⚠️ Disclaimer: The information provided in this article is for educational purposes only and does not constitute medical advice. RevisionTown does not provide diagnosis, treatment, or medical recommendations. Always consult a qualified healthcare professional regarding any medical condition, symptoms, or concerns.
Read More – 🏥 Medical Disclaimer
Comprehensive Report on Hepatitis
1. Overview
What is Hepatitis?
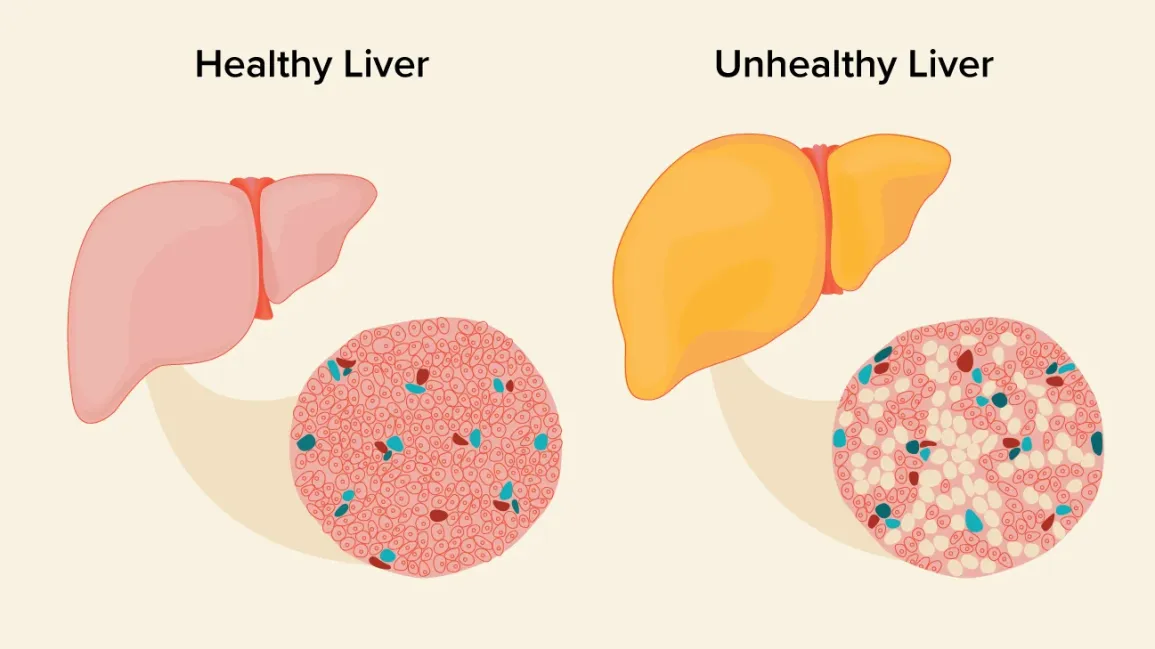
Hepatitis is a medical condition characterized by inflammation of the liver. The term “hepatitis” derives from the Greek words “hepar” (liver) and “itis” (inflammation). This inflammation can be acute (short-term) or chronic (long-term) and can range from mild to severe, potentially leading to liver fibrosis, cirrhosis, cancer, or failure.
Hepatitis encompasses a diverse group of liver diseases with varying etiologies:
Viral Hepatitis:
- Hepatitis A (HAV): Typically transmitted through the fecal-oral route
- Hepatitis B (HBV): Transmitted through blood, semen, and other body fluids
- Hepatitis C (HCV): Primarily transmitted through blood-to-blood contact
- Hepatitis D (HDV): A defective virus requiring HBV for replication
- Hepatitis E (HEV): Primarily transmitted through the fecal-oral route, similar to HAV
Non-Viral Hepatitis:
- Alcoholic Hepatitis: Caused by excessive alcohol consumption
- Autoimmune Hepatitis: Results from the immune system attacking liver cells
- Drug-Induced Hepatitis: Triggered by certain medications or toxins
- Nonalcoholic Steatohepatitis (NASH): Associated with fatty liver disease
- Toxic Hepatitis: Results from exposure to environmental toxins
Affected Body Parts/Organs
Primary Organ Affected:
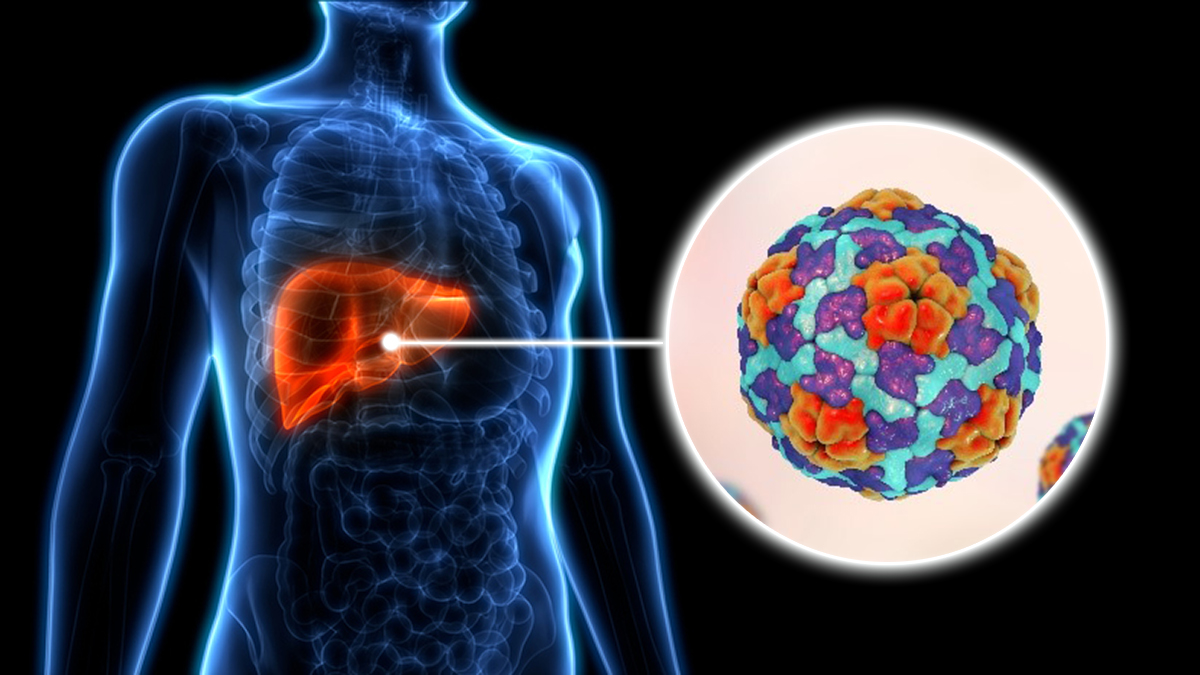
- Liver: A vital organ weighing approximately 1.5 kg in adults, located in the right upper quadrant of the abdomen beneath the diaphragm.
The liver performs over 500 essential functions, including:
- Metabolism of carbohydrates, fats, and proteins
- Detoxification of harmful substances
- Production of bile for fat digestion
- Storage of vitamins and minerals
- Synthesis of blood clotting factors and plasma proteins
- Immune function through specialized Kupffer cells
Secondary Systems Affected:
- Digestive System: Impaired bile production affects digestion and nutrient absorption
- Circulatory System: Portal hypertension, altered production of clotting factors
- Immune System: Altered immune responses and increased susceptibility to infections
- Endocrine System: Disrupted hormone metabolism
- Central Nervous System: Hepatic encephalopathy in severe cases
Prevalence and Significance
Global Burden:
- An estimated 325 million people worldwide live with viral hepatitis (HBV or HCV)
- Viral hepatitis causes approximately 1.4 million deaths annually
- Hepatitis B affects about 296 million people globally
- Hepatitis C affects about 58 million people globally
- Hepatitis A and E cause approximately 114 million infections annually
Economic Impact:
- The global economic burden of viral hepatitis is estimated at $500-600 billion annually
- Productivity losses due to premature mortality and disability
- Direct healthcare costs for treatment and management
- Catastrophic health expenditures for affected individuals in low-resource settings
Public Health Significance:
- Viral hepatitis is a leading cause of liver cancer and transplantation
- Ranked as the 7th leading cause of mortality worldwide
- Identified as a global health priority by the World Health Organization (WHO)
- Target for elimination by 2030 according to WHO’s global health strategy
- Uneven global distribution with disproportionate burden in low- and middle-income countries
Healthcare System Impact:
- Strain on healthcare resources, especially in endemic regions
- High cost of newer antiviral therapies for hepatitis C
- Long-term management costs for chronic hepatitis B
- Liver transplantation costs and organ shortages
- Prevention programs requiring sustained investment
Hepatitis represents a significant global health challenge, with varied presentation, multiple causes, and substantial impact on individual and public health. The diversity of hepatitis types necessitates different approaches to prevention, diagnosis, and treatment, making it a complex medical condition requiring comprehensive understanding and management strategies.
2. History & Discoveries
Early Recognition and Documentation
The history of hepatitis spans thousands of years, with evidence of liver disease documented in ancient texts:
- Babylonian Talmud (5th century BCE): Contains references to jaundice and its contagious nature
- Hippocratic Corpus (400-300 BCE): Describes epidemics of jaundice, likely representing outbreaks of hepatitis A
- Traditional Chinese Medicine texts (3rd century CE): Document “yellow disease” with symptoms consistent with hepatitis
- Middle Ages: Multiple documented outbreaks of jaundice during military campaigns
- 17th-18th centuries: Distinction between “catarrhal jaundice” (likely hepatitis A) and more severe forms
Scientific Recognition and Viral Discovery
Early Scientific Understanding:
- 1885: Lürman documented an outbreak of “serum hepatitis” after smallpox vaccination using human lymph
- 1908: McDonald published evidence suggesting fecal-oral transmission of epidemic jaundice
- 1937: Findlay and MacCallum proposed viral etiology for certain forms of jaundice
- 1940s: During World War II, distinct forms of hepatitis were recognized:
- “Infectious hepatitis” (later identified as hepatitis A)
- “Serum hepatitis” (later identified as hepatitis B)
Viral Hepatitis Discovery Timeline:
Hepatitis B:
- 1963: Baruch Blumberg discovered the “Australia antigen” (hepatitis B surface antigen, HBsAg) in the blood of an Australian Aboriginal person
- 1968: Alfred Prince independently identified the same antigen in patients with serum hepatitis
- 1970: Dane visualized the complete hepatitis B virus particle (Dane particle) using electron microscopy
- 1976: Blumberg awarded the Nobel Prize for his discovery
Hepatitis A:
- 1973: Feinstone identified the hepatitis A virus using immune electron microscopy in stool samples
- 1979: Provost successfully cultured HAV in cell culture
Hepatitis C:
- 1975: Recognition of “non-A, non-B hepatitis” as a cause of post-transfusion hepatitis
- 1989: Michael Houghton, Qui-Lim Choo, and George Kuo at Chiron Corporation, along with Daniel Bradley at the CDC, identified the hepatitis C virus using molecular cloning techniques
- 2020: Harvey Alter, Michael Houghton, and Charles Rice awarded the Nobel Prize for the discovery of HCV
Hepatitis D:
- 1977: Mario Rizzetto discovered the hepatitis D virus (delta antigen) in the liver of HBV-infected patients
- 1986: HDV genome fully characterized as a unique RNA pathogen
Hepatitis E:
- 1978: Evidence of enterically transmitted non-A, non-B hepatitis from a waterborne epidemic in India
- 1983: Balayan visualized virus-like particles in stool samples
- 1990: Reyes and colleagues cloned and sequenced the HEV genome
Major Treatment Breakthroughs
Hepatitis B:
- 1981: First approval of interferon alpha for chronic hepatitis B
- 1998: Lamivudine, the first oral antiviral for HBV
- 2005-2008: Approval of entecavir and tenofovir, highly effective antivirals with minimal resistance
Hepatitis C:
- 1991: Interferon alpha approved for HCV treatment (10-20% cure rates)
- 1998: Combination therapy with ribavirin improved cure rates to 40%
- 2011: First direct-acting antivirals (telaprevir and boceprevir) approved
- 2013-2014: Introduction of sofosbuvir and other highly effective direct-acting antivirals (DAAs) with >95% cure rates
- 2018-2020: Pan-genotypic regimens allowing simpler treatment approaches
Preventive Advances:
- 1969: First passive immunization against hepatitis B with hepatitis B immune globulin (HBIG)
- 1981: First hepatitis B vaccine (plasma-derived) approved
- 1986: First recombinant hepatitis B vaccine
- 1995: Hepatitis A vaccine approved
- 2012: First combination hepatitis A and B vaccine
Evolution of Medical Understanding
Conceptual Shifts:
- 1940s-1950s: Recognition of different types of viral hepatitis
- 1960s-1970s: Identification of specific viral agents
- 1980s: Understanding of viral replication and natural history
- 1990s: Recognition of the global burden and public health implications
- 2000s: Transition from interferon-based to direct-acting antiviral therapies
- 2010s: Concept of viral hepatitis elimination as a public health goal
- 2020s: Integration of viral hepatitis services into universal health coverage
Paradigm Shifts in Treatment:
- From management of symptoms to targeting viral replication
- From interferon-based therapies with significant side effects to well-tolerated oral antivirals
- From complex, lengthy regimens to simple, short-course treatments
- From treating advanced disease to preventing progression through early intervention
- From individual clinical management to population-based elimination strategies
The history of hepatitis represents one of the most remarkable stories in modern medicine, transitioning from mysterious epidemic jaundice to well-characterized viral diseases with effective preventive and therapeutic options. This evolution has occurred through collaborative global efforts spanning basic science, epidemiology, clinical research, and public health implementation.
