
⚠️ Disclaimer: The information provided in this article is for educational purposes only and does not constitute medical advice. RevisionTown does not provide diagnosis, treatment, or medical recommendations. Always consult a qualified healthcare professional regarding any medical condition, symptoms, or concerns.
Read More – 🏥 Medical Disclaimer
Comprehensive Report on Bladder Cancer Symptoms
1. Overview
What is Bladder Cancer?
Bladder cancer is a malignant neoplasm that develops in the tissues of the urinary bladder, the hollow muscular organ that stores urine before it is expelled from the body. It typically begins in the cells (urothelial cells) that line the inside of the bladder. The symptoms of bladder cancer are various manifestations that occur as a result of this malignant growth, ranging from urinary changes to systemic effects in advanced stages.
Affected Body Parts/Organs
Bladder cancer primarily affects the urinary bladder, but can also involve:
- The urethra (the tube through which urine exits the body)
- The ureters (tubes that carry urine from the kidneys to the bladder)
- Surrounding pelvic tissues and muscles
- Nearby organs such as the prostate in men or the uterus and vagina in women
- Lymph nodes in the pelvis and beyond
- Distant organs such as the lungs, liver, and bones in advanced metastatic cases
The symptoms experienced correlate with the location and extent of cancer involvement within these structures.
Prevalence and Significance
Bladder cancer represents a significant global health concern:
- It is the 10th most common cancer worldwide
- Approximately 573,000 new cases diagnosed globally each year
- About 213,000 deaths annually attributed to bladder cancer
- In the United States, over 81,000 new cases and 17,000 deaths annually
- 4th most common cancer in men, less common in women
- Approximately 75% of cases are diagnosed as non-muscle-invasive bladder cancer (NMIBC)
- 25% present as muscle-invasive or metastatic disease
The significance of recognizing bladder cancer symptoms lies in the potential for early detection:
- When diagnosed at early stages, the 5-year survival rate exceeds 95%
- If detected after spreading to nearby tissues or lymph nodes, 5-year survival drops to about 36%
- Late detection with distant metastasis has a 5-year survival rate of only 5%
- Bladder cancer has one of the highest lifetime treatment costs per patient of all cancers due to high recurrence rates and the need for lifelong surveillance
The early symptoms of bladder cancer are often subtle but recognizable, making awareness crucial for timely diagnosis and improved outcomes.
2. History & Discoveries
First Identification of Bladder Cancer Symptoms
The recognition of bladder cancer and its symptoms has a long history:
Ancient Times: Egyptian papyri from 1500 BCE contained descriptions of urinary conditions that may have included bladder cancer, including hematuria (blood in urine).
Hippocratic Era (circa 400 BCE): Greek physicians documented conditions of the bladder including tumors, noting symptoms such as painful urination and blood in the urine.
Middle Ages: Persian physician Avicenna (980-1037 CE) described bladder tumors and their symptoms in his medical encyclopedia “The Canon of Medicine.”
18th Century: The first detailed clinical description of bladder tumors was published by Italian anatomist Giovanni Battista Morgagni in 1761, who described both the gross appearance of bladder tumors and associated symptoms.
19th Century: In 1838, Joseph-Claude-Anthelme Récamier performed one of the first documented surgical procedures for bladder cancer removal after diagnosis based on hematuria and other urinary symptoms.
Key Figures in the History of Bladder Cancer
No single individual “discovered” bladder cancer, but several key figures advanced understanding of the disease and its symptoms:
Ludwig Rehn (1849-1930): German surgeon who first established the link between aniline dye exposure and bladder cancer in 1895, noting the unusual frequency of bladder tumors among dye workers. This was one of the first occupational cancers identified and led to increased attention to bladder cancer symptoms among high-risk populations.
Max Nitze (1848-1906): Developed the first practical cystoscope in 1877, revolutionizing the ability to visualize bladder tumors directly and correlate symptoms with visual findings.
Hugh Hampton Young (1870-1945): American urologist who developed surgical techniques for bladder cancer and improved understanding of symptom patterns associated with different tumor locations within the bladder.
Willem F. Wassink: In 1911, reported on the higher incidence of bladder cancer among workers in the aniline dye industry, further confirming the environmental links and associated symptom profiles.
Major Discoveries and Breakthroughs
1877: Invention of the cystoscope by Max Nitze allowed direct visualization of bladder tumors, transforming the understanding of how tumor characteristics corresponded to specific symptoms.
