
⚠️ Disclaimer: The information provided in this article is for educational purposes only and does not constitute medical advice. RevisionTown does not provide diagnosis, treatment, or medical recommendations. Always consult a qualified healthcare professional regarding any medical condition, symptoms, or concerns.
Read More – 🏥 Medical Disclaimer
Ovarian Cancer: A Comprehensive Report
1. Overview
What is ovarian cancer?
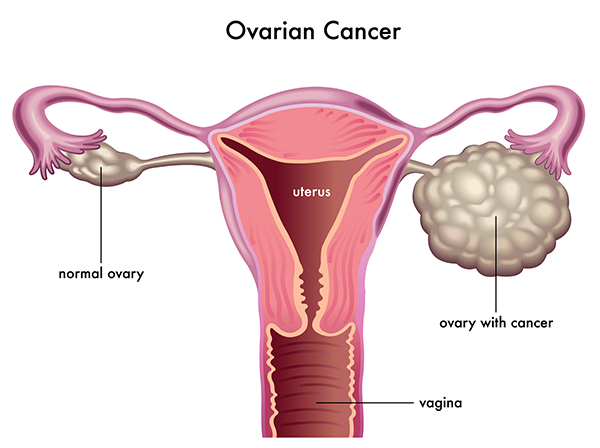
Ovarian cancer is a malignant disease that originates in the ovaries, the female reproductive organs responsible for producing eggs and the hormones estrogen and progesterone. It represents a group of different cancers that all share a common anatomic location. While often discussed as a single disease, ovarian cancer actually comprises several histopathological entities with distinct clinical behaviors and underlying biological mechanisms. The most common form is epithelial ovarian cancer (accounting for approximately 90% of cases), which arises from the outer surface of the ovary or the fallopian tube epithelium. Other less common types include germ cell tumors, sex cord-stromal tumors, and small cell carcinomas.
A concise yet detailed definition
Ovarian cancer is a heterogeneous group of malignancies arising from the ovaries or fallopian tubes, characterized by abnormal cell growth with the potential to invade or spread to other parts of the body. It is classified by cell type (epithelial, germ cell, stromal), grade (how abnormal the cells appear), and stage (extent of spread). The disease is particularly challenging because it frequently progresses with vague, nonspecific symptoms that may be attributed to common benign conditions, often resulting in diagnosis at advanced stages when treatment effectiveness is limited. It is distinguished by its tendency for peritoneal spread within the abdominal cavity before producing detectable symptoms.
The affected body parts/organs
Ovarian cancer primarily affects the ovaries and/or fallopian tubes, but due to its nature and pattern of spread, it impacts multiple organs and systems:
Primary sites:
- Ovaries: Paired reproductive organs located on either side of the uterus
- Fallopian tubes: Recent evidence suggests many “ovarian” cancers actually originate here
- Peritoneum: The membrane lining the abdominal cavity can be a primary site (primary peritoneal carcinoma)
Common sites of spread:
- Peritoneal cavity: Cancer cells often spread throughout the abdominal cavity
- Omentum: The fatty apron of tissue covering the abdominal organs is frequently involved
- Diaphragm: Cancer cells can implant on the diaphragmatic surface
- Bowel surfaces: Small and large intestines are common sites of metastasis
- Liver surface: Metastatic implants often appear on the liver capsule
- Lymph nodes: Particularly pelvic and para-aortic nodes
- Distant organs: Advanced disease can spread to the liver parenchyma, lungs, pleura, and rarely the brain
Affected systems:
- Reproductive system: Primary site of disease
- Gastrointestinal system: Involvement can cause bowel obstruction
- Urinary system: Ureteral obstruction may occur
- Lymphatic system: Regional and distant lymph node involvement
- Peritoneal and pleural spaces: Fluid accumulation (ascites, pleural effusion)
Prevalence and significance of the disease
Ovarian cancer represents a significant global health challenge, particularly due to its high mortality rate relative to incidence:
Epidemiological impact:
- Represents approximately 3% of cancers in women but causes more deaths than any other reproductive system cancer
- Lifetime risk for women in the general population is about 1.3% (1 in 78)
- Worldwide, over 310,000 women are diagnosed annually with about 207,000 deaths
- Fifth leading cause of cancer deaths among women in the United States
- Median age at diagnosis is 63 years
- Five-year survival rates vary dramatically by stage: over 90% for stage I but less than 30% for stage IV
Significance:
- Often called the “silent killer” due to subtle early symptoms leading to late-stage diagnosis
- Approximately 70-75% of women are diagnosed at advanced stages (III or IV)
- High recurrence rate (70-80%) even after successful initial treatment
- Substantial economic burden estimated at $5.7 billion annually in the United States alone
- Significant psychological impact due to effects on body image, reproductive capacity, sexuality, and quality of life
- Research has been historically underfunded relative to disease burden
- Recent advances in understanding genetic factors (particularly BRCA1/2) have improved risk identification
- Emerging precision medicine approaches show promise for improved outcomes
2. History & Discoveries
When and how was ovarian cancer first identified?
The recognition and understanding of ovarian cancer evolved gradually over centuries:
Ancient and medieval period:
- References to ovarian abnormalities date back to ancient Egyptian, Greek, and Roman medical texts
- Soranus of Ephesus (1st-2nd century CE) described ovarian swellings
- Galen (130-210 CE) documented ovarian abnormalities but had limited understanding of their nature
17th-18th centuries:
- 1686: Dutch physician Regnier de Graaf published detailed anatomical descriptions of the ovaries
- 1774: John Hunter in England described surgical removal of ovarian cysts
- 1793: Matthew Baillie published detailed pathological descriptions of ovarian tumors
19th century – formal recognition:
- 1809: Ephraim McDowell performed the first successful ovariotomy (removal of an ovarian tumor)
- 1839: Robert Bright published clear descriptions distinguishing benign and malignant ovarian tumors
- 1873: Walter Spence Wells documented 500 ovariotomies, establishing the surgical approach to ovarian tumors
- 1873: Heinrich Waldeyer proposed that many ovarian cancers arise from the ovarian surface epithelium
- 1895: Thomas Spencer Wells published landmark work on ovarian and uterine tumors
Early 20th century – classification and understanding:
- 1901: The first classification of ovarian tumors was proposed
- 1925: Gynecological oncology emerged as a specialty field
- 1932: First comprehensive staging system proposed for ovarian cancer
- 1940s: First chemotherapy treatments explored for ovarian malignancies
Who discovered it?
Rather than having a single discoverer, ovarian cancer’s identification and understanding emerged through contributions of numerous physicians and scientists:
Key historical figures:
- Matthew Baillie (1761-1823): Provided early detailed pathological descriptions
- Ephraim McDowell (1771-1830): Performed first successful ovarian tumor removal surgery in 1809
- Thomas Spencer Wells (1818-1897): Pioneered surgical techniques for ovarian tumors and documented outcomes
- Heinrich Waldeyer (1836-1921): Proposed the origin of ovarian cancer from surface epithelium
- Emil Novak (1883-1957): Developed early classification systems for ovarian tumors
- Howard Taylor (1900-1985): Advanced surgical techniques and treatment approaches
- Hugh Barber and Alexander Brunschwig (mid-20th century): Pioneered radical surgical approaches
Modern era pioneers:
- Robert C. Young: Advanced chemotherapy protocols in the 1970s-1980s
- Robert C. Bast Jr.: Led the discovery of CA-125 tumor marker in 1981
- Mary-Claire King and Mark Skolnick: Discovered BRCA1 and BRCA2 genes in the 1990s
- Beth Karlan and Ie-Ming Shih: Contributed to understanding fallopian tube origins of serous ovarian cancer
- Douglas Levine and David Huntsman: Identified distinct molecular subtypes of ovarian cancer
Major discoveries and breakthroughs in its research and treatment
Diagnostic breakthroughs:
- 1981: Discovery of CA-125 tumor marker by Robert Bast and colleagues
- 1990s: Development of transvaginal ultrasound techniques for ovarian imaging
- 1994-1995: Identification of BRCA1 and BRCA2 genes and their link to hereditary ovarian cancer
- 2000s: Recognition of distinct molecular subtypes of ovarian cancer
- 2010s: Development of multimodal screening approaches (combining CA-125, ultrasound, and algorithm-based monitoring)
- 2016-2020: Emergence of liquid biopsy techniques to detect circulating tumor DNA
Treatment milestones:
- 1950s: Introduction of nitrogen mustard chemotherapy
- 1970s: Introduction of platinum-based chemotherapy (cisplatin)
- 1980s: Development of carboplatin with improved toxicity profile
- 1990s: Introduction of paclitaxel, establishing platinum/taxane combinations as standard treatment
- 1990s: Development of intraperitoneal chemotherapy approaches
- 2003: Introduction of cytoreductive surgery concept “optimal debulking”
- 2004-2006: Demonstration of improved outcomes with intraperitoneal chemotherapy
- 2011: FDA approval of bevacizumab (Avastin), first targeted therapy for ovarian cancer
- 2014-2018: PARP inhibitors (olaparib, rucaparib, niraparib) approved for treatment
- 2020: Approval of maintenance therapies significantly extending progression-free survival
Scientific understanding:
- 1990s: Identification of the role of p53 mutations in high-grade serous ovarian cancer
- 2007: Paradigm shift recognizing many “ovarian” cancers originate in the fallopian tubes
- 2011: The Cancer Genome Atlas project characterized molecular features of high-grade serous ovarian cancer
- 2016: World Health Organization revised classification based on molecular features
- 2018-2020: Identification of homologous recombination deficiency as a biomarker for treatment selection
- 2020s: Improved understanding of tumor microenvironment and immune interactions
Evolution of medical understanding over time
Early concepts (pre-1950s):
- Ovarian cancer viewed primarily as a surgical disease
- Limited understanding of cellular origins and mechanisms
- Classification based entirely on morphology
- Poor prognosis with limited treatment options
- Considered a single disease entity
Mid-century developments (1950s-1970s):
- Recognition of potential for chemotherapy sensitivity
- Understanding the role of staging in prognosis
- Emergence of ovarian cancer as a target for clinical trials
- Beginning of specialized gynecologic oncology care
- Recognition of histological subtypes with different behaviors
Modern understanding (1980s-2000s):
- Recognition of the importance of surgical cytoreduction
- Development of combination chemotherapy approaches
- Understanding of molecular and genetic risk factors
- Emerging awareness of different cellular origins
- Appreciation of heterogeneity within ovarian cancer types
- Recognition of the importance of platinum-sensitivity
Contemporary paradigms (2000s-present):
- Recognition that many high-grade serous cancers originate in the fallopian tubes rather than ovaries
- Reclassification into five main subtypes with distinct origins, molecular features, and clinical behavior:
- High-grade serous carcinoma
- Low-grade serous carcinoma
- Clear cell carcinoma
- Endometrioid carcinoma
- Mucinous carcinoma
- Understanding ovarian cancer as many different diseases sharing an anatomic location
- Recognition of molecular pathways that drive different subtypes
- Application of precision medicine approaches based on molecular profiles
- Focus on early detection, prevention for high-risk populations
- Evolution toward maintenance therapy approaches for long-term disease control
- Emerging understanding of immune microenvironment and potential for immunotherapy
- Recognition of the continuum between borderline tumors and low-grade carcinomas
3. Symptoms
Early symptoms vs. advanced-stage symptoms
Early symptoms (Stage I-II): Early symptoms of ovarian cancer are often subtle, nonspecific, and easily attributed to benign conditions, contributing to diagnostic delays. These symptoms frequently include:
- Abdominal/pelvic discomfort: Vague discomfort, pressure, or pain in the abdomen or pelvis
- Bloating: Persistent abdominal distension that doesn’t resolve
- Early satiety: Feeling full quickly when eating
- Urinary frequency/urgency: Needing to urinate more often or with greater urgency
- Digestive changes: Mild constipation, indigestion, or other changes in bowel habits
- Fatigue: Unexplained tiredness not relieved by rest
- Menstrual irregularities: Changes in cycle, heavier or more painful periods (particularly in younger women)
- Dyspareunia: Pain during sexual intercourse, particularly with deep penetration
- Back pain: Lower back discomfort that may be persistent or intermittent
- Abdominal enlargement: Gradual increase in abdominal girth that may be mistaken for weight gain
Key characteristics of early symptoms:
- Often cyclical or intermittent initially
- Mild to moderate in intensity
- May be dismissed as normal bodily changes
- Typically present for 3-6 months before diagnosis
- Increase in frequency and persistence over time
- Usually represent a change from normal bodily patterns
Advanced-stage symptoms (Stage III-IV): As ovarian cancer progresses, symptoms become more pronounced and persistent due to tumor growth, metastatic spread, and complications:
- Pronounced abdominal distension: Due to ascites (fluid accumulation) and tumor mass
- Significant abdominal pain: More persistent and intense than early stages
- Ascites: Accumulation of fluid in the peritoneal cavity causing increased abdominal size
- Palpable abdominal/pelvic mass: Tumor growth large enough to be felt on examination
- Unintentional weight loss: Often significant (>5% of body weight)
- Severe fatigue: Debilitating tiredness affecting daily functioning
- Anorexia: Loss of appetite leading to reduced food intake
- Nausea and vomiting: Often related to partial bowel obstruction
- Constipation: Can be severe due to bowel involvement
- Shortness of breath: Due to pleural effusions or abdominal distension pushing up on the diaphragm
- Lymphedema: Swelling in the legs due to lymphatic obstruction
- Paraneoplastic phenomena: Hypercalcemia, hypercoagulability, or other systemic effects
Key characteristics of advanced symptoms:
- Persistent rather than intermittent
- Moderate to severe in intensity
- Multiple symptoms typically present simultaneously
- Significant impact on daily functioning and quality of life
- Often progressive despite symptomatic treatments
- May include emergency presentations (bowel obstruction, pulmonary embolism)
Common vs. rare symptoms
Common symptoms (occurring in >25% of patients):
- Abdominal bloating and distension (70-90%)
- Abdominal or pelvic pain/discomfort (60-80%)
- Early satiety or difficulty eating (50-60%)
- Urinary symptoms (frequency, urgency) (45-55%)
- Fatigue (50-75%)
- Constipation or changes in bowel habits (40-50%)
- Abdominal or pelvic pressure (40-45%)
- Back pain (30-45%)
- Dyspareunia (painful intercourse) (25-30%)
- Vaginal bleeding (postmenopausal) (25% in those past menopause)
Less common symptoms (10-25% of patients):
- Unexplained weight loss (15-25%)
- Nausea or vomiting (15-20%)
- Shortness of breath (15-20%)
- Leg swelling (unilateral or bilateral) (10-20%)
- Loss of appetite (15-25%)
- Dysmenorrhea (painful periods) (15-20% in premenopausal women)
- Diarrhea (10-15%)
- Extreme fatigue (20-25%)
- Pelvic heaviness (20-25%)
- Unexplained fever (10-15%)
Rare symptoms (<10% of patients):
- Paraneoplastic syndromes (5-8%):
- Hypercalcemia
- Dermatomyositis
- Cerebellar degeneration
- Lambert-Eaton myasthenic syndrome
- Superficial thrombophlebitis (Trousseau syndrome) (3-5%)
- Sister Mary Joseph nodule (umbilical metastasis) (1-3%)
- Pleural effusion with respiratory symptoms (5-8% as presenting symptom)
- Cushing’s syndrome (with certain stromal tumors) (<1%)
- Virilization (with certain stromal tumors) (2-5%)
- Abnormal uterine bleeding (with estrogen-producing tumors) (3-5%)
- Precocious puberty (with juvenile granulosa cell tumors) (<1%)
- Acanthosis nigricans (skin changes) (1-2%)
- Rectal bleeding (due to bowel invasion) (1-3%)
- Hemoptysis (with lung metastasis) (<1%)
How symptoms progress over time
Symptom evolution pattern:
Prodromal phase (months to years before diagnosis):
- Occasional, intermittent symptoms
- Symptoms often attributed to:
- Age-related changes
- Menopause
- Digestive disorders (IBS, constipation)
- Weight gain
- Stress
- Symptoms typically resolve temporarily, creating false reassurance
- Gradual increase in frequency, with longer symptom-free intervals
Early symptomatic phase (3-6 months before diagnosis):
- Symptoms become more frequent
- Multiple symptoms begin to cluster together
- Symptom-free intervals shorten
- Intensity increases gradually
- Symptoms begin to interfere with daily activities
- Medical attention often sought but misdiagnosis common:
- Irritable bowel syndrome
- Stress/anxiety
- Gastritis
- Menopause
- Depression
Progressive phase (1-3 months before diagnosis):
- Near-constant presence of multiple symptoms
- Significant increase in intensity
- Development of new symptoms
- Visible abdominal changes (distension)
- Symptoms interfere significantly with functioning
- Weight changes become apparent
- Response to symptomatic treatments diminishes
Advanced phase (at diagnosis for stage III-IV disease):
- Constellation of persistent, severe symptoms
- Functional limitations substantial
- Complications emerge (e.g., malnutrition, thrombosis)
- Emergency presentations common:
- Bowel obstruction
- Pulmonary embolism
- Severe pain crisis
- Pleural effusion causing respiratory distress
Symptom progression by type:
Abdominal/gastrointestinal symptoms:
- Initial: Occasional bloating after meals
- Progression: Persistent bloating regardless of food intake
- Advanced: Severe abdominal distension with ascites and pain
Pain:
- Initial: Vague discomfort, often positional or related to activity
- Progression: More persistent pain, less responsive to over-the-counter analgesics
- Advanced: Continuous pain requiring strong analgesics, may include breakthrough pain episodes
Urinary symptoms:
- Initial: Mild increase in frequency, particularly at night
- Progression: Frequency with urgency, pressure symptoms
- Advanced: Difficulty urinating, hydronephrosis due to ureteral obstruction
Constitutional symptoms:
- Initial: Mild fatigue, often attributed to daily stressors
- Progression: Fatigue despite adequate rest, affecting daily activities
- Advanced: Extreme fatigue, anorexia, cachexia (muscle wasting)
Temporal patterns:
- Symptoms tend to follow a progressive rather than stepwise pattern
- Average symptom duration before diagnosis: 3-6 months for advanced disease, potentially longer for early-stage disease
- Progression rate correlates with:
- Histologic subtype (faster in high-grade serous)
- Presence of genetic mutations (BRCA1/2)
- Patient age (often faster in younger women)
- Hormone receptor status
Key progression markers that should prompt investigation:
- Symptoms occurring daily or nearly daily for 2-3 weeks
- Multiple symptoms occurring together (symptom clustering)
- Rapid increase in symptom severity over weeks rather than months
- Symptoms that represent a clear change from normal bodily patterns
- Lack of response to treatments for presumed benign conditions
- Development of constitutional symptoms (fatigue, weight loss) alongside abdominal/pelvic symptoms
4. Causes
What are the biological and environmental causes?
