
⚠️ Disclaimer: The information provided in this article is for educational purposes only and does not constitute medical advice. RevisionTown does not provide diagnosis, treatment, or medical recommendations. Always consult a qualified healthcare professional regarding any medical condition, symptoms, or concerns.
Read More – 🏥 Medical Disclaimer
What is Porphyria?
Porphyria refers to a group of rare, inherited metabolic disorders caused by defects in the heme biosynthesis pathway. These conditions result from deficiencies in specific enzymes responsible for the production of heme, a vital component of hemoglobin, cytochromes, and other essential proteins. The accumulation of heme precursors (porphyrins and porphyrin precursors) leads to the characteristic clinical manifestations of these disorders.
Concise Yet Detailed Definition
Porphyrias are a heterogeneous group of eight distinct disorders, each caused by a deficiency in one of the eight enzymes in the heme biosynthetic pathway. They are classified into two main categories:
Acute Hepatic Porphyrias (affecting the liver):
- Acute intermittent porphyria (AIP)
- Variegate porphyria (VP)
- Hereditary coproporphyria (HCP)
- ALA dehydratase deficiency porphyria (ALAD)
Cutaneous Porphyrias (affecting the skin):
- Porphyria cutanea tarda (PCT)
- Erythropoietic protoporphyria (EPP)
- Congenital erythropoietic porphyria (CEP)
- Hepatoerythropoietic porphyria (HEP)
Affected Body Parts/Organs
Primary Organs Affected:
- Liver: Central to heme synthesis; affected in hepatic porphyrias
- Skin: Photosensitivity and lesions in cutaneous types
- Nervous System: Peripheral and central nervous system involvement in acute porphyrias
- Gastrointestinal System: Severe abdominal pain during acute attacks
- Cardiovascular System: Hypertension and tachycardia during acute episodes
Secondary Effects:
- Kidneys: Potential for chronic kidney disease
- Endocrine System: Reproductive hormone imbalances
- Respiratory System: Respiratory paralysis in severe acute attacks
- Hematologic System: Sometimes mild anemia
Prevalence and Significance
Global Prevalence:
- Overall prevalence: 1 in 20,000 to 1 in 200,000 people worldwide
- Geographic variations: Higher prevalence in certain populations due to founder effects
Type-Specific Prevalence:
- Acute Intermittent Porphyria: 1 in 20,000 (Northern European descent)
- Porphyria Cutanea Tarda: Most common type, 1 in 25,000
- Erythropoietic Protoporphyria: 1 in 140,000
- Congenital Erythropoietic Porphyria: <200 cases reported worldwide
Clinical Significance:
- Often underdiagnosed due to non-specific symptoms
- Can be life-threatening during acute attacks
- Significant impact on quality of life
- Important differential diagnosis for acute abdominal pain and neuropsychiatric symptoms
2. History & Discoveries
Initial Recognition and Discovery
Ancient Recognition:
- Purple-red urine described in ancient medical texts
- Hippocrates (460-370 BCE) described symptoms consistent with acute porphyria
Modern Era Discovery:
- 1871: Felix Hoppe-Seyler first described porphyrins in laboratory settings
- 1874: J.L.W. Thudicham identified porphyrins in urine of psychiatric patients
- 1889: B.J. Stokvis described acute intermittent porphyria in a patient with dark red urine
Who Discovered It?
Key Figures:
- Felix Hoppe-Seyler (1871): First isolated and named porphyrins
- Hans Günther (1911): Described congenital erythropoietic porphyria
- Jan Waldenström (1937): Characterized acute intermittent porphyria
- Claude Rimington (1930s-1950s): Pioneered porphyrin biochemistry
- Shigeru Sano (1960s): Elucidated the heme biosynthetic pathway
Major Discoveries and Breakthroughs
1880s-1920s: Classification of different porphyria types
- Günther distinguished “acute” from “cutaneous” forms
- Recognition of hereditary nature
1930s-1940s: Biochemical understanding
- Waldenström’s detailed clinical descriptions
- Rimington’s work on porphyrin metabolism
1950s-1960s: Enzyme pathway characterization
- Complete mapping of heme biosynthetic pathway
- Identification of specific enzyme deficiencies
1970s-1980s: Genetic basis elucidation
- Molecular genetics applications
- First cloning of heme pathway genes
1990s-2000s: Modern diagnostics and treatment
- DNA-based genetic testing
- Development of specific therapies like hemin
2010s-Present: Precision medicine approaches
- Gene therapy research
- Novel small molecule therapies
- Improved understanding of disease mechanisms
Evolution of Medical Understanding
Early Period (1871-1930):
- Focus on clinical description and urine abnormalities
- Recognition of familial clustering
Biochemical Era (1930-1970):
- Understanding of heme synthesis pathway
- Correlation of enzyme defects with clinical phenotypes
Molecular Era (1970-2000):
- Genetic characterization of all porphyria types
- Development of molecular diagnostics
Therapeutic Era (2000-Present):
- Evidence-based treatment protocols
- Development of disease-specific therapies
- Focus on prevention and management of acute attacks
3. Symptoms
Early vs. Advanced-Stage Symptoms
Acute Porphyrias – Early Symptoms:
- Gastrointestinal: Severe abdominal pain (often first symptom)
- Neurological: Anxiety, restlessness, insomnia
- General: Fatigue, muscle weakness
- Urinary: Dark red/brown urine during attacks
Acute Porphyrias – Advanced Symptoms:
- Neurological: Seizures, paralysis, respiratory failure
- Psychiatric: Hallucinations, psychosis, severe depression
