
⚠️ Disclaimer: The information provided in this article is for educational purposes only and does not constitute medical advice. RevisionTown does not provide diagnosis, treatment, or medical recommendations. Always consult a qualified healthcare professional regarding any medical condition, symptoms, or concerns.
Read More – 🏥 Medical Disclaimer
COMPREHENSIVE REPORT ON BRONCHITIS
1. Overview
What is Bronchitis?
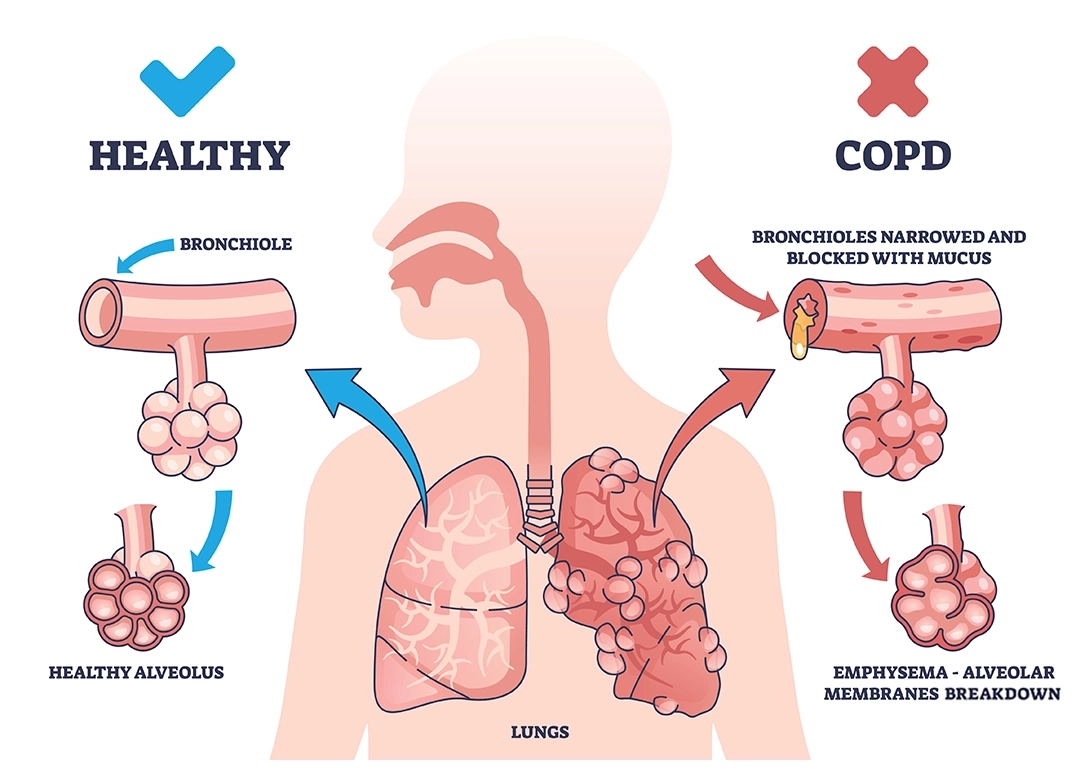
Bronchitis is an inflammation of the bronchial tubes (bronchi), the air passages that connect the trachea (windpipe) to the lungs. This inflammation causes the lining of these tubes to become swollen and produce excess mucus, leading to narrowing of the airways and difficulty breathing. Bronchitis can be categorized into two main types:
- Acute Bronchitis: A temporary inflammation usually caused by viral infections, lasting from a few days to a few weeks
- Chronic Bronchitis: A long-term condition characterized by productive cough that lasts for at least three months, with recurring bouts occurring for at least two consecutive years
Chronic bronchitis is one of the conditions included under the umbrella term Chronic Obstructive Pulmonary Disease (COPD), along with emphysema.
Affected Body Parts/Organs
Bronchitis primarily affects the respiratory system, specifically:
- Bronchial tubes (bronchi): The main airways that branch from the trachea into the lungs
- Bronchioles: Smaller branches of the bronchial tubes
- Lung tissue: Surrounding tissues can become affected due to inflammation and infection
- Respiratory muscles: May be affected indirectly due to increased work of breathing
- Cardiovascular system: Can be strained due to decreased oxygen levels in severe cases
The inflammation process leads to:
- Thickening of the bronchial walls
- Excess mucus production
- Narrowing of the airways
- Potentially, damage to the cilia (tiny hair-like structures that help clear mucus)
Prevalence and Significance
Bronchitis represents a significant global health burden:
Acute bronchitis:
- Affects approximately 5% of adults annually
- One of the most common conditions treated in outpatient settings
- Accounts for approximately 10 million physician visits per year in the United States alone
- Most common in fall and winter months
Chronic bronchitis:
- Affects approximately 3.7% of the global population
- In the United States, an estimated 9 million people (3.5% of adults) have chronic bronchitis
- Worldwide prevalence varies significantly by region (2-5% in Western countries, higher in regions with more pollution and smoking)
- Higher prevalence in adults over 45 years of age
The significance of bronchitis extends beyond its prevalence:
- Substantial economic burden from healthcare costs and lost productivity
- Significant impact on quality of life, especially in chronic cases
- Can lead to more serious conditions if left untreated
- Contributes to antibiotic overuse, as acute bronchitis is often inappropriately treated with antibiotics despite viral causes
- Chronic bronchitis represents a significant component of COPD, which is projected to become the third leading cause of death worldwide by 2030
2. History & Discoveries
First Identification
The history of bronchitis as a recognized medical condition dates back several centuries:
- Ancient observations: Hippocrates and other ancient physicians described respiratory conditions with symptoms resembling bronchitis as early as the 5th century BCE
- 17th century: The term “catarrh” was commonly used to describe conditions with excessive mucus production, including what we now know as bronchitis
- 1808: Charles Badham, a British physician, first used the term “bronchitis” in medical literature to describe the inflammation of the mucous membrane lining the bronchial tubes
- 1814: René Laennec, inventor of the stethoscope, provided detailed descriptions of bronchial inflammation in his treatise on diseases of the chest
- 1837: William Stokes published “A Treatise on the Diagnosis and Treatment of Diseases of the Chest,” which contained significant observations on bronchitis
Key Discoverers
Several key figures contributed to our understanding of bronchitis:
- Charles Badham (1780-1845): First coined the term “bronchitis” and described its clinical features
- René Laennec (1781-1826): Developed the stethoscope and described bronchitis sounds, distinguishing between different respiratory conditions through auscultation
- William Stokes (1804-1878): Further classified bronchitis and its clinical manifestations
- Sir William Osler (1849-1919): Provided comprehensive descriptions of acute and chronic bronchitis in his influential medical textbooks
- Fletcher and Peto (1970s): Conducted landmark studies on the natural history of chronic bronchitis and its relationship to smoking
Major Breakthroughs
Key developments in bronchitis research and treatment include:
- 1821: Invention of the stethoscope by Laennec, enabling better diagnosis of respiratory conditions including bronchitis
- Late 19th century: Recognition of the association between industrial pollution and increased rates of bronchitis
- 1930s-1940s: Development of bronchodilators for symptom relief in respiratory conditions
- 1950s: Establishment of the link between smoking and chronic bronchitis through epidemiological studies
- 1959: The Medical Research Council defined chronic bronchitis for research purposes as “chronic or recurrent increase in the volume of mucoid bronchial secretion sufficient to cause expectoration, occurring on most days for at least three months of the year, for at least two consecutive years”
- 1964: Surgeon General’s report confirmed the causal relationship between smoking and chronic bronchitis
- 1970s: Fletcher and Peto’s studies demonstrated the natural history and progression of chronic bronchitis
- 1975: First guidelines for the diagnosis and management of chronic bronchitis
- 1980s-1990s: Development of more effective inhaled bronchodilators and corticosteroids
- 2000s: Recognition of chronic bronchitis as a component of COPD and development of comprehensive management guidelines
Evolution of Medical Understanding
The conceptual understanding of bronchitis has evolved significantly over time:
- Early 19th century: Initially viewed as a separate disease entity defined by inflammation of the bronchi
- Mid-19th century: Recognition of acute and chronic forms with different clinical courses
- Early 20th century: Growing awareness of environmental and occupational factors
- 1950s-1960s: Establishment of smoking as a primary cause of chronic bronchitis
- 1970s-1980s: Definition of chronic bronchitis based on clinical symptoms for epidemiological studies
- 1990s: Recognition that chronic bronchitis often coexists with emphysema, leading to the COPD concept
- 2000s: Understanding of the inflammatory mechanisms and the complex interplay between genetic factors and environmental exposures
- 2010s-present: Greater appreciation of different phenotypes within chronic bronchitis, varying response to treatments, and the role of microbiome in both acute and chronic bronchitis
This evolution reflects the progressive refinement from a purely symptom-based description to a more comprehensive understanding of the underlying pathophysiological mechanisms and heterogeneity of the condition.
