
⚠️ Disclaimer: The information provided in this article is for educational purposes only and does not constitute medical advice. RevisionTown does not provide diagnosis, treatment, or medical recommendations. Always consult a qualified healthcare professional regarding any medical condition, symptoms, or concerns.
Read More – 🏥 Medical Disclaimer
What is Bronchiectasis?
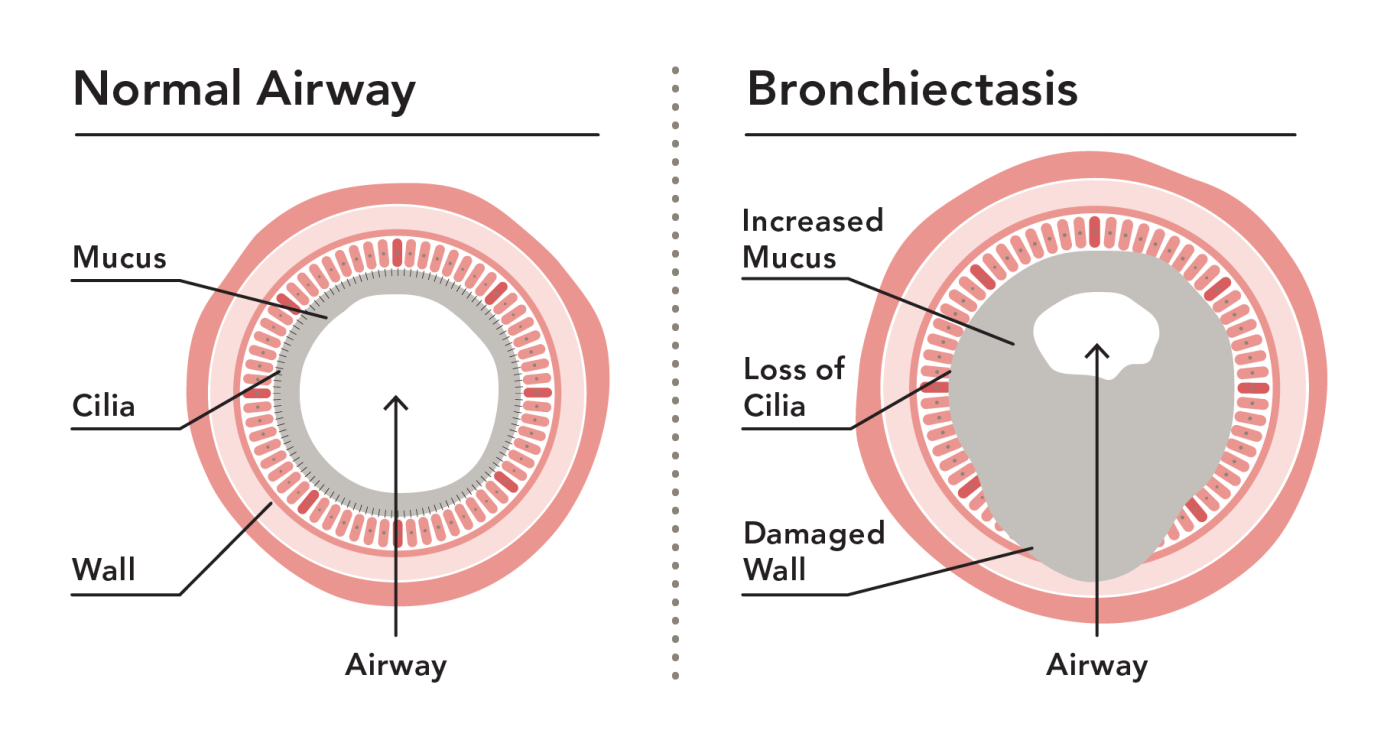
Bronchiectasis is a chronic respiratory condition characterized by permanent abnormal widening and damage of the bronchial airways in the lungs. In this condition, the airways (bronchi) become dilated, scarred, and lose their ability to effectively clear mucus. This leads to mucus build-up in the lungs, creating an environment where bacteria can grow more easily, resulting in recurring infections and inflammation.
Affected Body Parts/Organs
The primary affected organs are the lungs, specifically the bronchial tubes (airways). Unlike healthy airways that maintain their cylindrical shape and proper diameter, bronchiectatic airways become permanently widened, developing pouches or sac-like structures in severe cases. When the airways are damaged, they can’t clear mucus properly, which then pools in these widened areas, creating an ideal environment for bacterial growth and further inflammation.
Prevalence and Significance
Once considered a rare or “orphan” disease, bronchiectasis is now recognized as a significant global health concern. In the United States, estimates suggest between 350,000 to 500,000 people have bronchiectasis, including approximately 1 in 150 people aged 75 and older. However, the true prevalence is likely higher since many individuals can have the condition without experiencing symptoms.
In the UK, research shows that the prevalence of bronchiectasis has been increasing yearly. By 2013, the prevalence reached 566.1 per 100,000 in women and 485.5 per 100,000 in men. Similarly, studies in China showed the prevalence of bronchiectasis in adults increased 2.31-fold from 75.48 per 100,000 in 2013 to 174.45 per 100,000 in 2017.
The significance of bronchiectasis lies in its chronic and progressive nature, causing substantial morbidity, reduced quality of life, frequent hospitalizations, and increased healthcare costs. The condition often leads to repeated respiratory infections requiring long-term antibiotic therapies, disabling productive cough, shortness of breath, and occasional hemoptysis.
2. History & Discoveries
First Identification and Discovery
Bronchiectasis was first described in the early 19th century by the French physician René Théophile Hyacinthe Laennec (1781-1826). Laennec initially described the condition in the early 19th century, providing the first detailed medical documentation of this lung disease. His work was groundbreaking as he observed and documented the characteristic changes in lung structure found in patients with bronchiectasis during post-mortem examinations.
Laennec is perhaps better known as the inventor of the stethoscope in 1816, which revolutionized the diagnosis of chest diseases by allowing physicians to listen to internal sounds without placing their ear directly on the patient’s chest. This invention came at a time when direct auscultation (placing the ear on a patient’s chest) presented challenges related to obesity, hygiene, and modesty, especially with female patients.