- Cardiovascular: Severe hypertension, arrhythmias
- Respiratory: Respiratory muscle paralysis
Cutaneous Porphyrias – Early Symptoms:
- Skin: Photosensitivity, mild skin fragility
- Sun exposure: Immediate burning or stinging sensation
- Skin changes: Hyperpigmentation in sun-exposed areas
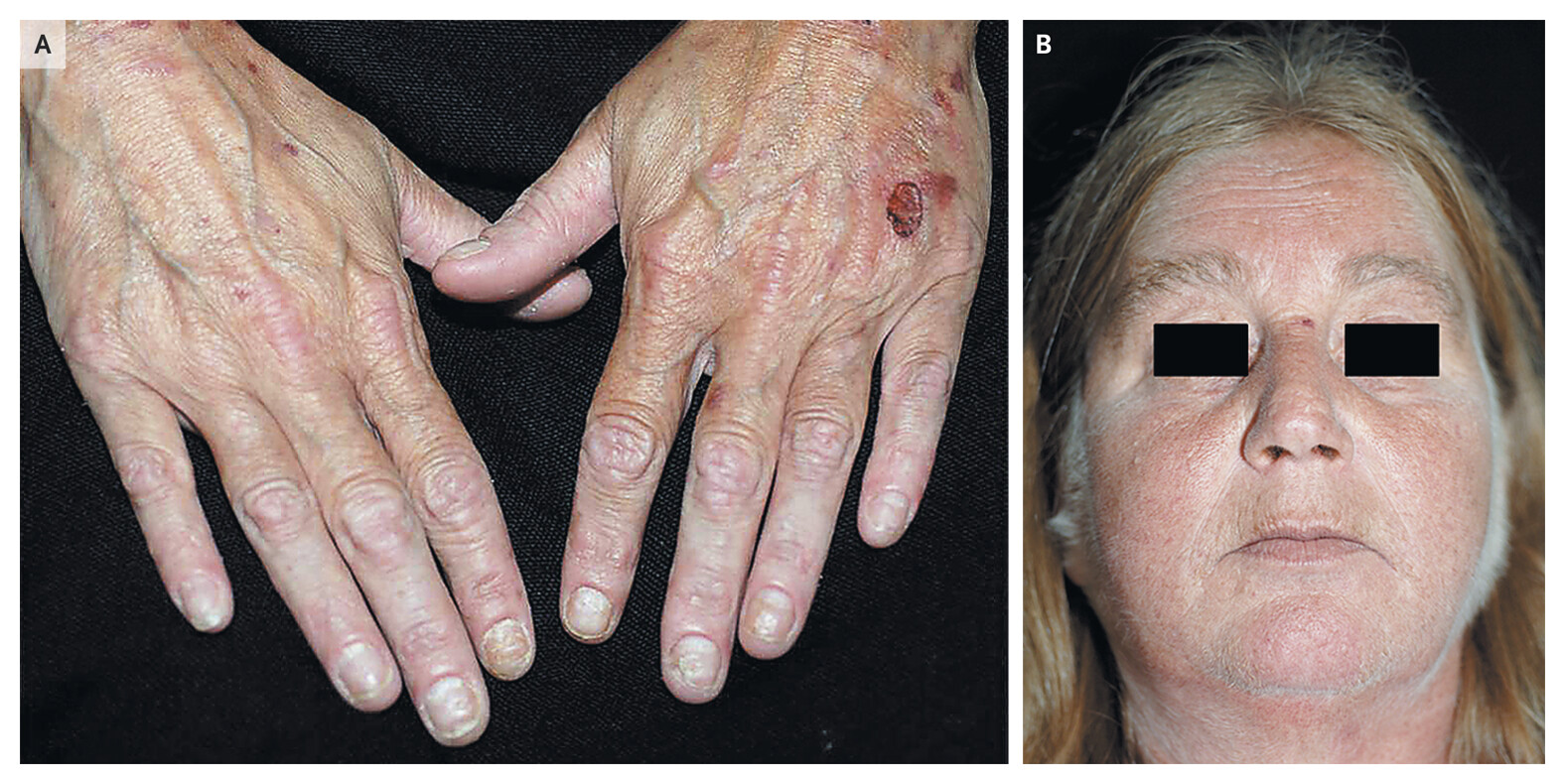
Cutaneous Porphyrias – Advanced Symptoms:
- Severe skin lesions: Bullae, scarring, milia
- Chronic changes: Hirsutism, scleroderma-like changes
- Hair growth: Excessive facial hair (especially in women)
Common vs. Rare Symptoms
Common Symptoms by Type:
Acute Intermittent Porphyria:
- Severe abdominal pain (85-95%)
- Vomiting and constipation (80-90%)
- Limb pain (50-70%)
- Muscle weakness (60-70%)
Porphyria Cutanea Tarda:
- Photosensitivity (100%)
- Skin fragility (90-95%)
- Hyperpigmentation (80-90%)
- Hirsutism (60-70%)
Erythropoietic Protoporphyria:
- Acute photosensitivity (100%)
- Burning pain on sun exposure (95-100%)
- Swelling of exposed skin (70-80%)
Rare Symptoms:
- Acute porphyrias: Seizures (5-20%), quadriplegia (<5%)
- Cutaneous porphyrias: Liver dysfunction (10-15% in PCT)
- All types: Chronic kidney disease (variable)
Symptom Progression Over Time
Acute Porphyrias:
- Pre-attack phase: Mood changes, premonitory symptoms
- Acute phase: Severe pain, neurological symptoms (hours to days)
- Recovery phase: Gradual resolution (days to weeks)
- Chronic effects: Possible chronic neuropathy, hypertension
Cutaneous Porphyrias:
- Initial presentation: Photosensitivity reactions
- Progressive changes: Chronic skin damage, scarring
- Advanced disease: Severe cosmetic and functional impairment
Age-Related Patterns:
- Acute porphyrias: Typically manifest after puberty, peak in reproductive years
- Cutaneous porphyrias: Can appear at any age, often worsen with sun exposure over time
4. Causes
Biological Causes
Primary Cause: Inherited deficiencies in enzymes of the heme biosynthetic pathway
The Heme Biosynthetic Pathway:
- ALA synthase: Glycine + Succinyl-CoA → ALA
- ALA dehydratase: ALA → Porphobilinogen
- PBG deaminase: Porphobilinogen → Hydroxymethylbilane
- Uroporphyrinogen III synthase: Hydroxymethylbilane → Uroporphyrinogen III
- Uroporphyrinogen decarboxylase: Uroporphyrinogen III → Coproporphyrinogen III
- Coproporphyrinogen oxidase: Coproporphyrinogen III → Protoporphyrinogen IX
- Protoporphyrinogen oxidase: Protoporphyrinogen IX → Protoporphyrin IX
- Ferrochelatase: Protoporphyrin IX + Fe²⁺ → Heme
Genetic and Hereditary Factors
Inheritance Patterns:
- Autosomal Dominant: AIP, VP, HCP, PCT (familial form)
- Autosomal Recessive: ALAD, CEP, HEP
- X-linked: None
- Variable pattern: EPP (mostly autosomal recessive)
Genetic Characteristics:
- Penetrance: Often incomplete (10-20% of carriers develop symptoms)
- Expressivity: Variable clinical severity even within families
- Founder effects: Higher prevalence in certain populations
Specific Gene Locations:
- AIP: HMBS gene (chromosome 11q23.3)
- PCT: UROD gene (chromosome 1p34)
- EPP: FECH gene (chromosome 18q21.3)
- CEP: UROS gene (chromosome 10q25.2-q26.3)
Environmental Triggers and Causes
Medication Triggers (primarily for acute porphyrias):
- Barbiturates: Highly porphyrinogenic
- Sulfonamides: Antibiotics
- Anticonvulsants: Carbamazepine, phenytoin
- Hormones: Estrogen, progesterone
- Anesthetics: Certain volatile agents
Lifestyle Triggers:
- Alcohol: Major trigger for acute attacks and PCT
- Fasting/Low-calorie diets: Reduce heme synthesis
- Stress: Physical or emotional stress
- Infections: Viral or bacterial infections
- Surgery: General anesthesia and stress
Environmental Factors:
- Iron overload: Contributes to PCT development
- Hepatitis C: Associated with sporadic PCT
- Lead exposure: Can mimic or worsen porphyria
- Chemical exposure: Industrial chemicals, pesticides
Hormonal Influences:
- Menstrual cycle: Attacks often cyclic in women
- Pregnancy: Can trigger or worsen attacks
- Oral contraceptives: May precipitate attacks
5. Risk Factors
Demographic Risk Factors
Age-Specific Risks:
- Children: Rare manifestation except for EPP and CEP
- Adults 20-40 years: Peak incidence for acute porphyrias
- Post-menopausal women: Increased risk for PCT
- Elderly: Generally lower risk, but more severe complications
Gender Differences:
- Acute porphyrias: 70-80% of attacks occur in women
- PCT: More common in men (3:1 ratio)
- EPP: Equal gender distribution
- Hormonal influences: Stronger in women due to estrogen/progesterone
Genetic Risk Factors
Family History:
- First-degree relatives: 50% risk of carrying gene (autosomal dominant types)
- Genetic testing: Recommended for family members
- Phenotypic expression: Only 10-20% of carriers develop symptoms
Population-Specific Risks:
- Northern Europeans: Higher AIP prevalence
- South African whites: VP founder effect (1 in 300 carry mutation)
- Finns: Higher AIP prevalence due to founder effect
- Consanguinity: Increases risk of recessive forms
Medical Risk Factors
Liver Conditions:
- Hepatitis C: Strong association with PCT
- Alcohol liver disease: Predisposes to PCT
- Iron overload: Hemochromatosis increases PCT risk
- Liver tumors: Rarely associated with porphyrias
Hormonal Factors:
- Oral contraceptive use: Increases acute attack risk
- Hormone replacement therapy: May trigger attacks
- Pregnancy: Variable effects, often reduces attack frequency
- Thyroid disorders: May influence porphyria severity
Other Medical Conditions:
- HIV infection: Associated with PCT
- End-stage renal disease: Can worsen photosensitivity in EPP
- Hemodialysis: May cause porphyrin accumulation
Environmental and Occupational Factors
Chemical Exposures:
- Industrial workers: Exposure to halogenated hydrocarbons
- Agricultural workers: Pesticide exposure
- Healthcare workers: Anesthetic agents
- Laboratory workers: Chemical solvents
Lifestyle Factors:
- Alcohol consumption: Major risk factor for PCT and acute attacks
- Smoking: May worsen cutaneous symptoms
- Diet: High-iron diet increases PCT risk
- Sun exposure: Critical factor in cutaneous porphyrias
Impact of Pre-existing Conditions
Hepatic Conditions:
- Significantly increase PCT risk
- May worsen acute porphyria attacks
- Require careful medication selection
Renal Disease:
- Affects porphyrin elimination
- May worsen photosensitivity in EPP
- Requires dosage adjustments for treatments
Psychiatric Conditions:
- May be triggered or worsened by porphyria attacks
- Complicate treatment selection (many psychiatric drugs contraindicated)
- Important to distinguish from porphyria-induced psychiatric symptoms
6. Complications
Acute Complications
Neurological Complications:
- Motor neuropathy: Progressive weakness, potentially leading to quadriplegia
- Respiratory paralysis: Life-threatening complication requiring ventilation
- Seizures: Occur in 10-20% of acute attacks
- Posterior reversible encephalopathy syndrome (PRES): Rare but serious
Cardiovascular Complications:
- Hypertensive crisis: Blood pressure >200/120 mmHg
- Cardiac arrhythmias: Due to electrolyte imbalances
- Sudden cardiac death: Rare but documented
Gastrointestinal Complications:
- Intestinal obstruction: From severe constipation
- Hepatic complications: Rare hepatic failure during attacks
Chronic Complications
Neurological Sequelae:
- Chronic peripheral neuropathy: Persists in 20-30% after attacks
- Chronic pain syndromes: Especially neuropathic pain
- Motor deficits: Permanent weakness in severe cases
Renal Complications:
- Chronic kidney disease: Occurs in 30-60% of acute porphyria patients
- Hypertensive nephropathy: From chronic hypertension
- Tubulointerstitial nephritis: Direct toxicity from porphyrin precursors
Hepatic Complications:
- Hepatocellular carcinoma: Increased risk in PCT and acute porphyrias
- Cirrhosis: In PCT with chronic liver disease
- Iron overload: Especially in PCT
Skin and Cosmetic Complications
Cutaneous Porphyrias:
- Permanent scarring: From photosensitivity reactions
- Milia formation: Small cysts on hands and face
- Hypertrichosis: Excessive hair growth, particularly facial
- Scleroderma-like changes: Skin thickening and tightening
Photosensitivity Complications:
- Chronic photodamage: Premature aging of exposed skin
- Secondary infections: From broken blisters and erosions
- Social and psychological impact: Disfigurement affecting quality of life
Long-term Impact on Organs
Liver:
- Fibrosis and cirrhosis: Especially in PCT
- Increased cancer risk: 60-fold increased risk of hepatocellular carcinoma
- Iron accumulation: Leading to further liver damage
Nervous System:
- Chronic polyneuropathy: May not fully resolve
- Cognitive impairment: Subtle deficits in some patients
- Psychiatric disorders: Depression, anxiety disorders
Kidneys:
- Progressive CKD: May require dialysis or transplantation
- Hypertension: Chronic and difficult to control
- Electrolyte disorders: Chronic hyponatremia in some patients
Disability and Fatality Rates
Mortality Rates:
- Acute porphyria attacks: 1-5% mortality during severe attacks
- Respiratory paralysis: 10-20% mortality if ventilation delayed
- Overall mortality: Increased standardized mortality ratio (2-3x normal)
- Hepatocellular carcinoma: Major cause of death in PCT
Disability Rates:
- Acute porphyrias: 20-40% have some degree of permanent disability
- Cutaneous porphyrias: Variable, depending on sun protection adherence
- Quality of life: Significantly impacted in 50-70% of patients
Prognostic Factors:
- Early diagnosis: Improves outcomes significantly
- Attack frequency: More frequent attacks associated with worse prognosis
- Adherence to trigger avoidance: Critical for preventing complications
7. Diagnosis & Testing
Clinical Diagnosis
Clinical Presentation:
- History: Family history, drug exposure, trigger identification
- Physical examination: Neurological assessment, skin examination
- Symptom patterns: Acute vs. chronic, photosensitivity vs. neurovisceral
Diagnostic Criteria:
- Acute porphyrias: Clinical symptoms + biochemical confirmation
- Cutaneous porphyrias: Photosensitivity + characteristic lesions + biochemical testing
- Genetic confirmation: Recommended but not always required for diagnosis
Biochemical Testing
First-Line Tests:
For Acute Symptoms:
- Urinary porphobilinogen (PBG): Markedly elevated during attacks
- Urinary aminolevulinic acid (ALA): Elevated in most acute porphyrias
- Spot urine test: Convenient for emergency settings
For Cutaneous Symptoms:
- Plasma/serum porphyrins: Elevated protoporphyrin in EPP
- Urinary porphyrins: Specific patterns for different types
- Fecal porphyrins: Useful for differentiating VP from AIP
Specialized Biochemical Tests:
- Enzyme activity assays: Direct measurement in red blood cells
- Fractionated porphyrin analysis: Determines specific porphyrin elevation patterns
- 24-hour urine collections: More accurate than spot urine
Genetic Testing
Molecular Genetic Analysis:
- DNA sequencing: Identifies specific mutations
- Family screening: Tests relatives of confirmed cases
- Prenatal testing: Available for severe forms
Genetic Test Interpretation:
- Pathogenic variants: Clearly disease-causing mutations
- Variants of uncertain significance: Require functional studies
- Penetrance considerations: Not all carriers develop symptoms
Imaging and Other Tests
Imaging Studies:
- MRI brain: For neurological complications (PRES, cerebral edema)
- CT/MRI abdomen: To exclude other causes of abdominal pain
- Ultrasound liver: Assessing for hepatomegaly, tumors
Additional Tests:
- Liver function tests: Often abnormal in PCT
- Iron studies: Elevated ferritin in PCT
- Hepatitis serology: Screen for hepatitis C in PCT
- Electrophysiology: Nerve conduction studies for neuropathy
Early Detection Methods
Screening Strategies:
- Family screening: Test relatives of known cases
- High-risk populations: Those with unexplained symptoms
- Pre-symptomatic carriers: Monitor with periodic testing
Point-of-Care Testing:
- Watson-Schwartz test: Historical bedside test for PBG
- Modern rapid tests: Under development for emergency use
Testing Effectiveness
Sensitivity and Specificity:
- Urinary PBG: 95-100% sensitive during acute attacks
- Plasma porphyrins: 95-100% sensitive for EPP
- Genetic testing: 95-99% detection rate for known mutations
Limitations:
- Between attacks: Normal results in acute porphyrias
- Medication interference: Some drugs affect test results
- Technical factors: Proper sample handling crucial
Optimal Testing Strategy:
- Clinical suspicion: Based on symptoms and family history
- Appropriate test selection: Based on presenting symptoms
- Confirmatory testing: Genetic testing for definitive diagnosis
8. Treatment Options
Standard Treatment Protocols
Acute Porphyria Attacks:
- Immediate management: Pain control, IV fluids, electrolyte correction
- Specific therapy: Hemin (heme arginate) 3-4 mg/kg/day for 4 days
- Trigger removal: Discontinue precipitating medications
- Supportive care: Monitoring for complications
Cutaneous Porphyrias:
- Sun protection: Primary intervention for all cutaneous types
- Symptom management: Topical treatments for skin lesions
- Underlying condition treatment: Address hepatitis C, iron overload
Medications
Specific Therapies:
Hemin/Heme Arginate:
- Mechanism: Replaces deficient heme, reduces ALA synthase
- Indications: Acute attacks, prevention in recurrent disease
- Administration: IV infusion over 30 minutes
- Efficacy: 80-90% response rate in acute attacks
Givosiran (Givlaari):
- Mechanism: siRNA targeting ALA synthase 1
- Indications: Prevention of acute attacks in AIP
- Administration: Monthly subcutaneous injection
- Efficacy: 74% reduction in annual attack rate
Symptom Management:
Pain Control:
- Opioids: Often required for severe pain
- Gabapentin: For neuropathic pain
- Avoid: Barbiturates, other contraindicated drugs
Antiemetics:
- Promethazine: Safe option for nausea
- Ondansetron: Generally safe and effective
Antihypertensives:
- Beta-blockers: Safe and effective
- ACE inhibitors: Usually well-tolerated
- Avoid: Methyldopa (porphyrinogenic)
Cutaneous Porphyria Treatments
PCT-Specific Treatments:
- Phlebotomy: 450-500 mL every 2 weeks until ferritin <20 μg/L
- Chloroquine: Low-dose 125 mg twice weekly
- Interferon: For hepatitis C-associated PCT
EPP-Specific Treatments:
- Afamelanotide: Approved in Europe for EPP
- Beta-carotene: Modest photoprotective effects
- Liver transplantation: For end-stage liver disease
Surgical Interventions
Liver Transplantation:
- Indications: End-stage liver disease (EPP, PCT)
- Outcomes: Excellent with proper management
- Considerations: May cure hepatic disease but not fully correct enzyme deficiency
Other Procedures:
- Plasmapheresis: Anecdotal use in severe acute attacks
- Hemodialysis: Limited role, mainly for metabolic complications
Supportive Therapies
Nutritional Support:
- Glucose administration: During acute attacks
- Adequate caloric intake: Prevent fasting states
- Iron management: Careful in PCT patients
Physical Therapy:
- During recovery: From motor neuropathy
- Respiratory therapy: For respiratory muscle weakness
Emerging Treatments and Clinical Trials
Gene Therapy:
- AAV vectors: Delivering normal enzyme genes
- Proof-of-concept studies: Showing promise in animal models
- Clinical trials: Phase I/II studies ongoing
Small Molecule Therapies:
- ALA synthase inhibitors: Beyond givosiran
- Mitocidrial targeting: Novel approaches under development
- Substrate reduction therapy: Alternative to enzyme replacement
Cell-Based Therapies:
- Hepatocyte transplantation: Experimental approach
- Stem cell therapy: Early research stages
- Gene editing: CRISPR applications being explored
Novel Drug Delivery:
- Subcutaneous hemin: Improved convenience
- Oral heme preparations: Under investigation
- Targeted delivery systems: Liver-specific targeting
Personalized Medicine Approaches
Pharmacogenomics:
- Drug metabolism: Tailored to individual genetics
- Safety profiles: Based on porphyria type and severity
- Efficacy prediction: Biomarkers for treatment response
Precision Dosing:
- Hemin dosing: Based on porphyrin levels
- Givosiran response: Monitored with biomarkers
- Individualized protocols: Based on attack patterns
9. Prevention & Precautionary Measures
Primary Prevention
Genetic Counseling:
- Family planning: Risk assessment for couples
- Prenatal testing: Available for severe forms
