provide diagnosis, treatment, or medical recommendations. Always consult a qualified healthcare professional regarding any medical condition, symptoms, or concerns.
Read More – 🏥 Medical Disclaimer
1. Overview
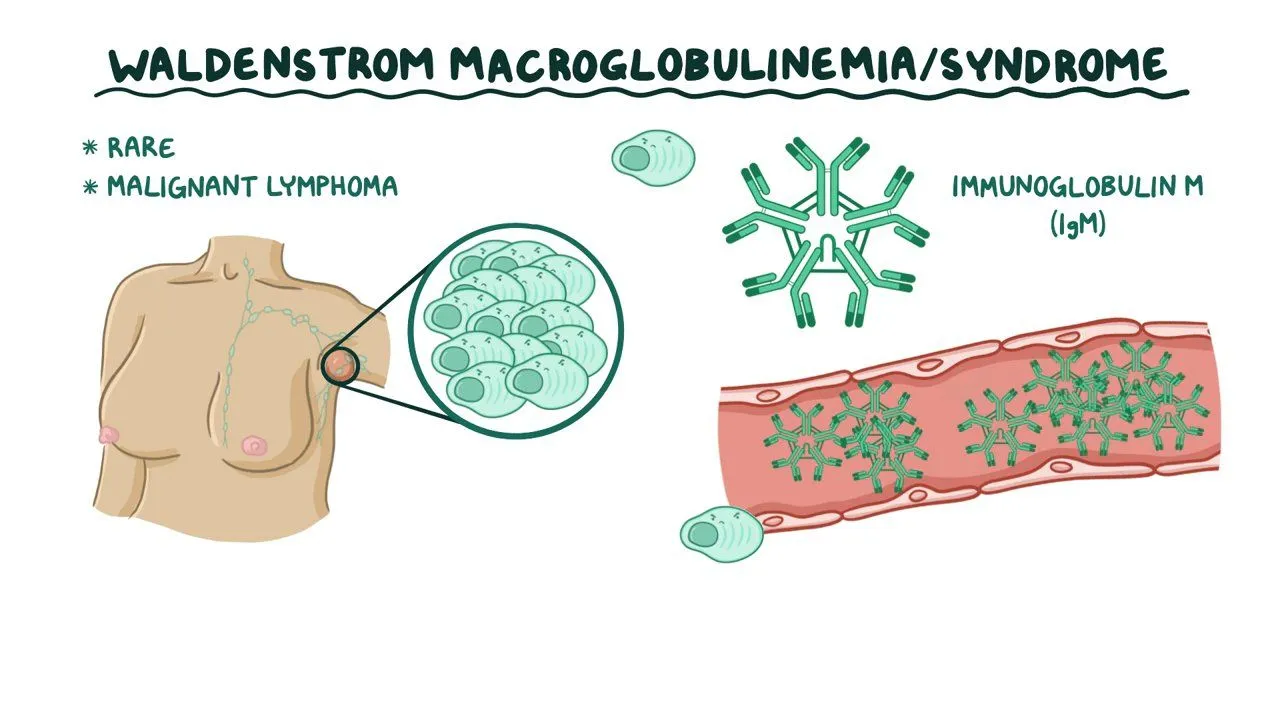
Waldenström macroglobulinemia (WM) is a rare type of slow-growing blood cancer classified as a non-Hodgkin lymphoma. It is characterized by an excess of abnormal white blood cells called B lymphocytes in the bone marrow, which produce large amounts of an abnormal protein called immunoglobulin M (IgM).
The disease primarily affects the bone marrow, lymph nodes, and spleen. The overproduction of IgM can cause the blood to become thick (a condition called hyperviscosity syndrome), which affects circulation and can lead to various complications.
In terms of prevalence, WM is considered rare, with an annual incidence of approximately 3 to 5 cases per million people. It accounts for approximately 1-2% of all hematologic malignancies. The disease is more common in older adults, with a median age at diagnosis of 65-70 years, and is slightly more prevalent in males than females. While rare, WM is significant because it requires careful management due to its chronic nature and potential complications.
