
⚠️ Disclaimer: The information provided in this article is for educational purposes only and does not constitute medical advice. RevisionTown does not provide diagnosis, treatment, or medical recommendations. Always consult a qualified healthcare professional regarding any medical condition, symptoms, or concerns.
Read More – 🏥 Medical Disclaimer
What is Ménière’s Disease?
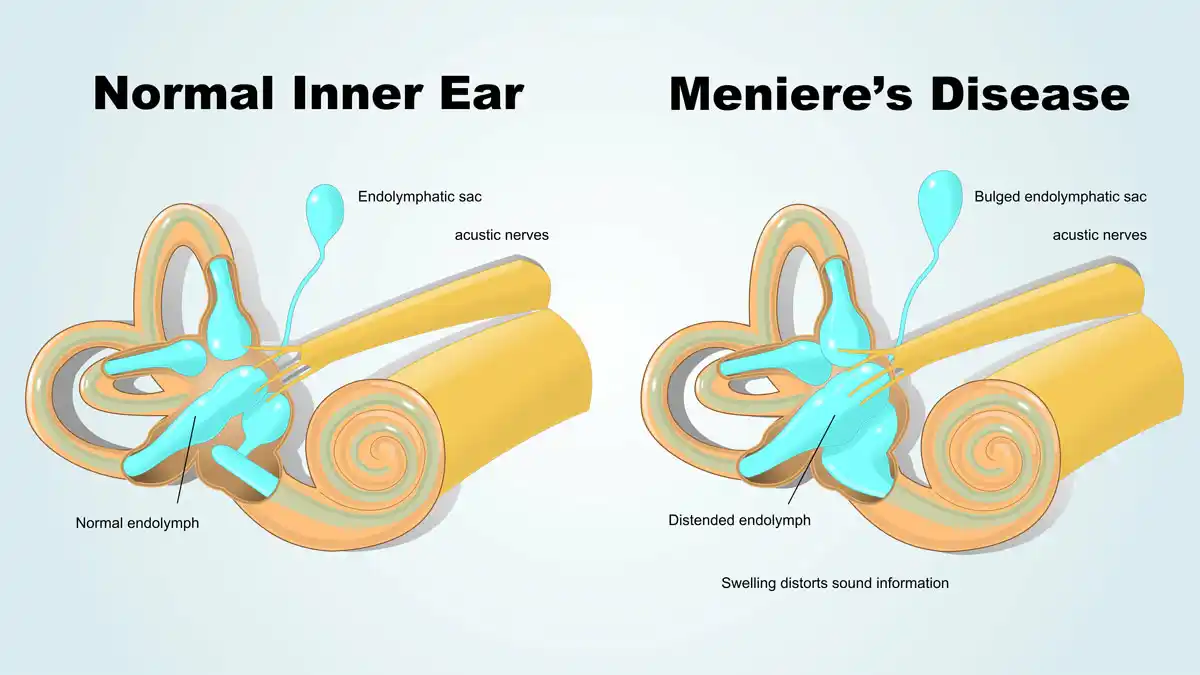
Ménière’s disease is a chronic inner ear disorder characterized by episodic vertigo, fluctuating sensorineural hearing loss, tinnitus, and aural fullness. It is caused by an abnormal accumulation of endolymph fluid in the membranous labyrinth of the inner ear, a condition known as endolymphatic hydrops. This excess fluid disrupts the normal balance and hearing functions of the inner ear, leading to the characteristic symptoms of the disease.
Affected Body Parts/Organs
Ménière’s disease primarily affects the inner ear, specifically the labyrinth, which contains both the cochlea (responsible for hearing) and the vestibular system (responsible for balance). The endolymphatic sac, which helps regulate fluid in the inner ear, is often implicated in the pathophysiology of the disease.
Prevalence and Significance
Ménière’s disease is relatively rare, affecting approximately 0.2% of the population in the United States, or about 615,000 people. Annually, around 45,500 new cases are diagnosed in the U.S. The prevalence varies internationally, with reported rates ranging from 17-34.5 per 100,000 in Japan to 200 per 100,000 in the United States. The disease typically appears between ages 40-60, though it can occur at any age. The impact of Ménière’s disease on quality of life can be substantial, as the unpredictable nature of attacks can cause significant anxiety and disrupt daily activities. Patients with Ménière’s disease report higher rates of anxiety and depression compared to the general population.