- Carrier identification: Testing family members
- Education: About inheritance patterns and risks
Lifestyle Modifications:
- Diet: Adequate carbohydrate intake, avoid fasting
- Alcohol: Complete avoidance in acute porphyrias
- Sleep: Regular sleep patterns, stress management
- Exercise: Regular moderate exercise
Secondary Prevention (Attack Prevention)
Trigger Avoidance:
Medications to Avoid:
- Barbiturates: Highly porphyrinogenic
- Sulfonamides: Most antibiotics in this class
- Hormones: Estrogen, progestins
- Anticonvulsants: Many are contraindicated
Safe Medications:
- Analgesics: Morphine, acetaminophen
- Antibiotics: Penicillins, fluoroquinolones
- Antihypertensives: Beta-blockers, ACE inhibitors
Lifestyle Factors:
- Stress management: Techniques to reduce psychological stress
- Infection prevention: Prompt treatment of infections
- Nutrition: Avoid prolonged fasting, maintain adequate calories
- Hormonal considerations: Careful contraception choices
Cutaneous Porphyria Prevention
Sun Protection:
- Physical barriers: Wide-brimmed hats, protective clothing
- Sunscreens: Broad-spectrum, high SPF
- Behavioral modifications: Avoid peak sun hours
- Window films: UVA-blocking for home and vehicles
Environmental Modifications:
- Work environment: Reduce fluorescent light exposure
- Home modifications: Install appropriate lighting
- Travel considerations: Plan for different climates
Preventive Medications
Hemin Prophylaxis:
- Indications: Recurrent acute attacks (>4 per year)
- Protocol: Weekly or biweekly infusions
- Efficacy: 70-80% reduction in attack frequency
Givosiran:
- Primary indication: Prevention in AIP patients
- Administration: Monthly subcutaneous injections
- Monitoring: Regular liver function tests
Emergency Preparedness
Medical Alert Identification:
- Medical bracelets: Identifying porphyria type
- Emergency cards: List of safe/unsafe medications
- Healthcare team contact: 24/7 accessible providers
Emergency Kits:
- Glucose preparations: For acute situations
- Contact information: Emergency contacts and specialists
- Medication lists: Current medications and allergies
Health Maintenance
Regular Monitoring:
- Annual assessments: Comprehensive health evaluations
- Laboratory monitoring: Porphyrin levels, liver function
- Complication screening: Kidney function, blood pressure
- Cancer screening: Enhanced surveillance for HCC
Specialized Care:
- Porphyria centers: Multidisciplinary expertise
- Regular follow-up: Frequency based on disease activity
- Family screening: Periodic testing of relatives
Education and Support
Patient Education:
- Disease understanding: Pathophysiology and triggers
- Self-management: Recognizing early symptoms
- Resource materials: Written guidelines and references
Support Systems:
- Patient support groups: American Porphyria Foundation
- Online resources: Reliable medical information
- Healthcare team: Coordinated care approach
10. Global & Regional Statistics
Global Prevalence and Incidence
Overall Prevalence:
- All porphyrias combined: 1 in 20,000 to 1 in 200,000
- Symptomatic cases: Much lower due to low penetrance
- Regional variations: Significant due to founder effects
Type-Specific Global Data:
Acute Porphyrias:
- AIP: 1-2 per 100,000 (highest in Northern Europeans)
- VP: 1 per 1,000,000 globally (higher in South Africa)
- HCP: 1 per 1,000,000 globally
- ALAD: <10 cases reported worldwide
Cutaneous Porphyrias:
- PCT: 1 per 25,000 (most common type)
- EPP: 1 per 140,000 to 1 per 200,000
- CEP: <200 cases reported globally
- HEP: <50 cases reported globally
Regional Variations
Europe:
- Northern European countries: Higher AIP prevalence
- Finland: 1 in 2,000 carry AIP gene due to founder effect
- Sweden: Well-documented AIP families
- UK: Comprehensive porphyria services and registries
Africa:
- South Africa: VP prevalence 1 in 300 in white population
- Founder effect: Single mutation in Afrikaner population
- Other regions: Limited data available
Asia:
- Japan: Lower overall prevalence
- China: Emerging recognition and diagnosis
- India: Underdiagnosis suspected
- Southeast Asia: Limited epidemiological data
Americas:
- United States: Well-characterized patient populations
- Canada: Similar patterns to Northern Europe
- Latin America: Variable data, likely underdiagnosed
- Brazil: Growing recognition and research
Oceania:
- Australia: European-like prevalence patterns
- New Zealand: Limited data but similar to Australia
Mortality and Survival Statistics
Mortality Rates:
Acute Porphyrias:
- During acute attacks: 1-5% mortality
- Long-term mortality: 2-3 fold increased risk
- Primary causes: Respiratory failure, cardiovascular events, cancer
Cutaneous Porphyrias:
- PCT: Increased liver cancer risk (60-fold)
- EPP: End-stage liver disease in 2-5%
- Overall: Good prognosis with proper management
Survival Rates:
- 10-year survival: 85-90% in acute porphyrias
- 20-year survival: 70-80% in acute porphyrias
- Factors affecting survival: Early diagnosis, proper management, complication prevention
Country-Specific Data
United States:
- Estimated cases: 10,000-15,000 total
- Most common: PCT (40%), AIP (30%), EPP (20%)
- Mortality: Standardized mortality ratio 2.6
- Healthcare costs: $50,000-100,000 per patient annually
United Kingdom:
- National registry: Comprehensive data collection
- Prevalence: Similar to other Northern European countries
- Specialized centers: Cardiff, London providing expert care
South Africa:
- VP prevalence: 1 in 300 in Afrikaner population
