⚠️ Disclaimer: The information provided in this article is for educational purposes only and does not constitute medical advice. RevisionTown does not provide diagnosis, treatment, or medical recommendations. Always consult a qualified healthcare professional regarding any medical condition, symptoms, or concerns.
Read More – 🏥 Medical Disclaimer
Comprehensive Report on Gastroesophageal Reflux Disease (GERD)
1. Overview
What is GERD?
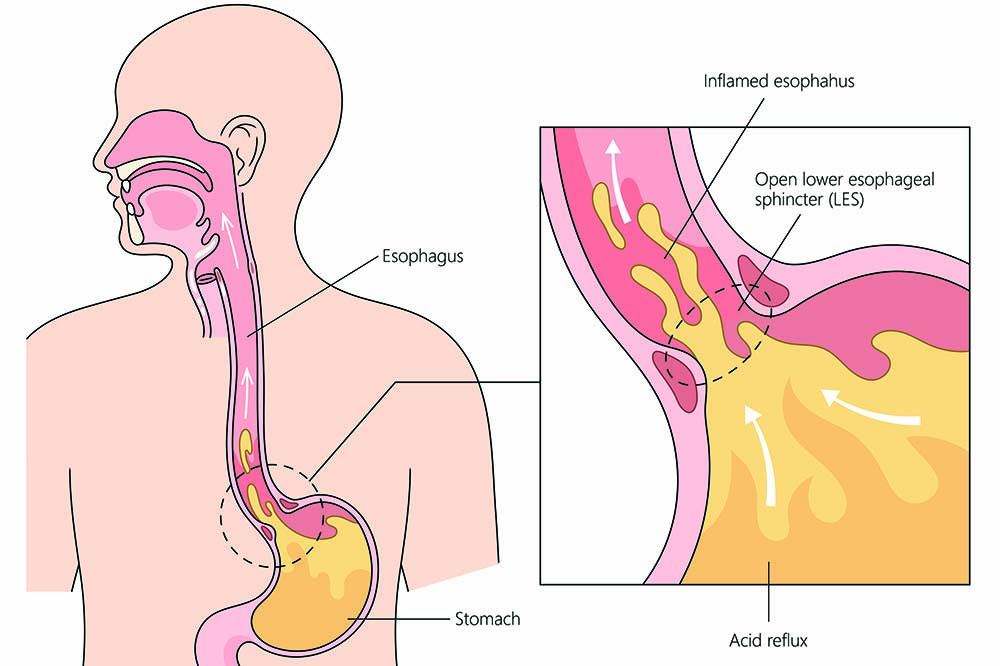
Gastroesophageal Reflux Disease (GERD) is a chronic digestive disorder characterized by the abnormal backflow of stomach contents, primarily acidic gastric juice, into the esophagus. This reflux occurs when the lower esophageal sphincter (LES), a ring of muscle between the esophagus and stomach, functions improperly by relaxing inappropriately or having inadequate pressure. While occasional acid reflux is common and not concerning, GERD involves persistent reflux that occurs more than twice a week, causing inflammation, injury to the esophageal lining, and a range of troublesome symptoms that can significantly impact quality of life.
GERD represents the more severe and chronic manifestation on a spectrum that includes occasional heartburn and acid reflux. The condition is marked not only by its frequency but also by the degree of tissue damage, symptom severity, and impact on daily functioning. It is a complex disorder with multifactorial origins, involving anatomical, physiological, and environmental factors.
Detailed Definition
From a pathophysiological perspective, GERD can be defined by three key components:
Mechanical Component: Abnormal exposure of the esophageal mucosa to gastric contents due to:
- Impaired function of the lower esophageal sphincter
- Hiatal hernia (protrusion of part of the stomach through the diaphragm)
- Impaired esophageal clearance mechanisms
- Delayed gastric emptying
Chemical Component: Damage to esophageal tissues from exposure to:
- Hydrochloric acid
- Pepsin (digestive enzyme)
- Bile acids (in cases of duodenogastroesophageal reflux)
Sensory Component: Heightened esophageal sensitivity to acid or mechanical stimulation, causing:
- Symptoms that may be disproportionate to the degree of acid exposure
- Persistent symptoms despite adequate acid suppression therapy
GERD is classified into several phenotypes:
- Non-erosive reflux disease (NERD): Symptoms present without visible mucosal damage during endoscopy
- Erosive esophagitis: Visible inflammation and erosions of the esophageal lining
- Barrett’s esophagus: Precancerous changes in the esophageal lining due to chronic GERD
- Extraesophageal manifestations: Symptoms affecting areas beyond the esophagus (respiratory, throat, dental)
Affected Body Parts/Organs
While GERD primarily affects the esophagus and stomach, its impact extends to various adjacent and distant organs:
Primary Affected Structures:
Esophagus:
- The lower esophageal sphincter (LES)
- Esophageal mucosa (lining)
- Esophageal muscles and nerves
Stomach:
- Gastric cardia (upper portion of the stomach)
- Gastroesophageal junction
Secondary Affected Areas:
Respiratory System:
- Lungs (through microaspiration)
- Bronchi and bronchioles
- Larynx (voice box)
- Pharynx (throat)
Oral Structures:
- Teeth (through acid erosion)
- Gums and oral mucosa
- Salivary glands
Other Systems:
- Sinuses and nasal passages
- Middle ear (via Eustachian tube)
- Autonomic nervous system components
The damage to the esophagus follows a progressive pattern, beginning with inflammation (esophagitis), potentially advancing to erosions, ulcerations, strictures (narrowing), Barrett’s esophagus (precancerous changes), and in rare cases, adenocarcinoma (cancer).
Prevalence and Significance
GERD represents one of the most prevalent digestive disorders worldwide, with substantial variation across geographic regions and populations:
Global Prevalence:
- Worldwide prevalence ranges from 8-33% of the population
- North America and Western Europe have the highest prevalence (18-28%)
- East Asian countries have traditionally had lower rates (5-8%), though these are increasing
- Middle East countries report high prevalence (12-25%)
- Approximately 1 in 5 Americans experiences GERD symptoms weekly
Demographic Patterns:
- Prevalence increases with age, with a notable rise after age 40
- Affects men and women almost equally, with slight male predominance in erosive disease
- Pregnancy increases risk temporarily in women (30-50% experience symptoms)
- Obesity correlates strongly with GERD prevalence across populations
Healthcare and Economic Impact:
- GERD accounts for approximately 5-7% of primary care physician visits annually
- In the United States, direct and indirect costs exceed $24 billion annually
- Acid-suppressing medications rank among the top-selling pharmaceuticals globally
- GERD is a leading cause of reduced workplace productivity due to both symptoms and side effects of treatments
Medical Significance:
- GERD substantially reduces quality of life, comparable to other chronic diseases
- It is the strongest risk factor for esophageal adenocarcinoma, a cancer with rapidly increasing incidence
- Barrett’s esophagus develops in 5-15% of chronic GERD patients
- GERD can exacerbate or mimic other conditions, including asthma, chronic cough, and cardiac disease
- Nocturnal GERD is associated with sleep disturbances, potentially contributing to other health issues
Public Health Relevance:
- Increasing prevalence globally, particularly in developing countries adopting Western lifestyles
- Major contributor to healthcare utilization and medication use
- Preventable through lifestyle modifications in many cases
- Often undertreated or inappropriately self-treated by patients
GERD’s significance extends beyond its immediate symptoms, affecting multiple dimensions of health, healthcare resources, and economic productivity. Its increasing global prevalence makes it a disorder of growing public health concern, particularly as its complications, including esophageal cancer, carry substantial morbidity and mortality.
2. History & Discoveries
First Identification and Early Understanding
The recognition of gastroesophageal reflux as a pathological condition evolved over centuries, with clear identification as a distinct clinical entity occurring relatively recently:
Ancient Observations:
- Symptoms resembling heartburn were described in ancient Egyptian, Greek, and Roman medical texts
- Avicenna (980-1037 CE) described “burning in the stomach” rising toward the throat
- In 1618, Fabricius Hildanus detailed “cardialgia” (heartburn) and proposed it originated from stomach acid
Early Modern Period (17th-19th Centuries):
- In 1724, Georg Stahl made the connection between stomach acid and esophageal symptoms
- In 1839, Thomas Allbutt described reflux of stomach contents as a mechanism for esophageal inflammation
- William Brinton (1867) detailed the relationship between hiatal hernia and reflux symptoms
Formal Recognition as a Disease (Early 20th Century):
- In 1925, Chevalier Jackson described “peptic esophagitis” as a distinct entity
- Asher Winkelstein published the first comprehensive description of reflux esophagitis in 1935, titled “Peptic Esophagitis: A New Clinical Entity”
- Winkelstein’s paper is often credited as the first formal identification of GERD as a distinct medical condition
- He proposed the now-accepted mechanism that “gastric juice is regurgitated into the lower esophagus, where it produces a peptic esophagitis”
Key Diagnostic Developments:
- Early diagnosis relied primarily on clinical symptoms and barium swallow studies
- The first flexible endoscope, developed by Rudolf Schindler in 1932, allowed direct visualization of esophageal damage
- In 1958, Bernstein and Baker developed the acid perfusion test, demonstrating that acid in the esophagus reproduced patients’ symptoms
- In the 1960s, intraesophageal pH monitoring was introduced, providing objective measurement of acid reflux
Key Historical Figures
Several pioneering individuals made crucial contributions to our understanding of GERD:
Asher Winkelstein (1891-1963):
- American gastroenterologist considered the “father of GERD”
- First to comprehensively describe reflux esophagitis in 1935
- Established the causal relationship between gastric acid reflux and esophageal damage
Norman Barrett (1903-1979):
- British thoracic surgeon who described the condition now known as Barrett’s esophagus in 1950
- Initially believed the affected tissue was a congenitally shortened esophagus
- His name remains attached to this important GERD complication, though his original interpretation was incorrect
Spencer Payne and Claude Clagett:
- Surgeons who developed the first major surgical approach for GERD in 1932
- Pioneered techniques that evolved into modern antireflux surgeries
Rudolf Nissen (1896-1981):
- German surgeon who developed the Nissen fundoplication procedure in 1955
- His technique remains the gold standard surgical approach for GERD
Johnson F. DeMeester:
- Developed the DeMeester score in the 1970s, a standardized system for quantifying acid reflux based on 24-hour pH monitoring
- Created objective diagnostic criteria that remain important today
James Dent:
- Pioneered ambulatory pH monitoring techniques in the 1980s
- Helped establish normal values and pathological thresholds for acid exposure
Major Discoveries and Breakthroughs
The understanding and management of GERD has progressed through several pivotal discoveries:
Pathophysiological Breakthroughs:
Lower Esophageal Sphincter (LES) Function:
- In 1956, Fyke, Code, and Schlegel demonstrated the high-pressure zone at the gastroesophageal junction
- In the 1960s, studies established that inappropriate LES relaxation was central to GERD pathophysiology
- By the 1970s, researchers identified factors affecting LES pressure, including hormones, foods, and medications
Hiatal Hernia Recognition:
- In 1951, Allison described the relationship between hiatal hernia and reflux
- In the 1960s-70s, evidence accumulated showing that hiatal hernia compromises the anti-reflux barrier
- By the 1980s, the combination of hiatal hernia and low LES pressure was recognized as particularly problematic
Esophageal Clearance Mechanisms:
- In the 1960s, researchers identified impaired esophageal peristalsis as a factor prolonging acid contact
- The protective role of saliva in neutralizing acid was established in the 1970s
- Studies in the 1980s demonstrated the concept of “acid clearance time” as an important factor in GERD severity
Diagnostic Advances:
Endoscopic Evaluation:
- Fiberoptic endoscopy in the 1960s revolutionized direct visualization of the esophagus
- In 1978, the Savary-Miller classification system standardized the grading of esophagitis
- The Los Angeles Classification (1990s) further refined endoscopic grading of GERD
pH Monitoring:
- Ambulatory 24-hour pH monitoring was introduced in the 1970s
- Dual-channel monitoring (measuring both distal and proximal esophageal pH) emerged in the 1980s
- Wireless pH monitoring systems were developed in the early 2000s
Esophageal Manometry:
- High-resolution manometry, developed in the 1990s-2000s, provided detailed mapping of esophageal pressures
- Impedance-pH monitoring (2000s) allowed detection of both acid and non-acid reflux
Treatment Milestones:
Pharmaceutical Advances:
- Antacids were the primary treatment until the 1970s
- H2 receptor antagonists (H2RAs), beginning with cimetidine in 1977, revolutionized acid suppression
- Proton pump inhibitors (PPIs), starting with omeprazole in 1989, provided superior acid control
- Combination approaches with prokinetics emerged in the 1990s
Surgical Innovations:
- Belsey Mark IV procedure (1955) offered thoracic approach to fundoplication
- Nissen fundoplication (1955) became the standard surgical approach
- Laparoscopic techniques for fundoplication were introduced in the early 1990s
- Magnetic sphincter augmentation (LINX device) was FDA-approved in 2012
Endoscopic Therapies:
- Endoscopic suturing and plication techniques emerged in the early 2000s
- Radiofrequency treatment of the LES (Stretta procedure) was developed in 2000
- Transoral incisionless fundoplication was introduced in the late 2000s
Evolution of Medical Understanding
The conceptualization of GERD has evolved significantly over the past century:
1930s-1950s: Mechanical Disease
- GERD viewed primarily as a mechanical failure of the gastroesophageal junction
- Focus on hiatal hernia as the predominant cause
- Treatment directed at anatomical correction through surgery
1960s-1970s: Acid-Driven Pathology
- Recognition of LES dysfunction as central to pathophysiology
- Understanding of the damaging effects of acid on esophageal mucosa
- Introduction of acid suppression as a primary treatment strategy
1980s-1990s: Multifactorial Disorder
- Recognition of multiple contributing factors:
- Transient LES relaxations
- Delayed gastric emptying
- Impaired esophageal clearance
- Hiatal hernia
- Reduced tissue resistance
- Development of the concept of “reflux disease spectrum”
2000s-Present: Heterogeneous Condition with Distinct Phenotypes
- Recognition of NERD as distinct from erosive esophagitis
- Identification of extraesophageal manifestations as part of the GERD spectrum
- Understanding of the role of non-acid reflux
- Recognition of functional heartburn as separate from GERD
- Appreciation for the overlap with other functional GI disorders
- Growing recognition of the gut-brain axis in symptom perception
Current Paradigm:
- GERD understood as a complex, chronic condition with multiple contributing factors
- Growing recognition of individual variations in presentation and response to treatment
- Movement toward personalized approaches based on specific patient characteristics
- Increasing emphasis on quality of life impacts and patient-reported outcomes
- Broader understanding of the potential consequences, including esophageal cancer risk
This evolution in understanding has transformed GERD from a condition requiring primarily surgical management to one with multiple treatment options based on disease phenotype, severity, and individual patient factors. The current approach recognizes GERD as a lifelong condition that requires tailored management strategies and, in many cases, ongoing therapy.