2. History & Discoveries
First Identification
Ménière’s disease was first described in 1861 by French physician Prosper Ménière. Before his discovery, vertigo and balance disorders were generally attributed to brain conditions, often referred to as “apoplectiform cerebral congestion.” Ménière was the first to recognize that symptoms of vertigo, hearing loss, and tinnitus could originate from the inner ear rather than the brain.
Key Discoveries
Prosper Ménière made his groundbreaking discovery while serving as the director of the first school for the deaf-mute in Paris. In his historical paper presented to the French Academy of Medicine, he described patients with episodic vertigo and hearing loss, and notably mentioned the postmortem examination of a young girl who experienced vertigo after a hemorrhage into the inner ear. This was revolutionary as it was the first evidence linking vertigo to inner ear damage.
The histopathological correlate of the disease—endolymphatic hydrops—was not discovered until the 1930s, about 70 years after Ménière’s initial description. This discovery confirmed that the excess fluid in the inner ear was the underlying pathological finding in patients with the disease.
Evolution of Understanding
Over the decades, our understanding of Ménière’s disease has evolved significantly:
- In the early 20th century, the focus was primarily on identifying the disease and its symptoms.
- By the mid-20th century, diagnostic criteria were established, though they have been revised multiple times since then.
- Modern advances in imaging technology, particularly MRI techniques developed in the last decade, have allowed visualization of endolymphatic hydrops in living patients, something previously only possible in postmortem examinations.
- Recent genetic research has identified several genes linked to familial Ménière’s disease, suggesting a genetic component to the condition.
- Current research explores the roles of autoimmunity, allergies, and vascular factors in the development of the disease.
3. Symptoms
Early Symptoms vs. Advanced-Stage Symptoms
Early Symptoms:
- Episodic vertigo (spinning sensation) lasting 20 minutes to 24 hours
- Fluctuating hearing loss, often affecting lower frequencies first
- Tinnitus (ringing, roaring, or buzzing in the ear)
- Aural fullness (feeling of pressure in the affected ear)
- Nausea and vomiting during vertigo attacks
Advanced-Stage Symptoms:
- Permanent hearing loss that progresses over time
- More frequent or more severe vertigo attacks
- Constant or more severe tinnitus
- Development of balance problems between vertigo episodes
- Possible spread to the other ear (bilateral disease)
- “Drop attacks” (Tumarkin’s otolithic crisis) in some cases, where patients suddenly fall without warning
Common vs. Rare Symptoms
Common Symptoms:
- Vertigo (affects up to 96% of patients)
- Tinnitus (affects about 91% of patients)
- Hearing loss (affects approximately 88% of patients)
- Aural fullness/pressure
- Nausea and vomiting during attacks
Rare Symptoms:
- Drop attacks (Tumarkin’s otolithic crisis)
- Visual disturbances or sensitivity to light during attacks
- Headaches similar to migraine
- Cognitive difficulties (“brain fog”) during or after attacks
- Severe anxiety or panic during attacks
Symptom Progression
The progression of Ménière’s disease is typically divided into stages:
Stage 1 (Early):
- Sudden, unpredictable episodes of vertigo lasting 20 minutes to several hours
- Fluctuating hearing loss that returns to normal between attacks
- Tinnitus and aural fullness that may intensify before or during attacks
Stage 2 (Intermediate):
- Continued vertigo attacks
- Fluctuating but progressively worsening hearing loss
- Persistent tinnitus and aural fullness
Stage 3 (Late):
- Less frequent vertigo attacks or complete cessation of vertigo
- Permanent hearing loss (typically moderate to severe)
- Persistent tinnitus
- Chronic balance problems even between vertigo attacks
The disease typically progresses over 5-15 years, with symptom patterns varying considerably between individuals. Some patients experience symptom-free periods (remissions) lasting months or even years.