3. Symptoms
Early Symptoms
The initial symptoms of bronchitis vary between acute and chronic forms:
Acute Bronchitis – Early Symptoms:
- Persistent cough, initially dry and non-productive
- Mild chest discomfort or tightness
- Slight wheezing or rattling sound when breathing
- Low-grade fever (typically 100-101°F or 37.8-38.3°C)
- Fatigue and general malaise
- Mild shortness of breath, especially with exertion
- Sore throat (often precedes other symptoms, as acute bronchitis frequently develops after upper respiratory infections)
Chronic Bronchitis – Early Symptoms:
- Persistent productive cough, typically worse in the morning
- Clear, white, or yellowish mucus production
- Mild shortness of breath with exertion
- Recurring respiratory infections
- Wheezing, especially during exertion
- Mild chest discomfort
- Frequent throat clearing
Advanced-Stage Symptoms
As bronchitis progresses, symptoms typically worsen:
Acute Bronchitis – Advanced Symptoms:
- Productive cough with yellow, greenish, or occasionally blood-tinged mucus
- More pronounced chest discomfort and possible pain with coughing
- Increased wheezing and rhonchi (coarse rattling sounds)
- Higher fever in some cases
- More significant fatigue
- Shortness of breath with minimal exertion
- Possible headaches from coughing
- Difficulty sleeping due to cough and congestion
Chronic Bronchitis – Advanced Symptoms:
- Persistent, severe cough with copious sputum production
- Increasing shortness of breath, even at rest
- Cyanosis (bluish discoloration) of lips and nail beds in severe cases
- Swollen ankles, feet, and legs (peripheral edema) from right-sided heart strain
- Weight loss and decreased appetite
- Pronounced wheezing and diminished breath sounds
- Barrel chest (increased anterior-posterior chest diameter)
- Reduced exercise tolerance and functional capacity
- Recurrent respiratory infections with prolonged recovery periods
- Morning headaches (due to retained carbon dioxide during sleep)
Common vs. Rare Symptoms
Common Symptoms:
- Persistent cough (hallmark symptom of both forms)
- Mucus production
- Fatigue
- Mild shortness of breath
- Wheezing
- Chest discomfort
- Low-grade fever (more common in acute bronchitis)
Rare Symptoms:
- High fever (>101.5°F or 38.6°C) – suggests possible pneumonia
- Severe chest pain – may indicate pleurisy or other complications
- Hemoptysis (coughing up blood) – requires immediate evaluation
- Severe weight loss – more common in other conditions like lung cancer or tuberculosis
- Syncope (fainting) during coughing episodes
- Severe headaches – may indicate hypercapnia (elevated carbon dioxide levels)
- Nocturnal sweating – might suggest tuberculosis or other infections
- Joint pain or rash – could indicate systemic inflammatory conditions
Symptom Progression Over Time
The progression of symptoms follows different patterns in acute and chronic bronchitis:
Acute Bronchitis Progression:
- Days 1-3: Typically begins with symptoms of upper respiratory infection (sore throat, runny nose), followed by development of dry cough
- Days 4-7: Cough becomes more persistent and begins to produce mucus, fever may peak
- Days 8-10: Productive cough continues, other symptoms begin to improve
- Days 11-14: Most symptoms resolve except for cough, which may persist
- Weeks 3-4: Cough typically resolves, though it may persist for up to 6 weeks in some cases
Chronic Bronchitis Progression:
- Early phase (months to years): Morning cough with clear sputum, often dismissed as “smoker’s cough”
- Established phase: Daily cough throughout the day with increased mucus, noticeable shortness of breath with exertion
- Progressive phase: Increased frequency and severity of exacerbations, worsening baseline symptoms
- Advanced phase: Significant dyspnea even at rest, features of cor pulmonale (right heart failure), dependency on oxygen therapy
- End-stage: Severe functional limitation, respiratory failure, significant weight loss, frequent hospitalizations
Chronic bronchitis typically follows a pattern of gradual decline punctuated by acute exacerbations. Each exacerbation may result in incomplete recovery, leading to stepwise deterioration in lung function and quality of life over time. The rate of progression varies considerably between individuals based on continued exposures, genetic factors, and adherence to treatment.
4. Causes
Biological and Environmental Causes
The development of bronchitis stems from various biological and environmental factors:
Biological Causes:
1. Infectious agents:
- Viruses (responsible for >90% of acute bronchitis cases):
- Rhinovirus
- Influenza virus
- Respiratory syncytial virus (RSV)
- Adenovirus
- Coronavirus
- Human metapneumovirus
- Bacteria (less common primary cause, often secondary infections):
- Mycoplasma pneumoniae
- Chlamydia pneumoniae
- Bordetella pertussis
- Streptococcus pneumoniae
- Haemophilus influenzae
- Moraxella catarrhalis
2. Inflammatory response:
- Epithelial cell damage in airways
- Neutrophil infiltration
- Release of inflammatory mediators (cytokines, chemokines)
- Goblet cell hyperplasia leading to increased mucus production
- Impaired mucociliary clearance
- Bronchial hyperresponsiveness
Environmental Causes:
1. Air pollutants:
- Tobacco smoke (most significant environmental cause of chronic bronchitis)
- Industrial emissions
- Vehicular exhaust
- Biomass fuel smoke (indoor cooking/heating with poor ventilation)
- Airborne particulate matter (PM2.5 and PM10)
- Nitrogen dioxide, sulfur dioxide, ozone
- Volatile organic compounds
2. Occupational exposures:
- Coal dust
- Silica dust
- Cotton dust (byssinosis)
- Grain dust
- Chemical fumes (acids, ammonia, chlorine)
- Metal fumes
- Welding fumes
3. Other environmental factors:
- Extreme weather conditions, particularly cold air
- High humidity environments promoting mold growth
- Allergens triggering bronchial inflammation
- Poor indoor air quality in sealed buildings
Genetic and Hereditary Factors
Genetic predisposition plays a significant role in bronchitis susceptibility and progression:
1. Alpha-1 antitrypsin deficiency:
- Genetic disorder affecting approximately 1 in 2,500 people
- Predisposes to early-onset chronic bronchitis and emphysema
- Caused by mutations in the SERPINA1 gene
2. Variations in detoxification enzymes:
- Glutathione S-transferase (GST) polymorphisms
- Cytochrome P450 variants affecting metabolism of inhaled toxins
3. Inflammatory response genes:
- Tumor necrosis factor-alpha (TNF-α) gene variations
- Interleukin (IL) gene polymorphisms (IL-6, IL-8, IL-13)
- Transforming growth factor-beta (TGF-β) variants
4. Oxidative stress response genes:
- Superoxide dismutase (SOD) variants
- NADPH oxidase system gene polymorphisms
5. Mucin gene variations:
- MUC5AC and MUC5B gene polymorphisms affecting mucus composition
- CFTR gene mutations (also responsible for cystic fibrosis) can influence bronchial secretions
6. Familial aggregation:
- Family history of chronic bronchitis increases risk by 2-3 times
- Twin studies suggest heritability of 40-60% for susceptibility to chronic bronchitis
Known Triggers and Exposure Risks
Several specific triggers and exposures can initiate or exacerbate bronchitis:
1. Acute infectious triggers:
- Upper respiratory tract infections
- Influenza outbreaks
- Community exposure during peak respiratory virus seasons
2. Environmental triggers:
- Sudden changes in temperature or humidity
- Air pollution episodes or smog events
- Occupational exposure to irritants without proper protection
- Moving to areas with poor air quality
3. Behavioral triggers:
- Initiation of smoking or increase in smoking frequency
- Exposure to secondhand smoke
- Use of e-cigarettes or vaping products
- Recreational drug inhalation
4. Specific high-risk exposures:
- Living near industrial facilities or high-traffic areas
- Working in mining, construction, textile production, or chemical manufacturing
- Using biomass fuels for cooking in poorly ventilated spaces
- Living in developing countries with limited environmental regulations
5. Seasonal factors:
- Winter months (increased viral circulation, indoor congregation)
- Seasonal allergen peaks triggering inflammation
- Inversion layers trapping pollution in urban areas
6. Healthcare-related exposures:
- Mechanical ventilation
- Aspiration events
- Intubation procedures
- Hospital-acquired respiratory infections
The development of bronchitis typically involves a complex interaction between these various causes and triggers, with most cases resulting from multiple contributing factors rather than a single cause.
