
⚠️ Disclaimer: The information provided in this article is for educational purposes only and does not constitute medical advice. RevisionTown does not provide diagnosis, treatment, or medical recommendations. Always consult a qualified healthcare professional regarding any medical condition, symptoms, or concerns.
Read More – 🏥 Medical Disclaimer
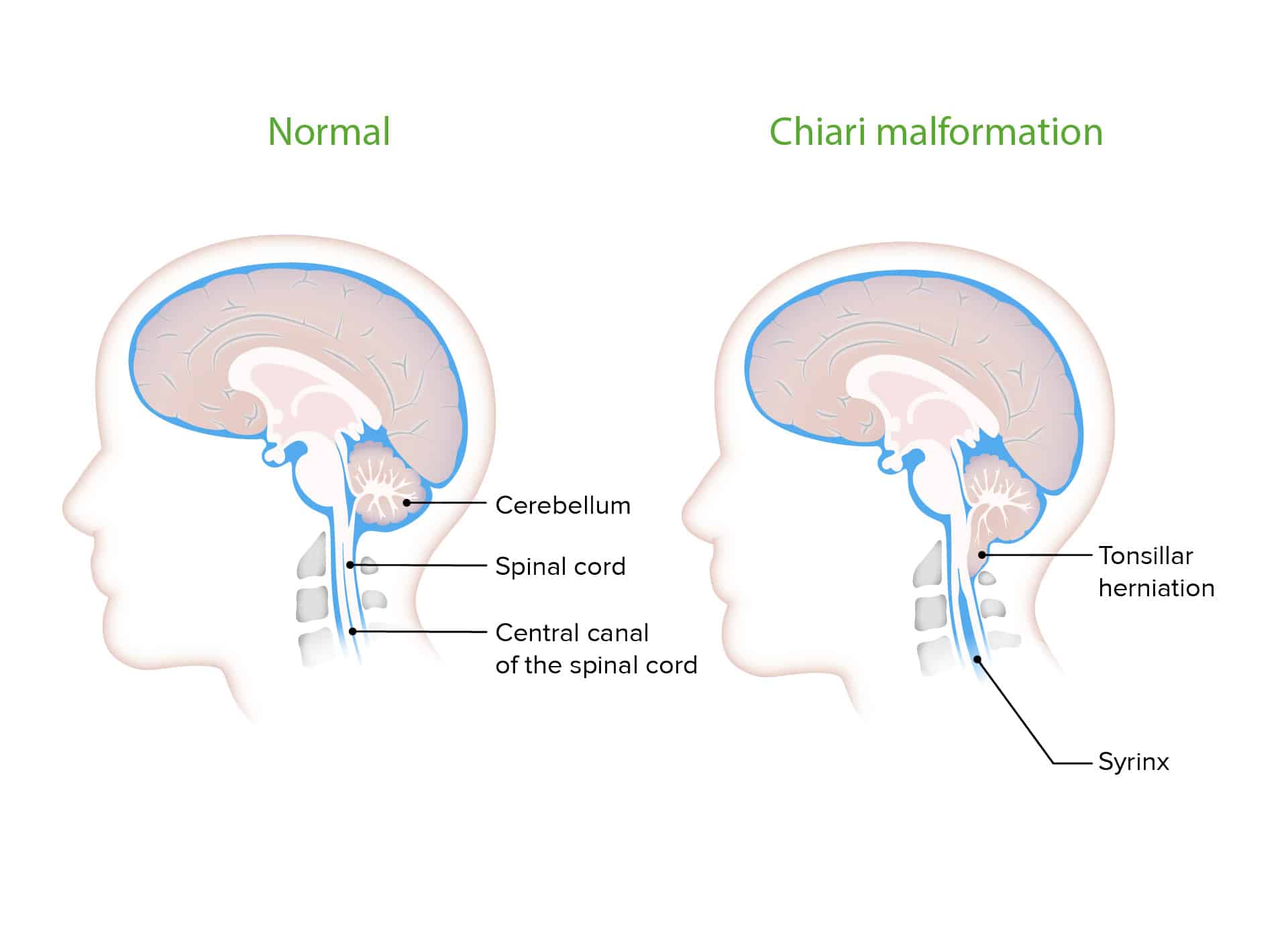
What is Chiari Malformation?
Chiari malformation is a structural abnormality in the base of the skull and cerebellum, characterized by the downward displacement of cerebellar tissue into the spinal canal through the foramen magnum (the opening at the base of the skull). This displacement can put pressure on the cerebellum and brainstem, potentially disrupting the normal flow of cerebrospinal fluid (CSF) between the brain and spinal cord.
