
⚠️ Disclaimer: The information provided in this article is for educational purposes only and does not constitute medical advice. RevisionTown does not provide diagnosis, treatment, or medical recommendations. Always consult a qualified healthcare professional regarding any medical condition, symptoms, or concerns.
Read More – 🏥 Medical Disclaimer
Comprehensive Report on Emphysema
1. Overview
What is Emphysema?
Emphysema is a chronic, progressive lung disease characterized by the destruction of alveolar walls and the abnormal, permanent enlargement of air spaces distal to the terminal bronchioles. This destruction results in decreased lung elasticity and reduced gas exchange capability, leading to air trapping and difficulty breathing.
Affected Body Parts/Organs
Emphysema primarily affects the respiratory system, with direct impact on:
- Lungs, particularly the alveoli (tiny air sacs where oxygen and carbon dioxide exchange takes place)
- Terminal bronchioles
- Pulmonary capillaries
- Respiratory muscles (including the diaphragm)
Secondary effects can impact:
- The heart (particularly the right ventricle)
- Systemic circulation
- Skeletal muscles (due to deconditioning and hypoxemia)
Prevalence and Significance
Emphysema is typically classified as a form of Chronic Obstructive Pulmonary Disease (COPD), alongside chronic bronchitis. Globally:
- An estimated 174 million people suffer from COPD, with emphysema comprising a significant portion
- In the United States, approximately 3.5 million people have been diagnosed with emphysema
- COPD (including emphysema) is the third leading cause of death worldwide, resulting in 3.23 million deaths in 2019
- The economic burden is substantial—in the U.S. alone, direct costs associated with COPD exceed $32 billion annually, with indirect costs adding billions more
- Emphysema contributes significantly to disability, reduced quality of life, and increased healthcare utilization across all demographic groups
2. History & Discoveries
First Identification
The history of emphysema’s recognition spans several centuries:
- Early descriptions of pulmonary emphysema appeared in medical literature as far back as the 17th century
- The term “emphysema” (from Greek, meaning “to inflate”) was first used to describe the lung condition in 1721 by Dutch anatomist Frederik Ruysch
Key Discoverers
Several key figures contributed to our understanding of emphysema:
- René Laënnec (1781-1826): Often credited with the first modern description of emphysema in 1819 in his treatise “De l’Auscultation Médiate.” He provided detailed pathological descriptions using his newly invented stethoscope.
- Matthew Baillie (1761-1823): Published early descriptions of emphysematous lungs in his “The Morbid Anatomy of Some of the Most Important Parts of the Human Body” (1793).
- J. B. Morgagni (1682-1771): Provided early anatomical descriptions of air-filled, enlarged lungs found during autopsies.
Major Breakthroughs
Several pivotal discoveries shaped our understanding and treatment of emphysema:
- 1950s: The association between smoking and emphysema was firmly established through epidemiological studies.
- 1963: The genetic basis for emphysema was discovered when Laurell and Eriksson identified alpha-1 antitrypsin deficiency.
- 1960s-1970s: The “protease-antiprotease” theory of emphysema pathogenesis was developed, explaining the mechanism of lung tissue destruction.
- 1970s: Development of controlled oxygen therapy for emphysema patients.
- 1980s: Introduction of modern bronchodilators and inhaled corticosteroids.
- 1990s: Development of lung volume reduction surgery techniques.
- 2000s: Validation of pulmonary rehabilitation as an essential component of emphysema management.
- 2010s: Implementation of endoscopic lung volume reduction techniques.
