
⚠️ Disclaimer: The information provided in this article is for educational purposes only and does not constitute medical advice. RevisionTown does not provide diagnosis, treatment, or medical recommendations. Always consult a qualified healthcare professional regarding any medical condition, symptoms, or concerns.
Read More – 🏥 Medical Disclaimer
What is Syphilis?
Syphilis is a sexually transmitted infection (STI) caused by the bacterium Treponema pallidum, specifically the subspecies T. pallidum pallidum. This gram-negative spirochete bacterium cannot survive outside the human body for extended periods and is primarily transmitted through direct contact with syphilitic sores (chancres) during vaginal, anal, or oral sex. The disease can also be transmitted from an infected mother to her baby during pregnancy or childbirth (congenital syphilis) and, rarely, through blood transfusions or organ transplants.
Concise Definition
Syphilis is a chronic systemic bacterial infection characterized by distinct clinical stages (primary, secondary, latent, and tertiary) that can affect virtually any organ system in the body. If left untreated, the disease progresses through these stages over decades, potentially causing severe complications including cardiovascular disease, neurological disorders, and death. The infection is remarkably adaptable, with the causative organism able to evade the immune system by altering its antigenic surface and establishing persistent infection.
Affected Body Parts/Organs
Syphilis is a truly systemic disease that can affect multiple organ systems throughout its various stages:
Primary Stage:
- Skin and mucous membranes (site of initial infection)
- Regional lymph nodes
Secondary Stage:
- Skin (generalized rash)
- Mucous membranes (oral, genital, anal)
- Lymph nodes (generalized lymphadenopathy)
- Eyes (ocular syphilis)
- Liver (hepatitis)
- Kidney (glomerulonephritis)
- Joints (arthralgia, arthritis)
Tertiary Stage:
- Cardiovascular system (aortic aneurysms, aortitis)
- Central nervous system (neurosyphilis)
- Skeletal system (gummas in bones)
- Skin (gummatous lesions)
- Other organs (spleen, liver, lungs, stomach)
Congenital Syphilis:
- Nervous system
- Bones and teeth
- Eyes
- Ears
- Skin
- Nasal cartilage
Prevalence and Significance
Global Prevalence:
- WHO estimates approximately 6.3 million people have syphilis worldwide
- Annual incidence: 6 million new cases per year
- Global prevalence rate: 0.5% of population aged 15-49
Epidemiological Significance:
- Fourth most common STI globally after chlamydia, gonorrhea, and trichomoniasis
- Remains a major public health concern despite effective treatment availability
- Increasing rates globally after decade of decline (2000-2010)
- Particular concern in men who have sex with men (MSM) populations
- Co-infection with HIV significantly increases transmission and progression
Clinical Significance:
- Complications: Untreated syphilis can cause irreversible damage to multiple organ systems
- Transmission Risk: Highly infectious during primary and secondary stages
- Pregnancy Complications: Congenital syphilis can cause stillbirth, neonatal death, and severe disabilities
- HIV Co-infection: Increases HIV viral load and risk of transmission; facilitates HIV acquisition
- Diagnostic Challenges: Long latent period can delay diagnosis and treatment
Economic Impact:
- Direct healthcare costs: Billions annually worldwide
- Indirect costs: Lost productivity, disability care, pregnancy complications
- Cost-effective prevention and treatment available
- Early detection significantly reduces healthcare burden
Public Health Importance:
- Indicator of overall STI control program effectiveness
- Sentinel for high-risk sexual behaviors
- Requires comprehensive contact tracing and partner notification
- Demonstrates antimicrobial resistance concerns (though T. pallidum remains universally sensitive to penicillin)
- Important component of antenatal screening programs
2. History & Discoveries
Origins and Early Recognition
First Historical Records:
- First documented outbreak in Europe: 1495 during the French siege of Naples
- Multiple theories about origins:
- Columbian Theory: Brought to Europe from the Americas by Columbus’s crew
- Pre-Columbian Theory: Existed in Europe before 1492, possibly confused with other diseases
- Unitary Theory: Related to yaws, endemic syphilis, and pinta (all caused by different treponemes)
Early Names and Descriptions:
- “French Disease” (by Italians)
- “Italian Disease” (by French)
- “Spanish Disease” (by northern Europeans)
- “Great Pox” (to distinguish from smallpox)
- Named “syphilis” in 1530 by Girolamo Fracastoro in his poem about the shepherd Syphilus
Key Historical Figures and Discoveries
Girolamo Fracastoro (1478-1553):
- Italian physician and poet
- Coined the term “syphilis” in 1530
- Described three stages of the disease
- Proposed the contagion theory
Hunter and the Self-Inoculation Experiment (1767):
- John Hunter intentionally inoculated himself with pus from a patient with gonorrhea
- Developed symptoms of both gonorrhea and syphilis (patient had both infections)
- Concluded incorrectly that they were the same disease
- This error influenced medical practice for decades
Augustus Quirinus Rivinus (1652-1723):
- Distinguished syphilis from other diseases
- Described detailed pathological changes
Fritz Schaudinn and Erich Hoffmann (1905):
- Discovered Treponema pallidum
- Used dark-field microscopy to visualize the spirochete
- Landmark achievement in understanding the causative agent
August von Wassermann (1906):
- Developed the first blood test for syphilis
- Wassermann test became standard diagnostic tool for decades
- Based on complement fixation
Paul Ehrlich (1909-1910):
- Developed Salvarsan (arsphenamine), first effective treatment
- “Magic bullet” concept of targeted chemotherapy
- Nobel Prize winner for immunology work
Alexander Fleming (1910s):
- Demonstrated arsenical drugs’ effectiveness against syphilis
- Before discovering penicillin, worked on syphilis treatment
John Mahoney (1943):
- Demonstrated penicillin’s effectiveness against syphilis
- Landmark study at Staten Island Marine Hospital
- Established penicillin as treatment of choice
Major Breakthroughs and Evolution of Understanding
19th Century Advances:
- 1838: Philippe Ricord distinguished gonorrhea from syphilis
- 1863: Discovery of aortic involvement (cardiovascular syphilis)
- 1879: Jean Alfred Fournier described juvenile general paralysis (congenital neurosyphilis)
- 1880s: Recognition of three stages: primary, secondary, tertiary
20th Century Milestones:
- 1906: Wassermann test revolutionized diagnosis
- 1909: Salvarsan introduced, first effective treatment
- 1910s: Malarial therapy for neurosyphilis (Wagner-Jauregg, Nobel Prize 1927)
- 1943: Penicillin proven effective
- 1950s: RPR (Rapid Plasma Reagin) test developed
- 1960s: TPPA (Treponema pallidum particle agglutination) introduced
- 1980s: HIV/AIDS epidemic changed syphilis epidemiology
- 1990s: PCR techniques for diagnosis
Modern Era Developments:
- 2000s: Molecular typing of T. pallidum strains
- 2010s: Whole genome sequencing of clinical isolates
- 2020s: Point-of-care testing advances
- Ongoing: Vaccine development efforts
Ethical Controversies and Historical Lessons
Tuskegee Syphilis Study (1932-1972):
- Unethical study by U.S. Public Health Service
- 600 poor African American men (399 with latent syphilis, 201 controls)
- Participants told they were receiving treatment for “bad blood”
- Denied treatment even after penicillin became available
- Led to major reforms in research ethics and informed consent
Guatemala Syphilis Experiments (1946-1948):
- Deliberately infected prisoners, soldiers, and psychiatric patients
- Conducted without consent
- Revealed in 2010, led to formal apology from U.S. government
Cultural and Social Impact
Historical Social Consequences:
- Stigmatization of affected individuals
- Influence on marriage laws and public health policies
- Impact on military recruitment and service
- Development of modern STI prevention programs
- Shaped attitudes toward sex education and condom use
Artistic and Literary References:
- Featured in works by Voltaire, Heinrich Heine, Charles Baudelaire
- Influenced prostitution laws and social purity movements
- Subject of numerous medical texts and public health campaigns
The history of syphilis demonstrates the evolution of medical understanding, diagnostic techniques, and treatment approaches. From its mysterious appearance in Renaissance Europe to modern molecular biology, the disease has served as a model for infectious disease research and public health responses. The ethical violations in historical studies led to fundamental reforms in medical research ethics, making syphilis not just a medical condition but a touchstone for discussions about research ethics, healthcare equity, and social justice in medicine.