Affected Body Parts/Organs
Chiari malformation primarily affects the cerebellum, brainstem, and upper spinal cord. The cerebellum, which controls balance and coordination, is the most directly impacted when its lower portions (cerebellar tonsils) extend below the foramen magnum. This can disrupt normal CSF flow, potentially leading to the development of syringomyelia (fluid-filled cavities in the spinal cord) in some cases.
Prevalence and Significance
While once considered rare, improved diagnostic imaging has revealed that Chiari malformation is more common than previously thought. Current estimates suggest that Type I Chiari malformation affects approximately 1 in 1,000 people symptomatically, although radiographic findings suggest up to 1 in 100 people may meet the anatomical criteria without having symptoms. Chiari malformation Type II is less common and almost always associated with spina bifida. Types III and IV are extremely rare.
The significance of this condition lies in its potential to cause a wide range of neurological symptoms that can significantly impact quality of life, from chronic headaches to balance problems, weakness, and even respiratory issues in severe cases. Early diagnosis and appropriate treatment are crucial for preventing progression and complications.
2. History & Discoveries
When and How Was Chiari Malformation First Identified?
The initial description of what would later be recognized as Chiari malformation dates back to 1883 when John Cleland described a child with spina bifida, hydrocephalus, and abnormalities of the cerebellum and brainstem. However, the condition is named after Hans Chiari, an Austrian pathologist who provided the first comprehensive classification of these brain abnormalities.
Key Discoverers
The malformation bears the name of Hans Chiari (1851-1916), who in 1891 published detailed descriptions of cerebellar abnormalities in the German medical literature. Chiari described several variations of the condition, categorizing them by severity into what would become known as Chiari malformation Types I, II, and III.
The term “Arnold-Chiari malformation” emerged later when Julius Arnold, a German pathologist, also made significant contributions to understanding the condition. In 1894, Arnold described similar findings in an infant with herniation of the cerebellar tonsils through the foramen magnum. The combined term “Arnold-Chiari” was popularized in 1907 by two of Arnold’s students, Schwalbe and Gredig, though today “Chiari malformation” is the more frequently used term, with “Arnold-Chiari” generally reserved for Type II malformations.
Major Discoveries and Breakthroughs
Several key developments have advanced our understanding and treatment of Chiari malformation:
Imaging advances: The development of MRI in the 1980s revolutionized diagnosis, making it possible to visualize the malformation non-invasively and with high precision.
Surgical techniques: In 1932, Van Houweninge Graftdijk reported the first surgical treatment of Chiari malformations, though all patients in this early attempt died from surgery or complications. By 1935, improved approaches were suggested when Russell and Donald proposed decompression of the spinal cord at the foramen magnum to improve CSF circulation.
Recognition of associated conditions: The identification of syringomyelia as a frequent complication of Chiari malformation by Gustafson and Oldberg in 1940 was another important milestone.
Expanded classification: Since Chiari’s original descriptions, researchers have identified additional variants, including Chiari 0, 1.5, 3.5, and 5.
Evolution of Medical Understanding
Medical understanding of Chiari malformation has evolved significantly over time:
- Initially viewed as a rare congenital anomaly with limited treatment options
- Now recognized as a spectrum of disorders with varying severity and presentation
- Better understanding of underlying mechanisms, including the role of a small posterior fossa
- Recognition of potential genetic factors and familial clustering in some cases
- Improved understanding of the relationship between Chiari malformation and associated conditions like syringomyelia, tethered cord syndrome, and connective tissue disorders
- Development of evidence-based surgical approaches and improved outcomes
- Growing recognition of the role of CSF flow dynamics in symptom development
3. Symptoms
Early Symptoms vs. Advanced-Stage Symptoms
Early Symptoms:
- Occipital headaches (at the back of the head), often exacerbated by coughing, sneezing, or straining
- Neck pain
- Balance problems
- Dizziness or vertigo
- Fatigue
- Sleep disturbances
- Numbness or tingling in the hands and feet
Advanced-Stage Symptoms:
- Progressive neurological deterioration
- Difficulty swallowing (dysphagia)
- Voice changes
- Muscle weakness and atrophy
- Impaired fine motor skills
- Gait disturbances
- Visual problems (blurred vision, double vision)
- Tinnitus (ringing in the ears)
- Breathing abnormalities, including sleep apnea
- In severe cases, paralysis
Common vs. Rare Symptoms
Common Symptoms:
- Headaches, particularly those triggered by coughing, sneezing, or physical exertion
- Neck pain and stiffness
- Balance problems
- Numbness or tingling in extremities
- Dizziness
Rare Symptoms:
- Drop attacks (sudden falls due to muscle weakness)
- Loss of pain and temperature sensation
- Vocal cord paralysis
- Apnea (especially in infants with Type II)
- Hydrocephalus (buildup of fluid in the brain)
- Scoliosis (related to syringomyelia)
- Opisthotonos (severe arching of the back) in infants
Symptom Progression Over Time
Chiari malformation symptoms can vary significantly in their progression pattern:
Stable Course: Some individuals with Chiari malformation remain asymptomatic or have mild, stable symptoms that don’t progress over time.