Major Discoveries and Breakthroughs
After Laennec’s initial description, several key breakthroughs advanced our understanding of bronchiectasis:
Pathological Understanding: Laennec became the first physician to reliably distinguish among bronchiectasis, emphysema, pneumothorax, lung abscess, hemorrhagic pleurisy, and pulmonary infarcts. This opened the door to modern understanding of various pulmonary conditions.
Radiological Diagnosis: The development of X-rays in the late 19th century, followed by computerized tomography (CT) scanning in the 1970s, transformed the diagnosis of bronchiectasis from a post-mortem finding to one that could be identified in living patients. High-resolution CT scanning, developed in the 1980s, became the gold standard for diagnosis.
Microbiology Advances: The identification of specific pathogens commonly found in bronchiectasis, particularly Pseudomonas aeruginosa, Haemophilus influenzae, and non-tuberculous mycobacteria, has improved targeted treatment approaches.
Genetic Understanding: Discoveries of genetic conditions associated with bronchiectasis, including cystic fibrosis and primary ciliary dyskinesia, have provided insights into underlying mechanisms of the disease.
Evolution of Medical Understanding
The understanding of bronchiectasis has evolved significantly over time:
From Fatal to Manageable: In the pre-antibiotic era, bronchiectasis was often fatal. The introduction of antibiotics in the mid-20th century dramatically changed the prognosis.
Shift in Etiology: While historically bronchiectasis was most commonly caused by infectious diseases like tuberculosis, pneumonia, or whooping cough, improved vaccination and antibiotic treatments have changed the typical causes in developed countries. Now, non-infectious causes like autoimmune conditions and congenital abnormalities are more prominent in developed nations.
Recognition of Heterogeneity: Modern research has recognized that bronchiectasis is not a single disease but a common endpoint of various pathological processes with diverse causes and clinical presentations.
Global Perspective: Recent research has highlighted geographical variations in the etiology, epidemiology, and microbiology of bronchiectasis, emphasizing the influence of environmental factors, genetics, and healthcare access on disease patterns worldwide.
The field continues to advance with the establishment of international registries, collaborative research networks, and increased attention to this previously neglected condition.
3. Symptoms
Early Symptoms
In the early stages of bronchiectasis, symptoms may be subtle and often mistaken for other respiratory conditions like chronic bronchitis or recurrent pneumonia. Early signs typically include:
Persistent Cough: A chronic cough that produces mucus is one of the earliest and most common symptoms of bronchiectasis.
Mucus Production: Regular production of mucus (sputum) that may be clear, yellowish, or green depending on whether infection is present.
Recurrent Respiratory Infections: Repeated colds and bronchial infections that seem to linger longer than expected or occur frequently.
Mild Shortness of Breath: Initially, breathlessness may only occur during physical activity.
Fatigue: General tiredness due to the increased energy expenditure required for breathing and fighting recurring infections.
Advanced-Stage Symptoms
As bronchiectasis progresses, symptoms typically become more severe and debilitating:
Copious Sputum Production: Large amounts of thick, often foul-smelling sputum.
Hemoptysis: Coughing up blood (hemoptysis), which can range from blood-streaked sputum to significant hemorrhage in severe cases.
Severe Shortness of Breath: Increased difficulty breathing, even during minimal exertion or at rest.
Chest Pain: Discomfort or pain in the chest, particularly during breathing or coughing.
Weight Loss: Unintentional weight loss due to increased energy expenditure and poor nutrient absorption.
Clubbing of Fingers: Swollen fingertips with curved nails (nail clubbing) may develop in advanced cases.
Wheezing and Crackles: Abnormal breath sounds that can be heard with a stethoscope.
Symptom Progression
The progression of bronchiectasis symptoms varies significantly among individuals and depends on factors such as the underlying cause, extent of lung damage, presence of comorbidities, and treatment adherence. Key aspects of symptom progression include:
Cyclical Pattern: Many patients experience periods of symptom stability alternating with acute exacerbations (flare-ups) when symptoms worsen dramatically.
Exacerbation Symptoms: During flare-ups, patients may experience extreme fatigue, fever, chills, increased shortness of breath, and night sweats.
Gradual Decline in Lung Function: Over time, recurrent infections and inflammation can lead to further airway damage and declining respiratory capacity.
Development of Complications: Progressive disease can lead to complications such as severe respiratory insufficiency, right-sided heart failure (cor pulmonale), and severe hemoptysis.
The rate of progression can be influenced by appropriate management, including airway clearance techniques, prompt treatment of infections, and addressing the underlying cause when possible. Early detection and intervention are critical to slowing symptom progression and preserving lung function.
4. Causes
Biological and Environmental Causes
Bronchiectasis develops when the bronchial walls become damaged and weakened, leading to permanent dilation. This damage can result from various biological and environmental factors:
Infections:
- Severe respiratory infections, particularly during childhood, can damage airways and lead to bronchiectasis. These include:
- Tuberculosis
- Severe pneumonia
- Whooping cough (pertussis)
- Measles
- Adenovirus infection
Airway Obstruction:
- Foreign body aspiration or tumors that block airways can lead to infection and damage behind the blockage.
