⚠️ Disclaimer: The information provided in this article is for educational purposes only and does not constitute medical advice. RevisionTown does not provide diagnosis, treatment, or medical recommendations. Always consult a qualified healthcare professional regarding any medical condition, symptoms, or concerns.
Read More – 🏥 Medical Disclaimer
Comprehensive Report on Hepatic Steatosis
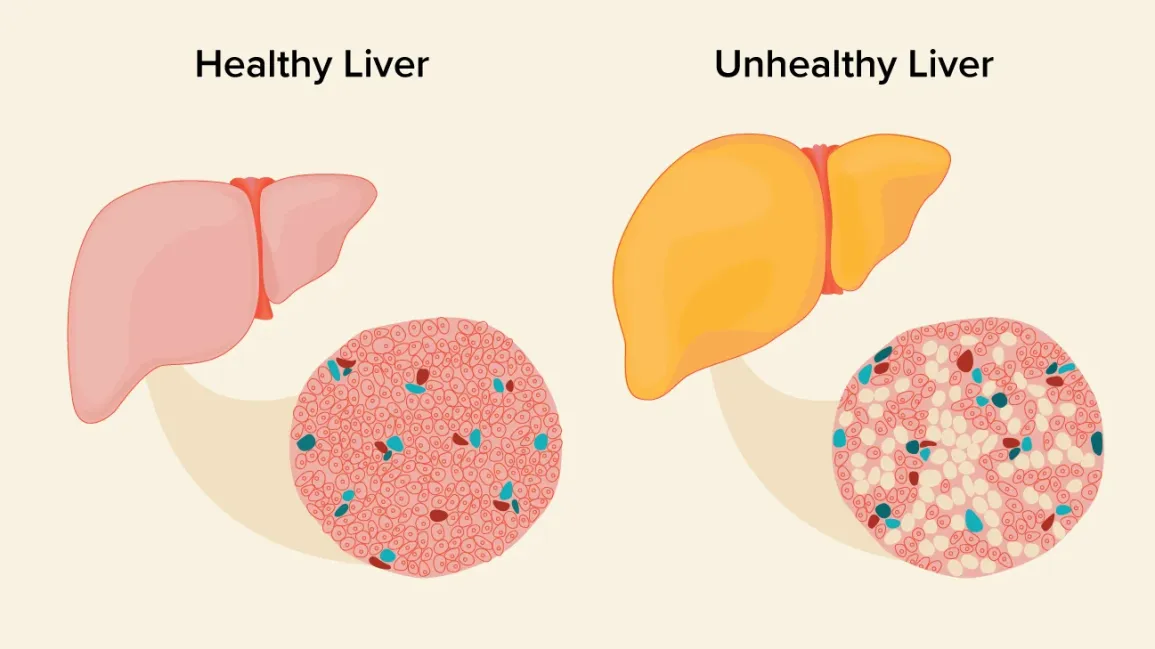
Hepatic steatosis, commonly known as fatty liver disease, is a condition characterized by excessive accumulation of fat in liver cells. It occurs when fat comprises more than 5% of the liver’s weight. The liver, the largest internal organ in the human body, normally contains a small amount of fat, but when this fat accumulation becomes excessive, it can impair liver function and potentially lead to more serious liver conditions.
Hepatic steatosis affects the liver parenchyma, causing enlargement of the liver (hepatomegaly) in some cases. The condition is increasingly recognized as a significant health concern due to its growing prevalence and association with metabolic disorders.
In terms of prevalence, hepatic steatosis has become one of the most common liver disorders globally. Current estimates suggest that approximately 25-30% of the general adult population worldwide is affected by fatty liver disease, with higher rates in certain regions and populations. The condition’s significance lies in its potential progression to more severe liver diseases, including steatohepatitis, fibrosis, cirrhosis, and even liver cancer in some cases, as well as its association with cardiovascular disease, type 2 diabetes, and metabolic syndrome.
2. History & Discoveries
The recognition of fatty liver as a pathological condition dates back to the 19th century when physicians began documenting abnormal fat accumulation in the liver during autopsies. Early descriptions noted the association between fatty liver and conditions such as alcohol consumption, malnutrition, and obesity.
In the late 1800s, medical researchers observed a connection between fatty liver and the development of liver fibrosis and cirrhosis. By the early 1900s, the association between fatty liver and diabetes was also documented, indicating early awareness of metabolic connections.
A significant milestone came in the 1980s when Ludwig and colleagues first described “nonalcoholic steatohepatitis” (NASH) as a distinct condition, distinguishing liver disease with fat accumulation not caused by alcohol from alcoholic liver disease. This differentiation was crucial as it recognized that liver damage similar to alcoholic liver disease could occur in non-drinkers.
Over time, medical understanding has evolved dramatically. Initially, fatty liver was primarily associated with alcohol consumption, but research in the late 20th century revealed multiple pathways leading to hepatic steatosis. The concept of non-alcoholic fatty liver disease (NAFLD) gained acceptance in the 1990s and early 2000s.
In 2023, a significant nomenclature shift occurred when experts renamed the condition to better reflect its causes. Non-alcoholic fatty liver disease (NAFLD) became metabolic dysfunction-associated steatotic liver disease (MASLD), and non-alcoholic steatohepatitis (NASH) became metabolic dysfunction-associated steatohepatitis (MASH). This change acknowledges the important role of metabolic factors in the development of the disease.
Major breakthroughs in research include the identification of genetic factors that influence susceptibility to hepatic steatosis, improved understanding of the role of insulin resistance in fat accumulation, and recognition of the disease’s relationship with metabolic syndrome. Advanced imaging techniques have also revolutionized diagnosis, allowing non-invasive assessment of liver fat content.
3. Symptoms
Hepatic steatosis is often described as a “silent disease” because it typically produces no symptoms in its early stages. Most patients are asymptomatic, and the condition is frequently discovered incidentally during imaging tests ordered for other reasons or through routine blood work showing elevated liver enzymes.