1895: Ludwig Rehn established the connection between chemical exposures and bladder cancer, leading to the first occupational safety measures and increased attention to early symptoms among at-risk workers.
1930s-1940s: Development of transurethral resection techniques for bladder tumors, which allowed for better understanding of the correlation between tumor stage and symptom presentation.
1956: Introduction of urine cytology by Papanicolaou and Marshall enabled non-invasive detection of bladder cancer cells, complementing symptom assessment.
1970s: Recognition of carcinoma in situ (CIS) as a high-risk, often symptomatically subtle form of bladder cancer that could present with irritative urinary symptoms without visible tumors.
1976: Introduction of intravesical BCG (Bacillus Calmette-Guérin) immunotherapy for non-muscle invasive bladder cancer, which dramatically changed symptom management and disease progression.
1990s: Development of improved tumor markers and molecular testing for bladder cancer, enhancing understanding of symptom-disease correlations.
2000s: Introduction of enhanced cystoscopy techniques (blue light, narrow band imaging) improving visualization of tumors that might cause symptoms but be difficult to detect with conventional methods.
Evolution of Medical Understanding
The understanding of bladder cancer symptoms has evolved significantly:
Early 20th Century: Symptoms were primarily recognized in advanced disease – gross hematuria, pain, and urinary obstruction were the classic triad, often indicating advanced disease.
Mid-20th Century: With improved cystoscopy, physicians began recognizing earlier manifestations and the intermittent nature of symptoms like hematuria.
1960s-1970s: Growing recognition that irritative voiding symptoms (urgency, frequency) could be indicators of certain bladder cancer types, particularly carcinoma in situ.
1980s-1990s: Better understanding of symptom patterns associated with different tumor locations within the bladder (e.g., trigone tumors causing more irritative symptoms).
2000-2010: Recognition of the importance of microscopic hematuria as an early symptom warranting investigation, with development of guidelines for evaluation.
2010-Present: Increased understanding of the molecular subtypes of bladder cancer and how they might present with different symptom patterns or progression rates.
Current Understanding: Recognition that women and elderly patients often experience delays in diagnosis despite presenting with classic symptoms, due to attribution of symptoms to other conditions (urinary tract infections, overactive bladder).
The evolution has moved from recognizing only obvious late-stage symptoms to a more nuanced understanding of subtle early manifestations, symptom patterns specific to tumor types, and the importance of symptom persistence even when mild.
3. Symptoms
Early Symptoms
Early bladder cancer often produces noticeable symptoms, though they may be intermittent and easily attributed to other conditions:
Blood in Urine (Hematuria)
- Gross hematuria (visible blood): Most common and earliest presenting symptom in 80-90% of patients
- Can range from slightly pink-tinged to bright red or dark brown urine
- Often painless and intermittent, appearing then disappearing for weeks or months
- May contain blood clots in some cases
- Microscopic hematuria (only detectable through urinalysis): Present in many early cases
Changes in Urination
- Increased urinary frequency: Needing to urinate more often than usual
- Urgency: Sudden, compelling need to urinate
- Dysuria: Painful or burning sensation during urination
- Nocturia: Increased need to urinate at night
- Difficulty starting the urinary stream
- Weakened or interrupted urinary stream
Other Early Symptoms
- Pelvic discomfort or pressure (usually mild)
- Lower back pain on one side (if tumor is blocking a ureter)
- Feeling of incomplete bladder emptying
- Urinary tract infection (UTI) symptoms that don’t resolve with antibiotics or recur quickly
Advanced-Stage Symptoms
As bladder cancer progresses and invades deeper tissues or spreads to other organs, more severe symptoms develop:
Locally Advanced Disease
- Persistent pelvic pain or pressure
- Severe or constant back pain
- Inability to urinate despite the urge (complete obstruction)
- Edema (swelling) in the lower extremities due to lymphatic or venous obstruction
- Abdominal distension or palpable mass
- Fistula formation (abnormal connections between bladder and other organs)
- Pneumaturia: Air in urine due to colovesical fistula
- Fecaluria: Fecal material in urine
- Vaginal leakage of urine in women (vesicovaginal fistula)
Metastatic Disease
- Unintentional weight loss
- Fatigue and weakness
- Loss of appetite
- Bone pain (often in pelvis, ribs, or vertebrae) from bone metastases
- Cough, shortness of breath, or hemoptysis (with lung metastases)
- Jaundice or abdominal pain (with liver metastases)
- Swelling of lymph nodes, particularly in the neck (Virchow’s node)
- Generalized malaise
- Night sweats
- Anemia symptoms (dizziness, weakness, pale skin)
Paraneoplastic Symptoms In rare cases, bladder cancer can cause paraneoplastic syndromes with symptoms seemingly unrelated to the urinary tract:
- Hypercalcemia (high blood calcium): Confusion, constipation, excessive thirst
- Hypercoagulability: Blood clots in legs or lungs
- Dermatomyositis: Muscle weakness and characteristic skin rash
- Peripheral neuropathy: Numbness, tingling, or weakness in extremities
Common vs. Rare Symptoms
Common Symptoms (Present in >30% of patients)
- Hematuria (80-90% of cases)
- Urinary frequency (30-40%)
- Urinary urgency (30-35%)
- Dysuria (30%)
- Pelvic discomfort (20-30%)
Less Common Symptoms (10-30% of patients)
- Recurrent UTI-like symptoms (15-20%)
- Lower back pain (15-20%)
- Flank pain (10-15%)
- Urinary hesitancy (10-15%)
- Incomplete emptying sensation (10-15%)
Rare Symptoms (<10% of patients)
- Pneumaturia (air in urine) (1-3%)
- Fecaluria (fecal material in urine) (1-2%)
- Urinary fistulas (2-3%)
- Paraneoplastic syndromes (<5%)
- Lower extremity edema without metastasis (5-8%)
- Spontaneous bladder perforation (<1%)
- Urinary retention as initial presentation (5-10%)
Symptom Progression Over Time
The progression of bladder cancer symptoms typically follows patterns that correlate with disease advancement:
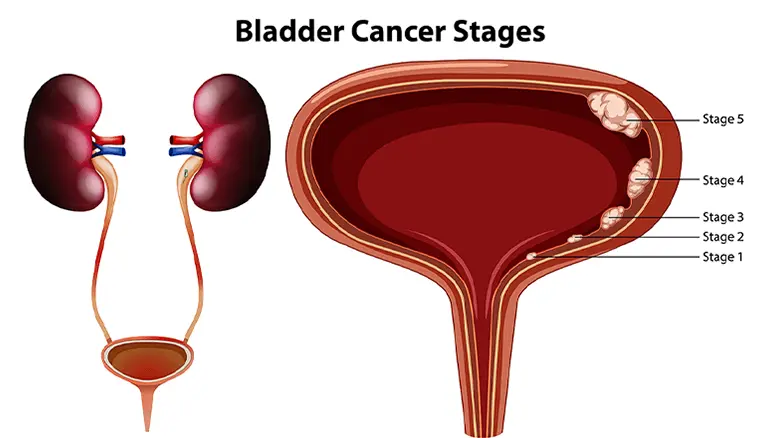
Stage 0-I (Non-muscle invasive)
- Often begins with intermittent, painless hematuria
- Potential for urinary frequency or urgency, especially with carcinoma in situ
- Symptoms may completely resolve spontaneously, then recur weeks or months later
- Duration: Symptoms can come and go for 6-12 months before diagnosis
Stage II (Muscle invasive)
- Hematuria becomes more frequent and persistent
- Increased urinary symptoms (frequency, urgency, dysuria)
- Development of pelvic discomfort or pressure
- Symptoms less likely to completely resolve without treatment
- Duration: Typically progresses over 3-6 months if untreated
Stage III (Locally advanced)
- Development of flank pain if ureters are obstructed
- More persistent and severe pelvic pain
- Potential urinary obstruction symptoms
- Constitutional symptoms begin (fatigue, weight loss)
- Duration: Progression typically occurs within 2-4 months if untreated
Stage IV (Metastatic)
- Systemic symptoms predominate (weight loss, fatigue, anemia)
- Symptoms specific to sites of metastasis emerge
- Original urinary symptoms may actually become less prominent as systemic disease advances
- Duration: Rapid progression typically within weeks to months
Special Symptom Patterns
- Carcinoma in situ: Often presents with irritative symptoms (frequency, urgency, dysuria) rather than hematuria
- Trigone tumors: Tend to cause more irritative symptoms and potential urinary obstruction earlier
- Dome tumors: May cause less urinary symptoms until larger, sometimes presenting with abdominal discomfort
- Diverticular tumors: Can cause minimal symptoms until advanced, leading to delayed diagnosis
The recognition of these symptom patterns and their progression is crucial for prompt medical evaluation, as earlier intervention consistently correlates with better outcomes.