2. History & Discoveries
Waldenström macroglobulinemia was first identified in 1944 by the Swedish physician Jan Gösta Waldenström (1906-1996). Dr. Waldenström described two patients with a condition characterized by oronasal bleeding, anemia, elevated erythrocyte sedimentation rate, lymphadenopathy, and a high concentration of a macroglobulin (now known as IgM) in the blood.
The discovery was significant because it identified a distinct clinical entity separate from other known blood disorders. Throughout the decades following its discovery, the understanding of WM evolved considerably:
- 1950s-1960s: The abnormal protein was identified as IgM and recognized as a product of abnormal B lymphocytes.
- 1970s-1980s: Advances in immunology provided better understanding of the cellular origin of the disease.
- 1990s: Introduction of flow cytometry and molecular testing improved diagnosis.
- 2000s: A major breakthrough occurred with the identification of the MYD88 L265P mutation in approximately 90% of WM patients.
- 2015: The FDA approved ibrutinib as the first drug specifically for WM, marking a significant milestone in treatment.
The evolution of WM understanding has transitioned from a purely clinical description to a molecularly defined entity, allowing for more targeted therapeutic approaches.
3. Symptoms
WM symptoms can vary widely among patients, with some remaining asymptomatic for years.
Early symptoms:
- Fatigue and weakness (often due to anemia)
- Unexplained weight loss
- Fever without apparent cause
- Night sweats
- Enlarged lymph nodes (lymphadenopathy)
- Headaches and blurred vision
- Easy bruising or bleeding, particularly from the nose and gums
Advanced-stage symptoms:
- Severe hyperviscosity syndrome characterized by:
- Visual disturbances including blurred vision and retinal hemorrhages
- Neurologic symptoms such as headache, dizziness, and vertigo
- Altered mental status
- Raynaud’s phenomenon (poor circulation to fingers and toes)
- Peripheral neuropathy (numbness, tingling, burning in extremities)
- Recurrent infections due to compromised immune function
- Hepatosplenomegaly (enlarged liver and spleen)
Common vs. rare symptoms: Common symptoms include fatigue, weakness, and unexplained weight loss, affecting 60-80% of patients. Rare manifestations include Bing-Neel syndrome (CNS involvement), occurring in less than 1% of cases, and amyloidosis (protein deposition in tissues), seen in about 5-10% of patients.
Symptom progression tends to be slow, often over years rather than months, reflecting the indolent nature of the disease. However, the rate of progression can vary significantly between individuals.
4. Causes
The exact cause of WM remains incompletely understood, but several biological factors have been identified:
Biological causes:
- The MYD88 L265P mutation is present in approximately 90% of WM cases, affecting a signaling pathway that promotes B-cell survival and proliferation.
- CXCR4 mutations occur in approximately 30-40% of patients, potentially influencing disease progression and treatment response.
- Chromosome abnormalities, particularly deletions in chromosomes 6q, 13q, and 17p, are observed in many WM patients.
Environmental causes:
- Some studies suggest associations with:
- Exposure to certain chemicals (solvents, pesticides, herbicides)
- Prior radiation exposure
- Hepatitis C virus infection (though the evidence is limited)
Genetic and hereditary factors:
- First-degree relatives of WM patients have a 20-fold increased risk of developing WM or related B-cell disorders.
- Familial predisposition is observed in approximately 20% of cases, suggesting genetic components.
- Specific inherited genetic variants that increase susceptibility are under investigation.
No definitive external triggers have been confirmed, though chronic antigenic stimulation from infections or autoimmune conditions may play a role in some cases.
5. Risk Factors
Demographic risk factors:
- Age: Risk increases with age, with median age at diagnosis being 65-70 years. WM is rare before age 40.
- Gender: Men are affected approximately 1.5-2 times more frequently than women.
- Ethnicity: Higher incidence in Caucasians, particularly those of Northern European descent, and lower incidence in Asian populations.
Environmental and occupational factors:
- Exposure to certain chemicals in agricultural, leather, rubber, and painting industries has been associated with increased risk.
- Radiation exposure may contribute to risk.