5. Risk Factors
Who is Most at Risk
Certain demographic and lifestyle factors significantly increase the risk of developing bronchitis:
Age-related risk:
- Acute bronchitis: Higher incidence in children under 5 and adults over 65
- Chronic bronchitis: Risk increases progressively with age, especially after 40
Gender differences:
- Acute bronchitis: Relatively equal gender distribution with slight female predominance
- Chronic bronchitis: Historically more common in men, but gap narrowing as female smoking rates have increased
- Current statistics show women may be more susceptible to the effects of smoking and develop disease with less exposure
Occupation-related risk:
- Coal miners and workers in coal processing
- Construction workers exposed to dust, silica, and asbestos
- Agricultural workers exposed to grain dust, animal dander, and pesticides
- Textile workers (cotton, flax, hemp)
- Metal industry workers exposed to metal fumes
- Chemical manufacturing workers
- Firefighters
- Traffic police and toll booth workers
Lifestyle factors:
- Smoking: Single most important risk factor for chronic bronchitis
- Current smokers have 4-5 times higher risk than never-smokers
- Risk correlates with pack-years of smoking
- Approximately 90% of chronic bronchitis cases are associated with smoking
- Secondhand smoke exposure: 20-30% increased risk
- Alcohol consumption: Heavy drinking impairs mucociliary clearance and immune function
- Physical inactivity: Associated with increased risk and worse outcomes
- Poor nutrition: Deficiencies in antioxidant vitamins (A, C, E) may increase risk
Environmental, Occupational, and Genetic Factors
A range of environmental and genetic factors influence bronchitis risk:
Environmental factors:
- Air pollution levels: Significant correlation between particulate matter (PM2.5, PM10) levels and bronchitis incidence
- Geographic location: Higher rates in urban industrial areas and developing countries with less stringent environmental regulations
- Climate: Cold, damp environments may increase risk
- Housing conditions: Overcrowding, poor ventilation, dampness, and mold exposure
- Socioeconomic status: Lower income associated with increased risk due to multiple factors (housing, healthcare access, occupational exposures)
Occupational exposures:
- Dust exposure: Particularly organic and mineral dusts
- Coal dust: 10-12% of miners develop chronic bronchitis
- Silica dust: 15-20% increased risk among exposed workers
- Cotton dust: Associated with 30-50% higher rates of bronchitis symptoms
- Chemical irritants:
- Sulfur dioxide: Strong association with acute and chronic bronchitis
- Chlorine and ammonia: Can cause acute irritant-induced bronchitis
- Isocyanates: Used in polyurethane production, associated with 20-25% higher bronchitis risk
- Duration and intensity of exposure: Dose-response relationship with cumulative exposure
Genetic factors:
- Alpha-1 antitrypsin deficiency: Particularly significant when combined with smoking
- Family history: 2-3 fold increased risk with first-degree relatives affected
- Genetic polymorphisms:
- MUC5AC gene variants: Associated with 15-30% increased risk
- Inflammatory cytokine gene variations: IL-1, IL-6, IL-8, TNF-α
- Detoxification enzyme variations: GSTM1, GSTP1
- Gene-environment interactions: Genetic factors often modify the effect of environmental exposures
Impact of Pre-existing Conditions
Several pre-existing medical conditions increase the risk and severity of bronchitis:
Respiratory conditions:
- Asthma: 3-4 times increased risk of chronic bronchitis
- Sinusitis: Associated with approximately 30% higher risk of acute bronchitis
- History of childhood respiratory infections: 2-fold increased risk of adult bronchitis
- Bronchiectasis: Often coexists with chronic bronchitis, each exacerbating the other
- Previous tuberculosis: Residual lung damage increases susceptibility
Systemic conditions:
- Immunodeficiency states: HIV, congenital immunodeficiencies, immunosuppressive therapy
- Autoimmune diseases: Rheumatoid arthritis, systemic lupus erythematosus
- Gastroesophageal reflux disease (GERD): Microaspiration can trigger or worsen bronchitis
- Cardiovascular disease: Associated with worse outcomes and complications
- Diabetes mellitus: Impairs immune function and increases infection risk
- Obesity: Associated with 50% higher risk of chronic bronchitis independent of other factors
Anatomical abnormalities:
- Tracheobronchomalacia: Weakness of airway walls
- Vocal cord dysfunction: Can mimic and exacerbate bronchitis
- Ciliary dyskinesia: Impairs mucociliary clearance
- Lung sequestration or other congenital lung anomalies
Other medical factors:
- Malnutrition: Weakens respiratory muscles and immune function
- Vitamin D deficiency: Associated with more frequent and severe respiratory infections
- History of organ transplantation: Immunosuppression increases infection risk
- Neuromuscular disorders: Impair cough effectiveness and secretion clearance
The presence of multiple risk factors has a synergistic effect, substantially increasing the likelihood of developing bronchitis and experiencing more severe disease. Understanding these risk factors is crucial for targeted prevention strategies and early intervention in high-risk populations.
6. Complications
What Complications Can Arise
Bronchitis can lead to various complications, from acute exacerbations to chronic sequelae:
Complications of Acute Bronchitis:
- Pneumonia: Occurs in approximately 5-10% of acute bronchitis cases
- Bacterial superinfection of virally-damaged airways
- Higher risk in elderly, immunocompromised, and those with underlying lung disease
- Acute respiratory failure: Rare, but can occur in severe cases with significant airway obstruction
- Worsening of underlying chronic respiratory conditions:
- COPD exacerbations
- Asthma exacerbations
- Bronchiectasis flares
- Sinusitis: Due to contiguous spread of infection
- Otitis media: Particularly in children
- Prolonged cough syndrome: Post-bronchitis cough persisting >3 weeks
- Reactive airway dysfunction: Temporary bronchial hyperresponsiveness after infection
Complications of Chronic Bronchitis:
- Acute exacerbations of chronic bronchitis (AECB):
- Average 1-4 episodes annually
- Each exacerbation accelerates disease progression
- Associated with permanent loss of lung function in 25-30% of episodes
- Respiratory failure:
- Type I (hypoxemic) – low oxygen levels
- Type II (hypercapnic) – elevated carbon dioxide levels
- Cor pulmonale (right-sided heart failure):
- Due to pulmonary hypertension from chronic hypoxemia
- Develops in approximately 10-30% of advanced cases
- Pneumothorax: Spontaneous lung collapse
- Pulmonary hypertension: Increased pressure in pulmonary arteries
- Chronic respiratory acidosis: Due to carbon dioxide retention
- Secondary polycythemia: Increased red blood cell production in response to chronic hypoxemia
- Malnutrition and muscle wasting: Due to increased energy expenditure from work of breathing
- Bronchiectasis: Permanent dilation of bronchi due to repeated inflammation and infection
- Atelectasis: Collapsed or airless areas of the lung due to mucus plugging
Long-term Impact on Organs and Overall Health
Bronchitis, especially the chronic form, affects multiple organ systems over time:
Respiratory system impact:
- Airways remodeling:
- Thickening of bronchial walls
- Goblet cell hyperplasia
- Destruction of ciliated epithelium
- Squamous metaplasia
- Progressive airflow limitation:
- Decline in FEV₁ (forced expiratory volume in 1 second)
- Increased residual volume
- Ventilation-perfusion mismatch
- Reduced gas exchange efficiency
- Decreased exercise capacity and fitness
- Increased susceptibility to respiratory infections
Cardiovascular system impact:
- Pulmonary hypertension:
- Increased right heart workload
- Right ventricular hypertrophy
- Systemic vascular inflammation:
- Increased risk of coronary artery disease
- Higher incidence of stroke
- Arrhythmias: Due to hypoxemia and electrolyte disturbances
- Peripheral edema: From right heart failure
Musculoskeletal impact:
- Respiratory muscle dysfunction:
- Diaphragm flattening and inefficiency
- Accessory muscle hypertrophy
- Generalized muscle wasting:
- Due to systemic inflammation
- Increased energy expenditure
- Reduced physical activity
- Osteoporosis: From steroid use, vitamin D deficiency, and reduced weight-bearing activity
Neurological and psychological impact:
- Cognitive impairment: From chronic hypoxemia
- Sleep disturbances:
- Nocturnal hypoxemia
- Increased work of breathing at night
- Higher prevalence of sleep apnea
- Depression and anxiety:
- 40-60% of patients with chronic bronchitis experience depression
- Anxiety prevalence 2-3 times higher than general population
- Social isolation and reduced quality of life
Metabolic and nutritional impact:
- Weight loss in advanced disease
- Sarcopenia (loss of muscle mass and strength)
- Micronutrient deficiencies
- Altered protein metabolism
- Insulin resistance
Potential Disability or Fatality Rates
The burden of disability and mortality from bronchitis varies by type and severity:
Acute Bronchitis:
- Mortality: Generally very low in otherwise healthy individuals (<0.1%)
- Increased mortality risk:
- Elderly (>75 years): 1-2%
- Immunocompromised patients: 2-5%
- Those with significant comorbidities: 1-3%
- Temporary disability:
- Average work/school days lost: 2-6 days per episode
- Restricted activity days: 4-10 days
- Long-term disability: Extremely rare from a single episode
Chronic Bronchitis:
- Mortality rates:
- Annual mortality in mild disease: 1-2%
- Moderate disease: 2-7%
- Severe disease: 10-15%
- Very severe disease: 20-30%
- 5-year survival rates:
- Mild disease (FEV₁ >80% predicted): >90%
- Moderate disease (FEV₁ 50-80% predicted): 70-85%
- Severe disease (FEV₁ 30-50% predicted): 45-65%
- Very severe disease (FEV₁ <30% predicted): 20-40%
- Disability metrics:
- Approximately 30-50% report significant activity limitation
- 20-40% unable to maintain full-time employment
- 10-25% require assistance with activities of daily living in advanced stages
- Disability-adjusted life years (DALYs) attributed to chronic bronchitis/COPD: 29.4 million globally
Factors affecting prognosis:
- Continued smoking: Increases mortality 2-3 fold
- Frequency of exacerbations: Each severe exacerbation increases mortality risk by approximately 30%
- Nutritional status: BMI <20 associated with 2-fold higher mortality
- Exercise capacity: 6-minute walk distance <350m associated with poorer survival
- Comorbidities: Presence of cardiovascular disease, diabetes, or lung cancer significantly worsens prognosis
- Age at diagnosis: Earlier onset generally associated with more rapid progression
The progressive nature of chronic bronchitis, especially as part of COPD, makes it a leading cause of disability worldwide and the third leading cause of death in many developed countries. However, early intervention, smoking cessation, and appropriate management can significantly improve outcomes and quality of life.