Evolution of Medical Understanding
Medical understanding of emphysema has evolved dramatically:
- Initially viewed simply as overinflated lungs with trapped air
- Progressed to recognizing the destructive nature of the disease with loss of alveolar walls
- Further developed to understand the inflammatory mechanisms and protease-antiprotease imbalance
- Modern understanding includes complex interactions between environmental exposures, genetic susceptibility, oxidative stress, chronic inflammation, and altered immune response
- Recognition of emphysema as a systemic disease with extrapulmonary manifestations, rather than purely a lung disorder
3. Symptoms
Early Symptoms
In its early stages, emphysema may present with subtle, often overlooked symptoms:
- Mild shortness of breath (dyspnea), initially only during physical exertion
- A chronic, mild cough (may be intermittent)
- Increased respiratory rate during activity
- Subtle decrease in exercise tolerance
- Occasionally morning headaches (due to mild CO₂ retention during sleep)
Advanced-Stage Symptoms
As emphysema progresses, symptoms become more severe and debilitating:
- Severe shortness of breath, even at rest
- Chronic cough, often with minimal sputum production
- Wheezing and chest tightness
- Barrel chest (increased anterior-posterior chest diameter)
- Use of accessory respiratory muscles
- Pursed-lip breathing
- Significant weight loss and cachexia
- Peripheral edema (due to right heart failure)
- Cyanosis (bluish discoloration of the lips and skin)
- Decreased mental alertness (from chronic hypoxemia and/or hypercapnia)
Common vs. Rare Symptoms
Common symptoms experienced by most patients include:
- Progressive dyspnea (shortness of breath)
- Reduced exercise capacity
- Fatigue and weakness
- Unintentional weight loss
Rarer symptoms that affect a smaller percentage of patients include:
- Spontaneous pneumothorax (collapsed lung)
- Hemoptysis (coughing up blood)
- Severe neck vein distention
- Asterixis (flapping tremor of the hands)
- Pulmonary hypertension symptoms
- Polycythemia (increased red blood cell count)
Symptom Progression
Emphysema typically follows a predictable progression pattern:
- Initial Phase: Minimal symptoms despite early lung changes; often undetected
- Early Disease: Mild dyspnea with exertion; symptoms often attributed to aging or deconditioning
- Moderate Disease: Noticeable dyspnea during everyday activities, chronic cough, beginning of activity limitation
- Advanced Disease: Severe dyspnea with minimal exertion, respiratory muscle fatigue, limited daily activities
- End-Stage Disease: Dyspnea at rest, severe limitation of activities, potential respiratory failure
This progression typically occurs over many years to decades, though rate of decline varies significantly between individuals based on continued exposures, genetics, and management.
4. Causes
Biological Causes
At the biological level, emphysema develops due to several interconnected processes:
- Protease-Antiprotease Imbalance: Excessive proteolytic enzyme activity (particularly elastase) overwhelms protective antiproteases, leading to destruction of lung elastin
- Oxidative Stress: Free radicals damage lung tissue and inactivate antiproteases
- Chronic Inflammation: Persistent inflammatory response with increased neutrophils, macrophages, and lymphocytes in the lungs
- Cellular Apoptosis: Programmed cell death of alveolar cells
- Ineffective Repair Mechanisms: Inadequate lung tissue repair after injury
- Accelerated Lung Aging: Telomere shortening and cellular senescence
Environmental Causes
Environmental factors represent the predominant causes of emphysema:
- Tobacco Smoke: By far the most significant cause, responsible for approximately 80-90% of emphysema cases
- Cigarette smoking (including secondhand exposure)
- Pipe and cigar smoking
- Marijuana smoking
- Air Pollution:
- Indoor air pollution (biomass fuel use, heating fuels)
- Outdoor air pollution (industrial emissions, traffic exhaust)
- Occupational Exposures:
- Coal dust
- Silica dust
- Cadmium and other heavy metals
- Chemical fumes
- Cotton dust
- Recurrent Respiratory Infections: Particularly during childhood
- Socioeconomic Factors: Poor housing conditions, inadequate ventilation, occupational hazards
Genetic and Hereditary Factors
Several genetic factors contribute to emphysema development:
- Alpha-1 Antitrypsin Deficiency: The most well-established genetic cause, responsible for about 1-2% of emphysema cases
- Autosomal recessive disorder
- Results in significantly reduced levels of alpha-1 antitrypsin, a key lung protector
- Often leads to early-onset emphysema, particularly in smokers
- Other Genetic Factors:
- Variations in genes controlling detoxifying enzymes (e.g., glutathione S-transferases)
- Polymorphisms in inflammatory mediator genes
- Variations in tissue repair genes
- Matrix metalloproteinase gene variants
- Telomere-related gene abnormalities
Known Triggers and Exposure Risks
Certain factors can trigger exacerbations or accelerate emphysema progression:
- Respiratory Infections: Viral and bacterial infections
- Air Pollution Episodes: Temporary spikes in particulate matter and other pollutants
- Allergen Exposure: In patients with co-existing allergic conditions
- Extreme Weather: Very cold air, high humidity, or extreme heat
- High Altitude: Reduced oxygen availability stresses compromised lungs
- Volatile Chemicals: Cleaning products, paints, solvents
- Smoke Exposure: Wildfires, industrial fires
- Comorbidities: Uncontrolled heart failure, pulmonary emboli, anemia
5. Risk Factors
Demographic Risk Factors
Certain demographic characteristics are associated with increased emphysema risk:
- Age: Risk increases with age; most diagnoses occur after age 40
- Sex: Historically more common in men, though female prevalence has increased significantly
- Race/Ethnicity:
- Higher rates observed in non-Hispanic whites and African Americans in the U.S.