- Enlarged lymph nodes compressing airways
Environmental Exposures:
- Toxic gas inhalation
- Smoke inhalation
- Aspiration of gastric acid (reflux)
- Occupational exposures to dust or chemicals
Inflammatory Conditions:
- Inflammatory bowel disease, including Crohn’s disease and ulcerative colitis
- Allergic bronchopulmonary aspergillosis (ABPA), a type of allergic lung inflammation of the airways
- Rheumatoid arthritis and other autoimmune disorders
Genetic and Hereditary Factors
Several genetic conditions are associated with the development of bronchiectasis:
Cystic Fibrosis (CF):
- The most common genetic cause of bronchiectasis in Western countries
- Caused by mutations in the cystic fibrosis transmembrane conductance regulator (CFTR) gene
- Results in thick, sticky mucus that clogs airways and leads to infections
Primary Ciliary Dyskinesia (PCD):
- A genetic condition affecting the small, hair-like structures (cilia) that line the airways
- Immotile or dysfunctional cilia cannot clear mucus effectively
- Often associated with Kartagener syndrome (a triad of bronchiectasis, sinusitis, and situs inversus)
Alpha-1 Antitrypsin Deficiency:
- A genetic disorder that can cause COPD and bronchiectasis
- Results in reduced protection against neutrophil elastase, which can damage lung tissue
Immunodeficiency Disorders:
- Primary immunodeficiencies (genetic defects in the immune system)
- Common variable immunodeficiency (CVID)
- Selective IgA deficiency
- X-linked agammaglobulinemia
Single CFTR Gene Mutations:
- Even a single mutation in the CFTR gene (without full CF) may increase susceptibility to bronchiectasis
Known Triggers and Exposure Risks
Certain triggers and exposures can worsen bronchiectasis or increase the risk of exacerbations:
Respiratory Infections:
- Viral infections (influenza, rhinovirus, respiratory syncytial virus)
- Bacterial infections (particularly Pseudomonas aeruginosa, Haemophilus influenzae, and Moraxella catarrhalis)
- Non-tuberculous mycobacterial infections
- Fungal infections (especially Aspergillus species)
Air Pollution:
- Indoor air pollutants (smoke, mold, chemicals)
- Outdoor air pollution (particulate matter, ozone, nitrogen dioxide)
Tobacco Smoke:
- Both active smoking and secondhand smoke exposure
Aspiration:
- Chronic pulmonary aspiration, problems with swallowing that causes food or fluids to get into the lungs
- Gastroesophageal reflux disease (GERD)
Comorbid Respiratory Conditions:
- COPD (occurs with bronchiectasis in 35-50% of cases)
- Severe asthma (occurs with bronchiectasis in 25-40% of cases)
Understanding these causes, genetic factors, and triggers is essential for proper management of bronchiectasis and prevention of disease progression. In many cases, identifying and addressing the underlying cause can significantly improve outcomes.
5. Risk Factors
Demographic Risk Factors
Several demographic factors influence the risk of developing bronchiectasis:
Age:
- The risk of developing bronchiectasis increases with age, though younger people can also be affected.
- Prevalence is highest in patients over 60 years of age.
Gender:
- Women are more likely to have bronchiectasis than men.
- Bronchiectasis is more common in women than in men.
- This gender disparity becomes more pronounced with increasing age.
Ethnicity and Geographic Location:
- Very high incidence is observed in Indigenous populations of New Zealand and Australia.
- In New Zealand, Pacific and Māori children have significantly higher incidence rates compared to European children.
- Various ethnic groups worldwide show different prevalence patterns, suggesting genetic, environmental, and socioeconomic factors at play.
Socioeconomic Status:
- Bronchiectasis occurs more frequently in less affluent communities.
- Limited access to healthcare, poor housing conditions, and overcrowding may contribute to this disparity.
Environmental and Occupational Factors
Several environmental and occupational exposures can increase the risk of developing bronchiectasis:
Air Pollution:
- Long-term exposure to indoor and outdoor air pollutants
- Particulate matter, gases, and chemicals that irritate the airways
Occupational Exposures:
- Workers in mining, textile manufacturing, and chemical industries
- Exposure to silica, coal dust, metal fumes, and other respiratory irritants
- Professions with high risk of inhaling organic dusts (farming, grain handling)
Smoking and Secondhand Smoke:
- Active smoking can exacerbate bronchiectasis and accelerate lung function decline
- Childhood exposure to secondhand smoke may increase susceptibility
Geographic Factors:
- Areas with high prevalence of tuberculosis
- Regions with limited access to healthcare and vaccination programs
- Areas with high levels of industrial pollution
Impact of Pre-existing Conditions
Several pre-existing conditions significantly increase the risk of developing bronchiectasis:
Respiratory Infections:
- History of severe pneumonia, particularly in childhood
- Tuberculosis infection
- Whooping cough (pertussis)
- Complicated measles or adenovirus infections
Chronic Respiratory Diseases:
- Chronic obstructive pulmonary disease (COPD) – bronchiectasis has been identified in up to 50% of these patients
- Severe asthma
- Recurrent aspiration pneumonia
Immune System Disorders:
- Primary immunodeficiencies
- HIV/AIDS
- Conditions requiring immunosuppressive therapy
Connective Tissue and Autoimmune Diseases:
- Rheumatoid arthritis
- Sjögren’s syndrome
- Inflammatory bowel disease
- Systemic lupus erythematosus (SLE)
Allergic Conditions:
- Allergic bronchopulmonary aspergillosis (ABPA)
Genetic Conditions:
- Family history of cystic fibrosis, Kartagener’s Syndrome, and primary ciliary dyskinesia (PCD) is important as these conditions share an autosomal recessive inheritance pattern.
- Alpha-1 antitrypsin deficiency
Gastroesophageal Disorders:
- Gastroesophageal reflux disease (GERD)
- Aspiration due to swallowing difficulties (dysphagia)
Structural Abnormalities:
- Congenital lung malformations
- Lung sequestration (abnormal lung tissue not connected to the normal bronchial system)
- Tracheoesophageal fistula
Understanding these risk factors is essential for early identification of individuals at high risk for bronchiectasis, enabling preventive measures and timely intervention to limit disease progression.
6. Complications
Common Complications
Bronchiectasis can lead to several serious complications affecting both respiratory and systemic health:
Recurrent Respiratory Infections:
- The most common complication, creating a vicious cycle of infection, inflammation, and further airway damage
- Bacterial, viral, and sometimes fungal infections
Hemoptysis (Coughing Up Blood):
- Can range from blood-streaked sputum to significant hemorrhage
- In severe cases, can be life-threatening and require emergency intervention
Atelectasis:
- Collapse or closure of a lung or lung segment
- Results from mucus plugging and airway obstruction
Lung Abscess:
- Localized collection of pus within the lung tissue
- Can develop from untreated or severe infections
Empyema:
- Collection of pus in the pleural space (between the lung and chest wall)
- Requires drainage and antibiotics
Pneumothorax:
- Air leakage into the pleural space, causing lung collapse
- More common in patients with severe or cystic bronchiectasis
Long-term Impact on Organs and Overall Health
Bronchiectasis can have widespread effects on multiple organ systems and overall health:
Respiratory System:
- Progressive decline in lung function
- Reduced exercise capacity
- Chronic hypoxemia (low blood oxygen)
Cardiovascular System:
- Cor pulmonale (right-sided heart failure as a result of lung disease)
- Pulmonary hypertension (high blood pressure in the arteries of the lungs)
- Increased risk of cardiovascular events
Systemic Inflammation:
- Chronic inflammation can affect multiple organ systems
- Increased levels of inflammatory markers in the bloodstream
Nutritional Status:
- Weight loss and malnutrition due to increased metabolic demands
- Reduced appetite during exacerbations
Psychological Health:
- Anxiety and depression related to chronic illness
- Reduced quality of life
- Sleep disturbances
Secondary Amyloidosis:
- A rare complication where protein deposits occur in organs due to chronic inflammation
- Can lead to renal failure through nephrotic syndrome
Disability and Fatality Rates
The impact of bronchiectasis on disability and mortality varies widely depending on disease severity, underlying cause, comorbidities, and access to appropriate care:
Disability:
- Bronchiectasis often leads to significant disability through reduced lung function, chronic symptoms, and frequent exacerbations
- Many patients experience limitations in daily activities and reduced work capacity
- Advanced disease may result in oxygen dependency and reduced mobility
Mortality:
- While bronchiectasis is a chronic condition, most people with bronchiectasis managed with proper treatment live a normal life span.