- Genetic studies: Well-characterized founder mutation
- Clinical experience: Largest VP cohort globally
Finland:
- AIP prevalence: Highest globally due to founder effect
- Genetic studies: Important contributions to understanding
- Population studies: Long-term outcome data
Demographic Patterns
Age Distribution:
- Acute porphyrias: Peak onset 20-40 years
- PCT: Peak onset 40-60 years
- EPP: Often presents in childhood
- CEP: Neonatal or early childhood onset
Gender Distribution:
- Acute attacks: 70-80% occur in women
- PCT: 3:1 male predominance
- EPP: Equal gender distribution
- Hormonal influence: Strong in acute porphyrias
Healthcare Burden
Economic Impact:
- Direct medical costs: $100-500 million annually (US)
- Indirect costs: Lost productivity, disability
- Emergency care: High utilization during acute attacks
- Specialist care: Concentration in tertiary centers
Healthcare Utilization:
- Emergency visits: 5-10 per year per active patient
- Hospitalizations: 2-5 per year in severe cases
- Specialist consultations: Multiple specialties involved
- Diagnostic delays: Average 15+ years for some types
Trends and Projections
Recent Trends (2010-2024):
- Increased recognition: Better diagnostic awareness
- Earlier diagnosis: Genetic testing availability
- Improved outcomes: Better acute management
- New treatments: Givosiran for AIP, afamelanotide for EPP
Future Projections:
- Improved diagnosis: Genetic testing becoming standard
- Better outcomes: New therapies reducing morbidity
- Gene therapy: May transform treatment landscape
- Global health: Increased awareness in developing countries
Research Contributions by Region
North America:
- Clinical trials: Major pharmaceutical company involvement
- Patient registries: Large cohort studies
- Basic research: Molecular mechanisms, gene therapy
Europe:
- International collaborations: European Porphyria Network
- Long-term studies: Multi-generational family studies
- Treatment development: Novel therapeutic approaches
Other Regions:
- Emerging research: Asia-Pacific porphyria research growing
- Global initiatives: WHO rare disease initiatives
- Collaborative networks: International porphyria organizations
11. Recent Research & Future Prospects
Gene Therapy Advances
Adeno-Associated Virus (AAV) Vectors:
- Proof-of-concept: Successful in mouse models of AIP and EPP
- Target tissues: Liver-directed gene therapy most promising
- Clinical trials: Phase I studies initiated for AIP
- Challenges: Vector immunogenicity, long-term safety
In Vivo Gene Editing:
- CRISPR-Cas9: Potential for correcting mutations
- Base editing: Precise correction without double-strand breaks
- Prime editing: New technique for exact corrections
- Delivery challenges: Efficient hepatocyte targeting needed
Ex Vivo Gene Therapy:
- Autologous hepatocytes: Gene correction followed by transplantation
- Induced pluripotent stem cells: Potential source of hepatocytes
- Manufacturing challenges: Scalability and cost considerations
Novel Pharmacological Approaches
RNA Therapeutics:
- Givosiran success: Validates siRNA approach for porphyrias
- Next-generation siRNAs: Improved potency and safety
- Antisense oligonucleotides: Alternative RNA-targeting approach
- microRNA modulators: Targeting regulatory pathways
Small Molecule Therapeutics:
- MT-7117: FECH stabilizer for EPP (Phase III trials)
- Molecular chaperones: Protein folding enhancement
- Allosteric modulators: Enhancing residual enzyme activity
- Metabolic modulators: Targeting heme synthesis pathway
Substrate Reduction Therapy:
- ALA synthase inhibitors: Beyond RNA approaches
- Heme oxygenase modulators: Balancing heme breakdown
- Iron chelation: For iron-overload porphyrias
- Combination therapies: Multiple pathway targeting
Biomarker Development
Predictive Biomarkers:
- Attack prediction: Metabolomic signatures pre-attack
- Treatment response: Markers for therapy selection
- Disease progression: Long-term prognosis indicators
- Toxicity monitoring: Safety biomarkers for new therapies
Liquid Biopsies:
- Circulating nucleic acids: Non-invasive monitoring
- Exosomes: Cellular communication markers
- Proteomics: Protein signatures in blood/urine
- Metabolomics: Comprehensive metabolite profiling
Diagnostic Innovations
Point-of-Care Testing:
- Rapid porphyrin assays: Emergency department use
- Smartphone-based detection: Colorimetric assays
- Biosensors: Real-time monitoring devices
- Artificial intelligence: Pattern recognition in symptoms
Advanced Imaging:
- Fluorescence imaging: Direct visualization of porphyrins
- Optical coherence tomography: Skin structure assessment
- Molecular imaging: Tracking enzyme activity in vivo
- Functional MRI: Neurological complication assessment
Personalized Medicine
Pharmacogenomics:
- Drug response prediction: Based on genetic variants
- Dosing algorithms: Personalized treatment protocols
- Safety profiling: Individual risk assessment
- Companion diagnostics: Therapy selection markers
Precision Therapy Selection:
- Mutation-specific treatments: Targeted to specific defects
- Phenotype-guided therapy: Based on clinical presentation
- Biomarker-driven decisions: Treatment choice algorithms
- Adaptive protocols: Dynamic treatment adjustment
Regenerative Medicine
Cell Therapy:
- Hepatocyte transplantation: Replacing deficient cells
- Mesenchymal stem cells: Tissue regeneration potential
- Induced pluripotent stem cells: Patient-specific therapies