Gradual Progression: Many patients experience a gradual worsening of symptoms over years, with new neurological deficits emerging as compression of neural structures continues or if syringomyelia develops.
Episodic Worsening: Some patients experience periods of stability interspersed with acute episodes of symptom exacerbation, often triggered by activities that temporarily increase intracranial pressure.
Rapid Deterioration: In rare cases, particularly with Type II malformations in infants, neurological deterioration can be rapid and severe, requiring urgent intervention.
Complication-Driven Progression: The development of secondary complications, particularly syringomyelia, can lead to a new onset or worsening of symptoms related to spinal cord dysfunction.
The rate and pattern of progression are influenced by the severity of the anatomical abnormality, the presence of associated conditions, and individual factors. Children may experience different symptom trajectories than adults, with the potential for symptoms to emerge or worsen during periods of growth.
4. Causes
Biological and Environmental Causes
Chiari malformation is primarily considered a developmental disorder of the brain and skull, though its exact etiology remains incompletely understood. Several biological and environmental factors have been implicated:
Biological Factors:
- Underdevelopment of the posterior fossa (the space in the skull that contains the cerebellum)
- Overcrowding of a normally developing hindbrain in an abnormally small posterior cranial fossa
- Abnormal CSF dynamics during development
- Tethered spinal cord pulling the cerebellum downward
Environmental Factors:
- Exposure to certain toxins during fetal development
- Maternal nutritional deficiencies during pregnancy
- Infection during critical developmental periods
- Some cases have been linked to hydrocephalus
Genetic and Hereditary Factors
There is growing evidence for genetic contributions to Chiari malformation:
- Familial Clustering: Studies have identified families with multiple affected members, suggesting genetic factors
- Genetic Studies: While no single “Chiari gene” has been identified, research suggests that multiple genes related to skull and brain development may be involved
- Associated Genetic Disorders: Chiari malformation is more common in individuals with certain genetic conditions, including:
- Ehlers-Danlos syndrome
- Marfan syndrome
- Klippel-Feil syndrome
- X-linked vitamin D-resistant rickets
- Neurofibromatosis Type I
Research into the genetic basis of Chiari malformation is ongoing, with studies examining both traditional genetic inheritance patterns and potential epigenetic factors (changes in gene expression without alterations to the DNA sequence).
Known Triggers or Exposure Risks
While Chiari malformation is typically congenital (present at birth), certain factors may trigger symptom onset or exacerbate existing symptoms:
- Physical Trauma: Head or neck injuries can sometimes trigger symptom onset in previously asymptomatic individuals with the anatomical malformation
- Activities that Increase Intracranial Pressure: Coughing, sneezing, straining during bowel movements, heavy lifting
- Pregnancy: In some women, symptoms may first appear or worsen during pregnancy
- Acquired Forms: In rare cases, Chiari-like malformations can develop later in life due to:
- Intracranial hypertension
- CSF leaks causing brain sagging
- Space-occupying lesions in the posterior fossa
- Excessive draining of CSF (e.g., after shunt placement for hydrocephalus)
5. Risk Factors
Who is Most at Risk?