- Lower rates in Asian populations
- Socioeconomic Status: Higher prevalence in lower socioeconomic groups
Lifestyle Risk Factors
Personal behaviors significantly influence emphysema risk:
- Smoking: The single most important risk factor
- Risk increases with both intensity (cigarettes per day) and duration
- Cumulative exposure measured in “pack-years” (packs per day × years smoked)
- Risk persists after cessation but declines over time
- Physical Inactivity: Associated with faster lung function decline
- Poor Nutrition: Vitamin deficiencies may increase susceptibility
- Alcohol Abuse: Associated with poorer outcomes and treatment compliance
Environmental and Occupational Factors
Environmental exposures contribute significantly to risk:
- Indoor Air Pollution:
- Biomass fuel use for cooking and heating (particularly in developing countries)
- Poor ventilation in homes
- Environmental tobacco smoke
- Outdoor Air Pollution:
- Industrial emissions
- Vehicle exhaust
- Particulate matter exposure
- Occupational Exposures:
- Mining (coal, silica)
- Textile industry
- Manufacturing with chemical exposures
- Agriculture (certain pesticides and organic dusts)
- Welding fumes
- Isocyanates and other industrial chemicals
Impact of Pre-existing Conditions
Several health conditions increase emphysema risk or accelerate its progression:
- Asthma: “Dutch hypothesis” suggests shared pathways with emphysema
- Chronic Bronchitis: Often co-exists with emphysema
- Recurrent Respiratory Infections: Particularly in childhood
- Tuberculosis: Prior infection increases risk
- HIV/AIDS: Associated with accelerated emphysema, even in non-smokers
- Connective Tissue Disorders: Certain disorders (e.g., Marfan syndrome, Ehlers-Danlos syndrome) associated with lung abnormalities
- Autoimmune Diseases: May increase risk through inflammatory pathways
6. Complications
Acute Complications
Emphysema can lead to several serious acute complications:
- Acute Exacerbations: Periods of significantly worsened symptoms, often triggered by infections
- Pneumothorax: Rupture of emphysematous bullae leading to lung collapse
- Respiratory Failure: Inability to maintain adequate gas exchange, requiring potential mechanical ventilation
- Pneumonia: Increased susceptibility to lung infections
- Pulmonary Embolism: Higher incidence due to immobility and inflammation
Chronic Complications
Long-term complications significantly impact quality of life and survival:
- Cor Pulmonale: Right-sided heart failure due to pulmonary hypertension
- Pulmonary Hypertension: Increased pressure in the pulmonary arteries
- Malnutrition and Weight Loss: Due to increased energy requirements and decreased intake
- Osteoporosis: Due to steroid treatment, vitamin D deficiency, and inactivity
- Sleep Disorders: Including sleep apnea and nocturnal oxygen desaturation
- Depression and Anxiety: Common psychological comorbidities
- Skeletal Muscle Dysfunction: Weakness and atrophy beyond what’s expected from deconditioning alone
- Pneumomediastinum: Air in the mediastinal space
- Giant Bullae: Large air spaces that can compress adjacent lung tissue
Long-term Impact on Organs and Systems
Emphysema affects multiple body systems beyond the lungs:
- Cardiovascular System: Increased cardiac workload, pulmonary hypertension, systemic inflammation
- Musculoskeletal System: Respiratory muscle remodeling, generalized muscle wasting
- Endocrine System: Metabolic abnormalities, diabetes risk with corticosteroid treatment
- Immune System: Altered immune response, increased infection risk
- Neurological System: Cognitive impairment due to chronic hypoxemia
- Gastrointestinal System: Reflux, altered nutritional status, liver abnormalities
- Renal System: Altered fluid balance, medication effects
Disability and Mortality