3. Symptoms
Clinical Stages Overview
Syphilis typically progresses through four distinct stages if left untreated, each with characteristic symptoms and manifestations:
- Primary Stage
- Secondary Stage
- Latent Stage (Early and Late)
- Tertiary Stage
Primary Syphilis
Timeline: 10-90 days after exposure (average 21 days)
Characteristic Features:
- Chancre: Painless, circular, firm ulcer at infection site
- Usually single, but multiple chancres possible
- 0.5-2 cm in diameter
- Clean base with indurated (hardened) edges
- Non-tender unless secondarily infected
- Heals spontaneously in 3-6 weeks even without treatment
Common Locations:
- Penis (glans, shaft, foreskin)
- Vulva, vagina, cervix
- Anus and rectum
- Lips, tongue, throat
- Fingers (healthcare workers)
- Nipples (breastfeeding)
Associated Symptoms:
- Regional lymphadenopathy (enlarged lymph nodes)
- Typically bilateral and non-tender
- Nodes feel rubbery and mobile
- Usually no systemic symptoms
- Chancre contains numerous spirochetes (highly infectious)
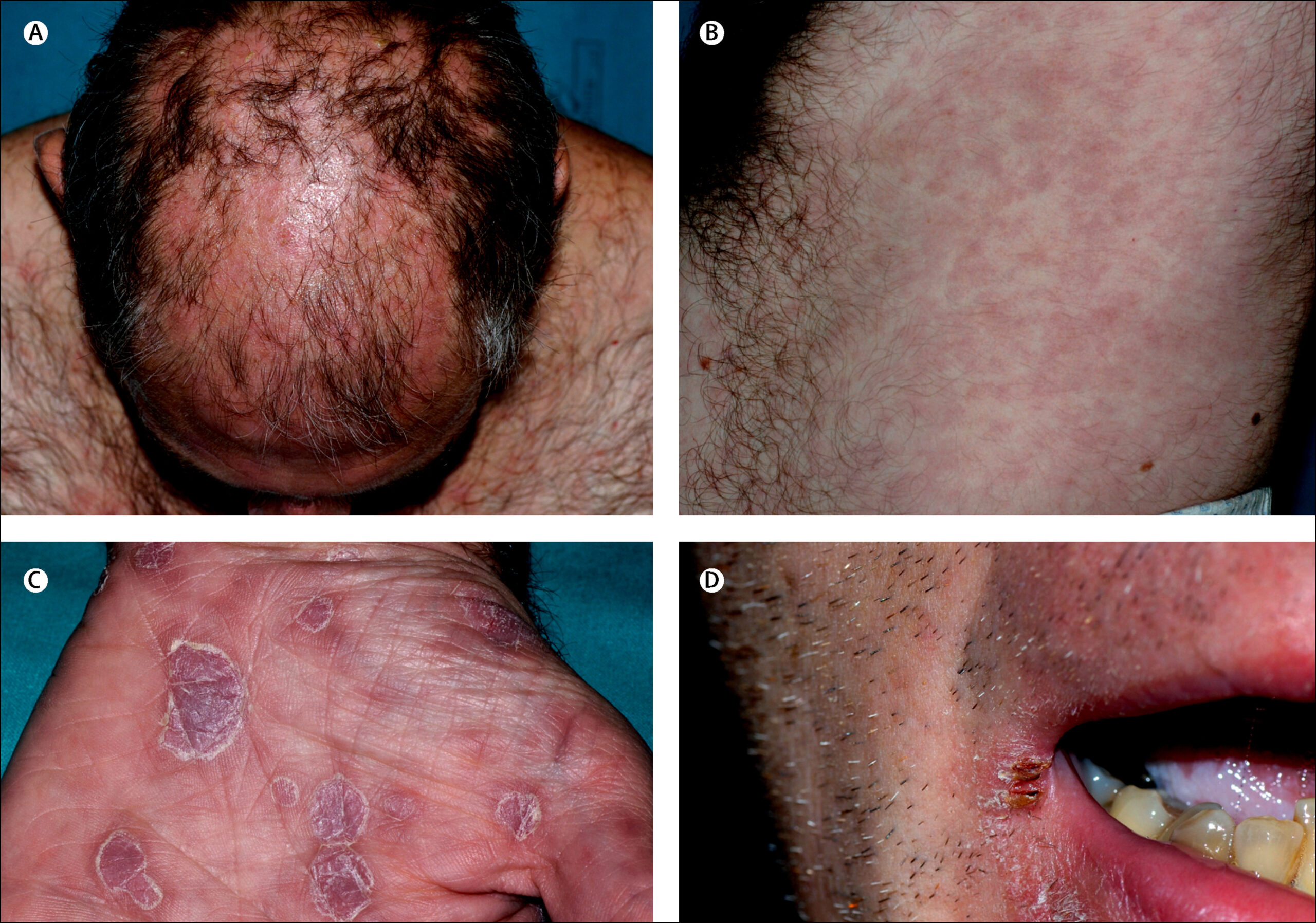
Secondary Syphilis
Timeline: 6-8 weeks after chancre appears (2-6 months after exposure)
Characteristic Features:
- Skin Rash: Most common manifestation
- Typically non-pruritic (non-itchy)
- Starts on trunk, spreads to extremities
- Involves palms and soles (pathognomonic)
- Various presentations:
- Macular (flat, round spots)
- Papular (small raised bumps)
- Pustular (rare, severe cases)
- Annular or psoriasiform (ring-shaped)
Mucocutaneous Manifestations:
- Mucous patches: Superficial, grayish-white ulcerations
- Oral cavity, vagina, anus
- Highly infectious
- Condyloma latum: Moist, wart-like lesions
- Perianal and genital areas
- Different from genital warts (condyloma acuminatum)
Systemic Symptoms:
- Fever (usually low-grade)
- Malaise and fatigue
- Headache
- Myalgia and arthralgia
- Generalized lymphadenopathy
- Weight loss
- Sore throat
- Alopecia (patchy hair loss, “moth-eaten” appearance)
Rare Manifestations:
- Hepatitis with jaundice
- Acute nephrotic syndrome
- Glomerulonephritis
- Gastric syphilis
- Ocular syphilis (eye involvement)
- Meningitis
Latent Syphilis
Definition: Infection without clinical signs or symptoms, diagnosed by serology
Subcategories:
Early Latent Syphilis (≤1 year):
- Higher likelihood of relapse
- Asymptomatic period after secondary stage
- Still infectious (especially first year)
- 25% may experience secondary stage recurrence
Late Latent Syphilis (>1 year):
- Lower transmission risk
- May persist for years or decades
- Can progress to tertiary stage
- No symptoms but infection persists
Clinical Features:
- No symptoms
- Positive serological tests
- No infectious lesions
- Requires careful history and examination
Tertiary Syphilis
Timeline: 3-15 years after initial infection (up to 40+ years)
Three Main Categories:
Cardiovascular Syphilis (80% of tertiary cases):
- Aortitis (inflammation of aorta)
- Aortic aneurysm formation
- Aortic valve insufficiency
- Coronary artery ostial stenosis
- Symptoms: Chest pain, dyspnea, cough, hoarseness
Neurosyphilis:
- Asymptomatic: Abnormal CSF without symptoms
- Meningovascular: Stroke-like symptoms, headache, dizziness
- General paresis: Dementia, personality changes, memory loss
- Tabes dorsalis: Ataxia, shooting pains, incontinence
- Syphilitic myelopathy: Spinal cord involvement
- Optic atrophy: Vision loss
Gummatous Syphilis (least common):
- Gummas: Granulomatous lesions
- Common sites: Skin, bone, liver, tests, brain
- Can ulcerate and destroy tissue
- Usually benign but can cause significant damage
Congenital Syphilis
Early Congenital Syphilis (<2 years):
- Prematurity, low birth weight
- Hepatosplenomegaly
- Jaundice and anemia
- Rhinitis (“snuffles”)
- Skin rash (similar to secondary syphilis)
- Pseudoparalysis
- Osteochondritis and periostitis
- Limb abnormalities
Late Congenital Syphilis (>2 years):
- Hutchinson’s triad:
- Notched incisors
- Interstitial keratitis
- Eighth cranial nerve deafness
- Other features:
- Rhagades (linear scars around mouth)
- Sabre shins (anterior tibial bowing)
- Mulberry molars
- Nasal septum perforation
- Clutton’s joints (bilateral knee effusions)
Symptom Progression and Patterns
Natural History Without Treatment:
- Primary stage: 10-90 days
- Secondary stage: 2-6 months after exposure
- Latent stage: Variable duration
- Tertiary stage: 3-40+ years after initial infection
Progression Rates:
- Approximately 30% of untreated patients develop tertiary syphilis
- 10% develop cardiovascular syphilis
- 5% develop neurosyphilis
- 16% develop gummatous lesions
- Many patients remain in latent stage indefinitely
Factors Affecting Progression:
- Host immune response
- Presence of other infections (especially HIV)
- Age at infection
- Pregnancy status
- Access to partial treatment
Unusual and Atypical Presentations
Malignant Syphilis:
- Rare, severe form
- Extensive skin ulceration
- Rapid progression
- More common in immunocompromised patients
Syphilis d’emblée:
- Primary and secondary stages overlap
- No clear separation between stages
Syphilis Décapitée:
- Secondary stage without preceding chancre
- Possibly due to early treatment of primary stage
Organ-Specific Variants:
- Otosyphilis (hearing loss)
- Ocular syphilis (vision problems)
- Gastric syphilis (stomach involvement)
- Renal syphilis (kidney involvement)
Understanding the varied manifestations of syphilis is crucial for diagnosis, as the disease can mimic numerous other conditions (the “great imitator”). The progression through distinct stages, each with characteristic symptoms, allows for clinical staging and appropriate treatment planning. However, atypical presentations, especially in immunocompromised patients or those with partial treatment, can complicate diagnosis and require careful clinical judgment.
