
⚠️ Disclaimer: The information provided in this article is for educational purposes only and does not constitute medical advice. RevisionTown does not provide diagnosis, treatment, or medical recommendations. Always consult a qualified healthcare professional regarding any medical condition, symptoms, or concerns.
Read More – 🏥 Medical Disclaimer
What is Myocardial Infarction?
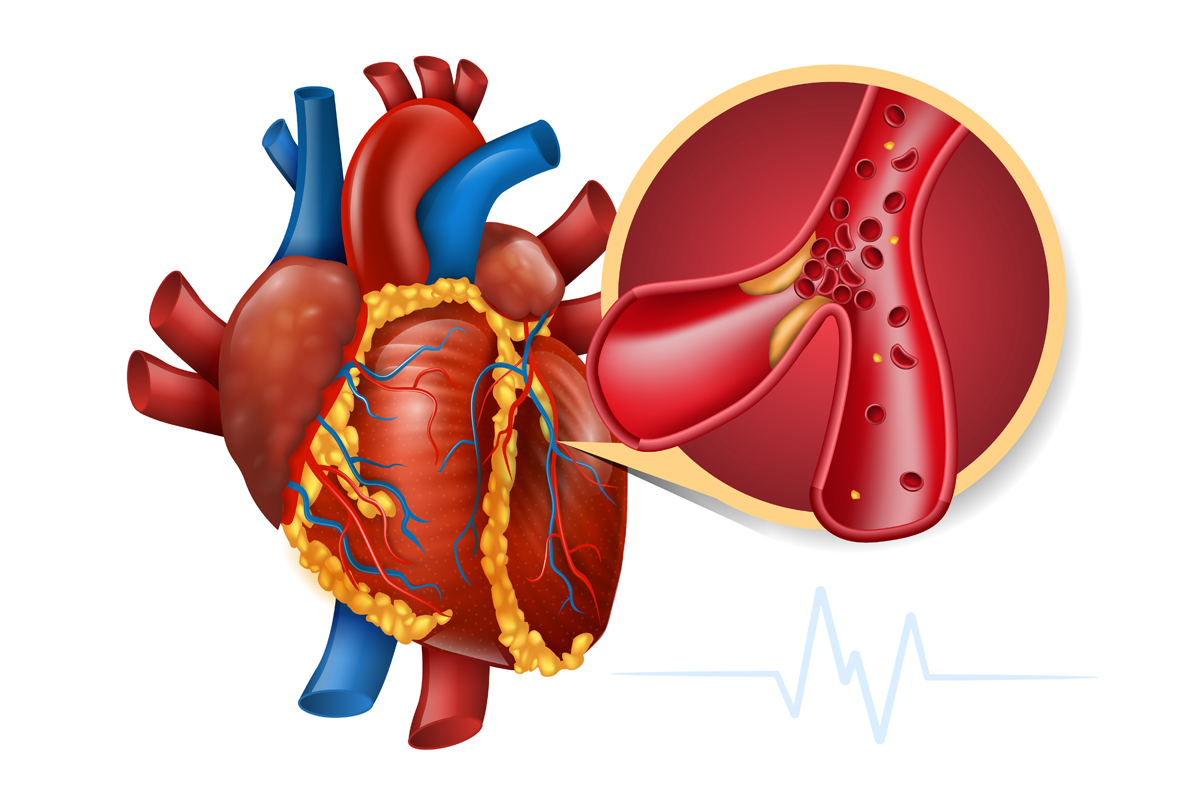
Myocardial infarction (MI), commonly known as a heart attack, is defined as the irreversible death (infarction) of heart muscle cells (myocardium) caused by prolonged lack of oxygen supply (ischemia). It represents one of the most severe manifestations of coronary artery disease and is a life-threatening medical emergency characterized by sudden cardiac death risk.
Affected Body Parts/Organs
MI specifically affects the heart muscle (myocardium). When blood flow to a portion of the heart is obstructed, the cardiac tissue in that region becomes deprived of oxygen and nutrients, leading to tissue death if blood flow is not promptly restored. This damage can affect various heart functions including:
- Contractility (the heart’s pumping ability)
- Electrical conduction system
- Ventricular wall integrity
- Valve function
Prevalence and Significance
Myocardial infarction represents a significant global health burden. The global prevalence of MI approaches 3 million people worldwide, with more than 1 million deaths annually in the United States alone. According to recent systematic reviews, the global prevalence of MI varies by age group, with approximately 3.8% prevalence in individuals under 60 years and 9.5% in those over 60 years of age. MI is notably more prevalent in males than females, with some studies showing nearly five times higher rates in men.
As a leading cause of morbidity and mortality worldwide, MI has enormous economic implications. In 2010, more than 1.1 million hospitalizations following MI were reported in the United States alone, with an estimated direct cost of $450 billion. Its significance extends beyond mortality, as survivors often face long-term complications including heart failure, arrhythmias, and decreased quality of life.
2. History & Discoveries
First Identification
The understanding of myocardial infarction evolved gradually over time. In the early 20th century, acute coronary artery thrombosis (which causes most MIs) was considered invariably fatal. This paradigm began to shift in the first decade of the 1900s with several key observations:
In 1901, Ludwig Krehl reported that coronary thrombosis did not always result in sudden death and noted that symptoms were more severe when arterial occlusion was sudden rather than progressive. He also recognized complications such as ventricular aneurysm formation and myocardial rupture.
In 1910, Russian physicians Obrastzov and Strazhesko published important reports on coronary thrombosis.
In 1912, James Herrick established myocardial infarction as a distinct clinical entity separate from angina pectoris. His work was crucial in identifying the relationship between coronary thrombosis and MI, establishing that patients could survive the condition.