Early Symptoms
When early symptoms do occur, they tend to be vague and nonspecific, including:
- Fatigue or general weakness
- Mild discomfort or a feeling of fullness in the upper right side of the abdomen (where the liver is located)
- General malaise
These symptoms are often so mild that patients may not seek medical attention for them, contributing to the underdiagnosis of the condition in its early stages.
Advanced-Stage Symptoms
As hepatic steatosis progresses, particularly if it develops into steatohepatitis, fibrosis, or cirrhosis, more pronounced symptoms may emerge:
- More significant abdominal pain or discomfort in the upper right quadrant
- Enlarged liver (hepatomegaly), which may be detected during physical examination
- Jaundice (yellowing of the skin and eyes)
- Spider angiomas (spider-like blood vessels visible on the skin)
- Unexplained weight loss
- Loss of appetite
In cases that progress to cirrhosis, complications can include:
- Ascites (fluid accumulation in the abdomen)
- Edema (swelling) in the legs and ankles
- Easy bruising and bleeding
- Confusion and difficulty concentrating (hepatic encephalopathy)
- Esophageal varices (enlarged veins that may bleed)
Symptom Progression
The progression of symptoms generally follows the pathological progression of the disease:
- Simple steatosis (fat accumulation) → typically asymptomatic
- Steatohepatitis (fat + inflammation) → may begin to cause mild symptoms
- Fibrosis (scarring) → more pronounced symptoms as liver function becomes compromised
- Cirrhosis (extensive scarring) → severe symptoms and complications
It’s important to note that progression is not inevitable, and with proper management, earlier stages of hepatic steatosis can be reversed before symptoms become severe.
4. Causes
Hepatic steatosis develops due to an imbalance between fat acquisition and removal in the liver. This imbalance can be triggered by various biological and environmental factors.
Biological Causes
Increased Fat Delivery to the Liver:
- Enhanced lipolysis in adipose tissue releases more free fatty acids into the bloodstream
- Increased dietary intake of fats leading to higher chylomicron delivery to the liver
- Altered fat distribution that favors visceral fat accumulation
Increased Fat Synthesis in the Liver:
- Upregulation of de novo lipogenesis (the liver’s creation of new fat from carbohydrates)
- Hyperinsulinemia stimulating fat synthesis pathways
- Dysregulation of transcription factors controlling lipid metabolism
Decreased Fat Export from the Liver:
- Impaired very low-density lipoprotein (VLDL) synthesis or secretion
- Disruptions in the packaging and transport of triglycerides
Decreased Fat Oxidation in the Liver:
- Mitochondrial dysfunction reducing the capacity to burn fatty acids
- Impairment of beta-oxidation pathways
- Alterations in peroxisome proliferator-activated receptor (PPAR) signaling
Environmental Causes
Dietary Factors:
- High caloric intake, particularly from simple carbohydrates and saturated fats
- High fructose consumption, which enhances de novo lipogenesis
- Western diet patterns rich in processed foods
Physical Inactivity:
- Sedentary lifestyle reducing energy expenditure and metabolic health
- Insufficient exercise limiting the utilization of fatty acids for energy
Alcohol Consumption:
- Excessive alcohol intake damaging mitochondria and impairing fat metabolism
- Alcohol promoting the generation of reactive oxygen species that cause cellular injury
Environmental Toxins:
- Exposure to certain industrial chemicals and pollutants that disrupt metabolism
- Some endocrine-disrupting compounds affecting lipid regulation
Medications:
- Various drugs including corticosteroids, tamoxifen, amiodarone, methotrexate, and some antipsychotics
Genetic and Hereditary Factors
Genetic variants significantly influence an individual’s susceptibility to developing hepatic steatosis. Key genetic factors include:
PNPLA3 Gene: The patatin-like phospholipase domain-containing protein 3 gene variant (I148M) is strongly associated with increased hepatic fat content and susceptibility to more advanced liver disease. This variant is more common in Hispanic populations, partly explaining the higher prevalence of fatty liver disease in this group.
TM6SF2 Gene: Transmembrane 6 superfamily member 2 gene variations affect lipoprotein metabolism and are associated with increased liver fat but paradoxically lower serum lipid levels.
MBOAT7 Gene: Membrane bound O-acyltransferase domain containing 7 gene variants alter phospholipid metabolism and are linked to increased steatosis and fibrosis risk.
GCKR Gene: Glucokinase regulatory protein gene polymorphisms influence glucose metabolism and increase susceptibility to hepatic steatosis.
HSD17B13 Gene: Variants in this gene encoding a liver-specific lipid droplet protein have been associated with reduced risk of progressive NASH and fibrosis.
Familial clustering of hepatic steatosis indicates strong heritability, with studies suggesting that genetic factors may account for up to 30-50% of the variability in liver fat content among individuals.
5. Risk Factors
Multiple factors increase the risk of developing hepatic steatosis, with significant variations across demographic groups.
Age, Gender, and Occupation
- Age: Prevalence increases with age, typically peaking in middle age (40s-60s). However, concerning trends show increasing rates in children and young adults.
- Gender: Males generally have a higher risk of developing fatty liver, particularly in earlier life stages. After menopause, females show increased susceptibility, suggesting hormonal influences.
- Occupation: Sedentary occupations with prolonged sitting increase risk, as do high-stress jobs that may promote unhealthy eating habits. Shift work disrupting circadian rhythms has also been linked to metabolic disturbances that predispose to fatty liver.
Lifestyle Factors
- Diet: High consumption of processed foods, refined carbohydrates, sugary beverages, and saturated fats significantly increases risk.
- Physical Inactivity: Sedentary lifestyle is a major risk factor independent of weight.
- Alcohol Consumption: Even moderate alcohol intake can exacerbate fatty liver in susceptible individuals.
