⚠️ Disclaimer: The information provided in this article is for educational purposes only and does not constitute medical advice. RevisionTown does not provide diagnosis, treatment, or medical recommendations. Always consult a qualified healthcare professional regarding any medical condition, symptoms, or concerns.
Read More – 🏥 Medical Disclaimer
Rheumatoid Arthritis: A Comprehensive Report
1. Overview
What is rheumatoid arthritis?
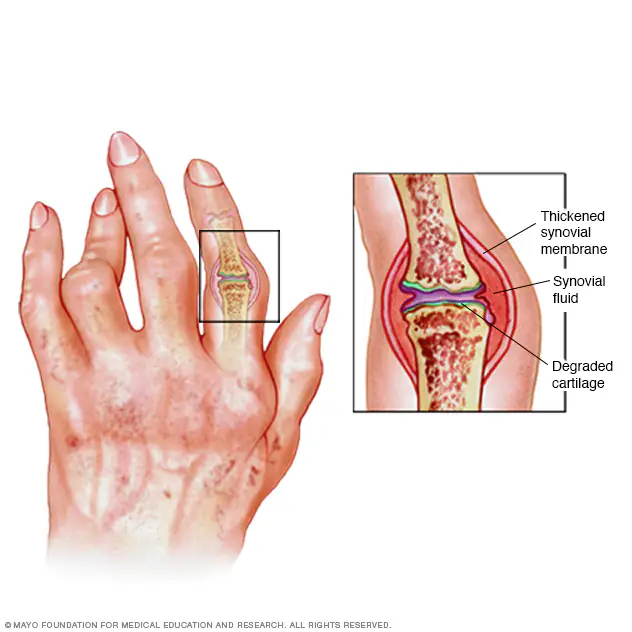
Rheumatoid arthritis (RA) is a chronic, progressive autoimmune disease characterized by inflammation of the synovial membrane that lines joints and tendons. In this condition, the immune system mistakenly attacks the body’s own tissues, primarily targeting the synovium—the thin membrane that lines the joints. This immune-mediated inflammatory process leads to pain, swelling, stiffness, and potential long-term joint damage and deformity. Unlike osteoarthritis, which results from mechanical wear and tear, RA is a systemic inflammatory disease that can affect multiple organs beyond the joints.
A concise yet detailed definition
Rheumatoid arthritis is a systemic autoimmune inflammatory disorder characterized by symmetric polyarthritis (inflammation of multiple joints on both sides of the body), morning stiffness lasting more than one hour, production of autoantibodies (rheumatoid factor and anti-citrullinated protein antibodies), persistent synovitis, and progressive joint destruction if left untreated. It follows a chronic course with periods of flares and remissions and can lead to extra-articular manifestations affecting cardiovascular, pulmonary, cutaneous, and other organ systems.
The affected body parts/organs
While RA primarily affects the joints, it can impact multiple body systems:
Primary joint involvement:
- Small joints of hands and feet (metacarpophalangeal, proximal interphalangeal, metatarsophalangeal joints)
- Wrists
- Elbows
- Shoulders
- Knees
- Ankles
- Cervical spine
Extra-articular manifestations:
- Cardiovascular system: increased risk of atherosclerosis, pericarditis, myocarditis
- Respiratory system: interstitial lung disease, pleural effusion, pulmonary nodules
- Skin: rheumatoid nodules, vasculitis, pyoderma gangrenosum
- Eyes: scleritis, episcleritis, keratoconjunctivitis sicca (dry eyes)
- Neurological system: peripheral neuropathy, mononeuritis multiplex, cervical myelopathy
- Hematologic system: anemia of chronic disease, Felty’s syndrome
- Exocrine glands: secondary Sjögren’s syndrome (dry eyes and mouth)
- Bones: osteoporosis, localized bone erosions
Prevalence and significance of the disease
Rheumatoid arthritis affects approximately 0.5-1% of the adult population worldwide, with some geographic variations. Key statistics include:
- Affects about 1.3 million Americans and more than 17 million people globally
- Women are 2-3 times more likely to develop RA than men
- Typical onset between ages 30-60, but can occur at any age
- Juvenile idiopathic arthritis affects approximately 1 in 1,000 children
- Economic burden estimated at $19.3 billion annually in the United States alone
- Leading cause of work disability among working-age adults
- Associated with reduced life expectancy of 3-10 years if inadequately treated
- Quality of life comparable to or worse than many advanced-stage cancers or heart diseases
- Approximately 20-30% of untreated patients become permanently work-disabled within 2-3 years of diagnosis
2. History & Discoveries
When and how was rheumatoid arthritis first identified?
While descriptions of arthritis date back to ancient times, rheumatoid arthritis as a distinct clinical entity emerged much later:
- Ancient times (4500-1000 BCE): Evidence of inflammatory arthritis in skeletal remains from ancient Egypt and Native American populations
- 1800 BCE: Early descriptions of a condition resembling RA in ancient Indian texts (Charaka Samhita)
- 1591: Guillaume de Baillou (Ballonius) distinguished arthritis from gout
- 1800: Dr. Augustin Jacob Landré-Beauvais from Paris formally described “primary asthenic gout” – the first recognized clinical description of RA
- 1858: Sir Alfred Baring Garrod coined the term “rheumatoid arthritis” to distinguish it from other forms of arthritis
- 1932: International Committee on Rheumatism established a standard nomenclature for the disease
- 1940s: RA officially classified as an autoimmune disease
Who discovered it?
Several key figures contributed to the identification and understanding of rheumatoid arthritis:
- Dr. Augustin Jacob Landré-Beauvais (1772-1840): French physician who published the first clinical description in 1800 as a separate entity from gout
- Sir Alfred Baring Garrod (1819-1907): British physician who coined the term “rheumatoid arthritis” in 1858
- Jean-Martin Charcot (1825-1893): French neurologist who further described joint deformities in RA
- Erik Waaler (1903-1997): Norwegian immunologist who discovered rheumatoid factor in 1937
- Henry Kunkel (1916-1983): American immunologist who characterized rheumatoid factor as an autoantibody
- Peter Schur and Philip Hench: Contributed significantly to understanding the immunological aspects of RA
Major discoveries and breakthroughs in its research and treatment
Diagnostic breakthroughs:
- 1937-1940: Discovery of rheumatoid factor by Erik Waaler and its clinical application by Rose
- 1964: American Rheumatism Association (now American College of Rheumatology) established first diagnostic criteria
- 1970s: HLA-DR4 association with RA identified
- 1998: Anti-citrullinated protein antibodies (ACPA) discovered, more specific than rheumatoid factor
- 2010: New ACR/EULAR classification criteria for RA established, focusing on earlier diagnosis
Treatment milestones:
- 1929: Gold compounds introduced for RA treatment
- 1938: Sulfasalazine developed
- 1949: Cortisone identified as effective for RA by Philip Hench (Nobel Prize in Medicine)
- 1951: Methotrexate synthesized (used for RA from the 1980s)
- 1950s-1960s: Development of non-steroidal anti-inflammatory drugs (NSAIDs)
- 1970s: Acceptance of Disease-Modifying Antirheumatic Drugs (DMARDs) concept
- 1980s: Combination DMARD therapy introduced
- 1998: FDA approval of the first TNF inhibitor (infliximab), revolutionizing RA treatment
- 2000s: Development of additional biologics targeting different inflammatory pathways (IL-6, T-cell co-stimulation)
- 2012: First Janus kinase (JAK) inhibitor approved, introducing targeted synthetic DMARDs
- 2021: Approval of dual JAK inhibitors with enhanced selectivity
Evolution of medical understanding over time
Early theories (pre-1900s):
- Initially considered a variant of gout
- Later thought to be caused by infections or “bad humors”
- Classified as a degenerative joint disease similar to osteoarthritis
Early 20th Century:
- Recognition as a distinct inflammatory disorder
- Suspected infectious etiology
- Focus primarily on joint symptoms
Mid-20th Century:
- Classification as an autoimmune disease
- Discovery of rheumatoid factor and autoimmune mechanisms
- Recognition of systemic nature beyond joints
- Emergence of steroids and early DMARDs
Late 20th Century:
- Identification of genetic susceptibility factors
- Understanding of complex interplay between genetics and environment
- Recognition of cytokines (particularly TNF-α) in disease pathogenesis
- Development of biologics targeting specific immune pathways
21st Century:
- Molecular classification of RA (seropositive vs. seronegative)
- Understanding of citrullination in pathogenesis
- Recognition of pre-clinical phases of RA
- Development of precision medicine approaches
- Treat-to-target strategy and window of opportunity concept
- Recognition of remission as an achievable goal
- Focus on prevention strategies for high-risk individuals
3. Symptoms
Early symptoms vs. advanced-stage symptoms
Early symptoms (First 6 months):
- Morning stiffness lasting more than 30-60 minutes
- Fatigue and general malaise
- Low-grade fever (occasionally)
- Symmetrical joint pain and tenderness, particularly in:
- Metacarpophalangeal (MCP) joints (knuckles)
- Proximal interphalangeal (PIP) joints (middle finger joints)
- Wrists
- Metatarsophalangeal (MTP) joints (base of toes)
- Joint swelling and warmth
- Decreased grip strength
- Weight loss and reduced appetite
- Increased joint pain with inactivity
- Numbness or tingling in hands from early carpal tunnel syndrome
Advanced-stage symptoms (Established RA, >2 years):
- Persistent joint pain, swelling, and stiffness
- Joint deformities:
- Ulnar deviation of fingers
- Swan-neck deformities (hyperextension of PIP joint with flexion of DIP joint)
- Boutonnière deformities (flexion of PIP joint with hyperextension of DIP joint)
- Z-thumb deformity
- Hallux valgus and cock-up toes
- Joint instability and subluxation
- Range of motion limitations
- Muscle atrophy around affected joints
- Rheumatoid nodules (firm subcutaneous lumps)
- Visible joint destruction on imaging
- Extra-articular manifestations:
- Dry eyes and mouth (Sjögren’s syndrome)
- Pleural effusions
- Pulmonary fibrosis
- Pericarditis
- Vasculitis
- Ocular inflammation
- Sensory or motor neuropathy
Common vs. rare symptoms
Common symptoms (affecting >30% of patients):
- Symmetric joint pain
- Morning stiffness
- Fatigue
- Joint swelling
- Reduced joint range of motion
- Hand grip weakness
- Elevated inflammatory markers
- Low-grade fever during flares
- Sleep disturbances
- Depression and anxiety
- Rheumatoid nodules (in seropositive patients)
Rare symptoms (affecting <5% of patients):
- Felty’s syndrome (RA with splenomegaly and neutropenia)
- Caplan’s syndrome (RA with pulmonary nodules in coal miners)
- Rheumatoid vasculitis (inflammation of blood vessels)
- Cricoarytenoid arthritis (affecting voice box joints)
- Scleritis (inflammation of the white of the eye)
- Episcleritis (inflammation of the tissue covering the sclera)
- Atlantoaxial subluxation (joint instability in upper spine)
- Amyloidosis (protein deposits in tissues)
- Baker’s cyst rupture
- Raynaud’s phenomenon (in overlap syndromes)
- Pericardial effusion and tamponade
- Libman-Sacks endocarditis (heart valve lesions, more common in lupus overlap)
How symptoms progress over time
Pre-clinical phase:
- Often asymptomatic
- Detectable autoantibodies in blood (RF, ACPA) years before symptoms
- Occasional non-specific symptoms like fatigue or arthralgias without objective findings
Prodromal phase (0-3 months):
- Intermittent joint pain without swelling
- Morning stiffness lasting <30 minutes
- Symptoms may come and go
- Symptoms often attributed to overuse or aging
- Subtle inflammation may be detected with sensitive imaging
Early RA (3-12 months):
- Persistent symptoms in multiple joints
- Morning stiffness extending beyond 1 hour
- Symmetric involvement becomes more apparent
- Visible joint swelling develops
- Difficulty with fine motor tasks
- Pain interferes with daily activities
- Early erosions may be visible on imaging
Established RA (1-5 years):
- Increasing functional limitations
- More persistent symptoms despite initial treatments
- Development of erosions visible on conventional radiographs
- More consistent elevations in inflammatory markers
- Initial joint deformities may begin to develop
- Extra-articular manifestations more likely to appear
- Comorbidities related to inflammation begin to develop
Advanced RA (>5 years if inadequately treated):
- Fixed joint deformities
- Significant joint destruction on imaging
- Loss of independence in activities of daily living
- Work disability
- Progression of extra-articular disease
- Significant impact on quality of life
- Reduced life expectancy due to cardiovascular and other complications
Disease patterns over time:
- Monocyclic: Single episode followed by sustained remission (10-20% of patients)
- Polycyclic: Alternating periods of flares and remissions (70-80% of patients)
- Progressive: Continuous disease activity without remission (10-15% of patients)
With modern treatment strategies including early intervention, treat-to-target approaches, and biologic therapies, many patients can achieve low disease activity or remission, significantly altering the natural progression described above.