7. Diagnosis & Testing
Common Diagnostic Procedures
Diagnosing bronchitis involves several clinical procedures and assessments:
Clinical evaluation:
- Comprehensive medical history:
- Duration and nature of symptoms
- Smoking history (current, former, pack-years)
- Occupational exposures
- Previous respiratory conditions
- Family history of respiratory diseases
- Physical examination:
- Vital signs assessment (respiratory rate, heart rate, temperature, blood pressure)
- Inspection for signs of respiratory distress
- Percussion of the chest (usually normal in bronchitis)
- Auscultation for abnormal breath sounds:
- Wheezes (musical sounds from narrowed airways)
- Rhonchi (low-pitched, rumbling sounds from secretions)
- Crackles (may indicate development of pneumonia)
- Assessment for signs of hypoxemia or cor pulmonale in chronic cases
Diagnostic criteria:
- Acute bronchitis:
- Cough as the predominant symptom
- Duration less than 3 weeks
- Absence of pneumonia or specific cause requiring other treatment
- Often diagnosed clinically without extensive testing
- Chronic bronchitis:
- Productive cough for at least 3 months
- Occurs in at least 2 consecutive years
- Other causes of chronic cough excluded
Pulmonary function testing:
- Spirometry:
- Not typically necessary for acute bronchitis
- Essential for diagnosing chronic bronchitis/COPD
- Measures FEV₁ (forced expiratory volume in 1 second)
- Assesses FVC (forced vital capacity)
- Calculates FEV₁/FVC ratio (reduced in obstructive diseases)
- Bronchodilator reversibility testing:
- Measures response to bronchodilator medication
- Helps differentiate from asthma (which typically shows greater reversibility)
- Lung volumes measurement:
- Body plethysmography
- Helium dilution technique
- Nitrogen washout method
Differential diagnosis approach:
- Ruling out pneumonia, asthma, bronchiectasis, tuberculosis, lung cancer
- Considering non-respiratory causes of cough (GERD, heart failure, ACE inhibitor use)
Medical Tests
Various tests help confirm the diagnosis and assess disease severity:
Imaging studies:
- Chest X-ray:
- Usually normal in uncomplicated bronchitis
- Helps exclude pneumonia, tuberculosis, lung cancer
- May show increased bronchovascular markings in chronic cases
- May reveal hyperinflation or flattened diaphragms in advanced disease
- CT scan:
- Not routine for bronchitis diagnosis
- High-resolution CT (HRCT) may be used to:
- Exclude bronchiectasis
- Assess for emphysematous changes
- Evaluate for other lung pathologies
- Shows bronchial wall thickening in chronic bronchitis
Laboratory tests:
- Blood tests:
- Complete blood count (CBC): May show leukocytosis in infectious exacerbations
- C-reactive protein (CRP): Elevated in bacterial infections
- Arterial blood gases (ABGs): For assessing oxygenation and ventilation in severe cases
- Alpha-1 antitrypsin level: In younger patients or those with family history
- Serum electrolytes: May show compensated respiratory acidosis in chronic cases
- Sputum analysis:
- Gram stain and culture: To identify specific pathogens during exacerbations
- Cytology: In cases with hemoptysis or suspicion of malignancy
- Acid-fast bacilli (AFB) testing: To exclude tuberculosis when clinically suspected
Specialized testing:
- Bronchoscopy:
- Not routine for bronchitis diagnosis
- May be performed to:
- Exclude other conditions
- Obtain samples for culture in refractory cases
- Evaluate hemoptysis
- Cardiopulmonary exercise testing:
- Assesses functional capacity
- Determines oxygen desaturation with exercise
- Distinguishes between cardiac and pulmonary limitations
- Sleep studies:
- When sleep-disordered breathing is suspected
- Evaluates nocturnal oxygen desaturation
- Exhaled nitric oxide measurement:
- Higher in asthma than bronchitis
- Helps in differential diagnosis
- Echocardiography:
- Assesses for pulmonary hypertension and cor pulmonale in advanced cases
Microbiological testing:
- Respiratory viral panel:
- PCR testing for common respiratory viruses
- Particularly useful during epidemics or in severe cases
- Specific pathogen testing:
- Mycoplasma pneumoniae
- Chlamydia pneumoniae
- Bordetella pertussis (in prolonged cases with paroxysmal cough)
Early Detection Methods and Their Effectiveness
Early identification of bronchitis, especially chronic forms, improves outcomes:
Screening approaches:
- Case-finding in high-risk populations:
- Smokers over age 40
- Workers with occupational exposures
- Those with respiratory symptoms
- Symptom questionnaires:
- COPD Assessment Test (CAT)
- Modified Medical Research Council (mMRC) Dyspnea Scale
- Sensitivity: 60-80%
- Specificity: 50-70%
- Office-based spirometry screening:
- Pre-bronchodilator screening
- Identifies airflow limitation
- Can detect disease before significant symptoms develop
Early detection effectiveness:
- Pre-bronchodilator spirometry:
- Sensitivity: 80-90% for detecting airflow obstruction
- Specificity: 80-95%
- Can detect early changes before clinical symptoms are prominent
- Cost-effective when targeted to high-risk populations
- Post-bronchometric questionnaire:
- Improved sensitivity (85-95%) when combined with spirometry
- Reduced false positives
- Microspirometry:
- Simpler devices for screening
- Sensitivity: 70-80%
- Specificity: 80-85%
- Lower cost and complexity than full spirometry
- Useful for primary care settings
Limitations of current detection methods:
- Underdiagnosis remains common (estimated 50-80% of cases undiagnosed)
- Symptoms often attributed to aging, deconditioning, or smoking
- Early stages may be asymptomatic despite lung function changes
- Access to spirometry limited in many primary care settings
- Lack of systematic screening programs in many countries
Emerging early detection approaches:
- Genetic testing for susceptibility:
- Currently research-focused
- May identify high-risk individuals for targeted intervention
- Biomarkers:
- Inflammatory markers (fibrinogen, IL-6, IL-8)
- Epithelial injury markers (CC-16, surfactant proteins)
- Extracellular matrix markers
- Currently not validated for routine clinical use
- Mobile health applications:
- Symptom tracking
- Peak flow monitoring
- Voice analysis for cough patterns
- Limited validation but promising preliminary results
Early detection of chronic bronchitis is particularly important as early intervention (especially smoking cessation) can significantly alter disease trajectory. However, the effectiveness of screening programs depends on targeting appropriate high-risk populations and linking detection to effective interventions.