3. Symptoms
General Symptom Patterns
The symptoms of hepatitis vary based on the cause, severity, and whether the condition is acute or chronic. Many cases of hepatitis are asymptomatic or present with nonspecific symptoms, particularly in the early stages or in chronic forms.
Common Early Symptoms Across Hepatitis Types:
- Fatigue and malaise: Often the earliest and most persistent symptom
- Low-grade fever: Typically 38-38.5°C (100.4-101.3°F)
- Nausea and/or vomiting: May be intermittent
- Abdominal discomfort: Often in the right upper quadrant
- Decreased appetite (anorexia): Can lead to unintended weight loss
- Myalgia (muscle pain): Similar to flu-like symptoms
- Arthralgia (joint pain): Particularly common in hepatitis B and autoimmune hepatitis
Characteristic Hepatitis Symptoms:
- Jaundice: Yellowing of skin and sclera due to elevated bilirubin
- Dark urine: Due to bilirubin excretion
- Clay-colored stool: Due to reduced bile flow
- Hepatomegaly: Enlarged liver, sometimes tender to palpation
- Pruritus (itching): Due to bile salt accumulation in the skin
Symptoms by Hepatitis Type
Hepatitis A (HAV):
- Acute onset: Typically develops 2-6 weeks after exposure
- Severity: Usually self-limiting with complete recovery within 2 months
- Distinctive features:
- More pronounced gastrointestinal symptoms
- Jaundice present in 70-80% of adults but less common in children
- Cholestatic pattern (prolonged jaundice) in some cases
- Never progresses to chronic hepatitis
Hepatitis B (HBV):
- Acute phase: Symptoms appear 60-150 days after exposure
- Distinctive features:
- Serum sickness-like syndrome in some cases (fever, rash, arthralgia)
- 30% of adults develop jaundice
- 90% of infected adults clear the virus without chronic infection
- 90% of infected neonates develop chronic infection
Hepatitis C (HCV):
- Acute phase: Often asymptomatic (80% of cases)
- Distinctive features:
- Jaundice in only 20-30% of acute infections
- Insidious onset of fatigue, often without other symptoms
- 55-85% develop chronic infection
- Extrahepatic manifestations common (cryoglobulinemia, rashes, kidney disease)
Hepatitis D (HDV):
- Co-infection with HBV: More severe acute hepatitis than HBV alone
- Superinfection of chronic HBV: Acceleration of liver disease
- Distinctive features:
- Rapid progression to cirrhosis in many cases
- Higher rates of fulminant hepatitis
- Biphasic elevations of liver enzymes
Hepatitis E (HEV):
- Acute onset: Similar to HAV, typically self-limiting
- Distinctive features:
- Particularly severe in pregnant women (mortality up to 25%)
- Rare progression to chronic infection (mainly in immunocompromised patients)
- Neurological manifestations in some cases
Alcoholic Hepatitis:
- Onset: Develops after prolonged, heavy alcohol use
- Distinctive features:
- Jaundice with high bilirubin levels
- Ascites and edema
- Fever despite absence of infection
- Spider angiomata and palmar erythema
- Encephalopathy in severe cases
Autoimmune Hepatitis:
- Onset: Often insidious with nonspecific symptoms
- Distinctive features:
- Women affected more commonly than men
- Associated extrahepatic autoimmune conditions
- Amenorrhea in young women
- Acne, hirsutism with corticosteroid treatment
Drug-Induced Hepatitis:
- Timing: Variable, from days to months after starting medication
- Distinctive features:
- Hypersensitivity reactions (fever, rash, eosinophilia) in some cases
- Usually resolves with discontinuation of the offending agent
- Pattern can mimic viral, cholestatic, or mixed hepatitis
Progression of Symptoms
Acute Hepatitis Progression:
Prodromal Phase (3-10 days):
- Nonspecific flu-like symptoms
- Fatigue, low-grade fever
- Nausea, anorexia
- Right upper quadrant discomfort
Icteric Phase (2-6 weeks):
- Development of jaundice
- Darkening of urine
- Clay-colored stools
- Initial symptoms may improve or worsen
Recovery Phase (weeks to months):
- Gradual resolution of jaundice
- Return of energy and appetite
- Normalization of liver function tests
- Potential for relapsing and remitting course
Chronic Hepatitis Progression:
Early Chronic Phase (often asymptomatic):
- Minimal to no symptoms
- Normal to mildly abnormal liver function tests
- Viral replication ongoing (in viral hepatitis)
Mid-stage Chronic Hepatitis:
- Intermittent fatigue
- Mild cognitive effects (“brain fog”)
- Subtle extrahepatic manifestations
- Progressive fibrosis on liver biopsy
Advanced Chronic Hepatitis (with cirrhosis):
- Persistent fatigue and weakness
- Weight loss and muscle wasting
- Portal hypertension symptoms (ascites, edema)
- Spider angiomata, palmar erythema
- Gynecomastia and testicular atrophy in men
- Easy bruising and bleeding
- Hepatic encephalopathy
Special Symptom Considerations
Asymptomatic Presentations:
- 60-70% of acute HBV infections are asymptomatic
- 80% of acute HCV infections have no symptoms
- Most cases of NAFLD/NASH are detected incidentally
- Chronic viral hepatitis may remain asymptomatic until cirrhosis develops
Rare Symptom Presentations:
- Fulminant hepatitis: Rapid onset of liver failure with encephalopathy (rare but life-threatening)
- Aplastic anemia: Rare complication of viral hepatitis (particularly HBV)
- Cryoglobulinemic vasculitis: Associated with HCV, causing palpable purpura and neuropathy
- Polyarteritis nodosa: Rare vasculitis associated with HBV infection
- Guillain-Barré syndrome: Rarely reported after acute viral hepatitis
Extrahepatic Manifestations:
- Hepatitis B: Glomerulonephritis, polyarteritis nodosa, cryoglobulinemia
- Hepatitis C: Mixed cryoglobulinemia, membranoproliferative glomerulonephritis, porphyria cutanea tarda, lichen planus
- Autoimmune hepatitis: Associated with other autoimmune conditions (thyroiditis, ulcerative colitis, rheumatoid arthritis)
Understanding the varied symptom presentations of hepatitis is crucial for early recognition and management. The diverse manifestations reflect different etiologies, host responses, and disease stages, highlighting the need for comprehensive diagnostic approaches when hepatitis is suspected.
4. Causes
Viral Causes
Hepatitis A Virus (HAV):
- Classification: Single-stranded RNA virus in the Picornaviridae family
- Transmission:
- Fecal-oral route
- Contaminated food and water
- Person-to-person contact
- Occasional foodborne outbreaks
- Epidemiology:
- Endemic in regions with poor sanitation
- No chronic state; acute infection only
- Lifelong immunity after infection
Hepatitis B Virus (HBV):
- Classification: Partially double-stranded DNA virus in the Hepadnaviridae family
- Transmission:
- Perinatal (mother to child)
- Blood exposure (transfusions, needle sharing)
- Sexual contact
- Household contact (less common)
- Viral Characteristics:
- Eight major genotypes (A-H) with different geographical distributions
- Integrates into host genome
- Forms covalently closed circular DNA (cccDNA) in hepatocytes
- Persistent infection in 5-10% of adult cases
Hepatitis C Virus (HCV):
- Classification: Single-stranded RNA virus in the Flaviviridae family
- Transmission:
- Blood exposure (transfusions before 1992, needle sharing)
- Healthcare-associated infections
- Sexual transmission (relatively inefficient)
- Perinatal transmission (5-10% risk)
- Viral Characteristics:
- Eight major genotypes with numerous subtypes
- High mutation rate leading to quasispecies
- No integration into host genome
- Persistent infection in 55-85% of cases
Hepatitis D Virus (HDV):
- Classification: Defective RNA virus requiring HBV for replication
- Transmission: Same routes as HBV
- Unique Features:
- Only infects individuals with HBV
- Can occur as co-infection or superinfection
- Associated with more severe disease and faster progression to cirrhosis
Hepatitis E Virus (HEV):
- Classification: Single-stranded RNA virus in the Hepeviridae family
- Transmission:
- Primarily fecal-oral route
- Zoonotic transmission from animals (pigs, deer)
- Contaminated water sources
- Epidemiological Features:
- Four main genotypes with different geographical distributions
- Genotypes 1 and 2 cause waterborne outbreaks in developing countries
- Genotypes 3 and 4 cause sporadic cases in developed countries
- Chronic infection possible in immunocompromised individuals
Non-Viral Causes
Alcoholic Hepatitis:
- Mechanism:
- Direct hepatotoxicity from alcohol metabolism
- Acetaldehyde formation
- Oxidative stress and mitochondrial dysfunction
- Increased gut permeability leading to endotoxemia
- Immune-mediated liver injury
- Risk Factors:
- Quantity and duration of alcohol consumption
- Pattern of drinking (binge drinking)
- Nutritional status
- Genetic factors (PNPLA3, TM6SF2 variants)
- Female gender (higher susceptibility)
Drug-Induced Hepatitis:
- Mechanisms:
- Direct hepatotoxicity
- Immune-mediated reactions
- Metabolic idiosyncrasy
- Mitochondrial toxicity
- Common Culprits:
- Acetaminophen (dose-dependent toxicity)
- Antibiotics (amoxicillin-clavulanate, isoniazid)
- NSAIDs
- Statins
- Antiepileptics
- Herbal supplements (kava, comfrey, green tea extract)
- Chemotherapeutic agents
Autoimmune Hepatitis:
- Mechanism: Loss of immune tolerance to hepatic antigens
- Subtypes:
- Type 1: Anti-smooth muscle antibodies (ASMA) and/or antinuclear antibodies (ANA)
- Type 2: Anti-liver kidney microsomal antibodies (anti-LKM1)
- Type 3: Antibodies against soluble liver antigen (anti-SLA)
- Genetic Associations:
- HLA-DR3 and HLA-DR4 haplotypes
- CTLA4 and TNF-α polymorphisms
Nonalcoholic Fatty Liver Disease (NAFLD) and Nonalcoholic Steatohepatitis (NASH):
- Mechanism:
- Insulin resistance
- Lipotoxicity
- Oxidative stress
- Gut microbiome dysbiosis
- Proinflammatory cytokine activation
- Risk Factors:
- Obesity
- Type 2 diabetes
- Metabolic syndrome
- Dyslipidemia
- Genetic factors (PNPLA3, TM6SF2)
Toxic Hepatitis:
- Environmental Toxins:
- Industrial chemicals (vinyl chloride, carbon tetrachloride)
- Aflatoxins (produced by Aspergillus fungi)
- Poisonous mushrooms (Amanita phalloides)
- Heavy metals (arsenic, copper)
- Mechanism: Direct cellular damage, mitochondrial dysfunction, or immune-mediated
Genetic and Hereditary Factors
Primary Genetic Liver Diseases:
- Alpha-1 antitrypsin deficiency: Misfolded protein accumulation leading to hepatitis and cirrhosis
- Hemochromatosis: Iron overload causing liver damage
- Wilson’s disease: Copper accumulation in the liver and other organs
- Glycogen storage diseases: Various enzymatic defects affecting liver function
Genetic Factors Influencing Viral Hepatitis:
- HBV clearance: HLA class II alleles influence spontaneous clearance rates
- HCV spontaneous clearance: IL28B polymorphism strongly affects clearance probability
- HCV treatment response: IL28B genotype affects response to interferon-based therapy
- HEV susceptibility: Increased in pregnant women, potentially due to hormonal factors
Genetic Susceptibility to Drug-Induced Liver Injury:
- Acetaminophen metabolism: Variations in CYP2E1, glutathione S-transferase
- Isoniazid hepatotoxicity: NAT2 slow acetylator phenotype
- Flucloxacillin injury: HLA-B*5701 association
- Amoxicillin-clavulanate: HLA-A0201 and DRB11501-DQB1*0602 haplotypes
Environmental and Trigger Factors
Environmental Exposures:
- Contaminated water sources: HAV and HEV transmission
- Food contamination: HAV in shellfish, HEV in undercooked pork
- Industrial chemicals: Vinyl chloride, carbon tetrachloride
- Agricultural toxins: Aflatoxins
- Healthcare-associated exposures: Needle-stick injuries, inadequate sterilization
Trigger Factors for Autoimmune Hepatitis:
- Viral infections: May trigger autoimmune response in genetically susceptible individuals
- Medications: Nitrofurantoin, minocycline, hydralazine
- Pregnancy and postpartum period: Hormonal fluctuations may trigger disease
- Environmental exposures: Specific triggers largely unknown
Factors Exacerbating Existing Hepatitis:
- Alcohol consumption: Accelerates progression in all forms of chronic hepatitis
- Obesity and metabolic syndrome: Increases fibrosis progression in viral hepatitis
- Hepatotoxic medications: Can worsen existing liver disease
- Viral co-infections: HBV/HCV, HBV/HDV, HIV co-infection accelerate disease
- Iron overload: Secondary iron accumulation worsens liver damage
The diverse causes of hepatitis highlight the liver’s vulnerability to various insults, whether infectious, toxic, metabolic, or immune-mediated. Understanding these causes is essential for prevention, accurate diagnosis, and appropriate management strategies. The complex interplay between genetic susceptibility and environmental factors contributes to the variable presentation and progression of hepatitis across individuals.