- Sleep Disruption: Poor sleep quality and sleep apnea are associated with increased risk.
Environmental Factors
- Urban Environment: Urban living is associated with higher rates, potentially due to food environments, stress, and reduced physical activity.
- Socioeconomic Status: Lower socioeconomic status correlates with higher risk, possibly due to limited access to healthy foods and healthcare.
- Exposure to Endocrine-Disrupting Chemicals: Certain industrial chemicals and pollutants may disrupt metabolic pathways.
Genetic and Ethnic Factors
- Ethnicity: Highest prevalence is observed in Hispanic populations (58-65%), followed by Caucasians (44-45%), with lower rates in Black populations (24-35%). This distribution is partly explained by genetic variants affecting fat metabolism.
- Family History: Having first-degree relatives with fatty liver increases risk substantially.
Pre-existing Conditions
- Obesity: Body Mass Index (BMI) >30 kg/m² is strongly associated with fatty liver, particularly when fat is distributed centrally (visceral adiposity).
- Metabolic Syndrome: A cluster of conditions including high blood pressure, high blood sugar, excess body fat around the waist, and abnormal cholesterol levels.
- Type 2 Diabetes: Insulin resistance is a key pathophysiological mechanism in fatty liver development.
- Dyslipidemia: High triglycerides and low HDL cholesterol increase risk.
- Polycystic Ovary Syndrome (PCOS): Women with PCOS have higher rates of fatty liver.
- Hypothyroidism: Thyroid dysfunction affects lipid metabolism.
- Obstructive Sleep Apnea: Associated with increased risk independent of obesity.
Understanding these risk factors helps identify individuals who may benefit from earlier screening and intervention. Many of these factors are modifiable, offering opportunities for prevention through lifestyle changes and management of underlying conditions.
6. Complications
Hepatic steatosis, once considered a benign condition, is now recognized as a potential precursor to serious liver and systemic complications. The progression and complications vary significantly between individuals, influenced by genetic predisposition, lifestyle factors, and comorbidities.
Liver Complications
Progressive Liver Disease:
- Steatohepatitis: Simple steatosis can progress to steatohepatitis (NASH/MASH), characterized by liver inflammation, which affects approximately 20-30% of individuals with fatty liver.
- Fibrosis: Persistent inflammation leads to scarring (fibrosis) as the liver attempts to repair itself. This occurs in about 30-40% of patients with steatohepatitis over 5-10 years.
- Cirrhosis: Advanced fibrosis can progress to cirrhosis, with extensive scarring that disrupts liver architecture and function. Approximately 10-15% of patients with NASH develop cirrhosis over 10-15 years.
- Hepatocellular Carcinoma (HCC): The risk of liver cancer is significantly increased in patients with fatty liver-related cirrhosis, with an annual incidence of 1-2%. Importantly, HCC can occasionally develop even in non-cirrhotic fatty liver disease.
- Liver Failure: End-stage liver disease requiring transplantation can result from advanced cirrhosis. Fatty liver disease is becoming a leading indication for liver transplantation in many countries.
Systemic Complications
Cardiovascular Complications:
- Patients with fatty liver have a 1.5-2 fold increased risk of cardiovascular events.
- Fatty liver is independently associated with coronary artery disease, cardiac dysfunction, and arrhythmias.
- Cardiovascular disease, rather than liver disease, is actually the leading cause of death in patients with fatty liver.
Metabolic Complications:
- Type 2 Diabetes: Fatty liver increases the risk of developing diabetes by 2-5 fold and worsens glycemic control in those with established diabetes.
- Insulin Resistance: Hepatic steatosis contributes to systemic insulin resistance, creating a vicious cycle that further worsens metabolic health.
Renal Complications:
- Increased risk of chronic kidney disease, with a 2-fold higher prevalence compared to matched controls without fatty liver.
- Accelerated progression of existing kidney disease.
Extrahepatic Cancers:
- Emerging evidence suggests associations with colorectal, breast, and other cancers, though causal relationships are still being investigated.
Impact on Organ Systems
Gastrointestinal System:
- Portal hypertension in advanced disease can lead to varices, ascites, and spontaneous bacterial peritonitis.
- Impaired bile production and flow in advanced disease.
Endocrine System:
- Disruption of multiple hormone pathways, including insulin, adipokines, and sex hormones.
- Thyroid dysfunction is more common in patients with fatty liver.
Central Nervous System:
- Hepatic encephalopathy in advanced disease, ranging from subtle cognitive changes to coma.
- Emerging evidence for associations with depression and cognitive decline even in non-cirrhotic fatty liver.
Immune System:
- Altered immune function with implications for response to infections and vaccine efficacy.
- Increased susceptibility to certain infections.
Long-term Health Impact
The long-term impact on health is substantial. Life expectancy in patients with advanced fatty liver disease may be reduced by 10-12 years, with mortality rates approximately 1.34 times higher than in the general population. Quality of life is often significantly impacted, particularly in those with progressive disease.
The presence of comorbidities dramatically increases complication rates. For instance, the combination of fatty liver with type 2 diabetes accelerates progression to advanced liver disease by 2-3 fold compared to fatty liver alone.
7. Diagnosis & Testing
Diagnosing hepatic steatosis involves various approaches, from clinical evaluation to advanced imaging techniques. Each method has specific advantages, limitations, and applications in clinical practice.
Clinical Evaluation
The diagnostic process typically begins with:
- Medical History: Assessment of risk factors (obesity, diabetes, metabolic syndrome), alcohol consumption, medication use, family history, and symptoms.
- Physical Examination: Checking for hepatomegaly (enlarged liver), splenomegaly, jaundice, and other signs of liver disease. However, physical findings are often absent in early-stage disease.
- Initial Laboratory Tests: Liver function tests including alanine aminotransferase (ALT), aspartate aminotransferase (AST), and gamma-glutamyl transferase (GGT). These enzymes are often elevated but can be normal despite significant steatosis.