4. Causes
What are the biological and environmental causes?
Biological mechanisms:
Autoimmune dysregulation:
- Loss of immune tolerance to self-proteins
- Abnormal activation of T cells, B cells, and innate immune cells
- Production of autoantibodies (RF and ACPA)
- Imbalance between pro-inflammatory and anti-inflammatory cytokines
Synovial pathology:
- Synovial hyperplasia (thickening of synovial lining)
- Formation of pannus (invasive granulation tissue)
- Neoangiogenesis (formation of new blood vessels)
- Infiltration of immune cells into the synovium
- Release of matrix metalloproteinases and other tissue-degrading enzymes
Inflammatory cascade:
- Elevated levels of pro-inflammatory cytokines (TNF-α, IL-1, IL-6, IL-17)
- Activation of osteoclasts leading to bone erosion
- Complement system activation
- Oxidative stress and reactive oxygen species production
Citrullination:
- Post-translational modification of proteins (conversion of arginine to citrulline)
- Mediated by peptidylarginine deiminase (PAD) enzymes
- Creation of neo-epitopes that trigger immune responses in genetically susceptible individuals
Environmental factors:
Smoking:
- Most well-established environmental risk factor
- Increases risk 2-4 fold, particularly in genetically susceptible individuals
- Induces citrullination of proteins in the lungs
- Promotes production of ACPAs in susceptible individuals
Infections:
- Periodontal disease: Porphyromonas gingivalis produces PAD enzyme
- Epstein-Barr virus: Molecular mimicry with self-antigens
- Mycoplasma: Potential trigger in some individuals
- Gut microbiome dysbiosis: Altered bacterial populations may contribute
Occupational exposures:
- Silica dust (in mining, ceramics, glass manufacturing)
- Mineral oils and hydraulic fluids
- Asbestos
- Organic solvents
Other environmental factors:
- Vitamin D deficiency
- Air pollution
- Ultraviolet radiation (may be protective)
- Diet (high consumption of red meat, low antioxidants)
- Obesity
- Psychological stress
Genetic and hereditary factors
Genetic risk contributors:
HLA (Human Leukocyte Antigen) region:
- HLA-DRB1 shared epitope alleles (particularly *04:01, *04:04, and *01:01)
- Accounts for approximately 30-40% of genetic risk
- Associated with ACPA-positive RA
Non-HLA genes:
- PTPN22 (protein tyrosine phosphatase non-receptor type 22)
- STAT4 (signal transducer and activator of transcription 4)
- PADI4 (peptidyl arginine deiminase type 4)
- TRAF1-C5 (TNF receptor-associated factor 1-complement component 5)
- TNFAIP3 (tumor necrosis factor alpha-induced protein 3)
- CCR6 (chemokine receptor 6)
- IL6R (interleukin 6 receptor)
Epigenetic factors:
- DNA methylation alterations
- Histone modifications
- MicroRNA dysregulation
- These changes can be influenced by environmental exposures
Hereditary patterns:
- Twin studies show 15-30% concordance in identical twins (vs. 5% in fraternal twins)
- Siblings of RA patients have 2-4 times increased risk
- First-degree relatives have 3-5 times increased risk
- Heritability estimated at 50-60%
- More pronounced genetic component in ACPA-positive RA
- Complex inheritance pattern (non-Mendelian)
- Gene-environment interactions significantly modify risk
Any known triggers or exposure risks
Established triggers for RA onset or flares:
Hormonal changes:
- Postpartum period (particularly after first pregnancy)
- Breastfeeding may be protective
- Menopause
- Use of certain hormonal contraceptives
Physical trauma:
- Major joint injury
- Surgery
- “Deep joint” infections
Psychological stressors:
- Major life events
- Chronic stress
- Post-traumatic stress disorder
Lifestyle factors:
- Initiation of smoking
- Sleep deprivation
- Sudden change in physical activity
Dietary factors:
- High sodium intake
- Excessive sugar consumption
- Food sensitivities in some individuals
Medications:
- Certain antibiotics (rare)
- Immune checkpoint inhibitors used in cancer treatment
- Interferon therapy
Infections:
- Viral infections (especially upper respiratory)
- Gastrointestinal infections
- Urinary tract infections
- COVID-19 (emerging evidence)
Weather changes:
- Rapid barometric pressure fluctuations
- Cold, damp conditions (may exacerbate existing symptoms)
Pregnancy and postpartum:
- Symptoms often improve during pregnancy (particularly 2nd and 3rd trimesters)
- Increased risk of flares in postpartum period
5. Risk Factors
Who is most at risk (age, gender, occupation, lifestyle, etc.)?
Demographic factors:
Gender:
- Women are 2-3 times more likely than men to develop RA
- Female predominance less pronounced in elderly-onset RA
- Men often have more severe disease when affected
Age:
- Peak onset between 30-60 years
- Can occur at any age, including childhood and elderly
- Bimodal distribution with peaks at 35-45 and 65-75 years
- Elderly-onset RA (>60 years) has distinct characteristics
Race/Ethnicity:
- Native American populations (particularly Pima and Chippewa tribes) have highest prevalence (5-7%)
- Higher prevalence in some Northern European populations
- Lower prevalence in Southern European and Asian populations
- African-Americans may have earlier onset and more aggressive disease
Occupation and socioeconomic factors:
Occupational exposures:
- Silica exposure: mining, stonecutting, glassmaking (RR 3-5)
- Textile industry workers
- Hairdressers (chemical exposures)
- Agricultural workers (pesticides)
- Manufacturing with mineral oils
Socioeconomic status:
- Lower education level associated with higher risk
- Lower income associated with poorer outcomes
- Limited healthcare access delays diagnosis and treatment
Lifestyle factors:
Smoking:
- Current smoking increases risk 2-4 fold
- 35-55% increased risk in past smokers
- Dose-dependent relationship (pack-years)
- Strongest environmental risk factor
Diet:
- High consumption of red meat and processed foods
- Low intake of omega-3 fatty acids
- Low antioxidant consumption (fruits, vegetables)
- High sodium intake
- Low vitamin D levels
Body composition:
- Obesity (BMI >30) increases risk by 1.5-2 fold
- Abdominal obesity particularly associated
- Severe obesity associated with poorer treatment response
Physical activity:
- Regular moderate physical activity may be protective
- Extremely strenuous activities may increase risk in some
Alcohol:
- Moderate alcohol consumption (particularly red wine) may be protective
- Heavy alcohol use may increase inflammation
Environmental, occupational, and genetic factors
Environmental factors:
Geography and climate:
- Higher prevalence in northern latitudes
- Urban environments have higher rates than rural
- Possible relationship with ambient air pollution
Early life exposures:
- Breastfeeding is protective for developing RA later in life
- Childhood adversity increases adult RA risk
- Birth weight extremes may influence risk
Infections:
- Periodontal disease (2-fold increased risk)
- Prior Epstein-Barr virus infection
- Recurrent urinary tract infections
- Intestinal dysbiosis
Pollutants:
- Air pollution (particulate matter)
- Pesticides
- Dioxins and polychlorinated biphenyls (PCBs)
- Heavy metals
Occupational factors:
Physical demands:
- Repetitive joint strain
- Vibration exposure
- Prolonged standing
- Heavy lifting
Chemical exposures:
- Organic solvents
- Crystalline silica (most significant occupational risk)
- Asbestos
- Metal fumes
Workplace stress:
- High demand/low control work environments
- Shift work disrupting circadian rhythms
- Workplace harassment and bullying
Genetic susceptibility:
HLA associations:
- HLA-DRB1 shared epitope (strongest genetic risk)
- Particularly HLA-DRB1*04:01, *04:04, *01:01, *10:01
- Different HLA associations in different ethnic groups
Polygenic risk scores:
- Combination of multiple gene variants
- Enhances predictive value when combined with environmental factors
- Different genetic profiles may predict different disease subtypes
Family history impact:
- First-degree relative with RA increases risk 3-5 fold
- Multiple affected relatives further increases risk
- Earlier age of onset in relatives associated with higher risk
Gene-environment interactions:
- HLA-DRB1 + smoking creates synergistic risk
- PTPN22 risk allele + smoking
- Epigenetic modifications from environmental exposures
Impact of pre-existing conditions
Autoimmune conditions:
- Sjögren’s syndrome: 10-15% of RA patients develop secondary Sjögren’s
- Autoimmune thyroid disease: 2-3 fold increased risk of RA
- Psoriasis: May develop psoriatic arthritis features or true RA
- Type 1 diabetes: Modest increased risk of RA
- Multiple sclerosis: Reduced risk of RA (possibly due to opposite genetic risk factors)
Metabolic conditions:
- Obesity: 1.5-2 fold increased risk; reduces treatment effectiveness
- Type 2 diabetes: Associated with more severe disease
- Metabolic syndrome: Associated with higher disease activity
- Hyperlipidemia: May contribute to systemic inflammation
Psychiatric conditions:
- Depression: Bidirectional relationship with RA development and severity
- Anxiety disorders: Associated with increased pain perception
- Post-traumatic stress disorder: Associated with higher RA risk
- Chronic stress: Alters immune function, potentially triggering autoimmunity
Other medical conditions:
- Periodontal disease: Strong bidirectional relationship with RA
- Chronic obstructive pulmonary disease: Shared risk factors with RA
- Interstitial lung disease: May precede joint symptoms in some RA patients
- Inflammatory bowel disease: Shared pathophysiological mechanisms
- Chronic kidney disease: May limit treatment options
- Prior joint injury: Local trauma may trigger RA in predisposed individuals
- Chronic infections: May prime autoimmune responses
6. Complications
What complications can arise from rheumatoid arthritis?