4. Causes
Biological and Environmental Causes
The exact cause of Ménière’s disease remains unknown, but it is generally considered to be multifactorial, with both biological and environmental factors playing roles:
Biological Factors:
- Abnormal fluid homeostasis in the inner ear, leading to endolymphatic hydrops
- Impaired absorption function of the endolymphatic sac
- Possible overproduction or underabsorption of endolymph
- Vascular abnormalities affecting blood supply to the inner ear
- Inner ear membrane ruptures or biomechanical changes
Environmental Factors:
- Viral infections (including herpes viruses, cytomegalovirus)
- Head trauma
- Allergic reactions
- Stress (can trigger or worsen attacks)
- Dietary factors (salt, caffeine, alcohol)
- Barometric pressure changes
Genetic and Hereditary Factors
While most cases of Ménière’s disease are sporadic, approximately 5-15% of cases show familial clustering, suggesting a genetic component:
- Multiple genes have been identified in association with Ménière’s disease
- Genes linked to familial Ménière’s disease include FAM136A, DTNA, PRKCB, COCH, DPT, SEMA3D, OTOG, and LSAMP
- In sporadic cases, mutations have been found in genes including GJB2, SLC26A4, and CLDN14
- Genetic studies show that Ménière’s disease likely has both monogenic forms (in isolated families) and polygenic forms (in most familial and sporadic cases)
- The pattern of inheritance in familial cases is most often autosomal dominant
Known Triggers and Exposure Risks
Several factors can trigger Ménière’s attacks or increase the risk of developing the disease:
Attack Triggers:
- High sodium intake
- Stress and anxiety
- Fatigue and exhaustion
- Alcohol consumption
- Caffeine
- Allergic reactions
- Barometric pressure changes (weather changes)
- Hormonal fluctuations (menstruation, pregnancy)
Exposure Risks:
- History of viral infections of the inner ear
- Previous head trauma
- Autoimmune disorders
- Allergies
- Migraine headaches
5. Risk Factors
Demographic Risk Factors
Age:
- Peak incidence is between 40-60 years of age
- Relatively uncommon in children and young adults
- Can occur in elderly individuals, though diagnosis may be complicated by other age-related balance and hearing issues
Gender:
- Some studies show a slightly higher prevalence in women
- The female-to-male ratio is approximately 1.3:1
Ethnicity:
- Higher prevalence reported in white populations
- Lower reported rates in Asian populations
- Limited data on prevalence in other ethnic groups
Geographical Factors:
- Variation in prevalence across different countries
- Higher reported rates in the United States and United Kingdom
- Lower reported prevalence in Japan
Environmental and Occupational Risk Factors
Environmental:
- Living in areas with significant barometric pressure fluctuations
- Exposure to certain toxins and chemicals that may affect inner ear function
- Noise exposure (may contribute to hearing loss component)
Occupational:
- Jobs with high stress levels may increase risk or trigger attacks
- Occupations with exposure to loud noise
- Work environments with changing pressure (aviation, diving)
- Certain occupations may be more difficult for those with Ménière’s disease due to safety concerns regarding unpredictable vertigo attacks
Impact of Pre-existing Conditions
Several pre-existing conditions may increase the risk of developing Ménière’s disease or influence its presentation:
Medical Conditions:
- Migraines (significant overlap with vestibular migraine)
- Autoimmune disorders (rheumatoid arthritis, lupus)
- Allergies and allergic disorders (allergic rhinitis, asthma)
- Thyroid disorders
- Syphilis (can cause symptoms similar to Ménière’s)
Other Inner Ear Conditions:
- History of other inner ear disorders
- Previous inner ear infections or trauma
- Otosclerosis
Vascular Conditions:
- Hypertension
- Vascular disorders affecting microcirculation
- Atherosclerosis
6. Complications
Potential Complications
Ménière’s disease can lead to several complications that affect quality of life and functioning:
Physical Complications:
- Permanent hearing loss, often progressing to moderate or severe levels
- Chronic balance problems even between acute vertigo episodes
- Increased risk of falls, especially in elderly patients
- “Drop attacks” (Tumarkin’s otolithic crisis), causing sudden falls without warning
Psychological Complications:
- Anxiety and depression (significantly higher rates than general population)
- Social isolation due to unpredictable nature of attacks
- Fear of having attacks in public (anticipatory anxiety)
- Reduced quality of life
- Sleep disturbances
Occupational and Lifestyle Complications:
- Inability to drive or operate heavy machinery safely
- Work restrictions or disability
- Limitations on travel
- Restricted participation in certain activities and social events
Long-term Impact on Health
The long-term impact of Ménière’s disease varies significantly between individuals:
Hearing:
- Progressive hearing loss is common, typically starting in the low frequencies
- 10-50% of patients develop bilateral disease (affecting both ears) over time
- Permanent hearing loss may require hearing aids or other assistive devices