Biological mechanisms of ovarian carcinogenesis:
Cellular origins and pathways:
- Fallopian tube origin theory: Strong evidence that high-grade serous carcinomas originate from the fallopian tube epithelium, particularly the fimbriated end
- Ovarian surface epithelium (OSE): Traditional view that epithelial ovarian cancers arise from the surface epithelium
- Endometriosis-associated: Clear cell and endometrioid carcinomas frequently arise from endometriotic lesions
- Cortical inclusion cysts: Formation of epithelial-lined cysts within the ovarian cortex that may undergo malignant transformation
- Hilum cells: Transitional area between OSE and tubal epithelium may be susceptible to malignant transformation
Molecular pathways in carcinogenesis:
- p53 mutations: Present in >95% of high-grade serous carcinomas
- BRCA1/2 dysfunction: Leads to defective DNA repair and genomic instability
- Homologous recombination deficiency: Present in approximately 50% of high-grade serous carcinomas
- PTEN/PIK3CA pathway: Frequently altered in endometrioid and clear cell carcinomas
- KRAS/BRAF mutations: Common in mucinous and low-grade serous carcinomas
- ARID1A mutations: Present in clear cell and endometrioid subtypes
- Microsatellite instability: Present in a subset of endometrioid carcinomas
- Hormone signaling: Estrogen and progesterone receptor pathways may influence carcinogenesis
Microenvironmental factors:
- Inflammation: Chronic inflammation may promote malignant transformation
- Oxidative stress: Damage from reactive oxygen species contributes to DNA damage
- Immune surveillance failure: Declining immune recognition of malignant cells
- Cancer-associated fibroblasts: Promote tumor growth and invasion
- Tumor angiogenesis: Formation of new blood vessels to support tumor growth
- Hypoxia: Low oxygen environments selecting for aggressive cancer cells
Environmental causes and contributors:
Reproductive and hormonal factors:
- Incessant ovulation hypothesis: Repeated ovulation cycles cause tissue damage and repair, increasing mutation risk
- Gonadotropin stimulation hypothesis: Excessive stimulation by pituitary hormones may promote carcinogenesis
- Hormonal exposure: Lifetime patterns of estrogen and progesterone exposure influence risk
External environmental factors:
- Talcum powder/asbestos: Controversial link with genital powder use (some studies show association, others do not)
- Industrial chemicals: Exposure to certain industrial chemicals associated with increased risk:
- Acrylamide
- Polychlorinated biphenyls (PCBs)
- Pesticides and herbicides
- Hormone replacement therapy (HRT): Estrogen-only HRT associated with slightly increased risk
- Radiation exposure: High-dose pelvic radiation associated with increased risk
- Infectious agents: Some evidence for potential role of:
- Pelvic inflammatory disease
- Chlamydia trachomatis
- Human papillomavirus (in specific subtypes)
- Endocrine-disrupting chemicals: Potential role of environmental compounds that interfere with hormone signaling
- Air pollution: Emerging evidence linking particulate matter exposure to increased risk
Lifestyle factors with biological impact:
- Obesity: Associated with increased risk through several mechanisms:
- Increased estrogen production in adipose tissue
- Chronic inflammation
- Insulin resistance and altered growth factor signaling
- Smoking: Associated with increased risk of mucinous subtype
- Alcohol consumption: High intake may increase risk through hormonal mechanisms
- Diet: High fat intake, particularly animal fats, may increase risk
- Physical inactivity: Associated with increased risk through multiple pathways
Genetic and hereditary factors
Major hereditary syndromes:
Hereditary Breast and Ovarian Cancer (HBOC) syndrome:
- BRCA1 mutations:
- 35-70% lifetime ovarian cancer risk
- Associated primarily with high-grade serous subtype
- Earlier age of onset (average 50-55 years)
- Located on chromosome 17q
- Higher penetrance for ovarian cancer than BRCA2
- BRCA2 mutations:
- 10-30% lifetime ovarian cancer risk
- Associated primarily with high-grade serous subtype
- Slightly later onset than BRCA1 (average 55-60 years)
- Located on chromosome 13q
- Higher risk for fallopian tube primary cancers
Lynch syndrome (Hereditary Non-Polyposis Colorectal Cancer):
- Caused by mutations in DNA mismatch repair genes:
- MLH1
- MSH2
- MSH6
- PMS2
- EPCAM
- 8-12% lifetime ovarian cancer risk
- Associated with endometrioid and clear cell subtypes
- Earlier age of onset (average 45-50 years)
- Better prognosis compared to sporadic cases
Other hereditary syndromes:
- BRIP1 mutations: 5-10% lifetime risk
- RAD51C/RAD51D mutations: 5-15% lifetime risk
- Peutz-Jeghers syndrome (STK11 mutations): 18-21% lifetime risk
- Cowden syndrome (PTEN mutations): Increased risk, precise percentage uncertain
- Li-Fraumeni syndrome (TP53 mutations): Increased risk for rare ovarian cancer subtypes
Polygenic risk factors:
- Multiple common genetic variants with small individual effects
- Genome-wide association studies (GWAS) have identified >30 risk loci
- Single nucleotide polymorphisms (SNPs) in:
- BABAM1, CYP11A1, TERT, CLPTM1L regions
- MYC, TIPARP, BNC2, CASP8 regions
- Polygenic risk scores under development to assess cumulative impact
Somatic genetic alterations:
- High-grade serous carcinoma:
- Nearly universal TP53 mutations
- Extensive copy number alterations
- Homologous recombination deficiency in ~50%
- CCNE1 amplification in ~20%
- NF1 and RB1 alterations
- Low-grade serous carcinoma:
- KRAS, BRAF, NRAS mutations
- Intact TP53
- Relatively stable genome
- Clear cell carcinoma:
- ARID1A mutations (30-50%)
- PIK3CA mutations (30-40%)
- PTEN alterations
- Endometrioid carcinoma:
- ARID1A mutations (30-55%)
- PTEN mutations (20-40%)
- PIK3CA mutations
- CTNNB1 (β-catenin) mutations
- Mucinous carcinoma:
- KRAS mutations (65-90%)
- TP53 mutations
- HER2 amplification in some cases
Inheritance patterns:
- Autosomal dominant: BRCA1/2, Lynch syndrome genes
- Incomplete penetrance: Not all mutation carriers develop cancer
- Variable expressivity: Different cancer types and ages of onset within families
- Paternal transmission: Often overlooked in family history assessment
- De novo mutations: May occur without family history
Genetic testing considerations:
- Recommended for all women with epithelial ovarian cancer
- Germline testing (inherited mutations) vs. somatic testing (tumor mutations)
- Panel testing approach covers multiple genes simultaneously
- Cascade testing for family members of mutation carriers
- Impact on treatment selection (e.g., PARP inhibitors for BRCA-mutated tumors)
- Psychological and ethical implications for patients and families
Any known triggers or exposure risks
Established triggers and exposures:
Hormonal exposures:
- Hormonal replacement therapy: Estrogen-only HRT increases risk by 20-40%
- Fertility treatments: Potential short-term risk increase with certain ovulation-inducing agents
- Early menarche/late menopause: Extended ovulatory years increase lifetime risk
- Endogenous hormone levels: Higher androgen levels associated with increased risk
- Polycystic ovary syndrome (PCOS): Associated with increased risk of specific subtypes
Inflammatory conditions:
- Endometriosis: Associated with 2-3 fold increased risk for clear cell and endometrioid subtypes
- Pelvic inflammatory disease: Recurrent episodes may increase risk
- Ovarian cysts: Some complex cysts may have malignant potential
- Tubal inflammation: Chronic salpingitis may contribute to malignant transformation
Environmental exposures:
- Talc/asbestos exposure: Genital talc use controversial but meta-analyses suggest possible 30-60% increased risk
- Radiation: High-dose pelvic radiation increases risk by 30-70%
- Asbestos: Occupational exposure associated with increased risk
- Pesticides/herbicides: Agricultural exposures linked to increased risk in some studies
- Tobacco smoke: Clear association with mucinous subtype (doubled risk)
- Air pollution: Emerging evidence for association with particulate matter exposure
Medical interventions affecting risk:
- Tubal ligation: Reduces risk by 30-50%, likely by blocking migration of carcinogens and preventing fallopian tube-derived lesions
- Hysterectomy: Moderate risk reduction (20-30%) even with ovarian preservation
- Salpingectomy: Risk reduction of 35-70% when fallopian tubes removed
- Prolonged androgen therapy: May increase risk of specific subtypes
Exposure patterns and considerations:
Timing of exposures:
- Early life exposures: May have greater impact on risk:
- In utero exposure to diethylstilbestrol (DES)
- Childhood/adolescent exposures during reproductive development
- Cumulative exposures: Lifetime accumulation of certain exposures:
- Years of talc use
- Cumulative radiation dose
- Duration of hormone therapy
- Critical windows: Certain periods of particular vulnerability:
- Perimenarchal period
- Pregnancy and postpartum
- Perimenopausal transition
Dose-response relationships:
- Talc exposure: Some evidence for dose-response with years of use
- Radiation: Clear dose-response relationship for radiation exposure
- Smoking: Stronger association with greater pack-years for mucinous subtype
- Hormone therapy: Risk increases with duration of use
Interaction effects:
- Genetic-environmental interactions:
- BRCA mutation carriers may be more susceptible to hormonal and reproductive risk factors
- Polymorphisms in detoxification enzymes may modify environmental exposure risks
- Synergistic exposures:
- Combined hormone therapy and obesity
- Multiple inflammatory conditions
- Smoking plus asbestos exposure
Latency periods:
- Hormonal exposures: Effects may manifest 5-10 years after exposure
- Inflammatory conditions: Extended latency of 10-20 years
- Chemical carcinogens: Variable latency periods of 10-30 years
- Radiation: Typically 10-15 year minimum latency
Risk-reducing behaviors:
- Oral contraceptive use: 30-50% risk reduction with long-term use (5+ years)
- Pregnancy and breastfeeding: Each full-term pregnancy reduces risk by approximately 10%
- Breastfeeding: Risk reduction of about 2-4% per month of breastfeeding
- Tubal ligation or salpingectomy: Surgical reduction of risk
- Regular physical activity: Moderate activity associated with 20-30% risk reduction
- Anti-inflammatory medication: Regular use of aspirin or NSAIDs may reduce risk by 10-20%
5. Risk Factors
Who is most at risk (age, gender, occupation, lifestyle, etc.)?
Demographic risk factors:
Age:
- Incidence increases steeply with age
- Median age at diagnosis: 63 years
- Peak incidence: 60-69 years
- Rare before age 30 (except for germ cell tumors)
- Age-specific incidence:
- Under 30: 1.5 per 100,000
- 30-39: 4.6 per 100,000
- 40-49: 13.4 per 100,000
- 50-59: 26.1 per 100,000
- 60-69: 40.5 per 100,000
- 70+: 46.8 per 100,000
- Early-onset disease (<50 years) more likely to have genetic component
Gender:
- Almost exclusively affects biological females with ovaries
- Primary peritoneal carcinoma (closely related) can rarely occur in males
- Transgender men who retain ovaries maintain risk
Race/Ethnicity:
- Highest rates in non-Hispanic white women in North America and Northern Europe
- Intermediate rates in Hispanic and Asian populations
- Lower rates in Black and African women
- Population-specific risk patterns:
- Ashkenazi Jewish: Higher rate of BRCA mutations (1 in 40 vs. 1 in 400 in general population)
- Japanese women: Higher proportion of clear cell carcinomas
- African American women: Lower incidence but worse survival outcomes
Geographic variation:
- Highest rates in developed regions (North America, Europe)
- Lower rates in Asia and Africa
- Variation by country:
- Highest: Latvia, Lithuania, Belarus (14-16 per 100,000)
- United States and UK: 11-12 per 100,000
- Lowest: China, India, African nations (3-6 per 100,000)
- Migrant studies show rates approach those of adoptive country over generations
Occupational risk factors:
Higher risk occupations:
- Hairdressers/Cosmetologists: 1.3-1.7 times increased risk, possibly related to chemical exposures
- Dry cleaning workers: 1.4-2.1 times increased risk from solvent exposure
- Agricultural workers: 1.4-2.0 times increased risk, likely from pesticide exposure
- Healthcare workers: Mixed evidence, possible increased risk from shift work disrupting circadian rhythms
- Industrial workers exposed to:
- Asbestos (1.5-2.5 times increased risk)
- Aromatic amines
- Metal working fluids
- Formaldehyde
- Printing industry workers: Possible increased risk from ink and solvent exposures
Lifestyle risk factors:
Reproductive patterns:
- Nulliparity: Never having given birth increases risk by 30-60%
- Late childbearing: First pregnancy after age 35 increases risk
- Infertility: Independent risk factor beyond nulliparity
- Never breastfeeding: Lack of lifetime breastfeeding increases risk
- Early menarche/Late menopause: Each year of ovulation increases risk by approximately 2%
Body composition:
- Obesity: BMI >30 increases risk by 30-70%, especially for non-serous subtypes
- Body fat distribution: Central adiposity particularly associated with increased risk
- Adult weight gain: Weight gain of >40 pounds after age 18 associated with increased risk
- Height: Taller stature associated with modest risk increase
Dietary patterns:
- High fat diet: Particularly animal fats associated with 20-30% increased risk
- High sugar consumption: Possible link through insulin pathway stimulation
- Low fruit and vegetable intake: Reduced protective antioxidants and phytonutrients
- High dairy consumption: Mixed evidence, possible moderate increase in risk
- Low vitamin D: Associated with increased risk in some studies
Physical activity:
- Sedentary lifestyle: Physical inactivity increases risk by 20-30%
- Insufficient regular exercise: Less than 2-3 hours of moderate activity per week
- Prolonged sitting time: Independent risk factor beyond general activity levels
Other lifestyle factors:
- Smoking: Mixed impact – increases risk for mucinous type, may decrease for other types
- Alcohol consumption: Heavy consumption (>3 drinks/day) may increase risk by 20-50%
- Sleep disruption: Chronic sleep disturbance and shift work may increase risk
- Stress: Limited evidence for chronic stress as risk factor
- Caffeine intake: No consistent association
Environmental, occupational, and genetic factors
Environmental risk factors:
Residential exposures:
- Air pollution: PM2.5 and nitrogen oxide exposure linked to increased risk
- Water contaminants: Possible associations with:
- Arsenic
- Trihalomethanes (chlorination byproducts)
- Nitrates
- Proximity to industrial facilities: Higher rates near certain manufacturing plants
- Pesticide drift: Residential exposure in agricultural areas
- Indoor air quality: Potential risk from household chemicals and particulates
Chemical exposures:
- Endocrine-disrupting chemicals:
- Bisphenol A (BPA)
- Phthalates
- Polychlorinated biphenyls (PCBs)
- Perfluoroalkyl substances (PFAS)
- Pesticides and herbicides:
- Organochlorines (e.g., DDT)
- Triazine herbicides
- Organophosphates
- Industrial chemicals:
- Formaldehyde
- Benzene
- Solvents (trichloroethylene, perchloroethylene)
- Heavy metals:
- Cadmium
- Lead
- Mercury
Radiation exposure:
- Medical radiation: High-dose pelvic radiation increases risk
- Occupational radiation: Healthcare workers, nuclear industry
- Background radiation: Varies by geographic location, building materials
- Radon exposure: Limited evidence for association
Occupational risk patterns:
High-risk industries:
- Beauty and personal care: Hairdressers, cosmetologists, nail technicians
- Dry cleaning and textile treatment: Chemical exposures
- Agriculture and farming: Pesticide and fertilizer exposure
- Chemical manufacturing: Multiple chemical exposures
- Healthcare: Radiation, chemotherapeutic agents, shift work
- Printing and painting: Solvents and pigments
- Metalworking: Metalworking fluids, metal dust
Exposure routes:
- Inhalation: Airborne particulates, volatile compounds
- Dermal absorption: Direct skin contact with chemicals
- Ingestion: Hand-to-mouth transfer of contaminants
- Combined exposure routes: Often multiple simultaneous pathways
Occupational co-factors:
- Duration of employment: Longer exposure periods increase risk
- Protective equipment use: Inconsistent use increases exposure
- Ventilation quality: Poor ventilation increases exposure levels
- Combined chemical exposures: Synergistic effects possible
- Work stress: May contribute to hormonal disruption
Genetic factors (expanded):
High-penetrance genes:
- BRCA1/2: Account for 10-15% of ovarian cancers
- Lynch syndrome genes: Account for 2-3% of cases
- BRIP1, RAD51C/D, PALB2: Moderate to high risk
- Penetrance modifiers: Environmental and other genetic factors affect expression
Moderate-risk genes:
- ATM: DNA damage response gene
- CHEK2: Cell cycle checkpoint regulator
- NBN: Component of MRE11/RAD50/NBN complex
- BARD1: BRCA1-associated RING domain protein
Low-penetrance genetic factors:
- Single nucleotide polymorphisms (SNPs): Small individual effects, cumulative impact
- Copy number variations: Structural variations affecting gene dosage
- Epigenetic modifications: Heritable changes not involving DNA sequence:
- DNA methylation patterns
- Histone modifications
- Non-coding RNAs
- Mitochondrial DNA variants: Possible influence on susceptibility
Genetic-environmental interactions:
- Gene-environment interactions: Genetic factors modifying response to:
- Hormone exposure
- Chemical carcinogens
- Inflammatory stimuli
- Oxidative stress
- Pharmacogenomics: Genetic variations affecting metabolism of:
- Hormonal medications
- Anti-inflammatory drugs
- Environmental toxins
Impact of pre-existing conditions
Gynecological conditions:
Endometriosis:
- 2-3 fold increased risk, particularly for:
- Clear cell carcinoma (3-fold)
- Endometrioid carcinoma (2-fold)
- Risk increases with severity and duration
- Approximately 5-10% of ovarian cancers associated with endometriosis
- Transformation likely occurs through accumulation of mutations in endometriotic tissue
- Risk-reducing surgeries may be considered in severe cases
Polycystic ovary syndrome (PCOS):
- 2-2.5 fold increased risk in some studies
- Associated with hormone imbalances:
- Elevated androgens
- Insulin resistance
- Chronic anovulation
- Greater impact on non-serous subtypes
- Management of hormonal disruption may modify risk
- Regular monitoring recommended
Pelvic inflammatory disease (PID):
- 1.5-2 fold increased risk with history of multiple episodes
- Chronic inflammation as potential mechanism
- Risk higher with:
- Chlamydia trachomatis infection
- Recurrent episodes
- Delayed or inadequate treatment
Ovarian cysts and benign tumors:
- Certain benign tumors have malignant potential:
- Borderline tumors: 5-10% risk of recurrence as invasive cancer
- Mucinous cystadenomas: Low but present risk
- Endometriomas: Associated with clear cell and endometrioid types
- Regular monitoring recommended for complex ovarian masses
Uterine fibroids:
- Inconsistent association in studies
- Possible shared hormonal risk factors
- May contribute to chronic inflammation
Metabolic and endocrine conditions:
Diabetes mellitus:
- 20-40% increased risk, particularly for non-serous types
- Mechanisms include:
- Insulin resistance and hyperinsulinemia
- Chronic inflammation
- Altered hormone metabolism
- More pronounced effect in type 2 diabetes
- Risk modification with metformin possible (30% reduction in some studies)
Obesity and metabolic syndrome:
- Obesity increases risk by 30-70%
- Metabolic syndrome components add cumulative risk:
- Insulin resistance
- Hypertension
- Dyslipidemia
- Central adiposity
- Risk increases with severity and duration
- Weight loss may modestly reduce risk
Thyroid disorders:
- Hypothyroidism associated with 1.2-1.5 fold increased risk
- Hyperthyroidism shows inconsistent associations
- Autoimmune thyroid disorders may share susceptibility with ovarian cancer
- Regular monitoring recommended in thyroid dysfunction
Inflammatory and autoimmune conditions:
Systemic lupus erythematosus (SLE):
- 1.5-2.5 fold increased risk
- Higher in patients with:
- Longer disease duration
- Greater disease activity
- Immunosuppressive therapy
- Shared genetic susceptibility possible
Rheumatoid arthritis:
- Moderate association in some studies (1.2-1.5 fold)
- Chronic inflammation as potential mechanism
- Possible impact of immunomodulatory treatments
Inflammatory bowel disease:
- Ulcerative colitis: Possible increased risk (1.3-1.8 fold)
- Crohn’s disease: Less consistent association
- Risk may correlate with disease extent and duration
- Shared inflammatory pathways
Other relevant conditions:
Prior cancer history:
- Breast cancer: 2-3 fold increased risk
- Higher with BRCA1/2 mutations
- Higher with early-onset breast cancer
- Treatment-related factors may contribute
- Colorectal cancer: 1.5-2 fold increased risk
- Higher with Lynch syndrome
- Shared inflammatory pathways
- Endometrial cancer: 2-fold increased risk
- Higher with Lynch syndrome
- Shared hormonal risk factors
Psychiatric conditions:
- Mixed evidence for association with:
- Depression
- Anxiety disorders
- Post-traumatic stress disorder
- Potential mechanisms:
- Neuroendocrine disruption
- Altered immune function
- Treatment effects
- Unhealthy coping behaviors
Management implications:
- Enhanced surveillance: More frequent or earlier screening for high-risk conditions
- Risk-reducing interventions: Consider prophylactic surgery for highest-risk conditions
- Symptom awareness: Education about ovarian cancer symptoms for at-risk individuals
- Modifiable factor management: Address weight, inflammation, hormone exposure
- Genetic counseling: Recommend for conditions with genetic overlap
- Holistic approach: Coordinate care between specialists for complex conditions
6. Complications
What complications can arise from ovarian cancer?