Genetic factors:
- Family history of WM or other B-cell lymphoproliferative disorders increases risk.
- Specific genetic polymorphisms related to immune function may contribute to susceptibility.
Pre-existing conditions:
- Certain autoimmune disorders, particularly Sjögren’s syndrome, have been associated with increased WM risk.
- Monoclonal gammopathy of undetermined significance (MGUS) of IgM type is considered a precursor state, with approximately 1.5-2% of patients progressing to WM annually.
- Hepatitis C infection has been implicated in some studies, though the association remains unclear.
6. Complications
WM can lead to various complications affecting multiple organ systems:
Hyperviscosity syndrome:
- Occurs in approximately 10-30% of patients
- Can cause visual disturbances, neurological symptoms, and cardiovascular problems
- May lead to heart failure or stroke if severe and untreated
Cryoglobulinemia:
- Proteins in the blood precipitate at cold temperatures
- Causes poor circulation, particularly in extremities
- Can lead to skin ulcers and tissue damage
Peripheral neuropathy:
- Affects approximately 20-25% of patients
- Can be disabling and significantly reduce quality of life
- May be irreversible even with successful WM treatment
Amyloidosis:
- Deposition of amyloid protein in tissues
- Can affect heart, kidneys, liver, and nervous system
- Associated with poorer prognosis
Increased susceptibility to infections:
- Due to compromised immune function
- Respiratory and urinary tract infections are common
- Can be life-threatening, particularly in elderly patients
Long-term impacts:
- Chronic fatigue and reduced quality of life
- Potential for transformation to more aggressive lymphoma (rare, <5% of cases)
- End-organ damage, particularly to kidneys and nervous system
Mortality:
- Five-year survival rates range from 60-90% depending on age, comorbidities, and risk stratification
- Median survival has improved significantly with newer treatments, now exceeding 10 years for many patients
- Primary causes of death include disease progression, complications from treatment, and infections
7. Diagnosis & Testing
Diagnostic criteria and procedures:
- Diagnosis requires:
- Detection of IgM monoclonal protein (M-protein) in serum
- Bone marrow infiltration by lymphoplasmacytic cells
- Immunophenotypic confirmation of clonal B-cells
Specific tests:
Blood tests:
- Complete blood count (CBC) – often shows anemia
- Comprehensive metabolic panel
- Serum protein electrophoresis (SPEP) and immunofixation to detect and quantify M-protein
- IgM level measurement
- Beta-2 microglobulin (prognostic marker)
- Serum free light chain assay
Bone marrow assessment:
- Bone marrow aspiration and biopsy – the gold standard for diagnosis
- Flow cytometry to characterize lymphocyte populations
- Immunohistochemistry to identify specific cellular markers
- FISH (Fluorescence In Situ Hybridization) for chromosomal abnormalities
- Molecular testing for MYD88 L265P and CXCR4 mutations
Imaging studies:
- CT scans to assess lymphadenopathy and organomegaly
- PET-CT scans may be used to evaluate disease extent
- MRI for specific concerns, particularly neurologic symptoms
Additional specialized tests:
- Plasma viscosity measurement for hyperviscosity syndrome
- Cryoglobulin testing if symptoms suggest cryoglobulinemia
- Nerve conduction studies for peripheral neuropathy
- Fundoscopic examination for retinal changes
Early detection: No routine screening tests exist for the general population due to the rarity of WM. Early detection typically occurs incidentally during blood tests performed for other reasons or when investigating nonspecific symptoms like fatigue. The IgM MGUS precursor state is sometimes identified during routine medical evaluations and can be monitored for progression to WM.
8. Treatment Options
Treatment for WM is not always initiated at diagnosis, particularly for asymptomatic patients. The approach is highly individualized based on symptoms, disease burden, and patient factors.