Balance:
- Chronic balance problems may persist even after vertigo attacks cease
- Vestibular rehabilitation therapy may be needed to improve balance function
- Compensation by the central nervous system can improve balance over time
Quality of Life:
- Most patients learn to manage the condition over time with treatment
- Some experience natural remission after 5-10 years
- Others develop coping strategies that allow them to maintain normal activities
- A small percentage experience severe, treatment-resistant symptoms
Disability or Fatality Rates
Ménière’s disease is not life-threatening, but it can cause significant disability:
- About 25-50% of patients experience some degree of work-related disability
- “Drop attacks” can lead to injuries from falls
- Physical disability is usually related to balance problems and unpredictable vertigo
- Mental health impacts can be as disabling as physical symptoms
- Patients with bilateral disease often experience greater disability
- The condition itself does not affect life expectancy
7. Diagnosis & Testing
Diagnostic Procedures
Diagnosis of Ménière’s disease is primarily clinical, based on history and symptoms. The Bárány Society (in collaboration with several international organizations) established the most recent diagnostic criteria in 2015:
Definite Ménière’s Disease:
- Two or more spontaneous episodes of vertigo, each lasting 20 minutes to 12 hours
- Audiometrically documented low- to medium-frequency sensorineural hearing loss in the affected ear on at least one occasion before, during, or after a vertigo episode
- Fluctuating aural symptoms (hearing, tinnitus, or fullness) in the affected ear
- Not better explained by another vestibular diagnosis
Probable Ménière’s Disease:
- Two or more episodes of vertigo or dizziness, each lasting 20 minutes to 24 hours
- Fluctuating aural symptoms (hearing, tinnitus, or fullness) in the affected ear
- Not better explained by another vestibular diagnosis
The diagnostic process typically includes:
- Detailed medical history
- Physical examination
- Audiological evaluation
- Vestibular function testing
- Imaging studies to rule out other conditions
Medical Tests
Several tests are used in the diagnostic process:
Audiological Tests:
- Pure-tone audiometry (shows characteristic low-frequency sensorineural hearing loss)
- Speech discrimination testing
- Electrocochleography (ECoG) – measures electrical potentials of the inner ear
- Otoacoustic emissions (OAEs)
- Auditory brainstem response (ABR)
Vestibular Tests:
- Videonystagmography (VNG) or electronystagmography (ENG)
- Caloric testing
- Rotary chair testing
- Video head impulse test (vHIT)
- Vestibular evoked myogenic potentials (VEMP)
Imaging Studies:
- MRI with gadolinium to rule out other pathologies (e.g., acoustic neuroma)
- MRI techniques for visualizing endolymphatic hydrops (specialized protocols)
- CT scan of temporal bones (in some cases)
Other Tests:
- Blood tests to rule out other disorders (autoimmune markers, thyroid function, syphilis)
- Glycerol test (historical test, less commonly used today)
Early Detection Methods and Effectiveness
Early detection of Ménière’s disease can be challenging due to:
- Symptom overlap with other vestibular disorders
- Intermittent nature of symptoms
- Initial presentation that may include only some of the cardinal symptoms
Early Detection Approaches:
- Serial audiometry (tracking hearing fluctuations over time)
- Electrocochleography (ECoG) – may show increased summating potential/action potential ratio
- Specialized MRI techniques to visualize endolymphatic hydrops
- Careful monitoring of patients with isolated low-frequency hearing loss or episodic vertigo
Effectiveness of Early Detection:
- Early detection allows for earlier intervention that may slow disease progression
- Serial audiometry is effective for documenting fluctuating hearing loss
- MRI visualization of endolymphatic hydrops has improved diagnostic accuracy
- No current screening method has high sensitivity and specificity for presymptomatic detection
- The fluctuating nature of symptoms can make confirmation challenging even with testing
8. Treatment Options
Standard Treatment Protocols
Treatment for Ménière’s disease is typically staged, beginning with the least invasive approaches:
First-Line Treatments:
- Lifestyle modifications (low-salt diet, avoiding caffeine and alcohol)
- Stress management techniques
- Vestibular rehabilitation therapy
- Medications for symptom control during acute attacks
Second-Line Treatments:
- Diuretic therapy (e.g., hydrochlorothiazide/triamterene)
- Betahistine (commonly used in Europe, not FDA-approved in the US)
- Intratympanic steroid injections
- Use of the Meniett device (applies low-pressure pulses to the ear)
Third-Line Treatments:
- Intratympanic gentamicin injections (chemical labyrinthectomy)
- Surgical procedures (for refractory cases)
Medications, Surgeries, and Therapies
Medications:
- For Acute Attacks:
- Antivertigo medications (meclizine, diazepam)
- Antiemetics (promethazine, ondansetron)
- Motion sickness medications
- Preventive Medications:
- Diuretics (hydrochlorothiazide, acetazolamide)
- Betahistine (Serc) – used widely outside the US
- Steroids (oral or intratympanic)
Surgical Procedures:
- Conservative Surgeries:
- Endolymphatic sac decompression/shunt
- Vestibular neurectomy (selectively cutting the vestibular portion of the vestibulocochlear nerve)
- Ablative Procedures:
- Labyrinthectomy (destruction of the labyrinth)
- Intratympanic gentamicin injections (chemical labyrinthectomy)
- Triple semicircular canal occlusion (newer technique)
Other Therapies:
- Vestibular rehabilitation therapy
- Tinnitus retraining therapy
- Cognitive behavioral therapy (for anxiety/depression)
- Sound therapy for tinnitus
- Hearing aids for hearing loss
- Pressure pulse treatment (Meniett device)
Emerging Treatments and Clinical Trials
Several promising treatments are under investigation:
Pharmaceutical Approaches:
- SPI-1005 (an oral drug that promotes production of glutathione peroxidase)
- OTO-104 (sustained-release dexamethasone for intratympanic delivery)
- Intratympanic methylprednisolone (PREDMEN trial)
- Venlafaxine (being studied for vertigo control)
- Antisecretory factor (dietary supplements containing specially processed cereals)
Surgical Innovations:
- Transcanal endoscopic infracochlear vestibular neurectomy
- New marsupiliazation techniques in endolymphatic sac surgery
- Tenotomy of the stapedius and tensor tympani muscles
- Less invasive variants of established surgical techniques
Other Approaches:
- Wearable vestibular stimulators
- Virtual reality-based vestibular rehabilitation
- Novel drug delivery systems for inner ear medications
- Gene therapy approaches (preclinical phase)
9. Prevention & Precautionary Measures
Prevention Strategies
While Ménière’s disease cannot be completely prevented since its exact cause remains unknown, several strategies may help prevent attacks or slow disease progression:
Dietary Modifications:
- Low-sodium diet (typically restricting intake to 1,500-2,000 mg per day)
- Avoiding caffeine, which can worsen tinnitus and may trigger attacks
- Limiting or avoiding alcohol consumption
- Regular meals and hydration to maintain stable metabolism
- Identifying and avoiding any personal food triggers
Lifestyle Adjustments:
- Stress management techniques (meditation, yoga, biofeedback)
- Regular sleep schedule to avoid fatigue
- Moderate, regular exercise (avoiding activities with rapid head movements if sensitive)
- Avoiding smoking (may affect inner ear blood supply)
- Managing allergies effectively
Medical Management:
- Regular check-ups with specialists to monitor hearing and balance
- Prompt treatment of ear infections or other ear conditions
- Management of associated conditions (migraines, allergies, autoimmune disorders)
- Preventive medications as prescribed (diuretics, betahistine)
Environmental Precautions
Several environmental factors may trigger Ménière’s attacks and should be managed:
Barometric Pressure:
- Being aware of weather changes that may trigger symptoms
- Some patients find barometric pressure apps helpful for prediction
- Using decongestants before air travel if pressure changes cause problems
Sound Exposure:
- Protecting ears from loud noise exposure
- Using hearing protection in noisy environments
- Avoiding sudden loud sounds
Other Environmental Factors:
- Avoiding strong smells or chemical exposures if they trigger symptoms
- Managing workplace environments to reduce potential triggers
- Creating a safe home environment to minimize fall risks during vertigo episodes
Preventive Screenings
No specific preventive screening exists for Ménière’s disease, but certain approaches may help with early detection:
For High-Risk Individuals:
- Regular hearing evaluations for those with family history
- Monitoring for early symptoms in patients with related conditions
- Follow-up of patients with isolated low-frequency hearing loss or unexplained vertigo
General Recommendations:
- Baseline hearing tests for middle-aged adults
- Prompt evaluation of new ear symptoms (tinnitus, hearing changes, dizziness)
- Education about early warning signs for those at higher risk
10. Global & Regional Statistics
Incidence and Prevalence Rates
Ménière’s disease shows significant variation in reported prevalence across different countries and regions:
Global Overview:
- Worldwide, prevalence estimates range from 17 to 513 per 100,000 population
- The large variation reflects differences in diagnostic criteria and reporting methods
Regional Breakdown:
- United States: Approximately 200 per 100,000 (0.2% of population)
- United Kingdom: 157 per 100,000 population
- Japan: 17-34.5 per 100,000 population
- Finland: 43 per 100,000 population
- Italy: Estimated at 8 new cases per 100,000 population annually
- Sweden: 46 per 100,000 population
- South Korea: Recent studies suggest rates similar to European countries
Incidence Rates:
- Annual incidence in the United States: 15 per 100,000
- New cases per year in the U.S.: Approximately 45,500
- Finland: Annual incidence of 4.3 per 100,000
Mortality and Survival Rates
Ménière’s disease is not directly life-threatening, and therefore has:
- No direct mortality associated with the condition itself
