
⚠️ Disclaimer: The information provided in this article is for educational purposes only and does not constitute medical advice. RevisionTown does not provide diagnosis, treatment, or medical recommendations. Always consult a qualified healthcare professional regarding any medical condition, symptoms, or concerns.
Read More – 🏥 Medical Disclaimer
Comprehensive Report on Crohn’s Disease
1. Overview
What is Crohn’s Disease?
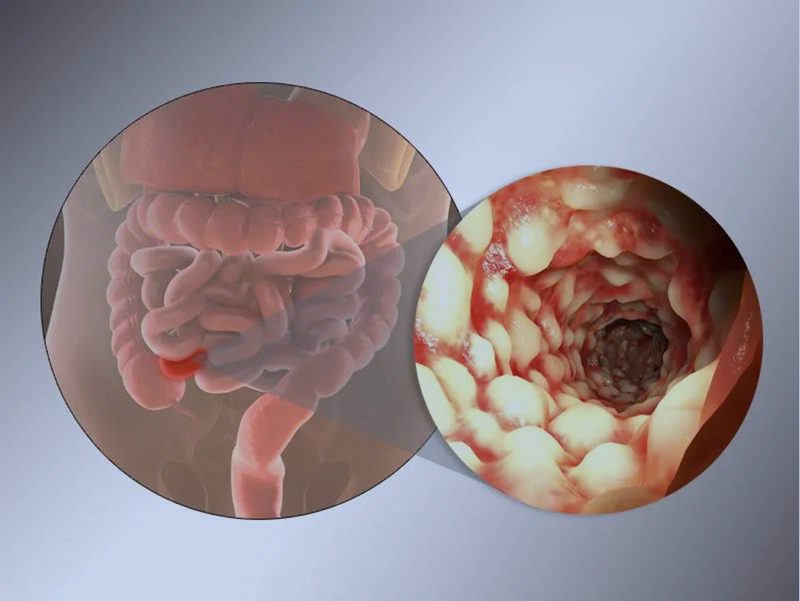
Crohn’s disease is a chronic inflammatory bowel disease (IBD) characterized by inflammation of the digestive tract lining. Unlike ulcerative colitis (another common IBD), Crohn’s disease can affect any part of the digestive tract from the mouth to the anus, often involving deeper tissue layers. The inflammation typically occurs in patches with healthy sections in between, rather than as a continuous area of inflammation.
Affected Body Parts/Organs
While Crohn’s disease can affect any part of the digestive tract, it most commonly involves:
- The terminal ileum (the end of the small intestine)
- The colon (large intestine)
- The ileocecal area (where the small and large intestines meet)
Less commonly, it may affect:
- The esophagus
- The stomach
- The duodenum (first part of the small intestine)
- The mouth
- The anus and perianal area
The inflammation can extend through all layers of the bowel wall (transmural inflammation), distinguishing it from ulcerative colitis, which typically affects only the innermost lining of the colon.
Prevalence and Significance
Crohn’s disease affects approximately 3-7 per 100,000 people in Western countries, with an estimated 780,000 Americans living with the condition. The prevalence has been increasing globally, particularly in industrialized regions and newly industrialized countries.
The disease typically manifests between ages 15-35, though it can occur at any age. There is a slight predominance in females, and a higher prevalence in Caucasians, particularly those of Ashkenazi Jewish descent.
Crohn’s disease represents a significant healthcare burden due to its chronic, relapsing nature, frequent hospitalizations, need for surgery, and impact on quality of life. The economic burden includes direct medical costs, lost productivity, and disability.
2. History & Discoveries
First Identification
Crohn’s disease was first officially described in 1932 by Dr. Burrill B. Crohn and his colleagues, Dr. Leon Ginzburg and Dr. Gordon D. Oppenheimer, in their landmark paper “Regional Ileitis: A Pathologic and Clinical Entity.” Their description focused on inflammation of the terminal ileum, which they called “terminal ileitis” or “regional ileitis.”
Key Discoverers
Although the disease bears Burrill Crohn’s name, several physicians had previously documented similar conditions:
- Giovanni Battista Morgagni described intestinal inflammation resembling Crohn’s in 1761
- Antoni Leśniowski, a Polish surgeon, described the condition in 1904
- In some European countries, particularly Poland, the disease is known as Leśniowski-Crohn’s disease
The alphabetical listing of authors placed Crohn’s name first on the 1932 publication, leading to the eventual naming of the condition.