Physical/anatomical complications:
Local disease complications:
- Ovarian torsion: Twisting of the ovary due to tumor mass, causing acute pain and vascular compromise
- Ovarian rupture: Spontaneous rupture causing acute abdominal pain and potential hemorrhage
- Tumor necrosis: Central death of tumor tissue causing pain and potential infection
- Local compression effects:
- Bladder compression causing urinary frequency or retention
- Rectal compression causing constipation or obstruction
- Ureteral compression leading to hydronephrosis
- Vascular compression causing lower extremity edema
- Direct invasion:
- Bowel perforation or fistula formation
- Bladder invasion
- Pelvic sidewall invasion with nerve involvement
Abdominal/peritoneal complications:
- Malignant ascites: Accumulation of fluid in the peritoneal cavity (present in 30-40% of cases)
- Causes abdominal distension, discomfort, early satiety
- Can lead to respiratory compromise when severe
- Risk of spontaneous bacterial peritonitis
- Peritoneal carcinomatosis: Widespread implantation throughout the peritoneal cavity
- Results in multiple adhesions and bowel dysfunction
- Can cause pain and malnutrition
- Bowel obstruction: Partial or complete blockage of intestines
- Occurs in 25-40% of advanced cases
- Can be mechanical (tumor mass) or functional (carcinomatosis)
- May require surgical intervention or stenting
- Significant cause of morbidity and mortality
- Portal hypertension: Due to liver metastases or portal vein compression
- Can cause variceal bleeding
- Contributes to ascites formation
Distant spread complications:
- Pleural effusion: Fluid accumulation in the pleural space
- Causes shortness of breath, cough, chest pain
- Present in 15-20% of advanced cases
- May require drainage procedures
- Lymphatic obstruction: Blockage of lymphatic drainage
- Results in lower extremity lymphedema
- May involve pelvic or para-aortic nodes
- Metastatic complications:
- Liver: Jaundice, right upper quadrant pain, hepatic failure
- Lung: Respiratory compromise, hemoptysis
- Brain: Neurological symptoms, intracranial pressure
- Bone: Pain, fractures, spinal cord compression
Systemic complications:
Hematological/metabolic:
- Anemia: Due to chronic disease, bleeding, or nutritional deficiency
- Present in 40-80% of patients
- Contributes to fatigue and reduced quality of life
- Thromboembolism: Increased clotting risk
- Deep vein thrombosis in 15-25% of patients
- Pulmonary embolism in 5-15%
- Arterial thrombosis in rare cases
- May be presenting feature (Trousseau syndrome)
- Hypercalcemia: Elevated calcium levels
- Occurs in 5-10% of cases
- Causes confusion, constipation, kidney problems
- Electrolyte abnormalities: Due to vomiting, diarrhea, or impaired intake
- Hypokalemia, hyponatremia, hypochloremia
- May cause cardiac arrhythmias and neurological symptoms
Paraneoplastic syndromes:
- Cushingoid syndrome: ACTH production by certain tumor types
- Hypercalcemia: PTH-related protein production
- Neurological syndromes:
- Cerebellar degeneration
- Limbic encephalitis
- Peripheral neuropathy
- Dermatomyositis/polymyositis: Inflammatory muscle disease
- Trousseau syndrome: Migratory thrombophlebitis
Treatment-related complications:
Surgical complications:
- Immediate postoperative:
- Bleeding requiring transfusion (10-15%)
- Infection (wound, abdominal, urinary) (5-10%)
- Thromboembolic events (2-5%)
- Gastrointestinal:
- Ileus (temporary bowel dysfunction) (15-20%)
- Anastomotic leak after bowel resection (1-3%)
- Fistula formation (1-2%)
- Genitourinary:
- Ureteral injury or fistula (1-2%)
- Bladder dysfunction (5-10%)
- Pelvic floor weakness
- Long-term surgical issues:
- Adhesions causing bowel obstruction
- Chronic incisional pain
- Hernia formation (8-12%)
- Lymphedema after lymph node dissection
Chemotherapy complications:
- Hematologic toxicity:
- Neutropenia and infection risk (30-40%)
- Anemia requiring transfusion (15-25%)
- Thrombocytopenia and bleeding risk (5-10%)
- Neurotoxicity:
- Peripheral neuropathy from taxanes and platinums (40-60%)
- Cognitive changes (“chemo brain”) (30-40%)
- Gastrointestinal:
- Nausea and vomiting (60-80%)
- Mucositis (10-20%)
- Diarrhea or constipation (30-50%)
- Other chemotherapy effects:
- Alopecia (hair loss) (80-90%)
- Fatigue (70-90%)
- Premature menopause in younger women
- Secondary malignancies (rare, 1-2%)
Targeted therapy complications:
- PARP inhibitors:
- Myelosuppression (30-50%)
- Fatigue (50-70%)
- Gastrointestinal symptoms (30-50%)
- Rare risk of myelodysplastic syndrome (<1%)
- Bevacizumab (anti-VEGF):
- Hypertension (20-30%)
- Proteinuria (10-20%)
- Wound healing complications (5-10%)
- Gastrointestinal perforation (2-3%)
- Arterial thromboembolism (2-3%)
Long-term impact on organs and overall health
Reproductive and hormonal systems:
Fertility and reproductive impacts:
- Complete loss of fertility: Due to bilateral oophorectomy
- Surgical menopause: Abrupt hormonal changes after oophorectomy in premenopausal women
- Hot flashes, night sweats (80-90%)
- Vaginal dryness and sexual dysfunction (50-70%)
- Sleep disturbances (40-60%)
- Mood changes (30-50%)
- Long-term hormonal consequences:
- Accelerated bone loss and osteoporosis risk
- Increased cardiovascular risk
- Cognitive changes
- Sexual function impacts
- Management challenges:
- Limited hormone replacement options
- Fertility preservation challenges
- Psychological impact of reproductive loss
Gastrointestinal system:
Short and long-term GI impacts:
- Altered bowel function: Due to surgical resection, adhesions, or nerve damage
- Chronic constipation (30-40%)
- Diarrhea or incomplete evacuation (20-30%)
- Alternating bowel patterns (25-35%)
- Nutritional challenges:
- Malabsorption after extensive bowel surgery
- Early satiety from altered anatomy
- Vitamin and mineral deficiencies
- Chronic symptoms:
- Abdominal pain (30-50%)
- Bloating (40-60%)
- Nausea (15-25%)
- Late complications:
- Adhesive small bowel obstruction (10-20% lifetime risk after surgery)
- Short bowel syndrome after extensive resection
- Chronic motility disorders
Urinary system:
Urinary tract impacts:
- Altered bladder function: Due to surgery, radiation, or nerve damage
- Urinary frequency (30-40%)
- Urgency or incontinence (20-30%)
- Incomplete emptying (15-25%)
- Kidney-related issues:
- Chronic kidney disease from obstructive uropathy
- Recurrent urinary tract infections
- Hydronephrosis from ureteral stricture or recurrent disease
- Long-term management:
- Need for urinary stents in some patients
- Potential for permanent urinary diversion
- Pelvic floor dysfunction requiring therapy
Neurological system:
Acute and chronic neurological impacts:
- Chemotherapy-induced peripheral neuropathy:
- Affects 30-70% of patients receiving taxane/platinum chemotherapy
- Persists beyond treatment in 30-40% of affected patients
- Symptoms include numbness, tingling, pain, and weakness
- Functional impact on fine motor skills and balance
- Cognitive changes:
- “Chemo brain” affecting memory and concentration
- Affects 30-40% during treatment, persisting in 10-20%
- Impact on work ability and quality of life
- Pain syndromes:
- Chronic pelvic pain (30-50%)
- Neuropathic pain (15-30%)
- Abdominal wall and incisional pain (10-20%)
- Psychological effects with neurobiological components:
- Anxiety
- Depression
- Post-traumatic stress disorder
- Sleep disturbances
Cardiovascular system:
Cardiac and vascular impacts:
- Treatment-related cardiac effects:
- Anthracycline-induced cardiomyopathy
- Targeted therapy cardiovascular effects
- Surgical menopause consequences:
- Accelerated atherosclerosis
- Increased risk of coronary artery disease
- Changes in lipid profile
- Vascular complications:
- Increased risk of hypertension
- Thromboembolic disease risk remains elevated
- Lymphatic dysfunction and lymphedema
- Long-term management:
- Cardiac surveillance needs
- Vascular risk factor management
- Lymphedema management
Skeletal system:
Bone health impacts:
- Accelerated bone loss:
- 5-10% bone density loss in first year after surgical menopause
- 2-fold increased fracture risk
- Vertebral compression fractures
- Contributors to bone loss:
- Estrogen deficiency from surgical menopause
- Nutritional deficiencies
- Reduced weight-bearing activity
- Platinum chemotherapy effects
- Long-term management:
- Bone density monitoring
- Calcium and vitamin D supplementation
- Bisphosphonates or other bone-directed therapy
- Physical therapy and exercise programs
Immunological system:
Immune function impacts:
- Cancer-related immune dysfunction
- Treatment effects on immunity:
- Sustained neutrophil and lymphocyte changes
- Altered T-cell function
- Impaired vaccine responses
- Susceptibility to infections:
- Higher rates of common infections
- Herpes zoster reactivation
- Opportunistic infections in some cases
- Autoimmune phenomena:
- Increased risk of autoimmune conditions
- Paraneoplastic autoimmune disorders
Psychological and social health:
- Psychosocial sequelae:
- Major depression (20-30%)
- Anxiety disorders (25-40%)
- Post-traumatic stress (15-25%)
- Body image disturbance
- Sexual dysfunction (40-60%)
- Social impacts:
- Relationship challenges
- Work and financial disruption
- Social role changes
- Caregiver burden
- Long-term management:
- Psychological support needs
- Sexual health interventions
- Social reintegration support
- Financial counseling
Potential disability or fatality rates
Mortality statistics:
Overall survival rates:
- 5-year relative survival (all stages combined): 49.1%
- Stage-specific 5-year survival:
- Stage I: 90-95%
- Stage II: 70-80%
- Stage III: 30-40%
- Stage IV: 15-20%
- 10-year relative survival: 35-40% overall
- Histology-specific survival (5-year rates):
- High-grade serous: 35-45%
- Low-grade serous: 70-80%
- Clear cell: 60-70% (stage-dependent)
- Endometrioid: 70-80%
- Mucinous: 60-70% (but poor if advanced stage)
Mortality patterns:
- Annual deaths globally: Approximately 207,000
- Mortality-to-incidence ratio: 0.67 (higher than most cancers)
- Median age at death: 71 years
- Years of life lost: Average 12-16 years per patient
- Trends: Mortality rates declining by 2% annually in developed countries
Cause-specific mortality:
- Disease progression: Primary cause in 70-80% of deaths
- Treatment complications: Account for 5-10% of deaths
- Thromboembolic events: 2-5% of deaths
- Infection/sepsis: 3-7% of deaths
- Other causes: 5-10% of deaths
Predictors of mortality:
- Disease factors:
- Stage at diagnosis (strongest predictor)
- Residual disease after surgery
- Histologic subtype and grade
- Platinum sensitivity/resistance
- Molecular features (BRCA status, homologous recombination deficiency)
- Patient factors:
- Age at diagnosis
- Performance status
- Comorbidities
- Nutritional status
- Socioeconomic factors
Disability and functional outcomes:
Physical disability:
- Performance status decline:
- 60-70% experience decline in functional status
- 30-40% require assistance with activities of daily living
- 15-25% become fully dependent in advanced disease
- Activity limitations:
- Mobility restrictions (50-70%)
- Lifting/carrying limitations (60-80%)
- Difficulty with stairs (40-60%)
- Driving limitations (30-50%)
- Symptom-related disability:
- Pain-related limitations (50-70%)
- Fatigue-induced disability (60-80%)
- Dyspnea-related restrictions (30-50% in advanced disease)
- Cognitive limitations (20-40%)
Work disability:
- Employment impact:
- 70-90% require some work absence during treatment
- 30-60% unable to return to previous employment
- 20-40% require disability benefits
- 10-30% permanent work disability
- Financial disability:
- Medical-related bankruptcy in 15-30% of cases
- Catastrophic health expenditures in 30-50%
- Lost income averaging $100,000-$200,000 per patient
- Career impact:
- Reduced work hours in 40-60%
- Career change necessity in 20-40%
- Early retirement in 15-30%
Long-term survivorship disability:
- Late effects causing disability:
- Chronic peripheral neuropathy (20-30%)
- Lymphedema (10-20%)
- Chronic pain syndromes (25-40%)
- Cognitive dysfunction (10-25%)
- Psychological sequelae (20-40%)
- Functional limitations in long-term survivors:
- Persistent fatigue (40-60%)
- Sexual dysfunction (50-70%)
- Sleep disorders (30-50%)
- Exercise intolerance (20-40%)
Quality of life impacts:
- Overall quality of life:
- Significant impairment in 50-70% during treatment
- Persistent moderate impairment in 30-50% of survivors
- Return to baseline in only 30-40% of survivors
- Domain-specific impacts:
- Physical wellbeing: Moderate-severe impact in 60-80%
- Emotional wellbeing: Moderate-severe impact in 50-70%
- Social functioning: Moderate-severe impact in 40-60%
- Role functioning: Moderate-severe impact in 50-70%
- Long-term impacts:
- Fear of recurrence affecting 60-80% of survivors
- Body image disturbance in 30-50%
- Sexual health impacts in 50-70%
- Existential concerns in 40-60%
Interventions affecting disability/mortality:
- Early detection: Stage shift can reduce mortality by 30-50%
- Surgical quality: Complete cytoreduction improves survival by 20-30%
- Maintenance therapy: PARP inhibitors reduce mortality by 30-70% in BRCA-mutated disease
- Rehabilitation interventions: Can reduce disability rates by 20-40%
- Survivorship care: Comprehensive programs improve functional outcomes by 15-30%
- Palliative integration: Early palliative care improves quality of life and may improve survival by 10-15%
7. Diagnosis & Testing
Common diagnostic procedures
Initial assessment:
Patient history and physical examination:
- Detailed symptom assessment: Nature, duration, progression of symptoms
- Risk factor evaluation: Family history, genetic risk, environmental exposures
- Physical examination components:
- Abdominal examination for masses or ascites
- Pelvic examination
- Lymph node assessment
- General health assessment
- Sensitivity/specificity: Pelvic exam alone has poor sensitivity (15-30%) but good specificity (85-90%)
Imaging studies:
Transvaginal ultrasound (TVUS):
- First-line imaging modality: Most accessible and cost-effective
- Features assessed:
- Ovarian size and volume
- Complex or solid components
- Presence of septations
- Papillary projections
- Bilateral involvement
- Ascites
- Doppler blood flow assessment
- Performance metrics:
- Sensitivity: 85-95%
- Specificity: 70-85%
- Positive predictive value: 60-75%
- Negative predictive value: 90-95%
- Risk stratification systems:
- International Ovarian Tumor Analysis (IOTA) simple rules
- Risk of Malignancy Index (RMI)
- ADNEX model (Assessment of Different NEoplasias in the adneXa)
Computed tomography (CT):
- Primary role: Staging once cancer is suspected or confirmed
- CT protocol: Contrast-enhanced of chest, abdomen, and pelvis
- Features assessed:
- Disease extent
- Metastatic spread
- Lymph node involvement
- Peritoneal implants
- Ascites volume
- Planning for potential surgery
- Performance metrics:
- Sensitivity for advanced disease: 85-95%
- Specificity: 85-90%
- Less sensitive for small peritoneal implants
Magnetic resonance imaging (MRI):
- Primary role: Characterization of indeterminate adnexal masses
- MRI protocol: T1, T2, diffusion-weighted imaging, dynamic contrast enhancement
- Features assessed:
- Tissue characterization (fat, blood, solid components)
- Complex internal architecture
- Invasion of adjacent structures
- Differentiation of benign from malignant features
- Performance metrics:
- Sensitivity: 80-90%
- Specificity: 85-95%
- Superior to CT for local disease extent
- Particularly useful for young women (avoids radiation)
Positron emission tomography/CT (PET/CT):
- Primary role: Detection of metastatic disease and recurrence
- Features assessed:
- Metabolic activity of primary and metastatic lesions
- Response to therapy
- Recurrent disease detection
- Performance metrics:
- Sensitivity for recurrence: 85-95%
- Specificity: 80-90%
- Limited use in initial diagnosis
- False positives with inflammatory conditions
Laboratory studies:
Serum tumor markers:
- CA-125:
- Primary ovarian cancer biomarker
- Elevated in 80% of epithelial ovarian cancers overall
- Elevated in only 50% of early-stage disease
- Higher sensitivity for serous subtype (90%)
- Lower sensitivity for mucinous subtype (50%)
- False positives with:
- Endometriosis
- Fibroids
- Pelvic inflammatory disease
- Menstruation
- Pregnancy
- Liver disease
- Heart failure
- HE4 (Human Epididymis Protein 4):
- Complementary to CA-125
- Fewer false positives with benign gynecologic conditions
- Sensitivity: 70-80%
- Specificity: 80-90%
- Risk of Malignancy Algorithm (ROMA):
- Combines CA-125, HE4, and menopausal status
- Sensitivity: 85-95%
- Specificity: 75-85%
- Other markers:
- CEA: Elevated in mucinous subtype
- AFP and hCG: For germ cell tumors
- Inhibin: For granulosa cell tumors
- LDH: For some ovarian tumors and advanced disease
Complete blood count and comprehensive metabolic panel:
- Anemia: Present in 30-40% of patients
- Thrombocytosis: Seen in 25-30% of cases
- Leukocytosis: May indicate infection or paraneoplastic effect
- Liver function abnormalities: With liver involvement or paraneoplastic effect
- Electrolyte disturbances: Due to vomiting or poor intake
- Albuminemia: May be low with advanced disease
Medical tests (e.g., blood tests, imaging, biopsies)
Pathological assessment:
Cytological examination:
- Ascitic fluid cytology:
- Obtained via paracentesis
- Sensitivity: 60-70%
- Specificity: 95-100%
- Can establish diagnosis in advanced disease
- Limitations in cell block preparation can improve yield
- Pleural fluid cytology:
- For cases with pleural effusion
- Sensitivity: 70-80%
- Can establish metastatic spread
- Peritoneal washing cytology:
- Obtained during surgery
- Important for staging
- Positive cytology upgrades to stage IC (if confined to ovary)
Tissue sampling and biopsy:
- Image-guided biopsy:
- Core needle biopsy of omental cake or peritoneal masses
- CT or ultrasound guidance