4. Causes
Biological Causes
Bladder cancer, like other malignancies, results from genetic alterations that disrupt normal cellular regulation. These alterations lead to the development of symptoms as the abnormal cells proliferate and interact with surrounding tissues:
Genetic and Molecular Mechanisms
- Chromosomal abnormalities: Deletions in chromosomes 9, 11, 13, and 17 are common
- Oncogene activation: FGFR3 mutations (common in low-grade tumors)
- Tumor suppressor gene inactivation:
- TP53 mutations (common in muscle-invasive disease)
- RB1 (retinoblastoma) gene alterations
- CDKN2A (p16) inactivation
- DNA repair gene defects: ERCC2, ATM, and other genes involved in maintaining genomic stability
- Telomerase activation: Allowing cancer cells to divide indefinitely
- Epigenetic alterations: DNA methylation changes affecting gene expression
Cellular Pathways Affected
- Cell cycle regulation disruption
- Apoptosis (programmed cell death) inhibition
- Angiogenesis (new blood vessel formation) promotion
- Cellular adhesion molecule alterations allowing invasion
- Immune evasion mechanisms
Symptom Development Mechanisms
- Hematuria results from tumor vascularity and friability
- Irritative urinary symptoms arise from inflammation and nerve irritation
- Pain develops from invasion into bladder wall with nerve involvement
- Obstruction symptoms occur from physical blockage of urine flow
- Constitutional symptoms result from inflammatory cytokines and metabolic demands
Environmental Causes
Environmental exposures account for a significant proportion of bladder cancer cases, with several well-established carcinogens:
Chemical Carcinogens
- Aromatic amines: Found in industrial chemicals, dyes, and rubber
- 2-Naphthylamine
- Benzidine
- 4-Aminobiphenyl
- o-Toluidine
- Polycyclic aromatic hydrocarbons: Present in combustion products
- Chlorination by-products in drinking water (trihalomethanes)
- Arsenic in drinking water in certain geographic regions
Tobacco Exposure
- Cigarette smoking is the most significant risk factor
- Contains over 60 known carcinogens that accumulate in urine
- Accounts for approximately 50-65% of all bladder cancer cases
- Smokers have 2-4 times higher risk than non-smokers
- Pipe and cigar smoking also increase risk, though less than cigarettes
Industrial Exposures
- Rubber manufacturing
- Leather tanning
- Textile dyeing
- Printing industry
- Hair dye production (especially before 1980)
- Aluminum production
- Truck driving (diesel exhaust exposure)
- Painters (solvent exposure)
Medications and Treatments
- Cyclophosphamide (chemotherapy drug)
- Pioglitazone (diabetes medication) with long-term use
- Phenacetin (painkillers containing this substance, now banned)
- Radiation therapy to the pelvis region
Genetic and Hereditary Factors
While most bladder cancer cases are not hereditary, genetic predisposition plays a role in some cases:
Hereditary Syndromes
- Lynch syndrome (hereditary non-polyposis colorectal cancer): 8x increased risk
- Cowden syndrome: PTEN gene mutations
- Retinoblastoma: RB1 gene mutations
Family History Impact
- First-degree relatives of bladder cancer patients have a 1.5-2x increased risk
- Suggests both shared genetic and environmental factors
- Stronger association in smoking families suggests gene-environment interactions
Genetic Polymorphisms
- N-acetyltransferase 2 (NAT2) slow acetylator phenotype: Reduces ability to detoxify carcinogens
- Glutathione S-transferase Mu 1 (GSTM1) null genotype: Impairs carcinogen detoxification
- APOBEC3 gene family variants: Affects DNA editing mechanisms
Known Triggers and Exposure Risks
Several specific triggers and exposure patterns have been associated with increased bladder cancer risk and subsequent symptoms:
Chronic Irritation
- Long-term catheterization: Creates chronic inflammation
- Bladder stones: Surface irritation and inflammation
- Chronic urinary tract infections: Inflammatory changes
- Schistosomiasis: Parasitic infection common in parts of Africa and the Middle East
- Bladder diverticula: Can harbor cancerous changes due to urine stasis
Fluid and Dietary Factors
- Inadequate fluid intake: Results in higher concentration of urinary carcinogens
- Arsenic in drinking water: Major problem in certain regions (Bangladesh, Chile, Taiwan)
- Low fruit and vegetable consumption: Reduced protective antioxidants
- High processed meat consumption: Contains nitrates and nitrites
Other Exposure Considerations
- Latency period: Typically 15-30 years between exposure and cancer development
- Dose-response relationship: Higher exposure levels and longer durations increase risk
- Synergistic effects: Combined exposures (e.g., smoking plus occupational exposure) multiply risk
Understanding these causal factors is essential for both prevention strategies and identifying high-risk individuals who might benefit from earlier or more intensive symptom evaluation and screening.