- In the UK, around 1,500 deaths are reported each year due to bronchiectasis.
- Studies show that patients with bronchiectasis have more than twice the mortality rate of the general population.
- In one UK study, the age-adjusted mortality rate for women with bronchiectasis was 1437.7 per 100,000 compared to 635.9 per 100,000 in the general population (2.26 times higher). For men, the rates were 1914.6 per 100,000 versus 895.2 per 100,000 (2.14 times higher).
Factors Affecting Prognosis:
- Presence of Pseudomonas aeruginosa colonization is associated with worse outcomes
- Frequent exacerbations (three or more per year) indicate poorer prognosis
- Comorbidities significantly impact survival rates
- All-cause mortality is higher in elderly patients and men with bronchiectasis.
- The risk of all-cause mortality is more prominent in those with airflow limitation and in ever smokers.
Cause of Death:
- Respiratory-related deaths and lung cancer-related deaths are significantly higher in bronchiectasis patients compared to the general population.
- Approximately 70% of deaths in bronchiectasis patients are due to respiratory causes, while about 30% are attributed to non-respiratory events.
Proper management, including airway clearance techniques, appropriate antibiotic therapy, and addressing the underlying cause, can significantly reduce complications and improve long-term outcomes for patients with bronchiectasis.
7. Diagnosis & Testing
Common Diagnostic Procedures
The diagnosis of bronchiectasis typically involves several steps and procedures:
Medical History:
- Evaluation of symptoms: chronic cough, sputum production, recurrent respiratory infections
- Family history of lung diseases
- History of conditions associated with bronchiectasis
- Assessment of potential exposures or risk factors
Physical Examination:
- Chest examination often reveals crackles (75% of patients) and wheezing (22% of patients) on auscultation.
- Assessment for clubbing of fingers (rare but significant sign)
- Evaluation of general health status
Sputum Analysis:
- Collection of sputum samples to check for viruses, bacteria, or other microorganisms.
- Assessment of sputum characteristics (volume, color, consistency)
Medical Tests
Several diagnostic tests are essential for confirming bronchiectasis and evaluating its extent and severity:
Imaging Studies:
- High-Resolution Computed Tomography (HRCT):
- A chest CT scan is the most common and definitive test for diagnosing bronchiectasis because a chest X-ray does not provide enough detail.
- HRCT can show the extent and location of lung damage, identifying dilated airways, thickened airway walls, and mucus plugging.
- Chest X-ray:
- Less sensitive than HRCT but may show abnormalities in more advanced cases
- Often used as an initial screening tool
- High-Resolution Computed Tomography (HRCT):
Pulmonary Function Tests:
- Spirometry to assess airflow limitation
- Lung volumes measurement
- Diffusion capacity testing to evaluate gas exchange
- Bronchodilator reversibility testing
Microbiological Testing:
- Sputum cultures to identify pathogens colonizing the airways, with Pseudomonas aeruginosa (found in 12% of patients), Staphylococcus aureus (6%), Mycobacterium avium complex (4%), and Aspergillus species (4%) being among the most common organisms.
- Specific testing for mycobacteria (including tuberculosis)
- Fungal cultures when appropriate
Blood Tests:
- Complete blood count to assess for inflammation or infection
- Immunoglobulin levels to rule out immunodeficiency
- Specific antibody responses to vaccines
- Alpha-1 antitrypsin levels
- Inflammatory markers (C-reactive protein, erythrocyte sedimentation rate)
- Rheumatoid factor and other autoimmune markers when indicated
Specialized Tests (based on clinical suspicion):
- Sweat chloride test and genetic testing for cystic fibrosis
- Ciliary function tests for primary ciliary dyskinesia
- Bronchoscopy to obtain samples, assess for structural abnormalities, or remove foreign bodies
- pH monitoring for gastroesophageal reflux
- Allergy testing for allergic bronchopulmonary aspergillosis
Early Detection Methods and Effectiveness
Early detection of bronchiectasis is crucial for implementing treatments that can prevent disease progression. The effectiveness of various detection methods varies:
High-Resolution CT Scanning:
- The most effective method for early detection
- Can identify bronchiectasis before it becomes clinically apparent
- Sensitivity approaches 100% for established bronchiectasis
Clinical Screening:
- Screening patients with chronic productive cough lasting more than 8 weeks
- Evaluating patients with recurrent lower respiratory tract infections (3+ per year)
- Assessing patients with unexplained hemoptysis
Targeted Screening of High-Risk Populations:
- Patients with primary immunodeficiencies
- Individuals with chronic respiratory symptoms and a history of severe childhood infections
- Patients with autoimmune diseases associated with bronchiectasis
- Those with a family history of bronchiectasis or related genetic conditions
Biomarkers:
- Currently limited role in clinical practice
- Research into inflammatory markers and genetic signatures is ongoing
- May become more important in the future for early detection
Challenges in Early Detection:
- Bronchiectasis remains underdiagnosed with an average of 5- to 10-year delays from symptom onset, often initially misattributed to asthma or chronic obstructive pulmonary disease.