- Sensitivity: 80-90%
- Complication rate: 1-3%
- Not routinely recommended for ovarian masses due to risk of spread
- Laparoscopic biopsy:
- Minimally invasive surgical approach
- Direct visualization with targeted sampling
- Sensitivity: 90-95%
- Allows assessment of disease extent
- Risk of port-site metastases: 1-2%
- Surgical pathology:
- Definitive diagnosis typically from surgical specimens
- Intraoperative frozen section:
- Sensitivity: 85-95%
- Specificity: 95-99%
- Guides surgical decision-making
- Final pathology with comprehensive assessment:
- Histologic type and grade
- Immunohistochemistry
- Staging information
Pathology assessment components:
- Gross examination: Size, appearance, capsular integrity
- Histologic evaluation:
- Tumor type classification
- Architectural patterns
- Cellular features
- Mitotic activity
- Necrosis
- Invasion assessment
- Immunohistochemistry panels:
- PAX8: Positive in müllerian-derived tumors
- WT1: Positive in serous carcinomas
- p53: Different patterns in high-grade vs. low-grade serous
- Napsin A and HNF1β: Clear cell markers
- ARID1A: Loss in clear cell and endometrioid types
- MMR proteins: For Lynch syndrome screening
- Hormone receptors (ER/PR): Variable expression
- Molecular testing:
- BRCA1/2 testing
- Homologous recombination deficiency (HRD)
- Microsatellite instability (MSI)
- Next-generation sequencing panels
Advanced diagnostic techniques:
Genetic testing:
- Germline genetic testing:
- Recommended for all epithelial ovarian cancer patients
- Tests for:
- BRCA1/2 mutations
- Lynch syndrome genes
- Other homologous recombination genes
- Methods:
- Multi-gene panel testing
- Sequential testing (starting with BRCA1/2)
- Point-of-care rapid testing
- Impact:
- Treatment selection (PARP inhibitors)
- Family risk assessment
- Prevention strategies
- Somatic tumor testing:
- BRCA1/2 mutations in tumor tissue
- Homologous recombination deficiency (HRD) testing
- Comprehensive genomic profiling
- Tumor mutational burden
Circulating tumor DNA (ctDNA):
- Applications:
- Detection of minimal residual disease
- Monitoring for recurrence
- Identification of resistance mutations
- Tumor heterogeneity assessment
- Performance metrics:
- Sensitivity varies by disease burden and assay (40-90%)
- Specificity: 90-95%
- Emerging technology, not yet standard of care
Functional imaging:
- Diffusion-weighted MRI:
- Assesses tissue cellularity
- Helps distinguish benign from malignant lesions
- Sensitivity: 85-95%
- Specificity: 80-90%
- Dynamic contrast-enhanced MRI:
- Evaluates tumor vascularity
- Enhancement patterns help characterize masses
- Sensitivity: 80-90%
- Specificity: 75-85%
- Emerging techniques:
- Radiomics (texture analysis)
- Artificial intelligence-based image analysis
- Multi-parametric MRI protocols
Staging procedures:
Surgical staging:
- Comprehensive surgical staging includes:
- Total hysterectomy and bilateral salpingo-oophorectomy
- Omentectomy
- Peritoneal biopsies from multiple sites
- Pelvic and para-aortic lymph node dissection
- Peritoneal washings
- Assessment of all peritoneal surfaces
- Appendectomy (particularly for mucinous histology)
- Minimally invasive approaches:
- Laparoscopic or robotic staging for apparent early disease
- Conversion to open surgery if advanced disease found
Non-surgical staging:
- CT-based staging: Primary non-invasive approach
- PET/CT: Particularly for lymph node assessment
- Diagnostic laparoscopy: For assessment of resectability
- Serum biomarkers: Supporting role in monitoring
Early detection methods and their effectiveness
Screening approaches and efficacy:
CA-125 blood test:
- Sensitivity for early-stage disease: 50-60%
- Specificity: 95-98% in postmenopausal women, 70-80% in premenopausal women
- Positive predictive value in general population: Very low (0.1-0.5%)
- Limitations:
- Misses 40-50% of early-stage cancers
- Many false positives in premenopausal women
- Not recommended as isolated screening test
- Evidence from trials:
- PLCO trial: No mortality reduction with CA-125 alone
- UK FOCSS: CA-125 with TVS detected earlier stage disease in high-risk women
Transvaginal ultrasound (TVS):
- Sensitivity for early-stage disease: 75-85%
- Specificity: 85-95% (experienced operators)
- Positive predictive value in general population: 1-2%
- Limitations:
- Operator-dependent
- Limited specificity for small complex masses
- High cost for population screening
- Evidence from trials:
- Kentucky Screening Study: Shift to earlier stage disease but no proven mortality benefit
- UKCTOCS: No significant mortality reduction overall
Multimodal screening approaches:
- Risk of Ovarian Cancer Algorithm (ROCA):
- Uses serial CA-125 measurements
- Detects patterns of change rather than absolute values
- Sensitivity: 85-90% (for all stages)
- Specificity: 99.8%
- Combination ROCA + TVS:
- Two-stage screening approach
- ROCA triggers TVS when indicated
- Reduces unnecessary ultrasounds
- Stage shift demonstrated in UKCTOCS
- Mortality benefit still uncertain (11% reduction did not reach statistical significance)
Emerging screening technologies:
- Multi-marker panels:
- OVA1, ROMA, OvaSure
- Sensitivity: 80-90%
- Specificity: 75-85%
- Not yet validated for screening
- Circulating tumor DNA:
- Emerging technology
- Potential for early detection
- Current sensitivity limitations for early disease
- Exosome-based tests:
- Tumor-derived exosomes as biomarkers
- Early research phase
- Cell-free DNA methylation patterns:
- Cancer-specific methylation signatures
- Promising early results
- Large validation studies pending
Effectiveness in different populations:
General population screening:
- Not currently recommended
- Numbers needed to screen: ~5,000 women to prevent one death
- Harms: Anxiety, unnecessary surgeries, complications
- Cost-effectiveness: Not demonstrated
- Current position statements:
- US Preventive Services Task Force: “D” recommendation (recommends against)
- American College of Obstetricians and Gynecologists: Not recommended
- National Comprehensive Cancer Network: Not recommended
- Society of Gynecologic Oncology: Not recommended
High-risk population screening:
- BRCA1 mutation carriers:
- Lifetime risk: 35-70%
- Screening recommended from age 30-35
- CA-125 every 6 months
- TVS every 6 months
- Sensitivity: 60-80%
- Risk-reducing surgery preferred when childbearing complete
- BRCA2 mutation carriers:
- Lifetime risk: 10-30%
- Screening recommended from age 30-35
- Similar protocol to BRCA1 carriers
- Somewhat better screening performance
- Lynch syndrome:
- Lifetime risk: 8-12%
- Screening recommended from age 30-35
- Endometrial sampling also recommended
- Consider risk-reducing surgery after childbearing
Symptomatic women detection:
- Symptom index tools:
- Goff Symptom Index
- Sensitivity: 65-85%
- Specificity: 85-90%
- Particularly effective for women >50 years
- Two-week wait referral pathways:
- Expedited evaluation for suspicious symptoms
- Improves early detection by 10-20%
- Cost-effective approach
- CA-125 in primary care:
- NICE guidelines recommend for persistent symptoms
- Threshold of 35 U/mL
- Reduces diagnostic delay by 2-3 months
- PPV in symptomatic women: 10-15%
Surveillance in special populations:
- Previous ovarian cancer:
- CA-125 every 3 months for 2 years, then every 6 months
- Imaging as clinically indicated
- Detects 50-70% of recurrences before symptoms
- Endometriosis patients:
- No specialized screening validated
- Heightened awareness of changing symptoms
- Consider annual TVS
- BRCA carriers who defer risk-reducing surgery:
- CA-125 every 3-6 months
- TVS every 6 months
- MRI may have added benefit
- Limited evidence for mortality benefit
8. Treatment Options
Standard treatment protocols
Treatment by stage:
Stage I (confined to ovaries):
- Surgery:
- Comprehensive surgical staging
- Total hysterectomy and bilateral salpingo-oophorectomy
- Omentectomy
- Peritoneal biopsies
- Pelvic and para-aortic lymph node assessment
- Peritoneal washings
- Fertility-sparing surgery may be considered in select cases
- Adjuvant chemotherapy:
- Stage IA, IB, grade 1-2: Observation (no chemotherapy)
- Stage IA, IB, grade 3: 3-6 cycles of platinum-based chemotherapy
- Stage IC: 6 cycles of platinum-based chemotherapy
- Surveillance:
- Physical exam every 3-6 months for 2 years, then every 6 months
- CA-125 at each visit if initially elevated
- Imaging as clinically indicated
Stage II (pelvic extension):
- Surgery:
- Comprehensive staging/debulking surgery
- Hysterectomy and bilateral salpingo-oophorectomy
- Omentectomy
- Removal of all visible disease when possible
- Complete lymph node dissection
- Adjuvant chemotherapy:
- 6 cycles of platinum-based chemotherapy (carboplatin/paclitaxel)
- Intraperitoneal chemotherapy may be considered
- Maintenance therapy:
- Consider PARP inhibitors for BRCA-mutated or HRD-positive disease
- Surveillance:
- Physical exam every 3 months for 2 years, then every 6 months
- CA-125 at each visit if initially elevated
- Imaging as clinically indicated
Stage III (abdominal/lymph node spread):
- Primary approach:
- Primary debulking surgery followed by chemotherapy when complete cytoreduction is feasible
- Neoadjuvant chemotherapy followed by interval debulking for bulky disease or poor surgical candidates
- Surgery:
- Radical debulking with goal of complete resection (no visible residual disease)
- May include:
- Bowel resection
- Splenectomy
- Diaphragm stripping/resection
- Extensive peritonectomy
- Chemotherapy:
- 6 cycles of intravenous carboplatin/paclitaxel
- Intraperitoneal chemotherapy for optimally debulked patients
- Dose-dense weekly paclitaxel regimens
- Targeted therapy:
- Bevacizumab may be added for high-risk features
- PARP inhibitor maintenance for:
- BRCA-mutated tumors
- HRD-positive tumors
- All responders to platinum therapy (depending on country/guidelines)
- Surveillance:
- Physical exam every 3 months for 2 years, then every 4-6 months
- CA-125 at each visit
- Imaging as clinically indicated
Stage IV (distant metastases):
- Individualized approach:
- Primary surgery for good performance status and limited metastatic disease
- Neoadjuvant chemotherapy more commonly employed
- Surgery:
- Debulking considered if complete or near-complete resection possible
- Palliative procedures for symptom control
- Systemic therapy:
- 6 cycles of platinum-based chemotherapy
- Bevacizumab commonly added
- PARP inhibitor maintenance for eligible patients
- Management of specific metastases:
- Pleural procedures for effusions
- Brain metastases: Surgery, radiation, or systemic therapy
- Liver metastases: Consider resection of isolated lesions
- Surveillance and supportive care:
- Similar to stage III
- Early integration of palliative care
- Symptom management emphasis
Recurrent disease management:
Platinum-sensitive recurrence (>6 months):
- Surgical options:
- Secondary cytoreductive surgery for selected patients
- Selection criteria: Limited sites of disease, complete resection likely
- Chemotherapy:
- Platinum-based combination therapy
- Options include:
- Carboplatin/paclitaxel
- Carboplatin/gemcitabine
- Carboplatin/pegylated liposomal doxorubicin
- Targeted therapy:
- PARP inhibitor maintenance therapy
- Bevacizumab may be added to chemotherapy
- Duration:
- Typically 6 cycles of chemotherapy
- Maintenance until progression or toxicity
Platinum-resistant recurrence (<6 months):
- Single-agent chemotherapy:
- Pegylated liposomal doxorubicin
- Weekly paclitaxel
- Gemcitabine
- Topotecan
- Etoposide
- Targeted approaches:
- Bevacizumab plus chemotherapy
- Clinical trials with novel agents
- Immunotherapy:
- Pembrolizumab for MSI-high/dMMR tumors
- Dostarlimab for MSI-high/dMMR tumors
- Goals of care:
- Symptom control
- Quality of life focus
- Palliative care integration
Special populations:
Elderly patients (>70 years):
- Surgical considerations:
- Comprehensive geriatric assessment before surgery
- Consider minimally invasive approaches
- Balance extent of surgery with recovery impact
- Chemotherapy adaptations:
- Carboplatin monotherapy option
- Weekly paclitaxel to reduce toxicity
- Dose adjustments based on organ function
- Growth factor support more liberally used
- Supportive care emphasis:
- Medication interactions
- Nutritional support
- Rehabilitation services
- Caregiver support
Young women with fertility desire:
- Fertility-sparing surgery:
- Unilateral salpingo-oophorectomy
- Comprehensive staging otherwise
- Limited to stage IA-IC with favorable histologies
- Not suitable for high-grade serous carcinoma
- Fertility preservation:
- Oocyte or embryo cryopreservation before treatment
- Ovarian tissue cryopreservation in select cases
- Surveillance:
- More intensive monitoring
- Completion surgery after childbearing
BRCA mutation carriers:
- Surgical considerations:
- Same surgical principles as non-carriers
- Discussion of risk-reducing surgery for contralateral breast cancer risk
- Targeted therapy:
- PARP inhibitors particularly effective
- Higher response rates to platinum chemotherapy
- Longer duration of benefit from maintenance therapy
- Cascade testing:
- Genetic counseling for family members
- Risk-reducing strategies for carriers
Medications, surgeries, and therapies
Chemotherapy agents:
Platinum compounds:
- Carboplatin:
- Cornerstone of ovarian cancer treatment
- Mechanism: DNA cross-linking agent
- Dosing: AUC 5-6, every 3 weeks
- Efficacy: Response rates 60-80% first-line
- Toxicities:
- Myelosuppression (especially thrombocytopenia)
- Nausea/vomiting
- Peripheral neuropathy
- Hypersensitivity reactions (10-15%)
- Renal toxicity (less than cisplatin)
- Cisplatin:
- Used less commonly than carboplatin
- Higher toxicity profile
- Used for intraperitoneal administration
- More severe nephrotoxicity and neurotoxicity
- May be used for platinum-resistant disease
Taxanes:
- Paclitaxel:
- Standard in combination with platinum
- Mechanism: Microtubule stabilizer
- Dosing options:
- Conventional: 175 mg/m², every 3 weeks
- Dose-dense: 80 mg/m², weekly
- Toxicities:
- Peripheral neuropathy (dose-limiting)
- Myelosuppression
- Hypersensitivity reactions
- Alopecia
- Myalgia/arthralgia
- Docetaxel:
- Alternative to paclitaxel
- Similar efficacy
- Different toxicity profile:
- Less neuropathy
- More bone marrow suppression
- Fluid retention
Other cytotoxic agents:
- Pegylated liposomal doxorubicin (PLD):
- Preferred for platinum-resistant disease
- Mechanism: DNA intercalation, topoisomerase II inhibition
- Dosing: 40-50 mg/m², every 4 weeks
- Toxicities:
- Palmar-plantar erythrodysesthesia
- Stomatitis
- Less cardiotoxicity than conventional doxorubicin
- Less alopecia and nausea
- Gemcitabine:
- Used for platinum-resistant disease
- Also in combination with carboplatin
- Mechanism: Nucleoside analog
- Toxicities:
- Myelosuppression
- Flu-like symptoms
- Rash
- Rarely pulmonary toxicity
- Topotecan:
- Option for recurrent disease
- Mechanism: Topoisomerase I inhibitor
- Toxicities:
- Myelosuppression (severe)
- Fatigue
- Diarrhea
- Etoposide:
- Oral option for recurrent disease
- Mechanism: Topoisomerase II inhibitor
- Toxicities:
- Myelosuppression
- Nausea
- Alopecia
Targeted therapies:
Anti-angiogenic agents:
- Bevacizumab:
- Monoclonal antibody targeting VEGF
- Approved in front-line, maintenance, and recurrent settings
- Dosing: 15 mg/kg every 3 weeks
- Efficacy: Improves progression-free survival by 3-6 months
- Toxicities:
- Hypertension (30-40%)
- Proteinuria (10-20%)
- Arterial thromboembolic events (2-3%)
- Bowel perforation (1-2%)
- Impaired wound healing
- Rare posterior reversible encephalopathy
PARP inhibitors:
- Olaparib:
- First-in-class PARP inhibitor
- Approved for:
- Maintenance after response to platinum
- Treatment of BRCA-mutated recurrent disease
- Dosing: 300 mg tablet twice daily
- Efficacy:
- BRCA-mutated: Hazard ratio 0.30
- HRD-positive: Hazard ratio 0.43
- All-comers: Hazard ratio 0.53
- Toxicities:
- Fatigue (50-70%)
- Nausea (70-80%)
- Anemia (40-50%)
- Neutropenia (20-30%)
- Rare MDS/AML (<1.5%)
- Niraparib:
- Once-daily PARP inhibitor
- Approved for maintenance therapy
- Dosing: 200-300 mg daily (weight-based)
- Toxicities:
- Thrombocytopenia (distinctive)
- Hypertension
- Similar to other PARP inhibitors otherwise
- Rucaparib:
- PARP inhibitor with additional activity
- Approved for treatment and maintenance
- Dosing: 600 mg twice daily
- Toxicities:
- Transaminitis (distinctive)
- Similar to other PARP inhibitors
Immunotherapy:
- Pembrolizumab:
- Anti-PD-1 monoclonal antibody
- Approved for MSI-high/dMMR tumors
- Dosing: 200 mg every 3 weeks
- Response rate: 30-40% in eligible patients
- Toxicities:
- Autoimmune phenomena
- Fatigue
- Rash
- Colitis
- Pneumonitis
- Endocrinopathies
- Dostarlimab:
- Anti-PD-1 monoclonal antibody
- Approved for MSI-high/dMMR tumors
- Similar efficacy and toxicity to pembrolizumab
Surgical approaches:
Initial surgical management:
- Comprehensive staging/debulking:
- Vertical midline incision
- Exploration of entire abdomen
- Peritoneal washings
- Hysterectomy and bilateral salpingo-oophorectomy
- Omentectomy
- Pelvic and para-aortic lymphadenectomy
- Peritoneal biopsies from multiple sites
- Resection of all visible disease when possible
- Minimally invasive surgery:
- Appropriate for:
- Apparent early-stage disease
- Diagnostic purposes
- Secondary look procedures
- Approaches:
- Laparoscopic
- Robotic-assisted
- Limitations:
- Tactile feedback reduced
- Complex resections challenging
- Tumor spillage risk
- Appropriate for:
- Fertility-sparing surgery:
- Unilateral salpingo-oophorectomy
- Preservation of uterus and contralateral ovary
- Appropriate for:
- Stage IA-IC, grade 1-2
- Non-epithelial ovarian cancers
- Select early epithelial cancers
Surgical techniques for advanced disease:
- Upper abdominal procedures:
- Diaphragm peritonectomy/resection
- Splenectomy
- Distal pancreatectomy
- Liver resection
- Partial gastrectomy
- Pelvic procedures:
- Radical hysterectomy