4. Causes
Biological Cause
Causative Organism:
- Treponema pallidum subspecies pallidum
- Gram-negative spirochete bacterium
- Highly motile with corkscrew-like movement
- 6-20 micrometers in length, 0.1-0.2 micrometers in width
- Cannot survive outside the human body for extended periods
- Currently uncultivable in standard laboratory media
Bacterial Characteristics:
Cell Structure:
- Outer membrane contains lipoproteins and lipids
- Periplasmic space with flagella
- Lacks classical gram-negative lipopolysaccharide
- Contains unique outer membrane proteins
Metabolic Features:
- Microaerophilic (requires low oxygen levels)
- Slow replication cycle (30-33 hour doubling time)
- Limited biosynthetic capabilities
- Relies heavily on host for nutrients
Virulence Factors:
- Hyaluronidase (tissue penetration)
- Adhesins for host cell attachment
- Immune evasion mechanisms
- Ability to cross blood-brain and placental barriers
Transmission Mechanisms
Primary Transmission Routes:
Sexual Transmission (90% of cases):
- Vaginal, anal, or oral sex
- Contact with syphilitic sores (chancres)
- Most infectious during primary and secondary stages
- Transmission requires direct contact with infectious lesions
Vertical Transmission (Mother to Child):
- Transplacental transmission
- Can occur at any stage of pregnancy
- Higher risk during primary and secondary stages
- Can result in stillbirth, neonatal death, or congenital syphilis
Blood Transfusion/Organ Transplant:
- Rare in countries with blood screening
- Can occur with fresh blood products
- Organ transplant from infected donor
Occupational Exposure:
- Healthcare workers handling infected materials
- Laboratory workers
- Requires direct contact with infectious material
Environmental and Host Factors
Environmental Conditions Affecting Survival:
- T. pallidum dies quickly outside the human body
- Sensitive to:
- Desiccation (drying)
- Temperature changes
- Soaps and disinfectants
- Oxygen exposure
- Cannot survive on toilet seats, doorknobs, or in swimming pools
Host Factors Influencing Infection:
Immune Status:
- Immunocompromised individuals at higher risk
- HIV co-infection accelerates progression
- Current infection provides no immunity to reinfection
Previous Exposure:
- Prior syphilis infection provides no protective immunity
- Can be reinfected multiple times
- Serological scars may persist after treatment
Pregnancy:
- Hormonal changes may affect disease progression
- Increased risk of transmission to fetus
- Pregnancy does not protect against infection
Age:
- All age groups susceptible
- Congenital form affects newborns
- Tertiary complications more common in older adults
Genetic and Hereditary Factors
Host Genetic Susceptibility:
- No clear genetic predisposition to syphilis infection
- Some variations in immune response genes may affect:
- Disease progression rate
- Symptom severity
- Treatment response
Population Differences:
- No racial or ethnic immunity or resistance
- Socioeconomic factors more important than genetic factors
- Historical population exposure doesn’t confer immunity
Bacterial Genetics:
- T. pallidum genome is remarkably stable
- Limited genetic diversity compared to other bacteria
- Recent molecular typing identifies strain differences
- No antibiotic resistance genes detected
Co-infection and Synergistic Factors
HIV Co-infection:
- Bidirectional relationship
- Syphilis increases HIV transmission risk
- HIV accelerates syphilis progression
- May alter typical syphilis presentations
- Requires modified treatment approaches
Other STI Co-infections:
- Common with gonorrhea, chlamydia
- May facilitate syphilis transmission
- Ulcerative STIs (herpes) increase transmission risk
- Shared risk factors and transmission routes
Risk Behaviors and Triggers
High-Risk Sexual Behaviors:
- Unprotected sex with infected partners
- Multiple sexual partners
- Anonymous sexual encounters
- Sex work (both selling and buying)
- Substance use during sexual activity
- “Chemsex” (drug use to enhance sex)
Substance Use:
- Illicit drug use (especially methamphetamines)
- Alcohol abuse reducing risk assessment
- Injection drug use (rare transmission route)
- Party drugs affecting judgment
Occupational Risks:
- Sex workers
- Healthcare workers
- Laboratory personnel
- First responders
Epidemiological Patterns
Geographic Factors:
- More common in urban areas
- Concentrated in specific communities
- Associated with poverty and social determinants
- Access to healthcare affects transmission
Social Determinants:
- Poverty and lack of education
- Limited access to healthcare
- Stigma preventing treatment seeking
- Social networks and partner notification challenges
Temporal Factors:
- Cyclical epidemics observed historically
- Current global resurgence
- Seasonal patterns in some regions
- Associated with major social events
Prevention Implications
Transmission Prevention:
- Consistent condom use reduces risk
- Regular STI screening
- Partner notification and treatment
- Safe sex practices education
Environmental Control:
- No environmental reservoirs to control
- Focus on behavioral interventions
- Healthcare setting infection control
Understanding the causes of syphilis extends beyond the simple identification of Treponema pallidum as the causative agent. The complex interplay between bacterial characteristics, host factors, environmental conditions, and social determinants creates a multifaceted challenge for prevention and control. While the bacterium itself has limited survival outside the human body, its ability to establish chronic infection and the various routes of transmission make comprehensive prevention strategies essential for controlling spread.
5. Risk Factors
Demographic Risk Factors
Age:
- Young Adults (15-24): Highest incidence rates in many countries
- Adults 25-34: Second highest risk group
- Congenital Risk: Linked to maternal infection status during pregnancy
- Older Adults: Lower incidence but higher tertiary complications
- Age-specific patterns: Vary by sexual orientation and geographic location
Gender:
- Men: Higher overall rates in many developed countries
- Men who have sex with men (MSM): Highest risk group globally
- Women: Greater risk during reproductive years
- Transgender individuals: Elevated risk in many populations
- Gender disparities: Reflect sexual network patterns and healthcare access
Race and Ethnicity:
- Disparities often reflect social determinants rather than biological factors
- In the US: Higher rates among African American and Hispanic populations
- Indigenous populations: Higher rates in several countries
- Disparities linked to socioeconomic factors and healthcare access
Behavioral Risk Factors
Sexual Behavior:
- Multiple sexual partners: Direct correlation with risk increase
- Anonymous sexual encounters: Difficult contact tracing
- Concurrent partnerships: Accelerates epidemic spread
- Group sex participation: Higher transmission likelihood
- Sex work involvement: Both providers and clients at elevated risk
- Sexual mixing patterns: Bridge populations between risk groups
High-Risk Sexual Practices:
- Unprotected anal sex: Highest transmission risk
- Unprotected vaginal or oral sex: Moderate transmission risk
- “Condom fatigue”: Reduced condom use in established relationships
- “Serosorting”: HIV status-based partner selection (may miss syphilis)
Substance Use:
- Methamphetamine use: Strongly associated with syphilis in MSM
- “Chemsex”: Drug use to enhance sexual experiences
- Alcohol abuse: Impaired judgment and risk-taking
- Injection drug use: Non-sexual transmission risk
Digital-Age Risk Factors:
- Dating apps: Anonymous connections, rapid partner turnover
- Social media: Facilitates anonymous encounters
- Online sex work: Changing risk landscapes
- Virtual communities: Both risk and prevention opportunities
Medical Risk Factors
HIV Status:
- HIV-positive individuals: 30-50% of MSM with syphilis are HIV-positive
- Syphilis in HIV-positive: More aggressive course, atypical presentations
- Bidirectional risk: Each infection increases transmission of the other
- Treatment considerations: Modified regimens often required
Other STIs:
- Current STIs: Increase syphilis transmission likelihood
- History of STIs: Marker for continued high-risk behavior
- Herpes simplex virus: Ulcers facilitate syphilis entry
- Hepatitis B/C: Similar transmission routes, higher co-infection rates
Immunosuppression:
- Systemic conditions: Diabetes, autoimmune diseases
- Medications: Corticosteroids, biologics, chemotherapy
- Organ transplant recipients: Increased risk and atypical presentations
- Pregnancy: Particularly after the first trimester
Socioeconomic Risk Factors
Economic Factors:
- Poverty: Limited access to prevention and healthcare
- Unemployment: Associated with higher-risk behaviors
- Homelessness: Barriers to consistent care and prevention
- Food insecurity: May lead to transactional sex
- Economic inequality: Broader social determinant
Education and Knowledge:
- Low education levels: Reduced health literacy
- Limited sex education: Inadequate prevention knowledge
- Language barriers: Access to healthcare information
- Health literacy: Understanding of transmission and prevention
Healthcare Access:
- Uninsured populations: Delayed or no treatment
- Rural residence: Limited specialized care access
- Provider bias: Discrimination affecting care quality
- Undocumented status: Fear of seeking care
Geographic and Environmental Risk Factors
Urban vs. Rural:
- Urban concentrations: Higher rates in metropolitan areas
- Rural disparities: Limited access to prevention and care
- Cross-border regions: Complex epidemiological patterns
- Tourism areas: Transient populations and sexual networks
Regional Patterns:
- “Syphilis belts”: Geographic clustering in certain regions
- Hot spots: Concentrated outbreaks in specific communities
- International travel: Risk in high-prevalence areas
- Border cities: Higher rates in some cross-border areas
Institutional Settings:
- Correctional facilities: Higher prevalence and limited care
- Military populations: Deployment and risk behaviors
- Sex work venues: Industry structure affects risk patterns
- Substance treatment facilities: High-risk populations
Occupational Risk Factors
Healthcare Workers:
- Physicians: Especially in primary care and STI clinics
- Nurses: Direct patient contact exposure
- Laboratory technicians: Handling infected specimens
- Emergency responders: Potential exposure risk
Service Industries:
- Sex work: Direct occupational exposure
- Entertainment industry: Higher exposure in some sectors
- Transportation workers: Mobile populations
- Hospitality workers: International exposure
Pregnancy-Specific Risk Factors
Maternal Factors:
- Lack of prenatal care: Missed screening opportunities
- Previous STIs: Increased likelihood of current infection
- Partner risk factors: Male partner STI history
- Substance use during pregnancy: Associated high-risk behaviors
Pregnancy Stage:
- Any trimester: Risk of congenital transmission
- Early pregnancy: Critical developmental period
- Late pregnancy: Higher transmission risk to fetus
- Postpartum period: Risk to newborn during delivery
Prevention Science Considerations
Vaccine-Preventable Disease Co-morbidity:
- HPV: Shared transmission routes
- Hepatitis B: Combined vaccination opportunities
- Future syphilis vaccine: Would modify risk landscape
Pre-Exposure Prophylaxis (PrEP):
- HIV PrEP users: May increase syphilis risk through behavioral changes
- Regular screening: Opportunities and challenges
- Risk compensation: Behavioral adaptations to medical interventions
Understanding these diverse risk factors is essential for:
- Developing targeted prevention programs
- Identifying high-risk populations for screening
- Designing culturally appropriate interventions
- Addressing health equity and access issues
- Planning public health resource allocation
The interplay between these risk factors often creates syndemic conditions where multiple health problems concentrate in vulnerable populations. Effective syphilis prevention requires comprehensive approaches that address not only individual behaviors but also social, economic, and structural determinants of health.