- Symptoms overlap with other common respiratory conditions
- Access to HRCT may be limited in some healthcare settings
- Lack of awareness among healthcare providers
Early detection is associated with better outcomes as it allows for prompt initiation of airway clearance techniques, targeted antimicrobial therapy, and management of underlying conditions. The earlier bronchiectasis is detected, the greater the opportunity to prevent further airway damage and preserve lung function.
8. Treatment Options
Standard Treatment Protocols
The management of bronchiectasis follows a multidisciplinary approach with several key components:
Airway Clearance Techniques:
- Airway clearance techniques are fundamental in bronchiectasis management to reduce symptom burden and improve quality of life.
- Methods include:
- Postural drainage
- Active cycle of breathing techniques
- Oscillatory positive expiratory pressure devices (e.g., Flutter, Acapella)
- Chest physiotherapy
- High-frequency chest wall oscillation vests
- Typically performed daily, with increased frequency during exacerbations
Infection Management:
- Prompt treatment of acute exacerbations with antibiotics
- Selection of antibiotics based on sputum culture results and local resistance patterns
- Course length typically 14 days
- Consideration of intravenous antibiotics for severe exacerbations
Chronic Infection Control:
- Pseudomonas aeruginosa eradication therapy when first detected
- Long-term suppressive antibiotic strategies for frequent exacerbations
- Rotation of antibiotics to prevent resistance development
Anti-inflammatory Approaches:
- Macrolide antibiotics for their anti-inflammatory properties
- Inhaled corticosteroids in select patients (particularly those with eosinophilic inflammation)
Bronchodilator Therapy:
- Short and long-acting bronchodilators for patients with airflow obstruction
- Combination therapy when appropriate
Treatment of Underlying Causes:
- Specific therapy for identified etiologies (e.g., immunoglobulin replacement for immunodeficiency)
- Management of comorbidities (GERD, sinusitis, etc.)
Supportive Care:
- Pulmonary rehabilitation programs
- Nutritional support
- Vaccination against pneumococcal disease and annual influenza
Medications, Surgeries, and Therapies
Medications
Antibiotics:
- For Acute Exacerbations:
- Oral options: amoxicillin-clavulanate, doxycycline, fluoroquinolones, azithromycin
- Intravenous options for severe cases: anti-pseudomonal penicillins, cephalosporins, aminoglycosides
- Long-term Suppressive Therapy:
- Macrolide antibiotics (azithromycin, erythromycin, clarithromycin) have shown benefits in reducing exacerbation rates.
- Inhaled antibiotics (tobramycin, colistin, aztreonam) for patients with chronic Pseudomonas infection.
- Rotating oral antibiotics in some cases
- For Acute Exacerbations:
Anti-inflammatory Medications:
- Macrolides (for their immunomodulatory effects)
- Inhaled corticosteroids in specific phenotypes
- Oral corticosteroids (short courses during severe exacerbations)
Bronchodilators:
- Short-acting beta-agonists (e.g., albuterol)
- Long-acting beta-agonists (e.g., formoterol, salmeterol)
- Long-acting muscarinic antagonists (e.g., tiotropium)
- Combination inhalers when appropriate
Mucoactive Agents:
- Hypertonic saline to improve mucus clearance
- N-acetylcysteine in selected cases
- Dornase alfa typically avoided in non-CF bronchiectasis
Surgeries
Surgical intervention is considered in specific circumstances:
Localized Disease:
- Surgery is usually only considered for bronchiectasis in rare cases where other treatments have not been effective, the damage to the bronchi is confined to a small area, and the patient is in good general health.
- Resection of a lobe or segment with severe, localized bronchiectasis unresponsive to medical management
Massive Hemoptysis:
- One of the most serious complications of bronchiectasis is coughing up large amounts of blood, caused by one of the blood vessels in the lungs splitting. This can be life-threatening and may require emergency surgery.
- Bronchial artery embolization is often attempted before surgical resection
Lung Transplantation:
- Considered for end-stage bronchiectasis with respiratory failure
- Reserved for patients with severe disease unresponsive to maximal medical therapy
Therapies
Pulmonary Rehabilitation:
- Structured exercise programs
- Education about disease management
- Breathing techniques
- Energy conservation strategies
Oxygen Therapy:
- Supplemental oxygen for patients with chronic hypoxemia
- Ambulatory oxygen for those who desaturate with exertion
Airway Clearance Support:
- A recent ERS statement highlighted airway clearance techniques as the key management strategy to improve mucus clearance and reduce exacerbations in adults with bronchiectasis.
- Respiratory physiotherapy
- Mechanical devices for home use
Emerging Treatments and Clinical Trials
The field of bronchiectasis is experiencing unprecedented growth in research and development of new therapies:
Novel Anti-inflammatory Approaches:
- Dipeptidyl peptidase-1 (DPP1) inhibitors, such as brensocatib, which reduce neutrophil serine proteases and showed promising results in reducing exacerbations in clinical trials.
- Biological medications targeting eosinophilic inflammation in the approximately 20% of bronchiectasis patients with this inflammatory phenotype.
Targeted Antimicrobial Therapies:
- New inhaled antibiotics in development, including Colistimethate sodium and AP-PA02.
- Bacteriophage therapy for resistant bacterial infections
- Novel antibiotic formulations with improved lung penetration
Mucoactive Agents:
- Novel mucolytic agents like AROMUC 5AC and SPL 5AC are under investigation.
- Compounds targeting specific aspects of mucus rheology
Genetic and Molecular Approaches:
- CFTR modulators being studied in patients with single mutant CFTR genes (heterozygotes).
- Therapies targeting ciliary function for primary ciliary dyskinesia
Immunomodulators:
- Biologics like Benralizumab and Itepekimab are being studied for bronchiectasis.
- Therapies targeting specific inflammatory pathways
Recent Clinical Trial Developments:
- In May 2024, Insmed Incorporated announced positive topline results from the ASPEN study, a Phase III study of brensocatib in patients with non-cystic fibrosis bronchiectasis.
- In July 2024, Armata Pharmaceuticals achieved full enrollment in its Tailwind Phase II clinical study of inhaled AP-PA02 in patients with bronchiectasis and chronic Pseudomonas aeruginosa infection.