Major Breakthroughs
- 1950s: Development of corticosteroids for treatment
- 1960s: Recognition that Crohn’s disease can affect the entire GI tract
- 1970s: Discovery of genetic predisposition factors
- 1980s: Development of immunomodulators like azathioprine and 6-mercaptopurine
- 1990s: Identification of the NOD2/CARD15 gene as the first gene linked to Crohn’s disease
- 1998: FDA approval of infliximab (Remicade), the first biologic therapy for Crohn’s
- 2000s: Genome-wide association studies identifying over 200 genetic loci associated with IBD
- 2010s: Development of new biologic therapies targeting different inflammatory pathways
- 2016: FDA approval of ustekinumab (Stelara), targeting IL-12/IL-23
- 2020-2023: Advances in JAK inhibitors and S1P receptor modulators
Evolution of Understanding
Medical understanding has evolved from viewing Crohn’s as a primarily infectious disease to recognizing it as a complex immune-mediated condition with genetic, environmental, and microbiome components. The concept of treating “beyond symptoms” to achieve mucosal healing and prevent long-term complications has transformed management approaches.
3. Symptoms
Early Symptoms
Early manifestations of Crohn’s disease often include:
- Persistent diarrhea
- Abdominal pain and cramping, typically in the lower right area
- Fatigue and general malaise
- Unintended weight loss
- Low-grade fever
- Blood in stool (less common than in ulcerative colitis)
- Reduced appetite
- Perianal discomfort or drainage
These symptoms may develop gradually and can be intermittent, making early diagnosis challenging.
Advanced-Stage Symptoms
As the disease progresses, symptoms may become more severe:
- Severe abdominal pain
- Profound weight loss and malnutrition
- Severe, chronic diarrhea
- Rectal bleeding
- Joint pain and swelling (arthritis)
- Skin manifestations such as erythema nodosum
- Eye inflammation (uveitis or episcleritis)
- Delayed growth and sexual development in children
- Fistula formation (abnormal connections between intestines and other organs)
- Intestinal strictures and obstruction
Progression Over Time
Crohn’s disease typically follows a relapsing-remitting course with periods of active disease (flares) alternating with periods of remission. Over time, untreated or poorly controlled disease can lead to:
- Increasing frequency and severity of flares
- Shorter periods of remission
- Development of complications such as strictures, fistulas, and abscesses
- Extraintestinal manifestations affecting the joints, skin, eyes, liver, and bile ducts
- Increased risk of colorectal cancer in patients with long-standing colonic disease
The disease course varies significantly between individuals, with approximately:
- 20% of patients experiencing a relatively mild course
- 50% having moderate disease with occasional flares
- 30% suffering from severe, frequently relapsing disease requiring intensive therapy
4. Causes
Biological Causes
The exact etiology of Crohn’s disease remains incompletely understood, but current evidence points to a complex interplay of factors:
Immune System Dysfunction:
- Abnormal immune response against harmless bacteria, food, and other substances in the intestine
- Dysregulated T-cell responses, particularly involving Th1 and Th17 cells
- Impaired intestinal barrier function allowing bacterial translocation
- Defective bacterial clearance by macrophages
Microbiome Alterations:
- Reduced microbial diversity in the gut
- Increased abundance of adherent-invasive Escherichia coli (AIEC)
- Decreased beneficial Firmicutes bacteria
- Disruption of the balance between commensal and pathogenic bacteria
Genetic Factors
Crohn’s disease has a strong genetic component:
- First-degree relatives have a 10-15 times higher risk
- 15% of patients have an affected family member
- Twin studies show 50-60% concordance in monozygotic twins
- Over 200 genetic loci have been associated with IBD
Key genetic associations include:
- NOD2/CARD15 gene mutations affecting bacterial recognition
- ATG16L1 and IRGM mutations impairing autophagy
- IL23R variants affecting inflammatory responses
- LRRK2 mutations linked to both Crohn’s and Parkinson’s disease
- Variants in XBP1 affecting endoplasmic reticulum stress responses
Environmental Triggers
Several environmental factors appear to trigger or exacerbate Crohn’s disease:
Dietary Factors:
- High consumption of processed foods, refined sugars, and animal proteins
- Low intake of fruits, vegetables, and fiber
- Food additives such as emulsifiers and artificial sweeteners
- Western diet high in saturated fats
Other Environmental Factors:
- Cigarette smoking (notably increases risk for Crohn’s, unlike ulcerative colitis)
- Nonsteroidal anti-inflammatory drug (NSAID) use
- Antibiotics altering gut microbiota, especially in early life
- Vitamin D deficiency
- Urban living environments
- Stress and psychological factors
- Air pollution and industrial chemicals
5. Risk Factors
Demographic Risk Factors
Age:
- Most commonly diagnosed between ages 15-35
- A second peak occurs between ages 60-80
- Pediatric onset occurs in approximately 25% of cases
Gender:
- Slight female predominance (1.1-1.3:1 ratio)
- The gender gap appears to be narrowing in recently industrialized countries
Ethnicity:
- Highest prevalence in Caucasians
- 3-5 times more common in Ashkenazi Jewish populations
- Increasing incidence in Asian, Hispanic, and African American populations
Geographic Distribution:
- Highest prevalence in North America and Northern Europe
- Rapidly increasing in Asia, South America, and the Middle East
- Urban areas have higher rates than rural areas
- North-south gradient with higher rates in northern latitudes
Lifestyle Factors
Smoking:
- Active smoking approximately doubles the risk
- Worsens disease course and increases need for surgery
- Associated with higher rates of disease recurrence after surgery
Diet:
- High intake of saturated fats and refined carbohydrates increases risk
- Low fiber intake associated with higher risk
- Mediterranean diet may be protective
Physical Activity:
- Sedentary lifestyle correlates with increased risk
- Regular physical activity may have protective effects
Stress and Sleep:
- Psychological stress may trigger flares in established disease
- Sleep disturbances associated with increased inflammation
Pre-existing Conditions
- Prior appendectomy (unlike its protective effect in ulcerative colitis)
- History of recurrent enteric infections
- Vitamin D deficiency
- Obesity (associated with more aggressive disease course)
- Prior antibiotic exposure, especially in childhood
- Oral contraceptive use (modest increase in risk)
- Nonsteroidal anti-inflammatory drug use
6. Complications
Intestinal Complications
Strictures:
- Narrowing of the intestinal lumen due to inflammation and fibrosis
- Affects 30-50% of patients over time
- May cause intestinal obstruction requiring endoscopic dilation or surgery
Fistulas:
- Abnormal connections between the intestine and other structures
- Occur in 20-40% of patients
- Types include enterocutaneous, enterovesical, enterovaginal, and perianal
Abscesses:
- Collections of pus due to infection
- Commonly associated with fistulas
- Require drainage and antibiotic therapy
Perforation:
- Complete penetration of the intestinal wall
- Medical emergency requiring urgent surgical intervention
- Carries significant morbidity and mortality
Malnutrition:
- Due to reduced nutrient absorption, increased losses, and decreased intake
- Specific deficiencies include iron, vitamin B12, folate, vitamin D, zinc
Small Bowel Bacterial Overgrowth:
- Excessive bacterial colonization of the small intestine
- Results from altered motility, structural changes, or fistulas
- Causes malabsorption and worsening symptoms
Extraintestinal Complications
Musculoskeletal:
- Peripheral arthritis (5-20% of patients)
- Ankylosing spondylitis and sacroiliitis (3-10%)
- Osteoporosis and osteopenia (30-60%)
Dermatological:
- Erythema nodosum (2-6%)
- Pyoderma gangrenosum (0.5-2%)
- Sweet’s syndrome
- Oral aphthous ulcers (10-20%)
Ocular:
- Episcleritis and scleritis (3-5%)
- Uveitis (0.5-3%)
- Keratopathy
Hepatobiliary:
- Primary sclerosing cholangitis (1-3%)
- Gallstones (increased risk by 2-3 fold)
- Fatty liver disease
- Autoimmune hepatitis
Hematologic:
- Anemia (iron deficiency, chronic disease, or vitamin deficiency)
- Thrombocytosis
- Hypercoagulable state with increased venous thromboembolism risk
Cardiovascular:
- Increased risk of coronary artery disease
- Vasculitis
- Pericarditis (rare)
Neurological:
- Peripheral neuropathy
- Central demyelination (rare)
- Cerebrovascular events
Long-term Impact and Mortality