- Rectosigmoid resection
- Pelvic peritonectomy
- Bladder resection (rare)
- Extensive peritoneal disease management:
- Peritoneal stripping
- Greater omentectomy
- Small bowel assessment and resection if needed
- Management of mesenteric involvement
Secondary surgical procedures:
- Secondary cytoreduction:
- For platinum-sensitive recurrent disease
- Patient selection criteria:
- Good performance status
- Long treatment-free interval (>12 months)
- Limited sites of recurrence
- Complete resection likely
- Improves survival in selected patients
- Palliative procedures:
- Bowel diversion for obstruction
- Feeding tube placement
- Paracentesis for malignant ascites
Other therapeutic modalities:
Radiation therapy:
- Limited role in modern management
- Palliative applications:
- Bone metastases
- Brain metastases
- Localized recurrence causing symptoms
- Whole abdominal radiation:
- Historical approach
- Rarely used due to toxicity and limited benefit
- Intensity-modulated techniques:
- For selected recurrences
- Reduced toxicity compared to older approaches
Intraperitoneal therapy:
- Intraperitoneal (IP) chemotherapy:
- Direct instillation of chemotherapy into peritoneal cavity
- Achieves high local drug concentrations
- Combined with intravenous therapy
- Efficacy: Improved survival by 16 months in GOG 172
- Toxicities:
- Catheter-related complications
- Abdominal pain
- Increased systemic toxicity
- Utilization limited by toxicity and technical challenges
- Hyperthermic intraperitoneal chemotherapy (HIPEC):
- Chemotherapy heated to 41-43°C and circulated in peritoneal cavity during surgery
- Mechanism: Heat enhances cytotoxicity and penetration
- Evidence: Improved survival in selected patients (van Driel trial)
- Most effective for:
- Primary advanced disease with complete cytoreduction
- Selected recurrent disease
- Toxicities:
- Increased surgical morbidity
- Renal impairment
- Bone marrow suppression
- Not universally adopted, ongoing debate about optimal patient selection
Hormonal therapy:
- Limited role in most ovarian cancers
- Low-grade serous carcinoma:
- Aromatase inhibitors (letrozole)
- Response rates: 10-15%
- Disease stabilization: 40-50%
- Minimal side effects
- Endometrioid ovarian cancer:
- May respond to hormonal approaches
- Tamoxifen, aromatase inhibitors
- Response correlates with hormone receptor status
- Granulosa cell tumors:
- Estrogen-producing tumors
- Aromatase inhibitors
- GnRH agonists
Supportive and palliative therapies:
- Ascites management:
- Therapeutic paracentesis
- Diuretics (spironolactone, furosemide)
- Intraperitoneal catheters for recurrent ascites
- Peritoneovenous shunts (rarely used)
- Bowel obstruction approaches:
- Conservative management (decompression, fluids)
- Pharmacological (octreotide, antimotility agents)
- Surgical intervention when appropriate
- Stenting procedures
- Pain management:
- Multimodal approach
- Opioid and non-opioid analgesics
- Nerve blocks for localized pain
- Integrative approaches (acupuncture, massage)
- Nutritional support:
- Oral nutritional supplements
- Enteral feeding when appropriate
- Parenteral nutrition in selected cases
- Dietary counseling
Emerging treatments and clinical trials
Novel targeted therapies:
Antibody-drug conjugates (ADCs):
- Mirvetuximab soravtansine:
- Targets folate receptor alpha
- Conjugated to maytansinoid DM4
- Phase III FORWARD I trial: Mixed results but activity in high FR-α expressors
- SORAYA trial: 32% response rate in platinum-resistant disease
- FDA breakthrough designation
- Side effects: Vision changes, neuropathy, fatigue
- Tisotumab vedotin:
- Targets tissue factor
- Early trials show activity in ovarian cancer
- Side effects: Neuropathy, ocular toxicity, bleeding
- Sacituzumab govitecan:
- Targets Trop-2
- Activity in triple-negative breast cancer
- Ongoing trials in ovarian cancer
- Side effects: Neutropenia, diarrhea, nausea
Cell cycle inhibitors:
- WEE1 inhibitors (adavosertib):
- Synthetic lethality with p53 mutations
- Preliminary activity in combination with chemotherapy
- Phase II trials ongoing
- Side effects: Myelosuppression, fatigue, diarrhea
- Cyclin-dependent kinase (CDK) inhibitors:
- CDK4/6 inhibitors (palbociclib, ribociclib)
- Most effective in low-grade serous carcinoma
- Side effects: Neutropenia, fatigue
- Aurora kinase inhibitors:
- Target mitotic process
- Early clinical development
- Side effects: Myelosuppression, GI toxicity
Novel DNA damage response inhibitors:
- ATR inhibitors:
- Synthetic lethality with ATM loss or BRCA mutations
- Examples: Ceralasertib, berzosertib
- Phase II trials in combination with chemotherapy
- Side effects: Myelosuppression, fatigue
- CHK1 inhibitors:
- Target checkpoint kinase
- Synergy with chemotherapy
- Side effects: Myelosuppression, GI toxicity
- Next-generation PARP inhibitors:
- Enhanced trapping activity
- Potential to overcome resistance
- Examples: Talazoparib, improved formulations
Immunotherapy approaches:
Checkpoint inhibitors:
- PD-1/PD-L1 inhibitors:
- Limited single-agent activity (10-15% response rate)
- Combination strategies:
- With PARP inhibitors
- With anti-angiogenic agents
- With chemotherapy
- Most effective in:
- Clear cell carcinoma
- MSI-high tumors
- BRCA-mutated tumors
- Key trials:
- KEYNOTE-100: Pembrolizumab monotherapy
- JAVELIN: Avelumab combinations
- IMAGINE: Dostarlimab combinations
- CTLA-4 inhibitors:
- Combination with PD-1/PD-L1 inhibitors
- Higher toxicity profile
- Trials ongoing in platinum-resistant disease
Adoptive cell therapy:
- Tumor-infiltrating lymphocytes (TILs):
- Extraction, expansion, and reinfusion of tumor-reactive T cells
- Early phase trials show promising activity
- Side effects: Cytokine release syndrome, neurotoxicity
- CAR-T cell therapy:
- Engineered T cells targeting ovarian cancer antigens
- Targets include:
- MUC16 (CA-125)
- Mesothelin
- FR-α
- Challenges:
- Identifying optimal target
- Solid tumor penetration
- Persistence of response
- Early-phase trials ongoing
Tumor microenvironment modulation:
- Anti-TGF-β approaches:
- Reduces immunosuppression in tumor environment
- Combination with checkpoint inhibitors
- Early clinical development
- Macrophage-directed therapy:
- CSF1R inhibitors
- Reprogramming tumor-associated macrophages
- Phase I/II trials in combination with standard therapy
- Adenosine pathway inhibitors:
- Target immunosuppressive adenosine signaling
- A2A receptor antagonists
- CD73 inhibitors
- Combinations with checkpoint inhibitors
Additional innovative approaches:
Epigenetic therapies:
- DNA methyltransferase inhibitors:
- Azacitidine, decitabine
- Potential to reverse platinum resistance
- Combination with chemotherapy or PARP inhibitors
- Side effects: Myelosuppression, fatigue
- Histone deacetylase inhibitors:
- Vorinostat, belinostat
- Activity in combination with chemotherapy
- Side effects: Fatigue, GI toxicity, QTc prolongation
- BET inhibitors:
- Target bromodomain proteins
- Preclinical activity in ovarian cancer models
- Early phase trials ongoing
Metabolic therapies:
- Glutaminase inhibitors:
- Target cancer cell metabolism
- CB-839 (telaglenastat) in clinical trials
- Side effects: Fatigue, nausea
- Metformin:
- Repurposed diabetes medication
- Potential synergy with standard therapies
- Multiple mechanisms:
- AMPK activation
- mTOR inhibition
- Reduced insulin signaling
- Several clinical trials ongoing
- IDO inhibitors:
- Target immunosuppressive tryptophan metabolism
- Combination with checkpoint inhibitors
- Mixed results in trials to date
Novel delivery systems:
- Nanoparticle formulations:
- Enhanced drug delivery
- Reduced systemic toxicity
- Examples:
- Nanoparticle albumin-bound paclitaxel
- Liposomal formulations
- Intraperitoneal drug-eluting implants:
- Sustained local drug delivery
- Bypass peritoneal-plasma barrier
- Early clinical development
- Tumor-targeted drug conjugates:
- Beyond antibody-drug conjugates
- Small molecule-drug conjugates
- Peptide-drug conjugates
- Enhanced tumor specificity
9. Prevention & Precautionary Measures
How can ovarian cancer be prevented?
Risk-reducing surgical interventions:
Risk-reducing salpingo-oophorectomy (RRSO):
- Procedure: Surgical removal of fallopian tubes and ovaries
- Effectiveness:
- BRCA1 mutation carriers: 80-90% risk reduction
- BRCA2 mutation carriers: 65-75% risk reduction
- Lynch syndrome: 60-80% risk reduction
- Timing recommendations:
- BRCA1 carriers: Age 35-40 or after childbearing
- BRCA2 carriers: Age 40-45 or after childbearing
- Lynch syndrome: Age 40-45 or after childbearing
- Additional benefits:
- 50% breast cancer risk reduction in BRCA carriers
- Endometrial cancer risk reduction in Lynch syndrome
- Drawbacks:
- Surgical menopause and associated symptoms
- Potential cognitive, cardiovascular, bone health impacts
- Psychological impact of fertility loss
- Management after RRSO:
- Hormone replacement until natural menopause age (age 50-51)
- Bone health monitoring
- Cardiovascular risk management
Opportunistic salpingectomy:
- Procedure: Removal of fallopian tubes during pelvic surgery for benign conditions
- Target population: Women undergoing:
- Hysterectomy for benign indications
- Tubal sterilization
- Other pelvic surgeries
- Effectiveness: Estimated 30-50% risk reduction
- Rationale:
- Many high-grade serous carcinomas originate in fallopian tubes
- Preserves ovarian function while reducing cancer risk
- Minimal additional surgical risk
- Implementation:
- Increasingly standard practice
- “Two-step” approach option: salpingectomy with delayed oophorectomy
- Patient counseling about risks and benefits essential
Risk-reducing hysterectomy:
- Most beneficial for:
- Lynch syndrome carriers (reduces endometrial and ovarian cancer risk)
- Women with BRCA mutations undergoing RRSO
- Considerations:
- More extensive surgery than RRSO alone
- Longer recovery time
- Additional surgical risks
- Definitive end to fertility
Pharmacological prevention:
Hormonal contraceptives:
- Effectiveness:
- 30-50% risk reduction with 5+ years of use
- Risk reduction persists for decades after discontinuation
- Protection increases with duration of use
- Mechanism:
- Suppression of ovulation
- Reduced gonadotropin levels
- Altered fallopian tube environment
- Options:
- Combined oral contraceptives
- Contraceptive patch
- Vaginal ring
- Progestin-only options (less evidence for protection)
- Considerations:
- Potential increased breast cancer risk
- Thromboembolism risk in susceptible individuals
- Reduced efficacy in BRCA1 carriers (but still beneficial)
- Most appropriate for women at average or moderate risk
Aspirin and NSAIDs:
- Effectiveness:
- 10-20% risk reduction with regular use
- Optimal dose and duration not established
- Mechanism:
- Anti-inflammatory effects
- COX-2 inhibition
- Reduced prostaglandin production
- Evidence quality:
- Primarily observational studies
- Limited randomized trial data
- Consistent modest protective effect
- Considerations:
- Gastrointestinal and bleeding risks
- Not recommended solely for ovarian cancer prevention
- May be considered in context of other health benefits
Other medications with potential benefit:
- Metformin:
- Observational data suggests possible risk reduction
- Mechanism may involve insulin pathway modulation
- Clinical trials ongoing
- Statins:
- Some evidence for modest risk reduction
- Anti-inflammatory properties may contribute
- Inconsistent results across studies
- Acetaminophen (paracetamol):
- Limited evidence for protective effect
- Different mechanism than NSAIDs
- Insufficient data for recommendations
Preventive measures for average-risk women:
Reproductive and hormonal factors:
- Pregnancy and childbearing:
- Each full-term pregnancy reduces risk by approximately 10%
- Earlier age at first birth provides greater protection
- Breastfeeding:
- 2-4% risk reduction per month of breastfeeding
- Cumulative benefit with longer duration
- Mechanism involves suppression of ovulation
- Avoiding late menopause induction:
- Limiting extended hormone replacement therapy
- Particularly estrogen-only HRT
Lifestyle modifications:
- Maintaining healthy weight:
- Obesity increases risk by 30-70%
- Weight loss may reduce risk in obese women
- Avoiding adult weight gain important
- Regular physical activity:
- 20-30% risk reduction with regular moderate exercise
- 3-4 hours per week of moderate activity recommended
- Lifetime activity patterns most important
- Dietary factors:
- Low-fat diet may provide modest benefit
- Higher vegetable consumption (especially cruciferous)
- Limited evidence for specific dietary interventions
- Avoiding known carcinogens:
- Limiting talc use in genital area (controversial)
- Reducing exposure to endocrine-disrupting chemicals
- Avoiding excessive alcohol consumption
Screening and surveillance for high-risk women:
- BRCA1/2 carriers:
- Transvaginal ultrasound every 6 months
- CA-125 blood test every 6 months
- Limited evidence for mortality benefit
- Consider risk-reducing surgery when appropriate
- Lynch syndrome carriers:
- Similar approach to BRCA carriers
- Additional endometrial cancer screening
- Earlier consideration of risk-reducing surgery
- Strong family history without identified mutation:
- Individualized surveillance based on risk assessment
- Consider genetic testing for extended panels
- Risk-reducing surgery based on risk level and age
Lifestyle changes and environmental precautions
Dietary and nutritional strategies:
Evidence-based dietary approaches:
- Mediterranean diet pattern:
- Emphasis on plant foods, olive oil, fish
- Limited red meat and processed foods
- 15-20% risk reduction in observational studies
- Anti-inflammatory effects
- Low-fat dietary pattern:
- Women’s Health Initiative showed modest risk reduction
- Most benefit for specific histological subtypes
- More impactful for women with normal BMI
- Specific food groups:
- Cruciferous vegetables: Contain indole-3-carbinol and sulforaphane
- Green tea: Polyphenols with anti-cancer properties
- Allium vegetables (garlic, onions): Organosulfur compounds
- Fatty fish: Omega-3 fatty acids with anti-inflammatory effects
Nutritional supplements and micronutrients:
- Vitamin D:
- Observational studies suggest protective association
- Optimal levels may reduce risk by 15-25%
- Recommended blood levels: 30-50 ng/mL (75-125 nmol/L)
- Sources: Sunlight exposure, fatty fish, fortified foods, supplements
- Antioxidants:
- Mixed evidence for supplement use
- Food sources preferred: colorful fruits and vegetables
- Selenium, vitamins C and E, carotenoids
- Other potentially beneficial nutrients:
- Omega-3 fatty acids: Anti-inflammatory effects
- Folate: DNA methylation and repair
- Calcium: Possible synergy with vitamin D
Dietary patterns to avoid:
- High glycemic load diets:
- Rapid blood sugar spikes
- Insulin pathway activation
- Associated with higher risk in some studies
- Processed meat consumption:
- Associated with modestly increased risk
- Nitrates and other preservatives concerning
- Trans fats and hydrogenated oils:
- Pro-inflammatory effects
- Associated with increased cancer risk overall
Physical activity and exercise:
Exercise recommendations:
- Aerobic activity:
- 150+ minutes per week of moderate activity
- 75+ minutes per week of vigorous activity
- Benefits increase with increasing amount (up to a point)
- Strength training:
- 2-3 times per week
- Major muscle groups
- Helps maintain healthy body composition
- Activity patterns:
- Avoiding prolonged sitting
- Breaking up sedentary time
- Daily activity preferable to occasional intense sessions
Mechanisms of protection:
- Hormonal effects:
- Reduced estrogen exposure
- Improved insulin sensitivity
- Decrease in inflammatory markers
- Immune function enhancement:
- Improved surveillance
- Reduced chronic inflammation
- Weight management:
- Prevention of obesity
- Reduction in metabolically active adipose tissue
- Oxidative stress reduction:
- Upregulation of antioxidant enzymes
- DNA repair enhancement
Exercise considerations for high-risk women:
- Post-surgical rehabilitation:
- Structured return to activity
- Pelvic floor-safe exercises
- Addressing surgical deconditioning
- During surveillance:
- Regular activity may improve detection of symptoms
- Potential benefit for quality of life during monitoring
- Special populations:
- BRCA carriers: No restriction on exercise type
- Endometriosis patients: Low-impact may be preferable
Weight management:
Weight and ovarian cancer risk:
- BMI relationship:
- Each 5-unit increase in BMI increases risk by 10-15%
- BMI >30 associated with 30-70% increased risk
- Most pronounced for non-serous histological subtypes
- Weight distribution:
- Central adiposity particularly associated with risk
- Waist-to-hip ratio strong predictor independent of BMI
- Weight changes:
- Adult weight gain associated with increased risk
- Weight cycling may increase inflammation and risk
Weight management strategies:
- Sustainable approaches:
- Focus on gradual, lasting changes
- Combined dietary and physical activity interventions
- Behavioral support and monitoring
- Timing considerations:
- Early adulthood weight management particularly important
- Avoiding weight gain during menopause transition
- Body composition focus:
- Reducing visceral adiposity
- Maintaining muscle mass
- Metabolic health beyond weight alone
Environmental exposures:
Occupational and environmental factors:
- Chemical exposures to minimize:
- Talc products (controversial but precautionary approach)
- Endocrine-disrupting chemicals in personal care products
- Industrial solvents and chemicals
- Pesticides and herbicides
- Radiation exposure:
- Minimizing unnecessary medical radiation
- Radon testing in homes
- Air pollution:
- Particulate matter exposure associated with risk
- HEPA filtration in high-pollution areas
- Limiting exposure during high pollution days
Household and consumer considerations:
- Personal care products:
- Avoiding talc-based powders in genital area