- Organoids: Disease modeling and drug testing
Tissue Engineering:
- Bioartificial liver: Temporary support during crises
- Liver tissue scaffolds: Supporting regeneration
- 3D printing: Custom tissue constructs
- Microfluidics: Organ-on-chip disease models
Digital Health and AI
Machine Learning Applications:
- Diagnostic algorithms: Pattern recognition in symptoms
- Predictive modeling: Attack prediction and prevention
- Drug discovery: AI-driven compound identification
- Clinical trial optimization: Patient selection and monitoring
Digital Therapeutics:
- Mobile health apps: Symptom tracking and management
- Wearable devices: Continuous monitoring
- Telemedicine: Remote specialist consultation
- Virtual reality: Pain management and therapy
Global Research Initiatives
International Collaborations:
- Global Porphyria Consortium: Multi-center studies
- Regulatory harmonization: Standardized endpoints
- Data sharing: International patient registries
- Capacity building: Research in developing countries
Rare Disease Networks:
- FDA Orphan Drug Program: Incentivizing development
- EMA COMP: European regulatory support
- IRDiRC: International coordination
- Patient organization partnerships: Research advocacy
Future Prospects (5-10 Year Outlook)
Near-term Expectations (2025-2030):
- Gene therapy approvals: First products likely for AIP
- Novel small molecules: Multiple new options available
- Improved diagnostics: Point-of-care testing widespread
- Personalized protocols: Standard care approach
Medium-term Vision (2030-2035):
- Curative treatments: Gene therapy becoming standard
- Prevention focus: Pre-symptomatic interventions
- Simplified monitoring: Non-invasive biomarkers
- Global access: Therapies available worldwide
Challenges Remaining:
- Cost considerations: Making therapies accessible
- Long-term safety: Gene therapy durability
- Rare variants: Treatment for extremely rare types
- Global implementation: Extending care to all regions
Research Priorities
Scientific Priorities:
- Mechanism understanding: Complete pathway elucidation
- Biomarker validation: Clinical utility demonstration
- Combination therapies: Synergistic approaches
- Prevention strategies: Pre-clinical intervention
Clinical Priorities:
- Natural history studies: Better prognostic understanding
- Quality of life research: Patient-centered outcomes
- Health economics: Cost-effectiveness analyses
- Implementation science: Real-world effectiveness
Translational Priorities:
- Companion diagnostics: Therapy selection tools
- Regulatory pathways: Efficient approval processes
- Manufacturing scale-up: Commercial viability
- Healthcare delivery: Optimal care models
12. Interesting Facts & Lesser-Known Insights
Historical Fascinations
The “Madness” of King George III:
- Historical diagnosis: Retrospective analysis suggests acute intermittent porphyria
- Symptoms documented: Attacks of abdominal pain, confusion, and dark urine
- Political implications: Regency Act of 1811 due to his incapacity
- Modern debate: Some experts argue bipolar disorder more likely
- Genetic studies: Attempted DNA analysis from hair samples
The Vampire Connection:
- Porphyria and vampire myths: CEP patients’ photophobia and red urine
- Garlic sensitivity: Some porphyria patients report garlic intolerance
- Behavioral changes: Psychiatric symptoms during attacks
- Physical appearance: Photosensitivity and pale skin
- Modern perspective: Coincidental similarities, not true connection
Royal Family Porphyria:
- House of Hanover: Multiple members suspected of porphyria
- Genetic analysis: Attempts to trace inheritance pattern
- Historical medical records: Detailed documentation of symptoms
- Modern skepticism: Alternative diagnoses proposed
Biochemical Curiosities
Porphyrin Fluorescence:
- Red fluorescence: Porphyrins glow red under UV light
- Diagnostic utility: Woods lamp examination for some types
- Artistic applications: Porphyrin-containing paints and dyes
- Natural occurrence: Present in chlorophyll and hemoglobin
Heme Biosynthesis Complexity:
- Ancient pathway: Evolutionary conserved across species
- Dual compartments: Mitochondrial and cytoplasmic steps
- Regulation: Complex feedback mechanisms
- Daily production: 6-8 grams of hemoglobin synthesized daily
Porphyrin Chemistry:
- Tetrapyrrole structure: Four pyrrole rings linked
- Metal chelation: Can bind various metals (iron, magnesium, cobalt)
- Photodynamic therapy: Porphyrins used in cancer treatment
- Industrial applications: Catalysts and sensors
Medical Mysteries
Low Penetrance Phenomenon:
- Genetic paradox: Most carriers never develop symptoms
- Environmental modifiers: Unknown factors determine expression
- Gender differences: Why women are more affected in acute types
- Age of onset: Why symptoms typically appear after puberty
Attack Triggers:
- Stress response: Why stress precipitates attacks unclear
- Hormonal influences: Complex interactions not fully understood
- Fasting physiology: Mechanisms of diet-induced attacks
- Drug interactions: How certain medications trigger attacks
Geographic Clusters:
- Founder effects: Isolated populations with high prevalence
- Migration patterns: How mutations spread globally
- Cultural factors: Diet and lifestyle influences on expression
- Environmental geography: Climate effects on symptoms
Diagnostic Challenges
The Great Masquerader:
- Appendicitis mimicry: Leading to unnecessary surgeries
- Psychiatric misdiagnosis: Attacks attributed to mental illness