5. Risk Factors
Demographic Risk Factors
Age-Related Factors:
- Hepatitis A:
- Children in endemic areas (often asymptomatic infections)
- Travelers from low to high endemic regions (all ages)
- Elderly have more severe disease if infected
- Hepatitis B:
- Neonates born to HBV-positive mothers (90% become chronically infected without intervention)
- Adults aged 20-40 (highest rates of new infections in many regions)
- Hepatitis C:
- Baby boomers (born 1945-1965) in the US (prevalence 2.6%, accounting for 75% of cases)
- Increasing infection rates in young adults (20-40) due to injection drug use
- Alcoholic Hepatitis:
- Peak age 40-60 years after decades of heavy drinking
- Autoimmune Hepatitis:
- Bimodal distribution: peaks in late teens/early 20s and in 50s-60s
- NAFLD/NASH:
- Increasing prevalence with age, peaking in 40s-60s
Gender Differences:
- Hepatitis B:
- Higher rates in males
- Men less likely to clear acute infection
- More rapid disease progression in men
- Hepatitis C:
- Slightly higher prevalence in males
- Women more likely to spontaneously clear acute infection
- Slower fibrosis progression in premenopausal women
- Alcoholic Hepatitis:
- Women more susceptible to alcohol-induced liver damage (develop at lower intake levels)
- Autoimmune Hepatitis:
- Strong female predominance (70-80% of cases)
- Type 2 AIH shows 90% female predominance
- NAFLD/NASH:
- Similar prevalence between genders, with slight male predominance in some studies
Racial and Ethnic Factors:
- Hepatitis B:
- High endemic rates in East Asia, sub-Saharan Africa
- 5-12% prevalence in Asian Americans and Pacific Islanders
- Lower rates in Western Europe and North America (0.2-0.5%)
- Hepatitis C:
- High prevalence in Egypt (>10%), Mongolia, Pakistan
- Higher rates in Hispanic and Black populations in the US
- Alcoholic Hepatitis:
- Variations in alcohol-metabolizing enzymes across ethnicities
- ALDH2 genetic variants common in East Asians (reduced alcohol tolerance)
- NAFLD/NASH:
- Higher prevalence in Hispanic populations
- Lower prevalence in African Americans despite similar obesity rates
- Autoimmune Hepatitis:
- Type 1 more common in Caucasians and Japanese
- Type 2 more common in Southern Europe
Behavioral and Lifestyle Risk Factors
Substance Use:
- Alcohol Consumption:
- Risk threshold: >40g/day for men, >20g/day for women
- Drinking pattern (binge drinking increases risk)
- Synergistic effect with viral hepatitis, NAFLD
- Injection Drug Use (IDU):
- Primary risk factor for HCV in developed countries
- Also significant risk for HBV
- Sharing of needles, syringes, or other equipment
- Higher risk with longer duration of IDU
- Non-Injection Drug Use:
- Intranasal cocaine use (sharing straws)
- Crack cocaine use (lip burns and sharing pipes)
Sexual Behaviors:
- Unprotected Sex:
- Major risk factor for HBV transmission
- Less efficient for HCV transmission (except in MSM with HIV)
- Multiple partners increase risk
- Men who have sex with men at higher risk
- Sex Work:
- Increased risk for both acquiring and transmitting HBV
- Variable risk for HCV depending on other practices
Dietary and Metabolic Factors:
- Obesity (BMI >30): Strong risk factor for NAFLD/NASH
- Western Diet:
- High in saturated fats, refined carbohydrates
- Low in polyunsaturated fats, fiber
- Associated with NAFLD progression
- Rapid Weight Changes:
- Quick weight loss can exacerbate NASH
- Yo-yo dieting may increase risk
- Sugar-Sweetened Beverages:
- Associated with increased hepatic fat
- Fructose particularly implicated
Occupational, Environmental, and Medical Risk Factors
Occupational Exposures:
- Healthcare Workers:
- Needle-stick injuries
- Exposure to blood and body fluids
- Risk reduced with universal precautions and vaccination
- Emergency Services Personnel:
- First responders, paramedics
- Exposure during trauma care
- Laboratory Workers:
- Handling biological specimens
- Research with infectious agents
- Sewage Workers:
- Potential exposure to HAV and HEV
- Slaughterhouse/Meat Processing Workers:
- Potential exposure to HEV from pigs
Environmental Factors:
- Contaminated Water Sources:
- Primary risk for HAV and HEV
- Public water systems in low-resource settings
- Well water in agricultural areas
- Food Contamination:
- Shellfish for HAV
- Undercooked pork for HEV
- Crops contaminated with aflatoxins
- Institutional Settings:
- Prisons, military barracks
- Long-term care facilities
- Daycare centers (HAV)
Medical and Iatrogenic Factors:
- Blood Transfusions:
- Major historical risk for HBV and HCV before screening
- Current risk very low in developed countries
- Remains a risk in regions without adequate screening
- Organ Transplantation:
- Similar risk profile as transfusions
- Donor screening has reduced risk substantially
- Hemodialysis:
- Increased risk for HBV and HCV
- Multiple exposures to blood products
- Shared equipment risk in inadequate settings
- Medical Procedures:
- Inadequate sterilization of equipment
- Unsafe injection practices
- Endoscopy with improper reprocessing
- Medications:
- Over 1,000 medications associated with drug-induced liver injury
- Immunosuppressive agents (reactivation of latent HBV)
- Estrogens (cholestatic liver injury)
- Methotrexate (cumulative hepatotoxicity)
Pre-existing Conditions and Genetic Predispositions
Pre-existing Health Conditions:
- HIV Infection:
- Accelerated progression of HBV and HCV
- Reduced response to HBV vaccination
- Higher risk of HCV sexual transmission
- Diabetes Mellitus:
- Increases risk and severity of NAFLD/NASH
- Associated with worse outcomes in all forms of hepatitis
- Increases HCC risk in chronic viral hepatitis
- Obesity:
- Primary driver of NAFLD/NASH
- Worsens progression of viral hepatitis
- Reduces response to HBV vaccination
- Other Autoimmune Diseases:
- Increased risk for autoimmune hepatitis
- Commonly co-occur with thyroid disorders, celiac disease
Genetic Predispositions:
- HLA Associations:
- HLA-DR3, DR4 for autoimmune hepatitis
- HLA-B*5701 for flucloxacillin hepatotoxicity
- HLA class II variants for HBV clearance
- Metabolic Gene Variants:
- PNPLA3 (I148M variant): Increases risk for alcoholic liver disease and NAFLD
- TM6SF2: Affects fat metabolism in the liver
- MBOAT7: Influences liver fat content
- Other Genetic Factors:
- IL28B polymorphisms: Affect spontaneous and treatment-induced HCV clearance
- Alpha-1 antitrypsin variants: Z and S alleles increase liver disease risk
- Hemochromatosis (HFE) mutations: Iron overload affecting liver
Understanding the complex interplay of risk factors is essential for identifying high-risk individuals, implementing targeted screening programs, and developing personalized prevention strategies. Many risk factors are modifiable, offering opportunities for public health interventions and individual lifestyle changes to reduce hepatitis burden globally.
6. Complications
Acute Complications
Fulminant Hepatic Failure:
- Definition: Severe liver dysfunction with encephalopathy developing within 8 weeks of symptom onset
- Incidence:
- Hepatitis A: <1% of cases
- Hepatitis B: 0.1-1% of acute cases
- Hepatitis E: 1-2% generally, up to 20-25% in pregnant women
- Drug-induced: Variable (high with acetaminophen overdose)
- Clinical Features:
- Jaundice
- Coagulopathy (INR >1.5)
- Hepatic encephalopathy
- Cerebral edema
- Multi-organ failure
- Outcomes:
- Mortality 60-80% without liver transplantation
- Liver transplantation improves survival to 60-80%
Severe Acute Alcoholic Hepatitis:
- Maddrey’s Discriminant Function >32 indicates severe disease
- Clinical Features:
- Jaundice
- Ascites
- Hepatic encephalopathy
- Fever and leukocytosis
- Complications:
- Hepatorenal syndrome
- Gastrointestinal bleeding
- Infections
- Mortality: 30-50% 30-day mortality without treatment
Acute Kidney Injury:
- Hepatorenal Syndrome:
- Type 1: Rapid progression, poor prognosis
- Type 2: Moderate renal dysfunction
- Acute Tubular Necrosis:
- From hypotension, sepsis
- Drug toxicity
- Incidence: Occurs in up to 20% of hospitalized patients with acute hepatitis
Electrolyte Disturbances:
- Hyponatremia: Common in advanced liver disease
- Hypokalemia: Due to secondary hyperaldosteronism
- Acid-base disorders: Respiratory alkalosis, metabolic acidosis
Acute Coagulopathy:
- Mechanism: Reduced synthesis of clotting factors, thrombocytopenia
- Clinical Significance: Increased bleeding risk, complicates invasive procedures
- Monitoring: INR, platelet count
Chronic Complications
Cirrhosis:
- Definition: Diffuse fibrosis and nodule formation, disrupting liver architecture
- Progression Rates:
- HBV: 2-10% per year in untreated chronic infection
- HCV: 15-30% develop cirrhosis within 20 years
- Alcoholic hepatitis: Variable, accelerated with continued drinking
- NASH: 20-30% of cases progress to advanced fibrosis
- Types:
- Compensated: Preserved liver function
- Decompensated: Clinical complications present
Portal Hypertension:
- Mechanism: Increased resistance to portal blood flow
- Clinical Manifestations:
- Esophageal and gastric varices
- Portal hypertensive gastropathy
- Splenomegaly
- Ascites
- Portosystemic encephalopathy
- Severity Measurement: Hepatic venous pressure gradient (HVPG)
Esophageal and Gastric Varices:
- Incidence: Develop in 50-60% of cirrhotic patients
- Bleeding Risk: 30-40% lifetime risk of variceal hemorrhage
- Mortality: 15-20% mortality per bleeding episode
Ascites:
- Definition: Pathological fluid accumulation in the peritoneal cavity
- Incidence: Develops in 50% of patients within 10 years of cirrhosis diagnosis
- Complications:
- Spontaneous bacterial peritonitis (SBP)
- Respiratory compromise
- Umbilical hernias
- Poor quality of life
- Refractory Ascites: 5-10% become resistant to diuretic therapy
Hepatic Encephalopathy:
- Definition: Neuropsychiatric syndrome due to liver dysfunction
- Prevalence: 30-45% of cirrhotic patients
- Grading:
- Grade 1: Mild confusion, attention deficit
- Grade 2: Lethargy, disorientation
- Grade 3: Somnolence, marked confusion
- Grade 4: Coma
- Precipitating Factors:
- Infections
- Gastrointestinal bleeding
- Electrolyte disturbances
- Medications (sedatives, diuretics)
- Constipation
- Dehydration
Hepatopulmonary Syndrome and Portopulmonary Hypertension:
- Hepatopulmonary Syndrome:
- Prevalence: 5-30% of cirrhotic patients
- Features: Intrapulmonary vascular dilations, hypoxemia
- Impact: Increases mortality, potential contraindication for transplant
- Portopulmonary Hypertension:
- Prevalence: 2-8% of cirrhotic patients
- Features: Pulmonary arterial hypertension due to portal hypertension
- Impact: Increases perioperative risk in transplantation
Hepatocellular Carcinoma (HCC)
Epidemiology:
- Annual Incidence in Cirrhosis:
- HBV-related: 2-8%
- HCV-related: 1-8%
- Alcoholic cirrhosis: 1-2%
- NASH cirrhosis: 1-2%
- Risk Factors:
- Male gender
- Older age
- Family history of HCC
- Alcohol consumption
- Aflatoxin exposure
- Obesity and diabetes
- Viral coinfections
Natural History:
- Development: Usually in the setting of cirrhosis (80-90% of cases)
- Growth Rate: Variable, doubling time of 2-6 months
- Spread: Intrahepatic metastasis common
Surveillance Recommendations:
- Populations: Cirrhotic patients, non-cirrhotic HBV carriers with risk factors
- Methods: Ultrasound ± alpha-fetoprotein every 6 months
- Benefit: Early detection improves treatment options and outcomes
Treatment Options:
- Curative Intent:
- Surgical resection
- Liver transplantation
- Ablative therapies (radiofrequency, microwave)
- Palliative:
- Transarterial chemoembolization (TACE)
- Radioembolization (Y90)
- Systemic therapy (kinase inhibitors, immunotherapy)
Extrahepatic Complications
Cryoglobulinemia (HCV-associated):
- Prevalence: 40-60% serological presence, 5-10% symptomatic
- Manifestations:
- Palpable purpura
- Arthralgia
- Peripheral neuropathy
- Membranoproliferative glomerulonephritis
- Treatment: Antiviral therapy plus immunosuppression in severe cases
Renal Complications:
- Membranoproliferative Glomerulonephritis (HCV)
- Membranous Nephropathy (HBV)
- IgA Nephropathy (Autoimmune and viral hepatitis)
- Polyarteritis Nodosa (HBV)
Hematological Complications:
- Thrombocytopenia: Due to hypersplenism, bone marrow suppression
- Anemia: Multiple etiologies
- Neutropenia: Especially with treatment (interferon)
- Coagulopathy: Factor deficiencies, dysfibrinogenemia
Endocrine and Metabolic Complications:
- Insulin resistance and diabetes: Common in HCV, NAFLD
- Hypogonadism: Low testosterone in men with cirrhosis
- Osteoporosis: Increased fracture risk
- Malnutrition: Poor nutrient absorption, altered metabolism
Disability and Mortality
Disability Impact:
- Work Productivity:
- 30-60% reduction in work productivity
- Higher rates of disability claims and early retirement
- Quality of Life:
- Significant impairment across physical and mental domains
- Fatigue as a predominant disabling symptom
- Sleep disturbances in 60-80% of patients
- Healthcare Utilization:
- Frequent hospitalizations
- High outpatient resource utilization
- Medication burden
Mortality Statistics:
- Acute Viral Hepatitis:
- Overall mortality <1% except in special populations
- Hepatitis E in pregnancy: 20-25% mortality
- Cirrhosis:
- Compensated: 5-year survival 80-85%
- Decompensated: 5-year survival 14-35%
- Alcoholic Hepatitis:
- Severe disease: 30-day mortality 30-50%
- 1-year mortality up to 70% with continued drinking
- Hepatocellular Carcinoma:
- Overall 5-year survival: 18% (US data)
- Early stage with curative treatment: 5-year survival 40-70%
- Advanced stage: Median survival <1 year
Global Mortality Burden:
- Viral hepatitis: 1.4 million deaths annually
- Alcoholic liver disease: 0.5-1 million deaths annually
- NAFLD/NASH: Rapidly increasing, currently 0.2-0.5 million annually
- Total liver disease: Approximately 2 million deaths annually
The complex spectrum of complications associated with hepatitis underscores the importance of early detection, appropriate management, and preventive strategies. Many complications can be prevented or ameliorated with timely intervention, highlighting the critical need for increased awareness, screening, and access to care for individuals at risk for or affected by hepatitis.