6. Complications
Primary and Secondary Syphilis Complications
Immediate Complications:
- Secondary bacterial infections: When primary chancres become superinfected
- Phimosis and paraphimosis: From genital chancres in uncircumcised males
- Urethral fistulas: Rare but severe penile complications
- Immune complex disorders: During secondary stage
- Acute renal failure: From glomerulonephritis
- Hepatitis: Secondary syphilis affecting the liver
Progression Risks:
- Without treatment: 100% progression to latent stage
- 30% of untreated cases progress to tertiary syphilis
- Early treatment prevents later complications
- Partial treatment may lead to atypical presentations
Cardiovascular Complications
Aortitis and Aneurysm Formation:
- Linear calcification: Characteristic “tree-bark” pattern
- Ascending aortic aneurysm: Most common cardiovascular manifestation
- Aortic valve insufficiency: Leading to heart failure
- Coronary ostial stenosis: Myocardial infarction risk
- Mortality rate: 10-40% of untreated cardiovascular syphilis cases
Clinical Manifestations:
- Chest pain and pressure
- Dyspnea on exertion
- Orthopnea and paroxysmal nocturnal dyspnea
- Dilated aorta on imaging
- Aortic insufficiency murmur
Management Challenges:
- Often diagnosed at late stage
- Surgical intervention high-risk
- Antibiotics don’t reverse structural damage
- Long-term cardiac monitoring required
Neurological Complications
Types of Neurosyphilis:
Asymptomatic Neurosyphilis:
- Abnormal CSF findings without symptoms
- 20-30% of latent syphilis cases
- Risk of progression to symptomatic forms
Acute Meningitis:
- Usually occurs in secondary syphilis
- Headache, fever, stiff neck
- Cranial nerve involvement possible
Meningovascular Syphilis:
- Stroke-like presentations
- Brain and spinal cord infarctions
- Cognitive impairment
- 5-10 year onset typically
General Paresis:
- Dementia and personality changes
- Memory loss and confusion
- Paranoid symptoms
- 10-20 year onset typically
Tabes Dorsalis:
- Loss of proprioception
- Shooting pains (“lightning pains”)
- Urinary and fecal incontinence
- Charcot joints
HIV-Associated Complications:
- Accelerated neurosyphilis progression
- Earlier onset of neurological symptoms
- Atypical presentations
- Higher CSF abnormality rates
Ocular Complications
Ocular Syphilis Presentations:
- Uveitis: Most common ocular manifestation
- Papilledema: Optic nerve involvement
- Retinal vasculitis: Vision-threatening inflammation
- Chorioretinitis: Retinal and choroid inflammation
- Optic atrophy: End-stage complication
Clinical Implications:
- Can occur at any stage of syphilis
- May present without other syphilis symptoms
- Requires both systemic and topical treatment
- Vision loss can be irreversible if untreated
- Considered neurosyphilis requiring neurosyphilis treatment regimen
Congenital Syphilis Complications
Early Complications (<2 years old):
- Stillbirth: 40% of untreated maternal syphilis
- Neonatal death: 20% of live births
- Premature birth: Increased risk
- Neonatal sepsis: Treponema bacteremia
- Hemolytic anemia: Severe cases
Late Complications (>2 years old):
- Developmental delays: Variable severity
- Hutchinson’s triad:
- Notched incisors
- Interstitial keratitis
- Eighth nerve deafness
- Skeletal abnormalities:
- Sabre shins
- Clutton’s joints
- Rhagades
- Neurological deficits: Similar to adult neurosyphilis
Gummatous Complications
Gumma Characteristics:
- Granulomatous lesions
- Can affect any organ
- Usually appear 3-15 years post-infection
- Painless but destructive
Common Locations and Effects:
- Skin: Ulcerative lesions
- Bones: Pathological fractures
- Liver: Hepatic failure (rare)
- Nose: Septal perforation
- Upper airway: Respiratory compromise
- Central nervous system: Space-occupying lesions
Treatment Complications
Jarisch-Herxheimer Reaction:
- Incidence: 30-60% during treatment
- Mechanism: Bacterial endotoxin release
- Symptoms: Fever, chills, myalgias, rash
- Onset: 2-8 hours after first treatment
- Duration: 12-24 hours typically
- Management: NSAIDs, corticosteroids in severe cases
Antibiotic-Related Complications:
- Allergy to penicillin: 5-10% population
- Desensitization risks: Anaphylaxis potential
- Alternative antibiotic failures: Rare but documented
- Drug interactions: Particularly in HIV co-infection
Long-term Disability and Mortality
Disability Rates:
- Tertiary syphilis: 30% of untreated cases
- Permanent neurological damage: 5-10% of all infections
- Visual impairment: 1-2% of all infections
- Cardiovascular disability: 8-10% of untreated tertiary cases
- Congenital syphilis disability: Varies widely
Mortality Statistics:
- Historical data: 23% mortality in untreated cases
- Modern era: <1% mortality with prompt treatment
- Cardiovascular syphilis: 10-40% mortality if untreated
- Neurosyphilis: Variable, depends on form
- Congenital syphilis: 40-60% perinatal mortality if untreated
Prevention of Complications
Early Detection Benefits:
- Treatment during primary stage: Nearly 100% cure rate
- Secondary stage treatment: Prevents tertiary complications
- Latent stage treatment: Stops progression
- Partner notification: Prevents reinfection
Screening Programs:
- Routine STI screening protocols
- Antenatal screening programs
- High-risk population targeted screening
- Regular monitoring for treatment success
Management After Complications:
- Supportive care for irreversible damage
- Cardiac interventions for vascular complications
- Neurological rehabilitation
- Ophthalmological care for ocular syphilis
- Psychological support for neurological sequelae
The complications of syphilis underscore the critical importance of early detection and treatment. While modern antibiotics can effectively eliminate the infection at any stage, damage to organs and tissues from tertiary syphilis is often irreversible. The rise in syphilis cases globally, particularly in vulnerable populations, makes understanding and preventing these complications essential for public health strategy and clinical practice.