Joint complications:
Structural damage:
- Joint erosions (bone destruction)
- Cartilage loss
- Joint space narrowing
- Subchondral cysts
- Ankylosis (joint fusion)
Deformities:
- Ulnar deviation of fingers
- Swan-neck deformities
- Boutonnière deformities
- Z-thumb (hitchhiker’s thumb)
- Hallux valgus (bunions)
- Cock-up toes
- Joint subluxation and dislocation
Biomechanical complications:
- Ligament laxity
- Tendon ruptures (especially extensor tendons)
- Carpal tunnel syndrome (median nerve compression)
- Trigger finger/thumb (stenosing tenosynovitis)
- Atlantoaxial subluxation (C1-C2 instability)
- Baker’s cysts (popliteal cysts)
Extra-articular complications:
Cutaneous:
- Rheumatoid nodules (15-20% of patients)
- Palmar erythema
- Vasculitic lesions and ulcers
- Pyoderma gangrenosum
- Neutrophilic dermatosis
- Raynaud’s phenomenon
Cardiovascular:
- Accelerated atherosclerosis
- Increased risk of myocardial infarction (1.5-2 fold)
- Pericarditis and pericardial effusion
- Myocarditis
- Conduction abnormalities
- Heart failure (2-fold increased risk)
- Valvular heart disease
Pulmonary:
- Interstitial lung disease (10-30% of patients)
- Pleural effusions
- Pulmonary nodules
- Bronchiectasis
- Pulmonary hypertension
- Cricoarytenoid arthritis affecting breathing
Neurological:
- Peripheral neuropathy
- Mononeuritis multiplex
- Cervical myelopathy from C1-C2 subluxation
- Entrapment neuropathies (carpal tunnel, tarsal tunnel)
- Posterior scleritis and scleromalacia perforans
Hematologic:
- Anemia of chronic disease (most common, 30-60%)
- Felty’s syndrome (RA + splenomegaly + neutropenia)
- Eosinophilia
- Thrombocytosis
- Lymphadenopathy
- Large granular lymphocyte syndrome
Ocular:
- Keratoconjunctivitis sicca (dry eyes)
- Episcleritis and scleritis
- Peripheral ulcerative keratitis
- Retinal vasculitis
- Cataracts (increased by steroid treatment)
Other systemic:
- Secondary amyloidosis (rare in developed countries)
- Fatigue and constitutional symptoms
- Cachexia and sarcopenia
- Osteoporosis (2.5-fold increased risk)
- Increased infection susceptibility
Long-term impact on organs and overall health
Cardiovascular system:
- 50-60% increased cardiovascular mortality
- Accelerated atherosclerosis independent of traditional risk factors
- Endothelial dysfunction from systemic inflammation
- Earlier onset of ischemic heart disease (8-10 years earlier than general population)
- Increased arterial stiffness
- Chronic inflammation contributes to plaque instability
Respiratory system:
- Interstitial lung disease affects up to 30% of patients
- Respiratory complications are second leading cause of RA-related mortality
- Progressive fibrosis can lead to respiratory failure
- Bronchiectasis from recurrent infections
- Increased susceptibility to pneumonia
- Methotrexate pneumonitis (rare drug complication)
Skeletal system:
- Systemic and localized bone loss
- 1.5-2 fold increased fracture risk
- Secondary osteoporosis from inflammation and glucocorticoid use
- Increased risk of fragility fractures
- Higher rate of delayed fracture healing
- Osteonecrosis (especially with steroid use)
Neurological system:
- Cognitive impairment associated with chronic inflammation
- Fatigue affecting cognitive performance
- Increased risk of depression and anxiety
- Sleep disturbances affecting overall health
- Chronic pain leading to central sensitization
Endocrine and metabolic impacts:
- Insulin resistance and metabolic syndrome
- Hypothalamic-pituitary-adrenal axis dysfunction
- Sarcopenia and cachexia from cytokine effects
- Altered lipid metabolism
- Increased visceral adiposity despite normal BMI (“rheumatoid cachexia”)
Immune system:
- Chronic immune dysregulation
- Increased risk of lymphoma (2-4 fold)
- Increased susceptibility to infections
- Reactivation of latent infections (tuberculosis, herpes zoster)
- Vaccine response may be attenuated
Renal system:
- Secondary amyloidosis (decreased with better treatments)
- Medication-related nephrotoxicity
- Increased risk of renal disease (1.5-2 fold)
- Glomerulonephritis in severe cases
Potential disability or fatality rates
Functional disability:
- Without treatment, 50-70% of patients develop work disability within 10 years
- With modern treatment, work disability reduced to 20-30% at 10 years
- Health Assessment Questionnaire (HAQ) scores increase by ~0.03 units/year without treatment
- 25-35% of patients require joint replacement surgery within 20 years
- 10-15% become wheelchair-dependent without adequate treatment
- Daily activity limitations affect >50% of patients at some point
Disability progression:
- Early RA: primarily reversible disability from pain and inflammation
- Established RA: mix of reversible and irreversible components
- Late-stage RA: primarily irreversible structural damage
- Most disability accrues in first 2 years without treatment
- Early treatment can prevent >60% of expected disability
- Independent predictors of disability: female sex, older age, lower education, higher baseline disability, positive RF/ACPA, erosions at diagnosis
Mortality rates:
- Standardized mortality ratio of 1.5-1.6 compared to general population
- Life expectancy reduced by 3-10 years
- Gap narrowing with modern treatments (from 1.5 to 1.2-1.3 standardized ratio)
- 5-year survival of 80-85% for severe, untreated disease
- 10-year survival >95% with modern early treatment approaches
- Leading causes of death: cardiovascular disease (40%), infections (25%), respiratory complications (10-15%), malignancy (10%)
- Mortality risk correlates with disease activity, functional disability, extra-articular manifestations, and comorbidities
Prognostic factors for severe disability/mortality:
- High levels of acute phase reactants (ESR, CRP)
- High number of swollen joints
- Early erosions on imaging
- Positive for both RF and ACPA, especially at high titers
- Extra-articular manifestations, particularly lung involvement
- Poor functional status at diagnosis
- Older age at onset
- Male sex associated with higher mortality but lower disability
- Lower socioeconomic status
- Delayed treatment initiation
- Poor response to initial therapy
7. Diagnosis & Testing
Common diagnostic procedures
Clinical assessment:
- Detailed medical history (joint symptoms, morning stiffness, systemic symptoms)
- Family history of autoimmune diseases
- Comprehensive physical examination
- Joint examination (swelling, tenderness, range of motion)
- Assessment for extra-articular manifestations
- Functional ability evaluation
- Disease activity scoring systems:
- Disease Activity Score-28 (DAS28)
- Clinical Disease Activity Index (CDAI)
- Simplified Disease Activity Index (SDAI)
- Routine Assessment of Patient Index Data 3 (RAPID3)
Laboratory testing:
- Inflammatory markers
- Erythrocyte sedimentation rate (ESR)
- C-reactive protein (CRP)
- Autoantibodies
- Rheumatoid factor (RF)
- Anti-citrullinated protein antibodies (ACPA/anti-CCP)
- Anti-nuclear antibodies (ANA)
- Complete blood count (CBC)
- Comprehensive metabolic panel
- Synovial fluid analysis (when available)
- Cell count and differential
- Crystal examination
- Culture if infection suspected
Imaging studies:
- Plain radiographs (X-rays) of hands, wrists, and feet
- Ultrasound of affected joints
- Magnetic resonance imaging (MRI)
- Dual-energy X-ray absorptiometry (DEXA) scan for bone density
Medical tests (e.g., blood tests, imaging, biopsies)
Blood tests in detail:
Rheumatoid factor (RF):
- Sensitivity: 60-80%
- Specificity: 70-80%
- Not specific for RA (can be positive in other conditions)
- Higher titers correlate with disease severity
- IgA RF may have higher specificity than IgM RF
Anti-citrullinated protein antibodies (ACPA/anti-CCP):
- Sensitivity: 60-75%
- Specificity: 95-98%
- Can be positive years before clinical symptoms
- Highly specific for RA
- Associated with more severe, erosive disease
- Multiple generations of tests (CCP1, CCP2, CCP3)
Anti-carbamylated protein antibodies (anti-CarP):
- Newer biomarker
- Can be present in ACPA-negative patients
- Associated with more severe disease
Other autoantibodies:
- Anti-mutated citrullinated vimentin (anti-MCV)
- Anti-RA33 (anti-hnRNP A2/B1)
- Anti-PAD4
Inflammatory markers:
- ESR: reflects fibrinogen levels, influenced by age, anemia
- CRP: more specific for acute inflammation, not affected by anemia
- Serum amyloid A (SAA): may correlate better with disease activity in some patients
Additional blood tests:
- Hematology panel (anemia, thrombocytosis common in active disease)
- Liver and kidney function tests (baseline and monitoring during treatment)
- Hepatitis B and C serology (before immunosuppressive therapy)
- Tuberculosis screening (before biologics)
- Cytokine panels (research setting)
Imaging modalities in detail:
Conventional radiography (X-rays):
- Standard imaging for diagnosis and monitoring
- Shows erosions, joint space narrowing, periarticular osteopenia
- Limited sensitivity for early disease
- Sharp/van der Heijde or Larsen scoring systems for quantification
- Typical changes: periarticular osteopenia, marginal erosions, uniform joint space loss
Musculoskeletal ultrasound:
- Detects synovitis, tenosynovitis, erosions earlier than X-rays
- Allows dynamic assessment
- Can guide joint aspirations and injections
- Doppler imaging assesses inflammation activity
- Operator-dependent technique
Magnetic resonance imaging (MRI):
- Highest sensitivity for early inflammatory changes
- Detects bone marrow edema (predictor of erosions)
- Visualizes synovitis, tenosynovitis, and erosions
- RAMRIS (Rheumatoid Arthritis MRI Scoring) system for standardization
- Limited by cost and availability
Computed tomography (CT):
- Superior to X-rays for detecting erosions
- Useful for assessing complex joints (spine, sacroiliac)
- Higher radiation exposure than X-rays
- Limited soft tissue contrast compared to MRI
Nuclear medicine imaging:
- Bone scintigraphy
- PET-CT with FDG can detect inflammatory activity
- Limited resolution but good for whole-body assessment
- Primarily used in research or atypical presentations
Biopsy and tissue testing:
Synovial biopsy:
- Not routine but helpful in unclear cases
- Obtained via arthroscopy, ultrasound-guided, or open procedure
- Histopathology shows synovial hyperplasia, increased vascularity, inflammatory infiltrates
- Useful for research on disease mechanisms
- May help differentiate RA from other arthritides
Rheumatoid nodule biopsy:
- Shows palisading granulomas
- Central fibrinoid necrosis surrounded by macrophages
- Helps confirm diagnosis in seronegative cases with nodules
Synovial fluid analysis:
- Cell count typically 2,000-50,000 cells/mm³ (inflammatory range)