8. Treatment Options
Standard Treatment Protocols
The management of bronchitis follows established guidelines based on type and severity:
Acute Bronchitis Treatment:
- Symptomatic treatment:
- Rest and adequate hydration
- Over-the-counter analgesics for pain and fever (acetaminophen, NSAIDs)
- Humidification of inspired air
- Avoidance of irritants (smoke, pollution)
- Antitussives:
- Used for severe, non-productive cough disrupting sleep
- Dextromethorphan or codeine-containing products
- Limited use due to potential for abuse and respiratory suppression
- Bronchodilators:
- Short-acting beta-agonists (albuterol/salbutamol)
- Primarily for patients with wheezing or history of reactive airways
- Not routinely recommended for all cases
- Antibiotics:
- Generally NOT recommended for uncomplicated acute bronchitis
- Most cases (>90%) are viral and self-limiting
- May be considered if:
- High fever persists >3 days
- Symptoms worsen after initial improvement
- Patient has significant comorbidities
- Clinical suspicion of pertussis or other specific bacterial etiology
Chronic Bronchitis Treatment:
- Smoking cessation:
- Single most effective intervention
- Behavioral counseling
- Nicotine replacement therapy
- Medications (varenicline, bupropion)
- Pharmacotherapy:
- Bronchodilators:
- Short-acting beta-agonists (SABA) for rescue use
- Long-acting beta-agonists (LABA) for maintenance
- Long-acting muscarinic antagonists (LAMA)
- Combination LABA/LAMA for more severe disease
- Anti-inflammatory therapy:
- Inhaled corticosteroids (ICS) for frequent exacerbations
- Combination ICS/LABA
- Roflumilast (phosphodiesterase-4 inhibitor) for severe disease with exacerbations
- Mucoactive agents:
- N-acetylcysteine
- Carbocisteine
- Guaifenesin
- Chronic macrolide therapy:
- Azithromycin three times weekly in selected patients with frequent exacerbations
- Mechanism involves both antimicrobial and anti-inflammatory effects
- Bronchodilators:
- Oxygen therapy:
- Long-term oxygen for patients with chronic hypoxemia
- Ambulatory oxygen for those who desaturate with exercise
- Nocturnal oxygen for sleep-related desaturation
Exacerbation management:
- Increased bronchodilator therapy
- Systemic corticosteroids:
- Prednisone 40mg daily for 5-7 days
- Shorter courses preferred to minimize side effects
- Antibiotics:
- For purulent sputum or signs of infection
- Common choices:
- Amoxicillin-clavulanate
- Macrolides (azithromycin, clarithromycin)
- Respiratory fluoroquinolones (levofloxacin, moxifloxacin)
- Tetracyclines (doxycycline)
- Selection based on local resistance patterns and patient factors
- Intensified airway clearance
- Hospitalization for severe cases:
- Respiratory failure
- Significant comorbidities
- Failure of outpatient management
Medications, Surgeries, and Therapies
A range of treatments address various aspects of bronchitis:
Medication classes and specific agents:
Bronchodilators:
- Short-acting beta-agonists:
- Albuterol/salbutamol
- Levalbuterol
- Long-acting beta-agonists:
- Salmeterol
- Formoterol
- Indacaterol
- Olodaterol
- Short-acting muscarinic antagonists:
- Ipratropium bromide
- Long-acting muscarinic antagonists:
- Tiotropium
- Umeclidinium
- Aclidinium
- Glycopyrronium
- Methylxanthines:
- Theophylline (less commonly used due to narrow therapeutic window)
- Short-acting beta-agonists:
Anti-inflammatory medications:
- Inhaled corticosteroids:
- Fluticasone
- Budesonide
- Beclomethasone
- Mometasone
- Ciclesonide
- Systemic corticosteroids:
- Prednisone
- Methylprednisolone
- Phosphodiesterase-4 inhibitors:
- Roflumilast
- Inhaled corticosteroids:
Combination products:
- LABA/LAMA combinations
- ICS/LABA combinations
- Triple therapy (ICS/LABA/LAMA)
Mucoactive agents:
- Expectorants (guaifenesin)
- Mucolytics (N-acetylcysteine, erdosteine)
- Mucoregulators (carbocisteine)
Anti-infective agents:
- Macrolides (both antimicrobial and anti-inflammatory)
- Beta-lactams
- Tetracyclines
- Fluoroquinolones
- Antivirals (primarily for influenza)
Surgical interventions (rare in bronchitis, more common in advanced COPD):
- Lung volume reduction surgery:
- Removes hyperinflated, poorly functioning lung tissue
- Primarily for emphysema component
- Bullectomy:
- Removal of large air spaces
- Improves breathing mechanics
- Lung transplantation:
- For end-stage disease
- Strict selection criteria apply
Non-pharmacological therapies:
- Pulmonary rehabilitation:
- Structured exercise program
- Education component
- Breathing techniques
- Nutritional counseling
- Psychological support
- Typically 6-12 weeks, 2-3 sessions per week
- Improves exercise tolerance, quality of life, and reduces hospitalizations
- Airway clearance techniques:
- Postural drainage
- Active cycle of breathing techniques
- Positive expiratory pressure (PEP) devices
- Oscillatory PEP devices
- High-frequency chest wall oscillation
- Breathing retraining:
- Pursed-lip breathing
- Diaphragmatic breathing
- Yoga-based approaches
- Nutritional therapy:
- Caloric supplementation for underweight patients
- Protein optimization
- Vitamin D supplementation when deficient
- Psychosocial interventions:
- Cognitive behavioral therapy for anxiety/depression
- Support groups
- Self-management education
Ventilatory support:
- Non-invasive ventilation:
- Primarily for hypercapnic respiratory failure
- Improves gas exchange
- Reduces work of breathing
- May be nocturnal or continuous based on severity
- Invasive mechanical ventilation:
- For acute respiratory failure not responding to non-invasive approaches
- Usually short-term during severe exacerbations
Emerging Treatments and Clinical Trials
Innovative approaches are being investigated for bronchitis management:
Biologic therapies:
- Anti-cytokine therapies:
- Anti-IL-5 (mepolizumab, reslizumab, benralizumab)
- Anti-IL-4/IL-13 (dupilumab)
- Anti-IL-17 agents
- CXCR2 antagonists targeting neutrophil recruitment
- Anti-inflammatory approaches:
- p38 MAPK inhibitors
- PI3K inhibitors
- NF-κB pathway modulators
- Pro-resolution mediators:
- Specialized pro-resolving mediators (SPMs)
- Resolvins and protectins
Novel bronchodilators and combination therapies:
- Dual-acting muscarinic antagonist/beta-agonist molecules
- Ultra-LABA (once-weekly dosing)
- Triple combination inhalers with improved delivery systems
- Nebulized formulations of existing agents for severe disease
Gene and cell-based therapies:
- CFTR modulators: Potentially beneficial for chronic bronchitis phenotype
- Stem cell therapies:
- Mesenchymal stem cells for anti-inflammatory effects
- Tissue repair and regeneration approaches
- RNA-based therapeutics:
- microRNA modulators
- Small interfering RNA (siRNA) targeting inflammatory pathways
Novel anti-infective approaches:
- Phage therapy for antibiotic-resistant pathogens
- Microbiome modulation:
- Probiotics targeting respiratory microbiome
- Precision antibiotics preserving beneficial bacteria
- Host defense peptide mimetics
- Anti-biofilm strategies
Significant clinical trials:
- AMAZE trial: Studying azithromycin for prevention of acute exacerbations
- RETHINC study: Examining treatment of symptomatic smokers without airflow obstruction
- TASCS trial: Testing targeted anti-inflammatory therapy based on sputum profiles
- COPD-INNOVATION: Evaluating mesenchymal stem cell therapy
- STARR-CF: Investigating CFTR modulators in chronic bronchitis without cystic fibrosis
Technology-based treatments:
- Endobronchial valve placement for hyperinflation
- Targeted lung denervation:
- Disrupting parasympathetic nerve input
- Mimicking antimuscarinic effects permanently
- Electromagnetic navigation bronchoscopy:
- For targeted delivery of therapeutics
- Bronchial thermoplasty:
- Reduces airway smooth muscle
- Used in asthma but being investigated for chronic bronchitis
Personalized medicine approaches:
- Biomarker-guided therapy:
- Eosinophil counts
- Exhaled nitric oxide
- Sputum neutrophil/eosinophil ratio
- Genetic signatures
- Phenotype-specific treatment algorithms:
- Frequent exacerbator phenotype
- Eosinophilic phenotype
- Chronic bronchitis phenotype
- Rapid decliner phenotype
The future of bronchitis treatment is moving toward more personalized approaches targeting specific pathophysiological mechanisms rather than symptom-based therapy alone. These emerging treatments hold promise for improved outcomes, particularly for patients who don’t respond adequately to current standard therapies.