- Selecting products without endocrine disruptors
- Fragrance-free options when possible
- Food-related exposures:
- Washing produce thoroughly
- Minimizing processed food consumption
- Reducing food packaging chemicals (BPA, phthalates)
- Home environment:
- Adequate ventilation
- Regular dust removal (where chemicals concentrate)
- Natural cleaning products when possible
- Water filtration if quality concerns exist
Vaccines and preventive screenings
Screening approaches:
Current screening recommendations for average-risk women:
- No effective screening method established
- USPSTF recommendation: Against routine screening (Grade D recommendation)
- American College of Obstetricians and Gynecologists (ACOG): Against routine screening
- Society of Gynecologic Oncology (SGO): Against routine screening
- Rationale for recommendations:
- Insufficient evidence for mortality benefit
- High false positive rates
- Unnecessary surgeries and complications
- Psychological harms from false positives
Screening modalities evaluated:
- CA-125 blood test:
- Sensitivity for early-stage disease: 50-60%
- False positives common, especially in premenopausal women
- Serial measurements more valuable than single tests
- Evidence insufficient for population screening
- Transvaginal ultrasound (TVS):
- Sensitivity: 80-90% for masses, lower for early cancer
- Specificity: 85-90%
- High rates of false positives
- Invasive procedures often required for follow-up
- Combined approaches:
- Risk of Ovarian Cancer Algorithm (ROCA)
- Multimodal screening with sequential CA-125 and TVS
- Showed promise but no definitive mortality benefit in UKCTOCS trial
- Research ongoing for optimized approaches
Screening for high-risk populations:
- BRCA1/2 mutation carriers:
- CA-125 every 6 months
- Transvaginal ultrasound every 6 months
- Begin at age 30-35
- Continue until risk-reducing surgery
- Limited evidence for mortality benefit
- Primarily for reassurance and early detection
- Lynch syndrome carriers:
- Similar approach to BRCA carriers
- Begin at age 30-35
- Consider endometrial sampling annually
- Strong family history:
- Individualized based on risk assessment
- Consider genetic testing first
- Similar approach to mutation carriers if testing negative
Symptom awareness and recognition:
- Symptom index tools:
- Goff Symptom Index and variants
- Focus on key symptoms:
- Bloating
- Pelvic/abdominal pain
- Difficulty eating/early satiety
- Urinary symptoms
- Positive if symptoms new, persistent (>12 times monthly), present <1 year
- Implementation approaches:
- Patient education materials
- Primary care provider education
- Symptom diaries for high-risk women
- Mobile applications for symptom tracking
- Effectiveness:
- May reduce diagnostic delays by 3-6 months
- Stage shift potential (earlier diagnosis)
- Cost-effective approach for awareness
- No proven mortality benefit but biologically plausible
Vaccines and prophylactic approaches:
Vaccine development status:
- No FDA-approved preventive vaccine available
- Therapeutic vaccines in development:
- Target tumor-associated antigens:
- CA-125 (MUC16)
- NY-ESO-1
- WT1
- HER2/neu
- p53
- Delivery platforms:
- Peptide vaccines
- Dendritic cell vaccines
- Viral vector vaccines
- mRNA vaccines
- Clinical trials ongoing, primarily in treatment setting
- Target tumor-associated antigens:
- Preventive vaccine research:
- MUC1 vaccine in high-risk populations
- Anti-mesothelin approaches
- Fallopian tube targeting vaccines
Prophylactic medications:
- Oral contraceptives:
- Most established preventive agent
- 30-50% risk reduction with 5+ years use
- Consider for average and moderate risk women
- Individualized risk-benefit assessment needed
- Aspirin and NSAIDs:
- Modest protective effect (10-20% reduction)
- Not recommended solely for ovarian cancer prevention
- May be reasonable in context of other health benefits
- Chemoprevention trials:
- Metformin in high-risk women
- Statins for prevention
- Anti-inflammatory approaches
- Results pending from several studies
Emerging preventive approaches:
- Novel surgical approaches:
- Fallopian tube fimbria-specific surgery
- Endoscopic fimbriectomy techniques
- Expanded indications for opportunistic salpingectomy
- Immunoprevention:
- Targeting precursor lesions
- Enhancing immune surveillance
- Combination approaches with vaccines
- Precision prevention:
- Risk stratification using polygenic risk scores
- Microbiome modulation
- Preventive strategies tailored to specific histologic subtypes
- Circulating tumor DNA (ctDNA) for early detection:
- Detecting preclinical disease
- Monitoring high-risk individuals
- Emerging technology, several years from clinical application
10. Global & Regional Statistics
Incidence and prevalence rates globally
Global burden:
- Annual incidence: Approximately 313,959 new cases worldwide (2020 data)
- Prevalence: Estimated 762,000 women living with ovarian cancer globally
- Ranking: Seventh most common cancer in women worldwide
- Trend: Overall increasing cases due to population growth and aging
- Age-standardized rate: 6.6 per 100,000 women globally
- Cumulative risk: 0.69% lifetime risk globally (average)
Regional variations in incidence:
High-incidence regions:
- Central and Eastern Europe:
- Highest rates globally (11.4 per 100,000)
- Lithuania, Latvia, Bulgaria with highest national rates
- Genetic factors and reproductive patterns contribute
- Northern Europe:
- 9.3-10.7 per 100,000
- Norway, Denmark, UK among highest
- Better detection and reporting may contribute
- North America:
- United States: 8.0 per 100,000
- Canada: 8.6 per 100,000
- Higher rates in white compared to Black populations
- Oceania:
- Australia: 7.9 per 100,000
- New Zealand: 8.8 per 100,000
- Higher in non-indigenous populations
Moderate-incidence regions:
- Western Europe:
- 7.3-8.9 per 100,000
- Higher rates in northern compared to southern countries
- Decreasing trends in recent years
- South America:
- 5.8-7.0 per 100,000
- Highest in Argentina and Uruguay
- Increasing trends in most countries
- East Asia (developed regions):
- Japan: 6.4 per 100,000
- South Korea: 6.7 per 100,000
- Rapidly increasing rates with westernization
Low-incidence regions:
- Africa:
- 4.2-5.0 per 100,000
- Highest in Southern Africa
- Significant underdetection likely
- South-Central Asia:
- 4.1-5.3 per 100,000
- India: 4.8 per 100,000
- Pakistan: 5.1 per 100,000
- Southeast Asia:
- 5.0-5.5 per 100,000
- Variability between countries
- Thailand and Singapore with higher rates
Histological subtype distribution:
- High-grade serous carcinoma:
- 65-70% globally
- Higher proportion in Western countries
- Associated with BRCA mutations
- Endometrioid carcinoma:
- 10-15% globally
- Higher rates in regions with high endometriosis prevalence
- Clear cell carcinoma:
- 3-10% globally
- Higher prevalence in East Asian populations (10-25%)
- Associated with endometriosis
- Mucinous carcinoma:
- 3-5% globally
- More uniform distribution
- Low-grade serous carcinoma:
- 3-5% globally
- Higher rates in younger women
Temporal trends:
- Developed regions:
- Stable or slightly decreasing rates
- Improved diagnostic precision
- Impact of oral contraceptive use
- Declining parity
- Developing regions:
- Increasing rates in most areas
- Westernization of lifestyle
- Changing reproductive patterns
- Improved detection and reporting
- Age-specific trends:
- Increasing rates in postmenopausal women
- Stable or declining rates in premenopausal women
- Shift toward older age at diagnosis
Mortality and survival rates
Global mortality:
- Annual deaths: Approximately 207,252 deaths worldwide (2020 data)
- Ranking: Eighth leading cause of cancer death in women globally
- Age-standardized mortality rate: 4.2 per 100,000 women
- Mortality-to-incidence ratio: 0.66 (higher than most cancers)
- Trend: Slowly decreasing in developed regions, increasing in many developing regions
Regional mortality patterns:
High-mortality regions:
- Eastern Europe:
- Highest mortality rates globally (6.6-7.1 per 100,000)
- Latvia, Bulgaria, Russia among highest
- Limited access to optimal treatment
- Late-stage diagnosis common
- Central Europe:
- 5.3-6.5 per 100,000
- Higher rates in Czech Republic, Hungary
- Improving but still high mortality
- South America:
- Especially in southern countries (Argentina, Uruguay)
- 4.5-5.3 per 100,000
- Limited specialized care in many areas
Moderate-mortality regions:
- North America:
- United States: 4.3 per 100,000
- Canada: 4.4 per 100,000
- Declining rates over past two decades
- Racial/ethnic disparities persist
- Western Europe:
- 4.3-5.1 per 100,000
- Higher in northern countries
- Declining trends in most countries
- Oceania:
- Australia: 4.3 per 100,000
- New Zealand: 4.8 per 100,000
- Indigenous populations with higher rates
Low-mortality regions:
- East Asia:
- 2.7-3.8 per 100,000 (excluding Japan)
- Japan: 4.0 per 100,000
- Increasing trends with westernization
- Southeast Asia:
- 3.0-3.6 per 100,000
- Limited access to specialized care
- Significant underreporting likely
- North Africa:
- 2.8-3.2 per 100,000
- Data quality issues present
Survival rates by region:
High-income countries:
- Five-year relative survival rates:
- United States: 48.6%
- Australia: 45.7%
- Northern Europe: 41.2-46.5%
- Western Europe: 40.8-43.5%
- Japan: 54.7%
- Stage-specific survival:
- Stage I: 89-94%
- Stage II: 70-78%
- Stage III: 35-40%
- Stage IV: 18-25%
- Trends: Generally improving over time
- 1-2% absolute improvement per decade
- Greatest improvements in younger patients
- Plateau in advanced-stage disease until recent years
Middle-income countries:
- Five-year relative survival rates:
- Eastern Europe: 31.6-39.3%
- South America: 30.5-41.2%
- Middle East: 35.5-42.7%
- China: 38.8%
- Stage distribution:
- Higher proportion of advanced-stage disease
- Limited access to specialized surgical care
- Restricted access to newer targeted therapies
- Trends: Modest improvements
- Slower rate of improvement than high-income regions
- Significant geographic and socioeconomic disparities within countries
Low-income countries:
- Five-year relative survival rates:
- Sub-Saharan Africa: 15.6-27.9%
- South Asia: 26.1-31.5%
- Limited data quality and availability
- Major challenges:
- Very late-stage diagnosis (80-90% stage III-IV)
- Limited surgical expertise
- Restricted chemotherapy access
- Minimal access to targeted therapies
- Inadequate supportive and palliative care
- Trends: Little improvement over time
- Survival gap widening compared to high-income regions
- Limited population-based data
Factors influencing survival:
Healthcare system factors:
- Specialized gynecologic oncology care:
- 9-15% survival advantage with specialist care
- Limited availability in many regions
- Multidisciplinary team approach:
- Associated with 7-11% survival improvement
- Standard in high-income regions, limited elsewhere
- Access to clinical trials:
- Survival benefit independent of treatment received
- Geographic and socioeconomic disparities in access
- Treatment guideline adherence:
- 15-25% survival difference between optimal and suboptimal care
- Varies significantly between and within countries
Patient factors:
- Socioeconomic status:
- Lower income associated with 10-15% lower survival
- Education level impacts survival independent of income
- Insurance status major factor in some countries
- Race/ethnicity:
- Black women: 10-12% lower survival in US studies
- Contributing factors:
- Access to care
- Treatment differences
- Comorbidities
- Tumor biology
- Age at diagnosis:
- Worse outcomes in very young (<30) and elderly (>75)
- Elderly often receive less aggressive treatment
- Comorbidities impact treatment tolerance
Country-wise comparison and trends
North America:
United States:
- Incidence: 21,410 new cases annually (11.6 per 100,000, age-adjusted)
- Mortality: 13,770 deaths annually (6.7 per 100,000, age-adjusted)
- Five-year relative survival: 48.6% overall
- Racial/ethnic patterns:
- Higher incidence in White women
- Lower incidence but worse survival in Black women
- Lower incidence in Hispanic and Asian populations
- Geographic variation:
- Highest in Northeast and Midwest
- Lower in South and West
- Rural-urban disparities in outcomes
- Trends:
- Decreasing incidence (-1.0% annually)
- Decreasing mortality (-2.3% annually)
- Improving survival (+0.6% annually)
- Histological shifts:
- Decreasing epithelial unspecified cases
- Better classification of histological subtypes
- Stable distribution of major subtypes
Canada:
- Incidence: 3,100 new cases annually (9.9 per 100,000, age-adjusted)
- Mortality: 1,950 deaths annually (5.4 per 100,000, age-adjusted)
- Five-year relative survival: 45.4% overall
- Geographic patterns:
- Higher rates in Eastern provinces
- Lower rates in British Columbia
- Significant indigenous population disparities
- Trends:
- Stable incidence
- Decreasing mortality (-2.0% annually)
- Provincial variation in outcomes
Europe:
United Kingdom:
- Incidence: 7,470 new cases annually (10.4 per 100,000, age-adjusted)
- Mortality: 4,230 deaths annually (5.1 per 100,000, age-adjusted)
- Five-year relative survival: 43.2% overall
- Trends:
- Stable incidence
- Decreasing mortality (-1.9% annually)
- Improved survival since national specialist care initiative
- Variations between NHS trusts
Germany:
- Incidence: 7,250 new cases annually (8.6 per 100,000, age-adjusted)
- Mortality: 5,370 deaths annually (4.8 per 100,000, age-adjusted)
- Five-year relative survival: 41.2% overall
- Trends:
- Slightly decreasing incidence
- Decreasing mortality
- East-West differences diminishing
- Specialized center certification improving outcomes
Italy:
- Incidence: 5,310 new cases annually (8.2 per 100,000, age-adjusted)
- Mortality: 3,260 deaths annually (3.7 per 100,000, age-adjusted)
- Five-year relative survival: 39.5% overall
- Patterns:
- North-South gradient in incidence and survival
- Better outcomes in Northern regions
- Access to specialized care varies by region
Eastern Europe:
- Incidence: 10-12 per 100,000 in most countries
- Mortality: 6-8 per 100,000
- Five-year survival: 31.6-39.3%
- Trends:
- High but stable or slightly decreasing incidence
- Mortality decreasing more slowly than Western Europe
- Improving access to modern treatments
- EU membership accelerating improvements in some countries
Asia-Pacific:
Japan:
- Incidence: 9,940 new cases annually (6.4 per 100,000, age-adjusted)
- Mortality: 5,010 deaths annually (2.5 per 100,000, age-adjusted)
- Five-year relative survival: 54.7% overall (highest globally)
- Distinctive features:
- Higher proportion of clear cell carcinoma (20-25%)
- Lower proportion of high-grade serous
- Better outcomes stage-for-stage
- Aggressive surgical approach
- Trends:
- Increasing incidence (+1.5% annually)
- Stable mortality
- Best survival outcomes globally
China:
- Incidence: 55,342 new cases annually (4.8 per 100,000, age-adjusted)
- Mortality: 37,519 deaths annually (2.9 per 100,000, age-adjusted)
- Five-year relative survival: 38.8% overall
- Patterns:
- Urban-rural disparities in incidence and survival
- Higher rates in industrialized eastern regions
- Limited data from rural western regions
- Trends:
- Rapidly increasing incidence (+3.5% annually)
- Slowly decreasing mortality
- Expanding access to specialized care
- Increasing use of targeted therapies
Australia:
- Incidence: 1,720 new cases annually (7.9 per 100,000, age-adjusted)
- Mortality: 1,040 deaths annually (4.3 per 100,000, age-adjusted)
- Five-year relative survival: 45.7% overall
- Patterns:
- Higher incidence in urban areas
- Indigenous population disparities
- Excellent data collection and cancer registries
- Trends:
- Stable incidence
- Decreasing mortality (-1.8% annually)
- National initiatives for earlier diagnosis
Developing regions:
India:
- Incidence: 45,701 new cases annually (4.8 per 100,000, age-adjusted)
- Mortality: 32,617 deaths annually (3.6 per 100,000, age-adjusted)
- Five-year relative survival: 29.2% overall
- Challenges:
- Very late-stage presentation (85% stage III-IV)
- Limited specialized surgical expertise
- Restricted access to newer therapies
- Significant data quality issues
- Trends:
- Increasing incidence with urbanization
- High mortality-to-incidence ratio
- Improving cancer registry data
Brazil:
- Incidence: 6,650 new cases annually (5.9 per 100,000, age-adjusted)
- Mortality: 3,879 deaths annually (3.7 per 100,000, age-adjusted)
- Five-year relative survival: 35.4% overall
- Patterns:
- Higher rates in southern regions
- Significant socioeconomic disparities
- Limited pathology resources in many regions
- Trends:
- Increasing incidence
- Stable mortality
- Improving specialized care in major centers
Sub-Saharan Africa:
- Incidence: 4.2-5.0 per 100,000 (likely underestimated)
- Mortality: 3.7-4.5 per 100,000
- Five-year relative survival: 15.6-27.9% (limited data)
- Major issues:
- Extremely late diagnosis
- Limited surgical and pathology resources
- Restricted chemotherapy access
- Minimal targeted therapy availability
- Competing health priorities
- Very limited cancer registry data
- Trends:
- Increasing reported incidence (likely due to improved detection)
- Stable or increasing mortality
- Limited progress in outcomes
Global comparisons and disparities:
Stage at diagnosis:
- High-income countries:
- Stage I-II: 30-35%
- Stage III: 40-45%
- Stage IV: 15-20%
- Middle-income countries:
- Stage I-II: 15-25%
- Stage III: 45-50%
- Stage IV: 25-35%
- Low-income countries:
- Stage I-II: 5-15%
- Stage III: 40-45%
- Stage IV: 40-50%
Treatment availability:
- Surgery by gynecologic oncologist:
- High-income: 70-90% of patients
- Middle-income: 25-50% of patients
- Low-income: <10% of patients
- Platinum-based chemotherapy access:
- High-income: >95% of appropriate patients
- Middle-income: 60-80% of appropriate patients
- Low-income: 20-40% of appropriate patients
- PARP inhibitor availability:
- High-income: Widely available, cost/insurance barriers