Key Researchers and Breakthroughs
Several key figures and discoveries have shaped our understanding and treatment of MI:
James Herrick – In addition to recognizing MI as a distinct clinical entity, Herrick introduced electrocardiography (invented by Willem Einthoven in 1902) to diagnose MI, which remains a cornerstone of diagnosis today.
Joseph Wearn – Published the first series of 19 patients with clinical diagnosis of MI confirmed at necropsy in 1923.
Desmond Julian – Introduced coronary care units (CCUs) in the 1960s, one of the greatest single advances in the treatment of MI, reducing mortality from approximately 30% to 15% in the early hours.
Andreas Gruentzig – Performed the first successful coronary angioplasty in 1977 using a double-lumen balloon catheter, revolutionizing treatment approaches.
Hugo A. Katus – Discovered troponin T and developed the troponin T assay, which has become the gold standard for diagnosing myocardial damage.
Evolution of Medical Understanding
The understanding of MI has evolved dramatically from a condition considered universally fatal to a treatable emergency with continuously improving outcomes:
1950s-1960s: Recognition that prolonged bed rest (previously prescribed for up to 6 weeks) could lead to complications like deep vein thrombosis. Bernard Lown recommended patients leave their beds earlier, reducing recovery time.
1960s: Introduction of coronary care units with specialized monitoring equipment and trained personnel.
1970s-1980s: Development of thrombolytic therapy to dissolve clots.
1980s-1990s: Advancements in pharmacological interventions (beta-blockers, aspirin, ACE inhibitors) to limit infarct size and improve outcomes.
1990s-Present: Refinement of percutaneous coronary intervention (PCI) techniques, including stents and drug-eluting stents, primary PCI becoming the gold standard treatment for STEMI.
2000s-Present: Improved understanding of genetics, development of high-sensitivity troponin assays, and recognition of different types of MI as codified in the Universal Definition of Myocardial Infarction.
3. Symptoms
Early Symptoms
The early symptoms of MI can vary widely between individuals, but typically include:
Chest Pain or Discomfort: The most common symptom, typically described as pressure, tightness, squeezing, or crushing in the center of the chest lasting more than a few minutes or coming and going.
Radiation of Pain: Pain or discomfort that spreads to the shoulders, arms (especially the left arm), neck, jaw, or back.
Shortness of Breath: May occur with or without chest discomfort.
Cold Sweat: Sudden onset of sweating with cool, clammy skin.
Nausea and Vomiting: Often accompanied by epigastric discomfort.
Lightheadedness or Dizziness: Feeling faint or weak.
Anxiety: A sense of impending doom or extreme anxiety.
Advanced-Stage Symptoms
As an MI progresses without intervention, symptoms may worsen and include:
Severe, Persistent Chest Pain: Unrelieved by rest or nitroglycerin.
Signs of Cardiogenic Shock: Rapidly falling blood pressure, rapid heartbeat, pale skin, confusion, and loss of consciousness.
Heart Failure Symptoms: Increasing shortness of breath, wheezing, rales (crackling sounds in the lungs), peripheral edema, and jugular venous distention.
Arrhythmias: Palpitations, irregular pulse, or sudden loss of consciousness due to dangerous heart rhythms.
Sudden Cardiac Arrest: Complete cessation of cardiac activity requiring immediate resuscitation.
Common vs. Rare Symptoms
Common Symptoms:
- Central chest pain or discomfort (about 90-95% of patients)
- Radiation to left arm, neck, jaw, or back
- Shortness of breath
- Sweating
- Nausea
Less Common or Rare Symptoms:
- Epigastric pain (mistaken for indigestion)
- Isolated pain in the jaw, neck, arm, or back without chest discomfort
- Overwhelming fatigue
- Syncope (fainting) as the presenting symptom
- Altered mental status, especially in elderly patients
- Palpitations as the only symptom
Symptom Progression
MI symptoms typically progress as follows:
Prodromal Phase: Some patients experience warning symptoms days or weeks before the actual MI, including intermittent chest discomfort, fatigue, or shortness of breath with exertion.
Acute Onset: Sudden development of severe chest pain or discomfort, often during physical exertion or emotional stress, but possibly during rest as well.
Peak Phase: Maximum intensity of pain and associated symptoms, typically lasting 30 minutes to several hours if untreated.
Resolution Phase: With appropriate medical intervention, symptoms typically begin to resolve within 20-120 minutes, depending on the treatment approach and timing.
Complications Phase: If untreated or treatment is delayed, symptoms of complications may develop, including arrhythmias, heart failure, or cardiogenic shock.
Special Considerations in Women and Elderly
Women and elderly patients often present with atypical symptoms, leading to delayed diagnosis and treatment:
Women:
- More likely to present without chest pain (30-40% of cases)
- More frequent presentation with fatigue, shortness of breath, upper back or shoulder pain, and nausea
- Often attribute symptoms to stress, influenza, or normal aging
Elderly:
- Higher likelihood of “silent” MI with minimal or no symptoms
- More common presentation with confusion, shortness of breath, syncope, or functional decline
- May have fewer complaints of pain due to altered perception
- Up to 40% of MIs in patients over 85 years may go unrecognized
4. Causes
Biological Causes
The primary biological causes of myocardial infarction include:
Atherosclerosis: The most common underlying cause, characterized by the buildup of cholesterol-laden plaques in the coronary arteries that supply the heart. Approximately 70% of fatal MI cases are attributed to occlusion caused by atherosclerotic plaques.
Plaque Rupture: The rupture of an atherosclerotic plaque exposes thrombogenic material to the bloodstream, initiating an inflammatory response involving monocytes and macrophages.
Thrombosis: Following plaque rupture, a blood clot (thrombus) forms at the site, potentially blocking blood flow completely or partially through the affected coronary artery.
Coronary Artery Spasm: Temporary, sudden narrowing of a coronary artery that can reduce or completely block blood flow to part of the heart muscle.