- Increased lifetime risk of colorectal cancer (particularly with colonic disease)
- Small bowel adenocarcinoma risk (30-50 times higher than general population)
- Psychosocial complications including depression, anxiety, and reduced quality of life
- Work disability affecting 35-40% of patients within 10 years of diagnosis
- Standardized mortality ratio of 1.3-1.5 compared to the general population
- Leading causes of death: complications of disease, surgical complications, malignancy, and infections
7. Diagnosis & Testing
Clinical Evaluation
- Comprehensive medical history
- Family history of IBD or other autoimmune conditions
- Physical examination including abdominal and perianal examination
- Growth and development assessment in pediatric patients
- Evaluation of extraintestinal manifestations
Laboratory Tests
Blood Tests:
- Complete blood count (anemia, thrombocytosis, leukocytosis)
- Inflammatory markers (ESR, CRP)
- Albumin (decreased in active disease/malnutrition)
- Liver function tests
- Vitamin and mineral levels (B12, folate, iron, zinc)
- Fecal calprotectin (sensitive marker of intestinal inflammation)
- Fecal lactoferrin (alternative marker of inflammation)
- Serological markers (ASCA, p-ANCA) – limited diagnostic value but may help differentiate from ulcerative colitis
Imaging Studies
Cross-sectional Imaging:
- CT enterography: Highly sensitive for wall thickening, strictures, fistulas
- MR enterography: Similar sensitivity to CT but without radiation exposure
- Ultrasound: Useful for assessing bowel wall thickness and complications, particularly in pediatric patients
- Small bowel follow-through: Traditional but less sensitive than cross-sectional imaging
Endoscopic Procedures:
- Ileocolonoscopy with biopsies: Gold standard for diagnosis
- Upper endoscopy: When upper GI symptoms are present
- Capsule endoscopy: Useful for small bowel disease when strictures are absent
- Balloon-assisted enteroscopy: Allows visualization and biopsy of the small intestine
- Endoscopic ultrasound: Helpful for perianal disease assessment
Histopathology
Characteristic findings include:
- Focal (discontinuous) chronic inflammation
- Transmural inflammation (affecting all layers of the bowel wall)
- Granulomas (in 15-70% of patients)
- Lymphoid aggregates
- Fissuring ulceration
- Crypt architectural distortion
- Neuronal hyperplasia
Diagnostic Criteria
Diagnosis typically requires:
- Compatible clinical presentation
- Endoscopic or radiologic evidence of disease
- Histological confirmation
- Exclusion of infectious causes
The International Organization for the Study of Inflammatory Bowel Diseases (IOIBD) uses a combination of clinical, endoscopic, histologic, and radiographic findings to establish the diagnosis.
Early Detection and Screening
- No population-wide screening programs exist
- Biomarkers like fecal calprotectin can help identify patients needing further investigation
- Genetic testing not recommended for screening but may guide therapy in the future
- Family members of affected individuals have higher pre-test probability warranting lower threshold for investigation
8. Treatment Options
Treatment Goals
Modern treatment aims to:
- Induce and maintain clinical remission
- Achieve mucosal healing (endoscopic remission)
- Prevent complications and disease progression
- Improve quality of life
- Minimize treatment-related side effects
- Reduce hospitalizations and surgeries
- Enable normal growth and development in pediatric patients
Conventional Medications
5-Aminosalicylates (5-ASAs):
- Examples: mesalamine, sulfasalazine, balsalazide
- Limited efficacy in Crohn’s, primarily useful for mild colonic disease
- Generally well-tolerated with minimal side effects
Corticosteroids:
- Examples: prednisone, budesonide, methylprednisolone
- Effective for inducing remission in moderate-to-severe flares
- Not suitable for maintenance due to side effects
- Budesonide offers more targeted delivery with fewer systemic effects
Immunomodulators:
- Thiopurines (azathioprine, 6-mercaptopurine)
- Effective for maintaining remission
- Require monitoring for myelosuppression, hepatotoxicity, and increased infection risk
- Methotrexate
- Weekly administration (oral or subcutaneous)
- Effective for maintenance, particularly in those with articular manifestations
- Requires folate supplementation and monitoring for hepatotoxicity
Antibiotics:
- Metronidazole and ciprofloxacin
- Useful for perianal disease, bacterial overgrowth, and certain complications
- Not recommended for primary treatment of luminal disease
Biologic Therapies
Anti-TNF Agents:
- Infliximab, adalimumab, certolizumab pegol, golimumab
- Highly effective for induction and maintenance
- Used for moderate-to-severe disease and fistulizing disease
- Require screening for tuberculosis and monitoring for infections, demyelinating disease, and psoriasis
Anti-Integrin Therapy:
- Vedolizumab
- Gut-selective anti-α4β7 integrin antibody
- Lower systemic immunosuppression risk
- Particularly effective for colonic disease
Anti-IL-12/23 Therapy:
- Ustekinumab
- Blocks the p40 subunit shared by IL-12 and IL-23
- Effective for both induction and maintenance
- Favorable safety profile
Anti-IL-23 Specific Therapy:
- Risankizumab, guselkumab, mirikizumab
- Target the p19 subunit of IL-23 specifically
- Promising results in clinical trials
- Approved or in late-stage development
JAK Inhibitors:
- Tofacitinib, upadacitinib, filgotinib
- Small molecules inhibiting Janus kinase signaling
- Oral administration
- Effective for moderate-to-severe disease
- Require monitoring for infections, lipid elevation, and thrombosis risk
S1P Receptor Modulators:
- Ozanimod, etrasimod
- Reduce lymphocyte trafficking to inflamed tissue
- Oral administration
- Promising results in clinical trials
- Require cardiac monitoring before initiation
Surgical Interventions
Approximately 70-80% of Crohn’s patients will require surgery within their lifetime:
Resection:
- Removal of severely diseased segments
- Minimally invasive approaches preferred when possible
- Conservative resection to preserve bowel length
Strictureplasty:
- Widens narrowed segments without removing tissue
- Preserves bowel length
- Particularly important in patients with extensive small bowel involvement
Diverting Ostomy:
- Temporary diversion of fecal stream
- May allow healing of severe disease or complex perianal fistulas
- Often later reversed if sufficient healing occurs
Abscess Drainage:
- Percutaneous or surgical drainage of intra-abdominal abscesses
- Often combined with antibiotic therapy
Surgery for Fistulas:
- Seton placement for perianal fistulas
- Fistulotomy or advancement flaps for selected cases
- Combined with medical therapy for optimal outcomes
Nutritional Therapies
Exclusive Enteral Nutrition (EEN):
- First-line therapy for pediatric Crohn’s disease in many centers
- Comparable to corticosteroids for inducing remission
- Improves nutritional status and growth
- Limited acceptance in adults due to adherence challenges
Specific Carbohydrate Diet:
- Eliminates most complex carbohydrates and processed foods
- Some evidence of benefit, primarily in pediatric populations
- Research ongoing
Partial Enteral Nutrition:
- Combines formula with allowed whole foods
- Better acceptance than EEN
- Emerging evidence of effectiveness
Parenteral Nutrition:
- Reserved for severe malnutrition or complications
- Short bowel syndrome
- Intractable symptoms with significant weight loss
Emerging Treatments
Stem Cell Therapy:
- Hematopoietic stem cell transplantation for refractory cases
- Mesenchymal stem cell therapy for fistulizing disease
Fecal Microbiota Transplantation:
- Mixed results in clinical trials
- Research focusing on optimal donor selection and delivery methods
Novel Small Molecules:
- TYK2 inhibitors (deucravacitinib)
- RORγt inhibitors
- SMAD7 antisense oligonucleotides (mongersen)
Anti-fibrotic Therapies:
- Targeting intestinal stricture formation
- Anti-TGF-β agents and matrix metalloproteinase modulators
Combination Therapies:
- Strategic combination of biologics targeting different pathways
- Precision medicine approaches based on individual disease characteristics
9. Prevention & Precautionary Measures
Primary Prevention
As Crohn’s disease has no definitively established preventable cause, true primary prevention is challenging. However, several measures may reduce risk:
Lifestyle Measures:
- Smoking cessation or avoidance
- Regular physical activity
- Maintaining healthy body weight
- Stress management techniques
Dietary Considerations:
- Mediterranean diet rich in fruits, vegetables, olive oil, and fish
- Adequate fiber intake
- Limiting processed foods, refined sugars, and saturated fats
- Adequate vitamin D intake/exposure