- Predominance of neutrophils (>75%)
- Low viscosity
- Poor mucin clot
- Glucose lower than serum
- Protein elevation
- Negative for crystals and microorganisms
Early detection methods and their effectiveness
Clinical prediction rules:
2010 ACR/EULAR Classification Criteria:
- Sensitivity: 80-85% for early RA
- Specificity: 80-85%
- Focuses on joint involvement, serology, acute phase reactants, and symptom duration
- Score ≥6/10 classifies as definite RA
van der Helm prediction rule:
- Combines clinical features and laboratory tests
- Sensitivity: 70%
- Specificity: 74% for progression to RA in undifferentiated arthritis
Leiden prediction rule:
- Predicts progression from undifferentiated arthritis to RA
- Includes age, joint distribution, morning stiffness, tender/swollen joint count, CRP, RF, ACPA
- Sensitivity: 70-75%
- Specificity: 70-80%
Serological biomarkers for early detection:
ACPA testing:
- Present in 50-70% of patients before clinical symptoms
- Can appear 5-10 years before diagnosis
- Effectiveness: ~95% specificity, 70% sensitivity
- Predictive value increases with higher titers
RF isotypes:
- IgM, IgA, and IgG RF
- Multiple isotype positivity increases diagnostic accuracy
- Effectiveness: Combined testing sensitivity 80%, specificity 85%
Biomarker panels:
- Combining multiple markers (RF, ACPA, anti-CarP, 14-3-3η protein)
- Improves sensitivity to 80-90% while maintaining specificity
- Commercially available multi-biomarker disease activity (MBDA) tests
Advanced imaging for early detection:
Power Doppler ultrasound:
- Detects subclinical synovitis
- Can identify patients at risk for developing RA
- Predictive of erosive progression
- Effectiveness: Sensitivity 85-90%, specificity 75-80% for early synovitis
MRI:
- Detects bone marrow edema before erosions develop
- Identifies synovitis not apparent on clinical examination
- Effectiveness: Sensitivity >90%, specificity 80-85% for early inflammatory changes
- Presence of bone marrow edema has 80% positive predictive value for erosion development
Early arthritis clinics:
- Specialized centers for rapid assessment of new joint symptoms
- Reduce time to diagnosis by 50-60%
- Decrease time to treatment initiation
- Improve long-term outcomes
- Cost-effective approach to early detection
Screening high-risk populations:
- First-degree relatives of RA patients
- Those with nonspecific musculoskeletal symptoms
- ACPA-positive individuals without arthritis
- Individuals with inflammatory arthralgia
- Effectiveness: Number needed to screen to identify one pre-clinical RA case: 50-100 in general population; 5-10 in high-risk groups
8. Treatment Options
Standard treatment protocols
Treatment strategy principles:
- Early aggressive intervention (“window of opportunity”)
- Treat-to-target approach (remission or low disease activity)
- Tight control with regular monitoring and adjustments
- Shared decision-making with patients
- Multidisciplinary team approach
- Consideration of comorbidities
Initial treatment approach:
- Early diagnosis (ideally within 12 weeks of symptom onset)
- Disease activity assessment using validated measures (DAS28, CDAI, SDAI)
- Prognostic factor evaluation (seropositivity, erosions, extra-articular features)
- Treatment initiation with DMARDs, often with short-term glucocorticoids
- Regular monitoring (every 1-3 months until target achieved)
- Treatment adjustment if target not reached within 3-6 months
Treatment guidelines (ACR/EULAR consensus):
Initial DMARD therapy for newly diagnosed patients:
- Methotrexate (MTX) monotherapy preferred initial agent (10-25 mg weekly)
- Alternatives: leflunomide, sulfasalazine, hydroxychloroquine
- Short-term low-dose glucocorticoids (prednisone ≤10 mg/day)
- NSAIDs as adjunctive therapy for symptom control
Moderate to high disease activity despite initial DMARD:
- Add or switch to combination conventional DMARDs (MTX + sulfasalazine + hydroxychloroquine) OR
- Add a biologic or targeted synthetic DMARD:
- TNF inhibitors (adalimumab, etanercept, infliximab, golimumab, certolizumab)
- IL-6 receptor antagonists (tocilizumab, sarilumab)
- T-cell co-stimulation modulator (abatacept)
- Anti-CD20 therapy (rituximab)
- JAK inhibitors (tofacitinib, baricitinib, upadacitinib, filgotinib)
Treatment failure on biologic/targeted DMARD:
- Switch to a different mechanism of action
- Consider cycling through available therapies
- Reevaluate diagnosis and comorbidities
- Consider combination therapy approaches
Sustained remission management:
- Maintain therapy for at least 6-12 months
- Consider gradual dose reduction (not discontinuation)
- Monitor closely for flares
- Adjust non-pharmacological approach
Treatment in special populations:
- Pregnancy: hydroxychloroquine, sulfasalazine, certolizumab considered safer
- Elderly: dose adjustment, close monitoring for adverse effects
- Hepatic/renal impairment: dose adjustment or alternative agents
- History of malignancy: abatacept or non-TNF biologics preferred
Medications, surgeries, and therapies
Pharmacological options:
Non-steroidal anti-inflammatory drugs (NSAIDs):
- Provide symptomatic relief without affecting disease course
- Examples: ibuprofen, naproxen, celecoxib, diclofenac
- Mechanism: COX-1/COX-2 inhibition
- Side effects: GI bleeding, cardiovascular risks, renal effects
- Used as adjunctive therapy, not disease-modifying
Glucocorticoids:
- Rapid anti-inflammatory effect
- Oral, intra-articular, or parenteral routes
- Bridging therapy until DMARDs take effect
- Low-dose (<10 mg prednisone equivalent daily)
- Side effects: osteoporosis, diabetes, hypertension, weight gain, cataracts
- Long-term use discouraged
Conventional synthetic DMARDs:
- Methotrexate:
- Cornerstone of RA treatment
- Weekly dosing (oral or subcutaneous)
- Mechanism: folate antagonism, adenosine-mediated
- Side effects: hepatotoxicity, pneumonitis, bone marrow suppression
- Requires folic acid supplementation
- Leflunomide:
- Daily oral dosing
- Mechanism: pyrimidine synthesis inhibition
- Similar efficacy to methotrexate
- Side effects: diarrhea, hepatotoxicity, teratogenicity
- Sulfasalazine:
- Oral dosing (typically 2-3 g/day)
- Mechanism: anti-inflammatory and immunomodulatory
- Side effects: GI intolerance, rash, bone marrow suppression
- Hydroxychloroquine:
- Oral dosing (up to 5 mg/kg/day)
- Mechanism: interference with antigen presentation
- Milder DMARD, often used in combination
- Side effects: retinopathy (rare), GI upset
- Others: azathioprine, cyclosporine, gold compounds (rarely used)
- Methotrexate:
Biological DMARDs:
- TNF inhibitors:
- Adalimumab, etanercept, infliximab, golimumab, certolizumab
- Subcutaneous or intravenous administration
- First biologic class for RA
- Side effects: infection risk, demyelinating disorders, heart failure
- IL-6 receptor antagonists:
- Tocilizumab, sarilumab
- Subcutaneous or intravenous administration
- Effective in TNF-resistant cases
- Side effects: neutropenia, lipid elevations, GI perforation risk
- T-cell co-stimulation modulator:
- Abatacept
- Intravenous or subcutaneous administration
- Blocks T-cell activation
- Side effects: generally well-tolerated, infection risk
- B-cell depleting therapy:
- Rituximab
- Intravenous infusion
- Depletes CD20+ B cells
- Side effects: infusion reactions, infection risk, hypogammaglobulinemia
- IL-1 receptor antagonist:
- Anakinra (less commonly used for RA)
- Daily subcutaneous injection
- Less effective than other biologics for RA
- TNF inhibitors:
Targeted synthetic DMARDs:
- JAK inhibitors:
- Tofacitinib, baricitinib, upadacitinib, filgotinib
- Oral administration
- Block intracellular signaling pathways
- Rapid onset of action
- Side effects: infection risk, herpes zoster, VTE risk, lipid elevations, cytopenias
- JAK inhibitors:
Surgical interventions:
Synovectomy:
- Removal of inflamed synovium
- Arthroscopic or open procedure
- Temporary relief, most effective for single joint involvement
- Less common with improved medical therapy
Tenosynovectomy:
- Removal of inflamed tendon sheaths
- Prevents tendon rupture
- Most common for extensor tendons of the hand
Arthrodesis (joint fusion):
- Permanently stabilizes a joint
- Relieves pain at cost of motion
- Most commonly performed in wrist, ankle, certain finger joints
Arthroplasty (joint replacement):
- Most common in knees, hips, shoulders, elbows
- Effectively relieves pain and improves function
- 20-25% of RA patients eventually need at least one joint replacement
- Modern implants last 15-20+ years
Reconstructive hand/foot surgery:
- Tendon transfers
- Metatarsal head resection
- Hammer toe correction
- Boutonnière or swan-neck deformity correction
Other procedures:
- Carpal tunnel release
- Cervical spine stabilization for atlantoaxial subluxation
- Resection of rheumatoid nodules
Non-pharmacological therapies:
Physical therapy:
- Therapeutic exercises to maintain range of motion
- Muscle strengthening programs
- Joint protection techniques
- Aerobic conditioning
- Effectiveness: improves function by 20-40% in most patients
Occupational therapy:
- Adaptive equipment and assistive devices
- Joint protection education
- Energy conservation techniques
- Splinting for pain relief or deformity prevention
- Effectiveness: improves daily function by 30-50%
Psychological interventions:
- Cognitive behavioral therapy for pain management
- Stress reduction techniques
- Depression/anxiety management
- Effectiveness: reduces pain perception by 15-30%
Nutrition and dietary approaches:
- Mediterranean diet
- Omega-3 fatty acid supplementation
- Elimination diets for identified sensitivities
- Maintenance of healthy weight
- Effectiveness: modest anti-inflammatory effects (10-15% symptom reduction)
Complementary therapies:
- Acupuncture
- Massage therapy
- Tai chi and yoga
- Heat and cold therapy
- Effectiveness: variable, generally adjunctive to conventional treatment
Emerging treatments and clinical trials
Novel Biologic Targets:
GM-CSF inhibitors:
Otilimab (GSK3196165):
- Phase III clinical trials (ContRAst program)
- Targets granulocyte-macrophage colony-stimulating factor
- Reduces neutrophil activation
- May have beneficial effects on fatigue
Mavrilimumab:
- GM-CSF receptor antagonist
- Phase II trials showed good efficacy
- Potentially effective in refractory disease
Anti-IL-17 approaches:
- Secukinumab and ixekizumab:
- Effective in psoriatic arthritis
- Mixed results in RA trials
- May benefit a subset of patients
- Secukinumab and ixekizumab:
Dual cytokine inhibition:
- ABBV-3373: combines TNF inhibition with glucocorticoid receptor modulation
- ABT-122: dual TNF/IL-17 inhibitor in early development