While Chiari malformation can affect anyone, certain demographic patterns have been observed:
Age:
- Type I Chiari malformation is most commonly diagnosed in late childhood, adolescence, or early adulthood
- Type II is present at birth and typically diagnosed in infancy
- Symptoms of Type I may not appear until the second or third decade of life
Gender:
- There appears to be a female predominance in Type I Chiari malformation, with some studies suggesting females are affected 1.5-3 times more frequently than males
Race/Ethnicity:
- No consistent racial or ethnic predisposition has been established, though further research is needed in diverse populations
Family History:
- Individuals with a family history of Chiari malformation have an increased risk
Environmental, Occupational, and Genetic Factors
Environmental Factors:
- Exposure to certain toxins during pregnancy may increase risk, though specific agents have not been conclusively identified
- Maternal nutritional status during pregnancy may play a role
Occupational Factors:
- No specific occupational risk factors have been established for developing Chiari malformation
- However, individuals with asymptomatic Chiari malformation may experience symptom onset in occupations requiring:
- Heavy physical exertion
- Valsalva maneuvers (straining)
- Activities that increase intracranial pressure
Genetic Factors:
- As mentioned in the Causes section, various genetic conditions are associated with increased risk
- Ongoing research suggests complex genetic inheritance patterns and potential polygenic contributions
Impact of Pre-existing Conditions
Several pre-existing conditions can increase the risk or complicate the management of Chiari malformation:
Conditions Associated with Increased Risk:
- Spina bifida (strongly associated with Type II)
- Hydrocephalus
- Tethered spinal cord
- Connective tissue disorders (Ehlers-Danlos syndrome, Marfan syndrome)
- Craniosynostosis (premature fusion of skull bones)
- Skeletal dysplasias
Conditions That May Complicate Management:
- Craniocervical instability
- Atlantoaxial instability
- Basilar invagination
- Klippel-Feil anomaly (fusion of cervical vertebrae)
- Scoliosis
- Intracranial hypertension
- Hypermobility syndromes
6. Complications
What Complications Can Arise?
Chiari malformation can lead to several serious complications if left untreated:
Syringomyelia:
- Development of fluid-filled cavities (syrinx) within the spinal cord
- Occurs in approximately 65-80% of symptomatic Chiari I patients
- Can cause progressive spinal cord damage if untreated
Syringobulbia:
- Extension of syrinx into the brainstem
- Less common but can cause significant cranial nerve dysfunction
Hydrocephalus:
- Buildup of cerebrospinal fluid in the brain
- More common in Type II malformation
Sleep Apnea:
- Central sleep apnea characterized by periods of breathing cessation during sleep
- Can lead to oxygen desaturation and sleep disturbance
Scoliosis:
- Abnormal curvature of the spine
- Frequently associated with syringomyelia
Tethered Cord Syndrome:
- Abnormal attachment of the spinal cord within the spinal canal
- Can occur in conjunction with Chiari malformation, especially Type II
Long-term Impact on Organs and Overall Health
The long-term impact of Chiari malformation depends on the severity, type, associated complications, and timing of intervention:
Neurological System:
- Progressive neurological deficits if untreated
- Permanent damage to the spinal cord or brainstem in severe cases
- Chronic pain syndromes
- Potential for irreversible motor or sensory deficits
Musculoskeletal System:
- Progressive scoliosis requiring surgical correction
- Muscle atrophy and weakness
- Joint problems related to altered biomechanics and proprioception
Respiratory System:
- Sleep-disordered breathing
- Risk of respiratory failure in severe cases, particularly with Type II
Psychological Impact:
- Chronic pain can lead to depression and anxiety
- Cognitive effects from sleep disturbance
- Impact on quality of life and daily functioning
Systemic Effects:
- Autonomic dysfunction affecting heart rate, blood pressure regulation
- Swallowing difficulties potentially leading to nutritional issues
- Lower cranial nerve dysfunction affecting speech and oral function
Potential Disability or Fatality Rates
Disability:
- Varies widely based on type and severity
- Type I: Many patients lead normal lives with appropriate treatment
- Type II: Associated with higher rates of significant disability
- Type III: Almost always associated with severe neurological impairment
- Types with syringomyelia have higher rates of progressive disability if untreated
Mortality:
- Type I: Rarely life-threatening in adults; surgical mortality rate is approximately 0.8-1.3%
- Type II: Higher mortality, particularly in infants with brainstem dysfunction
- Type III: Associated with high early mortality rate
- Overall Chiari-related mortality across all age groups is estimated at approximately 0.35 per 100,000
Surgical Outcomes:
- Approximately 70-80% of patients report improvement after decompression surgery
- Permanent surgical morbidity rates of 2-3%
- Surgical mortality rates of 0.6-1.3% depending on the type and surgical approach
- Long-term recurrence rates of neurological symptoms of approximately 10-15% within 10 years after surgery
7. Diagnosis & Testing
Common Diagnostic Procedures
The diagnosis of Chiari malformation typically follows a stepwise approach:
Clinical Evaluation:
- Comprehensive medical history with attention to characteristic symptoms
- Detailed neurological examination
- Assessment of cranial nerve function, motor strength, sensory function, reflexes, and coordination
Imaging Studies:
MRI (Magnetic Resonance Imaging): The gold standard for diagnosis
- Sagittal and axial views of the brain and cervical spine
- Measurement of tonsillar position relative to the foramen magnum
- Assessment of posterior fossa volume
- Evaluation for syringomyelia