Standard treatment protocols:
Watchful waiting:
- Appropriate for asymptomatic patients
- Regular monitoring without active treatment
- 30-40% of patients may not require immediate treatment at diagnosis
First-line treatments:
- Chemoimmunotherapy combinations:
- Bendamustine plus rituximab (BR) – often preferred for fit patients
- Rituximab, cyclophosphamide, and dexamethasone (RCD)
- Bortezomib, dexamethasone, and rituximab (BDR)
- BTK inhibitors:
- Ibrutinib (FDA-approved specifically for WM)
- Zanubrutinib (approved in 2021, showing improved efficacy and reduced toxicity)
- Plasmapheresis:
- For urgent management of hyperviscosity syndrome
- Mechanical removal of excess IgM from the blood
- Temporary measure, usually followed by systemic treatment
Salvage/relapsed disease treatments:
- Different chemoimmunotherapy regimen than used initially
- Alternative BTK inhibitor
- Proteasome inhibitors (e.g., bortezomib, carfilzomib)
- Venetoclax (BCL-2 inhibitor)
- PI3K inhibitors (e.g., idelalisib)
Emerging treatments and clinical trials:
- Combination therapies with novel agents
- Second-generation BTK inhibitors with improved specificity
- CAR-T cell therapy (in early investigational stages)
- Bispecific antibodies targeting B-cell markers
- Selective CXCR4 antagonists, particularly for patients with CXCR4 mutations
Stem cell transplantation:
- Autologous stem cell transplantation may be considered for eligible younger patients with high-risk disease
- Allogeneic transplantation is rarely used due to high treatment-related mortality
Treatment selection is increasingly guided by genetic profiling, particularly MYD88 and CXCR4 mutation status, allowing for more personalized therapeutic approaches.
9. Prevention & Precautionary Measures
Due to the idiopathic nature of WM and incomplete understanding of its causes, specific preventive measures remain limited:
Primary prevention:
- No established preventive strategies exist for WM
- General cancer prevention measures include:
- Avoiding exposure to known carcinogens and chemicals linked to lymphomas
- Maintaining healthy lifestyle habits
- Limiting radiation exposure when medically feasible
Risk reduction for those with predisposition:
- Regular medical check-ups for those with family history
- Monitoring of IgM MGUS patients with annual:
- Serum protein electrophoresis
- Complete blood count
- Clinical evaluation for symptoms
Management precautions for diagnosed patients:
Infection prevention strategies are important:
- Vaccination (influenza, pneumococcal, COVID-19)
- Proper hand hygiene
- Avoiding crowded areas during peak infection seasons
- Prompt treatment of infections
Avoiding extreme cold if cryoglobulinemia is present
Regular ophthalmologic examination if hyperviscosity is a concern
Monitoring for early signs of peripheral neuropathy to allow dose adjustment of neurotoxic medications
No specific screening recommendations exist for the general population due to the disease’s rarity. However, individuals with first-degree relatives affected by WM may benefit from increased vigilance and earlier investigation of suspicious symptoms.
10. Global & Regional Statistics
Global incidence and prevalence:
- Annual global incidence: approximately 3-5 cases per million population
- Estimated prevalence: 30-50 cases per million
- Approximately 1,500-2,000 new cases diagnosed annually in the United States
- Total WM patients worldwide estimated at 60,000-80,000
Regional variations:
- Higher incidence in North America and Northern Europe
- Lower incidence in Asian countries, particularly Japan and China
- Lowest reported rates in African and South American populations
Mortality and survival rates:
- Five-year relative survival rate: approximately 78%
- Ten-year relative survival rate: approximately 66%
- Median overall survival has improved from 5-6 years in the 1990s to >10 years currently
- Mortality rates have declined by approximately 30% over the past two decades with improved treatments
Age and gender distribution:
- Median age at diagnosis: 65-70 years
- Male to female ratio: approximately 2:1
- Extremely rare in individuals under 40 years of age (<2% of cases)
Temporal trends:
- Slight increase in reported incidence over time, likely due to improved diagnostic techniques
- Declining mortality rates due to novel therapies
- Increasing prevalence due to improved survival
These statistics demonstrate both the rarity of WM and the progress made in improving patient outcomes over recent decades.