Coronary Embolism: A blood clot, air bubble, or piece of fatty material that travels through the bloodstream and lodges in a coronary artery, accounts for approximately 2.9% of MI cases.
Coronary Artery Dissection: A tear in the inner lining of a coronary artery that allows blood to flow between the layers of the artery wall, potentially blocking blood flow.
Oxygen Supply-Demand Mismatch: Sometimes called Type 2 MI, occurs when increased oxygen demand or decreased supply leads to myocardial injury despite no acute plaque rupture (e.g., during severe anemia, respiratory failure, or shock).
Environmental Causes
Environmental factors that can trigger or contribute to MI include:
Air Pollution: Exposure to fine particulate matter (PM2.5) and other air pollutants is associated with increased MI risk, particularly in urban environments.
Extreme Weather: Both very cold and very hot temperatures can trigger cardiovascular events.
Workplace Exposures: Certain occupational exposures to chemicals, carbon monoxide, heavy metals, and particulate matter increase MI risk.
Acute Stress: Natural disasters, traumatic events, or significant emotional stressors can trigger MI in vulnerable individuals.
Genetic and Hereditary Factors
Genetic factors play a significant role in MI susceptibility:
Family History: Having a first-degree male relative (father, brother) who experienced MI before age 55 or a female first-degree relative before age 65 significantly increases risk.
Genetic Variants: Genome-wide association studies have identified at least 27 genetic variants associated with increased MI risk. The strongest association has been found with chromosome 9p21, containing genes CDKN2A and CDKN2B.
Specific Gene Associations: Genes with established associations with MI include PCSK9, SORT1, MIA3, LPA, APOA5, LDLR, and numerous others.
Familial Hypercholesterolemia: This inherited condition causes extremely high LDL cholesterol levels and dramatically increases MI risk if untreated.
Other Inherited Conditions: Various genetic disorders affecting lipid metabolism, arterial structure, or clotting factors can predispose to premature MI.
Known Triggers
Several acute triggers can precipitate an MI in individuals with underlying coronary artery disease:
Physical Exertion: Particularly in individuals unaccustomed to regular exercise or during unusually strenuous activity.
Emotional Stress: Acute anger, anxiety, grief, or emotional shock.
Respiratory Infections: Particularly influenza and pneumonia, which can increase risk for several weeks.
Cocaine and Other Stimulant Use: Causes immediate vasoconstriction and can trigger coronary spasm and MI.
Heavy Meal Consumption: Particularly high-fat meals, which can temporarily impair endothelial function.
Sexual Activity: Particularly in sedentary individuals or those with multiple risk factors.
Surgery: Non-cardiac surgery increases MI risk in the perioperative period, especially in patients with pre-existing coronary disease.
5. Risk Factors
Demographic Risk Factors
Age: Risk increases sharply with age. The prevalence of MI in people under 60 years is approximately 3.8%, rising to 9.5% in those over 60 years.
Gender: Men have a significantly higher risk than women, especially in younger age groups. Male prevalence is nearly five times greater than female prevalence in some studies.
Race/Ethnicity: African Americans have higher MI rates than whites. South Asians (from India, Pakistan, Bangladesh) have particularly high rates of premature coronary disease and MI.
Lifestyle Risk Factors
Smoking: One of the most potent modifiable risk factors, accounting for up to 80% of MI cases in patients under 55 years. Both active smoking and secondhand smoke exposure increase risk.
Diet: Diets high in saturated and trans fats, processed foods, refined carbohydrates, and sodium increase MI risk.
Physical Inactivity: Sedentary lifestyle is a major independent risk factor for MI. Regular physical activity reduces risk by 30-50%.
Alcohol Consumption: Heavy drinking increases risk, while moderate consumption (particularly of red wine) may be protective in some populations.
Stress: Chronic psychological stress, depression, anxiety, social isolation, and lack of social support all increase MI risk.
Medical Risk Factors
Hypertension: A major risk factor that accelerates atherosclerosis. Each 20 mmHg increase in systolic blood pressure doubles cardiovascular risk.
Dyslipidemia: Elevated LDL cholesterol and low HDL cholesterol are strong predictors of MI risk.
Diabetes Mellitus: Increases MI risk 2-4 times, with poorer outcomes after MI. Women with diabetes lose their gender-protective effect.
Obesity: Particularly central/abdominal obesity, independently increases risk and exacerbates other risk factors.
Metabolic Syndrome: A cluster of conditions (elevated blood pressure, high blood sugar, excess abdominal fat, abnormal cholesterol levels) that together dramatically increase MI risk.
Pre-existing Conditions
Several pre-existing conditions significantly increase MI risk:
Previous MI or Known Coronary Artery Disease: The strongest predictor of future events.
Heart Failure: Increases MI risk and worsens outcomes.
Peripheral Artery Disease: Indicates widespread atherosclerosis.
Chronic Kidney Disease: Accelerates atherosclerosis through multiple mechanisms.
Autoimmune Disorders: Conditions like rheumatoid arthritis and systemic lupus erythematosus increase MI risk through chronic inflammation.
Chronic Inflammatory Conditions: Psoriasis, inflammatory bowel disease, and others increase cardiovascular risk.
HIV Infection: Associated with accelerated atherosclerosis, both from the infection itself and some antiretroviral medications.
Sleep Apnea: Increases MI risk through multiple mechanisms including intermittent hypoxia and sympathetic activation.
The Role of Multiple Risk Factors
Risk factors for MI have a multiplicative rather than merely additive effect. The INTERHEART study found that nine modifiable risk factors (smoking, lipids, hypertension, diabetes, obesity, diet, physical activity, alcohol consumption, and psychosocial factors) account for over 90% of the attributable risk of MI. Comprehensive risk assessment tools like the Framingham Risk Score or the ASCVD Risk Calculator integrate multiple risk factors to estimate an individual’s 10-year risk of cardiovascular events.