The impact on function and survival is substantial:
- Disability: Progressive decline in functional capacity
- 50-70% of patients report significant activity limitations
- Advanced disease often leads to dependency for activities of daily living
- Quality of Life: Significantly reduced across all dimensions
- Mortality: Major contributor to global mortality
- 5-year survival rates of approximately 50-60% with moderate to severe disease
- Mortality strongly correlates with:
- Degree of airflow limitation (FEV₁)
- Exercise capacity reduction
- Dyspnea severity
- Nutritional status
- Presence of pulmonary hypertension
- Frequency of exacerbations
7. Diagnosis & Testing
Initial Evaluation
The diagnostic journey typically begins with:
- Medical History: Detailed assessment of symptoms, exposures, family history
- Physical Examination: Looking for characteristic findings such as:
- Hyperinflated chest (“barrel chest”)
- Reduced breath sounds
- Prolonged expiration
- Use of accessory respiratory muscles
- Digital clubbing (in advanced cases)
- Signs of weight loss and muscle wasting
- Screening Questionnaires: Tools like the COPD Assessment Test (CAT) and Modified Medical Research Council (mMRC) Dyspnea Scale
Pulmonary Function Tests
The cornerstone of emphysema diagnosis:
- Spirometry: Gold standard diagnostic test showing:
- Reduced FEV₁ (Forced Expiratory Volume in 1 second)
- Reduced FEV₁/FVC ratio (Forced Vital Capacity)
- Not fully reversible with bronchodilators
- Lung Volumes: Total Lung Capacity (TLC), Residual Volume (RV), and Functional Residual Capacity (FRC) typically increased
- Diffusing Capacity: DLCO (Diffusing capacity for carbon monoxide) reduced due to loss of alveolar-capillary surface area
- Body Plethysmography: Measures lung volumes and airway resistance
- Exercise Testing: Cardiopulmonary exercise testing to assess functional capacity and oxygen desaturation
Imaging Studies
Visualization techniques provide critical diagnostic information:
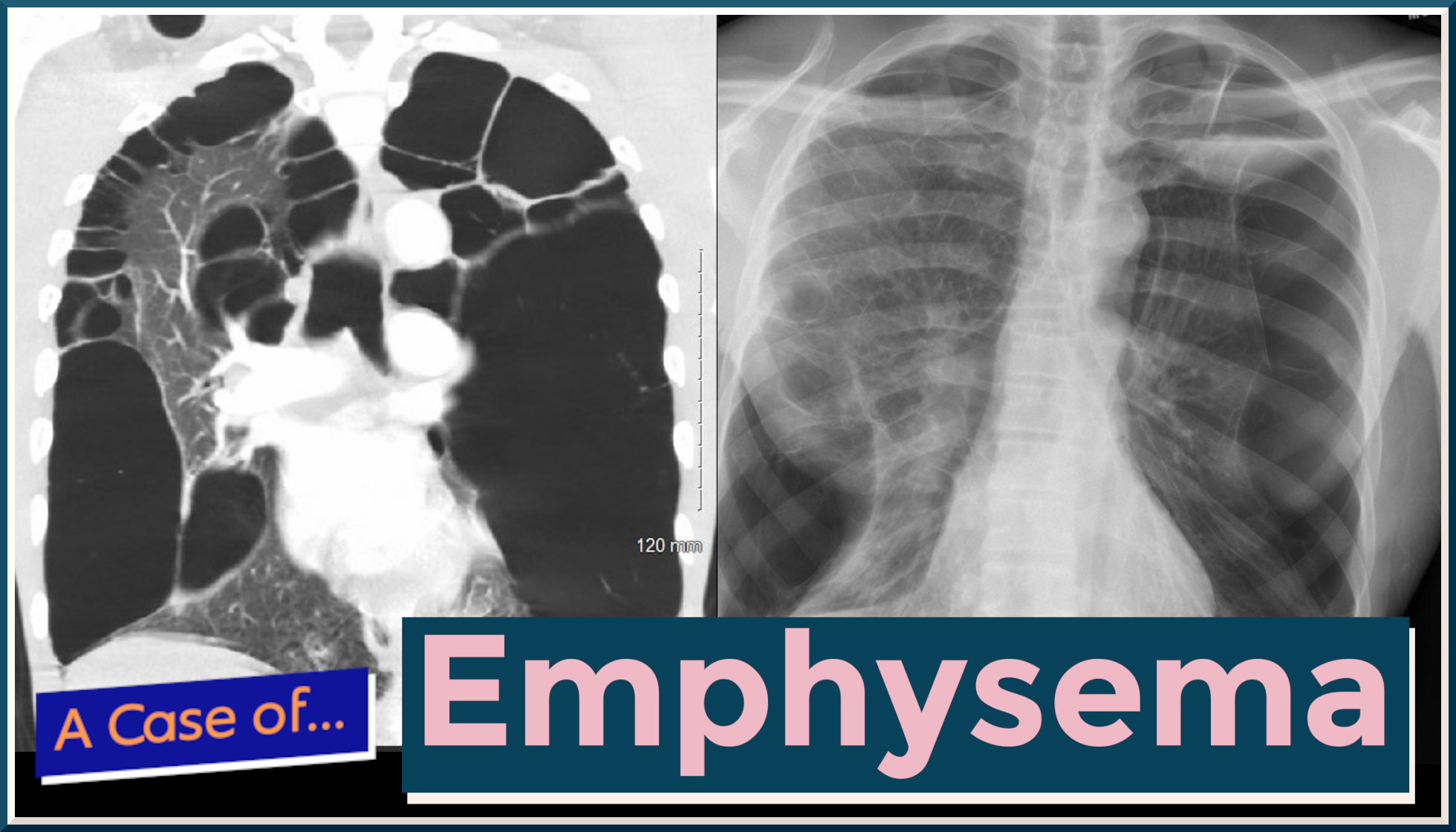
- Chest X-ray: May show:
- Hyperinflation
- Flattened diaphragms
- Increased retrosternal air space
- Bullae formation
- However, can be normal in mild disease
- CT Scan: High-resolution CT (HRCT) is the most sensitive imaging technique
- Reveals emphysematous changes not visible on chest X-ray
- Helps determine emphysema type (centrilobular, panlobular, paraseptal)
- Quantifies extent and distribution of disease
- Identifies bullae and other structural abnormalities
- Other Imaging: Less commonly used modalities include:
- Ventilation-perfusion scanning
- MRI with hyperpolarized gases
- PET scanning (primarily in research settings)
Laboratory Tests
While not diagnostic alone, laboratory studies can provide valuable information:
- Arterial Blood Gas Analysis: Assesses oxygenation and ventilation
- Hypoxemia (low PaO₂)
- Hypercapnia (elevated PaCO₂) in advanced disease
- Compensated respiratory acidosis
- Alpha-1 Antitrypsin Level: To screen for genetic deficiency
- Complete Blood Count: May show polycythemia (elevated red blood cells) in chronic hypoxemia
- Basic Metabolic Panel: To assess electrolyte balance and kidney function
- Biomarkers: Emerging role for inflammatory markers (fibrinogen, CRP, IL-6, TNF-α)
Specialized Testing
Additional tests for specific circumstances:
- Genetic Testing: Genotyping for alpha-1 antitrypsin deficiency variants
- Echocardiography: To assess for pulmonary hypertension and right heart function
- Sleep Studies: If sleep-disordered breathing is suspected
- Sputum Analysis: During exacerbations to identify pathogens
- Exercise Desaturation Studies: Six-minute walk test with oxygen saturation monitoring
- Bronchoscopy: Rarely needed for diagnosis, may help exclude other conditions
Early Detection and Screening
Approaches to identify emphysema at earlier stages:
- Targeted Screening: In high-risk populations (smokers, occupational exposures)
- Alpha-1 Antitrypsin Deficiency Screening: Recommended for:
- Early-onset emphysema (under age 45)
- Emphysema without significant smoking history
- Family history of emphysema
- Unexplained liver disease
- Limitations of Current Approaches:
- Many patients not diagnosed until moderate to advanced disease
- Symptoms often attributed to aging or deconditioning
- Spirometry underutilized in primary care
- Challenges in distinguishing from asthma in early stages
8. Treatment Options
Management Principles
Emphysema treatment follows several key principles:
- Individualized Approach: Therapy tailored to disease severity, phenotype, and comorbidities
- Multi-disciplinary Care: Involving pulmonologists, primary care, respiratory therapists, physiotherapists, dietitians, and psychologists
- Stepwise Approach: Treatment intensity increases with disease severity
- Goals: Reduce symptoms, improve quality of life, prevent exacerbations, slow disease progression, and reduce mortality
Lifestyle Modifications
Behavioral approaches form the foundation of management:
- Smoking Cessation: The single most effective intervention
- Pharmacotherapy (nicotine replacement, varenicline, bupropion)
- Behavioral counseling
- Combination approaches most effective
- Pulmonary Rehabilitation: Comprehensive program including:
- Exercise training
- Education
- Nutritional counseling
- Psychological support
- Shown to improve quality of life, exercise capacity, and reduce hospitalizations
- Nutritional Support: Addressing both underweight and obesity
- Vaccination: Influenza and pneumococcal vaccines to prevent infections
Pharmacological Treatments
Medications target symptoms and disease progression:
- Bronchodilators:
- Short-acting beta-agonists (SABA): For immediate symptom relief
- Long-acting beta-agonists (LABA): For maintenance therapy
- Short-acting muscarinic antagonists (SAMA)
- Long-acting muscarinic antagonists (LAMA): Cornerstone of maintenance therapy
- Anti-inflammatory Agents:
- Inhaled corticosteroids (ICS): Used in specific phenotypes
- Roflumilast: Phosphodiesterase-4 inhibitor for frequent exacerbators
- Combination Therapies:
- LAMA/LABA combinations
- ICS/LABA combinations
- Triple therapy (ICS/LABA/LAMA)
- Antibiotics:
- For acute exacerbations
- Prophylactic azithromycin in frequent exacerbators
- Mucolytics: N-acetylcysteine, carbocisteine
- Alpha-1 Antitrypsin Augmentation Therapy: Weekly intravenous infusions for those with genetic deficiency
Oxygen Therapy
Supplemental oxygen is crucial for hypoxemic patients:
- Long-term Oxygen Therapy (LTOT): Improves survival in patients with severe resting hypoxemia
- Ambulatory Oxygen: For patients with exercise desaturation
- Nocturnal Oxygen: For nocturnal desaturation
- Delivery Systems:
- Compressed oxygen cylinders
- Liquid oxygen
- Oxygen concentrators (stationary and portable)
Non-invasive Ventilation
Breathing support for selected patients:
- Non-invasive Positive Pressure Ventilation (NIPPV):
- Primarily for acute respiratory failure during exacerbations
- Selected stable patients with hypercapnia
- High-Flow Nasal Cannula (HFNC): Emerging role in acute and chronic care
Surgical and Bronchoscopic Interventions
Invasive options for appropriate candidates:
- Lung Volume Reduction Surgery (LVRS):
- Removal of most destroyed areas of lung
- Improves elastic recoil and diaphragm mechanics
- Benefits most pronounced in upper-lobe predominant emphysema with low exercise capacity
- Bullectomy: Surgical removal of large bullae that compress adjacent functional lung
- Lung Transplantation: For end-stage disease in appropriate candidates
- Bronchoscopic Lung Volume Reduction:
- Endobronchial valves
- Coils
- Thermal vapor ablation