3. Symptoms
Early Symptoms
The initial manifestations of GERD typically involve a characteristic set of symptoms, primarily related to the esophagus, though they can vary significantly between individuals:
Classic Early Esophageal Symptoms:
Heartburn (Pyrosis):
- Burning sensation behind the breastbone (retrosternal)
- Typically worse after meals, when lying down, or bending over
- Often radiates upward toward the throat
- Usually relieved temporarily by antacids
- Affects approximately 60-75% of GERD patients
Regurgitation:
- Effortless return of gastric contents into the throat or mouth
- Sour or bitter taste in the back of the throat
- May occur without nausea or retching
- Sometimes experienced as a “wet burp”
- Affects 40-65% of GERD patients
Dyspepsia:
- Upper abdominal discomfort or pain
- Feeling of fullness or bloating after eating
- Often confused with indigestion
- May accompany heartburn or present independently
- Present in 30-50% of patients with GERD
Early Extraesophageal Symptoms:
Throat Symptoms:
- Frequent throat clearing
- Sensation of a lump in the throat (globus sensation)
- Mild hoarseness, particularly in the morning
- Sore or irritated throat without apparent cause
Respiratory Symptoms:
- Occasional coughing, particularly after meals or at night
- Mild wheezing
- Subtle voice changes
Oral Symptoms:
- Morning bad breath (halitosis)
- Mildly sour taste in the mouth
- Increased salivation (water brash)
Temporal Pattern of Early Symptoms:
- Postprandial (after meals): Typically occur 30-60 minutes after eating
- Positional: Often triggered by lying down or bending forward
- Nocturnal: Commonly occur when recumbent, potentially disrupting sleep
- Intermittent: Initially may appear only occasionally, particularly after trigger foods
- Short-duration: Episodes typically last minutes to hours
- Self-limiting: Often resolve spontaneously or with over-the-counter remedies
Response to Modifying Factors:
- Relief with antacids within minutes (temporary)
- Worsening with large meals, fatty foods, alcohol, or coffee
- Improvement with upright posture
- Aggravation with tight clothing around the waist
Early GERD symptoms may be dismissed as occasional indigestion or normal digestive discomfort, leading to delays in seeking medical attention. Many individuals self-treat with over-the-counter medications for extended periods before consulting healthcare providers.
Advanced-Stage Symptoms
As GERD progresses, symptoms typically become more severe, frequent, and potentially include complications:
Progressive Esophageal Symptoms:
Intensified Heartburn:
- More frequent episodes (daily rather than occasional)
- Greater intensity and duration of burning
- Diminished response to over-the-counter remedies
- Nighttime symptoms disrupting sleep patterns
Dysphagia (Difficulty Swallowing):
- Initially with solid foods only
- Sensation of food “sticking” in chest
- Potentially progressing to difficulties with soft foods or liquids
- May indicate development of strictures or severe inflammation
- Affects 30-50% of patients with long-standing GERD
Odynophagia (Painful Swallowing):
- Sharp pain when swallowing
- May indicate ulceration or severe inflammation
- Often accompanies dysphagia
- Present in 15-25% of advanced cases
Persistent Regurgitation:
- More frequent and less related to position or meals
- May occur during sleep (nocturnal regurgitation)
- Potential for aspiration into lungs
- Less responsive to lifestyle modifications
Advanced Extraesophageal Manifestations:
Respiratory Complications:
- Chronic cough unresponsive to typical treatments
- Nocturnal asthma or worsening of existing asthma
- Recurrent bronchitis or pneumonia from aspiration
- Pulmonary fibrosis (rare but serious complication)
Otolaryngologic (ENT) Manifestations:
- Chronic laryngitis with persistent hoarseness
- Vocal cord granulomas or ulcerations
- Chronic sinusitis
- Otitis media (middle ear inflammation)
Dental Complications:
- Progressive enamel erosion, particularly on lingual surfaces
- Increased dental sensitivity
- Higher risk of caries (cavities)
- Periodontal disease exacerbation
Severe Throat Symptoms:
- Globus sensation becoming persistent rather than intermittent
- Frequent choking episodes, particularly at night
- Chronic sore throat resistant to typical treatments
Alarm/Warning Symptoms: These represent potentially serious developments requiring immediate evaluation:
- Dysphagia with progressive worsening
- Weight loss not attributable to other causes
- Hematemesis (vomiting blood)
- Melena (black, tarry stools indicating digested blood)
- Iron deficiency anemia
- Persistent vomiting
- Chest pain unresponsive to acid suppression (requires cardiac evaluation)
Sleep-Related Advanced Symptoms:
- Sleep fragmentation due to reflux events
- Nighttime choking or coughing episodes
- Morning hoarseness and throat pain
- Nocturnal chest pain awakening the patient
- Sleep apnea exacerbation
Advanced GERD symptoms often significantly impact quality of life, interfering with eating, sleeping, socializing, and working. The persistent nature of symptoms at this stage typically prompts medical attention if not sought earlier.
Common vs. Rare Symptoms
GERD presents with a spectrum of symptoms that vary in frequency among affected individuals:
Common Symptoms (Present in >30% of patients):
Heartburn:
- Affects 70-85% of GERD patients
- Cornerstone symptom for clinical diagnosis
- Most specific symptom for GERD
Regurgitation:
- Present in 50-70% of cases
- Highly specific for GERD when combined with heartburn
- Less responsive to acid suppression than heartburn
Dyspepsia:
- Occurs in 40-60% of patients
- Often overlaps with other functional gastrointestinal disorders
- Less specific for GERD
Chest Pain:
- Affects 30-50% of GERD patients
- May mimic cardiac pain (essential to exclude cardiac causes)
- Often described as pressure or squeezing rather than burning
Sleep Disruption:
- Reported by 40-60% of patients
- Particularly common in nocturnal GERD
- Manifests as difficulty falling asleep, frequent awakenings, or morning fatigue
Less Common Symptoms (Present in 10-30% of patients):
Chronic Cough:
- Present in 20-30% of GERD patients
- More common in non-erosive reflux disease
- Often lacks the typical esophageal symptoms
- May be the only manifestation of GERD in some patients
Dysphagia:
- Affects 20-30% of chronic GERD patients
- More common in erosive disease
- Increases in prevalence with disease duration
Hoarseness:
- Present in 15-25% of cases
- Typically worse in the morning
- Often misdiagnosed as allergic or viral laryngitis
Globus Sensation:
- Occurs in 15-25% of GERD patients
- Persistent feeling of a lump in the throat
- Not relieved by swallowing
Throat Clearing:
- Reported by 15-25% of patients
- Often habitual and unconscious
- Frequently misattributed to postnasal drip
Rare Symptoms (Present in <10% of patients):
Dental Erosions:
- Affect 5-10% of GERD patients
- More common in long-standing disease
- Often unrecognized until advanced
Otalgia (Ear Pain):
- Present in 3-8% of cases
- Referred pain via the vagus nerve
- Typically unilateral
Halitosis (Bad Breath):
- Reported in 5-10% of patients
- More common in those with significant regurgitation
- Often noticed by others rather than the patient
Waterbrash (Hypersalivation):
- Occurs in 5-10% of cases
- Sudden filling of the mouth with saliva
- Represents a vagal response to acid in the esophagus
Subxiphoid Pain:
- Reported by 3-5% of patients
- Sharp pain below the xiphoid process
- Often confused with gallbladder pain
Nausea Without Vomiting:
- Present in 5-7% of GERD patients
- More common in those with delayed gastric emptying
- Often morning-predominant
Laryngospasm:
- Affects 2-4% of patients
- Sudden, frightening inability to breathe or speak
- Typically occurs at night after reflux event
Atypical Presentations:
Silent Reflux (Laryngopharyngeal Reflux):
- Predominantly extraesophageal symptoms
- Minimal or absent heartburn/regurgitation
- Often misdiagnosed or treated as other ENT conditions
Cardiac-Predominant GERD:
- Primarily chest pain symptoms
- May be misdiagnosed as coronary disease
- Often refractory to typical GERD treatments
Respiratory-Predominant GERD:
- Primary manifestation as asthma, chronic cough, or recurrent pneumonia
- May lack typical reflux symptoms
- Often diagnosed after failure of standard respiratory treatments
The symptom profile of GERD is notably heterogeneous, with substantial overlap with other conditions. This diversity contributes to diagnostic challenges and treatment complexity.
Symptom Progression Over Time
GERD typically follows certain patterns of progression, though individual variations are common:
Typical Progression Timeline:
Initial Phase (Early GERD):
- Occasional postprandial heartburn (monthly to weekly)
- Symptoms primarily after trigger foods or large meals
- Good response to lifestyle modifications and over-the-counter remedies
- Minimal impact on quality of life
- Duration: Months to years
Established Phase (Developing GERD):
- Increased frequency of heartburn (weekly to several times weekly)
- Development of regurgitation symptoms
- Nighttime symptoms beginning to appear
- Decreased response to over-the-counter medications
- Beginning impact on meal choices and activities
- Duration: Often 1-5 years
Advanced Phase (Chronic GERD):
- Regular heartburn (daily or near-daily)
- Consistent regurgitation episodes
- Regular nighttime symptoms affecting sleep
- Development of extraesophageal manifestations
- Need for regular prescription medications
- Significant impact on quality of life
- Duration: Often >5 years if untreated
Complicated Phase:
- Development of GERD complications (Barrett’s esophagus, strictures)
- Potential emergence of alarm symptoms
- Refractory symptoms despite optimal medical therapy
- Significant life modifications required to manage symptoms
- Potential need for surgical intervention
Factors Affecting Progression Rate:
Treatment Factors:
- Appropriate medical therapy significantly slows or halts progression
- Compliance with lifestyle modifications affects trajectory
- Intermittent treatment may allow disease progression during untreated periods
Patient Factors:
- Age (faster progression in elderly patients)
- Comorbidities (especially obesity, diabetes)
- Pregnancy can accelerate symptoms temporarily
- Continued exposure to triggers accelerates progression
Anatomical Factors:
- Presence and size of hiatal hernia (larger hernias associate with faster progression)
- Baseline esophageal motility
- Gastric emptying rate
Genetic/Physiological Factors:
- Mucosal resistance characteristics
- Salivary production and buffering capacity
- Healing capacity and inflammatory response
Common Progression Patterns:
Gradual Linear Progression:
- Slow increase in symptom frequency and severity
- Typical pattern in majority of patients (60-70%)
- May accelerate with aging or weight gain
Stepwise Progression:
- Stable periods alternating with sudden symptom escalation
- Often associated with life events (stress, dietary changes)
- Present in approximately 15-20% of patients
Rapid Progression:
- Quick escalation from mild to severe symptoms
- More common in elderly patients
- Associated with large hiatal hernias
- Represents 5-10% of cases
Relapsing-Remitting Pattern:
- Periods of significant symptoms alternating with near-complete resolution
- Common in women with hormonal fluctuations
- Seen in 10-15% of patients
Plateau Pattern:
- Symptoms reach a certain level and remain stable for years
- More common with consistent treatment
- Approximately 20-30% of treated patients
Symptom Evolution Over Lifetime:
- Many patients experience onset in 30s-40s with gradual progression
- Pregnancy often triggers first significant GERD symptoms in women
- Middle age (40-60) typically represents period of symptom escalation
- Elderly patients often have more severe disease but sometimes decreased symptom perception
- Children may “grow out” of GERD as the lower esophageal sphincter matures
- Long-standing GERD can lead to complications even if symptoms improve (due to Barrett’s esophagus causing decreased sensation)
Understanding the typical progression patterns helps in patient education, treatment planning, and identification of individuals who may be experiencing atypical progression that warrants more aggressive evaluation or intervention.