6. Complications
Immediate Complications
Several serious complications can occur immediately or shortly after an MI:
Arrhythmias: Irregular heart rhythms, particularly ventricular fibrillation, are the most common cause of sudden death following MI.
Cardiogenic Shock: Occurs when the heart’s pumping ability is severely compromised, leading to insufficient blood flow to vital organs. Carries high mortality (40-50%) despite modern treatment.
Acute Heart Failure: Heart muscle damage can lead to inadequate pumping function and fluid accumulation in the lungs (pulmonary edema).
Mechanical Complications:
- Ventricular free wall rupture
- Ventricular septal rupture
- Papillary muscle rupture causing acute mitral regurgitation
- Left ventricular aneurysm formation
Pericarditis: Inflammation of the pericardium (the sac surrounding the heart) that may occur 2-3 days post-MI.
Conduction Abnormalities: Various heart block patterns can occur, especially in inferior MI or large anterior MI.
Long-Term Complications
If a patient survives the acute phase, several long-term complications may develop:
Chronic Heart Failure: The leading cause of hospital readmission after MI. May develop immediately or progressively over time as the heart remodels.
Recurrent Ischemia or Reinfarction: Patients with prior MI have substantially increased risk for subsequent events.
Ventricular Remodeling: Progressive enlargement and reshaping of the left ventricle that can lead to heart failure.
Ventricular Aneurysm: Outward bulging of the ventricular wall at the site of infarction, which can lead to blood clots, arrhythmias, and heart failure.
Dressler Syndrome: Autoimmune response occurring weeks after MI, causing pericarditis, pleural effusion, and fever.
Arrhythmias: Chronic rhythm disturbances, particularly atrial fibrillation and ventricular arrhythmias.
Depression and Anxiety: Affect up to 33% of post-MI patients and are associated with poorer outcomes.
Cognitive Decline: More common in patients after MI, particularly in older adults.
Impact on Organs and Overall Health
MI can affect multiple organ systems beyond the heart:
Kidney Function: Cardiorenal syndrome can develop due to decreased cardiac output or contrast media used during procedures.
Brain: MI can lead to embolic stroke if clots form in the heart chambers due to wall motion abnormalities.
Lungs: Pulmonary edema, pleural effusions, and pneumonia are common complications.
Liver: Congestive hepatopathy can develop in severe heart failure following MI.
Peripheral Circulation: Reduced cardiac output can lead to peripheral ischemia.
Metabolic Function: Alterations in glucose metabolism, insulin resistance, and metabolic syndrome often worsen after MI.
Fatality Rates
Despite advances in treatment, MI continues to carry significant mortality risk:
Pre-Hospital Mortality: Approximately one-third of MI patients die before reaching the hospital, primarily from ventricular fibrillation.
In-Hospital Mortality: With modern treatment, in-hospital mortality ranges from 5-10% for all MI patients, but varies significantly based on:
- Type of MI (STEMI vs. NSTEMI)
- Age (increasing exponentially with age)
- Presence of cardiogenic shock (40-50% mortality)
- Time to treatment
- Comorbidities
Long-Term Mortality: One-year mortality after MI is approximately 5-12%. Factors associated with increased long-term mortality include:
- Reduced left ventricular ejection fraction
- Incomplete revascularization
- Recurrent ischemia
- Heart failure
- Chronic kidney disease
- Diabetes
- Older age
7. Diagnosis & Testing
Clinical Evaluation
The initial evaluation of a patient with suspected MI includes:
Detailed History: Focusing on the nature, location, radiation, severity, onset, and duration of symptoms, as well as aggravating and relieving factors.
Physical Examination: Assessment of vital signs, heart sounds (including murmurs, extra sounds, or gallops), signs of heart failure (rales, edema, jugular venous distention), and peripheral perfusion.
Risk Factor Assessment: Evaluation of cardiovascular risk factors to determine the pre-test probability of MI.
Diagnostic Criteria
According to the Fourth Universal Definition of Myocardial Infarction (2018), MI is diagnosed when there is evidence of myocardial necrosis in a clinical setting consistent with myocardial ischemia. The diagnosis requires:
- Detection of a rise and/or fall of cardiac biomarker values (preferably cardiac troponin) with at least one value above the 99th percentile of the upper reference limit, PLUS at least one of the following:
- Symptoms of myocardial ischemia
- New ischemic ECG changes or development of pathological Q waves
- Imaging evidence of new loss of viable myocardium or regional wall motion abnormality
- Identification of an intracoronary thrombus by angiography or autopsy
MIs are classified into five types based on pathophysiology:
- Type 1: Spontaneous MI related to plaque rupture, erosion, or dissection
- Type 2: MI secondary to oxygen supply-demand imbalance
- Type 3: Cardiac death with symptoms suggestive of MI but before biomarkers could be obtained
- Type 4a: MI related to percutaneous coronary intervention
- Type 4b: MI related to stent thrombosis
- Type 5: MI related to coronary artery bypass grafting
Laboratory Tests
Several laboratory tests are essential for MI diagnosis and risk stratification:
Cardiac Biomarkers:
- Troponin T and I: The gold standard for detecting myocardial injury. High-sensitivity assays can detect very small amounts of myocardial damage.
- CK-MB: Less sensitive and specific than troponin but may provide complementary information about timing.
- Myoglobin: Rises early but lacks cardiac specificity.
Additional Laboratory Tests:
- Complete blood count
- Electrolytes
- Renal function tests
- Lipid profile
- Glucose
- Coagulation studies if anticoagulation or thrombolytic therapy is planned
- Inflammatory markers (C-reactive protein)
Imaging Studies
Multiple imaging modalities play important roles in MI diagnosis and management:
Electrocardiography (ECG): The cornerstone of initial evaluation. Key findings include:
- ST-segment elevation (STEMI)
- ST-segment depression or T-wave inversion (NSTEMI)
- New left bundle branch block
- Development of pathological Q waves
- Various patterns of ischemia based on the territory affected
Echocardiography: Provides information on:
- Regional wall motion abnormalities
- Left ventricular systolic and diastolic function
- Valvular function
- Mechanical complications
- Right ventricular involvement
Coronary Angiography: The gold standard for defining coronary anatomy and identifying the culprit lesion(s). Allows for immediate intervention if indicated.