Blood-Based Biomarkers
Several biomarkers and scores can aid in diagnosis:
- Fatty Liver Index (FLI): Combines BMI, waist circumference, triglycerides, and GGT to predict steatosis. A score ≥60 indicates likely hepatic steatosis with sensitivity of 61% and specificity of 86%.
- SteatoTest: A proprietary algorithm combining 10 markers with age, gender, height, and weight. Shows good diagnostic accuracy with AUROC of 0.79-0.80.
- Hepatic Steatosis Index (HSI): Based on ALT/AST ratio, BMI, gender, and presence of diabetes. A score >36 suggests steatosis.
- NAFLD Liver Fat Score: Incorporates insulin, AST, ALT, and presence of metabolic syndrome.
Blood tests for fibrosis assessment include:
- FIB-4 Score: Combines age, AST, ALT, and platelet count to predict fibrosis.
- NAFLD Fibrosis Score: Incorporates age, BMI, diabetes status, AST/ALT ratio, albumin, and platelet count.
- Enhanced Liver Fibrosis (ELF) Test: Measures three direct markers of fibrosis.
Imaging Studies
Non-invasive imaging plays a crucial role in diagnosis:
Ultrasound: First-line imaging technique with sensitivity of 85% and specificity of 94% for moderate-to-severe steatosis. However, sensitivity drops to 65% for mild steatosis. Advantages include wide availability, low cost, and absence of radiation.
Transient Elastography (FibroScan®) with Controlled Attenuation Parameter (CAP): Combines liver stiffness measurement (for fibrosis) with CAP (for steatosis quantification). CAP values ≥248 dB/m indicate steatosis with sensitivity of 78% and specificity of 79%.
Computed Tomography (CT): Liver attenuation values on non-contrast CT reflect fat content. Liver-to-spleen ratio <0.9 or liver attenuation <40 Hounsfield units suggests significant steatosis. Less sensitive than ultrasound for mild steatosis.
Magnetic Resonance Imaging (MRI): Most accurate non-invasive method. MRI-PDFF (proton density fat fraction) can detect as little as 3% liver fat with accuracy comparable to liver biopsy. Limitations include cost and availability.
Magnetic Resonance Spectroscopy (MRS): The gold standard non-invasive technique, capable of measuring liver fat with high precision. Limited by availability and expertise requirements.
Liver Biopsy
Despite advances in non-invasive methods, liver biopsy remains the definitive diagnostic tool:
Histological Assessment: Allows direct visualization and quantification of steatosis, inflammation, hepatocyte ballooning, and fibrosis. Steatosis is graded based on percentage of hepatocytes containing fat: grade 0 (<5%), grade 1 (5-33%), grade 2 (34-66%), and grade 3 (>66%).
Advantages: Provides comprehensive assessment of disease severity, identifies NASH/MASH, and excludes other liver diseases.
Limitations: Invasive procedure with risks of pain, bleeding, and rare mortality (0.01-0.1%). Subject to sampling error as only 1/50,000 of the liver is sampled.
Diagnostic Algorithms
Modern diagnostic approaches typically follow a stepwise algorithm:
- Initial Risk Assessment: Clinical evaluation and basic blood tests
- Non-invasive Testing: Combination of biomarkers and imaging (usually ultrasound first)
- Advanced Assessment: For indeterminate cases or to stage disease severity (specialized imaging or biomarkers)
- Liver Biopsy: Reserved for cases where non-invasive methods are inconclusive, or when precise staging is needed for treatment decisions
Early Detection Methods
Emerging approaches for early detection include:
- Multi-parametric MRI: Combining multiple MRI sequences for comprehensive assessment
- Novel Biomarkers: Including circulating miRNAs, metabolomics profiles, and proteomics
- Breath Tests: Analysis of volatile organic compounds as metabolic indicators
- Machine Learning Algorithms: Integrating clinical, laboratory, and imaging data for improved accuracy
The choice of diagnostic method depends on clinical context, local availability, cost considerations, and the specific question being addressed (detection of steatosis, staging of fibrosis, or monitoring response to treatment).
8. Treatment Options
The management of hepatic steatosis encompasses a range of approaches, from lifestyle modifications to pharmacological interventions and, in severe cases, surgical options. Treatment strategies are typically tailored to disease severity, comorbidities, and individual patient factors.
Lifestyle Modifications
Lifestyle changes form the cornerstone of treatment for hepatic steatosis:
Weight Loss: A reduction of 3-5% of body weight can improve steatosis, while 7-10% weight loss may resolve steatohepatitis and reduce fibrosis. Gradual weight loss (1-2 pounds/week) is recommended, as rapid weight loss can worsen liver inflammation.
Dietary Modifications:
- Mediterranean diet (rich in olive oil, nuts, fruits, vegetables, and fish) has shown significant benefits.
- Reduction in simple carbohydrates and fructose consumption.
- Moderate fat intake with emphasis on monounsaturated and omega-3 fatty acids.
- Limited processed foods and sugar-sweetened beverages.
- Caloric restriction of 500-1000 kcal/day below requirements.
Physical Activity:
- Regular aerobic exercise (150 minutes of moderate-intensity or 75 minutes of vigorous activity weekly).
- Resistance training twice weekly to improve muscle mass and insulin sensitivity.
- Even without significant weight loss, exercise alone can reduce hepatic fat by 20-30%.
Alcohol Abstinence/Reduction:
- Complete abstinence for those with alcohol-related fatty liver.
- Minimal consumption (if any) for those with metabolic-associated fatty liver.
Medications
Several medications show promise for treating hepatic steatosis, though few are specifically approved for this indication:
Antidiabetic Agents:
- Pioglitazone: A thiazolidinedione that improves insulin sensitivity and reduces liver fat, inflammation, and fibrosis. Recommended for patients with biopsy-proven NASH, particularly those with diabetes.