5. Risk Factors
Demographic Risk Factors
Age
- Median age at diagnosis: 73 years
- Rare before age 40 (less than 1% of cases)
- Incidence increases dramatically after age 55
- 90% of cases occur in individuals over 55 years
- Risk continues to increase with advancing age
Gender
- Men are 3-4 times more likely to develop bladder cancer than women
- However, women are often diagnosed at more advanced stages
- Women may experience longer delays in diagnosis due to symptoms being attributed to UTIs or gynecological conditions
- Despite lower incidence, women have a slightly worse prognosis stage-for-stage
Race and Ethnicity
- Highest incidence in Caucasians in North America and Europe
- In the US: White Americans have approximately twice the risk of African Americans
- Lower rates in Asian American and Hispanic/Latino populations
- However, non-white patients often present with more advanced disease
- Mortality rates are higher in African Americans despite lower incidence
Geographic Variation
- Highest rates in Southern and Eastern Europe, North America, and Egypt
- Lowest rates in Sub-Saharan Africa (excluding Egypt) and parts of Asia
- Regional variations reflect differences in tobacco use, occupational exposures, and endemic parasitic diseases
- Schistosomiasis (bladder parasites) in Egypt contributes to high rates and different histology (squamous cell carcinoma more common)
Environmental and Occupational Risk Factors
Tobacco Use
- Single most important risk factor
- Accounts for approximately 50-65% of cases in men and 20-30% in women
- Risk increases with:
- Duration of smoking (years)
- Intensity (cigarettes per day)
- Depth of inhalation
- Risk persists for 10-15 years after cessation but gradually decreases
- Second-hand smoke exposure increases risk by approximately 20-30%
Occupational Exposures
- Estimated to account for 5-25% of all cases
- Highest risk occupations:
- Rubber workers (1.5-3x increased risk)
- Painters (1.3x increased risk)
- Hairdressers/barbers (1.3-1.7x increased risk, particularly before 1980)
- Textile workers (1.7x increased risk)
- Aluminum production workers (1.6-2.8x increased risk)
- Truck drivers and diesel engine operators (1.2-1.5x increased risk)
- Metalworking occupations (1.3-2.0x increased risk)
- Leather workers (1.4-1.7x increased risk)
- Dry cleaners (1.4x increased risk)
- Chemical industry workers (1.9x increased risk)
- Latency period typically 15-30 years between exposure and cancer development
- Risk decreases after exposure cessation but never returns completely to baseline
Environmental Water Contaminants
- Arsenic in drinking water:
- Major risk factor in endemic areas (Bangladesh, parts of South America, Taiwan)
- Risk increases with concentration and duration of exposure
- 3-10x increased risk with high chronic exposure
- Chlorination byproducts:
- Trihalomethanes formed during water chlorination
- Modest increase in risk (1.4-1.5x) with long-term exposure to high levels
- Nitrates in drinking water from agricultural runoff
- Industrial pollutants in groundwater near manufacturing facilities
Radiation Exposure
- Pelvic radiation for other cancers increases bladder cancer risk
- Typically requires 5-10 year latency period
- Risk proportional to radiation dose
- Lifetime risk increase of approximately 1.5-4x depending on radiation dose
Genetic Risk Factors
While most bladder cancers are not inherited, certain genetic factors increase susceptibility:
Inherited Genetic Syndromes
- Lynch Syndrome (hereditary non-polyposis colorectal cancer): 8x increased risk
- Retinoblastoma: Increased risk due to RB1 gene mutations
- Cowden syndrome: PTEN mutations increase risk
Genetic Polymorphisms
- NAT2 slow acetylator phenotype: Reduced ability to detoxify aromatic amines, 1.4x increased risk
- GSTM1 null genotype: Impaired carcinogen detoxification, 1.5x increased risk
- APOBEC3 gene variants: DNA editing abnormalities, 1.2-1.5x increased risk
- Multiple polymorphisms in combination can multiply risk substantially
Family History
- First-degree relatives of bladder cancer patients have 1.5-2x increased risk
- Risk increases with:
- Multiple affected relatives
- Earlier age of onset in affected relatives
- Female relatives with bladder cancer (suggests stronger genetic component)
Impact of Pre-existing Conditions
Urological Conditions
- Chronic urinary tract infections: 2x increased risk with recurrent infections