Cardiac Magnetic Resonance Imaging (MRI): Provides detailed assessment of:
- Infarct size and location
- Viability assessment
- Ventricular function
- Microvascular obstruction
- Myocardial edema
Cardiac CT Angiography: Useful for ruling out coronary artery disease in low to intermediate-risk patients. Can also identify non-coronary causes of chest pain.
Nuclear Cardiology Studies: Including:
- SPECT myocardial perfusion imaging
- PET imaging for viability and perfusion
Early Detection Methods
Several approaches can help in early MI detection:
Pre-Hospital ECG: Performed in ambulances by emergency medical services to detect STEMI early and activate cardiac catheterization labs before hospital arrival.
Chest Pain Centers: Specialized units in emergency departments with standardized protocols for rapid evaluation of chest pain patients.
Accelerated Diagnostic Protocols: Combining risk scores, ECG, and serial troponin measurements to identify low-risk patients who can be safely discharged.
Point-of-Care Testing: Allows rapid measurement of cardiac biomarkers in emergency settings.
Wearable Technology: Emerging devices that can monitor heart rhythm and other parameters to potentially detect early signs of MI.
Effectiveness of Diagnostic Methods
The effectiveness of diagnostic methods varies:
ECG: Highly specific (95-97%) but low sensitivity (approximately 30%) for detecting MI.
Troponin: Current high-sensitivity assays have excellent sensitivity (>90%) and specificity (>90%) when used in the appropriate clinical context.
Echocardiography: Sensitivity of 90-95% for detecting wall motion abnormalities in acute MI, but abnormalities are not specific to acute MI.
Coronary Angiography: Nearly 100% sensitive for identifying significant coronary lesions but invasive and carries risks.
Multimodality Imaging: The combination of clinical assessment, ECG, biomarkers, and appropriate imaging yields the highest diagnostic accuracy.
8. Treatment Options
Emergency Management
The immediate treatment of suspected MI focuses on relieving symptoms, limiting infarct size, and preventing complications:
Initial Stabilization:
- Supplemental oxygen for patients with hypoxemia (oxygen saturation <90%)
- Aspirin (162-325 mg) administered immediately
- Nitroglycerin for ongoing chest pain
- Morphine or other opioids for pain unresponsive to nitrates
- Beta-blockers for patients without contraindications
- Statins initiated early
Reperfusion Strategies for STEMI:
- Primary Percutaneous Coronary Intervention (PCI): The preferred strategy if performed within 90-120 minutes of first medical contact
- Fibrinolytic Therapy: If primary PCI cannot be performed within the recommended timeframe and there are no contraindications
- Pharmaco-invasive Strategy: Fibrinolysis followed by routine coronary angiography within 3-24 hours
Management of NSTEMI:
- Risk stratification using validated scores (TIMI, GRACE)
- Early invasive strategy for high-risk patients
- Initial conservative strategy with selective invasive approach for low-risk patients
Medications
Several medication classes are used in the acute and long-term management of MI:
Antiplatelet Agents:
- Aspirin: Indefinite therapy for all patients without contraindications
- P2Y12 Inhibitors (clopidogrel, prasugrel, ticagrelor): Dual antiplatelet therapy with aspirin for 6-12 months after MI
- Glycoprotein IIb/IIIa Inhibitors: For high-risk PCI situations
Anticoagulants:
- Unfractionated Heparin
- Low Molecular Weight Heparin (enoxaparin)
- Direct Thrombin Inhibitors (bivalirudin)
- Factor Xa Inhibitors (fondaparinux)
Beta-Blockers:
- Reduce myocardial oxygen demand
- Decrease risk of arrhythmias
- Reduce infarct size and improve survival
ACE Inhibitors/ARBs:
- Reduce ventricular remodeling
- Improve survival, particularly in patients with reduced ejection fraction or anterior MI
Statins:
- High-intensity statin therapy recommended for all patients after MI
- Reduce recurrent events and improve survival
Aldosterone Antagonists:
- For patients with ejection fraction ≤40% and heart failure or diabetes
Other Medications:
- Nitrates: For symptom relief
- Calcium Channel Blockers: For hypertension or angina if beta-blockers are contraindicated
- PCSK9 Inhibitors: For patients not reaching LDL goals on maximum statin therapy
Surgical Interventions
Several surgical options may be considered for MI patients:
Coronary Artery Bypass Grafting (CABG):
- Preferred for patients with left main coronary artery disease
- Often indicated for three-vessel disease, especially with diabetes or reduced left ventricular function
- May be necessary for failed PCI or mechanical complications
Mechanical Circulatory Support:
- Intra-Aortic Balloon Pump: For cardiogenic shock or mechanical complications
- Ventricular Assist Devices: For refractory cardiogenic shock
- Extracorporeal Membrane Oxygenation (ECMO): For profound cardiogenic shock with multi-organ failure
Surgery for Mechanical Complications:
- Ventricular septal defect repair
- Papillary muscle or ventricular free wall rupture repair
- Left ventricular aneurysm repair
Emerging Treatments
Several innovative treatments are being investigated or recently implemented:
Novel Antiplatelet and Anticoagulant Strategies:
- Shorter duration DAPT with newer generation stents
- Low-dose anticoagulation plus antiplatelet therapy to reduce recurrent events
Cell-Based Therapies:
- Stem cell transplantation to improve cardiac regeneration
- Growth factor therapy to stimulate endogenous repair mechanisms
Gene Therapy:
- Targeting specific pathways involved in cardiac repair and regeneration
Device-Based Therapies:
- Bioresorbable vascular scaffolds
- Novel stent designs
- Left ventricular restraint devices to prevent adverse remodeling
Anti-Inflammatory Therapies:
- Targeted anti-inflammatory agents (e.g., canakinumab, colchicine) to reduce recurrent events after MI
Metabolic Modulation:
- Agents targeting cardiac metabolism to improve efficiency and function
Remote Ischemic Conditioning:
- Non-invasive technique to reduce reperfusion injury
9. Prevention & Precautionary Measures
Primary Prevention
Primary prevention aims to prevent the first occurrence of MI through risk factor modification:
Lifestyle Modifications:
- Smoking Cessation: The single most effective intervention, reducing risk by 36% within 2 years
- Regular Physical Activity: At least 150 minutes of moderate-intensity or 75 minutes of vigorous-intensity aerobic activity weekly
- Heart-Healthy Diet: Mediterranean, DASH, or other diets rich in fruits, vegetables, whole grains, and lean proteins
- Weight Management: Maintaining BMI between 20-25 kg/m² and waist circumference <94 cm for men and <80 cm for women
- Stress Management: Regular relaxation techniques, adequate sleep, and psychological support
Risk Factor Control:
- Hypertension Management: Target BP <130/80 mmHg for most patients
- Diabetes Management: Tight glycemic control (HbA1c <7%) and use of cardioprotective agents (SGLT2 inhibitors, GLP-1 receptor agonists)
- Lipid Management: Risk-based LDL-C targets, generally <70 mg/dL for high-risk individuals
- Obesity Treatment: Weight loss strategies including lifestyle, pharmacotherapy, and bariatric surgery when indicated
Preventive Medications:
- Aspirin: Low-dose (75-100 mg) for selected high-risk patients without increased bleeding risk
- Statins: For primary prevention based on calculated 10-year ASCVD risk
- Other Lipid-Lowering Therapies: For high-risk patients not reaching goals on statins
Secondary Prevention
Secondary prevention focuses on preventing recurrent MI in those who have already experienced one:
Comprehensive Cardiac Rehabilitation:
- Supervised exercise training
- Nutritional counseling
- Psychological support
- Smoking cessation programs
- Risk factor modification education
Aggressive Risk Factor Management:
- More intensive targets for BP, lipids, and glucose
- Complete smoking cessation
- Adherence to heart-healthy lifestyle
Medication Adherence:
- Long-term compliance with prescribed therapies
- Regular follow-up to adjust medications as needed
- Medication reconciliation at each visit
Ongoing Monitoring:
- Regular assessment of cardiac symptoms
- Periodic functional assessment
- Surveillance for complications
Environmental Precautions
Environmental factors can influence MI risk and should be addressed:
Air Quality Awareness:
- Limiting outdoor activities during high pollution days
- Using air purifiers in areas with poor air quality
- Advocating for environmental regulations to reduce pollution
Temperature Extremes:
- Avoiding excessive exertion in very hot or cold conditions
- Appropriate clothing and hydration
- Adequate heating and cooling in living environments
Workplace Modifications:
- Ergonomic adaptations to reduce physical stress
- Stress management programs
- Cardiovascular health promotion at work
Screening and Early Detection
Various screening approaches can identify individuals at risk for MI:
Cardiovascular Risk Assessment:
- Regular calculation of 10-year cardiovascular risk using validated tools
- Earlier and more frequent screening for those with family history
Subclinical Atherosclerosis Detection:
- Coronary artery calcium scoring
- Carotid intima-media thickness measurement
- Ankle-brachial index
Advanced Lipid Testing:
- Lipoprotein(a)
- Apolipoprotein B
- LDL particle number and size
Inflammatory Markers:
- High-sensitivity C-reactive protein
- Other emerging biomarkers
Genetic Testing:
- For familial hypercholesterolemia and other genetic disorders
- Polygenic risk scores for coronary artery disease
Effectiveness of Prevention Strategies
The impact of prevention strategies on MI incidence varies:
Population-Level Interventions:
- Smoking bans in public places: 10-20% reduction in MI hospitalizations
- Trans fat restrictions: 4-8% reduction in cardiovascular events
- Salt reduction initiatives: 2-5% reduction in cardiovascular events
Individual-Level Interventions:
- Smoking cessation: 36% reduction in recurrent MI
- Statin therapy: 25-35% reduction in major cardiovascular events
- Antihypertensive therapy: 20-25% reduction in MI risk
- Regular physical activity: 20-30% reduction in coronary events
- Mediterranean diet: 30% reduction in cardiovascular events
Comprehensive Approach:
- Multifactorial risk reduction strategies can reduce MI risk by 60-80% in high-risk individuals
- Cardiac rehabilitation after MI reduces mortality by approximately 20-25%
10. Global & Regional Statistics
Global Incidence and Prevalence
Myocardial infarction represents a significant global health burden:
Global Prevalence:
- The global prevalence of MI is approximately 3.8% in people under 60 years and 9.5% in those over 60 years
- More than 3 million people worldwide are affected by MI annually
Global Incidence:
- More than 3 million individuals develop ST-elevation MI each year
- More than 4 million people present with ST-elevation MI pathology
Regional Variations:
- Highest rates in Eastern Europe, Central Asia, and the Middle East
- Intermediate rates in North America, Western Europe, and Australia
- Historically lower but rapidly increasing rates in South and East Asia, Latin America, and Africa
Mortality and Survival Rates
Despite advances in treatment, MI continues to have significant mortality:
Global Mortality:
- Cardiovascular diseases are the leading cause of death globally, accounting for 17.9 million deaths annually
- MI specifically accounts for a substantial portion of these deaths
Regional Mortality Differences:
- Highest in low and middle-income countries (LMIC), where 80% of cardiovascular deaths occur
- Declining in high-income countries but increasing in many LMIC
Case Fatality Rates:
- Approximately one-third of MI patients die before reaching the hospital
- In-hospital mortality ranges from 5-10% in developed countries to 15-20% in some LMIC
- One-year mortality post-MI ranges from 5-12%
Survival Trends:
- Significant improvements in survival in recent decades in developed countries
- 30-day mortality has declined from 20% in the 1980s to 5-7% currently in many high-income countries
- Survival gains attributed to early reperfusion, modern pharmacotherapy, and secondary prevention
Country-Wise Comparison
MI epidemiology shows significant variations between countries:
High-Income Countries:
- United States: In 2022, approximately 702,880 people died from heart disease, representing about 1 in every 5 deaths. The economic burden is substantial, with costs related to heart disease estimated at $252.2 billion from 2019 to 2020.