Biomarker-Based Treatment Approaches:
- Research into biomarker-based stratification of patients to enable more personalized treatment approaches.
- Development of endotype-specific therapies
The future of bronchiectasis treatment is moving toward a more personalized approach, with therapies targeting specific disease mechanisms and patient phenotypes. The increasing interest from pharmaceutical companies and the growing number of clinical trials offer hope for improved management options in the coming years.
9. Prevention & Precautionary Measures
Prevention Strategies
While bronchiectasis cannot always be prevented, several strategies can reduce the risk of developing the condition:
Childhood Vaccination:
- The prevalence of severe cystic bronchiectasis has decreased because of the introduction of vaccination against childhood infections.
- Vaccines against measles, pertussis, pneumococcal disease, and Haemophilus influenzae type b have significantly reduced cases of post-infectious bronchiectasis.
Prompt Treatment of Respiratory Infections:
- Early and effective treatment of pneumonia, tuberculosis, and other respiratory infections
- Complete prescribed antibiotic courses to prevent complicated or prolonged infections
Early Diagnosis and Management of Predisposing Conditions:
- Timely identification and treatment of conditions that can lead to bronchiectasis:
- Immunodeficiencies
- Aspiration risk
- Foreign body aspiration (especially in children)
- Allergic bronchopulmonary aspergillosis
- Timely identification and treatment of conditions that can lead to bronchiectasis:
Preventing Foreign Body Aspiration:
- Child safety measures to prevent choking and aspiration
- Proper swallowing precautions for those at risk of aspiration
Tuberculosis Control:
- Public health measures for TB detection and treatment
- Contact tracing and prophylactic treatment when indicated
Lifestyle Changes and Environmental Precautions
Several lifestyle modifications and environmental precautions can help prevent bronchiectasis or slow its progression:
Smoking Cessation:
- Avoidance of tobacco smoke (both active smoking and secondhand exposure)
- Support programs for smoking cessation
Air Quality Management:
- Reducing exposure to indoor and outdoor air pollutants
- Use of air purifiers when appropriate
- Avoidance of occupational respiratory hazards
- Proper ventilation in living and working spaces
Respiratory Hygiene:
- Regular handwashing to prevent respiratory infections
- Avoiding close contact with people who have respiratory infections
- Proper cough etiquette
General Health Maintenance:
- Maintaining adequate hydration to help thin mucus
- Balanced nutrition to support immune function
- Regular physical activity to maintain lung function and overall health
- Stress management techniques
Occupational Considerations:
- Use of appropriate respiratory protection in high-risk occupations
- Workplace assessments and modifications for those with established disease
- Consideration of career changes in severe cases with ongoing harmful exposures
Vaccines and Preventive Screenings
Several vaccines and screening approaches are recommended for preventing bronchiectasis and its complications:
Recommended Vaccines:
- Pneumococcal vaccines to protect against Streptococcus pneumoniae
- Annual influenza vaccination
- Pertussis (whooping cough) vaccination and boosters
- Other routine childhood vaccines to prevent infections that can lead to bronchiectasis
- COVID-19 vaccination
Preventive Screenings:
- Early investigation of chronic cough (lasting more than 8 weeks)
- Evaluation of recurrent respiratory infections (three or more per year)
- Screening of family members of patients with genetic conditions associated with bronchiectasis
- Consideration of CT screening in high-risk populations (e.g., certain indigenous populations with high prevalence)
Regular Monitoring for Those at Risk:
- Pulmonary function testing for individuals with conditions predisposing to bronchiectasis
- Sputum surveillance cultures for those with established disease to detect new pathogens early
- Regular clinical assessment for early symptoms
Healthcare Provider Education:
- Increased awareness among primary care providers about bronchiectasis
- Low threshold for investigation of suspicious symptoms
- Recognition that bronchiectasis is often misdiagnosed as asthma or COPD, leading to delays in proper treatment
By implementing these preventive strategies and maintaining vigilance for early signs of bronchiectasis, many cases can be prevented or diagnosed at an earlier, more treatable stage. This is particularly important in high-risk populations and in regions where the disease burden is substantial.
10. Global & Regional Statistics
Incidence and Prevalence Rates Globally
Bronchiectasis prevalence varies significantly worldwide, with increasing recognition and diagnosis in recent years:
Global Overview:
- Once considered rare, bronchiectasis is now recognized as a significant global health issue
- Prevalence has been increasing across most studied regions, partly due to improved detection and longer life expectancy
Western Countries:
- United States:
- According to US healthcare claims data, bronchiectasis prevalence increased from over 500 per 100,000 persons in 2000 to over 800 per 100,000 persons in 2007.
- United Kingdom:
- A UK study found prevalence in men was 486/100,000 and 566/100,000 in women, with highest rates in patients over 60 years of age.
- Between 2004 and 2013, the point prevalence in women increased from 350.5/100,000 to 566.1/100,000 and in men from 301.2/100,000 to 485.5/100,000.
- The incidence also increased during this period, from 21.2/100,000 person-years to 35.2/100,000 person-years in women, and from 18.2/100,000 person-years to 26.9/100,000 person-years in men.
- United States:
Asia-Pacific Region:
- China:
- The prevalence of bronchiectasis in Chinese adults increased 2.31-fold, from 75.48 per 100,000 in 2013 to 174.45 per 100,000 in 2017.
- Australia and New Zealand:
- A study of Central Australian Aboriginal children found a prevalence of 1,470/100,000.
- Higher prevalence rates in Indigenous populations compared to non-Indigenous populations, with significant urban-rural differences (1800-3600 versus 500 per 100,000 in Australia).
- In New Zealand, reported prevalence is 3.7 per 100,000 population overall, but varies significantly by ethnicity.
- China:
Developing Regions:
- Limited data available from Africa, South America, and parts of Asia
- Higher suspected prevalence in regions with high tuberculosis burden
- Studies indicate bronchiectasis is likely underdiagnosed in several areas of the globe.
Mortality and Survival Rates
Mortality associated with bronchiectasis varies by region, severity of disease, and available healthcare resources:
Overall Mortality:
- Studies show that patients with bronchiectasis have more than twice the mortality rate of the general population.
- In the UK, the age-adjusted mortality rate for women with bronchiectasis was 1437.7 per 100,000 compared to 635.9 per 100,000 in the general population. For men, the rates were 1914.6 per 100,000 versus 895.2 per 100,000.