- Normal life expectancy for affected individuals
- Potential for injuries from falls during vertigo attacks or drop attacks
- Possible increased risk of accidents due to balance impairment
- No significant impact on survival compared to the general population
Country-wise Comparison and Trends
Several notable trends appear in the epidemiological data:
Demographic Patterns:
- Higher reported prevalence in Western countries compared to Asian countries
- Age of onset is similar across countries (typically 40-60 years)
- Female predominance in most studies, though the gender ratio varies
Diagnostic Differences:
- Variation in diagnostic criteria used across countries
- Differences in healthcare access and specialty referral patterns
- Cultural factors influencing symptom reporting and healthcare seeking
Temporal Trends:
- Increasing recognition and diagnosis in many regions
- In Japan, reported cases increased significantly after World War II
- Improved imaging and diagnostic techniques have led to more accurate identification
Bilateral Disease:
- Rates of bilateral involvement range from 9% to 50%
- Typically develops within 5-15 years of initial presentation
- Higher rates reported in studies with longer follow-up periods
11. Recent Research & Future Prospects
Latest Advancements
Recent years have seen significant advances in understanding and treating Ménière’s disease:
Diagnostic Advancements:
- Development of specialized MRI techniques for visualizing endolymphatic hydrops in living patients
- Refinement of diagnostic criteria by international consensus groups
- Advanced vestibular testing techniques for more precise evaluation
- Better understanding of the overlap with vestibular migraine and other disorders
Pathophysiological Insights:
- Identification of proteins within the otolithic and tectorial membranes potentially involved in disease mechanisms
- Recognition of the role of aquaporins (water channels) in inner ear fluid regulation
- Better understanding of the inflammatory and immune components
- Advances in genetics identifying several genes associated with the condition
Treatment Innovations:
- Improved techniques for intratympanic drug delivery
- Development of less invasive surgical approaches
- Exploration of novel therapeutic targets based on molecular pathways
- Better outcomes with vestibular rehabilitation approaches
Ongoing Studies
Multiple research efforts are currently underway:
Clinical Trials:
- SPI-1005 for treatment of Ménière’s disease (STOPMD-3 trial)
- Intratympanic methylprednisolone for vertigo control (PREDMEN trial)
- Venlafaxine for Ménière’s disease symptoms
- Various surgical technique modifications and their outcomes
Basic Science Research:
- Investigation of genetic factors in familial and sporadic cases
- Animal models of endolymphatic hydrops
- Role of autoimmunity and inflammation in disease development
- Inner ear fluid homeostasis mechanisms
Epidemiological Studies:
- Population-based studies of comorbidities
- Long-term natural history studies
- Factors affecting progression to bilateral disease
- Environmental and dietary influences
Future Medical Possibilities
Several promising directions may shape the future of Ménière’s disease management:
Potential Future Treatments:
- Gene therapy targeting specific genetic variants
- Drug delivery systems designed specifically for inner ear treatment
- Regenerative approaches for inner ear hair cells to address hearing loss
- Targeted immunomodulatory therapies for autoimmune variants
Diagnostic Improvements:
- Biomarkers for earlier and more accurate diagnosis
- Personalized predictive models for disease progression
- Advanced imaging techniques with higher resolution and sensitivity
- Genetic screening for high-risk individuals
Management Approaches:
- Telemedicine applications for remote monitoring and management
- Wearable devices to predict and potentially abort attacks
- Virtual reality applications for vestibular rehabilitation
- Improved hearing aid and implant technologies for hearing loss
12. Interesting Facts & Lesser-Known Insights
Uncommon Knowledge
Several interesting aspects of Ménière’s disease are not widely recognized:
- The disease was first described as an inner ear disorder at a time when vertigo was thought to originate from the brain, representing a major paradigm shift
- Ménière’s disease can present differently in men and women, with some studies suggesting that women may experience more frequent but less severe vertigo episodes
- Some patients report being able to predict attacks based on specific prodromal symptoms
- There is emerging evidence of seasonal patterns in symptom frequency for some patients
- About 10% of patients with Ménière’s disease have another family member with the condition
- The disease can occasionally go into spontaneous remission after several years
Myths vs. Medical Facts
Several misconceptions exist about Ménière’s disease:
Myth: Ménière’s disease always causes severe, disabling vertigo in all patients. Fact: The severity varies significantly between individuals, and some experience primarily hearing symptoms with minimal vertigo.