9. Prevention & Precautionary Measures
How Can Bronchitis Be Prevented
Several effective strategies can reduce the risk of developing bronchitis:
Primary prevention of acute bronchitis:
- Infection control measures:
- Regular handwashing with soap and water
- Use of alcohol-based hand sanitizers when handwashing isn’t possible
- Avoiding close contact with people who have respiratory infections
- Practicing respiratory hygiene (covering coughs and sneezes)
- Wearing masks during respiratory illness outbreaks
- Vaccination:
- Annual influenza vaccination reduces risk by 30-60%
- Pneumococcal vaccination for high-risk groups
- COVID-19 vaccination
- Pertussis vaccination (Tdap) to prevent Bordetella pertussis infection
- General health maintenance:
- Adequate hydration
- Balanced nutrition supporting immune function
- Regular physical activity
- Adequate sleep
Primary prevention of chronic bronchitis:
- Tobacco avoidance:
- Never starting to smoke
- Smoking cessation for current smokers
- Avoidance of secondhand smoke exposure
- Prevention programs targeting youth
- Public policy measures (taxation, advertising restrictions, smoke-free legislation)
- Occupational exposure mitigation:
- Engineering controls (ventilation, dust suppression)
- Administrative controls (job rotation, exposure limiting)
- Personal protective equipment (respirators, masks)
- Workplace monitoring programs
- Occupational health surveillance
- Environmental pollution reduction:
- Air quality improvement initiatives
- Indoor air filtration
- Proper ventilation
- Reduction of biomass fuel use for cooking/heating
- Avoidance of high pollution areas during peak hours
Secondary prevention (preventing progression or exacerbations):
- Early detection and management of initial stages of chronic bronchitis
- Prompt treatment of respiratory infections
- Self-management education:
- Recognition of early exacerbation symptoms
- Action plans for worsening symptoms
- Proper inhaler technique
- Airway clearance methods
- Pulmonary rehabilitation early in disease course
- Vaccination for those with established disease:
- Annual influenza vaccination
- Pneumococcal vaccination (both PCV13 and PPSV23)
- COVID-19 vaccination
- Avoidance of triggers that worsen symptoms
Lifestyle Changes and Environmental Precautions
Specific lifestyle modifications can significantly reduce bronchitis risk:
Tobacco-related measures:
- Smoking cessation strategies:
- Behavioral support (individual or group)
- Nicotine replacement therapy (patches, gum, lozenges)
- Medications (varenicline, bupropion)
- Alternative approaches (acupuncture, hypnotherapy)
- Combination approaches most effective
- Second-hand smoke avoidance:
- Smoke-free home policies
- Avoiding smoking venues
- Requesting smoke-free hotel rooms
- Avoiding smoking in vehicles
Dietary considerations:
- Anti-inflammatory diet:
- Rich in fruits and vegetables (5+ servings daily)
- Adequate omega-3 fatty acids
- Limited processed foods
- Moderate alcohol consumption
- Antioxidant-rich foods:
- Berries, citrus fruits
- Leafy green vegetables
- Nuts and seeds
- Adequate hydration:
- 8-10 glasses of water daily
- Increased during respiratory infections
- Warm fluids may help loosen secretions
Physical activity recommendations:
- Regular moderate exercise:
- 150+ minutes weekly of moderate-intensity activity
- Improves respiratory muscle strength
- Enhances immune function
- Reduces inflammation
- Breathing exercises:
- Diaphragmatic breathing
- Pursed-lip breathing
- Yoga-based approaches
- Gradual progression for deconditioned individuals
Environmental modifications:
- Home environment:
- HEPA air filtration systems
- Regular cleaning to reduce dust
- Control of humidity (40-50% ideal)
- Avoidance of harsh cleaning chemicals
- Proper ventilation, especially when cooking
- Elimination of mold
- Workplace measures:
- Use of assigned protective equipment
- Adherence to exposure limits
- Regular breaks from exposure
- Showering and changing clothes after exposure
- Outdoor precautions:
- Monitoring air quality reports
- Limiting outdoor activity during high pollution days
- Wearing masks in highly polluted environments
- Scheduling outdoor activities during lower pollution times
- Avoiding exercise near high-traffic areas
Stress management approaches:
- Mind-body practices:
- Meditation
- Yoga
- Tai chi
- Progressive muscle relaxation
- Adequate sleep (7-9 hours nightly)
- Work-life balance
- Social connections and support networks
Vaccines and Preventive Screenings
Specific preventive interventions can reduce bronchitis risk and catch it early:
Recommended vaccinations:
Influenza vaccine:
- Annual vaccination recommended for all adults
- Particularly important for those with:
- Chronic respiratory conditions
- Age >65 years
- Healthcare workers
- Caregivers of vulnerable individuals
- Reduces bronchitis risk by 30-60%
- Also reduces severity when breakthrough infections occur
Pneumococcal vaccines:
- PCV13 (pneumococcal conjugate vaccine):
- Recommended for adults ≥65 years
- Younger adults with chronic conditions
- PPSV23 (pneumococcal polysaccharide vaccine):
- For adults ≥65 years
- Adults with chronic lung disease
- Typically given 1 year after PCV13
- Reduces risk of pneumococcal infections, which can trigger bronchitis
- PCV13 (pneumococcal conjugate vaccine):
Pertussis vaccination:
- Tdap (tetanus, diphtheria, acellular pertussis) booster
- Particularly important for those in contact with infants
- Prevents pertussis, which can present as prolonged bronchitis
COVID-19 vaccination:
- Reduces risk of COVID-19, which can present with bronchitis-like symptoms
- Prevents complications in those with underlying respiratory conditions
- Booster doses recommended based on current guidelines
Preventive screening approaches:
Risk assessment tools:
- COPD Population Screener (COPD-PS)
- Lung Function Questionnaire (LFQ)
- COPD Assessment Test (CAT)
- Identify individuals who would benefit from diagnostic testing
Symptom-based screening:
- Chronic cough
- Dyspnea on exertion
- Frequent respiratory infections
- Sputum production
Lung function screening:
- Office-based spirometry
- Peak flow monitoring
- Particularly for those with:
- Smoking history
- Occupational exposures
- Family history of lung disease
- Respiratory symptoms
Occupational health surveillance:
- Baseline and periodic lung function testing
- Symptom monitoring
- Exposure tracking
- Required by regulations in many high-risk industries
Preventive health programs:
Workplace wellness initiatives:
- Smoking cessation programs
- Exercise promotion
- Respiratory protection education
- Vaccination clinics
Community-based prevention:
- Public education campaigns
- Air quality alerts and guidance
- Smoking prevention and cessation resources
- Mobile health screening units
Healthcare system approaches:
- Electronic medical record prompts for risk assessment
- Integration of prevention into primary care visits
- Telehealth monitoring for early symptom detection
- Care management programs for high-risk individuals
Effective prevention of bronchitis requires a multi-faceted approach combining individual behavioral changes, environmental modifications, appropriate vaccinations, and systematic screening for early detection. These preventive strategies are most effective when tailored to individual risk profiles and when addressing modifiable risk factors across the lifespan.
10. Global & Regional Statistics
Incidence and Prevalence Rates Globally
Bronchitis represents a significant global health burden with varying patterns across regions:
Global incidence of acute bronchitis:
- Estimated 44-46 million cases annually worldwide
- Incidence rate of approximately 40 cases per 1,000 person-years in adults
- Higher rates in children: 60-70 cases per 1,000 person-years
- Seasonal patterns with peaks during winter months in temperate climates
- Multiple annual peaks in tropical regions correlating with rainy seasons
Global prevalence of chronic bronchitis:
- Worldwide prevalence of 3.4-4.2% in adults
- Approximately 330-380 million people affected globally
- Prevalence increases with age:
- 1-2% in young adults (18-29 years)
- 3-5% in middle-aged adults (30-49 years)
- 6-10% in older adults (50+ years)
- Higher rates in men historically, though gender gap narrowing
Economic impact:
- Global costs estimated at $100-150 billion annually
- Direct healthcare costs represent 60-70% of total
- Indirect costs from lost productivity account for 30-40%
- Average cost per patient varies widely by country:
- $9,000-15,000 per year in high-income countries
- $500-2,000 per year in middle-income countries
- Limited data from low-income countries
Healthcare utilization:
- Acute bronchitis accounts for 2-5% of all primary care visits globally
- Chronic bronchitis responsible for:
- 5-7 million hospitalizations annually
- 20-30 million outpatient visits
- Substantial home healthcare services
Mortality and Survival Rates
The impact of bronchitis on mortality varies by type and severity:
Mortality from acute bronchitis:
- Generally low mortality (<0.1%) in otherwise healthy individuals
- Higher rates in vulnerable populations:
- Elderly (>75 years): 1-2%
- Immunocompromised: 2-4%
- Those with significant comorbidities: 1-3%
- Approximately 46,000-60,000 deaths annually attributed to complications of acute bronchitis
Mortality from chronic bronchitis/COPD:
- Chronic bronchitis as part of COPD is the third leading cause of death worldwide
- 3.17 million deaths annually attributed to COPD globally
- Mortality rates vary by disease severity:
- Mild disease: 1-2% annual mortality
- Moderate disease: 2-7% annual mortality
- Severe disease: 10-15% annual mortality
- Very severe disease: 20-30% annual mortality
- 5-year survival rates:
- Overall: 50-70% (varies by severity and age at diagnosis)
- Patients requiring oxygen therapy: 40-50%
- After hospitalization for exacerbation: 50% 5-year survival
Regional variations in mortality:
- Highest mortality rates in:
- Eastern Europe
- South Asia
- Western Pacific regions
- Lowest mortality rates in:
- Western Europe
- Australia
- Canada
- Mortality differentials between high and low-income countries:
- 2-3 fold higher age-adjusted mortality in low-income countries
- Largely due to differences in healthcare access and quality
Temporal trends:
- Declining age-adjusted mortality in high-income countries