- GLP-1 Receptor Agonists: Medications like semaglutide promote weight loss and improve liver histology. Recent clinical trials show significant benefits for steatohepatitis.
- Metformin: While it improves insulin sensitivity, evidence for direct benefit on liver histology is limited.
- SGLT2 Inhibitors: Emerging data suggest benefits through weight loss and improved metabolic parameters.
Vitamin E: A powerful antioxidant that reduces oxidative stress and inflammation. Recommended at 800 IU/day for non-diabetic patients with biopsy-proven NASH, but concerns exist about long-term safety.
Lipid-Lowering Agents:
- Statins: Safe in patients with fatty liver and may offer benefits beyond cardiovascular protection.
- Fibrates: Can improve metabolic parameters but have limited evidence for liver histology.
Novel Therapies in Late-Stage Development:
- Obeticholic Acid: A farnesoid X receptor agonist showing improvement in fibrosis.
- Resmetirom: A thyroid hormone receptor β agonist that reduces liver fat and improves NASH.
- Cenicriviroc: An inhibitor of CCR2/CCR5 chemokine receptors that targets inflammation and fibrosis.
- Aramchol: A synthetic fatty acid-bile acid conjugate that modulates SCD1 activity.
Surgical and Procedural Interventions
For patients with severe obesity or advanced disease:
Bariatric Surgery: Produces substantial and sustained weight loss with dramatic improvement in steatosis in 85-90% of patients, steatohepatitis resolution in 70%, and fibrosis reduction in 30-40%. Most effective interventions are gastric bypass and sleeve gastrectomy.
Liver Transplantation: For end-stage liver disease resulting from progression to cirrhosis. Fatty liver disease is now among the leading indications for liver transplantation in many countries.
Experimental Procedures: Endoscopic bariatric techniques such as intragastric balloons provide less invasive alternatives to surgery for selected patients.
Treatment Monitoring and Follow-up
Regular monitoring is essential to assess treatment response:
Clinical Assessment: Evaluation of symptoms, weight, and metabolic parameters every 3-6 months.
Laboratory Monitoring: Liver enzymes, lipid profile, glucose/HbA1c every 3-6 months.
Imaging: Reassessment of liver fat by ultrasound, FibroScan, or MRI at 6-12 month intervals.
Repeat Liver Biopsy: Considered in clinical trials or when assessing response to specific therapies, typically after 1-2 years of treatment.
Personalized Treatment Approaches
Treatment is increasingly personalized based on:
- Disease Phenotype: Presence of steatohepatitis, degree of fibrosis, and rate of progression.
- Genetic Factors: PNPLA3 and other genetic variants may influence treatment response.
- Comorbidities: Presence of diabetes, cardiovascular disease, or other conditions.
- Individual Barriers: Addressing psychological, socioeconomic, and behavioral factors affecting adherence.
Integrated Care Models
Multidisciplinary care involving hepatologists, endocrinologists, dietitians, exercise specialists, and mental health professionals provides comprehensive management for patients with fatty liver disease.
The treatment landscape continues to evolve rapidly, with numerous clinical trials investigating novel agents targeting specific pathways in fatty liver disease pathogenesis. In the absence of approved pharmacotherapy specifically for MASLD/MASH, lifestyle intervention remains the foundation of treatment, with medications primarily addressing comorbidities and advanced disease.
9. Prevention & Precautionary Measures
Preventing hepatic steatosis involves addressing modifiable risk factors through lifestyle choices and health management strategies. A comprehensive approach can significantly reduce the risk of developing fatty liver disease or slow its progression in those already affected.
Lifestyle Strategies
Dietary Recommendations:
- Adopt a Mediterranean-style diet rich in fruits, vegetables, whole grains, olive oil, nuts, and fish
- Limit intake of processed foods, refined carbohydrates, and sugar-sweetened beverages
- Reduce consumption of saturated and trans fats
- Moderate portion sizes to maintain a healthy caloric balance
- Include foods with anti-inflammatory properties (fatty fish, olive oil, nuts, turmeric)
- Consider intermittent fasting under medical supervision, which has shown promise in reducing liver fat
Physical Activity Guidelines:
- Aim for at least 150 minutes of moderate-intensity aerobic activity weekly
- Incorporate resistance training 2-3 times per week
- Reduce sedentary time with regular movement breaks throughout the day
- Start gradually and increase activity levels progressively if previously inactive
- Find enjoyable activities to promote long-term adherence
Weight Management:
- Maintain a healthy weight with BMI in the 18.5-24.9 kg/m² range
- If overweight or obese, aim for gradual weight loss of 0.5-1 kg per week
- Focus on sustainable dietary changes rather than extreme calorie restriction
- Consider medically supervised weight management programs for those with significant obesity
Alcohol Consumption:
- Limit alcohol intake to no more than one standard drink per day for women and two for men
- Consider complete abstinence if other risk factors for liver disease are present
- Avoid binge drinking patterns
- Be aware that alcohol may interact with medications and exacerbate liver damage
Environmental Precautions
Chemical Exposure Reduction:
- Minimize exposure to environmental toxins such as certain pesticides and industrial chemicals
- Use protective equipment when working with potential hepatotoxins
- Choose natural cleaning products and personal care items when possible
- Ensure proper ventilation when using chemical products
Workplace Considerations:
- Implement regular movement breaks in sedentary jobs
- Address workplace stress which can contribute to unhealthy eating patterns
- Encourage workplace wellness programs that promote physical activity and healthy eating
- Follow safety protocols when working with hepatotoxic chemicals
Medical Interventions
Vaccination Recommendations:
- Receive hepatitis A and B vaccines, as viral hepatitis can severely impact those with underlying fatty liver
- Stay current with recommended pneumococcal and influenza vaccinations, as chronic liver disease increases susceptibility to infections
Medication Management:
- Regularly review medications with healthcare providers to identify those that may affect liver health
- Use caution with over-the-counter pain relievers, particularly acetaminophen (paracetamol)
- Disclose all supplements and herbal remedies to healthcare providers, as some may affect the liver
- Follow prescribed regimens for managing diabetes, hypertension, and dyslipidemia to reduce metabolic risk factors