7. Diagnosis & Testing
Clinical Assessment and Initial Evaluation
History and Physical Examination:
Key History Elements:
- Risk factors for viral hepatitis
- Alcohol consumption (quantity, pattern, duration)
- Medication and supplement use
- Family history of liver disease
- Travel history
- Occupational exposures
- Timeline of symptom development
Physical Examination Findings:
- Jaundice (scleral icterus, skin yellowing)
- Hepatomegaly (enlarged liver)
- Splenomegaly (enlarged spleen)
- Ascites (fluid in peritoneal cavity)
- Spider angiomata (vascular lesions on skin)
- Palmar erythema (reddening of palms)
- Dupuytren’s contracture
- Asterixis (flapping tremor)
- Caput medusae (dilated periumbilical veins)
- Gynecomastia (breast enlargement in males)
- Testicular atrophy
- Peripheral edema
Initial Laboratory Tests:
Liver Function Tests:
- Aminotransferases (ALT, AST): Indicators of hepatocellular damage
- Alkaline phosphatase (ALP): Marker of biliary obstruction
- Gamma-glutamyl transferase (GGT): Sensitive but nonspecific
- Bilirubin (total and direct): Elevated in various liver disorders
- Albumin: Marker of synthetic function
- Prothrombin time (PT)/INR: Indicator of coagulation function
Complete Blood Count (CBC):
- Anemia (various etiologies)
- Thrombocytopenia (hypersplenism, bone marrow suppression)
- Leukocytosis (infection, alcoholic hepatitis)
- Leukopenia (viral suppression, hypersplenism)
Basic Metabolic Panel:
- Electrolyte abnormalities
- Renal function
- Glucose levels
Patterns of Laboratory Abnormalities:
- Hepatocellular pattern: Predominant elevation of ALT/AST
- Cholestatic pattern: Predominant elevation of ALP/GGT
- Mixed pattern: Both hepatocellular and cholestatic features
- Synthetic dysfunction: Low albumin, prolonged PT/INR
Specific Diagnostic Tests for Viral Hepatitis
Hepatitis A:
- Anti-HAV IgM: Indicates acute infection
- Anti-HAV IgG: Indicates prior infection or vaccination
- Interpretation:
- Acute HAV: Positive IgM, may or may not have IgG
- Prior HAV/Immunized: Negative IgM, positive IgG
Hepatitis B:
HBsAg (Hepatitis B surface antigen): Indicates active infection
Anti-HBs (Antibody to surface antigen): Indicates recovery or vaccination
HBeAg (Hepatitis B e antigen): Marker of viral replication
Anti-HBe (Antibody to e antigen): Indicates decreased viral replication
Anti-HBc IgM: Acute infection
Anti-HBc IgG: Previous exposure
HBV DNA: Measures viral load
Interpretation Examples:
- Acute HBV: HBsAg+, Anti-HBc IgM+, HBeAg+, HBV DNA high
- Chronic active HBV: HBsAg+, Anti-HBc IgG+, HBeAg+/-, HBV DNA detectable
- Resolved HBV: HBsAg-, Anti-HBs+, Anti-HBc IgG+
- Vaccinated: HBsAg-, Anti-HBs+, Anti-HBc-
Hepatitis C:
- Anti-HCV: Antibody indicating exposure
- HCV RNA: Confirms active infection, measures viral load
- HCV genotype: Determines treatment approach (less relevant with pan-genotypic DAAs)
- Interpretation:
- Current HCV: Anti-HCV+, HCV RNA+
- Cleared HCV (spontaneous or treated): Anti-HCV+, HCV RNA-
- False positive: Anti-HCV+, HCV RNA- (without prior infection)
Hepatitis D:
- Anti-HDV: Antibody indicating exposure
- HDV RNA: Confirms active infection
- Testing Context: Only relevant in HBsAg-positive individuals
Hepatitis E:
- Anti-HEV IgM: Acute infection
- Anti-HEV IgG: Prior infection
- HEV RNA: Confirms active infection (particularly important in immunocompromised)
Testing for Non-Viral Hepatitis
Alcoholic Liver Disease:
- Alcohol Biomarkers:
- Carbohydrate-deficient transferrin (CDT)
- Phosphatidylethanol (PEth)
- Ethyl glucuronide (EtG) and ethyl sulfate (EtS)
- Gamma-glutamyl transferase (GGT)
- Mean corpuscular volume (MCV)
- AST/ALT Ratio: Typically >2:1 in alcoholic hepatitis
- Other Tests: Exclude other etiologies
Nonalcoholic Fatty Liver Disease/NASH:
- Exclusion Diagnosis: Rule out other causes of hepatitis and significant alcohol consumption
- Scoring Systems:
- Fatty Liver Index (FLI)
- NAFLD Fibrosis Score
- FIB-4 index
- APRI score
- Specialized Tests:
- Cytokeratin-18 fragments (marker of hepatocyte apoptosis)
- Pro-C3 (marker of collagen formation)
Autoimmune Hepatitis:
- Autoantibodies:
- Antinuclear antibody (ANA)
- Anti-smooth muscle antibody (ASMA)
- Anti-liver kidney microsomal antibody (anti-LKM1)
- Anti-soluble liver antigen (anti-SLA)
- Immunoglobulins: Elevated IgG levels (typically >1.5x upper limit)
- Scoring Systems:
- International Autoimmune Hepatitis Group (IAIHG) score
- Simplified diagnostic criteria
Drug-Induced Liver Injury:
- Causality Assessment:
- RUCAM (Roussel Uclaf Causality Assessment Method)
- DILIN (Drug-Induced Liver Injury Network) scale
- Rechallenge: Generally avoided due to risk
- Drug-specific markers: Limited availability
Genetic and Metabolic Liver Diseases:
- Alpha-1 Antitrypsin: Serum levels and phenotyping
- Ceruloplasmin and Copper Studies: For Wilson’s disease
- Iron Studies: Ferritin, transferrin saturation for hemochromatosis
- Genetic Testing:
- HFE gene mutations (hemochromatosis)
- ATP7B mutations (Wilson’s disease)
- SERPINA1 mutations (alpha-1 antitrypsin deficiency)
Imaging and Invasive Procedures
Ultrasound:
- Applications:
- First-line imaging for hepatic evaluation
- Assessment of liver size, contour, echotexture
- Detection of focal lesions
- Evaluation of biliary system
- Portal vein assessment
- Guidance for procedures
- Advantages: Non-invasive, no radiation, widely available, relatively low cost
- Limitations: Operator-dependent, limited sensitivity for diffuse disease
Computed Tomography (CT):
- Applications:
- Detailed liver parenchyma evaluation
- Characterization of focal lesions
- Staging of malignancies
- Portal venous system assessment
- Evaluation of complications
- Advantages: Rapid acquisition, excellent detail, less operator-dependent
- Limitations: Radiation exposure, contrast risks, cost
Magnetic Resonance Imaging (MRI):
- Applications:
- Superior soft tissue characterization
- Fat quantification (MR spectroscopy)
- Iron quantification
- Biliary tract imaging (MRCP)
- Diffusion-weighted imaging for lesion characterization
- Advantages: No radiation, excellent contrast resolution, functional information
- Limitations: Cost, availability, contraindications (metallic implants)
Elastography Techniques:
- Transient Elastography (FibroScan):
- Non-invasive assessment of liver stiffness
- Correlates with fibrosis stage
- Can include controlled attenuation parameter (CAP) for steatosis
- Magnetic Resonance Elastography:
- More accurate than ultrasound techniques
- Evaluates entire liver
- Less affected by obesity
- Shear Wave Elastography:
- Incorporated into conventional ultrasound
- Real-time assessment
Liver Biopsy:
- Indications:
- Diagnosis of unclear etiology
- Assessment of disease severity/staging
- Evaluation of treatment response
- Diagnosis of focal lesions
- Approaches:
- Percutaneous (most common)
- Transjugular (for patients with coagulopathy or ascites)
- Surgical (open or laparoscopic)
- Endoscopic ultrasound-guided
- Information Provided:
- Inflammation grade
- Fibrosis stage
- Steatosis quantification
- Iron/copper deposition
- Architectural changes
- Specific histological patterns
- Limitations:
- Sampling error (examines ~1/50,000 of liver)
- Invasive procedure with complications
- Inter-observer variability
Nuclear Medicine Studies:
- Hepatobiliary Iminodiacetic Acid (HIDA) Scan:
- Assessment of biliary tract function
- Diagnosis of biliary obstruction
- FDG-PET/CT:
- Limited for primary HCC (often not FDG-avid)
- Useful for metastasis detection
- Evaluation of treatment response
Early Detection and Screening Approaches
Hepatitis B Screening:
- Recommended Populations:
- Individuals born in high-prevalence regions
- Men who have sex with men
- Injection drug users
- Household and sexual contacts of HBV-infected persons
- Pregnant women
- Individuals requiring immunosuppression
- Tests: HBsAg, anti-HBs, anti-HBc
- Frequency: One-time testing for most; periodic for ongoing risk
Hepatitis C Screening:
- Current Recommendations (many countries):
- Universal one-time screening for adults
- More frequent screening for high-risk individuals
- Tests: Anti-HCV followed by HCV RNA if positive
- Benefit: Early detection allows treatment before fibrosis development
Liver Cancer Surveillance:
- Target Populations:
- Cirrhotic patients of any etiology
- Non-cirrhotic HBV carriers with risk factors
- Non-cirrhotic F3 fibrosis in some guidelines
- Modality: Ultrasound ± alpha-fetoprotein
- Frequency: Every 6 months
- Efficacy: Early detection improves treatment options and outcomes
Emerging Biomarkers and Technologies:
- Liquid Biopsy:
- Circulating tumor DNA for HCC detection
- Cell-free DNA methylation patterns
- Proteomic Markers:
- Combinatorial protein panels
- Glycoprotein profiles
- MicroRNA Profiles:
- Serum miRNA signatures for disease detection
- Potential for early fibrosis detection
- Breath Testing:
- Volatile organic compounds as disease markers
- Non-invasive and potentially cost-effective
Accurate diagnosis of hepatitis requires a comprehensive approach integrating clinical, laboratory, imaging, and sometimes histological data. The diagnostic strategy should be tailored to the suspected etiology, available resources, and patient-specific factors. Early detection through appropriate screening of at-risk populations remains a cornerstone of effective hepatitis management, enabling timely intervention to prevent disease progression and complications.