- Biologic lung volume reduction
Emerging Treatments and Clinical Trials
Novel approaches under investigation:
- Targeted Biologic Therapies:
- Anti-cytokine therapies (anti-IL-5, anti-IL-33)
- Anti-elastase approaches
- Mesenchymal Stem Cell Therapy: To promote lung repair
- Gene Therapy: Particularly for alpha-1 antitrypsin deficiency
- CRISPR Gene Editing: Early research for genetic forms
- Novel Anti-inflammatory Pathways: Targeting specific inflammatory mediators
- Lung Regeneration Techniques: Bioengineering approaches to restore alveolar tissue
- New Bronchoscopic Techniques: Including targeted denervation to reduce hyperinflation
9. Prevention & Precautionary Measures
Primary Prevention
Strategies to prevent emphysema development:
- Tobacco Control: The most effective preventive measure
- Smoking prevention programs
- Public smoking bans
- Taxation policies
- Marketing restrictions
- Cessation support
- Occupational Health Measures:
- Workplace exposure limits
- Respiratory protection programs
- Ventilation improvements
- Worker education
- Air Pollution Reduction:
- Indoor air quality improvements
- Clean fuel initiatives
- Reduction of biomass fuel use
- Industrial emission controls
- Early Life Factors:
- Maternal smoking prevention
- Childhood asthma management
- Prevention of severe respiratory infections
Secondary Prevention
Approaches to prevent progression in at-risk individuals:
- Early Detection Programs: Targeted spirometry screening in high-risk populations
- Alpha-1 Antitrypsin Deficiency Screening: Family-based testing
- Occupational Surveillance: Regular lung function monitoring in high-risk occupations
- Smoking Cessation Support: Intensive interventions for smokers before disease develops
Tertiary Prevention
Measures to prevent complications in those with established emphysema:
- Optimal Medical Management: Adherence to treatment guidelines
- Exacerbation Prevention:
- Prompt treatment of respiratory infections
- Avoidance of respiratory irritants
- Appropriate vaccination
- Pulmonary Rehabilitation: Regular participation
- Self-Management Education:
- Recognition of exacerbation signs
- Action plans for worsening symptoms
- Proper inhaler technique
- Comorbidity Management: Addressing cardiovascular disease, depression, osteoporosis, etc.
Lifestyle Considerations
Behavioral approaches for prevention and management:
- Physical Activity: Regular, appropriate exercise
- Nutrition: Balanced diet with adequate protein and calories
- Stress Management: Techniques to reduce anxiety and stress
- Environment Control:
- Indoor air quality optimization
- Avoidance of extreme temperatures
- Humidity control
- Travel Considerations: Planning for altitude, air travel, and access to medical care
Vaccines and Preventive Medications
Specific interventions to reduce risk:
- Vaccinations:
- Annual influenza vaccine
- Pneumococcal vaccines (PPSV23 and PCV13)
- COVID-19 vaccination
- Pertussis (Tdap) protection
- Prophylactic Medications:
- Consideration of azithromycin in frequent exacerbators
- N-acetylcysteine in specific phenotypes
- Alpha-1 antitrypsin augmentation in deficient individuals
10. Global & Regional Statistics
Global Prevalence
Emphysema is a significant global health burden:
- Precise global prevalence of emphysema specifically is difficult to determine as it’s often reported as part of COPD
- COPD affects an estimated 384 million people worldwide
- Emphysema likely affects 15-20% of smokers, with varying severity
- Global prevalence increasing due to aging populations and continued smoking in many regions
Regional Variations
Substantial geographic differences exist:
- North America:
- U.S. prevalence of approximately 3.5 million emphysema cases
- Higher rates in rural and Appalachian regions
- Canada shows similar patterns to the U.S.