4. Causes
Biological Causes
GERD develops from a complex interplay of functional and anatomical abnormalities affecting the gastroesophageal junction and surrounding structures:
Defects in the Anti-reflux Barrier:
Lower Esophageal Sphincter (LES) Dysfunction:
- Hypotensive LES: Reduced resting pressure (<10 mmHg) allowing easier reflux
- Transient LES Relaxations (TLESRs): Inappropriate spontaneous relaxations unrelated to swallowing
- Impaired LES response: Failure to contract in response to increased abdominal pressure
- Shortened LES: Reduced length of the high-pressure zone (<2 cm)
Hiatal Hernia:
- Type I (Sliding): Upper stomach and gastroesophageal junction slide into chest
- Types II-IV (Paraesophageal): Various forms where stomach herniates adjacent to esophagus
- Hernia disrupts the normal angle of His (angle between esophagus and fundus)
- Creates a pocket (“acid pocket”) where acid can pool and reflux
- Impairs the diaphragmatic pinchcock mechanism that normally assists the LES
Crural Diaphragm Dysfunction:
- Weakening of the diaphragmatic muscle fibers that normally reinforce the LES
- Widening of the esophageal hiatus
- Loss of synchronized contraction during respiration and abdominal strain
Esophageal Clearance Abnormalities:
Impaired Peristalsis:
- Weak or ineffective peristaltic waves
- Failed peristalsis (aperistalsis)
- Uncoordinated contractions
- Results in prolonged acid contact time with esophageal mucosa
Reduced Salivary Neutralization:
- Decreased salivary flow (in certain conditions or medications)
- Reduced bicarbonate content of saliva
- Impaired swallowing frequency during sleep
Gravity-Related Factors:
- Recumbent position eliminating gravity’s assistance in clearance
- Increased reflux during bent-over positions
Gastric Factors:
Delayed Gastric Emptying:
- Results in prolonged gastric distention
- Increases likelihood of TLESRs
- Creates pressure gradient favoring reflux
- Present in 15-30% of GERD patients
Increased Gastric Acid Production:
- Hypersecretory conditions (rare)
- Helicobacter pylori negative status (controversial role)
- Excessive meal-stimulated acid production
Altered Gastric Accommodation:
- Impaired fundic relaxation after meals
- Dysfunction of the gastric accommodation reflex
- Contributes to increased intragastric pressure
Tissue Resistance Factors:
Impaired Esophageal Mucosal Defense:
- Reduced epithelial cell junctional complexes
- Decreased epithelial cell bicarbonate secretion
- Impaired blood flow to esophageal mucosa
- Reduced epithelial cell repair mechanisms
Altered Esophageal Sensitivity:
- Hypersensitivity to normal amounts of acid
- Visceral hypersensitivity (increased pain perception)
- Altered esophageal nociception
Neural and Hormonal Factors:
Autonomic Nervous System Dysfunction:
- Altered vagal tone affecting LES pressure
- Sympathetic-parasympathetic imbalance
- Dysfunction of the enteric nervous system
Hormonal Influences:
- Progesterone effects relaxing smooth muscle (including LES)
- Estrogen modulation of esophageal sensitivity
- Cholecystokinin and other gut peptides affecting LES pressure
Genetic and Hereditary Factors
Genetic components play a significant role in GERD susceptibility, though specific gene associations are still being elucidated:
Familial Predisposition:
Family Clustering:
- First-degree relatives of GERD patients have 2-4 times higher risk
- Twin studies show 30-45% heritability for GERD symptoms
- Monozygotic twins show higher concordance than dizygotic twins
- Family history is a stronger predictor in younger-onset GERD
Inherited Anatomical Factors:
- Familial patterns of hiatal hernia
- Inherited connective tissue characteristics affecting diaphragmatic hiatus
- Familial patterns of esophageal anatomy
Specific Genetic Associations:
Directly Associated Genes:
- COL3A1: Collagen type III gene variants linked to hiatal hernia
- MHC/HLA region: Several variants associated with GERD and Barrett’s esophagus
- FOXF1: Transcription factor gene with variants linked to GERD susceptibility
- GNB3: G-protein subunit affecting smooth muscle tone
Genes Affecting Comorbid Conditions:
- FTO, MC4R: Obesity-related genes indirectly increasing GERD risk
- GABPB1, BARX1: Associated with both GERD and Barrett’s esophagus
Pharmacogenetic Factors:
- CYP2C19: Affects metabolism of proton pump inhibitors
- MDR1: Influences drug transport and effectiveness
Genetic Syndromes with GERD Component:
Connective Tissue Disorders:
- Ehlers-Danlos syndrome
- Marfan syndrome
- Scleroderma (systemic sclerosis)
Neurological/Developmental Disorders:
- Cerebral palsy
- Down syndrome
- Cornelia de Lange syndrome
Metabolic Disorders:
- Zellweger syndrome
- Mitochondrial disorders
Genetic Contribution to GERD Complications:
Barrett’s Esophagus and Esophageal Adenocarcinoma:
- Stronger genetic component than GERD alone
- Specific variants in p53 pathway genes
- Variants in genes controlling cell cycle and DNA repair
- 2-4 fold increased risk in first-degree relatives
Severity and Response to Treatment:
- Genetic factors influence symptom severity
- Hereditary factors in esophageal acid sensitivity
- Genetic contribution to healing capacity and complications
Environmental Causes and Triggers
Environmental factors play a crucial role both in triggering acute GERD episodes and in promoting chronic disease:
Dietary Factors:
Foods That Decrease LES Pressure:
- Chocolate (theobromine)
- Peppermint and spearmint
- High-fat meals
- Onions and garlic
- Coffee and caffeinated beverages
- Alcohol (particularly wine and beer)
Foods That Irritate the Esophageal Mucosa:
- Citrus fruits and juices
- Tomato-based products
- Spicy foods
- Carbonated beverages
- Very hot beverages and foods
Eating Patterns:
- Large meals causing gastric distention
- Eating close to bedtime
- Rapid eating with aerophagia (air swallowing)
- Irregular meal timing
Lifestyle and Behavioral Factors:
Body Position and Activity:
- Recumbent position, especially post-meal
- Bending over or stooping
- Exercises increasing intra-abdominal pressure (weightlifting, sit-ups)
- Tight clothing around the abdomen
Smoking:
- Decreases LES pressure
- Reduces salivary bicarbonate production
- Impairs esophageal clearance
- Increases acid secretion
- Associated with more severe esophagitis and complications
Sleep Factors:
- Sleep position (right side and prone positions increase reflux)
- Flat sleeping position without head elevation
- Short dinner-to-bed interval
- Sleep apnea with increased respiratory effort
Medication-Induced GERD:
Medications That Decrease LES Pressure:
- Calcium channel blockers
- Nitrates
- Anticholinergics
- Beta-agonists
- Theophylline
- Progesterones and estrogens
- Benzodiazepines
Medications That Irritate the Esophagus:
- Nonsteroidal anti-inflammatory drugs (NSAIDs)
- Aspirin
- Potassium supplements
- Bisphosphonates
- Tetracycline antibiotics
- Iron supplements
Medications Affecting Gastric Emptying:
- Opioids
- Anticholinergics
- Some antidepressants
- Dopamine agonists
Stress and Psychological Factors:
Acute Stress Response:
- Alters gastric acid production
- Affects gastric emptying
- Increases perception of symptoms
- Changes eating behaviors
Chronic Stress:
- Altered autonomic function affecting LES pressure
- Heightened visceral sensitivity
- Long-term changes in motility patterns
- Immune system effects on tissue healing
Psychological Comorbidities:
- Anxiety disorders
- Depression
- Somatization disorders
- Sleep disorders
Environmental Exposures:
Occupational Factors:
- Jobs requiring heavy lifting or bending
- Occupations with irregular meal timing
- Shift work disrupting digestive patterns
- Occupational stress
Air Quality:
- Air pollution exposure (may increase extraesophageal symptoms)
- Workplace chemical irritants affecting respiratory symptoms
- Second-hand smoke
Temporal Triggers:
Diurnal Variation:
- Nighttime reflux (absence of gravity, reduced swallowing)
- Postprandial periods (meal-stimulated acid)
- Early morning reflux (circadian rhythm of acid production)
Seasonal Factors:
- Holiday seasons with dietary changes
- Allergy seasons exacerbating extraesophageal symptoms
- Cold weather with increased comfort food consumption
Understanding these multifactorial causes and triggers is essential for developing comprehensive management strategies. While genetic factors create susceptibility, environmental and lifestyle factors often determine whether GERD symptoms manifest and their severity. This complex interplay explains why GERD requires individualized approaches to management addressing both inherent biological factors and modifiable environmental triggers.
5. Risk Factors
Demographic Risk Factors
Certain demographic characteristics are associated with increased GERD prevalence and severity:
Age-Related Factors:
Prevalence by Age Group:
- Infants: 10-20% experience regurgitation, typically resolving by age 1
- Children: 2-8% prevalence, increasing in recent decades
- Young adults (20-30): 10-15% prevalence
- Middle age (30-50): 15-20% prevalence
- Older adults (>65): 20-30% prevalence
Age-Related Changes Contributing to GERD:
- Decreased LES pressure with aging
- Reduced esophageal clearance mechanisms
- Increased prevalence of hiatal hernia (25% by age 50, 60% by age 80)
- Altered perception of symptoms (elderly may have more severe disease with fewer symptoms)
- Age-related changes in saliva production and composition
Age and GERD Complications:
- Barrett’s esophagus risk increases with age (peak at 50-70 years)
- Esophageal adenocarcinoma rare before age 40, peaks at 60-70 years
- Peptic strictures more common with longer-duration disease
Gender-Related Factors:
Prevalence Differences:
- Overall similar prevalence between men and women
- Women: More frequent heartburn and regurgitation symptoms
- Men: Higher rates of erosive esophagitis and complications
Gender-Specific Risk Patterns:
- Women: Higher prevalence during reproductive years
- Men: Higher prevalence after age 50
- Women: More likely to have non-erosive reflux disease
- Men: 2-3 times higher risk of Barrett’s esophagus and esophageal adenocarcinoma
Hormonal Influences:
- Pregnancy: 30-80% experience GERD symptoms, typically resolving post-partum
- Menopause: Often associated with worsening symptoms
- Oral contraceptives and hormone replacement therapy may affect symptoms
Ethnicity and Geographic Factors:
Ethnic Variations in Prevalence:
- Highest: Western populations (North America, Europe, Australia)
- Intermediate: South America, Middle East
- Lower: East Asian populations (though increasing rapidly)
- African Americans: Similar prevalence to whites but lower rates of Barrett’s esophagus
Regional Differences:
- North America: 18-28% prevalence
- Western Europe: 15-25% prevalence
- Eastern Europe: 10-15% prevalence
- Middle East: 12-25% prevalence
- East Asia: Traditionally 5-8%, now increasing to 10-15%
- South Asia: 8-15% prevalence
- Africa: Limited data, estimated 10-15% in urban areas
Migration Effects:
- Immigrants from low to high prevalence regions show increased GERD rates over time
- Second-generation immigrants typically adopt prevalence patterns similar to host country
- Suggests strong environmental contribution to ethnic differences
Socioeconomic Factors:
Education and Income:
- Mixed associations across different populations
- Higher socioeconomic status associated with increased prevalence in developing countries
- Lower socioeconomic status associated with more severe disease and complications in developed countries
Healthcare Access:
- Affects diagnosis rates and management
- Influences progression to complications
- Impacts availability of advanced treatments
Occupational Patterns:
- White-collar workers: Higher reported prevalence in some studies
- Manual laborers: Higher risk for certain occupations requiring bending/lifting
- Healthcare workers, particularly shift workers: Higher prevalence
Lifestyle and Environmental Risk Factors
Lifestyle choices significantly influence GERD risk and symptom severity:
Body Weight and Composition:
Obesity:
- BMI >30 increases GERD risk 1.5-3 fold
- Linear relationship between BMI and symptom frequency
- Central obesity (high waist-to-hip ratio) more strongly associated than BMI alone
- Mechanisms:
- Increased intra-abdominal pressure
- Increased frequency of TLESRs
- Altered gastric emptying
- Hiatal hernia promotion
- Inflammatory mediators from adipose tissue
Weight Changes:
- Weight gain: 3.5kg gain increases GERD risk by 15-40%
- Weight loss: 10% body weight reduction improves symptoms in 80% of patients
- Rapid weight fluctuations may worsen symptoms temporarily
Dietary Factors:
Dietary Patterns Associated with Increased Risk:
- Western diet (high fat, processed foods, low fiber)
- High meat consumption
- Large portion sizes
- Irregular meal timing
- Fast food frequency >2 times per week
Specific Food-Related Risks:
- High-fat diet increases risk by 30-50%
- Regular chocolate consumption: 35% increased risk
- Coffee: Dose-dependent risk (controversial, may affect only susceptible individuals)
- Carbonated beverages: 20-30% increased risk with daily consumption
- Spicy foods: Variable impact based on individual sensitivity
Dietary Protective Factors:
- High fiber intake associated with 20-30% risk reduction
- Mediterranean diet pattern shows protective effect
- Regular consumption of fruits and vegetables
- Adequate water intake between meals
Substance Use:
Tobacco:
- Current smoking increases GERD risk by 30-70%
- Dose-response relationship with pack-years
- Affects both symptom frequency and complication rates
- Mechanisms:
- Decreased LES pressure
- Reduced salivary bicarbonate
- Impaired esophageal clearance
- Delayed gastric emptying
Alcohol:
- Regular consumption (>7 drinks/week) increases risk by 25-40%
- Type matters: Wine and liquor stronger association than beer
- Binge drinking particularly problematic
- Mechanisms:
- Direct mucosal irritation
- LES pressure reduction
- Delayed gastric emptying
- Increased gastric acid production
Caffeine:
- Moderate association (controversial)
- More likely to exacerbate existing GERD than cause new-onset disease
- Individual susceptibility varies significantly
- Both caffeinated and decaffeinated coffee may trigger symptoms
Physical Activity and Sleep:
Exercise Patterns:
- Sedentary lifestyle increases risk by 20-50%
- Moderate exercise (30 minutes daily) protective for most
- High-intensity or high-impact exercise may trigger symptoms
- Exercises involving abdominal compression (weightlifting, crunches) increase risk
Sleep Factors:
- Sleep deprivation (<6 hours/night) associated with increased symptoms
- Right-side sleeping position increases reflux episodes
- Elevation of head during sleep reduces nocturnal symptoms
- Late-night eating (within 3 hours of bedtime) increases risk
Environmental Exposures:
Occupational Exposures:
- Jobs requiring heavy lifting or bending
- Occupations with exposure to respiratory irritants
- Shift work disrupting normal eating patterns
- High-stress occupations
Air Quality:
- Air pollution exposure associated with increased extraesophageal GERD
- Indoor air quality (mold, allergens) may worsen respiratory manifestations
- Occupational dust exposure linked to increased symptoms
Medical and Genetic Risk Factors
Various medical conditions and genetic factors influence GERD susceptibility:
Gastrointestinal Conditions:
Hiatal Hernia:
- Present in 80-90% of patients with severe GERD
- Size matters: Hernias >2cm associated with more severe disease
- Types:
- Type I (sliding): Most common, strongest GERD association
- Types II-IV (paraesophageal): Less common, variable GERD risk
Helicobacter pylori Status:
- Complex relationship:
- H. pylori negative status associated with increased GERD in some populations
- Eradication sometimes leads to worsening GERD symptoms
- Corpus-predominant H. pylori gastritis may protect against GERD
- Antral-predominant pattern may worsen GERD
- Complex relationship:
Other GI Disorders:
- Gastroparesis: 3-4 fold increased risk
- Irritable bowel syndrome: 30-50% have concurrent GERD
- Celiac disease: 30% increased prevalence of GERD
- Eosinophilic esophagitis: Often coexists with GERD
- Achalasia (after treatment): Iatrogenic GERD common
Respiratory Conditions:
Asthma:
- Bidirectional relationship:
- 50-90% of asthmatics have GERD
- GERD patients have 1.5x higher asthma risk
- Mechanisms:
- Bronchospasm triggered by acid reflux
- Asthma medications affecting LES pressure
- Increased pressure gradient due to respiratory mechanics
- Bidirectional relationship:
Chronic Obstructive Pulmonary Disease (COPD):
- 50-60% of COPD patients have GERD
- Severity correlates with GERD prevalence
- Smoking as common factor
- Respiratory medications affecting LES
- Altered breathing mechanics
Sleep Apnea:
- 60-80% of sleep apnea patients have GERD
- Severity of apnea correlates with GERD severity
- Mechanisms:
- Increased negative intrathoracic pressure during apneic episodes
- Obesity as common factor
- Arousal-related LES relaxation
Connective Tissue and Autoimmune Disorders:
Scleroderma:
- 80-90% have GERD
- Often severe and refractory to treatment
- Due to esophageal smooth muscle atrophy and fibrosis
Other Connective Tissue Disorders:
- Ehlers-Danlos syndrome: 50-60% prevalence
- Marfan syndrome: 60-70% prevalence
- Mixed connective tissue disease: 50-70% prevalence
Autoimmune Conditions:
- Sjögren’s syndrome: Reduced saliva affecting esophageal clearance
- Rheumatoid arthritis: Higher prevalence, partly medication-related
- Lupus: 30-50% prevalence
Neurological Conditions:
Neurodegenerative Disorders:
- Parkinson’s disease: 60-80% have GERD
- Multiple sclerosis: 30-40% prevalence
- ALS: Progressive dysphagia and GERD
- Dementia: Often unrecognized GERD due to reporting limitations
Developmental and Congenital Disorders:
- Cerebral palsy: 70-90% have GERD
- Down syndrome: 50-75% prevalence
- Intellectual disability: Often more severe GERD presentation
Endocrine and Metabolic Conditions:
Diabetes Mellitus:
- Type 1: 30-40% prevalence, often with gastroparesis
- Type 2: 25-35% prevalence, often with obesity as common factor
- Glycemic control correlated with symptom severity
Thyroid Disorders:
- Hypothyroidism: Delayed gastric emptying contributing to GERD
- Hyperthyroidism: Accelerated gastric emptying may worsen duodenogastric reflux
Metabolic Syndrome:
- 30-40% higher GERD risk
- Components additively increase risk (especially central obesity)
Medication-Related Risk:
High-Risk Medications:
- Anticholinergics: 2-3 fold increased risk
- Calcium channel blockers: 1.5-2 fold increased risk
- Nitrates: 1.5-2 fold increased risk
- Progesterone and estrogens: Particularly during pregnancy
Moderate-Risk Medications:
- NSAIDs (including aspirin): 1.2-1.5 fold increased risk
- Bisphosphonates: Direct esophageal irritation
- Tricyclic antidepressants: Effects on motility and sensation
- Opioids: Delayed gastric emptying
Impact of Pre-existing Conditions
Certain pre-existing conditions significantly modify GERD presentation, progression, and management:
Cardiovascular Disease:
Coronary Artery Disease:
- Symptom overlap creates diagnostic challenges
- Treatment considerations:
- Nitrates worsen GERD but needed for angina
- Aspirin increases risk of esophageal injury
- Proton pump inhibitor interactions with clopidogrel (controversial)
Heart Failure:
- 30-50% prevalence of GERD
- Mechanisms:
- Increased abdominal pressure from ascites
- Medications affecting LES
- Pulmonary congestion promoting reflux
- Management complexity with fluid status and medication interactions
Psychiatric Conditions:
Depression and Anxiety:
- Bidirectional relationship:
- 30-60% of GERD patients have psychological comorbidities
- Depression/anxiety associated with 1.5-2 fold increased GERD risk
- Mechanisms:
- Altered symptom perception and reporting
- Autonomic nervous system effects
- Medication effects
- Lifestyle factors (diet, sleep, smoking)
- Bidirectional relationship:
Post-Traumatic Stress Disorder:
- 50-60% GERD prevalence
- Particularly high in veterans
- Hyperarousal state affecting autonomic function
- Treatment often requires addressing both conditions
Pregnancy:
GERD in Pregnancy:
- First trimester: 22% prevalence
- Second trimester: 39% prevalence
- Third trimester: 60-72% prevalence
- Mechanisms:
- Progesterone effects on LES pressure
- Mechanical pressure from enlarging uterus
- Altered gastric emptying
- Changes in intra-abdominal pressure
Management Challenges:
- Medication safety concerns
- Limited treatment options
- Positional therapy difficulties
- Usually resolves postpartum, but may recur in subsequent pregnancies
Post-Surgical States:
After Bariatric Surgery:
- Sleeve gastrectomy often worsens GERD (30-60% new-onset or worsening)
- Roux-en-Y gastric bypass typically improves GERD
- Risk factors for post-bariatric GERD:
- Pre-existing GERD
- Hiatal hernia
- Surgical technique variations
After Other Abdominal Surgeries:
- Anti-reflux surgery: 10-30% failure or recurrence rate
- Esophagectomy: Nearly universal reflux symptoms
- Gastrectomy: Bile reflux common
- Lung transplantation: 75-90% develop GERD
Chronic Kidney Disease:
GERD in CKD:
- Stage 3-5 CKD: 30-50% GERD prevalence
- Dialysis patients: 40-60% prevalence
- Mechanisms:
- Delayed gastric emptying
- Medication effects
- Autonomic neuropathy
- Fluid status fluctuations
Treatment Considerations:
- Medication dosing adjustments
- Aluminum-containing antacids contraindicated
- Drug interactions with phosphate binders
Chronic Liver Disease:
GERD in Liver Disease:
- Cirrhosis: 30-70% prevalence
- Mechanisms:
- Ascites increasing intra-abdominal pressure
- Portal hypertension affecting esophageal vasculature
- Delayed gastric emptying
Special Considerations:
- Varices and GERD coexistence
- Bleeding risk with esophagitis
- Medication metabolism altered by liver dysfunction
Understanding these comprehensive risk factors is essential for identifying high-risk individuals, implementing preventive strategies, and developing targeted management approaches. The multiplicative effect of multiple risk factors explains the wide variability in GERD presentation and response to treatment among affected individuals.