Myth: Ménière’s disease always leads to complete deafness. Fact: While progressive hearing loss is common, many patients retain functional hearing, especially with proper management.
Myth: Ménière’s disease is a psychological or stress-induced condition. Fact: It is a physical disorder of the inner ear, though stress can trigger or worsen attacks.
Myth: Salt restriction is only beneficial for people with hypertension. Fact: Salt restriction helps reduce endolymphatic hydrops independent of blood pressure effects.
Myth: All cases of Ménière’s disease will eventually affect both ears. Fact: While bilateral involvement develops in some cases (10-50%), many patients have only unilateral disease throughout their lifetime.
Impact on Specific Populations
Ménière’s disease affects various groups differently:
Professional Impact:
- Pilots, air traffic controllers, and other transportation professionals may face career limitations due to safety concerns
- Musicians and audio professionals face particular challenges due to hearing fluctuations and sensitivity
- Healthcare workers, teachers, and others who cannot suddenly leave their duties may experience significant workplace challenges
Age-Related Differences:
- Pediatric Ménière’s disease is rare but can affect educational development and social adjustment
- Elderly patients may face greater fall risks and safety concerns
- Diagnostic challenges exist in older adults due to overlap with other age-related balance and hearing disorders
Special Considerations:
- Pregnant women with Ménière’s disease may experience symptom changes due to hormonal fluctuations
- Athletes may need specific accommodations for training and competition
- Military personnel may face fitness-for-duty concerns
- People living in rural or remote areas may have limited access to specialists experienced in managing the condition
References
- Lopez-Escamez JA, et al. Diagnostic criteria for Menière’s disease. Journal of Vestibular Research. 2015;25(1):1-7.
- Nakashima T, et al. Visualization of endolymphatic hydrops in patients with Meniere’s disease. Laryngoscope. 2007;117:415-20.
- Gürkov R, et al. What is Menière’s disease? A contemporary re-evaluation of endolymphatic hydrops. Journal of Neurology. 2016;263:S71-S81.
- Alexander TH, Harris JP. Current epidemiology of Meniere’s syndrome. Otolaryngologic Clinics of North America. 2010;43(5):965-70.
- Nevoux J, et al. International consensus (ICON) on treatment of Ménière’s disease. European Annals of Otorhinolaryngology, Head and Neck Diseases. 2018;135:S29-S32.
- Basura GJ, et al. Clinical practice guideline: Ménière’s disease executive summary. Otolaryngology-Head and Neck Surgery. 2020;162:415-434.
- Foster CA, Breeze RE. Endolymphatic hydrops in Ménière’s disease: cause, consequence, or epiphenomenon? Otology & Neurotology. 2013;34(7):1210-4.
- Lopez-Escamez JA, et al. Recent advances in understanding molecular bases of Ménière’s disease. F1000Research. 2023;12:495.
- Shojaku H, et al. Changes in the characteristics of definite Meniere’s disease over time in Japan. Acta Otolaryngologica. 2009;129(2):155-60.
- Scarpa A, et al. Pharmacological, surgical and diagnostic innovations in Meniere’s disease: a review. Journal of Clinical Medicine. 2021;10(3):453.