8. Treatment Options
Viral Hepatitis Treatment
Hepatitis A:
- Primarily supportive care as the infection is self-limiting
- Treatment focuses on:
- Adequate hydration
- Nutritional support
- Symptomatic relief
- Avoidance of hepatotoxic medications and alcohol
- No specific antiviral therapy required
- Hospitalization for severe cases with:
- Dehydration
- Coagulopathy
- Encephalopathy
- Severe vomiting
Hepatitis B:
Acute Hepatitis B:
- Most cases resolve spontaneously with supportive care
- Antiviral therapy considered for:
- Severe or protracted cases
- Patients with underlying liver disease
- Healthcare workers (to expedite return to work)
- Options include entecavir or tenofovir
Chronic Hepatitis B:
- Treatment Indications:
- Elevated ALT and HBV DNA >2,000 IU/mL
- Cirrhosis with any detectable HBV DNA
- Family history of HCC
- Extrahepatic manifestations
- First-line Medications:
- Entecavir: One pill daily, minimal resistance, well-tolerated
- Tenofovir disoproxil fumarate (TDF): One pill daily, minimal resistance, bone/kidney monitoring
- Tenofovir alafenamide (TAF): One pill daily, improved safety profile compared to TDF
- Alternative Medications:
- Pegylated interferon alfa: 48-week course, immune modulator, higher side effect profile
- Lamivudine, adefovir, telbivudine: Less commonly used due to resistance issues
- Treatment Goals:
- Sustained suppression of viral replication
- HBeAg seroconversion (in HBeAg-positive patients)
- Biochemical normalization
- Histological improvement
- Rare cases achieve HBsAg clearance (functional cure)
- Treatment Duration:
- HBeAg-positive: Consider stopping after HBeAg seroconversion and 12 months consolidation
- HBeAg-negative: Typically indefinite treatment
- Cirrhotic patients: Indefinite treatment
Hepatitis C:
- Direct-Acting Antivirals (DAAs):
- Revolutionized treatment with >95% cure rates
- 8-12 week regimens
- Minimal side effects
- Oral administration
- Pan-genotypic Regimens:
- Sofosbuvir/velpatasvir: One pill daily for 12 weeks
- Glecaprevir/pibrentasvir: Three pills once daily for 8-12 weeks
- Sofosbuvir/velpatasvir/voxilaprevir: Rescue regimen for prior DAA failure
- Genotype-Specific Regimens (less commonly used now):
- Elbasvir/grazoprevir
- Sofosbuvir/ledipasvir
- Ombitasvir/paritaprevir/ritonavir plus dasabuvir
- Special Populations:
- Decompensated cirrhosis: Protease inhibitors contraindicated
- Renal impairment: Specific regimens indicated
- Post-transplant: Drug interactions important consideration
- HIV co-infection: Drug interactions with antiretrovirals
- Treatment Goal: Sustained virologic response (SVR) defined as undetectable HCV RNA 12 weeks after treatment completion (considered cure)
Hepatitis D:
- Bulevirtide (Hepcludex): First approved therapy for chronic HDV
- Blocks NTCP receptor preventing viral entry
- Administered subcutaneously
- 25-50% HDV RNA reduction rates
- Pegylated Interferon: Limited efficacy (25-30% response)
- 48-week treatment course
- High relapse rates
- Significant side effects
- Nucleos(t)ide Analogs: Suppress underlying HBV but minimal direct effect on HDV
- Combination Approaches: Under investigation
Hepatitis E:
- Acute Hepatitis E: Supportive care, usually self-limiting
- Chronic Hepatitis E (immunocompromised patients):
- Ribavirin: 12-24 weeks, 70-85% sustained response
- Reduction of immunosuppression when feasible
- Pegylated interferon in select cases
- Special consideration for pregnant women: Close monitoring due to high mortality
Non-Viral Hepatitis Treatment
Alcoholic Hepatitis:
- Abstinence: Cornerstone of therapy
- Addiction counseling
- Support groups
- Pharmacotherapy for alcohol use disorder (acamprosate, naltrexone)
- Nutritional Support:
- High-calorie, high-protein diet
- Vitamin supplementation (especially B vitamins)
- Enteral feeding if needed
- Pharmacological Treatment (for severe alcoholic hepatitis):
- Corticosteroids: Prednisolone 40mg daily for 4 weeks if Maddrey’s DF >32
- Pentoxifylline: Alternative if contraindications to steroids
- N-acetylcysteine: May improve outcomes when combined with steroids
- Liver Transplantation:
- Considered in select cases after established sobriety
- Early liver transplantation protocols under evaluation
Nonalcoholic Steatohepatitis (NASH):
- Lifestyle Modifications:
- Weight loss (7-10% body weight goal)
- Mediterranean diet
- Regular exercise (150+ minutes/week)
- Avoidance of excess fructose and saturated fat
- Pharmacological Approaches:
- Vitamin E: Shown benefit in non-diabetic NASH
- Pioglitazone: May improve histology
- GLP-1 receptor agonists: Promote weight loss and may improve liver histology
- Obeticholic acid: FXR agonist with promising results (pending approval)
- Bariatric Surgery:
- Considered for patients with BMI >35
- Significant improvements in NASH histology in many patients
- Emerging Therapies (in clinical trials):
- CCR2/CCR5 antagonists
- FGF21 analogues
- THR-β agonists
- Combination approaches
Autoimmune Hepatitis:
- Induction Therapy:
- Prednisone/prednisolone: 30-60 mg/day initially
- Often combined with azathioprine (50-150 mg/day)
- Response assessed at 2-4 weeks with follow-up liver tests
- Maintenance Therapy:
- Gradual steroid taper to lowest effective dose
- Long-term azathioprine monotherapy when possible
- Treatment duration typically years, often indefinite
- Alternative Treatments (for intolerance or inadequate response):
- Mycophenolate mofetil
- Calcineurin inhibitors (cyclosporine, tacrolimus)
- 6-mercaptopurine
- Methotrexate
- Rituximab
- Treatment Endpoints:
- Biochemical remission (normal ALT/AST)
- Histological remission (minimal inflammation)
- Relapse common after withdrawal (50-90%)
Drug-Induced Liver Injury:
- Primary Intervention: Discontinuation of the offending agent
- N-acetylcysteine: Effective for acetaminophen toxicity, may help in other cases
- Ursodeoxycholic acid: Sometimes used for cholestatic injury
- Corticosteroids: Considered for immune-mediated drug reactions with severe presentation
- Liver transplantation: For fulminant cases with poor prognosis
Management of Complications
Portal Hypertension and Varices:
- Primary Prophylaxis:
- Non-selective beta-blockers (NSBB): Propranolol, nadolol, carvedilol
- Endoscopic band ligation for high-risk varices
- Acute Variceal Bleeding:
- Hemodynamic stabilization
- Vasoactive drugs (octreotide, terlipressin)
- Endoscopic band ligation or sclerotherapy
- Transjugular intrahepatic portosystemic shunt (TIPS) for refractory bleeding
- Balloon tamponade as temporary rescue measure
- Secondary Prophylaxis:
- Combination of NSBB and endoscopic band ligation
- TIPS for recurrent bleeding despite medical therapy
Ascites:
- First-line Treatment:
- Sodium restriction (<2g/day)
- Diuretics: Spironolactone ± furosemide
- Refractory Ascites:
- Large volume paracentesis with albumin
- TIPS
- Peritoneovenous shunts (rarely used)
- Evaluation for liver transplantation
- Spontaneous Bacterial Peritonitis:
- Empiric antibiotics (third-generation cephalosporins)
- Albumin infusion to prevent hepatorenal syndrome
- Secondary prophylaxis with daily antibiotics
Hepatic Encephalopathy:
- Acute Management:
- Identification and treatment of precipitating factors
- Lactulose: Oral or rectal administration
- Rifaximin: Add-on for severe or recurrent cases
- Prevention of Recurrence:
- Lactulose titrated to 2-3 soft bowel movements daily
- Rifaximin for recurrent episodes despite lactulose
- Avoidance of precipitating medications
- Protein intake moderation rather than restriction
Hepatorenal Syndrome:
- Volume Expansion: Albumin infusion
- Vasoconstrictors:
- Terlipressin plus albumin
- Norepinephrine plus albumin
- Midodrine/octreotide plus albumin
- Renal Replacement Therapy: Bridge to transplant
- Definitive Treatment: Liver transplantation
Liver Transplantation
Indications:
- Decompensated cirrhosis
- Acute liver failure
- Early-stage hepatocellular carcinoma
- Metabolic liver diseases
- Specific indications:
- MELD score >15 (variable by region)
- Refractory complications (HE, ascites)
- Hepatopulmonary syndrome
- Poor quality of life
Contraindications:
- Absolute:
- Active alcohol or substance use (typically requires 6 months abstinence)
- Advanced HCC beyond transplant criteria
- Severe cardiopulmonary disease
- Active uncontrolled infection
- Advanced age with poor functional status
- Relative:
- Advanced age
- Psychosocial issues
- Medical comorbidities
- HIV with poorly controlled disease
- Previous abdominal surgery
Outcomes:
- Survival Rates:
- 1-year survival: 85-90%
- 5-year survival: 70-75%
- 10-year survival: 60-65%
- Etiology-Specific Considerations:
- HBV: Excellent outcomes with prophylaxis
- HCV: Previously problematic, now excellent with DAA therapy
- Alcohol-related: Good if abstinence maintained
- NASH: Increasing indication, outcomes comparable to other etiologies
Post-Transplant Management:
- Immunosuppression regimens
- Rejection monitoring and management
- Infection prophylaxis
- Metabolic complication management
- Disease recurrence prevention
Emerging Treatments and Clinical Trials
Novel Approaches for Hepatitis B:
- Nucleic Acid Polymers: Inhibit HBsAg release
- RNA Interference: Silence viral transcript expression
- Core Protein Allosteric Modulators: Interfere with capsid assembly
- Therapeutic Vaccines: Stimulate immune clearance
- CRISPR/Cas9: Gene editing approaches
- Combination Approaches: Functional cure strategies
Emerging NASH Therapies:
- FXR Agonists: Beyond obeticholic acid (cilofexor, tropifexor)
- PPAR Agonists: Lanifibranor, saroglitazar
- FGF21 Analogues: Pegbelfermin, efruxifermin
- THR-β Agonists: Resmetirom
- Acetyl-CoA Carboxylase Inhibitors: Firsocostat
- GLP-1/GIP/Glucagon Receptor Agonists: Tirzepatide, cotadutide
Advanced Approaches for Autoimmune Hepatitis:
- Selective JAK Inhibitors
- Anti-B Cell Therapies: Rituximab, belimumab
- Anti-Cytokine Approaches: IL-6 blockade
- More Selective Immunosuppression
- Regulatory T-Cell Therapies
Hepatocellular Carcinoma Innovation:
- Immunotherapy Combinations:
- Atezolizumab plus bevacizumab
- Multiple checkpoint inhibitor combinations
- Targeted therapy plus immunotherapy
- Novel Systemic Approaches:
- ADC (antibody-drug conjugates)
- CAR-T cell therapy
- Bispecific antibodies
- Metabolic targeting approaches
Cirrhosis and Portal Hypertension:
- Anti-fibrotic Agents:
- Targeting myofibroblast activation
- Matrix metalloproteinase modulators
- Targeting inflammatory drivers
- Gut Microbiome Modulation:
- Fecal microbiota transplantation
- Probiotics and prebiotics
- Engineered bacteria
- Cell-Based Therapies:
- Mesenchymal stem cells
- Hepatocyte transplantation
- Engineered cell products
The therapeutic landscape for hepatitis and related liver diseases has evolved dramatically in recent decades, with notable advances in viral hepatitis treatment, management of complications, and liver transplantation techniques. Ongoing research promises further improvements in outcomes through novel agents targeting specific disease mechanisms, combination approaches, and enhanced personalized medicine strategies.