- Middle-income: Limited availability, significant cost barriers
- Low-income: Generally unavailable
Economic impact:
- Treatment costs per patient:
- High-income: $50,000-$200,000 USD
- Middle-income: $15,000-$50,000 USD
- Low-income: $5,000-$15,000 USD
- Economic burden relative to healthcare spending:
- Disproportionate impact in lower-resource settings
- Catastrophic health expenditure common in many countries
- Lost productivity costs substantial globally
11. Recent Research & Future Prospects
Latest advancements in treatment and research
Targeted therapy innovations:
PARP inhibitor advances:
- Expanding indications:
- First-line maintenance regardless of BRCA status
- Combination strategies with bevacizumab
- Treatment setting (not just maintenance)
- Earlier disease stages (adjuvant trials ongoing)
- Novel agents and formulations:
- Next-generation PARP inhibitors with improved pharmacokinetics
- Brain-penetrant formulations for CNS disease
- Long-acting formulations for less frequent dosing
- Combined PARP/tankyrase inhibitors
- Resistance mechanisms and overcoming strategies:
- BRCA reversion mutations
- Drug efflux pumps
- Restoration of homologous recombination
- PARP inhibitor + ATR inhibitor combinations
- PARP inhibitor + WEE1 inhibitor combinations
Antibody-drug conjugates (ADCs):
- Mirvetuximab soravtansine:
- Targets folate receptor alpha
- SORAYA and FORWARD II trials: Activity in platinum-resistant disease
- FDA approval anticipated soon
- 32% objective response rate in platinum-resistant disease
- Manageable ocular toxicity
- Upifitamab rilsodotin (XMT-1536):
- NaPi2b-targeting ADC
- Phase I/II data showing activity in platinum-resistant disease
- Well-tolerated safety profile
- Development continuing
- Emerging ADC targets:
- Tissue factor (tisotumab vedotin)
- Trop-2 (sacituzumab govitecan)
- MUC16/CA-125 (STRO-002)
- HER2 (for rare HER2+ ovarian cancers)
- AXL (enapotamab vedotin)
Novel targeted approaches:
- Cell cycle inhibitors:
- WEE1 inhibitors (adavosertib): Synthetic lethality with p53 mutations
- CDK4/6 inhibitors: Activity in low-grade serous carcinoma
- CDK7 inhibitors: Targeting transcription regulation
- Aurora kinase inhibitors: Disrupting mitosis
- Other DNA damage response inhibitors:
- ATR inhibitors (ceralasertib, berzosertib): Synergy with chemotherapy
- CHK1 inhibitors: Cell cycle checkpoint targeting
- DNA-PK inhibitors: Blocking non-homologous end joining
- Epigenetic modulators:
- EZH2 inhibitors: Activity in ARID1A-mutated clear cell carcinoma
- BET inhibitors: Transcriptional regulation targeting
- HDAC inhibitors: Restoring platinum sensitivity
Immunotherapy innovations:
Checkpoint inhibitor strategies:
- Combination approaches:
- PD-1/PD-L1 + PARP inhibitors:
- TOPACIO/KEYNOTE-162: Pembrolizumab + niraparib
- MEDIOLA: Durvalumab + olaparib
- Enhanced responses in both BRCA-mutated and wild-type patients
- PD-1/PD-L1 + anti-angiogenics:
- IMagyn050: Atezolizumab + bevacizumab + chemotherapy
- ATALANTE: Atezolizumab + bevacizumab
- Targeting both immune and vascular components
- PD-1/PD-L1 + chemotherapy:
- JAVELIN Ovarian 200: Avelumab + pegylated liposomal doxorubicin
- NRG-GY009: Pembrolizumab + chemotherapy
- PD-1/PD-L1 + PARP inhibitors:
- Biomarker-guided approaches:
- MSI-high/dMMR selection (~3% of ovarian cancers)
- Tumor mutational burden assessment
- Gene expression profiles
- Tumor infiltrating lymphocyte analysis
- Multiplex immunohistochemistry
Cellular immunotherapy:
- Tumor-infiltrating lymphocytes (TILs):
- Ex vivo expansion and reinfusion
- Phase II results: 29% response rate in heavily pretreated patients
- Phase III trials ongoing
- LN-145/lifileucel in development
- Challenges: manufacturing complexity, patient selection
- CAR-T cell approaches:
- Targets in development:
- MUC16/CA-125
- Mesothelin
- Folate receptor alpha
- HER2
- NKG2D ligands
- Challenges:
- Solid tumor penetration
- Hostile tumor microenvironment
- Antigen heterogeneity
- On-target/off-tumor toxicity
- Targets in development:
- NK cell therapies:
- Allogeneic NK cell infusions
- CAR-NK cells
- NK cell engagers
- Advantages: reduced cytokine release syndrome, allogeneic potential
Tumor microenvironment modulation:
- Macrophage-directed therapies:
- CSF1R inhibitors to reprogram tumor-associated macrophages
- CD47 antagonists to enhance phagocytosis
- Anti-CCL2 approaches to limit macrophage recruitment
- Stromal targeting approaches:
- FAP-targeted therapies
- TGF-β pathway inhibitors
- Hyaluronidase to reduce stromal density
- Hedgehog pathway inhibitors
- Vascular normalization strategies:
- Low-dose anti-angiogenics
- Angiopoietin/Tie2 axis modulators
- Selective VEGFR inhibitors
- Dual VEGF/Ang2 inhibition
Precision medicine approaches:
Molecular profiling advances:
- Comprehensive genomic profiling:
- Standard of care for all high-grade disease
- Multi-gene panels including:
- Homologous recombination genes
- Cell cycle regulators
- PI3K/AKT/mTOR pathway
- RAS/RAF pathway
- Chromatin remodeling complex
- Refining classification beyond histology
- Treatment selection based on alterations
- RNA-based profiling:
- Gene expression signatures
- Fusion detection
- Alternative splicing analysis
- Non-coding RNA assessment
- Epigenetic profiling:
- DNA methylation patterns
- Histone modifications
- Chromatin accessibility
- Epigenetic vulnerability identification
Liquid biopsy applications:
- Circulating tumor DNA (ctDNA):
- Early detection of recurrence (3-6 months lead time)
- Real-time monitoring of treatment response
- Resistance mechanism identification
- Tumor heterogeneity assessment
- Minimal residual disease detection
- Circulating tumor cells (CTCs):
- Prognostic value
- Phenotypic and functional characterization
- Ex vivo drug testing potential
- Exosomes and microRNAs:
- Complementary to ctDNA
- Functional information beyond mutations
- Potential early detection biomarkers
Functional precision medicine:
- Patient-derived organoids (PDOs):
- 3D cultures from patient tumors
- Drug sensitivity and resistance testing
- 70-85% predictive accuracy for clinical response
- 2-3 week turnaround time
- Integration into clinical decision-making
- Patient-derived xenografts (PDXs):
- More accurate tumor microenvironment
- Testing of combination therapies
- Limitations: time, cost, scalability
- Ex vivo drug sensitivity testing:
- Fresh tumor tissue exposed to drug panels
- Rapid readouts (24-72 hours)
- Assessment of multiple drug combinations
- Integration with genomic data
Ongoing studies and future medical possibilities
Major clinical trials reshaping the field:
Front-line treatment trials:
- ATHENA (NCT03522246):
- Rucaparib + nivolumab as first-line maintenance
- Quadruple arm study with rucaparib, nivolumab, combination, and placebo
- Results expected 2023-2024
- DUO-O (NCT03737643):
- Standard chemotherapy + bevacizumab + durvalumab + olaparib
- Comprehensive immunotherapy + PARP approach
- Primary results expected 2023
- FIRST/ENGOT-OV44 (NCT03602859):
- Platinum + TSR-042 (dostarlimab) + niraparib
- Immunotherapy during and after chemotherapy
- Preliminary data shows promising results
- GINECO-ATARI (NCT04397289):
- Maintenance therapy selection based on molecular profile
- Personalized maintenance strategy
- Novel biomarker-driven design
Recurrent disease trials:
- INNOVATE-3 (NCT03940196):
- Tumor treating fields (TTFields) with paclitaxel
- Novel physical modality targeting dividing cells
- Based on promising phase II data
- MILO-4 (NCT04419402):
- VS-6766 (RAF/MEK inhibitor) + defactinib
- Targeting low-grade serous carcinoma
- KRAS-driven pathway inhibition
- ENGOT-OV57 (NCT04776018):
- Mirvetuximab soravtansine vs investigator’s choice
- FR-α positive platinum-resistant disease
- Potential practice-changing ADC
- PRO-BEAT (NCT03914612):
- Atezolizumab + bevacizumab vs chemotherapy
- Platinum-resistant setting
- Chemo-free immunotherapy approach
Novel therapeutic strategies in development:
Synthetic lethality beyond PARP:
- POLQ (polymerase theta) inhibitors:
- Synthetic lethality with BRCA1/2 mutations
- Active in PARP inhibitor-resistant models
- ART4215, ART6043 in early clinical development
- Potential for combinations with PARP inhibitors
- SLX4IP inhibitors:
- Novel synthetic lethal interaction with BRCA1/2
- Active in PARP inhibitor-resistant models
- Preclinical development
- BRCA1/2 synthetic lethal screens:
- CRISPR-based discovery of novel interactions
- Multiple targets in preclinical validation
- Expanding therapeutic options for BRCA-mutated disease
Metabolism-targeting approaches:
- Glutamine metabolism:
- Glutaminase inhibitors (telaglenastat)
- Particularly for clear cell subtype
- Phase II trials ongoing
- Lipid metabolism:
- Fatty acid synthase inhibitors
- Cholesterol pathway targeting
- HIF-2α inhibitors for clear cell histology
- Arginine deprivation:
- ADI-PEG 20 (pegylated arginine deiminase)
- For ASS1-deficient tumors
- Phase II trials in combination with chemotherapy
Microbiome modulation strategies:
- Gut microbiome optimization:
- Influence on chemotherapy efficacy
- Impact on immunotherapy response
- Trials of fecal microbiota transplantation
- Defined bacterial consortia approaches
- Vaginal microbiome:
- Influence on ovarian cancer risk
- Potential prevention strategies
- Impact on treatment response
- Microbial-derived metabolites:
- Short-chain fatty acids
- Tryptophan metabolites
- Bile acids
- Potential for therapeutic mimetics
Advanced delivery technologies:
- Nanoparticle formulations:
- Tumor-targeting ligands
- Environmentally responsive release
- Overcoming drug resistance
- Reducing systemic toxicity
- Intraperitoneal delivery innovations:
- Sustained-release implants
- Injectable depots
- Nanocomposite materials
- Pressurized intraperitoneal aerosol chemotherapy (PIPAC)
- Guided drug delivery:
- Ultrasound-triggered release
- Magnetic targeting
- Light-activated therapies
- Combined diagnostic/therapeutic (theranostic) approaches
Future diagnostic approaches:
Early detection innovations:
- Multi-cancer early detection (MCED) tests:
- Blood-based screening for multiple cancer types
- DNA methylation patterns
- Protein biomarkers
- Cell-free DNA fragmentation patterns
- Trials ongoing in high-risk populations
- Exhaled volatile organic compounds:
- Electronic nose technology
- Metabolomic signatures
- Non-invasive screening approach
- Early clinical validation
- Circulating microRNAs and exosomes:
- Specific signatures preceding clinical diagnosis
- Combined panels with traditional markers
- Longitudinal monitoring for high-risk women
- Advanced imaging approaches:
- Molecular imaging with targeted probes
- AI-enhanced ultrasound
- Novel MRI protocols
- Multimodal imaging integration
Response assessment innovations:
- Functional and molecular imaging:
- DWI-MRI for early response assessment
- PET with novel tracers (beyond FDG)
- Magnetic resonance spectroscopy
- Combined anatomic/functional assessment
- Circulating biomarkers for response:
- ctDNA dynamics during treatment
- Circulating tumor cells (CTCs)
- Protein signature changes
- Real-time resistance monitoring
- AI-powered response prediction:
- Radiomics features from standard imaging
- Deep learning integration of multiple data types
- Predicting response before treatment changes
- Treatment adaptation based on early signals
Artificial intelligence applications:
- Diagnostic accuracy enhancement:
- CT/MRI interpretation
- Ultrasound standardization
- Detecting subtle disease presence
- Reducing interobserver variability
- Pathology augmentation:
- Digital pathology with AI analysis
- Automated grading
- Biomarker quantification
- Integrated genomic-pathologic assessment
- Treatment selection decision support:
- Multimodal data integration
- Outcome prediction models
- Toxicity risk assessment
- Personalized dosing recommendations
Potential cures or innovative therapies under development
Transformative therapeutic approaches:
Novel immunotherapy platforms:
- Bispecific T-cell engagers (BiTEs):
- Simultaneously bind T cells and tumor cells
- Bypass traditional antigen presentation
- Targets in development:
- MUC16/CA-125
- Mesothelin
- EpCAM
- FR-α
- Phase I trials underway
- Potential for off-the-shelf solution
- Cancer vaccines:
- Personalized neoantigen vaccines
- Shared antigen approaches
- mRNA vaccine platforms
- Dendritic cell vaccines
- Combination with checkpoint inhibitors
- Phase I/II trials showing immune responses
- Oncolytic viruses:
- Direct tumor cell lysis
- Immune stimulation
- Delivery vehicle for immunomodulators
- Intraperitoneal administration advantage
- Phase I/II trials ongoing
Cell-based therapies beyond CAR-T:
- Tumor-infiltrating lymphocytes (TILs):
- Expanded clinical trials after promising phase II results
- Selection of tumor-reactive populations
- Combination with checkpoint inhibitors
- Potential for 25-35% response in advanced disease
- γδ T-cell therapy:
- Recognizes non-classical antigens
- MHC-independent recognition
- Lower risk of graft-versus-host disease
- Allogeneic potential
- Phase I trials initiating
- Engineered natural killer (NK) cells:
- CAR-NK cells
- Memory-like NK cells
- Off-the-shelf potential
- Reduced cytokine release syndrome
- Multiple targets in development
Gene editing approaches:
- CRISPR-based therapies:
- Ex vivo gene editing of immune cells
- Direct in vivo editing being explored
- Restoration of tumor suppressor function
- Disruption of oncogenic pathways
- Early clinical development
- Gene therapy:
- Viral vector delivery of therapeutic genes
- p53 restoration approaches
- Suicide gene therapy
- Immunomodulatory gene delivery
- Intraperitoneal administration advantage
- RNA therapeutics:
- siRNA targeting oncogenic drivers
- mRNA delivery of tumor suppressors
- microRNA modulation
- Phase I trials initiating
- Nanoparticle delivery systems
Combinatorial precision approaches:
Comprehensive molecular profiling:
- Integrated multi-omics:
- Genomics, transcriptomics, proteomics, metabolomics
- Single-cell approaches for heterogeneity assessment
- Spatial biology for microenvironmental context
- Clinical implementation beginning
- Functional drug screening:
- High-throughput ex vivo testing
- Organoid-based approaches
- Real-time drug sensitivity assessment
- Integration with molecular profiling
- AI-driven treatment algorithms:
- Learning from multi-institutional datasets
- Continuous improvement with outcomes data
- Integration of clinical, pathological, and molecular features
- Decision support systems in development
Targeting minimal residual disease:
- Post-surgical adjuvant approaches:
- PARP inhibitors in early-stage disease
- Immunotherapy to eliminate micrometastases
- Maintenance therapy selection based on ctDNA
- Personalized duration based on molecular response
- Systemic + regional therapy combinations:
- HIPEC + molecular targeted therapy
- Intraperitoneal immunotherapy
- Novel drug delivery systems
- Trials exploring optimal combinations
- Curative intent in oligometastatic disease:
- Aggressive surgical approaches
- Stereotactic radiotherapy
- Molecularly guided therapy selection
- 15-20% long-term disease-free survival potential
Prevention and interception strategies:
Hereditary cancer management:
- Enhanced risk prediction:
- Integration of germline, somatic, and polygenic risk
- Inclusion of reproductive and hormonal factors
- Environmental exposure assessment
- AI-enhanced risk models
- Risk-reducing surgery optimization:
- Salpingectomy with delayed oophorectomy
- Minimally invasive approaches
- Targeted removal of fimbrial tissue
- Preserving hormonal function when possible
- Chemoprevention trials:
- Novel agents in high-risk populations
- PARP inhibitors for prevention
- Immunopreventive approaches
- Anti-inflammatory strategies
Early interception approaches:
- Detection of STIC lesions:
- Improved imaging of fallopian tubes
- Molecular markers for premalignant changes
- Screening protocols for high-risk women
- Targeted intervention for precursors
- Liquid biopsy for pre-clinical detection:
- Ultra-sensitive ctDNA detection
- Protein biomarker panels
- Exosome analysis
- Years before clinical manifestation
- Immune surveillance enhancement:
- Vaccine approaches for premalignant lesions
- Immune modulation to eliminate early disease
- Microbiome optimization
- Lifestyle and nutritional approaches
Future challenges and directions:
Addressing treatment resistance:
- Combination strategies to prevent resistance:
- Vertical pathway inhibition
- Targeting multiple escape mechanisms
- Adaptive therapy approaches
- Intermittent high-dose strategies
- Tumor evolution monitoring:
- Real-time assessment of emerging resistance
- ctDNA-guided treatment switching
- Proactive rather than reactive adaptation
- Anticipating resistance mechanisms
Expanding effective therapies globally:
- Cost-effective approaches:
- Biosimilar development
- Generic targeted therapies
- Value-based pricing models
- Tiered access programs
- Implementation science:
- Adapting protocols for resource-limited settings
- Training programs for specialized surgical care
- Telemedicine approaches for expert consultation
- Simplified treatment regimens where necessary
Integration of quality of life considerations:
- Patient-reported outcome-guided therapy:
- Treatment selection considering quality and quantity of life
- De-escalation strategies when appropriate
- Toxicity management innovations
- Survivorship-focused approaches
- Financial toxicity mitigation:
- Value-based care models
- Financial navigation support
- Cost-effectiveness assessment
- Sustainable precision medicine approaches
12. Interesting Facts & Lesser-Known Insights
Uncommon knowledge about ovarian cancer
Historical perspectives:
Evolution of understanding the disease origin:
- The concept that most high-grade serous ovarian cancers actually originate in the fallopian tubes represents one of the most significant paradigm shifts in gynecologic oncology over the past two decades