Cine MRI/Phase-contrast MRI: Specialized MRI technique to assess CSF flow dynamics
- Can demonstrate abnormal CSF flow patterns
- May help predict surgical outcomes
CT (Computed Tomography): Less commonly used but may help evaluate bony abnormalities
- Useful for surgical planning
- Can show details of skull base anatomy
Medical Tests
Neurophysiological Testing:
- Somatosensory evoked potentials (SSEPs)
- Brainstem auditory evoked responses (BAERs)
- May help document functional impairment and establish baseline
Sleep Studies:
- Polysomnography to evaluate for sleep apnea
- Important in patients with sleep disturbances or daytime fatigue
Neuropsychological Testing:
- May be useful in patients with cognitive complaints
- Can establish baseline cognitive function
Genetic Testing:
- May be considered in cases with family history or associated syndromes
- Can help identify underlying genetic disorders
Early Detection Methods and Their Effectiveness
Prenatal Detection:
- Type II malformation may be detected on prenatal ultrasound, especially when associated with spina bifida
- Fetal MRI can provide more detailed evaluation when anomalies are suspected
Incidental Detection:
- Many Type I malformations are discovered incidentally during imaging for unrelated reasons
- The clinical significance of asymptomatic findings remains controversial
Screening in High-Risk Populations:
- Imaging may be recommended for:
- First-degree relatives of patients with Chiari malformation
- Patients with conditions associated with Chiari (e.g., Ehlers-Danlos syndrome)
- Children with unexplained scoliosis
- Patients with syringomyelia
Effectiveness of Early Detection:
- Earlier detection may prevent irreversible neurological damage, particularly in cases with progressive syringomyelia
- However, management of asymptomatic Chiari malformation remains controversial
- No standardized screening protocols exist, and the cost-effectiveness of screening has not been established
8. Treatment Options
Standard Treatment Protocols
Treatment approaches for Chiari malformation depend on the presence and severity of symptoms, associated complications, and type of malformation. The standard treatment protocols include:
Observation and Monitoring:
- Appropriate for asymptomatic patients with incidental findings
- Regular clinical follow-up and periodic MRI scans
- Monitoring for development of symptoms or progression of radiographic findings
Conservative Management:
- For patients with mild symptoms
- Pain management with medications
- Physical therapy for musculoskeletal symptoms
- Lifestyle modifications to avoid activities that exacerbate symptoms
Surgical Management:
- Primary treatment for symptomatic patients, especially those with progressive symptoms or syringomyelia
- Standard surgical approach is posterior fossa decompression
- Surgery aims to relieve pressure on the brainstem and restore normal CSF flow
Medications, Surgeries, and Therapies
Medications:
- Not curative but may help manage symptoms
- Analgesics for headache and pain
- Muscle relaxants for muscle spasms
- Anticonvulsants for neuropathic pain
- Anti-inflammatory drugs
Surgical Procedures:
Posterior Fossa Decompression (PFD): The most common surgical approach
- Suboccipital craniectomy (removal of bone from the back of the skull)
- C1 laminectomy (removal of part of the first cervical vertebra)
Duraplasty: Often performed in conjunction with PFD
- Opening and expanding the dura (the covering of the brain)
- Using either autologous tissue (patient’s own tissue) or synthetic materials
Cerebellar Tonsil Reduction: Sometimes performed in select cases
- Involves removing a portion of the descended cerebellar tonsils
Syrinx Shunting: For cases with significant syringomyelia
- Placement of a tube to drain fluid from the syrinx
- Generally considered when decompression alone is insufficient
CSF Shunting: For cases with hydrocephalus
- Ventriculoperitoneal (VP) shunt to drain excess CSF
Minimally Invasive Approaches:
- Emerging techniques using smaller incisions and specialized instruments
- May reduce recovery time and complications in selected patients
Therapeutic Interventions:
- Physical therapy to improve strength, balance, and coordination
- Occupational therapy for activities of daily living
- Pain management programs
- Psychological support for coping with chronic illness
Emerging Treatments and Clinical Trials
The field of Chiari malformation treatment continues to evolve, with several promising developments:
Advanced Surgical Techniques:
- Minimally invasive decompression using tubular retractors
- Endoscopic approaches for visualization during surgery
- Use of exoscopes for improved visualization and teaching
- Focused ultrasound (investigational)
Personalized Treatment Approaches:
- Computer modeling of CSF flow to predict surgical outcomes
- Patient-specific surgical planning based on biomechanical factors
- Development of outcome scores (like the Chicago Chiari Outcome Scale) to better assess surgical results
Current Clinical Trials and Research:
- The Park-Reeves Syringomyelia Research Consortium study for collecting data on surgical outcomes
- DNA methylation studies investigating epigenetic factors in familial Chiari malformation
- Studies evaluating duraplasty vs. bone-only decompression
- Research into the role of tethered cord in Chiari malformation
- Investigations of CSF hydrodynamics using advanced imaging techniques
Potential Future Directions:
- Gene therapy approaches for genetically influenced cases
- Development of biomarkers to predict disease progression
- Non-invasive treatments targeting CSF flow dynamics
- Improved imaging to better select surgical candidates
The global Chiari malformation treatment market was valued at approximately US $2.26 billion in 2023 and is projected to grow at a compound annual growth rate of 6.4% through 2033, reflecting ongoing investment in research and treatment development.