7. Diagnosis & Testing
Clinical Diagnosis
Clinical Evaluation:
- Comprehensive sexual history
- Physical examination including:
- Genital and anal examination
- Skin inspection (including palms and soles)
- Oral cavity assessment
- Lymph node palpation
- Neurological examination when indicated
Diagnostic Criteria:
- Clinical signs consistent with syphilis
- Laboratory confirmation
- Epidemiological links (sexual contacts)
- Response to treatment
Microscopic Examination
Dark-field Microscopy:
- Principle: Direct visualization of live treponemes
- Specimen sources:
- Exudate from chancres
- Moist lesions of secondary syphilis
- Regional lymph node aspiration
- Advantages:
- Immediate results (within minutes)
- Highly specific when positive
- Can detect early primary syphilis
- Limitations:
- Requires viable organisms
- Expertise required for interpretation
- Limited availability in many settings
- Cannot distinguish T. pallidum subspecies
Direct Fluorescent Antibody Testing (DFA-TP):
- Uses fluorescent-labeled anti-treponemal antibodies
- Can be performed on fixed specimens
- More versatile than dark-field microscopy
- Limited availability in routine settings
Serological Testing
Types of Serological Tests:
Non-treponemal Tests (Cardiolipin-based):
- Rapid Plasma Reagin (RPR)
- Venereal Disease Research Laboratory (VDRL)
Treponemal Tests (Specific for T. pallidum):
- Treponema pallidum particle agglutination (TPPA)
- Treponema pallidum enzyme immunoassay (TP-EIA)
- Chemiluminescence immunoassay (CIA)
- Fluorescent treponemal antibody absorption (FTA-ABS)
Traditional Algorithm (RPR/VDRL followed by treponemal test):
Screening: Non-treponemal test (RPR/VDRL)
- If positive: Confirm with treponemal test
- If negative in high-risk: Consider specific treponemal testing
Interpretation:
- Both positive: Active or previously treated syphilis
- Non-treponemal positive, treponemal negative: Likely false positive
- Non-treponemal negative, treponemal positive: Treated syphilis or late latent
Reverse Sequence Algorithm (Emerging Standard):
Screening: Treponemal test (EIA/CIA)
- If positive: Reflexively test RPR/VDRL
- If discordant: Second treponemal test
Advantages:
- Higher automation capability
- Detects more cases of late latent syphilis
- Cost-effective for high-volume laboratories
Challenges:
- May detect old, treated infections
- Requires careful clinical correlation
- Training needed for interpretation
Stage-Specific Testing Approaches
Primary Syphilis:
- Dark-field microscopy or DFA-TP (highly recommended)
- Serological tests may be negative (20-30%)
- Repeat serology in 2-3 weeks if high suspicion
Secondary Syphilis:
- Nearly 100% serologically positive
- High RPR/VDRL titers typical
- Treponemal tests usually strongly positive
Latent Syphilis:
- Diagnosis based on serology alone
- No clinical signs
- RPR/VDRL titers variable
- Treponemal tests remain positive lifelong
Tertiary Syphilis:
- Non-treponemal tests may be negative (25%)
- Treponemal tests usually positive
- Tissue biopsy may show characteristic findings
Special Testing Considerations
Congenital Syphilis:
- Maternal and infant serological testing
- Passive transfer of maternal antibodies
- Non-treponemal tests in infant at birth
- Serial infant titers to distinguish passive from active infection
- Dark-field examination of suspicious lesions
Neurosyphilis Evaluation:
- Cerebrospinal fluid (CSF) analysis:
- VDRL-CSF (specific but insensitive)
- Cell count, protein, glucose
- FTA-ABS-CSF (sensitive but less specific)
- Indications:
- Neurological symptoms
- Ocular symptoms
- HIV co-infection with high RPR titers
- Treatment failure
HIV Co-infection:
- More frequent serological monitoring
- Lower threshold for CSF examination
- Enhanced response expected with treatment
- Possible false-positive non-treponemal tests
Point-of-Care Testing
Rapid Treponemal Tests:
- Results in 10-20 minutes
- Useful in resource-limited settings
- Various formats: lateral flow, immunochromatographic
- Sensitivity: 70-98%, Specificity: 85-98%
- Cannot distinguish active from treated infection
Molecular Testing:
- PCR assays available in research settings
- Can detect T. pallidum DNA in various specimens
- Useful for:
- CSF analysis
- Amniotic fluid
- Skin lesions
- Not yet routinely available
Monitoring Treatment Response
Serological Follow-up:
- Non-treponemal test titers (RPR/VDRL) used to monitor response
- Expected response:
- 4-fold decline by 6 months (primary/secondary)
- 2-fold decline by 6 months (early latent)
- May not decline in late latent/tertiary
Treatment Failure Indicators:
- Rising titers
- Failure to decline appropriately
- Clinical signs of progression
- Serofast state (stable low titers)
Quality Assurance
Laboratory Standards:
- Proper specimen collection and handling
- Standardized testing protocols
- Regular proficiency testing
- Quality control measures
- Staff training and competency testing
Clinical Quality Measures:
- Appropriate test ordering
- Proper specimen collection
- Timely reporting of results
- Clinical correlation and follow-up
- Partner notification protocols
Future Diagnostic Directions
Emerging Technologies:
- Next-generation sequencing for strain typing
- Proteomics-based diagnostics
- Smartphone-based microscopy
- Multiplex molecular assays
- Biosensor development
Challenges and Opportunities:
- Integration with electronic health records
- Cost-effective scaling for resource-limited settings
- Rapid turnaround for decision-making
- Differentiation of active from treated infection
- Implementation of reverse sequence algorithms
The diagnosis of syphilis requires a combination of clinical acumen and appropriate laboratory testing. While the availability of multiple testing modalities provides clinicians with various options, proper test selection and interpretation remain crucial. The evolving landscape of diagnostic algorithms, including the shift toward reverse sequence screening, reflects both technological advances and the need for more efficient, automated testing processes. Understanding the strengths and limitations of each diagnostic approach is essential for providing optimal patient care and controlling the spread of syphilis in the community.
8. Treatment Options
Standard Treatment Protocols
Treatment Guidelines (Based on CDC/WHO Recommendations):
Primary, Secondary, and Early Latent Syphilis:
- First-line: Benzathine penicillin G 2.4 million units IM (single dose)
- Pregnancy: Same as non-pregnant
- Penicillin allergy: Doxycycline 100mg PO BID × 14 days OR Tetracycline 500mg PO QID × 14 days
Late Latent Syphilis and Tertiary Syphilis (excluding neurosyphilis):
- First-line: Benzathine penicillin G 2.4 million units IM weekly × 3 doses
- Pregnancy: Same as non-pregnant
- Penicillin allergy: Doxycycline 100mg PO BID × 28 days
Neurosyphilis:
- First-line: Aqueous crystalline penicillin G 18-24 million units/day IV (3-4 million units every 4 hours) × 10-14 days
- Alternative: Procaine penicillin 2.4 million units IM daily + Probenecid 500mg PO QID × 10-14 days
- Penicillin allergy: Desensitization required; no proven alternatives
Congenital Syphilis:
- First-line:
- Aqueous crystalline penicillin G 50,000 units/kg/dose IV every 12 hours (first 7 days), then every 8 hours (8-28 days)
- Procaine penicillin G 50,000 units/kg IM daily × 10 days
- Duration: 10 days minimum
Penicillin Allergy Management
Desensitization Protocol:
- Required for pregnant women and neurosyphilis patients
- Performed in ICU setting with immediate resuscitation capability
- Oral or intravenous protocols available
- Takes 4-12 hours typically
- Success rate >90%
Alternative Antibiotics (when desensitization not possible):
- Doxycycline (not in pregnancy)
- Ceftriaxone (limited data, not first-line)
- Azithromycin (resistance concerns)
- Tetracycline (not in pregnancy)
Special Populations
HIV Co-infection:
- Same antibiotic regimens as HIV-negative patients
- More aggressive follow-up required
- Higher risk of treatment failure
- More frequent serological monitoring
- Lower threshold for CSF examination
Pregnancy:
- Penicillin only recommended treatment
- Desensitization mandatory if allergic
- Treatment urgency to prevent congenital transmission
- Second dose recommended 1 week apart in some cases
- Fetal monitoring for Jarisch-Herxheimer reaction
Immunocompromised Patients:
- Standard regimens usually effective
- Extended therapy may be considered
- Close clinical monitoring
- Potential for atypical presentations
Management of Jarisch-Herxheimer Reaction
Characteristics:
- Fever, chills, myalgia, headache
- Onset: 2-8 hours after treatment
- Duration: 12-24 hours typically
- More common in early syphilis (30-60%)
Prevention and Management:
- Patient counseling about expected reaction
- NSAIDs for symptom relief
- Corticosteroids controversial (may blunt immune response)
- Hospitalization for high-risk patients (pregnancy, neurosyphilis)
- Supportive care
Treatment Failure
Definition:
- Persistent symptoms
- Rising RPR/VDRL titers
- Failure of titers to decline appropriately
- Clinical evidence of progression
Management:
- Re-evaluation for neurosyphilis
- CSF examination if indicated
- Extended treatment regimen
- Partner screening and treatment
- Search for re-infection source
Follow-up and Monitoring
Serological Follow-up:
- Primary/Secondary: 6, 12, and 24 months
- Early latent: 6, 12, and 24 months
- Late latent: 12 and 24 months
- Neurosyphilis: Every 6 months for 2 years
Expected Serological Response:
- 4-fold decline in RPR/VDRL titers by 6 months (early syphilis)
- Treponemal tests remain positive indefinitely
- Serofast state: Stable low-level titers common
Partner Management
Contact Notification:
- Sexual partners within 90 days (primary syphilis)
- 6 months (secondary/early latent)
- 12 months (late latent)
- Mother and infant pairs for congenital syphilis
Presumptive Treatment:
- Recommended for sexual partners
- Based on epidemiological linkage
- Same regimen as patient
Emerging and Experimental Treatments
Novel Antibiotics:
- Research into macrolides (post-resistance)
- New beta-lactam combinations
- Fluoroquinolone derivatives
- Combination therapy studies
Immunotherapy Approaches:
- Adjuvant immunotherapy
- Vaccine development (preventive and therapeutic)
- Monoclonal antibody therapy
- Immune modulation strategies
Quality of Care Measures
Clinical Management:
- Appropriate staging of infection
- Proper antibiotic selection and dosing
- Partner notification completion
- Documentation of treatment response
- Long-term follow-up maintenance
Patient Education:
- Disease transmission education
- Treatment importance and completion
- Safer sex practices
- Regular STI screening importance
- Signs requiring immediate medical attention
Cost-Effectiveness Considerations
Economic Analysis:
- Penicillin remains most cost-effective
- Early treatment prevents expensive complications
- Partner treatment reduces community transmission
- Screening programs save healthcare costs
Resource Allocation:
- Prioritization of high-risk populations
- Integration with HIV prevention services
- Point-of-care testing in resource-limited settings
- Community-based treatment programs
Future Treatment Directions
Pharmacological Advances:
- Long-acting injectable antibiotics
- Oral regimens for neurosyphilis
- Single-dose cures for all stages
- Combination prevention approaches
Precision Medicine:
- Genetic markers for treatment response
- Personalized dosing based on host factors
- Molecular resistance testing
- Strain-specific treatment approaches
Integration with Technology:
- Telemedicine for follow-up care
- Digital adherence monitoring
- Electronic partner notification
- Artificial intelligence for risk assessment
The treatment of syphilis represents a public health success story, with penicillin remaining universally effective after more than 75 years of use. However, challenges persist, including penicillin allergies, HIV co-infection, and ensuring treatment completion. The development of new treatment modalities and integration with modern technology offers promise for improving patient outcomes and reducing disease transmission. Success requires not only effective antimicrobial therapy but also comprehensive care including partner management, regular follow-up, and continued education about prevention.