- Despite being called “ovarian” cancer for over a century, pathologists in the early 2000s began identifying precursor lesions (serous tubal intraepithelial carcinoma or STIC) in the fallopian tubes of BRCA mutation carriers undergoing risk-reducing surgery
- This discovery has revolutionized prevention approaches, with some experts now advocating for the term “tubo-ovarian carcinoma” or “pelvic serous carcinoma” to more accurately reflect the disease origin
Historical treatment approaches:
- In the 1950s, radioactive phosphorus (32P) was instilled into the peritoneal cavity as a treatment for ovarian cancer, representing an early form of intraperitoneal therapy
- Before the development of effective chemotherapy, extended surgeries including partial liver resection, oophorectomy, and diaphragm stripping were used as primary therapy
- The first effective chemotherapy for ovarian cancer was nitrogen mustard, a derivative of the chemical warfare agent from World War I
- “Second-look” surgeries (operating to check for disease after completing chemotherapy) were standard practice until the 1990s but have been largely abandoned due to lack of survival benefit
Scientific curiosities:
Unique biological features:
- Ovarian cancer is one of the few solid tumors that spreads primarily by direct exfoliation and implantation rather than through blood vessels or lymphatics in early stages
- The peritoneal cavity functions as a unique microenvironment with specific immune properties that allow cancer cells to evade detection
- High-grade serous ovarian cancer has the highest frequency of TP53 mutations of any solid tumor (>95% of cases)
- Clear cell ovarian cancer shares more molecular similarities with clear cell renal carcinoma than with other ovarian cancer subtypes
- Mucinous ovarian cancers often harbor the same KRAS mutations found in pancreatic and colorectal cancers, suggesting potential similarities in pathogenesis
Immune system interactions:
- Despite having a high mutational burden, high-grade serous ovarian cancers typically have a “cold” immune microenvironment with few infiltrating T cells
- Patients with higher numbers of tumor-infiltrating lymphocytes have significantly better survival, independent of other factors
- CD8+ T cells in ovarian cancer often exhibit an “exhausted” phenotype that limits their effectiveness
- Ovarian cancers develop multiple immunosuppressive mechanisms, including recruitment of regulatory T cells and myeloid-derived suppressor cells
- Homologous recombination deficient tumors tend to have higher neoantigen loads and better response to immunotherapy
Hormonal influences:
- Despite being a cancer of reproductive organs, most high-grade serous ovarian cancers do not respond to hormonal therapies
- Low-grade serous and endometrioid subtypes often express estrogen and progesterone receptors and may respond to hormonal treatments
- Granulosa cell tumors produce estrogen that can cause breast tenderness, endometrial hyperplasia, and abnormal vaginal bleeding
- Pregnancy temporarily reprograms the fallopian tube secretory cells that give rise to most ovarian cancers, potentially explaining the protective effect of pregnancy
- Androgen receptors are present in many ovarian cancers and may represent a therapeutic target
Clinical pearls:
Diagnostic challenges:
- The symptoms of ovarian cancer (bloating, pelvic pain, early satiety, urinary frequency) occur an average of 3-6 months before diagnosis but are often misattributed to benign conditions
- Even advanced ovarian cancer can be missed on standard CT scans due to the diffuse, thin spread of peritoneal disease
- Up to 15% of apparent “ovarian” cancers are actually metastases from other primary sites, particularly the gastrointestinal tract and breast
- CA-125 can be normal in up to 50% of early-stage ovarian cancers and 20% of advanced cases
- Approximately 3-5% of women with apparent “primary peritoneal carcinoma” have occult fallopian tube primaries even after pathological examination
Treatment insights:
- Complete surgical cytoreduction to no visible residual disease improves survival more than any known drug therapy
- Intraperitoneal chemotherapy can achieve drug concentrations 20-1000 times higher in the peritoneal cavity than systemic administration
- Dose-dense weekly paclitaxel may be more effective than standard every-three-week dosing due to anti-angiogenic effects
- PARP inhibitors work not only by inhibiting the PARP enzyme but also by “trapping” PARP on DNA, creating toxic complexes
- Patients with CCNE1 amplification (cyclin E1) typically have poor response to platinum chemotherapy but may respond to specific cell cycle inhibitors
Unusual presentations:
- Some patients present with isolated remote metastases (e.g., axillary lymph nodes, brain) without obvious pelvic disease
- Sister Mary Joseph nodule (umbilical metastasis) can be the first sign of ovarian cancer
- Paraneoplastic cerebellar degeneration can precede diagnosis of ovarian cancer by months to years
- Ovarian cancer can present with autoimmune hemolytic anemia, dermatomyositis, or other paraneoplastic syndromes
- “Pseudomyxoma peritonei” is typically caused by appendiceal cancers rather than ovarian primaries, despite often being misdiagnosed initially
Myths and misconceptions vs. medical facts
Myth 1: Ovarian cancer is a “silent disease” with no early symptoms. Fact: While ovarian cancer was historically called the “silent killer,” research has shown that approximately 90% of women with ovarian cancer experience symptoms—typically bloating, pelvic/abdominal pain, difficulty eating or feeling full quickly, and urinary urgency or frequency—for an average of 3-6 months before diagnosis. These symptoms are often persistent, represent a change from normal, and occur frequently (more than 12 times per month). However, they are often misattributed to benign conditions like irritable bowel syndrome, menopause, or aging, leading to diagnostic delays.
Myth 2: Pap smears can detect ovarian cancer. Fact: Pap smears are designed to detect cervical cancer and precancerous changes of the cervix only. They do not sample cells from the ovaries or fallopian tubes and therefore cannot detect ovarian cancer. This misunderstanding may give women a false sense of security about ovarian cancer screening during gynecologic exams. Currently, there is no recommended screening test for ovarian cancer in average-risk women, and specialized testing (transvaginal ultrasound and CA-125) is only recommended for high-risk populations.
Myth 3: Ovarian cysts mean you have or will develop ovarian cancer. Fact: Ovarian cysts are extremely common and are usually benign functional structures related to normal ovulation. Most premenopausal women develop ovarian cysts regularly as part of their menstrual cycles. Even postmenopausal women can develop benign cysts. Only a small percentage of ovarian cysts are malignant, particularly in premenopausal women. Features that raise concern include solid components, papillary projections, septations, and increased blood flow on Doppler imaging. Simple cysts are rarely malignant regardless of size.
Myth 4: Removing your ovaries prevents breast cancer. Fact: While prophylactic oophorectomy reduces breast cancer risk in BRCA1/2 mutation carriers by approximately 50% when performed before natural menopause, it does not eliminate the risk entirely. Furthermore, for women without BRCA mutations, the breast cancer risk reduction from oophorectomy is much more modest (approximately 10-20%) and must be weighed against adverse effects of surgical menopause including increased risks of heart disease, osteoporosis, cognitive changes, and reduced quality of life when performed before the natural age of menopause.
Myth 5: Ovarian cancer is always hereditary. Fact: Only about 20-25% of ovarian cancers are associated with inherited genetic mutations. The most common genetic causes are BRCA1/2 mutations (15-20% of cases) and Lynch syndrome (2-3% of cases). The majority of ovarian cancers (75-80%) occur in women with no known genetic predisposition or family history. However, genetic testing is recommended for all women with epithelial ovarian cancer regardless of family history, as identification of genetic mutations has important implications for treatment selection and family risk assessment.
Myth 6: Fertility treatments increase ovarian cancer risk. Fact: Current evidence suggests that fertility treatments using ovulation-inducing medications do not significantly increase ovarian cancer risk in the general population. Earlier studies suggesting an association likely reflected the underlying risk associated with infertility itself rather than the treatments. Some studies even suggest that successful pregnancy following fertility treatment may reduce risk. However, for BRCA mutation carriers, the impact of fertility treatments on ovarian cancer risk remains an area of active investigation, and caution is warranted.
Myth 7: If you’ve had a hysterectomy, you can’t get ovarian cancer. Fact: A hysterectomy (removal of the uterus alone) does not prevent ovarian cancer unless the ovaries and fallopian tubes are also removed (oophorectomy and salpingectomy). However, even with removal of ovaries and fallopian tubes, a condition called primary peritoneal carcinoma—which is essentially the same disease as ovarian cancer—can still develop from the peritoneal lining that shares an embryologic origin with ovarian tissue. This risk is small but present, particularly in BRCA mutation carriers (1-2% lifetime risk despite risk-reducing surgery).
Myth 8: Talcum powder use is definitely linked to ovarian cancer. Fact: The relationship between talcum powder use in the genital area and ovarian cancer risk remains controversial. Some case-control studies have suggested a modest increased risk (20-30%), while larger cohort studies have found no significant association. The International Agency for Research on Cancer classifies genital use of talc-based body powder as “possibly carcinogenic.” While the potential risk, if present, appears to be small, many experts recommend avoiding talc application to the genital area as a precautionary measure, particularly for women with other risk factors.
Myth 9: All ovarian cancers are the same disease that requires the same treatment. Fact: Ovarian cancer comprises several distinct diseases with different cells of origin, molecular features, prognosis, and treatment responses. The major types include high-grade serous (70%), low-grade serous (5%), endometrioid (10%), clear cell (10%), and mucinous (3%) carcinomas. Treatment is increasingly tailored based on histologic subtype and molecular features. For example, high-grade serous responds well to platinum-based chemotherapy and PARP inhibitors, while clear cell and mucinous types often require different approaches. Precision medicine approaches based on molecular profiling are increasingly used to guide treatment decisions.
Myth 10: Once ovarian cancer recurs, it cannot be cured. Fact: While recurrent ovarian cancer is typically not curable in the majority of cases, a subset of patients with limited recurrence (oligometastatic disease) may achieve long-term disease-free survival or even cure with aggressive surgery and additional treatments. Furthermore, many women with recurrent disease can live for many years with good quality of life through sequential treatments. The treatment landscape has expanded dramatically in recent years with maintenance therapies, targeted treatments, and immunotherapies extending survival significantly for many patients. Some women with BRCA mutations who respond to PARP inhibitors can remain in remission for many years.
Impact on specific populations or professions
Age-specific considerations:
Young women (under 40):
- Represent only 5-10% of ovarian cancer cases
- More likely to have non-epithelial or uncommon epithelial subtypes
- Higher rates of fertility-preserving concerns and psychological impact
- Unique challenges:
- Delayed diagnosis due to low clinical suspicion
- Fertility preservation decisions under time pressure
- Treatment during reproductive years
- Premature menopause from treatments
- Long-term survivorship with treatment effects
- Relationship and family planning disruptions
- Specialized support needed:
- Reproductive endocrinology consultation
- Age-appropriate support groups
- Family building options after treatment
- Long-term health monitoring
Elderly women (over 70):
- Represent approximately 30-40% of cases
- Often diagnosed at more advanced stages
- Frequently undertreated despite evidence of benefit
- Special considerations:
- Balancing treatment intensity with quality of life
- Managing comorbidities alongside cancer
- Polypharmacy concerns
- Functional status impact on treatment tolerance
- Caregiver and social support needs
- End-of-life planning and preferences
- Adaptation strategies:
- Comprehensive geriatric assessment
- Dose modifications when appropriate
- Enhanced supportive care
- Simplified treatment regimens
- Close toxicity monitoring
High-risk genetic populations:
BRCA1/2 mutation carriers:
- BRCA1: 40-60% lifetime ovarian cancer risk
- BRCA2: 10-30% lifetime ovarian cancer risk
- BRCA1-associated cancers typically:
- Occur earlier (average age 50-55)
- High-grade serous histology
- More responsive to platinum and PARP inhibitors
- More likely to have visceral metastases
- Special management considerations:
- Risk-reducing surgery timing discussions
- Enhanced screening until surgery
- Balancing breast and ovarian cancer risks
- Impact on extended family
- Psychosocial support for chronic cancer worry
- Survivor guilt in families with multiple affected members
- Beneficial advances:
- Dramatic benefit from PARP inhibitors
- Improved surgical techniques
- Better hormone replacement options
- Extended genetic testing for family members
Lynch syndrome families:
- 10-12% lifetime ovarian cancer risk
- Primarily endometrioid and clear cell subtypes
- Earlier age of onset (average 45-50)
- Special considerations:
- Multiple cancer risks (colorectal, endometrial, others)
- Complex screening needs
- Surgical decision timing
- Family dynamics around genetic status
- Management approaches:
- Coordination of multiple cancer screenings
- Consideration of extended surgeries
- Immunotherapy may be effective for MMR-deficient tumors
- Family variance in cancer acceptance and prevention
Racial and ethnic disparities:
Black women:
- Later stage at diagnosis
- Less likely to receive standard of care treatment
- Lower rates of genetic testing
- Lower rates of clinical trial participation
- Lower survival rates even with equal treatment
- Contributing factors:
- Healthcare access barriers
- Medical mistrust based on historical abuses
- Provider bias and communication issues
- Socioeconomic factors affecting care quality
- Biological differences in tumor characteristics
- Intervention targets:
- Community education and outreach
- Culturally appropriate support resources
- Implicit bias training for providers
- Patient navigation programs
- Representation in clinical trials
Ashkenazi Jewish women:
- 1 in 40 carry BRCA mutations (vs. 1 in 400 in general population)
- Higher overall ovarian cancer rates
- Cultural and religious considerations:
- Genetic testing decisions influenced by community perspectives
- Reproductive decisions with religious implications
- Marriage prospects concerns in some communities
- Community support mechanisms
- Specialized approaches:
- Community-based education programs
- Rabbi and community leader engagement
- Cultural competence in genetic counseling
- Family-centered care approaches
Hispanic/Latina women:
- Rising incidence rates
- Later stage at diagnosis
- Genetic testing barriers
- Treatment adherence challenges
- Contributing factors:
- Language barriers
- Documentation status concerns
- Cultural beliefs about cancer
- Family role expectations during illness
- Limited culturally tailored resources
- Effective interventions:
- Spanish-language materials and services
- Family-centered decision making
- Community health worker programs
- Faith community partnerships
- Transportation and childcare support
Occupational and social considerations:
Healthcare professionals with ovarian cancer:
- Unique challenges:
- Professional identity disruption
- Self-diagnosis and self-treatment temptations
- Workplace accommodation needs
- Collegiality vs. patient role conflicts
- Medical knowledge as both asset and burden
- Support needs:
- Boundary setting guidance
- Professional identity preservation
- Return to work planning
- Peer support from medical colleagues with cancer
- Privacy management in professional settings
Rural women:
- Multiple barriers:
- Geographic distance to specialized care
- Fewer gynecologic oncologists
- Transportation challenges
- Limited clinical trial access
- Delayed diagnosis from primary care shortages
- Adaptation strategies:
- Telemedicine consultations
- Patient navigation services
- Treatment coordination with local providers
- Lodging support during treatment
- Mobile screening and treatment services
LGBTQ+ individuals:
- Transgender men with retained ovaries remain at risk
- Delayed care due to healthcare avoidance
- Fertility and hormonal management complexities
- Limited research on specific needs
- Healthcare discrimination concerns
- Support approaches:
- Gender-affirming cancer care
- Provider education on inclusive practices
- Recognition of chosen family support structures
- Hormone therapy management during cancer treatment
- Inclusive support group options
This comprehensive report provides an evidence-based overview of ovarian cancer, incorporating current medical understanding, emerging research, and practical considerations. While every effort has been made to ensure accuracy, this information should supplement, not replace, personalized medical advice from healthcare providers.