9. Prevention & Precautionary Measures
Primary Prevention of Viral Hepatitis
Hepatitis A Prevention:
Vaccination:
- Highly effective (>95%) inactivated vaccines
- Two-dose series for long-term protection
- Recommended populations:
- All children at age 1 year
- Travelers to endemic regions
- Men who have sex with men
- People who use drugs
- People with chronic liver disease
- Occupational risk groups
- Combined HAV/HBV vaccine available
Environmental Measures:
- Improved sanitation and clean water
- Proper sewage disposal systems
- Food safety practices (particularly for shellfish)
- Handwashing and hygiene education
Hepatitis B Prevention:
- Vaccination:
- Universal infant vaccination (global WHO recommendation)
- Catch-up vaccination for children and high-risk adults
- Three-dose series standard (alternative two-dose available)
- Efficacy >95% in producing protective antibody levels
- Post-vaccination testing for high-risk groups
- Perinatal Transmission Prevention:
- Universal screening of pregnant women
- Hepatitis B immune globulin (HBIG) plus vaccination for exposed newborns
- Antiviral therapy for pregnant women with high viral loads
- Efficacy >95% in preventing vertical transmission
- Blood Supply Safety:
- Universal screening of blood donations
- Nucleic acid testing implementation
- Donor selection criteria
- Injection Safety:
- Single-use syringes and needles
- Healthcare worker training
- Safe disposal systems
- Post-Exposure Prophylaxis:
- HBIG plus vaccination after significant exposures
- Efficacy decreases with time after exposure
Hepatitis C Prevention:
- No Vaccine Available
- Harm Reduction Strategies:
- Needle and syringe exchange programs
- Opioid substitution therapy
- Safe injection education
- Healthcare-Associated Prevention:
- Standard precautions implementation
- Injection safety
- Improved sterilization of instruments
- Regular testing of high-risk populations
- Blood and Organ Safety:
- Universal screening of donations
- NAT testing implementation
- Donor selection criteria
- Treatment as Prevention:
- Treating infected individuals reduces transmission
- High-risk group targeting strategies
- Micro-elimination approaches
Hepatitis D Prevention:
- Hepatitis B Vaccination: Prevents HDV as it requires HBV to replicate
- HBV Treatment: Reducing HBV levels may reduce HDV replication
Hepatitis E Prevention:
- Improved Water Safety in endemic regions
- Proper Cooking of Pork and game meat
- Vaccination: Available in China, not widely available globally
- Pregnancy Precautions: Avoidance of high-risk exposures
Prevention of Non-Viral Hepatitis
Alcoholic Liver Disease Prevention:
- Public Health Approaches:
- Alcohol taxation policies
- Minimum pricing strategies
- Advertising restrictions
- Access limitation strategies
- Educational campaigns
- Screening and Brief Interventions:
- AUDIT and other screening tools
- Physician-delivered brief advice
- Motivational interviewing
- Early referral to treatment
- Risk Reduction for Established Drinkers:
- Controlled drinking programs
- Harm reduction approaches
- Support groups
- Addressing concurrent mental health issues
NAFLD/NASH Prevention:
- Dietary Recommendations:
- Mediterranean diet pattern
- Reduced fructose consumption
- Decreased saturated fat
- Increased fiber intake
- Coffee consumption (associated with reduced risk)
- Physical Activity Guidelines:
- 150+ minutes moderate exercise weekly
- Resistance training 2-3 times weekly
- Reduced sedentary time
- Even modest activity shows benefit
- Weight Management:
- Gradual weight loss (1-2 lbs/week)
- Sustainable approaches
- 7-10% weight loss can improve NASH
- Maintenance strategies
- Metabolic Risk Factor Control:
- Diabetes management
- Dyslipidemia treatment
- Hypertension control
- Metabolic syndrome prevention
Drug-Induced Liver Injury Prevention:
- Medication Stewardship:
- Appropriate prescribing
- Necessary indications
- Lowest effective doses
- Shortest necessary duration
- Monitoring Protocols:
- Baseline liver function testing
- Regular monitoring with high-risk drugs
- Early detection of abnormalities
- Prompt discontinuation when indicated
- Patient Education:
- Acetaminophen dosing and combination awareness
- Alcohol avoidance with hepatotoxic medications
- Symptom recognition education
- Herbal/supplement caution
Autoimmune Hepatitis Prevention:
- No specific preventive measures identified
- Genetic predisposition not modifiable
- Environmental triggers poorly understood
- Early diagnosis important to prevent progression
Preventive Screening and Vaccination
Screening Recommendations:
- Hepatitis B:
- Universal prenatal screening
- One-time testing for high-risk groups
- Periodic testing for ongoing risk
- Testing before immunosuppressive therapy
- Hepatitis C:
- One-time testing for all adults (US and many countries)
- Regular testing for ongoing risk behaviors
- Screening of pregnant women
- Testing before certain medical procedures
- Liver Cancer Screening:
- Cirrhotic patients: Ultrasound ± AFP every 6 months
- Non-cirrhotic HBV carriers with risk factors
- Cost-effective in high-risk populations
Vaccination Programs:
- Hepatitis A:
- Childhood universal vaccination in many countries
- Targeted risk-group vaccination
- Outbreak response vaccination
- Hepatitis B:
- Universal infant vaccination in 189 countries
- Birth dose implementation (increasing)
- Catch-up programs for adolescents
- Adult risk-based vaccination
- Combined Vaccines:
- HAV/HBV combination (Twinrix)
- Incorporation into routine childhood schedules
- Traveler vaccination programs
Vaccine Development Challenges:
- Hepatitis C:
- High genetic diversity
- Complex envelope proteins
- Immune evasion mechanisms
- Several candidates in early development
- Hepatitis E:
- Single vaccine licensed in China only
- Limited global development effort
- Effective but access limited
Environmental and Behavioral Precautions
Water and Food Safety:
- Safe Water Practices:
- Water treatment systems
- Boiling when safety uncertain
- Bottled water in high-risk areas
- Avoiding ice in endemic regions
- Food Safety:
- Thorough cooking of shellfish
- Adequate cooking of pork and game meat
- Proper handling of raw foods
- Avoiding street food in high-risk areas
Personal Protective Measures:
- Barrier Methods:
- Condom use for sexual transmission prevention
- Gloves for healthcare and certain occupations
- Personal protective equipment in high-risk settings
- Injection Safety:
- Never sharing needles or injection equipment
- Proper disposal of sharps
- Accessing harm reduction services when needed
- Body Fluid Precautions:
- Avoiding sharing personal items (razors, toothbrushes)
- Covering cuts and wounds
- Cleaning blood spills with appropriate disinfectants
Occupational Precautions:
- Healthcare Settings:
- Standard precautions implementation
- Needle safety devices
- Post-exposure protocols
- Vaccination requirements
- First Responders:
- Appropriate protective equipment
- Training on exposure risks
- Post-exposure protocols
- Vaccination requirements
- Laboratory Workers:
- Biosafety protocols
- Proper specimen handling
- Vaccination requirements
- Exposure response plans
- Other High-Risk Occupations:
- Sewage workers: Hepatitis A vaccination
- Tattoo/piercing professionals: Infection control training
- Morticians/funeral workers: Standard precautions
Global Health Strategies
WHO Elimination Goals:
- Viral Hepatitis Elimination by 2030:
- 90% reduction in new infections
- 65% reduction in mortality
- 90% diagnosis rate for HBV and HCV
- 80% treatment rate for eligible HBV and HCV patients
- Strategic Directions:
- Information for focused action
- Interventions for impact
- Delivering for equity
- Financing for sustainability
- Innovation for acceleration
Country-Level Implementation:
- National Hepatitis Plans:
- Developed in 84 countries as of 2022
- Integration with other health programs
- Context-specific approaches
- Resource allocation prioritization
- Micro-Elimination Approaches:
- Focusing on specific populations
- Geographic targeting
- Institutional settings
- Demonstrating feasibility
- Public-Private Partnerships:
- Vaccine access initiatives
- Treatment access programs
- Diagnostic capacity building
- Innovative financing mechanisms
Prevention of hepatitis requires a multifaceted approach encompassing vaccination, screening, behavioral interventions, and environmental measures. While significant progress has been made, particularly for viral hepatitis, substantial challenges remain in achieving global elimination goals. Integration of hepatitis prevention into broader health systems strengthening efforts offers the most sustainable path forward, with continued innovation in vaccines, diagnostics, and delivery approaches providing hope for further progress.
10. Global & Regional Statistics
Global Burden and Prevalence
Viral Hepatitis Burden:
- Total Impact:
- 354 million people living with chronic hepatitis B or C
- 1.1 million deaths annually from viral hepatitis
- 10 million new infections yearly
- 58% of liver cancer cases attributable to HBV or HCV
- Over 90% of affected people unaware of their infection
- Hepatitis B:
- 296 million people living with chronic infection
- 820,000 deaths annually
- 1.5 million new infections yearly
- 2.5-3.5% global prevalence (variable by region)
- Hepatitis C:
- 58 million people with chronic infection
- 290,000 deaths annually
- 1.5 million new infections yearly
- 0.8-1.1% global prevalence
- Hepatitis A:
- 1.4 million cases annually
- 7,000 deaths annually
- Highly variable regional endemicity
- Hepatitis E:
- 20 million infections annually
- 44,000 deaths annually
- 3.3 million symptomatic cases
Non-Viral Hepatitis Burden:
- Alcoholic Liver Disease:
- 1-2 million deaths attributable annually
2% global prevalence of alcohol use disorders
- Highly variable by country (correlates with alcohol consumption)
- NAFLD/NASH:
- 1.9 billion affected globally (25% of population)
- 20% of NAFLD cases progress to NASH
- 200-300 million with NASH worldwide
- Rapidly increasing prevalence with obesity epidemic
- Drug-Induced Liver Injury:
- Leading cause of acute liver failure in developed countries
- Accounts for 10% of all adverse drug reactions
- True global burden difficult to estimate due to underreporting
Overall Liver Disease Impact:
- Global Mortality:
- 2 million liver-related deaths annually
- 8th leading cause of death worldwide
- Increasing relative to other major causes
- Disability-Adjusted Life Years (DALYs):
- 52 million DALYs lost annually to liver diseases
- Disproportionate impact on working-age adults
- Significant economic impact through lost productivity
Regional Variations and Patterns
Hepatitis B Distribution:
- High Prevalence Regions (>8%):
- Western Pacific Region (China, Pacific Islands)
- African Region (Sub-Saharan Africa)
- Parts of Eastern Mediterranean Region
- Intermediate Prevalence (2-7%):
- Eastern Europe
- Central Asia
- Southeast Asia
- Amazon Basin
- Low Prevalence (<2%):
- North America
- Western Europe
- Australia/New Zealand
- Southern South America
Hepatitis C Distribution:
- High Prevalence Countries (>3%):
- Egypt (10-15%)
- Pakistan (4.8%)
- Mongolia (6.4%)
- Parts of Central Africa
- Central Asia
- Moderate Prevalence (1.5-3%):
- Eastern Mediterranean countries
- Eastern Europe
- Parts of Africa
- Low Prevalence (<1.5%):
- Western Europe
- North America
- Australia
- Most of Asia-Pacific
Hepatitis A Endemicity:
- High Endemicity: Sub-Saharan Africa, parts of South Asia
- Intermediate Endemicity: Eastern Europe, Middle East, parts of Latin America
- Low Endemicity: North America, Western Europe, Australia, Japan
- Very Low Endemicity: Scandinavia
Hepatitis E Distribution:
- Epidemic Pattern: Central and Southeast Asia, Middle East, North Africa
- Sporadic Pattern: Europe, Americas (primarily genotype 3)
- Zoonotic Transmission: Higher in regions with raw/undercooked pork consumption
NAFLD Regional Patterns:
- Highest Prevalence: Middle East (32%), South America (30%)
- High Prevalence: Asia (27%), North America (24%), Europe (23%)
- Lower Prevalence: Africa (13.5%)
- Urban vs. Rural: Higher rates in urban settings globally
Alcoholic Liver Disease Patterns:
- High Burden: Eastern Europe, Russia
- Increasing Burden: East Asia, India
- Moderate Burden: Western Europe, North America
- Low Burden: Middle East, North Africa (religious restrictions)
Mortality and Survival Rates
Overall Liver Disease Mortality:
- Global Distribution:
- High-income countries: 2-3% of all deaths
- Middle-income countries: 3-5% of all deaths
- Low-income countries: 3-4% of all deaths
- Trend Analysis:
- Increasing in most regions
- Decreasing for HBV in high-vaccination regions
- Decreasing for HCV in regions with DAA access
- Rapidly increasing for NAFLD/NASH globally
Viral Hepatitis Mortality:
- Hepatitis B:
- Case fatality rate: 0.5-1% annually in cirrhotic patients
- HCC development rate: 2-8% annually in cirrhosis
- Geographic variation: Higher mortality in resource-limited settings
- Hepatitis C:
- Pre-DAA era: 350,000-500,000 deaths annually
- Post-DAA potential: Significant mortality reduction
- Current challenge: Diagnosis and treatment access gaps
- Acute Viral Hepatitis:
- HAV: <0.5% mortality overall, higher in elderly
- HEV: 0.5-4% generally, 20-25% in pregnancy
Liver Cirrhosis Mortality:
- Global Distribution:
- Highest: Eastern Europe, Central Asia
- High: Parts of Latin America, Sub-Saharan Africa
- Moderate: East Asia, North America
- Lower: Western Europe, Australia
Hepatocellular Carcinoma:
- Incidence-to-Mortality Ratio: Nearly 1:1 indicating poor survival
- 5-Year Survival: 18% overall (varies by region and stage)
- Geographic Variation:
- Highest mortality: East Asia, Africa
- Intermediate: Southern Europe
- Lower: Northern Europe, North America
Survival Data by Etiology:
- Viral Hepatitis:
- Untreated chronic HBV: 15-40% lifetime risk of cirrhosis
- Untreated chronic HCV: 15-30% develop cirrhosis in 20 years
- Treated HBV: Significantly reduced progression
- Treated HCV: >95% cure with modern DAAs
- Alcoholic Liver Disease:
- Severe alcoholic hepatitis: 50-65% short-term survival
- Alcoholic cirrhosis with abstinence: 60-70% 5-year survival
- Continued drinking: <50% 5-year survival
- NAFLD/NASH:
- Simple steatosis: Similar to general population
- NASH with fibrosis: Increased mortality
- NASH cirrhosis: Similar to other cirrhosis etiologies
Country-Specific Data and Trends
Notable Country-Specific Situations:
China:
- 86 million HBV infections (28% of global burden)
- Universal infant vaccination since 1992
- Declining HBV prevalence in younger cohorts
- Rising NAFLD prevalence (29%) with economic development
- 50% of global liver cancer deaths
India:
- 40 million HBV infections
- 6-12 million HCV infections
- Variable HBV vaccination implementation
- Rising alcoholic liver disease
- Increasing NAFLD with urbanization
- Limited treatment access for most of population
Egypt:
- Historically highest HCV prevalence globally (10-15%)
- Result of mass parenteral antischistosomal therapy (1950s-1980s)
- Ambitious national elimination program
- Treated over 4 million HCV patients since 2014
- Reduced prevalence to approximately 4.6%
United States:
- 2.4 million HCV infections
- 862,000 HBV infections
- Rising alcoholic liver disease mortality
- NAFLD affecting 24-30% of population
- Increasing liver disease in younger adults
- Disparities in disease burden and treatment access
Russia and Eastern Europe:
- High alcoholic liver disease burden
- High HCV prevalence in some countries (2-3%)
- Limited treatment access in many areas
- Highest liver disease mortality in European region
Sub-Saharan Africa:
- High HBV endemicity (5-10%)
- Growing HCV burden
- Limited diagnostic and treatment infrastructure
- Youngest affected population globally
- Increasing implementation of birth-dose HBV vaccination
Global Trends Analysis:
- Declining Trends:
- HBV in regions with established vaccination programs
- HAV with improved sanitation and vaccination
- HCV in countries with broad DAA access
- Increasing Trends:
- NAFLD/NASH globally
- Alcoholic liver disease in many regions
- Liver disease in younger adults
- Disease burden in resource-limited settings
- Emerging Concerns:
- Impact of COVID-19 on liver disease care
- Climate change effects on water-borne hepatitis
- Migration impacts on disease patterns
- Treatment access inequalities
The global burden of hepatitis and liver disease shows substantial geographic variation, reflecting differences in risk factors, prevention efforts, healthcare access, and socioeconomic conditions. While progress has been made in some areas, particularly viral hepatitis, the overall burden continues to increase due to population growth, aging, metabolic syndrome, and alcohol use. Addressing these challenges requires targeted strategies that account for regional variations while working toward global elimination goals.