9. Prevention & Precautionary Measures
Primary Prevention Strategies
Behavioral Interventions:
Safe sex practices:
- Consistent and correct condom use
- Dental dams for oral-anal contact
- Reducing number of sexual partners
- Mutual monogamy with tested partners
Sexual health education:
- Comprehensive sex education programs
- Community-based education initiatives
- Peer education for high-risk groups
- Health literacy improvement
Risk reduction counseling:
- Personalized risk assessment
- Motivational interviewing techniques
- Goal setting for behavior change
- Regular counseling sessions for high-risk individuals
Secondary Prevention
Screening Programs:
Routine STI Screening:
- Annual screening for sexually active individuals
- Every 3-6 months for high-risk groups
- Pre-exposure prophylaxis (PrEP) users
- Men who have sex with men (MSM)
Pregnancy Screening:
- First prenatal visit
- Third trimester (28-32 weeks)
- Delivery (if high-risk or no prenatal care)
- Postpartum screening in high-risk mothers
Targeted Screening:
- Sex workers and clients
- Persons with HIV infection
- Those with recent STI history
- Incarcerated populations
Early Detection Benefits:
- Prevention of transmission to partners
- Avoidance of complications
- Cost-effective compared to treating advanced disease
- Interruption of transmission chains
Condom Use and Barrier Methods
Effectiveness:
- Consistent use reduces syphilis transmission by 50-70%
- Less effective than for other STIs due to syphilis lesions outside covered areas
- Combined with other prevention strategies increases effectiveness
Proper Usage:
- Use from start to finish of sexual activity
- Water-based lubricants to prevent breakage
- New condom for each sexual encounter
- Disposal method and hygiene
Barrier Method Options:
- Male and female condoms
- Dental dams
- Polyurethane alternatives for latex allergies
- Internal condoms for receptive partners
Partner Notification and Treatment
Contact Tracing:
Time periods for notification:
- Primary syphilis: 90 days before symptom onset
- Secondary syphilis: 6 months before diagnosis
- Early latent: 12 months before diagnosis
Methods:
- Patient referral
- Provider referral
- Contract referral
- Digital notification platforms
Presumptive Treatment:
- Treatment without testing for exposed partners
- Prevents ongoing transmission
- Addresses possible false-negative tests
- Reduces loss to follow-up
Population-Specific Prevention
Men Who Have Sex with Men (MSM):
- Regular screening every 3-6 months
- Biomedical prevention integration (PrEP programs)
- Community-based education and testing
- Apps and technology-based interventions
Sex Workers:
- Workplace interventions
- Peer education programs
- Regular clinical services
- Occupational health approaches
Pregnant Women:
- Universal prenatal screening
- Partner screening and treatment
- Resources for social support
- Substance abuse treatment integration
Adolescents and Young Adults:
- School-based education
- College health center programs
- Youth-friendly clinical services
- Social media education campaigns
Biomedical Prevention
HIV Pre-Exposure Prophylaxis (PrEP) Integration:
- Routine syphilis screening for PrEP users
- Regular clinical follow-up
- STI treatment protocols
- Sexual health counseling
Antimicrobial Prophylaxis:
- Not routinely recommended for syphilis
- Post-exposure treatment considerations
- High-risk situations (known exposure)
- Pregnancy considerations
Community and Structural Interventions
Public Health Measures:
- Disease surveillance systems
- Outbreak response protocols
- Public awareness campaigns
- Policy advocacy for prevention
Healthcare System Integration:
- STI services in primary care
- Integration with HIV services
- Harm reduction programs
- Substance abuse treatment linkage
Social Determinants Approach:
- Addressing poverty and inequality
- Improving healthcare access
- Reducing stigma and discrimination
- Supporting vulnerable populations
Technology-Enhanced Prevention
Digital Health Tools:
- Dating app interventions
- Text messaging reminders
- Online testing and results
- Virtual counseling services
Electronic Health Records:
- Automated screening reminders
- Clinical decision support
- Partner notification integration
- Care coordination
Social Media and Apps:
- Health education content
- Anonymous notification systems
- Risk assessment tools
- Appointment scheduling
Vaccine Development
Current Status:
- No licensed syphilis vaccine currently available
- Multiple candidates in development
- Challenges: Antigenic variation, immune evasion
- Animal models showing promise
Future Prospects:
- Combined STI vaccines
- Therapeutic vaccine approaches
- Novel adjuvants and delivery systems
- Population-specific formulations
Educational Initiatives
School-Based Programs:
- Age-appropriate sex education
- Inclusion in health curricula
- Teacher training programs
- Parent engagement strategies
Community Education:
- Faith-based initiatives
- Cultural competency considerations
- Language-appropriate materials
- Health fair participation
Healthcare Provider Education:
- CME on syphilis recognition
- Cultural sensitivity training
- Communication skills development
- Update protocols and guidelines
Policy and Advocacy
Public Policy Initiatives:
- Funding for prevention programs
- Insurance coverage for screening
- Comprehensive sex education laws
- Anti-discrimination legislation
Legal Considerations:
- Partner notification confidentiality
- Mandatory reporting compliance
- Treatment access protections
- Criminal law impacts on disclosure
Evaluation and Quality Improvement
Program Monitoring:
- Screening coverage rates
- Treatment completion rates
- Partner notification success
- Reinfection rates
Outcome Measures:
- Incidence reduction
- Complications prevented
- Cost-effectiveness analysis
- Community health impact
Continuous Improvement:
- Regular program evaluation
- Stakeholder feedback
- Evidence-based updates
- Innovation implementation
Prevention of syphilis requires a comprehensive, multi-modal approach addressing individual, community, and structural factors. While behavioral interventions remain central, integration with biomedical prevention, use of technology, and addressing social determinants of health are increasingly important. Success depends on sustained political commitment, adequate funding, and coordination between healthcare, education, and social service sectors. The goal extends beyond individual infection prevention to interrupting transmission chains and ultimately eliminating syphilis as a public health threat.