11. Recent Research & Future Prospects
Recent research advancements:
Genomic landscape characterization:
- Beyond MYD88 and CXCR4, whole genome sequencing has identified additional recurrent mutations (e.g., ARID1A, CD79B)
- Epigenetic alterations and their role in WM pathogenesis are being explored
Novel therapeutic approaches:
- Second-generation BTK inhibitors (zanubrutinib, acalabrutinib, pirtobrutinib) with improved efficacy and reduced toxicity
- BCL-2 inhibitor venetoclax showing promising results in clinical trials
- Combination therapy approaches to prevent resistance development
Biomarker development:
- Circulating tumor DNA (ctDNA) for non-invasive monitoring
- Metabolomic profiles for treatment response prediction
- Refined risk stratification models incorporating molecular markers
Ongoing clinical trials:
- Combination studies of BTK inhibitors with anti-CD38 antibodies
- Evaluation of chimeric antigen receptor (CAR) T-cell therapy targeting B-cell markers
- CXCR4 antagonists for patients with CXCR4 mutations
- Immunomodulatory approaches targeting the tumor microenvironment
Future therapeutic directions:
- Development of MYD88-specific inhibitors targeting the fundamental driver mutation
- Expanded use of circulating tumor DNA for minimal residual disease monitoring
- Immunotherapy approaches exploiting WM’s genetic vulnerabilities
- Machine learning algorithms for personalized treatment selection
- Time-limited treatment strategies to maintain efficacy while reducing toxicity
Curative approaches under investigation:
- Modified cellular therapies with improved safety profiles
- Combination strategies targeting multiple pathways simultaneously
- Novel immunotherapeutic approaches (bispecific antibodies, checkpoint inhibitors)
While WM remains incurable with conventional approaches, the rapid advances in targeted therapies and immunotherapies present promising avenues for achieving deeper and more durable remissions, potentially approaching functional cures for some patients.
12. Interesting Facts & Lesser-Known Insights
Historical and epidemiological curiosities:
- Jan Waldenström initially described the disease in two patients who presented with oronasal bleeding, anemia, and lymphadenopathy in 1944, but the disease wasn’t officially classified as a distinct entity until decades later.
- WM has one of the highest hereditary predispositions among blood cancers, with approximately 20% of patients having relatives with WM or related B-cell disorders.
Unique clinical features:
- “Schnitzler syndrome,” a rare manifestation associated with WM, presents with chronic urticaria, fever, and bone pain along with the typical IgM monoclonal gammopathy.
- Some WM patients experience a phenomenon called “flare” when starting rituximab treatment, where symptoms temporarily worsen due to rapid release of IgM from dying tumor cells.
Biological peculiarities:
- WM cells typically do not express CD5, a marker commonly found in chronic lymphocytic leukemia, another B-cell malignancy that can sometimes be confused with WM.
- The MYD88 L265P mutation found in 90% of WM cases is relatively rare in other lymphomas, making it a valuable diagnostic marker.
Myths and misconceptions:
- Contrary to common belief, WM is not always a disease of the elderly; approximately 10-15% of patients are diagnosed before age 50.
- While often described as “indolent,” WM can be aggressive in some patients, requiring immediate and intensive treatment.
- IgM levels do not always correlate with symptom severity; some patients with high IgM levels remain asymptomatic while others with relatively lower levels may have significant symptoms.
Clinical research insights:
- WM has served as a model disease for understanding how specific genetic mutations can drive cancer development and be targeted therapeutically.
- The success of BTK inhibitors in WM has influenced treatment approaches for other B-cell malignancies.
- Ibrutinib was approved for WM based on a relatively small study (63 patients), highlighting the challenges of conducting large clinical trials in rare diseases.
Impact on specific populations:
- Firefighters have been reported to have a higher incidence of WM in some epidemiological studies, possibly due to chemical exposures.
- Individuals with autoimmune conditions, particularly Sjögren’s syndrome, have an increased risk of developing WM.
- First-degree relatives of WM patients are often advised to inform their physicians about their family history, as early symptoms may be mistaken for more common conditions.
These lesser-known aspects of WM illustrate the complexity of this rare disease and the substantial progress made in understanding its unique biology and clinical manifestations.