9. Prevention & Precautionary Measures
How Can Chiari Malformation Be Prevented?
Chiari malformation, particularly Type I, is generally considered a congenital condition with no known direct preventive measures. However, some associated conditions and secondary complications may be preventable:
Primary Prevention:
- There are no established methods to prevent the development of Chiari malformation itself
- Genetic counseling may be appropriate for families with a known history
- Folic acid supplementation during pregnancy is recommended to reduce the risk of neural tube defects, which are associated with Type II Chiari malformation
Secondary Prevention (Preventing Complications):
- Early diagnosis and appropriate treatment of symptomatic Chiari malformation
- Regular monitoring of asymptomatic cases
- Prompt treatment of associated conditions (hydrocephalus, tethered cord)
- Surgical intervention before irreversible neurological damage occurs
Lifestyle Changes and Environmental Precautions
While lifestyle modifications cannot prevent Chiari malformation, they may help manage symptoms and prevent exacerbations:
Activity Modifications:
- Avoiding activities that increase intracranial pressure (heavy lifting, straining)
- Modifying high-impact activities that may worsen symptoms
- Proper body mechanics to reduce neck strain
- Adequate rest and stress management
Environmental Considerations:
- Ergonomic workstations to minimize neck strain
- Proper sleeping position and supportive pillows
- Avoiding high-altitude environments in severe cases (may exacerbate symptoms)
Lifestyle Recommendations:
- Maintaining healthy weight to reduce strain on the spine
- Regular, gentle exercise as tolerated
- Adequate hydration to support CSF production
- Avoiding excessive caffeine and alcohol, which can affect CSF dynamics
Preventive Screenings
While no population-wide screening programs exist for Chiari malformation, targeted screening may be appropriate in certain situations:
High-Risk Groups That May Benefit From Screening:
- First-degree relatives of individuals with Chiari malformation
- Patients with unexplained neurological symptoms consistent with Chiari
- Individuals with conditions associated with Chiari (e.g., Ehlers-Danlos syndrome, syringomyelia)
- Children with unexplained scoliosis
Screening Methods:
- MRI remains the standard for detection
- Focused neurological examination by specialists familiar with the condition
- Follow-up imaging for patients with borderline findings
Guidelines for Monitoring:
- No universally accepted guidelines exist for screening intervals
- Recommendations for asymptomatic individuals with known Chiari typically include:
- Regular clinical evaluations
- MRI scans at intervals determined by the neurosurgeon (typically every 1-3 years)
- Education about symptom recognition
10. Global & Regional Statistics
Incidence and Prevalence Rates Globally
Determining accurate global statistics for Chiari malformation has been challenging due to variability in diagnostic criteria, imaging availability, and reporting practices. However, recent studies provide some insights:
Global Prevalence:
- Type I Chiari malformation: Estimated at 1 in 1,000 symptomatic cases
- Radiographic prevalence (including asymptomatic cases): As high as 1 in 100 based on MRI studies
- Higher prevalence in females (female-to-male ratio of approximately 1.5-3:1)
- Type II Chiari malformation: Closely linked to the prevalence of myelomeningocele (approximately 1 in 1,000 live births)
- Types III and IV: Extremely rare, with prevalence estimates below 1 in 100,000
Age Distribution:
- Type I is most commonly diagnosed in late childhood through early adulthood
- Prevalence appears higher in younger age groups based on imaging studies
- Radiographic findings of Chiari I are less common in elderly populations
Incidence Trends:
- Increased detection rates over the past decades largely attributed to:
- Broader availability of MRI technology
- Incidental findings during imaging for unrelated conditions
- Greater awareness among medical professionals
- True incidence (new cases) is difficult to determine due to the congenital nature of most cases
Mortality and Survival Rates
Mortality directly attributable to Chiari malformation varies by type and associated complications:
Overall Mortality:
- Chiari malformation-related deaths across all age groups: Approximately 0.35 per 100,000 population
Surgical Mortality:
- Modern surgical series report mortality rates of 0.5-1.3% for decompression procedures
- Higher rates in complex cases with multiple abnormalities
- Mortality risk increases with repeated surgeries
Survival Rates:
- Type I: Generally good long-term survival with appropriate treatment
- Type II: Higher mortality, particularly in infancy; survival rates have improved with advances in neurosurgical care
- Type III: Historically poor survival; limited modern data due to rarity
- Type IV: Very poor prognosis with high early mortality
Prognostic Factors:
- Presence and severity of brainstem compression
- Development of syringomyelia
- Age at symptom onset