- Fibromyalgia overlap: Chronic pain syndromes
- Multiple sclerosis confusion: Neurological symptoms
Laboratory Quirks:
- Light sensitivity: Samples must be protected from light
- Storage requirements: Specific temperature and pH needs
- False positives: Other conditions can elevate porphyrins
- Normal results: Can occur between acute attacks
Historical Misdiagnoses:
- Hysteria label: Particularly for women with acute attacks
- Appendectomies: Unnecessary surgeries for abdominal pain
- Psychiatric admissions: Misinterpreted neuropsychiatric symptoms
- Lead poisoning: Similar presentations causing confusion
Cultural and Social Impacts
Porphyria in Literature:
- Gothic novels: Influenced vampire and werewolf myths
- Medical thrillers: Featured in various mystery novels
- Case studies: Fascinating medical literature throughout history
- Patient narratives: Powerful autobiographical accounts
Support Communities:
- Patient organizations: American Porphyria Foundation (1982)
- Online communities: Global patient networks
- Advocacy efforts: Raising awareness and research funding
- Patient registries: Contributing to medical research
Social Challenges:
- Invisible illness: Symptoms not always apparent
- Emergency care: Educating emergency departments
- Work accommodations: Light sensitivity and unpredictable attacks
- Family dynamics: Genetic implications and family planning
Modern Paradoxes
Medication Safety:
- Drug databases: Comprehensive lists of safe/unsafe medications
- Pharmacist education: Specialized training needed
- Emergency protocols: Ensuring proper drug selection
- Research challenges: Limited clinical trials due to rarity
Technology Applications:
- UV protective clothing: Advanced materials development
- LED lighting: Reduced triggering of photosensitivity
- Mobile apps: Medication checking and symptom tracking
- Genetic counseling: Online risk assessment tools
Global Health Disparities:
- Diagnosis delays: Longer in developing countries
- Treatment access: Hemin availability limited globally
- Specialist distribution: Concentrated in developed nations
- Research participation: Geographic bias in studies
Unusual Presentations
Pediatric Porphyrias:
- EPP in infants: Screaming with sun exposure
- CEP severity: Life-threatening photosensitivity
- Growth effects: Impact on development
- Educational challenges: School accommodation needs
Occupational Considerations:
- Healthcare workers: Balancing patient care with photosensitivity
- Artists: Some use porphyrin fluorescence creatively
- Pilots: Restrictions due to photosensitivity and attacks
- Shift workers: Circadian disruption effects
Athletic Participation:
- Outdoor sports: Major lifestyle restrictions
- Olympic athletes: Documented cases with porphyria
- Exercise physiology: Effects on heme metabolism
- Performance implications: Energy metabolism challenges
Research Serendipities
Accidental Discoveries:
- DNA discovery: Griffith’s transformation experiments
- Enzyme purification: Advances from porphyria research
- Photodynamic therapy: Developed from porphyrin studies
- Gene therapy vectors: Liver targeting optimized for porphyrias
Model Organism Studies:
- Mouse models: Essential for therapy development
- Yeast genetics: Basic pathway understanding
- Zebra fish: Developmental biology insights
- Cell culture: High-throughput screening platforms
Unexpected Connections:
- Cancer metabolism: Heme pathway in tumor cells
- Neurodegeneration: Iron metabolism connections
- Aging research: Cellular energy production
- Circadian biology: Heme regulation of biological clocks
Future Implications
Precision Medicine Pioneer:
- Rare disease model: Template for other genetic conditions
- RNA therapeutics: Porphyria leading the way
- Gene therapy: Liver-directed approaches
- Biomarker development: Non-invasive monitoring methods
Global Health Lessons:
- Rare disease networks: International collaboration models
- Patient advocacy: Effective partnership with researchers
- Regulatory innovation: Orphan drug development
- Healthcare delivery: Specialized care models
Scientific Legacy:
- Biochemistry foundations: Heme metabolism understanding
- Genetics principles: Penetrance and expressivity concepts
- Molecular medicine: From genes to therapies
- Personalized care: Individual variation in disease expression
Myths vs. Reality
Common Misconceptions:
- “Vampire disease”: Oversimplified media portrayal
- “Always fatal”: Most patients live normal lifespans
- “Extremely rare”: More common than often thought
- “No treatment”: Multiple effective therapies exist
Public Education Needs:
- Emergency awareness: ER education about porphyrias
- Primary care training: Recognition and referral
- Patient empowerment: Self-advocacy skills
- Family education: Genetic implications and testing
Research Mythology:
- “Simple genetic disease”: Actually quite complex
- “Single gene therapies”: Multiple factors involved
- “Easy diagnosis”: Often challenging to confirm
- “Uniform presentation”: Highly variable disease expression
The study of porphyrias continues to yield insights not only into these fascinating disorders themselves but also into fundamental aspects of human biology, genetics, and metabolism. From their role in the discovery of DNA to their position at the forefront of modern gene therapy, porphyrias represent both a medical challenge and a scientific opportunity that continues to drive innovation in rare disease research and treatment.