10. Global & Regional Statistics
Global Burden of Syphilis
Overall Prevalence (2021 WHO Data):
- Global prevalence: 7.1 million cases (18-49 age group)
- Incidence: 8 million new cases annually
- Global prevalence rate: 0.9% among adults aged 15-49
- Estimated 200,000 stillbirths and early neonatal deaths from maternal syphilis annually
Epidemiological Trends:
- 52% increase in global cases from 2012-2019
- Temporary decrease during COVID-19 pandemic
- Resurgence in 2021-2022
- Rising rates in developed and developing countries
Regional Distribution
WHO African Region:
- Prevalence: 2.3% (highest globally)
- Key countries: South Africa, Nigeria, Kenya, Uganda
- Congenital syphilis rates: 2-3% of live births in some areas
- Challenges: Limited healthcare access, HIV co-infection
WHO South-East Asia Region:
- Prevalence: 0.7%
- Key countries: India, Indonesia, Bangladesh
- Improving detection and treatment programs
- Large population denominators affect total numbers
WHO Eastern Mediterranean Region:
- Prevalence: 0.3%
- Data quality varies by country
- Conflict zones show higher rates
- Limited surveillance in some areas
WHO Western Pacific Region:
- Prevalence: 0.5%
- Key countries: China, Philippines, Vietnam
- Rapid economic development affecting patterns
- Concentrated epidemics in urban areas
WHO European Region:
- Prevalence: 0.3%
- Rising incidence in Western Europe
- MSM-concentrated epidemics
- Eastern Europe: Substance use-associated transmission
WHO Region of the Americas:
- Prevalence: 1.4%
- United States: Rising rates since 2000
- Latin America: Persistent high rates
- Caribbean: High rates, HIV co-infection concerns
Country-Specific Data
United States:
- 128,465 reported cases in 2021
- 65% increase from 2017-2021
- Primary and secondary: 53,767 cases
- Congenital syphilis: 2,677 cases
- Geographic concentration: Southern states
China:
- 650,000 reported cases annually
- Rural-urban disparities
- Congenital syphilis: 8-10 per 100,000 live births
- Eastern provinces higher rates
Russia:
- 150,000 reported cases annually
- Substance use-associated transmission
- Prison populations at high risk
- Economic factors influencing access
Brazil:
200,000 reported cases annually
- High congenital syphilis rates
- Regional disparities
- Public health program impacts
South Africa:
- Prevalence: 2.5-3% of adults
- Higher rates in rural areas
- ANC (Antenatal Care) prevalence: 1-2%
- Strong association with HIV
High-Risk Populations
Men Who Have Sex with Men (MSM):
- 5-15% prevalence in many countries
- 50-70% of early syphilis cases in developed countries
- Co-infection with HIV common
- Concentrated urban epidemics
Sex Workers:
- 2-20% prevalence globally
- Higher rates in resource-limited settings
- Client population also affected
- Occupational health considerations
Pregnant Women:
- Screening coverage varies: 50-95% globally
- Prevalence: 0.1-10% by country
- Treatment rates: 60-90% where screening occurs
- Direct impact on congenital cases
Incarcerated Populations:
- 2-5 times general population rates
- Limited screening and treatment access
- Post-release community impact
- Reentry programs important
Congenital Syphilis
Global Statistics:
- 140,000 stillbirths annually
- 62,000 early neonatal deaths
- 80,000 affected live births
- 200,000+ clinical impacts total
Regional Variations:
- Sub-Saharan Africa: 10-20 per 1,000 live births
- United States: 77.9 per 100,000 live births (2021)
- China: 8-10 per 100,000 live births
- Brazil: 8.5 per 1,000 live births
Prevention Impact:
- Countries with effective ANC screening: <1 per 10,000 births
- PAHO/WHO initiative target: <0.5 per 1,000 live births
- Cost-effective intervention
- Significant mortality/morbidity reduction potential
Economic Burden
Healthcare Costs:
- Global: $1.2 billion annually (estimated)
- United States: $15 billion over 10 years
- Treatment costs vs. complication costs
- Pregnancy-related costs significant
Economic Impact:
- Lost productivity from disability
- Healthcare system burden
- Prevention vs. treatment economics
- Indirect costs to families and communities
Surveillance Quality
Reporting Completeness:
- Varies significantly by country
- WHO surveillance network covers 129 countries
- Case definitions not standardized globally
- Private sector reporting challenges
Data Quality Issues:
- Underreporting common
- Case definition variations
- Laboratory capacity differences
- Stigma affecting reporting
Recent Trends and Patterns
Increasing Incidence:
- Global resurgence after 2000s decline
- Online dating impact
- Substance use patterns
- COVID-19 disruption and recovery
Shifting Demographics:
- Younger age of initial infection
- Heterosexual transmission increasing
- Urban concentration growing
- Social media and transmission
Co-epidemic Patterns:
- HIV co-infection remains high
- Hepatitis C co-infection
- Substance use disorders
- Mental health comorbidities
Public Health Response
Global Initiatives:
- WHO Global Health Sector Strategy
- UNAIDS Fast-Track targets
- PAHO congenital syphilis elimination
- National elimination programs
Success Stories:
- Cuba: Elimination of mother-to-child transmission
- Thailand: Significant reduction program
- Specific urban program successes
- Military screening program impacts
Intervention Impact:
- Screening program effectiveness
- Partner notification success rates
- Treatment coverage improvements
- Community education impact
Future Projections
Epidemiological Modeling:
- Continued increase predicted without intervention
- Potential 50% reduction with comprehensive programs
- Regional variations in trajectory
- Urbanization impact projections
Elimination Targets:
- WHO 90% reduction goal by 2030
- National elimination timelines
- Sub-population targets
- Realistic implementation scenarios
The global statistics on syphilis reveal a disease that, despite effective treatment availability, continues to cause significant morbidity and mortality worldwide. The patterns of infection reflect broader social, economic, and healthcare system inequalities. The recent resurgence in many regions underscores the need for sustained prevention efforts, robust surveillance systems, and targeted interventions for high-risk populations. Success in syphilis control requires integrated approaches addressing both individual risk factors and broader social determinants of health.
11. Recent Research & Future Prospects
Vaccine Development
Current Research Pipeline:
- Multiple candidate vaccines in preclinical and early clinical phases
- Approaches include:
- Outer membrane protein-based vaccines
- Whole-cell killed vaccines
- Recombinant protein subunit vaccines
- Live attenuated vaccines
- DNA and RNA vaccines
Key Challenges:
- Complex antigenic structure of T. pallidum
- Immune evasion mechanisms
- Lack of vaccine correlates of protection
- Limited animal models for testing
- Phase variation and antigenic diversity
Promising Developments:
- Identification of potential protective antigens (TprK, Tp0136, Tp0453)
- Novel adjuvant development
- Combination vaccine approaches with HIV prevention
- Therapeutic vaccine concepts for reducing transmission
Diagnostic Innovations
Next-Generation Testing:
Molecular Diagnostics:
- CRISPR-based detection systems
- Loop-mediated isothermal amplification (LAMP)
- Multiplex PCR for simultaneous STI detection
- Point-of-care molecular testing
Novel Biomarkers:
- Host immune response signatures
- Metabolomic profiling
- Proteomic approaches
- MicroRNA biomarkers
Digital Health Integration:
- AI-powered diagnostic algorithms
- Smartphone-based microscopy
- Remote specimen collection protocols
- Blockchain for laboratory result management
Therapeutic Advances
Novel Antimicrobials:
- Investigation of macrolide derivatives
- Beta-lactam combinations
- Antimicrobial peptides
- Bacteriophage therapy exploration
- Combination therapy optimization
Adjunctive Therapies:
- Immune modulation strategies
- Biofilm disruption agents
- Host-directed therapies
- Microbiome modulation approaches
Personalized Medicine:
- Pharmacogenomic-guided dosing
- Host genetic factors in treatment response
- Parasite genotyping for treatment selection
- Precision monitoring protocols
Epidemiological Research
Mathematical Modeling:
- Network analysis of transmission patterns
- Intervention impact modeling
- Resource allocation optimization
- Elimination scenario planning
Social Network Analysis:
- Digital epidemiology approaches
- Online dating app data integration
- Community structure mapping
- High-risk network identification
Real-time Surveillance:
- Syndromic surveillance integration
- Wastewater epidemiology
- Social media monitoring
- Electronic health record mining
Behavioral Research
Implementation Science:
- Optimization of screening intervals
- Partner notification effectiveness studies
- Prevention program evaluation
- Healthcare delivery model assessment
Technology-Enhanced Interventions:
- App-based prevention tools
- Gamification of sexual health education
- Virtual reality counseling
- Wearable technology for risk assessment
Public Health Innovation
Elimination Strategies:
- Micro-elimination approaches
- Test-and-treat programs
- Community-wide screening initiatives
- Integrated STI control programs
Healthcare Delivery Models:
- Community-based testing networks
- Pharmacy-based screening
- School-based interventions
- Occupational health integration
Social Determinants Research:
- Structural intervention evaluation
- Health equity impact assessments
- Policy intervention studies
- Community empowerment approaches
Basic Science Advances
Pathogenesis Research:
- Host-pathogen interaction mechanisms
- Immune evasion strategies
- Biofilm formation in chronic infection
- Neurotropism molecular basis
Genomics and Proteomics:
- Complete genome characterization of clinical isolates
- Proteomic analysis of infection stages
- Evolutionary studies of T. pallidum
- Comparative genomics with related species
Immunology Research:
- Memory immune response characterization
- Mucosal immunity in syphilis
- Immune exhaustion in chronic infection
- Therapeutic vaccine target identification
Technology Integration
Artificial Intelligence Applications:
- Machine learning for risk prediction
- Natural language processing for surveillance
- Computer vision for microscopy
- AI-driven clinical decision support
Blockchain Technology:
- Secure health record sharing
- Anonymous partner notification
- Supply chain management for medications
- Clinical trial data integrity
Internet of Things (IoT):
- Connected monitoring devices
- Smart pill technologies
- Environmental monitoring for outbreak detection
- Integrated sexual health ecosystems
Global Health Research
Implementation Research:
- Low-resource setting adaptations
- Context-specific intervention design
- Sustainability of prevention programs
- Community engagement strategies
Health Systems Research:
- Integration with HIV services
- Primary care capacity building
- Laboratory system strengthening
- Quality improvement methodologies
Future Research Priorities
Short-term (1-3 years):
- Point-of-care molecular diagnostics
- Second-generation strain typing
- Enhanced partner notification tools
- Microelimination demonstration projects
Medium-term (3-7 years):
- First-generation preventive vaccines
- Novel antimicrobial combinations
- Integrated digital health platforms
- Population-wide elimination strategies
Long-term (7+ years):
- Sterilizing vaccine development
- Synthetic biology applications
- Personalized prevention approaches
- Syphilis eradication feasibility
Funding and Research Infrastructure
International Collaborations:
- Global research consortia
- North-South research partnerships
- Public-private partnerships
- Open science initiatives
Research Funding Trends:
- Increasing NIH/CDC investment
- Gates Foundation STI initiatives
- EU Horizon research programs
- Country-specific research priorities
Ethical Considerations
Research Ethics:
- Community engagement in study design
- Benefit sharing in low-resource settings
- Vulnerable population protection
- Data privacy and ownership
Implementation Ethics:
- Resource allocation fairness
- Health equity considerations
- Cultural sensitivity in interventions
- Sustainability and local capacity building
The future of syphilis research and control is promising, with multiple innovative approaches converging on the common goal of elimination. From vaccine development to digital health innovations, the scientific community is developing a comprehensive toolkit for combating this ancient disease. Success will require sustained funding, international collaboration, and integration of technological advances with proven public health strategies. The next decade presents unprecedented opportunities to make significant progress toward syphilis elimination, transforming a disease that has plagued humanity for centuries into a manageable and potentially eradicable condition.