- Anti-TNF/IL-6 bispecific antibodies
- Potential for greater efficacy with single agent
Other investigational biologics:
- Anti-BAFF/APRIL: targeting B-cell survival factors
- Anti-CD19 therapies: alternative B-cell depletion
- Anti-CD38: for plasma cell targeting
- PD-1/PD-L1 pathway modulation
Advanced Small Molecule Approaches:
Next-generation JAK inhibitors:
- Selective JAK1 inhibitors: filgotinib, upadacitinib (approved)
- JAK3-selective inhibitors: decernotinib
- TYK2 inhibitors: deucravacitinib
- Potentially improved safety profiles with selectivity
Novel intracellular signaling targets:
- BTK inhibitors: evobrutinib, fenebrutinib
- SYK inhibitors: lanraplenib
- PI3K inhibitors
- IRAK4 inhibitors
- Target specific inflammatory pathways
Epigenetic modifiers:
- BET inhibitors
- HDAC inhibitors
- DNA methyltransferase inhibitors
- Modifying gene expression patterns in immune cells
Cell-based and gene therapies:
CAR-T cell therapy:
- Engineering T-cells to target specific immune cells
- Early phase clinical trials
- Potential for long-lasting disease modification
Mesenchymal stem cell therapy:
- Immunomodulatory and tissue-regenerative properties
- Both autologous and allogeneic approaches
- Phase II trials show promise in refractory disease
Tolerance induction approaches:
- Autologous tolerogenic dendritic cells
- Regulatory T-cell expansion
- Aiming to restore immune self-tolerance
- Phase I/II clinical trials underway
RNA interference (RNAi) therapeutics:
- Targeting specific inflammatory gene expression
- Localized joint delivery systems
- Preclinical and early human studies
Precision medicine approaches:
Biomarker-guided therapy:
- Multi-biomarker disease activity tests
- Genetic/transcriptomic profiles to guide treatment selection
- Synovial tissue analysis to predict response
- Several clinical trials testing personalized algorithms
Drug response prediction:
- Pharmacogenomic testing
- Serum drug level monitoring
- Antidrug antibody measurement
- Machine learning for treatment response prediction
Novel delivery systems:
- Intra-articular sustained release formulations
- Nanoparticle drug delivery
- Ultrasound-guided delivery technologies
- Joint-specific targeting to reduce systemic effects
Notable clinical trials:
- TARGET-JAK: Testing selective JAK inhibitors in different patient subgroups
- INBUILD-RA: Investigating early treatment of RA-associated interstitial lung disease
- TARA (Tapering And Discontinuing Antirheumatic Drugs): Treatment de-escalation strategies
- NORD-STAR: Head-to-head comparisons of different treatment strategies
- R4RA: Stratifying patients for rituximab vs. tocilizumab based on synovial biopsy
- SMART-CHOICE: Comparing different maintenance strategies after achieving low disease activity
- IDEA-RA: Implementing digital health tools for RA management
- PreventRA: Testing interventions in high-risk pre-clinical RA patients
9. Prevention & Precautionary Measures
How can rheumatoid arthritis symptoms be prevented?
Primary prevention (preventing disease onset):
Smoking cessation:
- Most modifiable risk factor
- Reduces risk by 30-40%
- Risk gradually decreases after quitting
- Public health campaigns targeting high-risk groups
Maintaining oral health:
- Regular dental care
- Treatment of periodontal disease
- May reduce risk by 15-20%
- Especially important in genetically susceptible individuals
Dietary approaches:
- Mediterranean diet rich in olive oil, fish, fruits, vegetables
- Omega-3 fatty acid consumption
- Limited red meat intake
- Moderate alcohol consumption (particularly red wine)
- May reduce risk by 10-30%
Weight management:
- Maintaining healthy BMI
- Avoiding central obesity
- Risk reduction proportional to weight normalization
- Decreases inflammatory burden
Physical activity:
- Regular moderate exercise
- 150+ minutes weekly
- Strengthening and aerobic components
- Reduces risk by 15-35%
Secondary prevention (early disease intervention):
Recognition of arthralgias in high-risk individuals:
- Prompt assessment of inflammatory symptoms
- Screening in first-degree relatives
- Evaluation of ACPA-positive individuals without arthritis
- Early arthritis clinics
Treatment in pre-clinical phases:
- Clinical trials examining very early intervention
- Hydroxychloroquine for undifferentiated arthritis
- Biologics in high-risk autoantibody-positive individuals
- Window of opportunity concept
Addressing environmental triggers:
- Occupational exposure modification
- Stress management strategies
- Vitamin D supplementation when deficient
- Potential microbiome interventions
Tertiary prevention (preventing complications):
Tight disease control:
- Early DMARD therapy
- Treat-to-target approach
- Regular disease activity monitoring
- Prevents 70% of joint damage
Joint protection strategies:
- Ergonomic techniques
- Activity modification
- Assistive devices
- Splinting when indicated
Comorbidity management:
- Cardiovascular risk assessment and intervention
- Osteoporosis prevention
- Infection prevention (vaccinations)
- Mental health support
Regular monitoring:
- Radiographic assessment
- Function and quality of life measures
- Extra-articular manifestation screening
- Medication toxicity monitoring
Lifestyle changes and environmental precautions
Physical activity recommendations:
Aerobic exercise:
- Low-impact activities (swimming, cycling, walking)
- 150 minutes per week moderate intensity
- Divided into 10-30 minute sessions
- Gradually increasing intensity and duration
Strength training:
- 2-3 sessions weekly
- Focus on major muscle groups
- Lightweight, higher repetitions
- Proper technique to avoid joint stress
Flexibility exercises:
- Daily gentle stretching
- Range of motion exercises
- Yoga or tai chi classes modified for RA
- Focus on commonly affected joints
Rest and pacing:
- Balance activity with rest
- Activity pacing techniques
- Energy conservation strategies
- Listening to body signals
Dietary considerations:
Anti-inflammatory diet components:
- Omega-3 rich foods (fatty fish, flaxseed, walnuts)
- Antioxidant-rich fruits and vegetables
- Olive oil as primary fat
- Whole grains and legumes
- Turmeric, ginger, and other anti-inflammatory spices
Foods to limit:
- Processed foods high in trans fats
- Refined carbohydrates and sugars
- Excessive red meat
- Alcohol (if taking methotrexate or experiencing liver issues)
- Individual trigger foods (identified through elimination trials)
Supplements with evidence:
- Fish oil (2-4g daily)
- Vitamin D (if deficient)
- Curcumin (turmeric extract)
- Probiotics
- Gamma-linolenic acid
Occupational and environmental modifications:
Workplace adaptations:
- Ergonomic workstation assessment
- Adaptive equipment
- Regular position changes
- Voice recognition software
- Flexible scheduling
Home modifications:
- Lever door handles
- Raised toilet seats
- Grab bars in bathroom
- Kitchen adaptations
- Removal of fall hazards
Exposure avoidance:
- Smoking (active and passive)
- Silica dust
- Mineral oils
- Cold, damp environments
- Air pollution when possible
Stress management techniques:
Mind-body approaches:
- Meditation and mindfulness
- Progressive muscle relaxation
- Guided imagery
- Biofeedback
- Cognitive behavioral therapy
Social support:
- Patient support groups
- Family education
- Open communication with providers
- Online communities
- Relationship nurturing
Sleep hygiene:
- Consistent sleep schedule
- Comfortable mattress and pillows
- Pain management before bed
- Sleep environment optimization
- Addressing sleep apnea if present
Vaccines and preventive screenings
Immunization recommendations:
Standard adult vaccines:
- Influenza vaccine annually
- Pneumococcal vaccines (PCV13 and PPSV23)
- Tetanus-diphtheria-pertussis (Tdap) booster
- Herpes zoster vaccine (recommended at 50+ years)
- COVID-19 vaccination and boosters
Special considerations for RA patients:
- Live vaccines contraindicated on certain biologics/immunosuppressants
- Vaccinate before starting immunosuppressive therapy when possible
- Schedule vaccines between rituximab courses
- May have reduced response to vaccines
- Higher priority due to increased infection risk
Vaccine timing:
- Optimal: 2-4 weeks before starting immunosuppression
- If on treatment: consider temporary hold for certain vaccines
- Coordinate with rheumatologist for individualized schedule
- Family/household member vaccination important
Preventive health screenings:
Cardiovascular screening:
- Annual blood pressure monitoring
- Lipid profile every 1-2 years
- Consider advanced cardiovascular risk assessment
- ECG baseline and periodically
- More aggressive targets given increased risk
Bone health assessment:
- DEXA scan at diagnosis and periodically
- Vitamin D level monitoring
- Fracture risk assessment (FRAX score)
- Especially important if on glucocorticoids
Cancer screenings:
- Age-appropriate standard screenings
- Skin examinations (increased risk with some biologics)
- Consider more frequent screenings with certain therapies
- Lymphoma vigilance (slightly increased risk)
Lung assessment:
- Baseline pulmonary function tests
- Chest imaging if respiratory symptoms develop
- TB screening before biologics
- Regular assessment in patients with ILD
Medication monitoring:
- Methotrexate: CBC, liver enzymes, creatinine every 4-12 weeks
- TNF inhibitors: TB screening, hepatitis B screening
- JAK inhibitors: lipid profile, CBC monitoring
- Hydroxychloroquine: eye examinations
- Tailored to specific medication regimen
Regular rheumatology assessment:
- Disease activity scoring (DAS28, CDAI, RAPID3)
- Functional assessment (HAQ)
- Joint examinations
- Radiographic monitoring
- Treatment response evaluation
Pre-disease preventive approaches (emerging):
Screening high-risk individuals:
- First-degree relatives of RA patients
- ACPA testing in high-risk populations
- Genetic testing for research purposes
- Ultrasound screening for subclinical synovitis
Intervention studies in pre-clinical RA:
- PRAIRI trial: single rituximab dose in at-risk individuals
- TREAT-EARLIER: DMARD therapy in arthralgia at-risk patients
- STOP-RA: hydroxychloroquine in ACPA-positive subjects
- StopRA: abatacept in ACPA-positive without clinical RA
Preventive counseling:
- Smoking cessation for at-risk individuals
- Dental health education
- Early symptom recognition education
- Lifestyle modification guidance
10. Global & Regional Statistics
Incidence and prevalence rates globally
Global prevalence:
- Worldwide prevalence: 0.5-1% of adult population
- Approximately 17-50 million people affected globally
- Annual incidence: 40 per 100,000 population