- Timing of surgical intervention
- Associated anomalies and complications
Country-wise Comparison and Trends
Comparative international data on Chiari malformation is limited, but some regional patterns have been observed:
Regional Variations:
- No conclusive evidence for significant geographical variations in prevalence
- Apparent differences likely reflect variations in:
- Access to advanced imaging
- Diagnostic practices
- Reporting systems
- Healthcare access
Developed vs. Developing Regions:
- Higher diagnosed rates in countries with widespread MRI availability
- Potential underdiagnosis in regions with limited healthcare access
- Treatment outcomes generally better in countries with specialized neurosurgical centers
Recent Trends:
- Increasing diagnosis rates worldwide, particularly in countries adopting advanced imaging technologies
- Growing emphasis on specialized centers for Chiari treatment
- International collaboration in research through registries and consortia
- Development of standardized outcome measures to facilitate international comparisons
The absence of comprehensive global registries makes precise international comparisons difficult. Efforts to establish international databases, such as the Park-Reeves Syringomyelia Research Consortium, aim to improve understanding of regional variations and outcomes.
11. Recent Research & Future Prospects
Latest Advancements in Treatment and Research
Recent years have seen significant advancements in our understanding and management of Chiari malformations:
Imaging Innovations:
- Advanced CSF flow studies using phase-contrast MRI
- Diffusion tensor imaging to assess white matter tract integrity
- Volumetric analysis of posterior fossa structures
- Computational fluid dynamics modeling of CSF flow
Surgical Advances:
- Minimally invasive decompression techniques using tubular retractors
- Endoscope-assisted visualization during surgery
- Development of standardized outcome measures like the Chicago Chiari Outcome Scale
- Improved duraplasty materials and techniques
- Focused ultrasound technology (experimental)
Biological Research:
- Identification of genetic variants associated with Chiari malformation
- Investigation of epigenetic factors in familial cases
- Better understanding of the role of connective tissue disorders
- Research into the developmental mechanisms of hindbrain malformation
Outcome Assessment:
- Long-term follow-up studies demonstrating durability of surgical results
- Better identification of prognostic factors
- Development of predictive models for surgical outcomes
- Improved quality-of-life assessment tools specific to Chiari patients
Ongoing Studies and Future Medical Possibilities
Several ongoing research initiatives hold promise for improving Chiari management:
Major Research Initiatives:
- The Park-Reeves Syringomyelia Research Consortium: Multi-institutional database collecting prospective and retrospective data
- Chiari Surgery Outcomes Study: Evaluating surgical approaches and outcomes
- DNA Methylation in Familial Chiari I Malformation: Investigating epigenetic factors
- CSF Dynamics Research: Exploring the relationship between CSF flow abnormalities and symptoms
Emerging Research Areas:
- Machine learning approaches to predict surgical outcomes
- Development of biomarkers for disease progression
- Investigation of the role of inflammation in symptom development
- Cross-disciplinary approaches incorporating neurosurgery, genetics, and bioengineering
Future Possibilities:
- Personalized treatment algorithms based on genetic and imaging profiles
- Non-surgical interventions targeting CSF dynamics
- Early interventions to prevent progression in asymptomatic cases
- Regenerative approaches for neural tissue affected by long-standing compression or syringomyelia
Potential Cures or Innovative Therapies Under Development
While a definitive “cure” for Chiari malformation remains elusive, several innovative approaches are under investigation:
Advanced Surgical Approaches:
- Customized 3D-printed implants for posterior fossa reconstruction
- Robot-assisted surgical techniques for greater precision
- Tissue engineering approaches for dural reconstruction
Pharmacological Interventions:
- Research into medications that may modify CSF production or absorption
- Neuroprotective agents to prevent secondary damage
- Targeted therapies for management of neuropathic pain
Genetic and Molecular Approaches:
- Gene therapy for cases with identified genetic causes
- Stem cell therapies for neural regeneration in cases with spinal cord damage
- Molecular targeting of pathways involved in skull and brain development
Non-invasive Interventions:
- Transcranial magnetic stimulation for symptom management
- Transcranial direct current stimulation
- Advanced physical therapy protocols using virtual reality
The global Chiari malformation treatment market is expected to grow at a compound annual growth rate of 6.4% between 2023 and 2033, reaching an estimated US $4.2 billion by 2033. This growth reflects both the increasing recognition of the condition and investment in new therapeutic approaches.