- Western Europe: Lower rates than the US, with significant north-south gradient (higher in northern countries)
- Japan: Among the lowest rates of coronary heart disease and MI globally
Middle-Income Countries:
- China: Rapidly increasing rates with urbanization and lifestyle changes
- Russia and Eastern Europe: Among the highest rates globally
- Brazil and Mexico: Intermediate and increasing rates
Low-Income Countries:
- Limited data but growing burden, particularly in urban areas
- Earlier age of onset compared to high-income countries
- Higher case fatality due to limited healthcare resources
Trends Over Time
MI epidemiology has shown notable trends over recent decades:
Developed Countries:
- Steady decline in age-adjusted incidence since the 1970s
- Shift toward NSTEMI rather than STEMI presentation
- Significant improvements in case fatality rates
- Rising proportion of MI in elderly populations
- Concerning increases in younger adults (under 55), particularly women
Developing Countries:
- Rising incidence as populations adopt Western lifestyles
- Younger average age of presentation
- Increasing prevalence of risk factors, particularly smoking, diabetes, and obesity
- Limited access to modern treatments resulting in higher mortality
Global Projections:
- Cardiovascular disease burden expected to increase by 50% by 2030
- Shifts in geographical distribution with largest increases in South Asia, Middle East, and Africa
- Growing economic impact, particularly in low and middle-income countries
11. Recent Research & Future Prospects
Latest Advancements in Treatment
Recent years have seen significant advances in MI treatment approaches:
Interventional Cardiology:
- Bioresorbable Vascular Scaffolds: Temporary stents that dissolve after healing
- Drug-Coated Balloons: For selected lesions without requiring stent implantation
- Novel Stent Designs: Including ultra-thin struts and specialized coatings
- Complete Revascularization: Growing evidence for treating non-infarct arteries during primary PCI
- Transcatheter Structural Interventions: For mechanical complications of MI
Pharmacotherapy:
- PCSK9 Inhibitors: Dramatically reduce LDL cholesterol and improve outcomes
- Anti-Inflammatory Therapies: Colchicine shown to reduce cardiovascular events after MI
- Novel Antithrombotic Strategies: Including shortened DAPT duration with newer-generation stents
- SGLT2 Inhibitors and GLP-1 Receptor Agonists: Shown to reduce cardiovascular events in high-risk patients
Imaging and Diagnostic Advances:
- High-Sensitivity Troponin Assays: Allow earlier diagnosis and rule-out of MI
- Advanced Intracoronary Imaging: OCT and IVUS guiding interventions
- Cardiac MRI: Improved techniques for assessing viability and microvascular obstruction
- Artificial Intelligence: For ECG interpretation and risk prediction
Ongoing Studies
Numerous ongoing clinical trials are investigating promising approaches:
Regenerative Medicine:
- Stem cell therapies using various cell types and delivery methods
- Growth factor and cytokine therapies to stimulate endogenous repair
- Tissue engineering approaches to replace damaged myocardium
- Exosome and microvesicle therapies for cardiac repair
Novel Drug Targets:
- Therapies targeting mitochondrial function
- RNA-based therapies to modify cardiac repair
- Selective anti-inflammatory approaches
- NLRP3 inflammasome inhibitors
Precision Medicine Approaches:
- Genetic and biomarker-guided therapy selection
- Pharmacogenomic testing to optimize medication selection
- Personalized risk stratification models
- Tailored rehabilitation programs
Digital Health and Remote Monitoring:
- Wearable technologies for early detection of ischemia
- Smartphone-based cardiac rehabilitation
- Telemedicine approaches for post-MI care
- Implantable monitoring devices for high-risk patients
Future Medical Possibilities
Several exciting possibilities may transform MI care in the coming decades:
Preventive Approaches:
- Genomic Medicine: CRISPR and other gene-editing technologies to correct genetic risk factors
- Vaccines: Against atherosclerosis components
- Nanotechnology: Targeted drug delivery to atherosclerotic plaques
- Precision Prevention: Tailored to individual genetic and environmental risk profiles
Diagnostic Innovations:
- Liquid Biopsies: Blood tests to detect atherosclerotic plaque vulnerability
- Molecular Imaging: To identify high-risk plaques before rupture
- Artificial Intelligence: Integration of multiple data sources for personalized risk prediction
- Point-of-Care Testing: Immediate diagnosis in community settings
Therapeutic Breakthroughs:
- Cardiac Regeneration: Inducing cardiomyocyte proliferation and repair
- 3D Bioprinting: Creating functional cardiac tissue
- Robot-Assisted Interventions: More precise and less invasive procedures
- Gene Therapy: Correcting specific genetic defects contributing to coronary disease
Progress Toward Better Outcomes
Significant progress has been made in improving MI outcomes over recent decades:
Systems of Care:
- Regional STEMI networks with rapid transfer protocols
- Pre-hospital triage and direct transport to PCI-capable centers
- Standardized quality metrics and public reporting
- Implementation of evidence-based protocols
Risk Stratification:
- More sophisticated models incorporating biomarkers, imaging, and genetic factors
- Artificial intelligence algorithms predicting individual patient outcomes
- Identification of high-risk subgroups requiring intensive management
Secondary Prevention:
- Comprehensive cardiac rehabilitation programs
- Digital health interventions to improve medication adherence
- Community-based prevention initiatives
- Policy changes to support heart-healthy environments
12. Interesting Facts & Lesser-Known Insights
Uncommon Knowledge
Several fascinating aspects of MI are not widely known:
Silent MIs: Approximately 20-30% of all MIs are asymptomatic or have atypical symptoms, often discovered incidentally during subsequent testing. These “silent” MIs carry a prognosis similar to symptomatic events.