6. Complications
Direct Complications of GERD
When left untreated or inadequately managed, GERD can lead to several significant complications affecting the esophagus and adjacent structures:
Esophageal Complications:
Erosive Esophagitis:
- Prevalence: Occurs in 30-40% of untreated GERD patients
- Pathophysiology: Acid exposure leading to inflammation and erosion of esophageal mucosa
- Classification: Graded using Los Angeles Classification (Grades A-D based on severity)
- Symptoms: Increased heartburn, pain, dysphagia, potential bleeding
- Outcomes: Typically heals with acid suppression but may recur when treatment stops
Peptic Stricture:
- Prevalence: Develops in 5-15% of chronic GERD patients
- Pathophysiology: Chronic inflammation leading to scarring and narrowing of the esophageal lumen
- Location: Most common in distal esophagus at gastroesophageal junction
- Symptoms: Progressive dysphagia, initially with solids then advancing to soft foods
- Complications: Food impaction, malnutrition, aspiration
- Management: Typically requires endoscopic dilation in addition to acid suppression
Barrett’s Esophagus:
- Prevalence: Develops in 5-15% of chronic GERD patients
- Pathophysiology: Metaplastic change from normal squamous epithelium to intestinal-type columnar epithelium
- Significance: Precancerous condition with 0.1-0.3% annual risk of progression to adenocarcinoma
- Risk Factors for Development: Long-standing GERD (>5 years), male gender, age >50, obesity, smoking
- Symptoms: May have reduced heartburn sensation compared to non-Barrett’s GERD
- Surveillance: Requires regular endoscopic monitoring (every 1-5 years depending on presence of dysplasia)
Esophageal Adenocarcinoma:
- Prevalence: 0.5-1% lifetime risk in chronic GERD patients; higher with Barrett’s
- Pathophysiology: Progression from metaplasia to low-grade dysplasia to high-grade dysplasia to cancer
- Risk Factors: Barrett’s esophagus, male gender, Caucasian race, obesity, smoking
- Symptoms: Progressive dysphagia, weight loss, anemia (often develops late)
- Prognosis: 5-year survival 15-20% overall; 80-90% if detected early
Esophageal Ulceration:
- Prevalence: 2-5% of chronic GERD patients
- Pathophysiology: Deep mucosal damage from prolonged acid exposure
- Complications: Bleeding, perforation (rare)
- Symptoms: Severe pain, hematemesis, melena
Extraesophageal Complications:
Respiratory Complications:
- Aspiration Pneumonia:
- Microaspiration of gastric contents into lungs
- More common in elderly, neurologically impaired
- Can be acute or chronic/recurrent
- Pulmonary Fibrosis:
- Chronic microaspiration leading to interstitial lung disease
- Often under-recognized etiology
- Typically in severe, longstanding GERD
- Bronchiectasis:
- Permanent enlargement of airways from chronic inflammation
- GERD is a contributing factor in 20-40% of cases
- Aspiration Pneumonia:
Otolaryngological Complications:
- Chronic Laryngitis:
- Inflammation of laryngeal structures from refluxate
- Manifests as chronic hoarseness, throat clearing
- Visible changes on laryngoscopy (posterior laryngitis, vocal cord erythema)
- Contact Ulcers and Granulomas:
- Focal ulcerative lesions on vocal processes
- Can cause significant voice changes
- May require surgical intervention in addition to GERD treatment
- Laryngeal/Subglottic Stenosis:
- Narrowing of the airway from chronic inflammation
- Can cause stridor, breathing difficulties
- May require procedural intervention
- Chronic Laryngitis:
Dental Complications:
Dental Erosion:
- Irreversible loss of tooth structure from acid exposure
- Typically affects lingual and palatal surfaces
- Prevalence: 10-42% of GERD patients
- Progressive nature can lead to significant dental problems
- Treatment includes addressing GERD plus dental restorations
Periodontal Disease:
- Higher prevalence in GERD
- Altered oral pH affecting gingival health
- May contribute to halitosis
Long-term Impact on Health
Chronic GERD affects multiple aspects of health beyond direct tissue damage:
Nutritional Impact:
Dietary Restriction:
- Self-limitation of food variety to avoid triggers
- Potential nutritional deficiencies from restricted diet
- Weight loss from food avoidance
- In severe cases, fear of eating (sitophobia)
Malabsorption:
- Occurs primarily with complicated GERD
- Strictures limiting nutritional intake
- Medication effects (PPIs reducing B12, calcium absorption)
Medication Interactions:
- Long-term PPI use affecting absorption of:
- Iron
- Calcium
- Magnesium
- Vitamin B12
- Various medications requiring acidic environment
- Long-term PPI use affecting absorption of:
Sleep-Related Health Effects:
Sleep Disturbances:
- 40-60% of GERD patients report sleep disruption
- Average sleep loss: 1-3 hours nightly in symptomatic patients
- Nocturnal reflux associated with longer acid clearance time
- REM sleep particularly affected
Consequences of Sleep Disruption:
- Daytime fatigue and decreased productivity
- Cognitive impairment
- Mood disturbances
- Increased accident risk
- Potential cardiovascular consequences of chronic sleep deprivation
Quality of Life Impact:
Physical Functioning:
- Activity limitation from symptoms
- Exercise avoidance due to symptom triggering
- Dietary and social restrictions
Psychological Impact:
- Anxiety about symptom occurrence
- Depression (2-3 times more common in GERD)
- Social isolation from dietary restrictions
- Intimacy issues from symptom concerns
Economic Impact:
- Work productivity loss: 6-10 hours weekly during symptom flares
- Absenteeism: 1-4 days monthly in severe cases
- Healthcare utilization costs
- Medication expenses
Medication-Related Long-term Effects:
PPI-Associated Concerns:
- Potential associations (most with weak evidence):
- Increased pneumonia risk (slight)
- Clostridium difficile infection risk
- Small intestinal bacterial overgrowth
- Osteoporosis and fracture risk
- Kidney disease (conflicting evidence)
- Dementia (inconsistent evidence)
- Micronutrient deficiencies
- Acid rebound upon discontinuation
- Potential associations (most with weak evidence):
Other Medication Effects:
- H2 receptor antagonist side effects with long-term use
- Antacid overuse consequences:
- Aluminum-containing: Constipation, phosphate depletion
- Magnesium-containing: Diarrhea, hypermagnesemia in renal insufficiency
- Calcium-containing: Hypercalcemia, rebound acid secretion
Potential Disability or Fatality Rates
While GERD itself rarely causes death directly, its complications can have serious consequences:
Morbidity and Disability:
Functional Disability:
- 10-15% of chronic GERD patients report significant limitation in daily activities
- 20-40% report moderate impact on work productivity
- Quality-adjusted life year (QALY) reduction of 0.05-0.1 per year of active disease
Chronic Pain Syndrome:
- Develops in 5-10% of patients with refractory symptoms
- Central sensitization contributing to persistent symptoms
- Often requires multimodal pain management approach
Psychological Disability:
- Anxiety disorders: 20-30% of chronic GERD patients
- Depression: 15-25% of chronic GERD patients
- Sleep disorders: 30-50% of chronic GERD patients
Esophageal Complication Outcomes:
Barrett’s Esophagus Progression:
- Annual risk of progression to cancer: 0.1-0.3% without dysplasia
- Annual risk with low-grade dysplasia: 0.5-1%
- Annual risk with high-grade dysplasia: 5-10%
- Surveillance reduces mortality by enabling early intervention
Esophageal Adenocarcinoma Outcomes:
- Overall 5-year survival: 15-20%
- Stage-specific survival:
- Stage I: 80-90%
- Stage II: 30-40%
- Stage III: 10-15%
- Stage IV: <5%
- GERD-associated adenocarcinoma accounts for approximately 10,000 deaths annually in the US
Stricture Complications:
- Recurrence after dilation: 30-40% within 1 year
- Perforation risk during dilation: 0.1-0.4%
- Aspiration risk: 5-10% in severe cases
- Malnutrition risk: 5-15% in elderly with severe strictures
Extraesophageal Complication Outcomes:
Respiratory Consequences:
- GERD-associated pneumonia mortality: 2-5 times higher in elderly
- GERD as exacerbating factor in:
- Asthma: Contributes to 15-20% of difficult-to-control cases
- COPD: Associated with more frequent exacerbations
- Pulmonary fibrosis: Associated with more rapid progression
Laryngeal Complications:
- Voice-dependent professionals: Career-threatening in 5-10%
- Laryngospasm: Rare but potentially serious with respiratory compromise
- Quality of life impact: Comparable to other chronic diseases
Mortality Considerations:
Direct Mortality:
- Esophageal adenocarcinoma: Primary cause of GERD-related death
- Esophageal perforation: Rare but carries 10-40% mortality
- Massive upper GI bleeding from severe erosive esophagitis: <0.01% of cases
Indirect Contribution to Mortality:
- Aspiration pneumonia: Significant contributor in elderly, neurologically impaired
- Medication complications: Rare but potentially serious
- Malnutrition from severe dysphagia: Particularly in elderly
Overall Mortality Impact:
- All-cause mortality: No significant increase with uncomplicated GERD
- Slight increase in mortality rates with Barrett’s esophagus (primarily from cancer risk)
- Statistically significant increase with severe complications (strictures, adenocarcinoma)
While GERD itself is rarely life-threatening, its complications can cause significant morbidity and, in the case of esophageal adenocarcinoma, substantial mortality. The chronic nature of GERD means that even moderate symptoms can have a cumulative negative impact on quality of life and functional status over time. Early intervention and appropriate management significantly reduce the risk of these serious complications.