- Women-to-men ratio: 3:1 during reproductive years; approaching 1:1 in elderly
- Geographic variations: 0.3-1.7% depending on region
Regional prevalence rates:
North America:
- United States: 0.5-1.0% (1.3-1.5 million people)
- Canada: 0.9% (300,000 people)
- Annual incidence: 40-50 per 100,000
Europe:
- Northern Europe: 0.7-1.0%
- Southern Europe: 0.3-0.7%
- Eastern Europe: 0.5-0.8%
- United Kingdom: 0.8% (approximately 400,000 people)
- Annual incidence: 20-50 per 100,000
Asia:
- Japan: 0.2-0.3%
- China: 0.2-0.4%
- India: 0.5-0.75%
- South Korea: 0.4-0.6%
- Annual incidence: 10-25 per 100,000
Latin America:
- Brazil: 0.5-1.0%
- Mexico: 0.8-1.2%
- Colombia: 0.4-0.6%
- Annual incidence: 20-40 per 100,000
Africa:
- Urban South Africa: 0.7-1.0%
- Rural African regions: 0.1-0.3%
- North Africa: 0.3-0.5%
- Annual incidence: 15-30 per 100,000
Oceania:
- Australia: 0.5-0.7%
- New Zealand: 0.7-0.9%
- Pacific Islands: variable, limited data
- Annual incidence: 25-45 per 100,000
Demographic patterns:
Age distribution:
- Peak incidence in women: 55-64 years
- Peak incidence in men: 65-74 years
- Juvenile onset (<16 years): 1 in 10,000 children
- Young-onset RA (16-40 years): 5-10% of cases
- Late-onset RA (>60 years): 20-30% of cases
Urban vs. rural:
- Higher prevalence in urban settings: 0.6-1.0%
- Lower in rural settings: 0.3-0.7%
- Greatest urban-rural differences in developing countries
Socioeconomic factors:
- Inverse relationship with socioeconomic status in many regions
- Education level inversely associated with prevalence
- More severe disease outcomes in lower socioeconomic groups
- Access to biologics highly variable by country income level
Mortality and survival rates
Mortality statistics:
- Standardized mortality ratio (SMR): 1.5-1.6 compared to general population
- Life expectancy reduction: 3-10 years depending on disease severity and treatment
- 5-year survival rate: 80-85% for severe disease; >95% with modern treatment
- 10-year survival rate: 70-75% for severe disease; 90-95% with modern treatment
- Annual mortality rate: 2.5% among RA patients vs. 1.5% in age-matched controls
Cause-specific mortality:
Cardiovascular disease:
- Leading cause of death (35-40%)
- 50-60% increased cardiovascular mortality
- Myocardial infarction risk: 2-fold increase
- Heart failure risk: 2-fold increase
- Sudden cardiac death: 1.5-fold increase
Infections:
- Second leading cause (25-30%)
- Pneumonia: 2-4 fold increased risk
- Sepsis: 2-fold increased risk
- Skin/soft tissue infections: 1.7-fold increase
- Mortality from infections doubled with biologics
Respiratory complications:
- Third leading cause (10-15%)
- Interstitial lung disease: 3-year survival 60-80%
- Bronchiectasis: 1.8-fold increased mortality
- COPD exacerbations: 1.5-fold increased risk
- Pulmonary hypertension: 5-year survival 50-60%
Malignancy:
- Fourth leading cause (8-10%)
- Lymphoma risk: 2-4 fold increase
- Lung cancer: 1.6-fold increase
- No significant increase in most solid tumors
- Treatment-related malignancy risk remains controversial
Gastrointestinal complications:
- Fifth leading cause (5-8%)
- GI bleeding: 1.5-2 fold increased risk
- Liver disease mortality: 1.3-fold increase
- Mainly related to treatment complications
Survival trends over time:
- 1960s-1970s: 5-year survival 50-60%
- 1980s-1990s: 5-year survival 70-75%
- 2000s-2010s: 5-year survival 85-90%
- 2020s: 5-year survival approaching 95%
- Gap between RA patients and general population narrowing
- Mortality improvements largely attributed to better disease control
Prognostic factors affecting survival:
- Disease severity: High disease activity doubles mortality risk
- Extra-articular manifestations: 3-fold increased mortality risk
- Functional status: HAQ score >2 associated with 4-fold mortality increase
- Seropositivity: RF/ACPA positivity increases mortality by 30-40%
- Early erosions: 50% increased mortality risk
- Treatment response: Achieving remission reduces mortality by 30-50%
- Comorbidities: Each major comorbidity adds 30-50% mortality risk
Country-wise comparison and trends
Disease burden by country income level:
High-income countries:
- Prevalence: 0.5-1.0%
- Biologic treatment access: 30-50% of eligible patients
- Work disability rate: 20-35% at 10 years
- Annual direct costs: $12,000-25,000 per patient
- Decreasing disability trends with modern treatment
Upper-middle-income countries:
- Prevalence: 0.4-0.9%
- Biologic treatment access: 5-30% of eligible patients
- Work disability rate: 40-60% at 10 years
- Annual direct costs: $5,000-15,000 per patient
- Significant urban-rural treatment disparities
Lower-middle-income countries:
- Prevalence: 0.3-0.8%
- Biologic treatment access: <5% of eligible patients
- Work disability rate: 50-70% at 10 years
- Annual direct costs: $1,000-5,000 per patient
- Significant delays in diagnosis and treatment
Low-income countries:
- Prevalence: 0.2-0.6% (likely underestimated)
- Biologic treatment access: <1% of eligible patients
- Work disability rate: 60-80% at 10 years
- Annual direct costs: $500-2,000 per patient
- Limited rheumatology specialists and diagnostic capacity
Notable country-specific data:
United States:
- Prevalence: 0.6% (1.5 million people)
- Annual direct costs: $19 billion
- Annual indirect costs: $40 billion
- Average annual per-patient cost: $30,000
- Work disability: 35% at 10 years
- Treatment disparities by insurance status and geography
United Kingdom:
- Prevalence: 0.8% (400,000 people)
- NHS annual expenditure: £700 million
- Regional variations in biologic access (28-42%)
- Work disability: 30% at 10 years
- NICE guidelines standardize care nationwide
Japan:
- Prevalence: 0.3% (380,000 people)
- Higher rates of interstitial lung disease (30-40%)
- Earlier biologic introduction compared to Europe
- Lower TNF inhibitor dosing common
- Lower rates of obesity-associated comorbidities
Brazil:
- Prevalence: 0.5-1.0% (1-2 million people)
- Universal health coverage includes DMARDs
- Biologic access: 10-15% of eligible patients
- Regional disparities in specialized care
- Social security disability costs: $1.8 billion annually
India:
- Prevalence: 0.5-0.75% (6-9 million people)
- Significant urban-rural diagnosis gap
- Local biosimilar production increasing access
- High out-of-pocket costs limit treatment options
- Traditional medicine widely used alongside conventional
South Africa:
- Prevalence: 0.7-1.0% (urban), 0.1-0.3% (rural)
- HIV-associated RA challenges in diagnosis and treatment
- Public sector access to biologics extremely limited (<1%)
- Only 1 rheumatologist per 1.8 million population
- Higher tuberculosis risk complicating biologic use
Global trends and patterns:
Treatment access disparities:
- High-income countries: 30-50% of patients on biologics
- Middle-income countries: 5-15% on biologics
- Low-income countries: <5% on biologics
- 90% of global biologic use concentrated in high-income countries
- 7:1 ratio in DMARD access between high and low-income regions
Epidemiological shifts:
- Declining incidence in some developed nations
- Rising diagnosis rates in urbanizing regions
- Narrowing gender gap in elderly-onset disease
- Decreasing extra-articular manifestations with better treatment
- Reduced severity at presentation with earlier diagnosis
Healthcare system impacts:
- Direct medical costs: 0.3-0.8% of national healthcare expenditures
- Indirect costs typically 2-3 times direct medical costs
- Biologics represent 30-60% of direct RA medical costs
- Rising biosimilar use reducing cost burden (10-30% savings)
- Telemedicine increasing care access in remote regions
Disease burden and disability:
- Global DALYs (disability-adjusted life years): 4.8 million annually
- Ranks 42nd among global disease burdens
- Economic impact: $12,000-15,000 per patient per year globally
- Productivity losses account for 50-75% of total costs
- Intangible costs (pain, reduced quality of life) difficult to quantify
11. Recent Research & Future Prospects
Latest advancements in treatment and research
Treatment paradigm innovations:
Precision medicine approaches:
- Synovial biopsies for treatment selection:
- R4RA trial: Identifying rituximab vs. tocilizumab responders
- Synovial myeloid vs. lymphoid phenotypes guide therapy
- Ultrasound-guided minimally invasive biopsy techniques
- Pharmacogenomic markers:
- HLA-DRB1 genotype predicting methotrexate response
- TNF inhibitor response prediction algorithms
- MTHFR polymorphisms and methotrexate toxicity
- JAK inhibitor response markers
- Multi-omics prediction models:
- Combined genomic, transcriptomic, proteomic markers
- Machine learning algorithms integrating clinical and biomarker data
- PRECiSE RA initiative to identify responder subgroups
- Synovial biopsies for treatment selection:
Strategic treatment innovations:
- Pre-RA intervention studies:
- ARIAA trial: Abatacept in ACPA+ arthralgia
- TREAT EARLIER: Treatment in clinically suspect arthralgia
- APPIPRA: Abatacept in ACPA+ arthralgia without clinical arthritis
- Tapering and discontinuation approaches:
- POET study: Controlled withdrawal of TNF inhibitors
- DRESS strategy: Disease activity-guided dose reduction
- IMPROVED study: Drug-free remission strategies
- Predictors of successful tapering being identified
- Combination therapy refinements:
- Triple therapy optimization
- Biologic + JAK inhibitor combination safety studies
- Low-dose combination strategies
- Sequential monotherapy approaches
- Pre-RA intervention studies:
Novel therapeutic targets:
Emerging cytokine targets:
- IL-23/IL-17 pathway:
- Guselkumab, risankizumab (IL-23 inhibitors)
- Mixed results in RA despite efficacy in psoriatic arthritis
- Subset of patients may respond
- IL-2 pathway modulation:
- Low-dose IL-2 for regulatory T-cell expansion
- DICER trial: Selective IL-2 agonism
- Potential for immune tolerance induction
- GMCSF inhibition:
- Otilimab (GSK3196165) in phase III trials
- Particular benefits for fatigue symptoms
- Different mechanism from existing biologics
- IL-23/IL-17 pathway:
Cellular targets:
- Plasma cell depletion:
- Anti-CD38 therapies adapted from multiple myeloma
- Targeting long-lived antibody-producing cells
- Early trials in refractory disease
- Regulatory T-cell enhancement:
- Ex vivo expanded autologous Tregs
- Low-dose IL-2 therapy
- Tolerance induction protocols
- Synovial fibroblast targeting:
- Cadherin-11 inhibition
- Fibroblast activation protein (FAP) targeting
- Disrupting disease-associated fibroblast phenotypes
- Plasma cell depletion:
Intracellular signaling advances:
- Selective JAK inhibition:
- JAK1-selective: filgotinib, upadacitinib
- JAK3-selective: decernotinib
- TYK2 inhibition: deucravacitinib