Early Life Factors:
- Breastfeeding when possible (may offer protective effects)
- Judicious use of antibiotics in childhood
- Avoiding unnecessary cesarean sections
- Natural childbirth exposure to maternal microbiota
Secondary Prevention
For those with established disease, preventing flares and complications:
Medication Adherence:
- Consistent use of maintenance therapies
- Regular monitoring of drug levels when applicable
- Vaccination against preventable infections before immunosuppression
Lifestyle Management:
- Smoking cessation (of particular importance in Crohn’s)
- Regular exercise appropriate to energy levels
- Stress reduction techniques
- Adequate sleep hygiene
Dietary Management:
- Identifying and avoiding personal trigger foods
- Maintaining good nutritional status
- Adequate hydration
- Potential benefit from specific dietary approaches (Mediterranean, SCD)
Regular Monitoring:
- Scheduled follow-up with healthcare providers
- Periodic laboratory assessment
- Disease activity monitoring (symptoms, biomarkers)
- Age-appropriate cancer screening
Tertiary Prevention
For those with advanced disease, preventing further deterioration:
Complication Surveillance:
- Regular imaging in patients at risk for strictures
- Monitoring for nutritional deficiencies
- Bone density assessment for osteoporosis risk
- Appropriate cancer surveillance
Optimized Treatment:
- Therapeutic drug monitoring to ensure adequate drug levels
- Timely adjustment of therapy based on disease activity
- Multidisciplinary approach to complex disease
Psychosocial Support:
- Mental health services
- Support groups
- Disease education
- Occupational rehabilitation when needed
Vaccination Recommendations
Patients on immunosuppressive therapy have specific vaccination needs:
Live Vaccines (contraindicated on immunosuppression):
- MMR
- Varicella
- Zoster (live version)
- Yellow fever
- Oral typhoid
Inactivated Vaccines (recommended):
- Annual influenza
- Pneumococcal vaccines (PCV13 and PPSV23)
- Hepatitis B
- Hepatitis A
- Human papillomavirus (HPV)
- Tetanus, diphtheria, pertussis
- COVID-19
- Recombinant zoster vaccine
- Meningococcal vaccines
Ideally, vaccination status should be assessed and updated before initiating immunosuppressive therapy.
10. Global & Regional Statistics
Global Prevalence
- Highest in North America: 319 per 100,000 population
- Western Europe: 322 per 100,000
- Oceania: 155 per 100,000
- Southern Latin America: 74 per 100,000
- Eastern Europe: 67 per 100,000
- Asia: 5-44 per 100,000 (rapidly increasing)
- Africa: 4-20 per 100,000 (limited data available)
Incidence Trends
- North America: 20.2 per 100,000 person-years
- Europe: 12.7 per 100,000 person-years
- Asia and Middle East: 5.0 per 100,000 person-years (with rapid increases)
- Global incidence increasing by approximately 3-5% annually
- Particularly rapid increases in newly industrialized countries
- Pediatric incidence increasing faster than adult incidence in many regions
Demographic Patterns
- Male-to-female ratio: approximately 1:1.1-1.3
- Age distribution:
- Peak onset: 15-35 years
- Second smaller peak: 60-80 years
- Pediatric onset (under 18): 25% of cases
- Very early onset (under 6): approximately 4-5% of pediatric cases
- Ethnic distribution:
- Highest in Caucasians and Ashkenazi Jews
- Increasing in Hispanic, Asian, and African populations
Economic Burden
- United States: $3.5-4 billion in direct healthcare costs annually
- European Union: €4.6-5.6 billion annually
- Average lifetime cost per patient: $622,000 (US estimate)
- Work disability affects 35-40% of patients within 10 years
- Productivity losses account for 28-68% of total disease costs
Mortality Statistics
- Standardized mortality ratio: 1.3-1.5 compared to general population
- Mortality higher in:
- Older-onset disease
- Stricturing or penetrating phenotypes
- Upper gastrointestinal involvement
- Persistent active disease
- 10-year survival: approximately 96%
- 20-year survival: approximately 91%
- Leading causes of death:
- Disease complications
- Surgical complications
- Malignancy
- Infections related to immunosuppression
Country-Specific Data
- United States: 780,000 affected (241 per 100,000)
- Canada: 129,000 affected (319 per 100,000)
- United Kingdom: 115,000 affected (157 per 100,000)
- Germany: 150,000 affected (147 per 100,000)
- France: 100,000 affected (110 per 100,000)