Preventive Screening:
- Regular check-ups including liver function tests for those with risk factors
- Consider periodic ultrasonography for high-risk individuals
- Early detection of metabolic disorders that may contribute to fatty liver development
- Genetic counseling for families with hereditary forms of fatty liver disease
Special Populations
Children and Adolescents:
- Promote healthy eating habits and physical activity from an early age
- Limit screen time which contributes to sedentary behavior
- Address childhood obesity through family-based interventions
- Screen at-risk youth for early signs of fatty liver disease
Pregnant Women:
- Maintain appropriate weight gain during pregnancy
- Screen for gestational diabetes and manage effectively if diagnosed
- Follow nutritional guidelines specific to pregnancy
- Be aware of acute fatty liver of pregnancy as a rare but serious condition requiring immediate medical attention
Older Adults:
- Adapt physical activity recommendations to ability level
- Maintain muscle mass through resistance training and adequate protein intake
- Consider age-related changes in metabolism when developing prevention strategies
- Be vigilant about medication interactions and cumulative effects
Public Health Approaches
Education and Awareness:
- Increase public knowledge about fatty liver disease and its risk factors
- Provide accessible information about prevention strategies
- Incorporate liver health into broader health education initiatives
- Use technology and social media to disseminate evidence-based prevention information
Policy Interventions:
- Support urban planning that promotes physical activity
- Advocate for food policies that improve access to healthy, affordable foods
- Develop workplace wellness programs that address liver health
- Implement school-based programs promoting healthy lifestyles
By implementing these preventative measures at individual and community levels, the rising tide of hepatic steatosis may be stemmed, reducing the burden of liver disease and associated complications globally.
10. Global & Regional Statistics
Hepatic steatosis has emerged as a significant global health challenge with varying prevalence across different regions and populations. Understanding these epidemiological patterns is crucial for developing targeted public health strategies.
Global Prevalence
Recent meta-analyses indicate that the global prevalence of hepatic steatosis has risen dramatically:
Overall Prevalence: Current estimates suggest that 25-30% of the global adult population has some form of fatty liver disease, with approximately 30.1-32.4% of adults worldwide affected according to the most comprehensive studies.
Temporal Trends: The global prevalence has increased by more than 50% over the past three decades, rising from approximately 25.3% in the 1990-2006 period to 38.0% in the 2016-2019 period.
Non-alcoholic Forms: Metabolic dysfunction-associated steatotic liver disease (MASLD, formerly NAFLD) accounts for the majority of cases globally, affecting an estimated 30-38% of the adult population.
Steatohepatitis: The inflammatory form (MASH/NASH) affects approximately 3-5% of the global population, representing about 20% of those with fatty liver disease.
Regional Variations
Significant geographic disparities exist in the prevalence of hepatic steatosis:
Middle East and South America: Highest regional prevalence (30-35%), particularly in countries experiencing rapid nutritional transition.
Asia: Historically lower rates, but experiencing the fastest increase, with prevalence now ranging from 15-30% depending on the country. Urban China has seen rates increase to 20-30% in recent years.
Europe: Prevalence ranges from 20-30%, with higher rates in Southern European countries (25-30%) compared to Northern European countries (20-25%).
North America: Very high prevalence, with rates of 24-32% in the United States, 25% in Canada, and similar rates in Mexico.
Africa: Limited data suggests lower but rising prevalence (10-20%), with significant urban-rural disparities and higher rates in North Africa compared to Sub-Saharan regions.
Oceania: Prevalence of 20-30% in Australia and New Zealand, with significantly higher rates among indigenous populations.
Demographic Patterns
Prevalence varies substantially across demographic groups:
Ethnicity: Within multiethnic societies, Hispanic populations typically show the highest prevalence (58-65%), followed by Caucasians (44-45%), with lower rates among Black populations (24-35%). These differences appear partly related to genetic factors, particularly PNPLA3 gene variants.
Age: Prevalence increases with age, typically peaking in the 40-60 year age range, though alarming increases have been noted in children and young adults in recent decades.
Gender: Generally higher prevalence in males during early and middle adulthood, with the gap narrowing or reversing after menopause, suggesting hormonal influences.
Urban vs. Rural: Consistently higher rates in urban settings across all regions, reflecting differences in diet, physical activity, and overall lifestyle.
Mortality and Disease Burden
The impact of fatty liver disease on global health outcomes is substantial:
Mortality: Fatty liver-related mortality has increased by approximately 65% globally since 1990, with the most pronounced increases in developing countries experiencing nutritional transition.
Years of Life Lost: Fatty liver disease accounts for an estimated 4.5-5.5 million disability-adjusted life years (DALYs) globally.
Cirrhosis Progression: Approximately 20% of individuals with steatohepatitis progress to cirrhosis over 10-15 years, with regional variations influenced by genetic factors and access to healthcare.
Liver Transplantation: Fatty liver-related liver failure has become the second leading indication for liver transplantation in many Western countries and is projected to become the leading cause within a decade.
Economic Impact
The economic burden of hepatic steatosis varies by region but is universally significant:
Healthcare Costs: Direct annual healthcare costs attributable to fatty liver disease range from $103 billion in the United States to €35 billion in European Union countries.
Productivity Losses: Indirect costs through decreased productivity and increased absenteeism add substantially to the economic burden, estimated at $120-150 billion annually in North America alone.
Cost Projection: Models predict that healthcare costs related to fatty liver disease will increase by 40-60% by 2030 if current trends continue.
Future Projections
Modeling studies provide concerning projections for the coming decades:
Prevalence Growth: Global prevalence is projected to exceed 40% by 2030 based on current trends.