- Europe:
- Wide variations between countries
- Higher rates in Eastern European countries
- Lower rates in Mediterranean countries
- Asia:
- Rising prevalence in China and India
- Relatively lower rates in Japan
- Increasing burden in Southeast Asia
- Africa:
- Limited data available
- Rising concern due to increasing tobacco use
- Additional burden from biomass fuel exposure
- Latin America:
- High variability between countries
- Uruguay, Chile, and Cuba with higher rates
- Associated with smoking patterns and biomass exposure
Mortality Statistics
Emphysema contributes significantly to global mortality:
- COPD (including emphysema) is the third leading cause of death worldwide
- Annual global COPD deaths approximately 3.23 million
- Mortality varies widely:
- Highest in lower-middle-income countries
- Higher in rural regions of many countries
- Significant gender variations, with male predominance shifting in many regions
- Mortality trends:
- Declining in some high-income countries due to reduced smoking and improved treatment
- Rising in many low and middle-income countries
Economic Impact
The financial burden is substantial:
- Global economic cost of COPD estimated at $2.1 trillion
- Direct healthcare costs (hospitalizations, medications, oxygen)
- Indirect costs (lost productivity, early retirement, caregiver burden)
- In the U.S., average annual cost per patient ranges from $1,681 for mild disease to $10,812 for very severe disease
- Economic burden predicted to increase through 2030
Health Disparities
Emphysema demonstrates significant disparities:
- Socioeconomic Status: Higher burden in lower socioeconomic groups
- Healthcare Access: Significant disparities in diagnosis, treatment, and outcomes
- Gender Disparities: Historically male-predominant, but female prevalence rising rapidly
- Racial/Ethnic Differences: Varying prevalence and outcomes among different racial/ethnic groups
- Rural vs. Urban: Often higher rates and worse outcomes in rural areas
11. Recent Research & Future Prospects
Latest Research Developments
Recent scientific advances include:
- Phenotyping and Endotyping: Identification of distinct biological subtypes of emphysema
- Microbiome Research: Understanding the role of lung microbiome in disease progression and exacerbations
- Genetic Studies: Genome-wide association studies identifying new genetic risk factors
- Biomarker Development: Blood and breath biomarkers for diagnosis and monitoring
- Advanced Imaging Techniques: Functional MRI, PET-CT, and quantitative CT for better assessment
- Cellular Mechanisms: Deeper understanding of cell senescence, mitochondrial dysfunction, and autophagy
- Inflammaging: Connection between aging-related inflammation and emphysema
- Environmental Interactions: Epigenetic changes from environmental exposures
Emerging Therapeutic Approaches
Novel treatment strategies under development:
- Biologics: Targeted therapies for specific inflammatory pathways
- Anti-IL-5 and anti-IL-5R antibodies
- Anti-IL-33 and anti-TSLP approaches
- CXCR2 antagonists to reduce neutrophil recruitment
- Cell-Based Therapies:
- Mesenchymal stem cells
- Induced pluripotent stem cells
- Extracellular vesicles from stem cells
- Novel Drug Delivery Systems:
- Smart inhalers
- Long-acting formulations
- Targeted nanoparticle delivery
- Cellular Senescence Interventions: Senolytics to remove senescent cells
- Mitochondrial Therapies: Addressing mitochondrial dysfunction
- Lung Microbiome Modulation: Probiotics, prebiotics, and targeted antibiotics
- Advanced Bronchoscopic Techniques: Next-generation volume reduction approaches
Ongoing Clinical Trials
Key trials exploring new treatments:
- GALACTIC-1: Investigating galectin-3 inhibitor TD139 in IPF and other fibrotic lung diseases
- ETHOS/KRONOS Extensions: Long-term triple therapy efficacy and safety
- STARR-Lung: Stem cell therapy for lung regeneration
- Various Biologic Trials: Targeting specific inflammatory pathways
- Endobronchial Valve Studies: Refining patient selection and technique
- Pulmonary Rehabilitation Innovations: Telerehabilitation, digital coaching
- Alpha-1 Antitrypsin Augmentation: Optimizing dosing and delivery
- RNA Interference Therapies: For genetic forms of emphysema
Future Research Directions
Areas of increasing scientific focus:
- Precision Medicine: Tailoring treatment to individual genetic and molecular profiles
- Artificial Intelligence Applications: For imaging analysis, risk prediction, and treatment selection
- Regenerative Medicine: Restoring lung architecture and function
- Early Disease Modification: Interventions before significant symptoms develop