11. Recent Research & Future Prospects
Recent Advances in Hepatitis Treatment
Viral Hepatitis Breakthroughs:
- Hepatitis B Functional Cure Research:
- Novel combination approaches targeting multiple viral lifecycle steps
- RNA interference therapies (e.g., bepirovirsen) showing promising results
- Core protein allosteric modulators (CpAMs) in Phase 2/3 trials
- Therapeutic vaccines stimulating immune clearance
- TLR agonists boosting innate immune responses
- Hepatitis C Treatment Refinements:
- Pan-genotypic regimens simplifying treatment approaches
- Shortened treatment duration protocols (8 weeks standard, 6 weeks in some cases)
- Special population optimization (renal disease, decompensated cirrhosis)
- Simplified monitoring approaches
- Point-of-care diagnostics facilitating test-and-treat models
- Hepatitis D Advances:
- Bulevirtide (Hepcludex) approval—first specific HDV therapy
- Lonafarnib (prenylation inhibitor) development
- Combination strategies showing enhanced efficacy
- Hepatitis E Management:
- Improved diagnostic capabilities
- Better characterization of chronic infection
- Optimized ribavirin protocols
Non-Viral Hepatitis Innovation:
- NAFLD/NASH Pipeline:
- FXR agonists (obeticholic acid, cilofexor, tropifexor) modulating bile acid signaling
- THR-β agonists (resmetirom) enhancing hepatic fat metabolism
- PPAR agonists (lanifibranor, elafibranor) with anti-inflammatory and metabolic effects
- FGF21 analogues (pegbelfermin, efruxifermin) improving insulin sensitivity and lipid metabolism
- Combination approaches addressing multiple pathways simultaneously
- GLP-1 receptor agonists (semaglutide) showing significant benefit beyond weight loss
- Alcoholic Hepatitis Innovations:
- G-CSF (granulocyte colony-stimulating factor) promoting liver regeneration
- IL-22 based therapies restoring hepatocyte function
- Gut microbiome modulation through fecal microbiota transplantation
- Anti-inflammatory approaches targeting specific cytokines
- Combination therapies with traditional treatments
- Extracorporeal liver support systems bridging to recovery
- Autoimmune Hepatitis Approaches:
- More selective immunosuppressive agents minimizing side effects
- Biologics targeting specific immune pathways (anti-TNF, anti-IL-6)
- B-cell depletion strategies (rituximab) for refractory cases
- Biomarker-guided personalized therapy
- Novel corticosteroid formulations with improved safety profiles
- Regulatory T-cell modulation approaches
Advanced Liver Disease Management:
- Anti-fibrotic Therapies:
- Inhibitors of fibrosis-promoting pathways (galectin-3, LOXL2)
- Antioxidant strategies (cenicriviroc, selonsertib)
- Matrix modulation approaches
- Cell-based antifibrotic therapies
- Portal Hypertension Innovations:
- Novel beta-blockers with improved efficacy
- Statins as adjunctive therapy for portal hypertension
- Vascular targeting approaches
- TIPS refinements with covered stents and controlled deployment
- Hepatic Encephalopathy Advances:
- Gut microbiome modulation beyond rifaximin
- Ammonia scavenging strategies (glycerol phenylbutyrate)
- Novel mechanisms targeting neuroinflammation
- Biomarkers for early detection and intervention
Cutting-Edge Research Initiatives
Innovative Diagnostic Approaches:
- Liquid Biopsy Development:
- Circulating cell-free DNA for fibrosis assessment
- Extracellular vesicles as disease biomarkers
- miRNA signatures for disease classification
- Proteomic profiles for disease activity monitoring
- Advanced Imaging Technologies:
- MR elastography refinements for fibrosis staging
- Contrast-enhanced ultrasound for lesion characterization
- Photoacoustic imaging for metabolic assessment
- AI integration for enhanced diagnostic accuracy
- Point-of-Care Diagnostics:
- Portable viral load quantification
- Rapid fibrosis assessment tools
- Smartphone-based diagnostic platforms
- Low-cost screening approaches for resource-limited settings
Regenerative Medicine Applications:
- Cell-Based Therapies:
- Mesenchymal stem cell treatments for various liver diseases
- Hepatocyte transplantation techniques
- Induced pluripotent stem cell (iPSC) derived hepatocytes
- Bioengineered liver tissue constructs
- Gene Editing Approaches:
- CRISPR/Cas9 for genetic liver disease correction
- Base editing for point mutation correction
- Prime editing offering precise genetic modifications
- In vivo gene therapy delivery systems
- Bioengineered Liver Technologies:
- 3D bioprinting of liver tissue
- Liver-on-a-chip for drug testing
- Decellularized liver scaffolds for regeneration
- Artificial liver support devices with biological components
Immunological Research Frontiers:
- Precision Immunotherapy:
- Tumor-specific neoantigen vaccines for HCC
- CAR-T cell approaches for liver tumors
- Bispecific antibodies for enhanced targeting
- Immune checkpoint inhibitor combinations
- Immune Regulation in Autoimmunity:
- Regulatory T-cell based therapies
- Tolerance induction strategies
- Antigen-specific immunotherapy
- Microbiome modulation for immune regulation
- Innate Immunity Targeting:
- STING pathway modulation for viral hepatitis
- NK cell-based therapies
- Macrophage reprogramming approaches
- Inflammasome targeting strategies
Key Global Research Networks and Initiatives
Collaborative Research Platforms:
- Hepatitis B Cure Initiative:
- International Coalition to Eliminate HBV (ICE-HBV)
- HBV Cure Forum bringing together academia and industry
- Chan Zuckerberg Biohub HBV programs
- NIH-funded HBV research networks
- NASH Research Networks:
- LITMUS (Liver Investigation: Testing Marker Utility in Steatohepatitis) in Europe
- NIMBLE Consortium in the US
- NAFLD Clinical Research Network
- Industry-led NASH consortia developing biomarkers and endpoints
- Hepatitis Elimination Programs:
- WHO Global Hepatitis Programme
- Coalition for Global Hepatitis Elimination
- Clinton Health Access Initiative HCV programs
- Regional elimination research networks
Data Science and AI Integration:
- Big Data Approaches:
- Large-scale electronic health record analysis
- Integration of genomics, transcriptomics, and clinical data
- Population-level intervention modeling
- Real-world evidence generation
- Artificial Intelligence Applications:
- AI-assisted image interpretation
- Machine learning for outcome prediction
- Natural language processing of clinical notes
- Deep learning for treatment response prediction
- Digital Health Innovations:
- Telehealth optimization for liver disease
- Mobile health applications for treatment adherence
- Remote monitoring platforms
- Virtual care models for hepatitis management
Future Therapeutic Directions
Next-Generation Treatment Paradigms:
- Hepatitis B Curative Strategies:
- Multi-modal approaches targeting cccDNA, viral antigens, and host immunity
- Single-administration curative regimens
- Personalized combination treatments based on viral and host factors
- Preventive and therapeutic vaccination
- Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD/MASH):
- Replacement terminology for NAFLD/NASH reflecting pathophysiology
- Multi-targeted combination therapies
- Precision medicine approaches based on disease subtypes
- Early intervention strategies preventing progression
- Advanced Cirrhosis Management:
- Regression of fibrosis as treatment goal
- Integrated care models combining pharmacological and non-pharmacological approaches
- Bioartificial liver devices for acute decompensation
- Bridging technologies to transplantation or regeneration
Implementation and Access Innovations:
- Generic Manufacturing and Access Programs:
- Voluntary licensing expansions
- Patent pooling for newer treatments
- Technology transfer to increase production capacity
- Tiered pricing strategies for global access
- Simplified Treatment Models:
- Decentralized care delivery
- Task-shifting to non-specialist providers
- Integration with primary care
- Differentiated service delivery models
- Global Health Financing Mechanisms:
- Innovative financing instruments
- Results-based funding approaches
- Microfinance and revolving fund models
- Public-private partnerships for access
Long-term Visions:
- Global Elimination of Viral Hepatitis:
- Comprehensive prevention programs
- Universal screening approaches
- Pan-genotypic, single-dose cures
- Integration with broader health systems
- Artificial Liver Technologies:
- Fully functional bioengineered liver constructs
- Implantable artificial liver devices
- 3D-printed personalized liver scaffolds
- Cell-free liver support systems
- Predictive and Preventive Approaches:
- Risk stratification based on genetic and environmental factors
- Precision prevention strategies
- Early interventions before clinical disease
- Pre-emptive immunomodulation
The research landscape for hepatitis and liver diseases is experiencing unprecedented innovation, with advances spanning molecular biology, immunology, regenerative medicine, and data science. These developments promise to transform the management of hepatitis from a model of chronic disease control to one of cure and prevention. While significant challenges remain, particularly in global implementation and access, the scientific foundations for dramatically improved outcomes are rapidly developing across the spectrum of hepatitis etiologies.
12. Interesting Facts & Lesser-Known Insights
Historical and Scientific Curiosities
Evolution of Hepatitis Knowledge:
- The term “hepatitis” was first used by Hippocrates around 400 BCE, describing “epidemic jaundice” likely representing hepatitis A outbreaks.
- The earliest documented hepatitis outbreak was recorded in Babylon over 2500 years ago, with yellowing of the skin described in the Talmud.
- During the 18th and 19th centuries, “campaign jaundice” was recognized during military conflicts, with major outbreaks during the American Civil War and both World Wars.
- The distinction between “infectious hepatitis” (hepatitis A) and “serum hepatitis” (hepatitis B) was first proposed during World War II based on epidemiological patterns.
- The hepatitis B virus surface antigen was initially called the “Australia antigen” because it was first identified in an Australian Aboriginal person’s blood sample.
Scientific Surprises:
- The hepatitis D virus is unique among human pathogens as a “defective” virus that requires hepatitis B virus to complete its life cycle.
- The hepatitis B virus genome is unusually compact, with overlapping genes that encode multiple proteins from the same DNA sequence.
- Despite causing liver inflammation, many hepatitis viruses are not directly cytopathic—much of the liver damage comes from the immune response rather than from the virus directly killing hepatocytes.
- The hepatitis C virus has one of the highest mutation rates of any known virus, allowing it to rapidly develop resistance to immune responses and medications.
- Hepatitis E was once thought to be exclusively a disease of the developing world, but is now recognized as endemic in many developed countries through zoonotic transmission from pigs and other animals.
Nobel Prize Connections:
- Three separate Nobel Prizes have been awarded for hepatitis research:
- 1976: Baruch Blumberg for discovering the hepatitis B virus
- 1976: Carleton Gajdusek for work on slow virus infections (sharing the prize with Blumberg)
- 2020: Harvey Alter, Michael Houghton, and Charles Rice for discovering the hepatitis C virus
- The 44-year gap between Nobel Prizes for hepatitis B and C represents one of the longest periods between awards for related discoveries in the same field.
Unusual Hepatitis Phenomena:
- The phenomenon of “hepatitis of happiness” describes transient liver enzyme elevations following extremely positive life events, possibly related to altered metabolism and stress hormones.
- Some patients with autoimmune hepatitis experience dramatic clinical and biochemical improvement during pregnancy, only to flare after delivery.
- Multiple hepatitis viruses show seasonal variation in transmission patterns, with hepatitis A and E showing higher rates in summer and fall in many regions.
- The liver is one of the few organs capable of significant regeneration—it can recover from loss of up to 75% of its mass, which explains why many hepatitis patients can recover full function despite extensive damage.
Myths and Misconceptions vs. Medical Facts
Common Myths about Hepatitis Transmission:
Myth 1: “Hepatitis can be caught from casual contact like handshakes or hugs.”
- Fact: None of the hepatitis viruses spread through casual contact. Different viruses have specific transmission routes:
- Hepatitis A and E: Fecal-oral route
- Hepatitis B, C, and D: Blood, body fluids, sexual contact (with varying efficiency)
- Casual household contact carries minimal to no risk for HBV and no risk for HCV
Myth 2: “All forms of hepatitis are highly contagious and dangerous.”
- Fact: The different hepatitis viruses have vastly different infectivity and outcomes:
- Hepatitis A: Highly contagious but rarely causes chronic disease
- Hepatitis B: Moderately contagious with age-dependent chronic infection risk
- Hepatitis C: Less contagious than HBV but higher rate of chronic progression
- Alcoholic and NAFLD/NASH: Not contagious at all
Myth 3: “Hepatitis is always accompanied by jaundice (yellowing of skin/eyes).”