- Improved safety/efficacy balance
- Beyond JAK/STAT:
- BTK inhibitors: evobrutinib, fenebrutinib
- IRAK4 inhibition: disrupting IL-1/TLR signaling
- PI3K-δ inhibitors for B-cell modulation
- RORγt inhibitors affecting Th17 differentiation
- Selective JAK inhibition:
Diagnostic and monitoring advances:
Molecular biomarkers:
- Expanded autoantibody profiling:
- Anti-CarP (anti-carbamylated protein) antibodies
- Anti-acetylated protein antibodies
- Autoantibody fine specificity and epitope spreading
- IgG subclass and glycosylation patterns
- Cytokine and chemokine signatures:
- Multi-marker panels to predict disease progression
- Pre-clinical signatures in high-risk individuals
- Treatment response prediction
- Flare prediction biomarkers
- Expanded autoantibody profiling:
Advanced imaging:
- Molecular imaging:
- PET-CT with synovitis-specific tracers
- Labeled antibody imaging of specific targets
- Early detection of subclinical inflammation
- Artificial intelligence applications:
- Automated joint space measurement
- Deep learning for erosion detection
- Radiomic feature extraction
- Integrated imaging biomarkers with clinical data
- Molecular imaging:
Digital health technologies:
- Remote monitoring devices:
- Wearable activity monitors
- Digital grip strength measurement
- Home-based joint temperature monitoring
- Smartphone-based gait analysis
- Patient-reported outcome platforms:
- Electronic symptom tracking
- Integrated PRO and biometric data
- Predictive algorithms for flare detection
- Digital therapeutic programs
- Remote monitoring devices:
Ongoing studies and future medical possibilities
Major clinical research initiatives:
Pathobiology-focused studies:
- REASON consortium: Synovial tissue analysis to determine disease endotypes
- AMP (Accelerating Medicines Partnership) RA Phase 2: Single-cell transcriptomics, spatial biology
- R4RA trial: Synovial biopsy-driven precision medicine
- TACERA: Identifying pre-clinical autoimmunity signatures
Treatment strategy trials:
- NORD-STAR: Head-to-head comparison of treatment strategies
- TARA: Controlled treatment tapering approaches
- MONITOR: Biomarker-guided vs. clinical tapering strategies
- SATORI: Sustained remission-oriented tapering
- SELECT-COMPARE extension: Long-term JAK vs. TNF inhibition
Prevention studies:
- StopRA: Abatacept to prevent RA in high-risk individuals
- STAPRA: Statins for prevention in at-risk individuals
- APIPPRA: Abatacept prevention in autoantibody-positive non-arthritic individuals
- TREAT EARLIER: Testing very early intervention
- PREDIRA: Prednisolone to prevent RA development
Real-world evidence initiatives:
- CORRONA: Large US-based RA registry
- ARCTIC REWIND: Real-world tapering strategies
- RABBIT: German biologics registry
- RISE Registry: ACR’s rheumatology informatics system
- iSPY-RA: Adaptive platform trial for treatment decisions
Emerging therapeutic approaches:
Immune tolerance induction:
- Antigen-specific immunotherapy using citrullinated peptides
- Tolerogenic dendritic cell therapy
- Regulatory T-cell expansion protocols
- Nanoparticle-based tolerance induction
- Potential for “functional cure” in early disease
Local/intra-articular therapies:
- Microsphere drug delivery systems for sustained release
- Gene therapy approaches for local expression of anti-inflammatory proteins
- Hydrogel-based drug delivery platforms
- Targeted nanoparticles for synovium-specific delivery
- Less systemic exposure, potentially better safety
Microbiome-based interventions:
- Fecal microbiota transplantation trials
- Microbiome-modulating probiotics
- Prevotella copri-targeted approaches
- Metabolite supplementation from beneficial bacteria
- Personalized dietary interventions based on microbiome
Cell-based therapies:
- CAR-T cell therapy targeting autoimmune B cells
- Mesenchymal stem cell treatments
- Induced pluripotent stem cell (iPSC) applications
- Exosome-based cell-free approaches
- Combination cellular therapies
Future directions in prevention and management:
Pre-symptomatic identification and intervention:
- Risk stratification algorithms for first-degree relatives
- Preventive therapy in high-risk individuals
- Mucosal site immune modulation (lung, gums)
- Lifestyle interventions for high-risk groups
- “RA prevention clinics” concept
Digital health transformation:
- Remote monitoring integrated with treat-to-target
- AI-assisted treatment decision support
- Virtual reality rehabilitation programs
- Patient-led data collection and management
- Decentralized clinical trials using digital platforms
Healthcare delivery innovations:
- Value-based care models for RA
- Integrated multidisciplinary care pathways
- Telemedicine for rural and underserved areas
- Non-physician provider models to extend specialist care
- Global access initiatives for essential medicines
Potential cures or innovative therapies under development
Transformative therapeutic concepts:
Curative approaches in development:
- Antigen-specific tolerance induction:
- Autologoen (Dendright): Tolerogenic dendritic cells loaded with citrullinated peptides
- Phase 1 completed, Phase 2 planned
- Aims to “reprogram” immune response to citrullinated proteins
- Potential for long-term remission without continuous therapy
- Targeted immune reset strategies:
- Intensive immunosuppression followed by stem cell support
- Moderately intensive lymphodepletion with anti-CD20 and cyclophosphamide
- “Reset and maintenance” protocols
- Most effective in early disease before established chronicity
- Regulatory T-cell therapy:
- Ex-vivo expanded autologous Tregs
- Phase 1/2 trials underway
- CAR-Tregs engineered for joint-specific targeting
- Potential for long-term immune regulation
- Antigen-specific tolerance induction:
Gene therapy approaches:
- Local anti-inflammatory gene delivery:
- ART-I02: intra-articular gene therapy expressing interferon-β
- Phase 1 safety established
- Long-term expression in synovial tissue
- Potential for single or occasional dosing
- Systemic RNA interference:
- siRNA targeting key inflammatory mediators
- Nanoparticle delivery systems
- Selective tissue targeting
- Reversible gene suppression approach
- CRISPR-based therapies:
- Ex-vivo modification of immune cells
- Correction of risk-associated genetic variants
- Early preclinical development
- Highly personalized approach
- Local anti-inflammatory gene delivery:
Restorative therapies:
- Joint tissue regeneration:
- 3D-bioprinted cartilage replacement
- Scaffold-based cartilage regeneration
- Growth factor-eluting implants
- Matrix-induced chondrogenesis
- Combination regenerative-immunomodulatory:
- MSCs with anti-inflammatory gene modifications
- Bioscaffolds with drug-eluting properties
- Sequential inflammation control then regeneration
- Articular cartilage restoration plus synovial modulation
- Neural pathway modulation:
- Vagus nerve stimulation for anti-inflammatory effects
- Implantable microdevices for neuroimmune modulation
- External ultrasound-based neuromodulation
- Targeting the cholinergic anti-inflammatory pathway
- Joint tissue regeneration:
Revolutionary platform technologies:
mRNA therapeutics:
- Transient expression of anti-inflammatory proteins
- Tolerance-inducing mRNA approaches
- Potential for self-amplifying mRNA technology
- Lipid nanoparticle delivery to immune cells
- Personalized mRNA cocktails based on patient characteristics
Biomaterial platforms:
- Controlled-release drug reservoirs
- Stimulus-responsive drug delivery
- Joint-resident drug depots lasting 6-12 months
- Combination drug delivery systems
- “Smart” materials that respond to inflammation
Synthetic biology approaches:
- Engineered cells as “living therapeutics”
- Cells programmed to sense inflammation and respond
- Synthetic gene circuits with feedback control
- Bacterial chassis engineered to deliver therapeutics
- Self-regulating systems that maintain homeostasis
Breakthrough technologies on the horizon:
Multi-specific antibody formats:
- Bispecific antibodies targeting multiple cytokines
- Trispecific molecules with synergistic mechanisms
- Cytokine-neutralizing plus cell-targeting combinations
- “Switchable” antibodies with controllable activity
- Tissue-targeted antibody platforms
Advanced immune modulation:
- Selective proteasome inhibition
- Protein-protein interaction disruptors
- Targeted protein degradation (PROTACs)
- Inflammasome inhibitors
- Metabolic reprogramming of immune cells
Individualized medicine approaches:
- Functional genomic screening to identify personal drug targets
- Patient-derived organoids for drug testing
- AI-designed treatment combinations
- Longitudinal multi-omic profiling and adaptation
- Digital twin models for virtual treatment testing
12. Interesting Facts & Lesser-Known Insights
Uncommon knowledge about rheumatoid arthritis
Historical perspectives:
Ancient presence:
- Evidence of RA in Native American skeletal remains from 4500 BCE
- Not clearly described in ancient European or Asian medical texts
- Possible “new world” origin theory
- Term “rheumatoid arthritis” only coined in 1859 by Alfred Garrod
- Distinguished from gout only in the 18th century
Notable figures with RA:
- Pierre-Auguste Renoir continued painting despite severe hand deformities
- Peter Paul Rubens’ later works show evidence of his developing RA
- Auguste Rodin likely had RA, influencing his sculptural style
- Lucille Ball suffered from RA beginning in her teens
- Kathleen Turner’s acting career was significantly impacted by RA
Treatment evolution:
- Gold therapy was the first “disease-modifying” treatment (1920s)
- Discovered accidentally while treating tuberculosis
- Methotrexate was initially used as a chemotherapy agent
- Used at 1/100th the cancer dose for RA
- First biologic (infliximab) developed in the 1990s revolutionized treatment
Scientific curiosities:
Geographic and temporal patterns:
- RA is rare in rural Africa but increases with urbanization
- Prevalence in Japan has tripled since World War II
- Native American tribes have 5-7 times higher rates than European populations
- Incidence appears to be declining in some developed nations
- Prevalence increases with distance from the equator
Biological peculiarities:
- RA synovial fibroblasts develop cancer-like invasive properties
- Can migrate between joints, potentially “spreading” the disease
- Synovial fluid in active RA glows under UV light (fluorescence)
- Joint inflammation follows a circadian rhythm (worse in morning)
- Left-handed people may have higher RA risk
Pregnancy effects:
- 75-80% of women experience remission during pregnancy
- Symptoms often flare within 3 months after delivery