Complications: The number of cases with advanced fibrosis is expected to increase by 63% between 2015 and 2030.
Mortality Increase: Liver-related mortality due to fatty liver disease is projected to increase by 178% in the United States, 157% in France, and 200-300% in developing Asian countries by 2030.
These statistics underscore the urgent need for comprehensive public health strategies addressing the growing epidemic of hepatic steatosis, with particular attention to high-risk regions and populations.
11. Recent Research & Future Prospects
The field of hepatic steatosis research is rapidly evolving, with significant advancements in understanding disease mechanisms and developing novel therapeutic approaches. Current research trends and future directions show promise for improved management of this increasingly common condition.
Recent Advances in Understanding
Pathophysiological Mechanisms:
- Discovery of multiple parallel pathways contributing to steatosis development, moving beyond the traditional “two-hit” hypothesis
- Identification of gut microbiota’s critical role in modulating liver fat accumulation and inflammation through metabolites and immune signaling
- Better understanding of mitochondrial dysfunction as a central mechanism in disease progression
- Recognition of the complex interplay between genetic variants and environmental factors in determining individual susceptibility
Genetic and Epigenetic Insights:
- Genome-wide association studies have identified over 20 genetic variants associated with fatty liver susceptibility and progression
- Emerging evidence of epigenetic modifications (DNA methylation, histone modifications, non-coding RNAs) in regulating gene expression related to hepatic steatosis
- Integration of genetic, epigenetic, and metabolomic data to develop personalized risk profiles and treatment strategies
Biomarker Development:
- Advanced metabolomic and proteomic approaches identifying novel circulating biomarkers of disease activity
- Development of liquid biopsy techniques to detect cell-free DNA and extracellular vesicles as indicators of liver damage
- Creation of multi-parameter algorithms combining biomarkers for improved non-invasive assessment of disease severity
Emerging Treatment Approaches
Pharmacological Innovations:
- Metabolic Pathway Modulators: Novel agents targeting specific metabolic pathways, including acetyl-CoA carboxylase inhibitors (reduce de novo lipogenesis) and SCD1 inhibitors (alter fatty acid composition)
- Anti-inflammatory and Anti-fibrotic Agents: Compounds targeting specific inflammatory pathways (e.g., CCR2/CCR5 antagonists) and fibrogenic mechanisms (e.g., galectin-3 inhibitors)
- Nuclear Receptor Modulators: Selective agonists for FXR, PPAR-α/δ, and THR-β that regulate lipid metabolism and inflammation with fewer side effects than earlier generations
Combination Therapy Approaches:
- Synergistic medication combinations targeting multiple disease pathways simultaneously
- Sequential therapy strategies based on disease stage and dominant pathophysiological mechanisms
- Integration of pharmacological with lifestyle interventions for enhanced efficacy
Microbiome-Based Therapies:
- Prebiotics, probiotics, and synbiotics designed to modify gut microbiota composition and function
- Fecal microbiota transplantation being investigated for severe cases
- Targeted bacterial metabolite modulation to improve gut-liver axis function
Cell-Based and Genetic Therapies:
- Mesenchymal stem cell therapy showing promise in early clinical trials for reducing inflammation and promoting liver regeneration
- Gene editing approaches (CRISPR-Cas9) being explored in preclinical models to correct genetic variants associated with disease susceptibility
- RNA interference technologies targeting specific pathogenic pathways
Clinical Trials Landscape
Numerous clinical trials are underway, with several promising candidates in late-stage development:
- Phase 3 Trials: Obeticholic acid, resmetirom, aramchol, and semaglutide have shown positive results in improving liver histology
- Novel Endpoints: Development of non-invasive surrogate endpoints to replace liver biopsy in clinical trials, accelerating drug development
- Combination Approaches: Trials evaluating synergistic effects of combining agents with different mechanisms of action
- Patient Stratification: Increasing focus on identifying patient subgroups most likely to benefit from specific interventions based on genetic profiles and disease phenotypes
Technological Innovations
Advanced Imaging Techniques:
- Development of multiparametric MRI protocols that simultaneously assess steatosis, inflammation, and fibrosis
- Artificial intelligence algorithms enhancing the diagnostic accuracy of conventional imaging modalities
- Point-of-care ultrasound technologies with automated quantification of liver fat content
Digital Health Solutions:
- Mobile applications supporting lifestyle modifications with personalized feedback
- Remote monitoring tools allowing continuous assessment of treatment adherence and response
- Machine learning algorithms predicting disease progression and treatment response based on comprehensive patient data
Precision Medicine Approaches:
- Integration of genetic, metabolomic, clinical, and environmental data to develop personalized risk models
- Tailoring of treatment strategies based on individual disease drivers and response predictors
- Development of point-of-care genetic testing to guide therapy selection
Future Research Directions
Key Areas for Future Investigation:
- Mechanisms linking hepatic steatosis to extrahepatic manifestations, particularly cardiovascular disease
- Factors determining the transition from simple steatosis to steatohepatitis and progressive fibrosis
- Optimal combinations and sequences of therapeutic interventions based on disease stage and individual characteristics
- Long-term safety and efficacy of emerging pharmacological approaches
- Strategies for early identification of high-risk individuals before disease manifestation
- Cost-effective implementation of preventive and therapeutic interventions at population scale
Collaborative Research Initiatives:
- International consortia establishing standardized assessments and biorepositories
- Public-private partnerships accelerating drug development
- Multidisciplinary research teams combining expertise in hepatology, endocrinology, nutrition, genetics, and data science
The future of hepatic steatosis management looks promising, with the convergence of advances in basic science, drug development, technology, and precision medicine approaches. The translation of these research findings into clinical practice is expected to significantly improve outcomes for the growing population affected by this condition in the coming decade.