- Rising absolute numbers due to population aging
- Increasing rates in many middle-income countries due to rising smoking prevalence
- Projections suggest chronic bronchitis/COPD will remain a leading cause of death through 2030
Country-wise Comparison and Trends
Significant variation exists between countries in bronchitis burden:
Highest prevalence countries for chronic bronchitis:
- China: 8.2-8.6% prevalence, 92 million affected, highest absolute numbers globally
- India: 6.5-7.0% prevalence, 55 million affected, rapidly increasing
- Russia: 5.9-6.4% prevalence, particularly high in industrial regions
- USA: 3.7-4.2% prevalence, 16 million affected by COPD overall
- Indonesia: 5.6-6.1% prevalence, primarily related to tobacco and biomass fuel use
Lowest prevalence countries:
- Japan: 1.4-1.9% prevalence, despite high smoking rates
- Sweden: 2.1-2.5% prevalence, successful tobacco control measures
- Australia: 2.3-2.7% prevalence, comprehensive COPD management programs
- Iceland: 1.8-2.2% prevalence, low smoking rates
- Netherlands: 2.4-2.9% prevalence, early detection programs
Regional trends and patterns:
North America:
- USA: Stable or slightly declining prevalence (3.7-4.2%)
- Canada: Lower prevalence (2.8-3.3%), comprehensive care
- Mexico: Rising prevalence (4.3-4.8%), increasing urbanization
Europe:
- Eastern Europe: Higher prevalence (5-7%), high smoking rates
- Western Europe: Lower prevalence (2-4%), better healthcare access
- Mediterranean countries: Moderate prevalence (3-5%), gender differences less pronounced
Asia:
- China: High prevalence with urban-rural differences
- India: Rapidly increasing, biomass fuel exposure significant
- Japan: Surprisingly low prevalence despite smoking rates
- Southeast Asia: Varying rates (3-7%), increasing with industrialization
Africa:
- Sub-Saharan Africa: Limited data, estimated 3-6% prevalence
- North Africa: 4-6% prevalence, high smoking rates in men
- Common underdiagnosis and attribution to tuberculosis or other infections
South America:
- Brazil: 5.3-5.9% prevalence, significant regional variations
- Argentina: 4.8-5.3% prevalence, higher in urban centers
- Colombia and Chile: 3-4% prevalence, improving detection
Socioeconomic correlations:
Within-country disparities:
- Lower socioeconomic groups have 2-3 times higher prevalence
- Educational level inversely correlated with chronic bronchitis risk
- Rural-urban disparities in many countries
Between-country patterns:
- Inverse relationship with healthcare expenditure per capita
- Positive correlation with income inequality measures
- Relationship with GDP follows inverted U-shape (initially rising, then falling with development)
Future projections:
- Projected 30% increase in chronic bronchitis globally by 2030
- Largest increases expected in:
- Africa (60-70% increase)
- Southeast Asia (50-60% increase)
- Western Pacific (40-50% increase)
- Potential decreases in some high-income countries with successful prevention programs
- Shifting gender distribution with increasing female prevalence
These global statistics highlight the significant and variable burden of bronchitis across regions, the complex interplay of risk factors and healthcare access, and the need for targeted interventions based on regional patterns and trends.
11. Recent Research & Future Prospects
Latest Advancements in Treatment and Research
Recent scientific developments have improved our understanding and management of bronchitis:
Pathophysiological insights:
- Microbiome research:
- Recognition of the lung microbiome’s role in bronchitis
- Dysbiosis patterns associated with disease progression
- Microbiome alterations preceding exacerbations
- Potential for microbiome-based diagnostics and therapeutics
- Inflammatory pathway elucidation:
- Identification of neutrophil extracellular traps (NETs) in chronic bronchitis
- Recognition of specific inflammatory endotypes
- Understanding the role of inflammasomes
- Epithelial-immune cell interactions in disease progression
- Mucus biology advances:
- Characterization of pathological mucins (MUC5AC, MUC5B)
- Understanding hyperconcentrated mucus in disease
- Discovery of mucin tethering mechanisms
- Identification of ion channel dysfunction contributing to abnormal mucus
Diagnostic advances:
- Point-of-care biomarkers:
- Exhaled breath condensate analysis
- Portable sputum inflammatory marker testing
- Blood-based biomarker panels
- Machine learning algorithms for diagnostic accuracy
- Imaging innovations:
- Functional respiratory imaging
- Hyperpolarized gas MRI
- Optical coherence tomography
- AI-assisted CT interpretation
- Novel lung function testing:
- Forced oscillation technique
- Impulse oscillometry
- Multiple breath washout
- More sensitive for early disease detection
Treatment innovations:
- Targeted anti-inflammatory therapy:
- CXCR2 antagonists reducing neutrophilic inflammation
- p38 MAPK inhibitors
- Neutrophil elastase inhibitors
- Anti-IL-17 and anti-IL-23 approaches
- Novel bronchodilator approaches:
- Dual-acting molecules
- Extended-release formulations
- Smart inhaler technology with monitoring
- Nebulized long-acting formulations
- Mucoactive advances:
- ENaC inhibitors to improve hydration
- Novel mucolytics targeting mucin structure
- CFTR modulators for non-CF bronchitis
- Combination mucoactive approaches
- Anti-infective strategies:
- Inhaled antibiotic formulations
- Phage therapy for resistant pathogens
- Host defense peptide mimetics
- Quorum sensing inhibitors
Ongoing Studies and Future Medical Possibilities
Numerous promising approaches are under investigation:
Major clinical trials:
- DYNAMIC study: Evaluating disease progression biomarkers
- SPIROMICS 2: Longitudinal study of COPD subtypes
- RETHINC follow-up: Treatment of symptomatic smokers without airflow obstruction
- COPD Gene 2: Genetic determinants of disease progression
- CLEAR trial: Testing CXCR2 antagonists in specific inflammatory phenotypes
- AEROS study: Anti-elastase compounds for bronchitis symptoms
Therapeutic areas under intense investigation:
- Precision medicine approaches:
- Biomarker-guided therapy selection
- Genetic profiling for treatment response
- Endotype-specific intervention
- Personalized exacerbation prediction models
- Regenerative medicine:
- Mesenchymal stem cell therapy
- Growth factor administration
- Lung progenitor cell activation
- Extracellular vesicle therapy
- Gene-based therapies:
- CRISPR/Cas9 approaches for genetic risk factors
- RNA interference targeting inflammatory mediators
- Epigenetic modifiers
- Gene delivery systems specific for airway epithelium
- Digital health integration:
- Remote monitoring platforms
- Predictive analytics for exacerbations
- Virtual rehabilitation programs
- AI-assisted management algorithms
Emerging research directions:
- Air pollution mitigation strategies:
- Personal exposure monitoring
- Protective interventions for vulnerable individuals
- Policy-level pollution reduction approaches
- Climate change impacts:
- Changing patterns of respiratory infections
- Effects of extreme weather events
- Altered allergen patterns
- Aging and senescence in bronchitis:
- Senolytic approaches
- Telomere biology in disease progression
- Age-related immune dysfunction
- Early life influences:
- Developmental origins of bronchitis
- Childhood exposures affecting adult risk
- Transgenerational effects
Potential Cures or Innovative Therapies Under Development
While a complete “cure” for chronic bronchitis remains elusive, several innovative approaches show promise:
Disease-modifying approaches:
- CFTR modulators beyond cystic fibrosis:
- Tezacaftor/ivacaftor combinations
- Elexacaftor/tezacaftor/ivacaftor
- CFTR activation for non-genetic dysfunction
- Particularly promising for chronic bronchitis phenotype
- ENaC inhibitors:
- BI 1265162
- SPX-101
- Improve airway surface hydration
- Enhance mucociliary clearance
- Anti-inflammatory biologics:
- Anti-TSLP antibodies
- Anti-IL-33 approaches
- NLRP3 inflammasome inhibitors
- Targeting upstream inflammatory initiators
Restoration approaches:
- Epithelial repair enhancers:
- IL-22 based therapies
- Amphiregulin modulation
- HGF-mimetics
- Notch pathway modulators
- Ciliary function restorers:
- Dynein assembly modulators
- Ciliary beat enhancers
- Motility promoting compounds
- Airway basal cell therapies:
- Stimulation of endogenous progenitors
- Cell transplantation approaches
- Growth factor cocktails
- Bioengineered airway tissues
Novel delivery systems:
- Nanoparticle-based delivery:
- Targeted to specific cell types
- Sustained release formulations
- Penetration enhancers for mucus barriers
- Combination therapeutics in single platforms
- Smart inhalers and devices:
- Breath-actuated delivery
- Particle size optimization for specific airway targeting
- Connected devices with monitoring
- Adaptive dosing based on disease status
- Advanced nebulization technologies:
- Vibrating mesh devices
- Acoustic nebulizers
- Smart nebulization systems
- Bronchoscopic drug delivery:
- Targeted therapy to affected airways
- Sustained-release implants
- Thermosensitive gels
Transformative approaches:
- 3D bioprinting:
- Personalized airway stents
- Engineered airway replacements
- Bioprinted tracheal/bronchial grafts
- Microbiome therapeutics:
- Engineered commensal bacteria
- Selective antimicrobials preserving beneficial species
- Bacterial metabolite modulation
- Phage therapy for pathogen control
- Exosome therapy:
- Mesenchymal stem cell-derived exosomes
- Engineered exosomes with therapeutic cargoes
- Immunomodulatory vesicles
- RNA delivery platforms
Timeline perspectives:
- Near-term (1-3 years):
- Improved inhaler technologies
- Novel combinations of existing drugs
- Better phenotyping for personalized treatment
- Enhanced telehealth monitoring systems
- Mid-term (3-7 years):
- Targeted biologics for specific inflammatory patterns
- Mucoactive agents with novel mechanisms
- CFTR/ENaC modulators for non-CF bronchitis
- Advanced biomarker-guided therapy
- Long-term (7+ years):
- Regenerative therapies
- Gene editing approaches
- Tissue engineered solutions
- True disease-modifying interventions
While complete reversal of established chronic bronchitis remains challenging, these emerging approaches offer hope for substantially improved symptom control, slowed disease progression, and potentially disease modification in the coming decades.