Regional Variation in the UK:
- In 2012, of the 1,567 people who died from bronchiectasis in the UK, 123 were aged 15-64 and 1,444 were aged 65 and above.
- Higher mortality rates were observed in the North East, North West, East Midlands, West Midlands, and South East compared to the UK average.
- Lower death rates were noted in the East of England, London, and the South West.
Indigenous Populations:
- Mortality rates of Indigenous people with bronchiectasis in Australia ranged between 34.2% and 42.5%, with an estimated annual mortality of 4.5-7.5%.
- The mean age of death was 16-20 years lower in Indigenous compared to non-Indigenous people.
Prognostic Factors:
- Presence of Pseudomonas aeruginosa colonization significantly increases mortality risk
- Frequent exacerbations associated with higher mortality
- Concurrent COPD increases mortality risk
- All-cause mortality is higher in elderly patients and men with bronchiectasis.
- The risk of all-cause mortality is more prominent in those with airflow limitation and in smokers.
Country-wise Comparison and Trends
Regional variations in bronchiectasis prevalence, causes, and outcomes reveal important patterns:
Prevalence Patterns:
- Higher rates generally observed in countries with aging populations
- Significant variation between high-income and low/middle-income countries
- Higher prevalence in regions with historical tuberculosis burden
Etiology Differences:
Post-infectious causes:
- Predominant in Asia, particularly post-tuberculosis bronchiectasis
- A pan-Indian study identified post-infection (41%) as the primary cause, with post-tuberculous disease as the predominant etiology (29.8%)
Idiopathic bronchiectasis:
- More common in Western countries
- Also highly prevalent in some Asian populations – studies from the Han population of mainland China found rates of idiopathic bronchiectasis at 66%
Genetic causes:
- Cystic fibrosis-related bronchiectasis more common in populations of European descent
- Primary ciliary dyskinesia prevalence varies by region
Microbiology Variations:
- Pseudomonas aeruginosa and Haemophilus influenzae are the most common bacteria detected in bronchiectasis airways globally, although proportions vary among different populations.
- Non-tuberculous mycobacteria more commonly isolated in the United States and East Asia
- Regional differences in antimicrobial resistance patterns
Healthcare Access and Outcomes:
- Limited access to healthcare and higher rates of acute respiratory infections linked to worse outcomes in certain populations.
- Significant differences in hospitalization rates and healthcare utilization between countries
- In England, higher rates of emergency admission were observed in the North East, North West, Yorkshire and the Humber, and the East Midlands compared with the UK average.
Trends Over Time:
- Increasing prevalence across most studied regions
- Shifting etiology from predominantly post-infectious to more diverse causes in developed countries
- Improving survival rates with better management strategies and earlier detection
- Development of national and international registries enhancing understanding of regional variations
These global and regional statistics highlight the complex and variable nature of bronchiectasis around the world. Understanding these patterns is crucial for developing appropriate public health strategies and targeted interventions for different populations and healthcare settings.
11. Recent Research & Future Prospects
Latest Advancements in Treatment and Research
The field of bronchiectasis has seen remarkable progress in recent years, with several key advancements:
Novel Anti-inflammatory Approaches:
- A new generation of anti-inflammatory therapies such as dipeptidyl peptidase-1/cathepsin C inhibitors are in advanced clinical development, based on a shift in understanding bronchiectasis as an inflammatory airway condition rather than just a problem of impaired mucociliary clearance.
- In May 2024, Insmed Incorporated announced positive topline results from the ASPEN study, a Phase III study of brensocatib in patients with non-cystic fibrosis bronchiectasis.
Targeted Antimicrobial Strategies:
- Development of new inhaled antibiotic formulations with improved lung penetration
- Armata Pharmaceuticals’ Phase II clinical study of inhaled AP-PA02 for patients with chronic Pseudomonas aeruginosa infection reached full enrollment in July 2024.
- Exploration of bacteriophage therapy for resistant infections
- Novel drug delivery systems for prolonged antibiotic release
Endotype-Based Treatment Approaches:
- Recognition that about 20% of bronchiectasis patients have eosinophil-predominant inflammation that may respond to asthma biologic medications.
- Discovery that primary ciliary dyskinesia is present in approximately 10% of adults with bronchiectasis, rather than the previously estimated 1-2%.
- Investigation of CFTR modulators for patients with single mutant CFTR genes.
Advanced Imaging Techniques:
- Functional MRI to assess ventilation heterogeneity
- PET-CT to identify areas of active inflammation
- Artificial intelligence applications for automated detection and quantification
Microbiome Research:
- Translational research into the microbiome to better understand the complex bacterial communities in bronchiectasis airways.
- Investigation of the role of the virome and mycobiome
- Exploration of potential microbiome-modulating therapies
Ongoing Studies and Future Medical Possibilities
Numerous studies and initiatives are currently underway, promising further advances in bronchiectasis management:
Clinical Trials of Novel Therapies:
- Over 15 companies are progressing through clinical trials with promising pipeline therapies including Colistimethate sodium, Benralizumab, Brensocatib, AP-PA02, Ensifentrine, HSK31858, ColiFin, and others.
- 30 Technology received approval for a Phase I/IIa trial evaluating nebulized Nitric Oxide Formulations in non-cystic fibrosis bronchiectasis patients with Pseudomonas Aeruginosa or other pathogens.
International Research Collaborations:
- Multinational, multicentre, prospective cohorts are now established worldwide, advancing understanding of bronchiectasis.
- The European Bronchiectasis Registry (EMBARC)
- The U.S. Bronchiectasis Research Registry
- The Australian Bronchiectasis Registry
- The China Bronchiectasis Registry (EMBACC)
Biomarker Development:
- Research focused on biomarker-based stratification of patients to enable personalized treatment approaches.
- Identification of predictive markers for treatment response
- Development of point-of-care tests for exacerbation management
Digital Health Applications:
- Remote monitoring technologies for early detection of exacerbations
- Mobile applications for tracking symptoms and treatment adherence
- Telemedicine approaches to improve access to specialist care
Novel Mucoactive Therapies:
- Development of mucolytic agents like AROMUC 5AC and SPL 5AC.