7. Diagnosis & Testing
Clinical Evaluation
The diagnostic process for GERD begins with a thorough clinical assessment, which often provides sufficient information for a presumptive diagnosis:
History Taking:
Symptom Assessment:
- Characteristic symptoms: heartburn, regurgitation, chest pain
- Symptom frequency, severity, and duration
- Timing in relation to meals, position changes, and sleep
- Aggravating and alleviating factors
- Response to previous treatments, particularly acid suppression
- Impact on quality of life and daily functioning
GERD-Specific Questionnaires:
- GERD Questionnaire (GerdQ): 6-item validated tool with 80% sensitivity and specificity
- Reflux Disease Questionnaire (RDQ): 12-item assessment focusing on symptom frequency and severity
- GERD Impact Scale (GIS): Evaluates impact on daily activities
- ReQuest™: Comprehensive 67-item assessment of GERD symptoms
Alarm Features Requiring Urgent Evaluation:
- Dysphagia (difficulty swallowing)
- Odynophagia (painful swallowing)
- Weight loss
- Gastrointestinal bleeding (hematemesis, melena)
- Persistent vomiting
- Family history of esophageal or gastric cancer
- Anemia
- Age >50-55 years with new-onset symptoms
Extraesophageal Symptom Assessment:
- Chronic cough
- Hoarseness
- Throat clearing
- Globus sensation
- Dental erosions
- Asthma or wheezing
- Recurrent laryngitis
- Sleep disturbances
Physical Examination:
General Assessment:
- Vital signs: typically normal in uncomplicated GERD
- BMI: obesity as common associated factor
- Abdominal examination: epigastric tenderness in some patients
- Chest examination: to rule out cardiac or pulmonary causes
Focused Evaluations:
- Oral Examination: Evidence of dental erosion
- Neck Examination: Enlarged thyroid potentially affecting esophagus
- Respiratory Assessment: Wheezing or other signs of respiratory involvement
- Abdominal Examination: Epigastric tenderness, organomegaly, ascites
Yield of Physical Examination:
- Generally normal in uncomplicated GERD
- More valuable for identifying alternative diagnoses
- Signs of complications may be present in advanced disease
Empiric Diagnostic Trial:
Proton Pump Inhibitor (PPI) Trial:
- Standard approach: once or twice daily PPI for 2-4 weeks
- Positive response (symptom improvement ≥50%) supports GERD diagnosis
- Sensitivity: 75-90%, Specificity: 65-85%
- Advantages: therapeutic and diagnostic simultaneously
- Limitations: not specific for GERD; may miss NERD or refractory cases
Interpretation of Response:
- Complete response: strongly supports GERD diagnosis
- Partial response: suggests possible GERD plus other factors
- No response: suggests alternative diagnosis or refractory GERD
Structured Approaches:
- Symptom index: ratio of symptoms associated with reflux events
- Symptom association probability: statistical association between symptoms and reflux
Differential Diagnosis Considerations:
Cardiac Conditions:
- Coronary artery disease/angina
- Pericarditis
- Aortic dissection
Other Esophageal Disorders:
- Achalasia
- Esophageal spasm
- Eosinophilic esophagitis
- Infectious esophagitis
- Pill-induced esophagitis
Upper GI Disorders:
- Peptic ulcer disease
- Functional dyspepsia
- Gastroparesis
- Gallbladder disease
- Gastric or pancreatic malignancy
Miscellaneous Conditions:
- Medication side effects
- Functional heartburn
- Rumination syndrome
- Chest wall pain
- Psychiatric disorders (anxiety, somatization)
Diagnostic Tests
When clinical evaluation is insufficient or complications are suspected, various diagnostic tests can provide objective evidence of GERD:
Endoscopic Evaluation:
Upper Endoscopy (Esophagogastroduodenoscopy, EGD):
- Indications:
- Presence of alarm symptoms
- Persistent symptoms despite appropriate therapy
- Screening for Barrett’s esophagus in high-risk patients
- Evaluation before anti-reflux surgery
- Symptoms for >5 years
- Findings:
- Erosive esophagitis (30-40% of GERD patients)
- Barrett’s esophagus (5-15% of chronic GERD)
- Strictures or other complications
- Hiatal hernia
- Classification Systems:
- Los Angeles Classification for esophagitis (Grades A-D)
- Prague C&M Criteria for Barrett’s esophagus
- Limitations:
- Normal in 50-70% of symptomatic GERD patients (NERD)
- Not sensitive for diagnosis of uncomplicated GERD
- Limited correlation between endoscopic findings and symptom severity
- Indications:
Narrow Band Imaging (NBI) and Other Enhanced Imaging:
- Higher sensitivity for subtle mucosal changes
- Better characterization of Barrett’s esophagus
- Improved detection of dysplasia
- Limited additional value for standard GERD diagnosis
Endoscopic Ultrasonography (EUS):
- Not routine for GERD diagnosis
- Useful for evaluating Barrett’s-associated masses or nodules
- Staging of esophageal adenocarcinoma if present
Ambulatory Reflux Monitoring:
24-hour pH Monitoring:
- Technique: Transnasal catheter with distal pH sensor positioned 5cm above LES
- Parameters Measured:
- Acid exposure time (% time pH <4)
- Number of reflux episodes
- Longest reflux episode
- Symptom association with reflux events
- Indications:
- Persistent symptoms despite PPI therapy
- Atypical symptoms with uncertain diagnosis
- Before considering anti-reflux surgery
- Distinguishing GERD from functional heartburn
- Interpretation:
- Abnormal if acid exposure time >4-6% of total time
- Symptom association considered positive if symptom index >50%
- DeMeester score >14.7 considered abnormal (composite score)
- Limitations:
- Invasive, uncomfortable
- Cannot detect non-acid reflux
- May miss reflux in patients on acid suppression
Wireless pH Monitoring (Bravo):
- Technique: Capsule attached to esophageal mucosa during endoscopy
- Advantages:
- Greater patient tolerance
- Extended monitoring (48-96 hours)
- More normal activity and diet during testing
- Higher sensitivity due to longer monitoring
- Limitations:
- Requires endoscopy for placement
- Chest discomfort in 5-10% of patients
- Higher cost
- Cannot measure impedance
Combined pH-Impedance Monitoring:
- Technique: Multielectrode catheter measuring both pH and electrical impedance
- Parameters Measured:
- Acid reflux (pH <4)
- Weakly acidic reflux (pH 4-7)
- Non-acid reflux (pH >7)
- Height of refluxate
- Liquid vs. gas vs. mixed reflux
- Key Advantages:
- Detects all types of reflux regardless of pH
- Particularly useful for evaluating patients on PPI therapy
- Better correlation with symptoms in some patients
- Limitations:
- More complex interpretation
- Higher cost
- Limited standardization of normal values
Esophageal Function Testing:
High-Resolution Manometry:
- Technique: Pressure measurements throughout esophagus using closely spaced sensors
- Parameters Assessed:
- LES pressure and length
- Esophageal peristalsis
- Upper esophageal sphincter function
- Presence of hiatal hernia
- Role in GERD Diagnosis:
- Not primary diagnostic test for GERD
- Identifies contributing factors (weak LES, ineffective motility)
- Essential before anti-reflux surgery
- Helps exclude alternative diagnoses (achalasia, esophageal spasm)
- Findings in GERD:
- Hypotensive LES (<10 mmHg)
- Ineffective esophageal motility (30-50% of GERD patients)
- Increased transient LES relaxations
Barium Esophagography:
- Technique: Fluoroscopic imaging while patient swallows barium
- Utility:
- Evaluates esophageal morphology and motility
- Identifies hiatal hernia, strictures, rings
- Assesses emptying and clearance
- Role in GERD:
- Not sensitive for uncomplicated GERD diagnosis
- Useful for evaluating dysphagia
- Good for anatomical assessment before surgery
- May detect large volume reflux or delayed emptying
- Limitations:
- Poor sensitivity for mild-moderate GERD
- Cannot document acid exposure
- Limited correlation with symptoms
Biomarker and Novel Tests:
Salivary Pepsin:
- Non-invasive marker of reflux
- Simple collection via saliva sample
- Moderate sensitivity (60-80%) and specificity (60-70%)
- More studies needed for validation
Mucosal Impedance:
- Measures esophageal mucosal integrity
- Lower impedance indicates impaired mucosa from reflux
- Promising but not yet widely available
Histological Examination:
- Microscopic changes from biopsies
- Dilated intercellular spaces
- Basal cell hyperplasia
- Papillary elongation
- Limited specificity but may support diagnosis
Diagnostic Algorithms and Approaches
Various diagnostic strategies exist, depending on clinical presentation and available resources:
Initial Diagnostic Approach:
For Typical GERD Symptoms Without Alarm Features:
- Clinical diagnosis based on characteristic symptoms
- Empiric PPI trial (2-4 weeks)
- If good response: Confirm diagnosis and continue management
- If partial/no response: Proceed to further investigation
For Alarm Symptoms or Age >50-55 with New Symptoms:
- Prompt upper endoscopy
- Further testing based on endoscopic findings
- Consider alternative diagnoses
For Extraesophageal Symptoms:
- Rule out other causes specific to symptoms (ENT evaluation, pulmonary testing)
- Consider empiric PPI trial (often higher dose, longer duration)
- If no response: Reflux monitoring before attributing to GERD
Specialized Diagnostic Pathways:
Refractory GERD Evaluation:
- Confirm medication compliance
- Upper endoscopy (if not recently performed)
- pH or pH-impedance monitoring (preferably off PPI if possible)
- High-resolution manometry
- Consider functional esophageal disorders if negative evaluations
Pre-Surgical Evaluation:
- Upper endoscopy
- High-resolution manometry (essential)
- Reflux testing (pH or pH-impedance)
- Barium esophagography (in some centers)
- Gastric emptying study if gastroparesis suspected
Barrett’s Esophagus Screening:
- Endoscopy recommended for:
- Multiple risk factors (chronic GERD >5 years, male, age >50, obesity, smoking)
- Family history of Barrett’s or esophageal adenocarcinoma
- Systematic biopsies according to Seattle protocol
- Surveillance intervals based on dysplasia status
- Endoscopy recommended for:
Cost-Effective Diagnostic Strategies:
Step-up Approach:
- Begin with clinical evaluation and empiric therapy
- Progress to endoscopy if fails to respond
- Reserve functional testing for refractory cases
- Most cost-effective for typical presentations
Step-down Approach:
- Begin with comprehensive testing
- Particularly for atypical presentations
- Higher initial cost but may avoid prolonged empiric therapy
- May be more efficient for complex cases
Hybrid Approaches:
- Tailored to individual presentation and risk factors
- Consider health system resources and patient preferences
- Shared decision-making regarding extent of testing
Diagnostic Test Accuracy:
| Test | Sensitivity | Specificity | Best Use Case | Limitations |
|---|---|---|---|---|
| Symptom Assessment | 70-80% | 50-60% | Initial evaluation | Subjective, overlaps with other conditions |
| PPI Trial | 75-90% | 65-85% | Typical symptoms, therapeutic trial | Not specific, misses non-acid reflux |
| Endoscopy | 30-40% | 90-95% | Detecting complications, alternate diagnoses | Poor sensitivity for NERD |
| 24-hr pH Monitoring | 77-100% | 85-100% | Quantifying acid exposure | Invasive, misses non-acid reflux |
| Impedance-pH | 80-95% | 80-90% | Evaluating all reflux types, particularly on PPI | Complex interpretation, limited availability |
| Barium Study | 30-40% | 70-80% | Structural abnormalities, dysphagia | Poor for uncomplicated GERD |
| Manometry | N/A | N/A | Pre-surgical evaluation, ruling out motility disorders | Not primary GERD diagnostic test |
The diagnostic approach to GERD has evolved from primarily symptom-based to incorporating objective testing when needed. The choice of diagnostic tests should be individualized based on clinical presentation, available resources, and the specific diagnostic questions being addressed. While invasive testing is unnecessary for most patients with typical symptoms, it plays a crucial role in evaluating atypical presentations, refractory symptoms, and before considering surgical intervention.
8. Treatment Options
Standard Treatment Protocols
GERD management typically follows a stepwise approach, incorporating lifestyle modifications, medications, and in select cases, interventional procedures:
Step 1: Lifestyle and Dietary Modifications
These are recommended for all GERD patients regardless of severity:
Dietary Adjustments:
- Meal Pattern Modifications:
- Smaller, more frequent meals
- Avoiding eating within 3 hours of bedtime
- Slower eating with thorough chewing
- Food Triggers to Limit/Avoid:
- High-fat foods (fried foods, fatty meats, cream)
- Acidic foods (citrus, tomatoes)
- Spicy foods
- Chocolate
- Coffee and caffeinated beverages
- Carbonated beverages
- Alcohol, particularly wine and spirits
- Mint and peppermint
- Potentially Beneficial Foods:
- High-fiber foods
- Alkaline foods (bananas, melons, oatmeal)
- Protein-rich, low-fat foods
- Non-citrus fruits and vegetables
- Meal Pattern Modifications:
Position and Posture Adjustments:
- Sleep Positioning:
- Head of bed elevation (6-8 inches)
- Left side sleeping position
- Avoiding right-side or prone positioning
- Daytime Posture:
- Avoiding prolonged stooping or bending
- Maintaining upright posture after meals
- Loose clothing around abdomen
- Activity Timing:
- Avoiding exercise within 2 hours after eating
- Avoiding positions that increase abdominal pressure
- Sleep Positioning:
Weight Management:
- Goal of BMI <25 if overweight/obese
- Even 5-10% weight loss can significantly improve symptoms
- Combination of dietary changes and physical activity
Smoking Cessation:
- Complete cessation rather than reduction
- Multiple mechanisms of benefit for GERD
- May require formal smoking cessation program
Efficacy of Lifestyle Modifications:
- Varies significantly between individuals
- Most effective for mild to moderate symptoms
- Often insufficient as sole therapy for severe GERD
- Better outcomes when multiple modifications implemented simultaneously
- Critical for long-term management even with medication
Step 2: Over-the-Counter Medications
For mild or intermittent symptoms:
Antacids:
- Mechanism: Neutralize stomach acid
- Examples: Calcium carbonate, aluminum hydroxide, magnesium hydroxide
- Dosing: As needed for symptom relief
- Benefits: Rapid onset (5-15 minutes), generally safe
- Limitations: Short duration (30-60 minutes), limited efficacy for severe symptoms
- Side effects: Constipation (aluminum/calcium), diarrhea (magnesium), potential for drug interactions
H2 Receptor Antagonists (H2RAs):
- Mechanism: Block histamine receptors that stimulate acid production
- Examples: Famotidine, cimetidine, ranitidine (withdrawn in many markets)
- Dosing: Once or twice daily
- Benefits: Longer action than antacids (6-10 hours), moderate efficacy
- Limitations: Tachyphylaxis (decreased effectiveness over time), less potent than PPIs
- Side effects: Generally well tolerated; potential for headache, dizziness, drug interactions (particularly cimetidine)
Over-the-Counter PPIs:
- Mechanism: Block proton pump in gastric parietal cells
- Examples: Omeprazole, lansoprazole, esomeprazole (lower dose than prescription)
- Dosing: Once daily, 30-60 minutes before first meal
- Benefits: More effective acid suppression than H2RAs
- Limitations: Slower onset (1-4 days for full effect), limited duration of approved use without medical supervision
- Side effects: Similar to prescription PPIs but lower risk due to shorter intended use
Combination Products:
- Antacid + H2RA combinations
- Antacid + alginate formulations (form physical barrier to reflux)
- Generally more effective than single agents
Step 3: Prescription Medications
For moderate to severe GERD or inadequate response to over-the-counter treatments:
Proton Pump Inhibitors (PPIs):
First-line therapy for erosive esophagitis and moderate-severe GERD
Mechanism: Irreversibly inhibit the H+/K+ ATPase pump in gastric parietal cells
Standard Agents:
- Omeprazole: 20-40mg daily
- Esomeprazole: 20-40mg daily
- Lansoprazole: 15-30mg daily
- Pantoprazole: 20-40mg daily
- Rabeprazole: 20mg daily
- Dexlansoprazole: 30-60mg daily
Dosing Strategies:
- Standard: Once daily, 30-60 minutes before breakfast
- Twice daily: For severe or nocturnal symptoms
- “On-demand” therapy: For intermittent symptoms after initial healing
Efficacy:
- Heartburn relief in 70-80% of patients
- Healing of erosive esophagitis in 80-90% after 8 weeks
- Superior to all other medical therapies
Long-term Considerations:
- Safety concerns with prolonged use (>1 year):
- Potential increased risk of fractures
- Vitamin B12 and magnesium deficiency
- Increased risk of C. difficile and other enteric infections
- Potential interaction with clopidogrel (controversial)
- PPI deprescription strategies for long-term users
- Lowest effective dose for maintenance
- Safety concerns with prolonged use (>1 year):
Prokinetic Agents:
Mechanism: Enhance gastric emptying and esophageal clearance
Available Agents:
- Metoclopramide: 10mg before meals and bedtime (limited by neurological side effects)
- Domperidone: 10mg before meals (not available in US, limited cardiac concerns)
- Prucalopride: 1-2mg daily (newer agent with fewer side effects)
Role in GERD Management:
- Adjunctive therapy to acid suppression
- Particularly useful for delayed gastric emptying
- Limited by side effects and modest efficacy alone
Side Effect Concerns:
- Metoclopramide: Tardive dyskinesia with long-term use (FDA black box warning)
- Domperidone: QT prolongation
- Generally not recommended as monotherapy
Baclofen:
- Mechanism: Reduces transient LES relaxations (TLESRs)
- Dosing: 5-20mg three times daily
- Benefits: Particularly helpful for refractory regurgitation
- Limitations: Neurological side effects (drowsiness, dizziness)
- Role: Third-line therapy for selected patients not responding to standard approaches
Sucralfate:
- Mechanism: Forms protective barrier on damaged mucosa
- Dosing: 1g four times daily
- Benefits: Local action with minimal systemic absorption
- Role: Alternative for patients who cannot take acid suppressants
- Limitations: Multiple daily dosing, poor symptom control alone
Step 4: Combination Therapies for Refractory GERD
For the 10-40% of patients with incomplete response to standard PPI therapy:
Optimization Strategies:
- Split-dose PPI (twice daily before meals)
- Adding bedtime H2RA for nocturnal symptoms
- Addition of alginate-based preparations
- Combining PPI with prokinetic agent
- Adding baclofen for regurgitation-predominant symptoms
Considerations for Refractory GERD:
- Confirm compliance with medication and lifestyle measures
- Rule out alternate diagnoses (eosinophilic esophagitis, achalasia)
- Consider functional esophageal disorders
- Investigate for delayed gastric emptying
- Consider surgical or endoscopic interventions
Surgical and Interventional Therapies
For select patients with proven GERD who have incomplete response to medical therapy or prefer a non-pharmacological approach:
Surgical Approaches:
Laparoscopic Fundoplication:
- Gold standard surgical intervention
- Technique: Wrapping the gastric fundus around the lower esophagus
- Types:
- Nissen (360° wrap) – most common
- Toupet (270° partial posterior wrap)
- Dor (180-200° anterior wrap)
- Ideal Candidates:
- Documented GERD (abnormal pH study)
- Good response to PPI therapy
- Normal esophageal motility (for Nissen)
- Young patients facing lifetime of medication
- Large hiatal hernia
- Outcomes:
- 85-90% satisfaction at 5 years
- 70-75% satisfaction at 10 years
- 80-85% can discontinue PPI therapy
- Potential Complications:
- Dysphagia (10-15%, usually transient)
- Gas-bloat syndrome (5-15%)
- Inability to belch or vomit
- Wrap herniation or disruption (5-10% over time)
- Reoperation rate: 3-6% at 5 years
Magnetic Sphincter Augmentation (LINX):
Technique: Placement of magnetic beads around lower esophagus
Mechanism: Beads separate to allow food passage but prevent reflux
Advantages:
- Less anatomic alteration than fundoplication
- Preserves ability to belch and vomit
- Shorter procedure with faster recovery
- Lower rate of gas-bloat syndrome
Limitations:
- Contraindicated in MRI need or metal allergies
- Less data on long-term outcomes
- Not suitable for large hiatal hernias (>3cm)
- Device erosion risk (rare)
Outcomes:
- 80-85% able to discontinue PPI therapy
- 85-90% satisfaction at 3-5 years
- 5-10% removal rate within 5 years
Roux-en-Y Gastric Bypass:
- Primary bariatric procedure that also treats GERD
- Particularly effective for obese patients with GERD
- Superior GERD control compared to sleeve gastrectomy
- 80-90% resolution of GERD symptoms
Endoscopic Approaches:
Transoral Incisionless Fundoplication (TIF):
Technique: Endoscopic creation of a partial fundoplication
Mechanism: Recreates anti-reflux barrier without incisions
Advantages:
- Outpatient procedure
- No external incisions
- Fewer side effects than surgical fundoplication
Limitations:
- Less effective than surgical fundoplication
- Not suitable for large hiatal hernias
- Limited long-term data
Outcomes:
- 60-70% able to discontinue PPI therapy
- 70-75% satisfaction at 3 years
- 10-15% may require revision or conversion to surgery
Radiofrequency Treatment (Stretta):
Technique: Delivery of radiofrequency energy to LES
Mechanism: Stimulates collagen deposition and LES remodeling
Candidates:
- Uncomplicated GERD with incomplete PPI response
- BMI <35
- No significant hiatal hernia
Outcomes:
- Modest efficacy: 50-60% improvement in symptoms
- 40-50% able to discontinue PPI therapy
- Multiple treatments sometimes needed
- Minimal side effects or complications
Other Endoscopic Techniques:
- Medigus Ultrasonic Surgical Endostapler (MUSE)
- Anti-reflux mucosectomy (ARMS)
- Endoscopic suturing devices
- Injection of bulking agents
- Generally limited by insufficient long-term data and variable availability
Emerging Treatments and Clinical Trials
Several innovative approaches to GERD management are in various stages of development and clinical testing:
Novel Pharmacological Approaches:
Potassium-Competitive Acid Blockers (P-CABs):
- Mechanism: Reversible inhibition of the gastric H+/K+ ATPase
- Examples:
- Vonoprazan: Available in Asia, under FDA review in the US
- Tegoprazan: Available in South Korea
- Revaprazan: Available in limited markets
- Advantages:
- More rapid onset of action than PPIs (1-2 hours)
- More consistent 24-hour acid suppression
- No need for meal timing
- Effective regardless of CYP2C19 metabolizer status
- Clinical Data:
- Non-inferior or superior to PPIs for erosive esophagitis healing
- Potentially superior for severe (LA Grade C/D) esophagitis
- Effective for PPI-resistant GERD
- Status: Phase III trials completed for vonoprazan in US/Europe
TLESR-Targeting Medications:
- Novel GABA-B Agonists: Less CNS side effects than baclofen
- Metabotropic Glutamate Receptor 5 Antagonists:
- Reduce TLESRs without GABA-related side effects
- Several compounds in Phase II development
- Cannabinoid Receptor Modulators:
- Selective peripheral CB1 agonists
- Reduce TLESRs without psychoactive effects
- Early-stage clinical development
Esophageal Mucosal Protectants:
- Mucosa-Adherent Formulations:
- Novel bioadhesive formulations
- Provide physical protection from refluxate
- Examples: Esoxx, Giapza, Esolgafate
- Bile Acid Sequestrants:
- Target non-acid reflux components
- Particularly for bile reflux symptoms
- Under investigation for PPI-refractory GERD
- Mucosa-Adherent Formulations:
Novel Devices and Interventions:
Electrical Stimulation Therapy:
- Lower Esophageal Sphincter Stimulation:
- EndoStim device: Implantable LES stimulator
- Improves LES pressure and function
- Promising data from European trials
- Company currently restructuring after initial bankruptcy
- Vagal Nerve Stimulation:
- Modulates esophageal and gastric function
- Early trials showing symptom improvement
- Less invasive than traditional surgery
- Lower Esophageal Sphincter Stimulation:
Advanced Endoscopic Procedures:
- Antireflux Mucosectomy (ARMS):
- Gastric cardia mucosectomy to induce scarring and reduce reflux
- Promising data from Asian centers
- Less invasive than fundoplication
- Ultrasonic Esophageal Sphincter Augmentation:
- MUSE system: Ultrasound-guided full-thickness plication
- Outpatient procedure with minimal side effects
- FDA approved but limited adoption
- Antireflux Mucosectomy (ARMS):
Novel Materials:
- Reflux Band (Reza Band):
- External neck device applying pressure to UES
- For extraesophageal GERD symptoms
- FDA cleared as non-invasive option
- Hydrogel Injections:
- Biocompatible materials to augment LES
- Adjustable and potentially reversible
- Early animal and human studies ongoing
- Reflux Band (Reza Band):
Personalized Medicine Approaches:
Pharmacogenomic Testing:
- CYP2C19 genotyping to guide PPI selection and dosing
- Identifies rapid metabolizers who need higher doses
- Growing evidence for clinical utility
Biomarker-Guided Therapy:
- Salivary pepsin levels to identify reflux phenotypes
- Bile acid measurement for duodenogastroesophageal reflux
- Impedance patterns to customize therapy
Comprehensive Phenotyping:
- Integration of clinical, endoscopic, physiologic, and molecular data
- Machine learning algorithms to predict treatment response
- Tailored therapy selection based on individual characteristics
Regenerative Medicine Approaches:
Cell Therapy:
- Autologous muscle cell injections into LES
- Preliminary studies show increased LES pressure
- Potential for long-term improvement
- Stem Cell Applications:
- Esophageal mucosal regeneration after injury
- Enhancement of barrier function
- Preclinical development stage
- Autologous muscle cell injections into LES
Tissue Engineering:
- Bioengineered LES constructs
- Scaffolds for esophageal repair after extensive damage
- Currently in preclinical testing
The management of GERD continues to evolve with greater recognition of disease heterogeneity and the need for personalized approaches. While acid suppression remains the cornerstone of therapy, emerging treatments targeting diverse mechanisms offer hope for patients with refractory symptoms or those seeking alternatives to lifelong medication or traditional surgery.
9. Prevention & Precautionary Measures
Primary Prevention Strategies
While GERD often cannot be completely prevented due to genetic and structural predispositions, several strategies can reduce the risk of developing the condition:
Lifestyle and Behavioral Approaches:
Weight Management:
- Maintaining Healthy BMI:
- Single most effective preventive measure
- Targeting BMI <25 kg/m²
- Preventing weight gain even if already overweight
- Weight Distribution:
- Reducing central adiposity particularly important
- Waist circumference targets:
- Men: <40 inches (102 cm)
- Women: <35 inches (88 cm)
- Sustainable Approaches:
- Focus on permanent lifestyle changes vs. crash diets
- Combined dietary modification and physical activity
- Regular monitoring and adjustments
- Maintaining Healthy BMI:
Dietary Habits:
- Meal Pattern Optimization:
- Smaller, more frequent meals to avoid gastric distension
- Regular meal timing to establish digestive rhythms
- Allowing 3-4 hours between last meal and bedtime
- Dietary Composition:
- Mediterranean diet pattern associated with lower GERD risk
- Higher fiber intake protective (25-30g daily)
- Lower fat consumption, particularly saturated fats
- Adequate but not excessive protein intake
- Food Choices:
- Minimizing known trigger foods before symptoms develop
- Limiting alcohol consumption (≤1 drink daily)
- Reducing caffeine intake
- Moderating spicy and acidic food consumption
- Meal Pattern Optimization:
Physical Activity:
- Beneficial Exercise Types:
- Regular moderate aerobic activity (150+ minutes weekly)
- Low-impact exercises less likely to trigger reflux
- Core strengthening without increasing intra-abdominal pressure
- Exercise Timing:
- Avoiding vigorous activity within 2 hours after eating
- Morning or midday exercise preferable to evening
- Positional Considerations:
- Avoiding exercises requiring prolonged bent-over positions
- Modifying activities that cause symptom provocation
- Beneficial Exercise Types:
Smoking Prevention and Cessation:
- Never starting smoking as primary prevention
- Complete cessation for current smokers
- Avoiding secondhand smoke exposure
- Utilizing cessation resources (nicotine replacement, counseling)
Environmental and Occupational Measures:
Sleep Hygiene and Positioning:
- Optimal Sleep Position:
- Left-side sleeping reduces reflux risk
- Head of bed elevation (6-8 inches) using bed risers
- Avoiding right-side and prone positions
- Sleep Timing:
- Consistent sleep schedule
- Adequate sleep duration (7-9 hours for adults)
- Allowing sufficient post-meal interval before lying down
- Optimal Sleep Position:
Clothing Choices:
- Avoiding tight clothing around abdomen and waist
- Choosing looser-fitting garments, particularly after meals
- Selecting lower-pressure waistbands
Occupational Considerations:
- Posture Management:
- Ergonomic workspace design
- Regular posture breaks if prolonged sitting required
- Avoiding prolonged bending or stooping
- Job Modification:
- Task rotation for jobs requiring positions that increase reflux
- Scheduled meal breaks away from workstation
- Stress management techniques in high-pressure occupations
- Posture Management:
Stress Management:
- Regular stress reduction practices (meditation, yoga, etc.)
- Cognitive behavioral techniques for stress-triggered GERD
- Adequate leisure and recovery time
Secondary Prevention Measures
For individuals already experiencing occasional reflux or those at high risk due to unavoidable factors (family history, certain medications, etc.):
Early Intervention Approaches:
Symptom Monitoring:
- Maintaining symptom diaries to identify patterns and triggers
- Tracking relationship between specific foods and symptoms
- Noting positional or activity-related symptom provocation
Incremental Dietary Modifications:
- Systematic Elimination:
- Temporary elimination of suspected trigger foods
- Methodical reintroduction to confirm associations
- Individualized restriction of confirmed triggers
- Timing Modifications:
- Adjusting meal size and frequency
- Redistributing daily caloric intake
- Implementing food-specific timing (e.g., caffeine only before noon)
- Systematic Elimination:
Proactive Medication Use:
- As-needed antacids before anticipated trigger situations
- Preplanned H2RA use before occasional dietary indiscretions
- Short courses of PPIs during high-risk periods (e.g., vacations with dietary changes)
Positional Therapy:
- Implementing positional modifications before symptoms become persistent
- Utilizing specialized pillows or wedges designed for reflux
- Practicing post-meal upright positioning
Risk Reduction for Those on Necessary Medications:
Medication Timing and Administration:
- Taking potentially refluxogenic medications with plenty of water
- Remaining upright for 30+ minutes after medication
- Separating refluxogenic medications from meals when possible
Medication Adjustments (with medical supervision):
- Using enteric-coated or delayed-release formulations
- Splitting doses to reduce peak irritation
- Exploring alternative medications with less GERD impact
Protective Approaches:
- Antacid administration before necessary NSAIDs
- Mucosa-protective agents with irritating medications
- Maintaining hydration with all medications
Pregnancy-Related GERD Prevention:
Anticipatory Guidance:
- Pre-pregnancy counseling about GERD risk
- Early implementation of preventive measures
- Education about safe management options
Progressive Interventions:
- Sequential approach as pregnancy advances:
- Initial dietary and positional modifications
- Adding approved antacids if needed
- H2RAs (except ranitidine) for persistent symptoms
- PPIs only if benefits outweigh risks
- Sequential approach as pregnancy advances:
Postpartum Planning:
- Gradual discontinuation of interventions after delivery
- Monitoring for symptom resolution
- Weight loss strategies if pregnancy weight retained
Prevention of Complications
For those with established GERD, preventing progression and complications becomes the focus:
Medical Management:
Optimizing Treatment Adherence:
- Patient education about medication timing and administration
- Simplifying regimens when possible
- Using technology (apps, reminders) to improve compliance
- Regular follow-up to assess effectiveness and adjust as needed
Appropriate Maintenance Therapy:
- Lowest effective dose of acid suppression
- Consideration of step-down approaches when possible
- Intermittent therapy for mild, intermittent symptoms
- Continuous therapy for severe, complicated GERD
Complication Surveillance:
- Barrett’s Esophagus Screening:
- Endoscopic evaluation for high-risk individuals
- Risk factors: chronic GERD (>5 years), male sex, age >50, obesity, smoking
- Surveillance intervals based on findings
- Structured Follow-up:
- Periodic reassessment of symptoms and treatment efficacy
- Evaluation of alarm symptoms if they develop
- Monitoring for medication side effects
- Barrett’s Esophagus Screening:
Lifestyle Reinforcement:
Sustained Weight Management:
- Long-term maintenance of weight loss achieved
- Regular physical activity program
- Ongoing dietary vigilance
Progressive Dietary Adherence:
- Moving from strict elimination to measured reintroduction
- Finding sustainable dietary patterns
- Balancing GERD control with quality of life
Sleep Position Maintenance:
- Consistent use of elevation strategies
- Proper pillow support for comfort and adherence
- Side-sleeping habit development
Special Populations:
Prevention in the Elderly:
- Medication review to minimize GERD-inducing drugs
- Swallowing evaluation if dysphagia present
- Fall risk assessment with elevation strategies
- Simplified dietary guidelines focusing on key triggers
Pediatric Considerations:
- Proper infant feeding and positioning techniques
- Thickened feeds for infants with significant regurgitation
- Educational support for school-age children with GERD
- Transition planning for adolescents managing their own condition
Occupational Modifications:
- Workplace accommodations for meal timing and space
- Adaptive equipment for jobs requiring bending/lifting
- Stress management programs in high-pressure environments
Preventive Screening
While no formal population-based screening program exists specifically for GERD, targeted screening approaches are recommended for high-risk individuals:
Risk-Based Approaches:
High-Risk Screening Categories:
- Chronic GERD symptoms (>5 years)
- Multiple risk factors for Barrett’s esophagus
- Family history of esophageal adenocarcinoma
- Alarm features with GERD symptoms
Recommended Screening Methods:
- Upper endoscopy with systematic biopsy protocol
- Newer technologies (narrow-band imaging, confocal microscopy) for improved detection
- Potentially non-endoscopic methods (Cytosponge) in development
Screening Intervals:
- Initial endoscopy for high-risk individuals
- Subsequent intervals based on findings:
- No Barrett’s: Generally no routine surveillance needed
- Barrett’s without dysplasia: Every 3-5 years
- Low-grade dysplasia: Every 6-12 months
- High-grade dysplasia: Consider eradication therapy
Effectiveness of Prevention Strategies:
Evidence for Primary Prevention:
- Weight loss: 50-80% symptom reduction with 10% weight loss
- Smoking cessation: 30-40% symptom improvement
- Head of bed elevation: 67% symptom reduction
- Combined lifestyle approaches: Up to 70% may avoid medication need
Evidence for Complication Prevention:
- Acid suppression: 80-90% reduction in esophagitis recurrence
- Barrett’s surveillance: 80-90% of detected cancers are early stage
- Anti-reflux surgery: May reduce, but not eliminate, cancer risk
- PPI therapy: May slow Barrett’s progression (controversial)
Cost-Effectiveness Considerations:
- Lifestyle modifications: Highly cost-effective, minimal risk
- Targeted screening: Cost-effective for highest risk groups
- Barrett’s surveillance: Cost-effective for certain populations
- General population screening: Not cost-effective given prevalence
The prevention of GERD and its complications requires a multifaceted approach combining lifestyle optimization, targeted medical therapy, and appropriate surveillance for those at highest risk. While complete prevention is not always possible, significant reduction in both incidence and complications can be achieved through systematic implementation of these strategies.