- Protective effect strongest in third trimester
- Fetal-maternal HLA incompatibility may contribute to improvement
- Breastfeeding associated with longer post-pregnancy remission
Clinical insights:
Unusual manifestations:
- Cricoarytenoid joint involvement can cause vocal changes or breathing difficulties
- Temporomandibular joint arthritis affects 30-50% but often overlooked
- Cervical spine involvement can lead to dangerous C1-C2 subluxation
- “Palindromic rheumatism” – dramatic, recurring flares that completely resolve
- “Rheumatoid nodulosis” – nodules with minimal arthritis
Paradoxical relationships:
- Smoking increases RA risk but may improve ulcerative colitis
- RA protective against multiple sclerosis and vice versa
- RA associated with reduced risk of Parkinson’s disease
- Inverse relationship between RA and osteoarthritis in same joints
- RA protective against some allergic conditions
Therapeutic surprises:
- Antibiotics (minocycline) have disease-modifying effects
- Antimalarials (hydroxychloroquine) effective despite no malaria link
- Electrical vagus nerve stimulation reduces inflammation
- Fish oil at high doses (4g/day) has measurable benefits
- Helminth therapy (controlled worm infection) explored as treatment
Myths and misconceptions vs. medical facts
Myth 1: RA is just a type of arthritis affecting older people. Fact: RA is an autoimmune disease distinct from wear-and-tear osteoarthritis. It can affect people of any age, including children and young adults. While peak onset is between 30-60 years, approximately 2% of cases are juvenile-onset. RA affects the synovial lining through immune-mediated inflammation rather than mechanical degeneration.
Myth 2: RA only affects the joints. Fact: While joint inflammation is the hallmark of RA, it’s a systemic disease that can affect multiple organs. Up to 40% of patients develop extra-articular manifestations including lung disease, eye inflammation, cardiovascular complications, and rheumatoid nodules. Systemic inflammation can lead to fatigue, anemia, and increased risk of other conditions.
Myth 3: Weather and diet are the main causes of RA. Fact: RA results from a complex interaction between genetic susceptibility and environmental triggers. While weather changes may temporarily affect symptoms, they don’t cause the disease. Diet can influence inflammation levels but isn’t a primary cause. The strongest environmental risk factor is smoking, which increases risk 2-4 fold, particularly in genetically susceptible individuals.
Myth 4: RA always leads to disability and wheelchair use. Fact: With modern treatment strategies, particularly early intervention with DMARDs and biologics, the outlook for RA patients has dramatically improved. Only about 10% of patients treated according to current standards develop significant disability. Remission or low disease activity is now an achievable goal for 60-70% of patients.
Myth 5: Exercise worsens RA joint damage. Fact: Appropriate exercise is beneficial for RA management. Studies show that moderate exercise programs improve function, reduce pain, and do not accelerate joint damage. Range-of-motion, strengthening, and low-impact aerobic exercises are recommended components of RA management. Physical activity actually helps maintain joint function and reduces inflammation when properly prescribed.
Myth 6: All RA medications are dangerous and toxic. Fact: While RA medications can have side effects, the risk-benefit ratio strongly favors treatment for most patients. Untreated RA typically causes more harm than medication side effects. Modern DMARDs and biologics have improved safety profiles compared to older drugs. Regular monitoring minimizes risks, and many patients take these medications for decades without significant complications.
Myth 7: Alternative therapies like copper bracelets can cure RA. Fact: No alternative therapy has been scientifically proven to cure RA. While some complementary approaches like acupuncture, massage, or mindfulness may help manage symptoms, they should complement rather than replace conventional medicine. Many unproven treatments exploit vulnerable patients, resulting in delayed effective treatment and unnecessary expense.
Myth 8: Once damage occurs, nothing can be done to improve function. Fact: Even with existing joint damage, function can improve substantially. Modern medications can halt progression and reduce inflammation, decreasing pain and improving mobility. Rehabilitation, assistive devices, and joint protection techniques can maximize function. Surgical interventions including joint replacement can dramatically restore function in damaged joints.
Myth 9: RA is contagious or directly inherited. Fact: RA is neither contagious nor follows simple inheritance patterns. While first-degree relatives have 3-5 times increased risk, suggesting genetic factors, most people with RA have no family history. The genetic component involves multiple genes interacting with environmental triggers. Even identical twins have only 15-30% concordance, highlighting the importance of non-genetic factors.
Myth 10: Diet changes alone can cure RA. Fact: While anti-inflammatory diets may modestly improve symptoms in some patients, no dietary approach alone has been proven to induce remission or cure RA. Mediterranean, plant-based, and elimination diets show modest benefits in some studies, but effects are generally complementary to medication. Diet should be viewed as one component of comprehensive management rather than a standalone treatment.
Impact on specific populations or professions
Occupational impacts:
Healthcare workers:
- Higher ergonomic challenges in nursing and physical therapy
- Hand-intensive specialties (dentistry, surgery) particularly affected
- Increased risk of work disability (30-40% higher than general population)
- Adaptive equipment allows many to continue practice
- Workplace accommodations including lifting restrictions crucial
- Exposure to infections more problematic when immunosuppressed
Manual labor professions:
- Construction workers face difficult workplace adaptations
- Agricultural workers experience significant hand/wrist limitations
- Manufacturing positions requiring repetitive motions particularly challenging
- Vibration exposure (machinery operators) exacerbates symptoms
- Retraining programs often necessary for long-term employment
- Disability rates 40-60% higher than knowledge workers
Office and knowledge workers:
- Computer use limitations from hand involvement
- Prolonged sitting challenges with knee/hip involvement
- Ergonomic workstation modifications essential
- Voice recognition technology enables continued productivity
- Flexible work arrangements accommodate fatigue and appointments
- Lower overall work disability rates with proper accommodations
Artists and musicians:
- Fine motor limitations impact technique and endurance
- Hand deformities particularly devastating for precision work
- Adaptive instruments and tools may extend careers
- Notable examples of continued artistry despite severe disease (Renoir)
- Modified techniques developed to accommodate limitations
- Pain management crucial for performance demands
Demographic considerations:
Women of childbearing age:
- Family planning complicated by medication considerations
- Pregnancy often temporarily improves symptoms (75-80%)
- Postpartum flares common (90% within 6 months)
- Breastfeeding decisions complicated by medication safety
- Childcare physical demands challenging with active disease
- Support systems particularly important during this life stage
Pediatric population (Juvenile Idiopathic Arthritis):
- Growth and development impacts from inflammation
- Educational accommodations often necessary
- Different drug safety profiles and considerations
- Longer lifetime disease duration
- Transition to adult care challenging (18-25 years)
- Social development and peer relationships affected
- Superior treatment outcomes compared to adult-onset RA
Elderly patients:
- Polypharmacy concerns with multiple medications
- Comorbidities complicating treatment decisions
- Increased infection risks with immunosuppression
- Falls risk elevated with joint involvement
- Differentiating RA from other conditions more difficult
- Different treatment goals focusing on function over remission
- Often undertreated due to safety concerns
Rural populations:
- Limited access to rheumatology specialists
- Transportation barriers to care with mobility limitations
- Telehealth improving access but hands-on assessment limited
- Agricultural occupations potentially more difficult to modify
- Environmental exposures (silica, pesticides) may increase risk
- Lower adoption rates of advanced therapies
- Greater reliance on primary care management
Socioeconomic factors:
Economic disparities:
- Treatment access dramatically different by income level
- Biologic therapy inaccessible to many globally
- Indirect costs (lost work, caregiver expenses) often exceed direct costs
- Disability benefits systems vary widely by country
- Educational level influences disease outcomes independent of income
- Lower socioeconomic status associated with more severe disease
- Financial toxicity from treatment costs affects adherence
Healthcare system variations:
- Universal healthcare systems provide more equitable access
- Specialty medication approval processes vary by country
- Wait times for rheumatology consultation range from weeks to years
- Treatment guidelines implementation varies widely
- Multidisciplinary team availability limited in many regions
- Patient cost-sharing significantly impacts treatment decisions
- Biosimilar adoption changing treatment economics globally
Educational and social factors:
- Health literacy strongly influences treatment adherence
- Social support networks critical for psychological adjustment
- Stigma around invisible illness affects workplace accommodations
- Self-advocacy skills influence treatment quality
- Community resources vary dramatically by region
- Patient organization involvement improves outcomes
- Cultural attitudes toward disability affect coping strategies
This comprehensive report has provided an evidence-based overview of rheumatoid arthritis, covering epidemiology, pathophysiology, clinical features, diagnostic approaches, treatment strategies, and future directions. The information presented reflects current scientific understanding as of 2025, drawing from medical literature, clinical guidelines, and epidemiological data. For personalized medical advice, patients should consult qualified healthcare providers specializing in rheumatology.