- Japan: 55,000 affected (42 per 100,000)
- China: 166,000 affected (12 per 100,000, but rapidly increasing)
- India: 116,000 affected (9.3 per 100,000, but limited data)
- Brazil: 34,000 affected (22 per 100,000)
Healthcare Utilization
- Hospitalization rates: 20-30% of patients annually
- Surgery rates: 50-70% within 10 years of diagnosis
- Emergency department visits: 2-3 times higher than general population
- Medication adherence: 40-60% (varies by treatment regimen)
- Biologic therapy usage: 20-40% of patients (varies by region and healthcare system)
11. Recent Research & Future Prospects
Recent Advances (2020-2024)
Novel Therapeutic Targets:
- JAK inhibitors: Upadacitinib approved for moderate-to-severe Crohn’s disease
- Anti-IL-23p19 antibodies: Risankizumab approved for Crohn’s disease
- S1P receptor modulators: Ozanimod showing promising results in phase 3 trials
- TYK2 inhibitors: Deucravacitinib in clinical trials with encouraging early results
Precision Medicine Approaches:
- Multi-omics profiling to predict treatment response
- Pharmacogenomic testing to optimize therapy selection
- Transcriptomic signatures to identify disease subtypes
- Machine learning algorithms predicting disease course and complications
Microbiome Interventions:
- Targeted bacteriotherapy with specific bacterial consortia
- Phage therapy against adherent-invasive E. coli
- Engineered bacteria producing anti-inflammatory compounds
- Prebiotic and postbiotic compounds modulating microbiota
Cell-Based Therapies:
- Mesenchymal stem cells for fistulizing disease (Darvadstrocel/Alofisel)
- Regulatory T-cell therapy to restore immune tolerance
- CAR-T cells targeting inflammatory pathways
- Intestinal organoids for personalized drug testing
Advanced Drug Delivery:
- Oral biologic formulations using various technologies
- Janus kinase (JAK) inhibitor microspheres for prolonged release
- Dual-targeted antibodies combining TNF and IL-23 blockade
- Microbiota-activated drug delivery systems
Ongoing Clinical Trials
Phase 3 Trials:
- Multiple anti-IL-23p19 antibodies (mirikizumab, guselkumab)
- Novel JAK inhibitors with improved selectivity
- Combination therapy strategies
- Head-to-head trials of biologics
- Oral formulations of biologics
Phase 2 Trials:
- RIPK2 inhibitors
- Anti-TL1A antibodies
- Microbial consortia therapies
- Anti-fibrotic agents for stricturing disease
- Selective sphingosine-1-phosphate modulators
Phase 1 Trials:
- NLRP3 inflammasome inhibitors
- MicroRNA-based therapies
- Gut-restricted JAK inhibitors
- Gene editing approaches
Future Therapeutic Directions
Pathway-Based Therapies:
- Epithelial barrier enhancement strategies
- Targeting the inflammasome pathway
- Mucosal healing accelerators
- Fibrosis reversal agents
Microbiome-Directed Approaches:
- Personalized dietary interventions based on microbiome analysis
- Microbial metabolite supplementation
- Bacteriophage cocktails targeting pathobionts
- Precision prebiotics modulating specific bacterial taxa
Genetic Therapies:
- Gene therapy for monogenic very-early-onset IBD
- CRISPR-based approaches correcting risk variants
- RNA interference targeting inflammatory mediators
- Antisense oligonucleotides for selected targets
Bioengineering Solutions:
- Bioengineered intestinal tissue for severe disease
- 3D-printed drug delivery devices
- Implantable anti-inflammatory drug reservoirs
- Smart sensors monitoring intestinal inflammation
AI and Digital Health:
- Machine learning algorithms predicting flares
- Digital biomarkers through mobile health technologies
- Virtual reality for pain management and patient education
- Telemedicine platforms optimizing care delivery
Potential for Cure
While a definitive cure remains elusive, several approaches show promise:
Disease Interception:
- Early intervention in high-risk individuals based on genetic, serologic, and microbiome markers
- Pre-emptive therapy before clinical manifestations
- Modulating environmental factors in genetically susceptible individuals
Immune Tolerance Induction:
- Antigen-specific tolerance strategies
- Regulatory T-cell expansion and infusion
- Tolerogenic dendritic cell therapy
- Nanoparticle-based tolerance induction
Comprehensive Microbiome Reprogramming:
- Complete microbiome restoration beyond FMT
- Personalized synthetic microbial communities