12. Interesting Facts & Lesser-Known Insights
Beyond the standard medical understanding of hepatic steatosis, there are numerous fascinating aspects and lesser-known insights that provide a deeper appreciation of this condition.
Historical Perspectives
Ancient Recognition: References to fatty liver can be found in ancient medical texts from both Eastern and Western traditions. Hippocrates described liver enlargement associated with dietary excess, while traditional Chinese medicine recognized connections between liver health and dietary balance.
Wartime Observations: During World War II, autopsies of young soldiers revealed unexpected fatty liver changes, providing early insights into non-alcoholic forms of the condition and challenging the assumption that fatty liver was primarily alcohol-related.
Naming Evolution: The condition has undergone multiple naming conventions over decades, reflecting evolving understanding. The most recent shift from NAFLD to MASLD (Metabolic dysfunction-Associated Steatotic Liver Disease) in 2023 represents a conceptual recognition of underlying metabolic dysfunction rather than simply defining the condition by what it is not (non-alcoholic).
Biological Curiosities
The Lean Paradox: Approximately 10-20% of patients with fatty liver disease have normal body weight (lean MASLD). These individuals often have worse outcomes than their overweight counterparts, possibly due to genetic predisposition, altered fat distribution, or sarcopenia (muscle loss).
Circadian Rhythm Connection: Liver fat accumulation shows circadian variations, with disrupted sleep patterns and shift work strongly associated with increased risk. The liver’s metabolic functions are tightly regulated by internal body clocks.
Fructose Sensitivity: The liver processes fructose differently from other sugars, converting it directly to fat through de novo lipogenesis without the regulatory steps that exist for glucose metabolism. This makes high-fructose diets particularly problematic for liver health.
Microbiome Signature: Specific gut bacterial compositions have been identified in patients with fatty liver, with some bacteria producing metabolites that directly influence liver fat accumulation and inflammation. Fecal transplant studies in animals have demonstrated that fatty liver can be “transmitted” through gut microbiota.
Epidemiological Surprises
Gender Paradox: While men have higher rates of simple steatosis, women with the condition appear more likely to progress to advanced disease stages. This paradox may relate to hormonal influences, body fat distribution, or genetic factors.
Coffee’s Protective Effect: Multiple studies show that regular coffee consumption (typically 2-3 cups daily) is associated with a 30-40% reduced risk of fatty liver disease progression. The benefit appears independent of caffeine content, suggesting other coffee compounds may be responsible.
Altitude Effect: Populations living at high altitudes have lower rates of fatty liver disease, even when controlling for lifestyle factors. This may relate to hypoxia-induced metabolic adaptations or differences in gut microbiota at higher elevations.
Global Variations Beyond Lifestyle: Even when controlling for obesity rates and dietary patterns, significant geographic variations in fatty liver prevalence persist, suggesting environmental or genetic factors not yet fully understood.
Clinical Misconceptions
Not Just a Liver Disease: Fatty liver is increasingly recognized as a systemic condition with implications far beyond the liver itself. Some researchers propose it may be considered a standalone cardiometabolic risk factor.
Reversibility Window: While early fatty liver is highly reversible, there appears to be a “point of no return” in disease progression where fibrotic changes become self-perpetuating even after the initial triggers are removed.
Silent but Not Benign: The traditional view of simple steatosis as a benign condition is being challenged by longitudinal studies showing increased long-term mortality even in patients with minimal or no progression to advanced liver disease.
Beyond Obesity and Alcohol: Lesser-known causes include certain medications (amiodarone, tamoxifen, corticosteroids), rapid weight loss, jejunoileal bypass, total parenteral nutrition, and rare genetic disorders.
Occupational and Environmental Factors
Occupation-Specific Risks: Certain professions show higher rates of fatty liver independent of traditional risk factors. These include long-haul truck drivers (disrupted sleep patterns), shift workers, and workers exposed to certain industrial chemicals.
Endocrine-Disrupting Chemicals: Environmental pollutants like bisphenol A, phthalates, and perfluorinated compounds have been linked to hepatic steatosis development through disruption of metabolic regulation.
Built Environment Impact: Urban planning features like walkability, green space access, and food environment significantly influence fatty liver prevalence at community levels.
Future Directions and Innovations
Wearable Tech Applications: Emerging technology may soon allow continuous monitoring of biomarkers related to liver health through non-invasive wearable devices, potentially enabling early intervention.
Chronotherapy Potential: Timing medication administration to align with circadian rhythms of liver metabolism may enhance therapeutic efficacy for fatty liver disease.
Climate Change Connections: Rising global temperatures may indirectly increase fatty liver disease burden through effects on physical activity patterns, food systems, and potential direct effects of heat stress on metabolic function.
Intergenerational Transmission: Emerging evidence suggests maternal fatty liver disease during pregnancy may “program” offspring for increased susceptibility through epigenetic mechanisms, potentially contributing to disease clusters within families beyond shared genetics and lifestyle.
These lesser-known aspects of hepatic steatosis highlight the complexity of the condition and the multidisciplinary approach needed for its understanding and management. They also point to exciting avenues for future research and intervention development.
References
This comprehensive report draws upon a wide range of scientific literature, clinical guidelines, and recent research in the field of hepatic steatosis. Key references include studies on prevalence, diagnostic methods, treatment approaches, and emerging research directions.
For specific statistics, diagnostic criteria, and treatment recommendations, authoritative sources such as the American Association for the Study of Liver Diseases (AASLD), European Association for the Study of the Liver (EASL), and World Gastroenterology Organisation have been consulted.
Recent meta-analyses on global prevalence and epidemiological trends provide the foundation for statistical information, while clinical practice guidelines inform the sections on diagnosis and treatment.
The content on emerging research and future directions is based on the most current publications in high-impact medical journals and presentations at international hepatology conferences.
This report represents a synthesis of current knowledge in the field of hepatic steatosis as of May 2025, with the understanding that this is a rapidly evolving area of medical science.