- Research into compounds targeting specific aspects of mucus rheology
- Investigation of therapies to restore ciliary function
Potential Cures or Innovative Therapies Under Development
While a complete cure for bronchiectasis remains elusive, several innovative approaches hold promise for transforming treatment:
Regenerative Medicine Approaches:
- Stem cell therapies to regenerate damaged bronchial tissue
- Growth factors to promote airway repair
- Bioengineered tissues for severely damaged regions
Gene-Targeted Therapies:
- Research into CFTR modulator therapy for heterozygous CFTR mutations in non-CF bronchiectasis.
- Gene therapy approaches for primary ciliary dyskinesia
- RNA-based treatments targeting specific genetic causes
Precision Medicine Strategies:
- Development of biological drugs for patients with severe disease based on specific endotypes.
- Personalized treatment algorithms based on patient characteristics, microbiology, and inflammatory profiles
- Conceptualizing bronchiectasis as an inflammatory airway condition rather than just a problem of impaired mucociliary clearance leading to bacterial infection.
Immunomodulatory Approaches:
- Targeted biologics for specific inflammatory pathways
- Investigation of therapies like Itepekimab and AZD-0292 that target specific immune mechanisms.
- Vaccines against common bronchiectasis pathogens
Comprehensive Management Programs:
- Development of integrated care models
- Standardized pulmonary rehabilitation programs specific to bronchiectasis
- Patient education and self-management tools
The future of bronchiectasis research and treatment is evolving toward a precision medicine approach that recognizes the heterogeneity of the condition and tailors therapies to specific patient phenotypes and endotypes. With continued momentum, the concept of precision medicine in bronchiectasis will soon be a reality, offering a promising future for patients with this condition.
12. Interesting Facts & Lesser-Known Insights
Uncommon Knowledge About Bronchiectasis
Several fascinating aspects of bronchiectasis are not widely recognized:
Historical Perspective:
- René Laennec, who first described bronchiectasis, also invented the stethoscope and coined the term “melanose” (from Greek for “black”) to describe melanoma. He is considered the father of clinical auscultation.
- Laennec himself may have suffered from bronchiectasis based on his medical history of chronic cough, sputum production, and intermittent wheeze, which lasted for at least 20 years.
Changing Demographics:
- While historically more common in children due to post-infectious causes, bronchiectasis has evolved to become predominantly an adult disease in developed countries.
- Two-thirds of bronchiectasis cases are in women, but it’s more common in young boys than in girls.
Global Disparities:
- The prevalence of bronchiectasis in Indigenous populations of New Zealand and Australia is dramatically higher than in populations of European descent in the same regions.
- In New Zealand, Pacific children under 15 years have an estimated incidence rate of bronchiectasis of 17.8 per 100,000, compared to 4.8 for Māori and 1.5 for New Zealand European children.
Respiratory Microbiome:
- Unlike many infections where a single pathogen is identified, bronchiectasis involves complex microbial communities that interact and evolve over time.
- The composition of these microbial communities can predict disease progression and treatment response.
Sensory Impact:
- Many patients with bronchiectasis experience alterations in their sense of smell and taste, particularly during exacerbations.
- Some can “taste” when their infection is worsening before other symptoms develop.
Myths and Misconceptions vs. Medical Facts
Several misconceptions about bronchiectasis persist in both public and medical communities:
Myth: Bronchiectasis is always caused by tuberculosis or severe pneumonia. Fact: While these are important causes, many cases are associated with autoimmune conditions, allergic reactions, genetic disorders, or unknown causes (idiopathic).
Myth: Bronchiectasis is a single disease entity. Fact: Bronchiectasis is better understood as a common endpoint of multiple pathological processes with diverse underlying mechanisms, requiring individualized management approaches.
Myth: Bronchiectasis always leads to severe disability and shortened lifespan. Fact: Most people with bronchiectasis live a normal life span by managing their symptoms with a provider’s advice and medication, although the condition does require ongoing management.
Myth: All patients with bronchiectasis should avoid exercise. Fact: Regular physical activity is generally beneficial for bronchiectasis patients, improving airway clearance, exercise tolerance, and quality of life. Pulmonary rehabilitation programs are recommended for many patients.
Myth: Inhaled corticosteroids should be avoided in all bronchiectasis patients. Fact: While historically avoided due to concerns about infection risks, the potential benefits of treating eosinophilic inflammation with inhaled corticosteroids in certain phenotypes is being reevaluated.
Myth: Bronchiectasis is immediately obvious on a chest X-ray. Fact: High-resolution CT scanning is the gold standard for diagnosis. Chest X-rays often miss early or mild bronchiectasis.
Impact on Specific Populations or Professions
Bronchiectasis affects certain populations and professions in unique ways:
Indigenous Populations:
- Indigenous populations in Australia and New Zealand experience significantly higher rates of bronchiectasis, with earlier onset and more severe disease.
- Limited access to healthcare and higher rates of acute respiratory infections contribute to these disparities.
Socioeconomic Impact:
- Figures for 2004-12 show that the chances of being diagnosed with bronchiectasis in the UK increase with better socioeconomic status, likely reflecting access to diagnostic services rather than true disease prevalence.
Occupational Considerations:
- Workers in dusty environments (mining, construction, agriculture) with bronchiectasis may experience accelerated disease progression.
- Musicians who play wind instruments often develop specialized techniques to manage their condition.
- Singers with bronchiectasis face unique challenges but can often adapt with proper training and management.
Maternal Health:
- Women with bronchiectasis can generally have successful pregnancies, but require careful management due to physiological changes during pregnancy that can affect mucus clearance and respiratory function.
- Genetic counseling may be important for those with hereditary forms of bronchiectasis.
Competitive Sports:
- Several professional athletes have competed successfully despite having bronchiectasis, demonstrating that with proper management, high-level physical performance is possible.
- Swimming is often particularly beneficial for people with bronchiectasis, combining exercise with the humidity that helps moisturize airways.
These lesser-known aspects of bronchiectasis highlight the complexity of the condition and the importance of personalized, holistic approaches to management that consider the individual’s unique circumstances, needs, and goals. As awareness of bronchiectasis continues to grow, addressing these misconceptions and understanding these nuances will be increasingly important for both healthcare providers and patients.