10. Global & Regional Statistics
Incidence and Prevalence Rates
GERD represents one of the most common gastrointestinal disorders globally, although with significant geographic variation:
Global Prevalence:
Worldwide Estimates:
- Overall global prevalence: 8-33% of adults
- Approximately 1 billion individuals affected worldwide
- Weekly symptom prevalence: 13% global average
- Daily symptom prevalence: 5% global average
Temporal Trends:
- Increasing prevalence in most regions over past 2-3 decades
- 30-50% increase in Western countries since the 1990s
- More dramatic increases (2-3 fold) in Asian countries
- Generally stable rates in recent years in North America and Europe
Age-Related Patterns:
- Peak incidence: 30-60 years
- Prevalence increased with age in most populations
- Pediatric GERD: 2-8% of children, higher in infants (up to 20% with regurgitation)
- Elderly prevalence (>65 years): 10-30% depending on region
Regional Prevalence Variations:
North America:
- United States: 18-28% prevalence
- Canada: 17-24% prevalence
- Higher rates in Midwestern and Southern states
- Slightly higher prevalence in Caucasian vs. non-Caucasian populations
Europe:
- Western Europe: 15-24% prevalence
- Highest: UK, Netherlands, Sweden (20-25%)
- Moderate: Germany, Spain, Italy (15-20%)
- Eastern Europe: 8-15% prevalence
- North-South gradient with higher rates in Northern countries
- Western Europe: 15-24% prevalence
Asia:
- Traditional low prevalence rapidly increasing
- East Asia:
- Japan: 6-10% (doubled in last 20 years)
- China: 5-17% (urban > rural)
- South Korea: 5-12%
- South Asia:
- India: 7-18% (higher in urban centers)
- Pakistan: 7-15%
- Bangladesh: 5-10%
- Southeast Asia: 6-10% overall
Middle East:
- High prevalence region: 12-25%
- Turkey: 20-25%
- Iran: 18-22%
- Saudi Arabia: 15-20%
- Higher rates than expected based on obesity prevalence
South America:
- Brazil: 12-21%
- Argentina: 16-24%
- Chile: 15-19%
- Significant urban-rural differences (urban 1.5-2x higher)
Africa:
- Limited data available
- Estimated ranges: 7-18%
- Urban centers: 12-18%
- Rural areas: 7-12%
- Nigeria: 9-15%
- South Africa: 12-15%
Australia/New Zealand:
- Australia: 18-23%
- New Zealand: 15-22%
- Similar patterns to Western Europe
Incidence Rates:
New Case Development:
- Annual incidence: 0.5-1% of population in Western countries
- Higher incidence in:
- Individuals with new-onset obesity
- Pregnancy (30-50% develop GERD)
- Following certain surgeries
Age-Specific Incidence:
- Highest in 30-40 year age group
- Second peak in elderly (>70 years)
- Pediatric incidence: 1-3 per 1000 children annually
Gender-Specific Incidence:
- Similar overall incidence between genders
- Slightly higher incidence in men over 50
- Higher incidence in women during reproductive years
Mortality and Morbidity
While GERD itself rarely causes death directly, its complications contribute to significant morbidity and occasional mortality:
Mortality Data:
Direct GERD-Related Mortality:
- Extremely low for uncomplicated GERD
- Primary mortality from complications:
- Esophageal adenocarcinoma: Approximately 16,000 deaths annually in the US
- Aspiration pneumonia: Significant contributor in elderly and neurologically impaired
- Hemorrhagic esophagitis: Rare but potentially fatal
Esophageal Adenocarcinoma Statistics:
- 5-year survival rates:
- Overall: 20-25%
- Localized disease: 45-50%
- Regional spread: 25-30%
- Distant metastasis: 5-8%
- GERD increases risk 5-7 fold
- Barrett’s esophagus increases risk 30-60 fold
- 5-year survival rates:
Procedure-Related Mortality:
- Anti-reflux surgery: 0.1-0.5% mortality
- Endoscopic complications: <0.01%
- Mortality higher in elderly and comorbid patients
Morbidity Measures:
Quality of Life Impact:
- Comparable to other chronic diseases (diabetes, heart failure)
- SF-36 scores show significant impairment across multiple domains
- Work productivity impacted in 30-50% of patients
- Sleep disturbance in 60-80% of patients with nocturnal symptoms
Healthcare Utilization:
- Outpatient visits: 4-5 million annually in the US
- Hospitalizations: 80,000-100,000 annually in the US for GERD and complications
- Medication use: PPIs among most commonly prescribed medications globally
- Diagnostic procedures: Millions of endoscopies performed annually for GERD
Economic Burden:
- Direct costs: $10-15 billion annually in the US
- Indirect costs: $75-100 billion annually worldwide
- Individual patient costs: $1,000-3,000 annually in the US
- Work absenteeism: 16 million days annually in the US
Complication Rates:
- Barrett’s esophagus: 5-15% of chronic GERD patients
- Erosive esophagitis: 30-40% of GERD patients at endoscopy
- Strictures: 5-15% of untreated chronic GERD
- Dental erosions: 10-30% of GERD patients
Regional Patterns and Trends
Several interesting patterns emerge when examining GERD on a global scale:
Geographic Variations:
Regional Phenotypes:
- Western pattern: Higher erosive esophagitis rates
- Asian pattern: Predominantly non-erosive disease
- Middle Eastern pattern: Higher extraesophageal manifestations
Symptom Differences:
- North American/European focus: Heartburn predominant
- Asian focus: Regurgitation and dyspeptic symptoms more common
- Latin American pattern: Mixed symptom profile
Complication Patterns:
- Highest adenocarcinoma rates: Northern Europe, North America
- Lowest adenocarcinoma rates: East Asia, Africa
- Barrett’s esophagus: Racial variations independent of GERD prevalence
Socioeconomic Influences:
Economic Development Correlation:
- Strong positive correlation with GDP per capita
- Rapid increases with Westernization and economic development
- Urban-rural divide in developing countries (2-3x higher in urban areas)
Access to Care Variations:
- Diagnostic rates vary by healthcare system accessibility
- Treatment patterns differ by economic status:
- High-income countries: High PPI use
- Middle-income: Mixed OTC and prescription approaches
- Low-income: Predominantly untreated or traditional remedies
Insurance and Coverage Impact:
- Countries with universal healthcare: Earlier diagnosis, more consistent treatment
- Countries with limited coverage: Higher complication rates, less optimal management
Temporal Trends:
Historical Progression:
- 1970s-1980s: Recognition as common disorder
- 1990s: Dramatic increase in Western countries
- 2000s: H2RA to PPI transition globally
- 2010s-present: Increasing awareness of PPI risks, emphasis on appropriate use
Recent Developments (2015-2025):
- Plateau in Western prevalence
- Continuing increase in developing regions
- Growth in minimally invasive treatment options
- Greater recognition of GERD heterogeneity
Projected Future Trends:
- Expected continued increase in developing countries
- Aging global population likely to increase overall prevalence
- Greater emphasis on non-pharmacological management
- Personalized medicine approaches becoming more widespread
Cultural and Dietary Influences:
Diet-Related Patterns:
- Mediterranean diet regions: Lower prevalence despite other risk factors
- High fast-food consumption regions: Higher prevalence
- Traditional East Asian diet: Historically protective, changing with Westernization
Lifestyle Factors:
- Work-stress correlation: Higher in countries with longer work hours
- Physical activity correlation: Lower in more physically active populations
- Smoking impact: Declining influence as smoking rates decrease
Cultural Healthcare Behaviors:
- Self-medication practices vary greatly by region
- Threshold for seeking medical care differs culturally
- Acceptance of long-term medication vs. surgical approaches
Special Population Considerations:
Pediatric GERD:
- Highest infant regurgitation rates: Western countries
- Cultural infant positioning differences affect prevalence
- Diagnosis rates vary by healthcare system
Pregnancy-Related GERD:
- Consistent 30-50% prevalence across regions
- Treatment approaches vary significantly by country
- Cultural practices during pregnancy influence management
Elderly Patterns:
- Highest prevalence in aging populations (Japan, Western Europe)
- Complication rates higher in regions with limited healthcare access
- Polypharmacy contributing to GERD more common in developed regions
Understanding these regional patterns and trends is essential for developing appropriate public health strategies, allocating healthcare resources, and identifying high-risk populations. The dramatic variations in GERD epidemiology around the world highlight the importance of environmental and lifestyle factors in this condition’s development and progression.
11. Recent Research & Future Prospects
Latest Advancements in Treatment and Research
Recent years have witnessed significant progress in understanding and managing GERD, with several key advancements:
Diagnostic Innovations:
Improved Reflux Monitoring:
- High-resolution impedance-pH monitoring:
- More precise characterization of reflux events
- Better correlation with symptoms
- Differentiation of acid vs. non-acid reflux
- Wireless pH capsule refinements:
- Extended monitoring duration (up to 96 hours)
- Improved attachment mechanisms reducing dislodgement
- Integration with smartphone technology for real-time monitoring
- High-resolution impedance-pH monitoring:
Novel Biomarker Approaches:
- Salivary pepsin testing:
- Point-of-care lateral flow devices (Peptest)
- Non-invasive screening tool for GERD
- Particularly useful for extraesophageal reflux
- Exhaled breath testing:
- Volatile organic compounds as GERD markers
- Electronic “nose” technology for pattern recognition
- Early research showing promising sensitivity/specificity
- Salivary pepsin testing:
Advanced Imaging:
- Confocal laser endomicroscopy:
- Real-time cellular visualization during endoscopy
- Detection of microscopic esophageal changes
- Improved Barrett’s esophagus assessment
- Functional lumen imaging probe (FLIP):
- Evaluates esophagogastric junction distensibility
- Helps predict response to interventions
- Guides selection of surgical candidates
- Confocal laser endomicroscopy:
Pharmacological Advancements:
Potassium-Competitive Acid Blockers (P-CABs):
- Vonoprazan:
- Rapidly becoming first-line therapy in Asian countries
- Superior acid suppression to PPIs
- Particularly effective for severe esophagitis
- FDA review for US approval underway
- Next-generation P-CABs:
- Improved pharmacokinetic profiles
- Reduced drug interaction potential
- Multiple compounds in clinical development
- Vonoprazan:
Reflux Inhibitors:
- Lesogaberan and other GABA-B agonists:
- Reduce transient LES relaxations
- Fewer central nervous system effects than baclofen
- Beneficial for regurgitation symptoms
- Metabotropic glutamate receptor 5 antagonists:
- Novel mechanism targeting TLESRs
- Several compounds in Phase II development
- Potential for combination with acid suppressants
- Lesogaberan and other GABA-B agonists:
Mucosal Protection Innovations:
- Bioadhesive formulations:
- Create protective barrier on esophageal mucosa
- Combined with acid neutralizing agents
- Examples: Esoxx, Giapza (alginate-hyaluronic acid combinations)
- Tissue restoration compounds:
- Promote mucosal healing and integrity
- Enhanced recovery of tight junctions
- Potential adjunct to standard therapy
- Bioadhesive formulations:
Surgical and Endoscopic Innovations:
Refinements in Laparoscopic Fundoplication:
- Tailored approach based on preoperative testing:
- High-resolution manometry guiding wrap type
- Impedance-pH patterns predicting response
- Individual anatomic considerations
- Technical improvements:
- Robot-assisted techniques improving precision
- Standardization of approach reducing complications
- Long-term outcome improvements
- Tailored approach based on preoperative testing:
Magnetic Sphincter Augmentation Advancements:
- LINX device refinements:
- Expanded sizing options for better fit
- Improved implantation techniques
- Wider patient selection criteria
- Long-term data emerging:
- 5+ year outcomes showing durability
- Lower rates of gas-bloat syndrome than fundoplication
- Preservation of ability to belch and vomit
- LINX device refinements:
Novel Endoscopic Approaches:
- Endoscopic sleeve gastroplasty:
- Simultaneous weight loss and GERD improvement
- Less invasive than bariatric surgery
- Emerging data showing promising results
- Antireflux mucosectomy (ARMS):
- Circumferential mucosectomy of gastric cardia
- Creates scarring to reduce reflux
- Primarily developed in Asian centers
- Endoscopic sleeve gastroplasty:
Basic Science Breakthroughs:
Genetic Understanding:
- Genome-wide association studies:
- Identification of genetic loci associated with GERD
- Overlap with genetic factors for Barrett’s esophagus
- Potential for risk stratification and personalized approaches
- Twin studies:
- Demonstrated 30-40% heritability of GERD
- Shared genetic factors with irritable bowel syndrome
- Epigenetic factors being elucidated
- Genome-wide association studies:
Microbiome Research:
- Esophageal microbiome characterization:
- Distinct patterns in GERD vs. healthy esophagus
- Changes preceding Barrett’s development
- Potential therapeutic target
- Oral microbiome connections:
- Correlations with extraesophageal symptoms
- Interaction with salivary components
- Modulation as potential therapy
- Esophageal microbiome characterization:
Neurogastroenterology Advances:
- Esophageal hypersensitivity mechanisms:
- Central and peripheral sensitization pathways
- TRPV1 receptor involvement
- Explanation for symptom-reflux discordance
- Brain-gut axis in GERD:
- Functional MRI studies showing central processing differences
- Stress-related autonomic influences
- Cognitive-behavioral therapy mechanisms
- Esophageal hypersensitivity mechanisms:
Ongoing Studies and Research Directions
Multiple research initiatives are currently exploring various aspects of GERD, potentially transforming future management:
Major Clinical Trials:
Pharmacological Studies:
- Vonoprazan trials:
- PHALCON-EE and PHALCON-HP trials
- Comparing vonoprazan to PPIs for erosive esophagitis
- Healing rates and maintenance of remission
- P-CAB combination studies:
- Adding prokinetics or mucosal protectants
- Targeting multiple pathophysiological mechanisms
- Potentially superior to acid suppression alone
- Vonoprazan trials:
Surgical Comparison Studies:
- CALIBER trial:
- Magnetic sphincter augmentation vs. fundoplication
- Patient-reported outcomes and objective measurements
- Cost-effectiveness analysis
- Endoscopic vs. Surgical approaches:
- TIF 2.0 procedure vs. laparoscopic fundoplication
- Less invasive options for appropriate candidates
- Quality of life and healthcare utilization outcomes
- CALIBER trial:
Barrett’s and Cancer Prevention Trials:
- Chemoprevention studies:
- PPIs, aspirin, and combination approaches
- Prevention of progression to dysplasia
- Long-term cancer prevention potential
- Screening modality trials:
- Non-endoscopic screening tools (Cytosponge, breath testing)
- Risk stratification approaches
- Cost-effectiveness of various strategies
- Chemoprevention studies:
Emerging Research Areas:
Precision Medicine Approaches:
- Phenotyping studies:
- Categorization of GERD into distinct subgroups
- Predictive models for treatment response
- Tailored therapeutic selection
- Pharmacogenomic research:
- Genetic determinants of medication response
- Metabolism variations affecting dosing
- Prediction of side effect risk
- Phenotyping studies:
Digital Health Applications:
- Remote monitoring systems:
- Wearable pH/impedance sensors
- Smartphone-connected symptom tracking
- AI algorithms for pattern recognition
- Digital therapeutic approaches:
- App-based cognitive behavioral therapy
- Digital lifestyle modification programs
- Virtual support communities
- Remote monitoring systems:
Regenerative Medicine:
- Stem cell approaches for LES dysfunction:
- Autologous muscle-derived stem cells
- Tissue engineering for sphincter reinforcement
- Early-stage animal and human studies
- Mucosal regeneration:
- Growth factors promoting barrier integrity
- Bioactive molecules enhancing healing
- Potential application in refractory GERD
- Stem cell approaches for LES dysfunction:
Collaborative Research Networks:
International GERD Consortia:
- Global GERD registry initiatives
- Standardized outcome measurements
- Pooling data across diverse populations
Multidisciplinary Research Teams:
- Integrating gastroenterology, surgery, pathology, and molecular biology
- Comprehensive approach to complex GERD questions
- Translational research from bench to bedside
Patient-Centered Research Networks:
- Incorporation of patient priorities in study design
- Patient-reported outcome measure development
- Involvement of patient advocates in research planning
Future Therapeutic Prospects
Several promising directions may transform GERD management in the coming decade:
Near-Horizon Developments (1-3 years):
New Medication Approvals:
- Vonoprazan and other P-CABs in Western markets
- Novel combination formulations
- Extended-release formulations of existing medications
Enhanced Diagnostic Algorithms:
- Integration of multiple testing modalities
- Symptom pattern recognition software
- More precise patient selection for interventions
Expanded Minimally Invasive Options:
- Wider adoption of magnetic sphincter augmentation
- Refinement of endoscopic therapies
- More targeted patient selection
Mid-Term Prospects (3-7 years):
Personalized GERD Medicine:
- Genetic testing to guide therapy selection
- Physiological phenotyping for intervention matching
- Predictive models for treatment response
Novel Therapeutic Targets:
- Esophageal barrier function modulators
- Sensory nerve modulating compounds
- Refluxate composition modification
Integration of Technology:
- Implantable monitoring systems
- On-demand therapy delivery systems
- Virtual reality for behavioral modification
Long-Term Possibilities (7-10+ years):
Curative Approaches:
- Gene therapy for LES dysfunction
- Bioengineered LES replacement
- Permanent restoration of antireflux barrier
Microbiome-Based Therapies:
- Esophageal microbiome modification
- Probiotic formulations for symptom reduction
- Metabolomic approaches targeting refluxate composition
Preventive Strategies:
- Early identification of high-risk individuals
- Pre-symptomatic intervention
- Population-level prevention programs
Potential Game-Changing Innovations:
Artificial Intelligence Applications:
- AI-driven diagnostic algorithms
- Automated image analysis during endoscopy
- Predictive modeling for disease progression
CRISPR and Gene Editing:
- Correction of genetic predisposition factors
- Modified cells for sphincter reinforcement
- Targeted mutation repair in Barrett’s esophagus
Drug Delivery Innovations:
- Esophageal-targeting formulations
- Extended-release implants
- Smart delivery systems responsive to pH changes
Neuromodulation Approaches:
- Targeted vagal nerve stimulation
- LES electrical stimulation refinements
- Central nervous system modulation for hypersensitivity
The future of GERD management is likely to be characterized by greater precision, less invasiveness, and more personalized approaches. As our understanding of the complex pathophysiology continues to evolve, therapeutic strategies will increasingly target specific mechanisms rather than employing the current one-size-fits-all approach. The integration of technology, pharmacology, endoscopic techniques, and potentially regenerative medicine promises to transform the landscape of GERD treatment in the coming decade.
12. Interesting Facts & Lesser-Known Insights
Uncommon Knowledge About GERD
Beyond the standard medical understanding, several fascinating and lesser-known aspects of GERD deserve attention:
Historical Perspectives:
Ancient Recognition:
- Egyptian papyri from 1550 BCE described what appears to be heartburn, recommending milk and herb mixtures
- Hippocrates (400 BCE) noted that “lying flat increases burning in the chest” and advised elevated sleeping
- Traditional Chinese Medicine texts described “stomach fire rising” with symptoms matching GERD
Presidential GERD:
- President Barack Obama underwent endoscopy in 2009 for GERD evaluation
- President Bill Clinton was known to have GERD and occasionally carried antacids
- These high-profile cases raised public awareness significantly
The PPI Revolution:
- The development of omeprazole in the 1980s was initially met with skepticism about the safety of profound acid suppression
- Became one of the most commercially successful drug classes in history
- Changed the paradigm from surgery to medical management as primary approach
Physiological Curiosities:
The “Acid Pocket”:
- After meals, a layer of highly acidic gastric juice floats on top of food in the stomach
- This “acid pocket” sits precisely at the gastroesophageal junction
- Makes postprandial period particularly vulnerable to acid reflux despite food buffering
- Discovered relatively recently (2001) and explains why reflux often worsens after meals
Salivary Protection:
- Humans produce 0.5-1.5 liters of saliva daily
- Contains bicarbonate that neutralizes refluxed acid
- Swallowing occurs 500-700 times during waking hours but only 5-10 times per hour during sleep
- Explains why nighttime reflux causes more damage
Supragastric Belching:
- Some GERD patients inadvertently suck air into the esophagus then immediately expel it
- This “supragastric belching” can occur hundreds of times daily
- Often mistaken for reflux but actually a behavioral pattern
- Can be effectively treated with speech therapy techniques
The Second Brain Connection:
- The enteric nervous system (“second brain”) contains 100 million neurons
- Independently regulates many digestive functions including LES pressure
- Explains why stress and psychological factors significantly impact GERD
- Target of emerging neuromodulation therapies
Clinical Pearls:
The Rogue’s Gallery of Medications:
- Over 80 common medications can trigger or worsen GERD
- Beyond the well-known culprits (NSAIDs, calcium channel blockers), surprising offenders include:
- Selective serotonin reuptake inhibitors (SSRIs)
- Some antibiotics (tetracyclines, clindamycin)
- Vitamin C supplements (ascorbic acid)
- Iron supplements
- Some asthma medications
The Silent Majority:
- Up to 40% of people with endoscopically proven GERD have no typical symptoms
- Called “silent refluxers” or having “atypical presentations”
- Often diagnosed only after complications develop
- May present only with extraesophageal manifestations
The Water Myth:
- Contrary to popular belief, drinking water with meals doesn’t worsen GERD
- May actually help by diluting stomach acid and aiding clearance
- Exception: Carbonated water can increase reflux events
- Room temperature water may be better than very cold water
The Left-Side Advantage:
- Sleeping on the left side reduces reflux episodes by 50-70% compared to right side
- Due to anatomical positioning of stomach junction below esophageal entry point
- One of the simplest yet most effective lifestyle interventions
- Ancient ayurvedic texts recommended this position thousands of years ago
Research Surprises:
The Helicobacter Paradox:
- H. pylori infection, which causes ulcers, may partially protect against GERD
- Eradication sometimes leads to new-onset or worsening GERD
- Declining H. pylori rates globally may contribute to rising GERD prevalence
- Demonstrates complex ecological relationship within the stomach
The Hiatal Hernia Controversy:
- Once considered the primary cause of GERD
- Then thought to be coincidental finding
- Now understood as important contributor but not necessary or sufficient
- Demonstrates evolution of medical understanding
The Barrett’s Protection Effect:
- Paradoxically, some patients develop less heartburn after developing Barrett’s esophagus
- The metaplastic tissue is less pain-sensitive than normal esophageal lining
- Can lead to dangerous delay in seeking care despite ongoing damage
- Underscores importance of continued monitoring despite symptom improvement
Myths and Misconceptions
Several persistent myths about GERD continue to influence public perception and sometimes management:
Myth 1: GERD is always caused by excess acid production. Reality: Most GERD patients produce normal amounts of acid. The problem is where the acid goes (reflux), not how much is produced. Mechanical factors like LES dysfunction and hiatal hernia play larger roles than acid hypersecretion in most cases.
Myth 2: Spicy foods cause GERD. Reality: While spicy foods can trigger symptoms in those who already have GERD, they don’t cause the underlying condition. Some spicy components like capsaicin may actually have beneficial effects on gastric emptying. Individual tolerance varies significantly.
Myth 3: GERD is just a nuisance, not a serious medical condition. Reality: Chronic GERD can lead to significant complications including Barrett’s esophagus, strictures, and esophageal adenocarcinoma. The quality of life impact rivals other chronic diseases like diabetes and heart failure.
Myth 4: Milk is a good remedy for heartburn. Reality: While milk temporarily buffers stomach acid, it subsequently stimulates acid production. The fat content can also delay gastric emptying and relax the LES, potentially worsening symptoms later.
Myth 5: GERD medications are completely safe for long-term use. Reality: While generally safe, long-term PPI use has been associated with several potential risks including vitamin/mineral malabsorption, increased fracture risk, and slightly higher rates of certain infections. Risk-benefit assessment is important for long-term users.
Myth 6: More acid suppression is always better. Reality: Complete acid suppression isn’t the goal and may have downsides. Some acid is necessary for digestion, pathogen defense, and nutrient absorption. The “minimal effective dose” approach is now preferred.
Myth 7: GERD always causes heartburn. Reality: Up to 40% of GERD patients don’t experience typical heartburn. Atypical symptoms like cough, hoarseness, or chest pain may be the only manifestations.
Myth 8: Surgery provides a permanent cure for GERD. Reality: While anti-reflux surgery can be very effective, 10-30% of patients experience symptom recurrence within 5-10 years. Some eventually return to medication use. Proper patient selection is critical for good outcomes.
Myth 9: GERD is an adult disease. Reality: GERD affects all age groups, including infants and children. Presentation may differ, with more regurgitation and respiratory symptoms in younger patients.
Myth 10: Acid reflux only damages the esophagus. Reality: Refluxed contents can damage the throat, larynx, respiratory tract, and even teeth. Microaspiration can contribute to lung disease, and dental erosion is a common manifestation.
Impact on Specific Populations
GERD affects certain populations in unique ways that deserve special attention:
Occupational Impacts:
Professional Voice Users:
- Prevalence: 30-50% of singers, teachers, call center workers, and public speakers
- Impact: Voice quality changes, vocal fatigue, career-threatening in severe cases
- Unique challenges: Performance anxiety increasing symptoms, limited medication timing around performances
- Management considerations: Specialized voice therapy, pre-performance protocols
Night Shift Workers:
- Prevalence: 1.5-2 times higher than day workers
- Mechanisms: Circadian disruption affecting gastric emptying and LES pressure
- Complications: More severe esophagitis due to sleeping during acid secretion peak
- Strategies: Specialized meal timing, sleep positioning, potentially different medication scheduling
Transportation Professionals:
- High-risk groups: Long-haul truck drivers, pilots, train engineers
- Contributing factors: Irregular meals, limited healthy options, sedentary periods
- Safety concerns: Chest pain causing distraction, sleep disruption affecting alertness
- Industry challenges: Limited access to consistent healthcare, diagnostic delays
First Responders:
- Prevalence factors: Irregular eating, stress, equipment pressure on abdomen
- Specific issues: Gear and equipment exacerbating symptoms, limited treatment options during shifts
- Diagnostic challenges: Distinguishing from cardiopulmonary conditions
- Intervention approaches: Adapted meal scheduling, modified equipment positioning
Special Clinical Populations:
Post-Bariatric Surgery Patients:
- Sleeve gastrectomy: 20-30% develop new-onset GERD
- Roux-en-Y gastric bypass: Often improves existing GERD
- Diagnostic challenges: Altered anatomy complicating endoscopy and pH testing
- Management complexities: Medication absorption issues, limited surgical options
Pregnant Women:
- Prevalence progression: First trimester: 22%, Second: 39%, Third: 72%
- Multiple mechanisms: Hormonal, mechanical, motility changes
- Treatment limitations: Safety concerns with medications
- Postpartum course: Resolves within 4-6 weeks in 70-80%
Cystic Fibrosis Patients:
- Prevalence: 50-90% have significant GERD
- Bidirectional relationship: GERD worsens pulmonary function, respiratory issues worsen GERD
- Treatment considerations: Medication interactions, aggressive management beneficial for lung function
- Unique features: Higher prevalence of bile reflux due to pancreatic insufficiency
Scleroderma Patients:
- Prevalence: 80-90% develop significant GERD
- Mechanism: Smooth muscle atrophy affecting both LES and esophageal clearance
- Severity: Often refractory to standard treatments
- Complication risk: Much higher rates of Barrett’s esophagus and strictures
Age-Specific Considerations:
Pediatric GERD:
- Infants: Peak regurgitation at 4 months, 60-70% resolve by 18 months
- Children: More respiratory manifestations than adults
- Adolescents: Adult-like presentation but often with atypical symptoms
- Growth concerns: Weight and height affected in severe cases
- Neurodevelopmental impact: Sleep disruption affecting learning and behavior
Elderly Patients:
- Presentation differences: Less typical heartburn, more complications at diagnosis
- Polypharmacy issues: Average elderly GERD patient on 5+ medications
- Comorbidity interactions: Particularly with heart disease, respiratory conditions
- Treatment considerations: Increased side effect risk, medication interactions
- Institutional challenges: High prevalence (40-50%) in nursing home settings
Cultural and Geographic Variations:
East Asian Perspectives:
- Traditional belief systems linking GERD to energy imbalances
- Higher prevalence of dyspeptic symptoms vs. classic heartburn
- Lower erosive esophagitis rates despite similar acid exposure
- Different treatment-seeking behaviors and medication adherence patterns
Middle Eastern Context:
- High prevalence despite different obesity patterns
- Ramadan fasting creating unique symptom patterns
- Specific dietary triggers (mint tea, specific spice combinations)
- Higher rates of extraesophageal manifestations in some populations
Western Diet Impact:
- Fast food frequency directly correlates with GERD severity
- Processed food consumption associated with earlier onset
- Ultra-processed food additives potentially affecting LES function
- Portion size contributing to gastric distension and mechanical factors
Understanding these population-specific aspects of GERD helps tailor management approaches to individual needs and circumstances. The remarkable variability in presentation, triggers, and optimal management strategies underscores the necessity of personalized approaches to this common but complex condition.