- Long-term microbiome modulation strategies
- Combined prebiotic-probiotic-postbiotic approaches
Combined Genetic and Environmental Approach:
- Multi-modal strategies addressing genetic predisposition, microbiome, barrier function, and environmental triggers simultaneously
- Personalized prevention and treatment algorithms
Biomarker-Guided Therapy Withdrawal:
- Identifying deep remission with multiple parameters
- Reliable prediction of sustained remission off therapy
- Sequential therapy de-escalation protocols
12. Interesting Facts & Lesser-Known Insights
Historical Perspectives
- Crohn’s-like conditions were described in medical literature dating back to Hippocrates
- Sir Samuel Wilks described the condition in 1859 as “simple ulcerative colitis”
- The differentiation between ulcerative colitis and Crohn’s disease wasn’t firmly established until the 1960s
- The disease was temporarily thought to be caused by Mycobacterium paratuberculosis, similar to Johne’s disease in cattle
Geographical Phenomena
- “IBD Belt” along northern latitudes correlates with vitamin D exposure
- Lower incidence near the equator with gradient increasing toward poles
- “Westernization” of societies correlates with rising incidence
- Immigration studies show that first-generation immigrants maintain their country-of-origin risk, while second-generation adopt the host country’s risk profile
Unusual Manifestations
- Orofacial granulomatosis can precede intestinal symptoms by years
- Sweet’s syndrome (acute febrile neutrophilic dermatosis) can be the first manifestation
- Pleuropericarditis as an extraintestinal manifestation
- Granulomatous mastitis in females
- Genital lymphedema (rare but distinctive)
Therapeutic Curiosities
- Thalidomide and lenalidomide show efficacy in refractory cases
- Low-dose naltrexone has shown benefit in some patients
- Helminths (intestinal worms) were investigated as potential therapy based on the “hygiene hypothesis”
- Cannabis has demonstrated symptomatic benefit in some studies
- Nicotine patches can paradoxically help some ex-smokers with post-cessation flares
Special Populations
- Pregnancy often induces remission, especially in the third trimester
- Astronauts with Crohn’s face unique challenges in space due to altered microbiome and stress
- High-performance athletes with Crohn’s may experience different flare patterns related to exercise physiology
- Certain occupations show slight variations in prevalence (indoor sedentary jobs higher than outdoor active ones)
Psychological Aspects
- Hypnotherapy has shown efficacy in reducing inflammation markers
- Mindfulness-based stress reduction can extend remission periods
- “Nocebo effect” significant in patients with anxiety about medication side effects
- Cognitive behavioral therapy specifically developed for IBD shows promise
Misconceptions vs. Facts
Myth: Crohn’s is caused by specific foods Fact: While diet can trigger symptoms, no single food causes the disease
Myth: Crohn’s is contagious Fact: There is no evidence of person-to-person transmission
Myth: Stress causes Crohn’s disease Fact: Stress may trigger flares but doesn’t cause the disease itself
Myth: Surgery cures Crohn’s disease Fact: Recurrence after surgery is common (70-90% endoscopic recurrence within 1 year)
Myth: Patients should avoid exercise Fact: Appropriate exercise is beneficial for most patients
Myth: Crohn’s affects only the digestive system Fact: It’s a systemic disease with numerous extraintestinal manifestations
Myth: Biologics are “last resort” therapies Fact: Early biologic therapy can change disease course and prevent complications
Myth: Pregnancy is contraindicated in Crohn’s disease Fact: With proper planning and management, most women with Crohn’s have normal pregnancies
Emerging Research Curiosities
- Circadian rhythm disruption significantly impacts disease activity
- Artificial sweeteners may influence disease through microbiome effects
- Environmental pollutants show correlations with disease flares
- Specific fungi (mycobiome) may play a larger role than previously thought
- Appendix may serve as a reservoir for bacteria that influence disease course
This comprehensive report provides an evidence-based overview of Crohn’s disease based on current medical understanding. As research is ongoing, certain aspects of our understanding may evolve with new discoveries.