Circadian Patterns: MI occurrence follows a circadian rhythm with a peak incidence in the morning hours (6 AM to noon), likely related to morning surges in catecholamines, blood pressure, and platelet aggregability.
Seasonal Variation: MI rates increase during winter months in both northern and southern hemispheres, with peaks often correlating with lowest temperatures and respiratory infection seasons.
Takotsubo Cardiomyopathy: Also known as “broken heart syndrome,” this condition mimics MI but typically occurs after extreme emotional stress without coronary blockage. It predominantly affects post-menopausal women.
Protective Effect of Prior Angina: Patients who experience angina before their MI often have smaller infarcts and better outcomes, a phenomenon called “ischemic preconditioning.”
Myths vs. Medical Facts
Several misconceptions exist about MI:
Myth: MIs always cause crushing chest pain. Fact: Up to 30% of MIs present with minimal or atypical symptoms, particularly in women, elderly, and those with diabetes.
Myth: Young people don’t have heart attacks. Fact: While less common, MI can occur at any age, with increasing incidence in young adults due to premature atherosclerosis, substance use, and genetic factors.
Myth: Rest is the best treatment after MI. Fact: Early mobilization and cardiac rehabilitation with structured exercise are associated with better outcomes.
Myth: Once you have an MI, you must avoid all physical activity. Fact: Regular, appropriate exercise is one of the most effective strategies for preventing recurrent events.
Myth: Women don’t need to worry about heart attacks until after menopause. Fact: While pre-menopausal women have lower rates than men, MI remains a leading cause of death in women of all ages.
Population-Specific Insights
MI manifests differently and has varying impacts across populations:
Gender Differences:
- Women typically present with MI 7-10 years later than men
- Women more commonly experience atypical symptoms (fatigue, shortness of breath, back pain)
- Women have higher mortality rates after MI, particularly younger women
- Women less likely to receive guideline-directed therapies
Ethnic/Racial Variations:
- South Asians have higher rates of MI at younger ages
- African Americans have higher hypertension-related MI
- Hispanic populations show the “Hispanic paradox” of lower than expected MI rates despite risk factor prevalence
- East Asians have lower rates of MI but higher rates of hemorrhagic stroke
Socioeconomic Factors:
- Lower socioeconomic status strongly associated with higher MI incidence and mortality
- Educational level inversely correlates with MI risk
- Access to healthcare substantially impacts outcomes
- Social determinants of health explain much of the variation in MI outcomes not accounted for by traditional risk factors
Geographic Patterns:
- Rural areas typically have higher MI mortality due to delayed access to care
- “Stroke Belt” in southeastern US also shows higher MI rates
- Urban air pollution associated with higher MI incidence in metropolitan areas
- Remote regions face challenges in implementing optimal STEMI care systems
Occupational Considerations
Certain occupations have particular associations with MI risk:
High-Stress Professions:
- First responders (police, firefighters, paramedics) have higher MI rates
- Air traffic controllers and other high-responsibility positions show increased risk
- Executive positions with high demand/low control dynamics
Shift Workers:
- Night shift and rotating shifts associated with 40% higher MI risk
- Disruption of circadian rhythms affects multiple cardiovascular parameters
Manual Labor:
- Occupations requiring high physical exertion without adequate conditioning
- Jobs exposing workers to extreme temperatures
- Occupations with high noise levels show increased MI risk
Chemical Exposures:
- Carbon disulfide in rayon manufacturing
- Lead and cadmium exposure
- Particulate matter exposure in mining, construction, and manufacturing
Professional Drivers:
- Long-haul truck drivers have multiple risk factors (sedentary behavior, poor diet, stress)
- Taxi and bus drivers in urban areas exposed to high pollution levels
References
Thygesen K, et al. Fourth Universal Definition of Myocardial Infarction (2018). Journal of the American College of Cardiology. 2018;72(18):2231-2264.
Rajati F, et al. The prevalence of myocardial infarction in the elderly: A systematic review and meta-analysis. ARYA Atherosclerosis. 2024;20(2):61-73.
Martin SS, et al. 2024 heart disease and stroke statistics: a report of US and global data from the American Heart Association. Circulation. 2024;149:e347-913.
Reddy K, Khaliq A, Henning RJ. Recent advances in the diagnosis and treatment of acute myocardial infarction. World Journal of Cardiology. 2015;7(5):243-276.
Ibanez B, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. European Heart Journal. 2018;39(2):119-177.
Collet JP, et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. European Heart Journal. 2021;42(14):1289-1367.
World Health Organization. Cardiovascular diseases fact sheet. 2021.
Centers for Disease Control and Prevention. Heart Disease Facts. 2025.
Herrick JB. Clinical features of sudden obstruction of the coronary arteries. JAMA. 1912;59:2015-2022.
Julian DG. Treatment of cardiac arrest in acute myocardial ischemia and infarction. Lancet. 1961;2:840-844.
De Luca G, et al. Time delay to treatment and mortality in primary angioplasty for acute myocardial infarction: every minute of delay counts. Circulation. 2004;109(10):1223-1225.
Yusuf S, et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case-control study. Lancet. 2004;364(9438):937-952.