- Fact: Many cases of hepatitis, especially chronic forms, never develop visible jaundice:
- 70-80% of acute hepatitis C infections are anicteric (without jaundice)
- Most chronic hepatitis B and C patients do not have jaundice until advanced stages
- NAFLD/NASH typically progresses without jaundice until cirrhosis develops
Myths about Hepatitis Treatment and Outcomes:
Myth 4: “Hepatitis C cannot be cured.”
- Fact: Modern direct-acting antivirals cure over 95% of hepatitis C infections with 8-12 weeks of well-tolerated oral therapy. This represents one of the most remarkable medical advances of recent decades.
Myth 5: “If you’ve had one type of hepatitis, you’re immune to all types.”
- Fact: Each hepatitis virus is distinct, and infection or vaccination against one type provides no cross-protection against the others. It’s possible to be infected with multiple hepatitis viruses simultaneously.
Myth 6: “Liver damage from hepatitis is always permanent.”
- Fact: The liver has remarkable regenerative capacity. With proper treatment:
- Acute viral hepatitis often resolves completely without residual damage
- Alcoholic hepatitis can show significant improvement with abstinence
- Early stages of fibrosis can reverse with effective treatment
- Even cirrhosis can show some regression in certain circumstances
Myth 7: “Natural remedies and liver cleanses can cure hepatitis.”
- Fact: No “liver cleanse” or herb has been scientifically proven to cure viral hepatitis. Some supplements marketed for liver health can actually cause liver injury. Evidence-based treatments include:
- Antiviral medications for viral hepatitis
- Lifestyle modifications for NAFLD/NASH
- Abstinence and potentially corticosteroids for alcoholic hepatitis
- Immunosuppression for autoimmune hepatitis
Impact on Specific Populations and Professions
Vulnerable and Special Populations:
Indigenous Communities:
- Native American, First Nations, Aboriginal, and other indigenous populations often have 2-3 times higher rates of chronic viral hepatitis compared to non-indigenous populations.
- Historical factors including lack of access to healthcare, higher rates of injection drug use, and inadequate screening contribute to this disparity.
- Cultural approaches to healing can be effectively integrated with modern hepatitis treatments to improve outcomes.
- Some populations show genetic factors affecting disease progression and treatment response.
Migrant and Refugee Communities:
- Immigrants from high-endemic regions may have hepatitis B prevalence of 5-15% versus <1% in the general population of receiving countries.
- Linguistic and cultural barriers often delay diagnosis and treatment.
- Stigma may be particularly pronounced in certain cultural contexts.
- Screening programs specifically targeting migrant populations have demonstrated high cost-effectiveness.
People Who Use Drugs:
- Injection drug use remains the primary risk factor for HCV transmission in many developed countries.
- Successful models combining harm reduction, addiction treatment, and hepatitis services show dramatic improvements in outcomes.
- Stigma and discrimination remain significant barriers to care.
- Novel point-of-care testing and treatment delivery models adapted to this population have shown promise.
Incarcerated Populations:
- Prisons and jails have hepatitis C prevalence 10-20 times higher than the general population.
- Represent unique opportunity for diagnosis and treatment of a hard-to-reach population.
- Successful prison-based treatment programs demonstrate public health and economic benefits.
- Legal challenges regarding access to treatment have established precedents in many jurisdictions.
Occupational Considerations:
Healthcare Workers:
- Historical risk: Before universal precautions, healthcare workers had 3-5 times higher HBV risk
- Modern safety: Universal vaccination and safety devices have dramatically reduced risk
- Post-exposure protocols: Established guidelines for potential exposures
- Return-to-work considerations: Special guidelines for infected healthcare workers performing exposure-prone procedures
Body Art Professionals:
- Tattoo and piercing artists have elevated hepatitis risk without proper precautions
- Industry regulation varies widely globally
- Education and certification programs have successfully reduced risk
- Client education remains an important prevention strategy
Unique Populations:
Competitive Athletes:
- Contact sports athletes historically faced stigma regarding HBV/HCV
- Modern guidelines allow participation with proper precautions
- Drug testing concerns intersect with treatment considerations
- Performance impacts of chronic liver disease require specialized management
Performers and Artists:
- Entertainment industry has seen high-profile hepatitis cases
- Touring performers face challenges with treatment continuity
- Substance use issues in some entertainment sectors increase risk
- Advocacy by celebrities has reduced stigma and increased awareness
Fascinating Clinical and Epidemiological Insights
Rare Clinical Phenomena:
- Fibrosing Cholestatic Hepatitis: An accelerated and often fatal form of viral hepatitis seen in immunosuppressed patients, particularly following organ transplantation.
- Post-transfusion Hepatitis: Once affected up to 30% of patients receiving multiple transfusions before modern screening, driving major advances in blood safety.
- Reactivation Hepatitis: Dormant HBV can reactivate decades after initial infection when the immune system is suppressed, causing potentially fatal acute liver injury.
- Vanishing Bile Duct Syndrome: A rare complication of drug-induced liver injury that leads to progressive loss of bile ducts and can necessitate liver transplantation.
Unique Epidemiological Events:
- The largest recorded hepatitis outbreak occurred in Shanghai in 1988, when almost 300,000 people developed hepatitis A from eating contaminated clams.
- A 2016-2018 hepatitis A outbreak in San Diego primarily affected homeless populations, leading to novel public health approaches including sidewalk sanitization and mobile vaccination units.
- The controversial “Tuskegee of the North” refers to a 1970s study where researchers identified hepatitis B carriers in Inuit communities but failed to inform them or provide treatment.
- Egypt’s hepatitis C epidemic (highest global prevalence) resulted largely from a public health campaign against schistosomiasis that used inadequately sterilized needles between the 1950s and 1980s.
Unexpected Connections:
- Coffee consumption is associated with reduced liver enzyme levels, slower fibrosis progression, and lower liver cancer risk across multiple forms of liver disease.
- Hepatitis A infection appears to offer some protection against nonalcoholic fatty liver disease through unclear mechanisms.
- Individuals with certain genetic hemochromatosis mutations may have relative protection against hepatitis C progression.
- Cholesterol-lowering statin medications appear to reduce liver cancer risk in patients with chronic hepatitis B and C.
Modern Challenges:
- “NASH Trash” is a controversial term describing the phenomenon of patients being denied liver transplantation due to obesity and metabolic factors despite appropriate medical need.
- “Transplant Tourism” refers to traveling to countries with less regulated organ procurement for liver transplantation, raising significant ethical concerns.
- The “Treatment Cliff” describes the dramatic disparities in hepatitis C treatment access based on fibrosis stage, insurance status, and geography.
- “Diagnostic Limbo” refers to patients with features of both autoimmune hepatitis and other liver diseases (overlap syndromes) who require specialized management approaches.
Understanding these lesser-known aspects of hepatitis provides context to the scientific advances, challenges, and human stories behind the disease. While scientific progress has transformed many forms of hepatitis from deadly diseases to preventable or curable conditions, persistent myths, special population considerations, and unique clinical challenges highlight the continuing need for education, research, and accessible care models.
References
World Health Organization. (2022). Global Hepatitis Report 2022. Geneva: World Health Organization.
Centers for Disease Control and Prevention. (2023). Viral Hepatitis Surveillance – United States, 2021. Atlanta: U.S. Department of Health and Human Services.
Thomas, D. L. (2019). Global Elimination of Chronic Hepatitis. New England Journal of Medicine, 380(21), 2041-2050.
Younossi, Z. M., Koenig, A. B., Abdelatif, D., Fazel, Y., Henry, L., & Wymer, M. (2016). Global epidemiology of nonalcoholic fatty liver disease—Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology, 64(1), 73-84.
European Association for the Study of the Liver. (2022). EASL Clinical Practice Guidelines on the management of hepatitis B virus infection. Journal of Hepatology, 77(1), 220-293.
Ghany, M. G., Morgan, T. R., & AASLD-IDSA Hepatitis C Guidance Panel. (2020). Hepatitis C guidance 2019 update: AASLD-IDSA recommendations for testing, managing, and treating hepatitis C virus infection. Hepatology, 71(2), 686-721.
Terrault, N. A., Lok, A. S., McMahon, B. J., Chang, K. M., Hwang, J. P., Jonas, M. M., … & Wong, J. B. (2018). Update on prevention, diagnosis, and treatment of chronic hepatitis B: AASLD 2018 hepatitis B guidance. Hepatology, 67(4), 1560-1599.
Singal, A. K., Bataller, R., Ahn, J., Kamath, P. S., & Shah, V. H. (2018). ACG Clinical Guideline: Alcoholic Liver Disease. The American Journal of Gastroenterology, 113(2), 175-194.
Chalasani, N., Younossi, Z., Lavine, J. E., Charlton, M., Cusi, K., Rinella, M., … & Sanyal, A. J. (2018). The diagnosis and management of nonalcoholic fatty liver disease: Practice guidance from the American Association for the Study of Liver Diseases. Hepatology, 67(1), 328-357.
Manne, V., Akhtar, E., & Saab, S. (2014). Cirrhosis regression in patients with viral hepatitis B and C: a systematic review. Journal of Clinical Gastroenterology, 48(9), e76-e84.
Lazarus, J. V., Pericàs, J. M., Picchio, C., Cernosa, J., Hoekstra, M., Luhmann, N., … & Colombo, M. (2019). We know DAAs work, so now what? Simplifying models of care to enhance the hepatitis C cascade. Journal of Internal Medicine, 286(5), 503-525.
Newsome, P. N., Buchholtz, K., Cusi, K., Linder, M., Okanoue, T., Ratziu, V., … & Sanyal, A. J. (2021). A placebo-controlled trial of subcutaneous semaglutide in nonalcoholic steatohepatitis. New England Journal of Medicine, 384(12), 1113-1124.
Feld, J. J., Jacobson, I. M., Hézode, C., Asselah, T., Ruane, P. J., Gruener, N., … & Zeuzem, S. (2015). Sofosbuvir and velpatasvir for HCV genotype 1, 2, 4, 5, and 6 infection. New England Journal of Medicine, 373(27), 2599-2607.
Thursz, M. R., Richardson, P., Allison, M., Austin, A., Bowers, M., Day, C. P., … & STOPAH Trial. (2015). Prednisolone or pentoxifylline for alcoholic hepatitis. New England Journal of Medicine, 372(17), 1619-1628.
Papatheodoridis, G. V., Dimou, E., Dimakopoulos, K., Manolakopoulos, S., Rapti, I., Kitis, G., … & Hadziyannis, S. J. (2008). Outcome of hepatitis B e antigen–negative chronic hepatitis B on long-term nucleos(t)ide analog therapy starting with lamivudine. Hepatology, 42(1), 121-129.
Polaris Observatory Collaborators. (2018). Global prevalence, treatment, and prevention of hepatitis B virus infection in 2016: a modelling study. The Lancet Gastroenterology & Hepatology, 3(6), 383-403.
Wong, R. J., Aguilar, M., Cheung, R., Perumpail, R. B., Harrison, S. A., Younossi, Z. M., & Ahmed, A. (2015). Nonalcoholic steatohepatitis is the second leading etiology of liver disease among adults awaiting liver transplantation in the United States. Gastroenterology, 148(3), 547-555.
Alvarez-Sola, G., Uriarte, I., Latasa, M. U., Jimenez, M., Barcena-Varela, M., Santamaría, E., … & Avila, M. A. (2018). Engineered fibroblast growth factor 19 protects from acetaminophen-induced liver injury and stimulates aged liver regeneration in mice. Cell Death & Disease, 9(6), 1-16.
Blach, S., Zeuzem, S., Manns, M., Altraif, I., Duberg, A. S., Muljono, D. H., … & Polaris Observatory HCV Collaborators. (2017). Global prevalence and genotype distribution of hepatitis C virus infection in 2015: a modelling study. The Lancet Gastroenterology & Hepatology, 2(3), 161-176.
Wong, V. W. S., Adams, L. A., de Lédinghen, V., Wong, G. L. H., & Sookoian, S. (2020). Noninvasive biomarkers in NAFLD and NASH—current progress and future promise. Nature Reviews Gastroenterology & Hepatology, 17(8), 455-470.
Lok, A. S., McMahon, B. J., Brown, R. S., Wong, J. B., Ahmed, A. T., Farah, W., … & Mohammed, K. (2016). Antiviral therapy for chronic hepatitis B viral infection in adults: a systematic review and meta-analysis. Hepatology, 63(1), 284-306.
Parikh, N. D., Marrero, W. J., Wang, J., Steuer, J., Tapper, E. B., Konerman, M., … & Singal, A. G. (2019). Projected increase in obesity and non-alcoholic steatohepatitis-related liver transplantation waitlist additions in the United States. Hepatology, 70(2), 487-495.
Cooke, G. S., Andrieux-Meyer, I., Applegate, T. L., Atun, R., Burry, J. R., Cheinquer, H., … & Hepatitis C Elimination & Prevention Public Policy Network. (2019). Accelerating the elimination of viral hepatitis: a Lancet Gastroenterology & Hepatology Commission. The Lancet Gastroenterology & Hepatology, 4(2), 135-184.
Thursz, M., & Morgan, T. R. (2016). Treatment of severe alcoholic hepatitis. Gastroenterology, 150(8), 1823-1834.
Buti, M., & Esteban, R. (2021). Hepatitis B: Treatment of the ‘special populations’. Liver International, 41(S1), 73-81.