12. Interesting Facts & Lesser-Known Insights
Historical Curiosities
The Great Imitator Phenomenon:
- Syphilis was so prevalent in Victorian England that medical students were taught “Know syphilis, and you know medicine”
- The disease could mimic almost any medical condition, leading to over-diagnosis
- Some famous historical figures misdiagnosed with syphilis actually had other conditions
Bizarre Treatment Attempts:
- Mercurial Fumigation: Patients were enclosed in boxes with burning cinnabar, inhaling mercury vapors
- Hot Box Treatment: Patients were placed in heated cabinets to induce sweating
- Deliberate Malaria Infection: Used to create fever that supposedly killed syphilis bacteria
- Salvarsan Shock: Early arsenic treatments sometimes caused dramatic neurological reactions
Famous Sufferers (Confirmed and Suspected):
- Confirmed: Christopher Columbus’s crew, King Henry VIII, Vincent van Gogh, Friedrich Nietzsche
- Disputed: Beethoven, Oscar Wilde, Adolf Hitler, Al Capone
- Medical Mystery: Some “mad” monarchs may have had neurosyphilis
Scientific Oddities
Bacterial Peculiarities:
- T. pallidum cannot be grown in laboratory culture, making it unique among major human pathogens
- The bacterium has one of the slowest replication rates – dividing only every 30-33 hours
- It has fewer genes than most bacteria but can still cause complex, multi-system disease
- The organism can survive dormant in cerebrospinal fluid for decades
Evolutionary Mysteries:
- Syphilis, yaws, pinta, and bejel are caused by nearly identical bacteria with different transmission patterns
- Some scientists believe all treponemal diseases evolved from a single ancestral organism
- The bacterium appears to have very low mutation rates, making it highly stable genetically
Immunological Paradox:
- Despite strong antibody responses, the immune system fails to clear the infection
- Syphilis can induce autoimmune responses that contribute to disease manifestations
- Previous infection provides minimal protection against reinfection
- Some individuals remain infected but never develop symptoms (immune tolerance)
Medical Anomalies
The Jarisch-Herxheimer Reaction:
- Named after two dermatologists who described it independently
- Can paradoxically make patients feel worse immediately after treatment
- In pregnancy, can cause premature labor
- Sometimes used as a crude “test” to confirm syphilis diagnosis before modern tests
Congenital Syphilis Facial Features:
- Mulberry molars: First molars with multiple small cusps resembling mulberries
- Hutchinson’s incisors: Notched front teeth
- Saber shins: Curved tibias from periostitis
- Saddle nose: Collapsed nasal bridge from cartilage destruction
Atypical Presentations:
- Lues maligna: A rare, severe form with widespread ulceration
- Syphilis d’emblée: Primary and secondary stages occurring simultaneously
- Quaternary syphilis: Proposed fourth stage with parasitic cysts
- Cardiovascular syphilis can cause aortic aneurysms visible on chest X-rays as “egg shell” calcification
Cultural and Social Impact
The Origin of Common Phrases:
- “Mad as a hatter”: Mercury poisoning from treatment, not the occupational hazard
- “Treatment worse than the disease”: Originated from syphilis therapy
- “A pox on both your houses”: Shakespeare reference to syphilis
- “No cure for love”: Often referred euphemistically to syphilis
Art and Literature Influences:
- Inspired countless works of art depicting moral decay
- Influenced the development of medical photography
- Became a metaphor for social corruption in literature
- Shaped early public health propaganda posters
Social Consequences:
- Led to the development of organized prostitution regulation
- Influenced marriage laws requiring blood tests
- Created the first mass public health education campaigns
- Shaped early sex education programs
Myths and Misconceptions
Persistent Myths:
- Myth: Syphilis can be caught from toilet seats
- Fact: The bacterium dies rapidly outside the human body
- Myth: Syphilis always affects the brain
- Fact: Only 5-10% develop neurosyphilis without treatment
- Myth: Once treated, you’re immune
- Fact: Reinfection is common and immunity is minimal
- Myth: Syphilis is always fatal
- Fact: With treatment, prognosis is excellent at any stage
Scientific Misconceptions:
- Misconception: Penicillin resistance is developing
- Reality: T. pallidum remains universally sensitive to penicillin
- Misconception: Condom use completely prevents transmission
- Reality: Provides partial protection; lesions can occur outside covered areas
- Misconception: Blood tests immediately detect infection
- Reality: There’s a window period before serological tests become positive
Modern Curiosities
Digital Age Phenomena:
- “Syphilis parties”: Underground gatherings where infected individuals share contacts
- Dating app-associated outbreaks tracked through geospatial analysis
- Social media “syphilis influencers” promoting unsafe practices
- Cryptocurrency used in some underground treatment markets
Economic Ironies:
- The same penicillin costing pennies is marked up thousands of times in some healthcare systems
- Syphilis tests can identify the disease but can’t distinguish current from past infection
- Treatment is extremely cheap, but healthcare costs for complications are enormous
- Black market trade in antibiotics despite legitimate availability
Research Paradoxes:
- We can sequence the entire genome but can’t grow it in a lab
- Despite being “The Great Imitator,” diagnosis is often straightforward
- Modern molecular techniques may be less specific than old microscopy
- Global resurgence despite simple, effective treatment
Lesser-Known Statistics
Survival Records:
- Some patients with untreated syphilis have survived 50+ years with the infection
- Neurosyphilis can manifest up to 40 years after initial infection
- Latent syphilis can remain dormant for entire lifetimes without progressing
- Some individuals clear the infection spontaneously (extremely rare)
Testing Oddities:
- False positive syphilis tests can occur during pregnancy
- Autoimmune diseases can cause false positive screening tests
- Some individuals never develop positive blood tests despite confirmed infection
- Successful treatment may leave “serological scars” for life
Geographic Curiosities:
- Iceland has one of the lowest syphilis rates globally (0.0001%)
- Certain Pacific islands had entire populations infected before European contact
- Some communities developed partial population immunity to yaws that affects syphilis susceptibility
- Urban centers consistently show higher rates than rural areas
Future Implications
Evolutionary Projections:
- T. pallidum shows remarkably little genetic change over centuries
- Some predict eventual bacterial adaptation to modern antibiotics
- Speculation about engineered probiotic treatments
- Possibility of synthetic biology applications
Societal Changes:
- Climate change may affect transmission patterns in some regions
- Space travel considerations for long-term missions
- Potential biomarker for overall population sexual health
- Integration with broader pandemic preparedness planning
The story of syphilis is far richer than a simple tale of sexually transmitted infection. It’s interwoven with human history, scientific discovery, social evolution, and cultural development. From the courts of Renaissance Europe to modern digital dating, from medieval mercury treatments to cutting-edge vaccine research, syphilis continues to surprise, challenge, and inform our understanding of infectious disease, human behavior, and public health. These fascinating aspects remind us that behind every statistic and clinical finding lies a complex narrative of human experience, scientific progress, and social change.
Understanding these lesser-known aspects of syphilis enriches our appreciation of the disease’s impact beyond its immediate medical consequences. They also highlight how a single pathogen can serve as a lens through which to examine broader themes of human history, social justice, scientific advancement, and public health policy. As we work toward elimination, these insights remind us that success requires not just medical interventions but also cultural understanding, historical awareness, and social sensitivity.