- Prevention Strategies: More effective approaches to smoking cessation and avoidance
- Digital Health Solutions: Remote monitoring, telehealth, and smart devices
- Social Determinants of Health: Addressing underlying disparities
- Comorbidity Management: Integrated approaches to multiple conditions
- Global Capacity Building: Improving diagnosis and care in resource-limited settings
12. Interesting Facts & Lesser-Known Insights
Historical Perspectives
Fascinating historical aspects of emphysema:
- Ancient Recognition: Emphysematous changes were described in Egyptian mummies dating back to 1550 BCE
- Laennec’s Insight: The inventor of the stethoscope, René Laennec, not only described emphysema pathologically but suffered from it himself, eventually dying from complications
- Presidential Connection: Several U.S. presidents likely suffered from emphysema, including Dwight D. Eisenhower
- Literary References: Emphysema appears in various literary works, including Thomas Mann’s “The Magic Mountain”
- Terminology Evolution: The word “emphysema” derives from Greek, meaning “to inflate” or “blow in”
Surprising Clinical Facts
Lesser-known clinical aspects:
- Non-Smoking Emphysema: Up to 25% of emphysema cases occur in never-smokers, challenging the common perception
- Early Onset: Emphysematous changes can begin decades before clinical symptoms appear
- Reversibility Aspects: While largely irreversible, some aspects of emphysema (particularly inflammation and hyperinflation) can improve with treatment
- Exercise Paradox: Despite breathing difficulties, regular exercise is one of the most effective treatments
- Different Phenotypes: Not all emphysema is the same—upper lobe, lower lobe, and homogeneous distributions represent different disease processes
- Protected Populations: Certain populations show relative protection despite smoking, suggesting genetic or environmental modifiers
Myths and Misconceptions
Common misunderstandings about emphysema:
- Myth: Emphysema only affects older, male smokers Fact: Affects all ages, genders, and can occur in non-smokers
- Myth: Nothing can be done once diagnosed Fact: Multiple interventions can improve symptoms and quality of life
- Myth: Exercise should be avoided to prevent breathlessness Fact: Regular, appropriate exercise is essential for management
- Myth: Oxygen therapy is addictive or dangerous Fact: Properly prescribed oxygen improves survival and quality of life
- Myth: All emphysema patients are thin Fact: Body composition varies; obesity can coexist with emphysema
- Myth: Emphysema and asthma are the same condition Fact: Fundamentally different diseases with different pathophysiology
- Myth: Emphysema only affects the lungs Fact: Has systemic effects on multiple organ systems
Unique Population Impacts
Special considerations for specific groups:
- Musicians: Wind and brass musicians face unique challenges with emphysema
- High-Altitude Populations: Different adaptations and challenges in mountainous regions
- Firefighters: Higher risk due to smoke and particulate exposure
- Textile Workers: “Byssinosis” or brown lung disease shares features with emphysema
- Marijuana Users: Different pattern of lung damage compared to tobacco
- Early-Life Air Pollution Exposure: Can program lifelong increased susceptibility
- Disaster Survivors: WTC first responders, industrial accidents, and mining disasters
Cutting-Edge Research Insights
Emerging scientific understanding:
- Microbiome Connection: The lung microbiome differs in emphysema patients and may influence disease progression
- Accelerated Aging: Emphysema represents a form of accelerated lung aging
- Autoimmune Components: Evidence for autoimmune mechanisms in some forms of emphysema
- Circadian Rhythms: Symptoms and lung function follow circadian patterns
- Brain-Lung Axis: Neurological influences on respiratory control and perception of dyspnea
- Epigenetic Changes: Environmental exposures cause lasting epigenetic modifications
- Fat-Lung Interactions: Adipose tissue influences inflammatory processes in emphysema
- Biomechanical Factors: Chest wall mechanics and respiratory muscle adaptation critically important beyond airflow limitation
This comprehensive report provides an in-depth overview of emphysema, from its biological mechanisms and clinical manifestations to global impact and future therapeutic directions. While the disease remains a significant global health challenge, advances in understanding, prevention, diagnosis, and treatment offer hope for improved outcomes. The complex interplay of genetics, environment, and lifestyle in emphysema development highlights the importance of multifaceted approaches to both prevention and management.