12. Interesting Facts & Lesser-Known Insights
Uncommon Knowledge About Chiari Malformation
Historical Curiosities:
- The condition was once thought to be extremely rare, with early case series including only a handful of patients
- Before the advent of MRI, most cases were diagnosed only at autopsy or during surgery for other conditions
- The term “Arnold-Chiari” became popular even though Arnold’s contribution was secondary to Chiari’s original descriptions
Anatomical Variations:
- Beyond the classic four types, researchers have described additional variants including Chiari 0, 1.5, and 3.5
- Some cases involve “complex Chiari,” with multiple associated craniovertebral junction abnormalities
- The position of the cerebellar tonsils can naturally vary with age, with higher positions typically seen in elderly individuals
Clinical Peculiarities:
- Some patients experience exacerbation of symptoms with weather changes, possibly related to barometric pressure effects on CSF dynamics
- “Chiari crashes” describe episodic severe symptom exacerbations that can occur unpredictably
- Despite significant anatomical abnormalities, some individuals remain completely asymptomatic throughout life
Research Insights:
- Recent studies suggest potential connections between Chiari malformation and orthostatic intolerance (difficulty maintaining blood pressure when standing)
- The cerebellum plays roles beyond motor coordination, and Chiari patients sometimes report cognitive symptoms (“brain fog”) that may reflect cerebellar cognitive functions
- Preliminary research suggests possible links between Chiari and certain autoimmune conditions
Myths and Misconceptions vs. Medical Facts
Myth: Chiari malformation is always symptomatic. Fact: Many individuals with radiographic Chiari malformation (particularly Type I) remain asymptomatic throughout life.
Myth: The degree of tonsillar herniation directly correlates with symptom severity. Fact: Studies show poor correlation between the extent of herniation and symptom severity. Some patients with minimal herniation have severe symptoms, while others with significant herniation remain asymptomatic.
Myth: All patients with Chiari malformation require surgery. Fact: Management decisions are based primarily on symptoms and progression, not solely on imaging. Asymptomatic patients typically require monitoring rather than intervention.
Myth: Surgery always resolves all symptoms. Fact: While many patients experience significant improvement, complete resolution of all symptoms occurs in only about 60-75% of cases. Some symptoms, particularly those present for a long duration, may persist.
Myth: Chiari malformation is always congenital. Fact: While most cases are believed to be congenital, acquired Chiari malformation can develop secondary to conditions like intracranial hypotension, mass lesions, or after shunting procedures.
Myth: MRI findings alone can determine the need for treatment. Fact: Clinical symptoms and their impact on quality of life remain the primary determinants for treatment decisions, not imaging findings alone.
Impact on Specific Populations or Professions
Athletes:
- Athletes participating in high-impact or contact sports may face increased risks of symptom exacerbation
- Activities that involve the Valsalva maneuver (straining) can worsen symptoms
- Some professional sports organizations have developed specific protocols for athletes with Chiari malformation
Musicians:
- Wind and brass instrument players may experience increased symptoms due to increased intrathoracic pressure
- Violinists and similar instrumentalists may face challenges related to neck positioning
- Some professional musicians have required career modifications after diagnosis
Military Personnel:
- Aviation and diving duties may be restricted due to pressure changes potentially affecting symptoms
- Physical training requirements may need modification
- Some military branches have specific medical standards regarding Chiari malformation
Pregnant Women:
- Pregnancy can sometimes trigger symptom onset or exacerbation
- Labor and delivery considerations may include avoiding prolonged Valsalva maneuvers
- Special anesthesia considerations may apply during childbirth
Children:
- Presentation in children can differ from adults, with more subtle neurological signs
- Educational accommodations may be necessary for children with cognitive symptoms
- Growth and development need to be monitored carefully, especially with associated conditions like syringomyelia
Understanding these population-specific considerations helps tailor management approaches to individual patient needs and life circumstances.
This comprehensive report on Chiari Malformation provides an overview of current medical understanding, from basic definitions to cutting-edge research. While efforts have been made to include the most up-to-date information, medical knowledge continues to evolve. Patients should consult with healthcare providers for personalized medical advice.