12. Interesting Facts & Lesser-Known Insights
Uncommon Knowledge About Bronchitis
Several fascinating aspects of bronchitis remain under-appreciated:
Historical perspectives:
- The term “bronchitis” has been in medical literature for over 200 years, first coined by Charles Badham in 1808
- Ancient Greek and Roman physicians described conditions resembling bronchitis, with Hippocrates noting the connection between climate and respiratory symptoms
- In the Victorian era, bronchitis was called the “English disease” due to its prevalence in London’s foggy, polluted environment
- Early treatments included bloodletting, blistering agents, and various herbal preparations including licorice, honey, and thyme
- The first bronchodilator treatments were derived from the herb Datura stramonium (jimsonweed), which contains atropine-like compounds
Biological curiosities:
- The human airways produce approximately 100 ml of mucus daily in healthy individuals, but this can increase to over 300 ml in chronic bronchitis
- Bronchial epithelium completely renews itself every 30-50 days under normal conditions
- Respiratory cilia beat 12-15 times per second, moving mucus upward at 2-25 mm per minute
- The sensation of cough is mediated by at least five different types of sensory nerves in the airways
- The bronchial tree contains approximately 23 generations of branches between the trachea and alveoli
- Mucins, the gel-forming proteins in mucus, can expand in volume up to 1000 times when secreted and hydrated
Counterintuitive findings:
- Many patients with chronic bronchitis have normal spirometry results, especially in early disease
- The prevalence of chronic bronchitis in never-smokers is approximately 2-4%, indicating other important causative factors
- Productive cough, the hallmark of bronchitis, can actually be protective by clearing pathogens and irritants
- Some individuals with severe smoking history never develop chronic bronchitis due to genetic protective factors
- Viral infections can provide temporary protection against certain bacterial infections through interferon-mediated immunity
- The lungs have their own microbiome, and some bacteria may play protective roles rather than causing harm
Geographic and cultural aspects:
- The traditional Chinese medicine concept of “wind-cold” or “wind-heat” invading the lungs closely parallels Western descriptions of acute bronchitis
- In Scandinavian countries, sauna use has been associated with reduced incidence of respiratory infections, possibly due to improved mucociliary clearance
- In parts of Eastern Europe, salt cave therapy (halotherapy) is used as a complementary treatment for bronchitis
- The prevalence of chronic bronchitis varies up to 10-fold between different geographic regions, even after accounting for smoking rates
- Traditional remedies for bronchitis from around the world often contain similar active ingredients (thyme, honey, eucalyptus) despite developing independently
Myths and Misconceptions vs. Medical Facts
Several misconceptions about bronchitis persist:
Myth: Bronchitis always requires antibiotics for treatment. Fact: Acute bronchitis is viral in over 90% of cases and antibiotics are generally not beneficial. Inappropriate antibiotic use contributes to resistance and side effects.
Myth: Bronchitis always produces green or yellow sputum, indicating a bacterial infection. Fact: Sputum color is determined by the presence of inflammatory cells (neutrophils) and their enzymes, not necessarily bacteria. Viral infections can also cause colored sputum.
Myth: Bronchitis is not serious and is just a “chest cold.” Fact: While acute bronchitis is typically self-limiting, chronic bronchitis represents serious airway pathology and can lead to progressive respiratory decline if not properly managed.
Myth: Only smokers get chronic bronchitis. Fact: While smoking is the predominant risk factor, approximately 25-30% of chronic bronchitis cases occur in non-smokers due to other exposures or genetic factors.
Myth: Bronchitis is contagious for the duration of cough symptoms. Fact: The infectious phase of viral bronchitis typically lasts only 3-7 days. The lingering cough, which can persist for weeks, is due to airway hyperreactivity and healing, not ongoing infection.
Myth: Milk and dairy products increase mucus production in bronchitis. Fact: Scientific studies have not demonstrated that dairy consumption increases mucus production, though it may temporarily change the perceived thickness of saliva.
Myth: Bronchitis is always distinct from pneumonia. Fact: Bronchitis and pneumonia exist on a spectrum, and patients can have elements of both simultaneously. The distinction is not always clear-cut.
Myth: A negative chest X-ray rules out serious respiratory disease. Fact: Chest X-rays can be normal in bronchitis and early COPD despite significant disease. Functional testing is more important for diagnosis.
Myth: Over-the-counter cough suppressants are effective for bronchitis. Fact: Evidence for OTC cough suppressants in bronchitis is limited, and they may be counterproductive when productive cough is helping clear secretions.
Myth: Children with bronchitis should not exercise or attend school. Fact: Mild activity is generally beneficial once fever resolves, and children with simple bronchitis can typically return to school after the acute infectious phase (48-72 hours).
Impact on Specific Populations or Professions
Bronchitis affects various groups in unique ways:
Occupational impacts:
- Coal miners: Historically significant group with “coal worker’s bronchitis”
- Prevalence 2-3 times higher than general population
- Often complicated by pneumoconiosis
- Specific regulations for monitoring and compensation
- Firefighters:
- Acute exposure causing irritant-induced bronchitis
- Cumulative effects from repeated exposures
- Increased risk persisting years after retirement
- Specialized respiratory protection protocols
- Healthcare workers:
- Higher exposure to respiratory pathogens
- Increased risk of work-related asthma that can mimic bronchitis
- Occupational transmission of antibiotic-resistant organisms
- Vaccination requirements and personal protective equipment protocols
- Construction workers:
- Silica and construction dust exposure
- Often complicated by mixed exposures (dust, chemicals, fumes)
- Weather-related exposures intensifying symptoms
- Challenges in consistent respiratory protection use
Special populations:
- Musicians (particularly wind and brass players):
- Bronchitis significantly impacts performance ability
- Higher awareness of subtle respiratory changes
- Specialized respiratory training techniques
- Enhanced recovery protocols to maintain performance schedules
- Professional vocalists:
- Bronchitis directly affects primary professional tool
- Higher sensitivity to minimal symptoms
- Specialized treatment protocols prioritizing vocal function
- Use of humidification and vocal rest strategies
- Air pollution activists and researchers:
- “Bucket brigades” and citizen scientists monitoring air quality
- Personal experiences with bronchitis driving advocacy
- Development of community-centered solutions
- Integration of environmental justice perspectives
- Athletes:
- Particular impact on endurance athletes
- Exercise-induced symptoms even after recovery
- Performance timing around respiratory health
- Strategies to maintain training during illness
Geographic communities:
- Arctic and sub-Arctic populations:
- “Arctic bronchitis” phenomenon in indigenous communities
- Indoor air pollution from heating methods
- Limited healthcare access for early intervention
- Traditional remedies integrated with modern care
- Developing world urban slums:
- Multiple environmental exposures (traffic, industry, cooking)
- Limited healthcare resources
- Higher prevalence in children
- Community-based management approaches
- Post-disaster communities:
- Increased bronchitis following natural disasters
- “World Trade Center cough” after 9/11
- Long-term respiratory monitoring after wildfires
- Special compensation programs for affected individuals
Age-specific considerations:
- Elderly living in long-term care:
- Atypical presentation common (confusion rather than cough)
- Higher mortality from complications
- Challenging medication management due to comorbidities
- Swallowing impairment affecting airway protection
- School-age children:
- Significant cause of school absenteeism
- Impact on academic performance
- School-based prevention programs
- Classroom air quality considerations
These population-specific aspects highlight the wide-ranging impact of bronchitis across different groups and the need for tailored approaches to prevention, diagnosis, and management based on specific risk factors and needs.
This comprehensive report on bronchitis presents current medical understanding, epidemiology, and management approaches. While significant advances have been made in diagnosis and treatment, challenges remain in prevention, especially related to environmental factors and occupational exposures. The burden of bronchitis, particularly the chronic form, continues to be substantial worldwide, with significant variations by region, population, and access to healthcare. Emerging treatments and diagnostic approaches offer hope for improved outcomes, but addressing root causes through environmental and policy measures remains essential to reducing the global impact of this common but consequential respiratory condition.