- Urinary stones: 1.5-2.3x increased risk
- Bladder diverticula: 2-6x increased risk for tumors within diverticula
- Chronic indwelling catheters: 4-5x increased risk after 10+ years
- Neurogenic bladder: 1.5-2x increased risk
- Bladder exstrophy: 80x increased risk (rare congenital condition)
Other Medical Conditions
- Diabetes mellitus: 1.2-1.5x increased risk, higher with longer duration
- Chronic kidney disease: 1.3x increased risk
- Liver cirrhosis: 1.8x increased risk
- Prostate enlargement/hyperplasia: May mask early symptoms, delaying diagnosis
Iatrogenic Risk Factors
- Cyclophosphamide (chemotherapy): 5-7x increased risk, dose-dependent
- Pioglitazone for diabetes: 1.2-1.4x increased risk with >5 years of use
- Pelvic radiation: 1.5-4x increased risk
- Aristolochic acid (found in some herbal remedies): Strong association with urothelial cancers
Prior Bladder Cancer
- Highest risk factor for developing subsequent bladder cancer
- 50-70% recurrence rate for non-muscle invasive tumors
- Requires lifelong surveillance
- Risk factors for recurrence include:
- Multiplicity of original tumors
- Size >3cm
- High grade
- Presence of carcinoma in situ
- Incomplete initial resection
Understanding these risk factors is essential for both prevention strategies and identifying high-risk individuals who might benefit from earlier or more intensive screening and symptom evaluation. The synergistic effect of multiple risk factors significantly amplifies an individual’s likelihood of developing bladder cancer.
6. Complications
Direct Complications of Bladder Cancer Symptoms
Urinary Complications
- Urinary tract infections: Recurrent infections due to tumor disruption of normal bladder function
- Urinary retention: Inability to empty the bladder due to tumor obstruction or nerve involvement
- Hydronephrosis: Kidney swelling due to obstruction of ureter by tumor
- Renal insufficiency/failure: Progressive kidney damage from prolonged obstruction
- Bladder perforation: Rare but life-threatening rupture of bladder wall from tumor invasion
- Bladder hemorrhage: Severe bleeding requiring transfusion and/or intervention
Structural Complications
- Fistula formation: Abnormal connections between the bladder and other organs
- Vesicovaginal (bladder to vagina)
- Vesicoenteric (bladder to intestine)
- Vesicoskin (bladder to skin surface)
- Ureteral obstruction: Blockage of urine flow from kidneys to bladder
- Lymphatic obstruction: Lower extremity edema from lymph node involvement
- Venous obstruction: Pelvic or leg swelling from tumor pressure on veins
Metabolic and Systemic Complications
- Anemia: From chronic blood loss in hematuria
- Cachexia: Severe weight loss and muscle wasting in advanced disease
- Paraneoplastic syndromes: Rare systemic effects from tumor-produced substances
- Hypercalcemia
- Hypercoagulability (increased blood clotting)
- Neuropathies
Infection-Related Complications
- Urosepsis: Life-threatening infection spreading from urinary tract to bloodstream
- Pyelonephritis: Kidney infection from ascending bacteria
- Perivesical abscess: Collection of infected fluid around the bladder
Long-term Impact on Organs and Overall Health
Urinary System Impact
- Reduced bladder capacity: From tumor itself or treatment effects
- Bladder fibrosis: Stiffening of bladder wall from radiation or chronic inflammation
- Chronic kidney disease: From prolonged obstructive uropathy
- Urinary incontinence: Loss of normal bladder control function
- Recurrent urinary tract infections: From altered bladder anatomy and function
Impact on Surrounding Organs
- Bowel dysfunction: From tumor invasion or treatment effects
- Diarrhea
- Constipation
- Bowel obstruction
- Sexual dysfunction:
- In men: Erectile dysfunction from tumor or treatment
- In women: Vaginal stenosis, dryness, and dyspareunia
- Pelvic floor disorders: Weakness of supporting structures
Systemic Health Impact
- Chronic pain syndromes: Persistent pain after treatment
- Psychological effects:
- Anxiety and depression
- Body image concerns
- Fear of recurrence
- Nutritional deficiencies: From reduced appetite or absorption issues
- Osteoporosis: From hormonal changes after certain treatments
- Secondary malignancies: Increased risk from treatment (particularly radiation)
Treatment-Related Complications
- Post-cystectomy complications:
- Altered body image with external urinary diversion
- Vitamin B12 deficiency with ileal conduits
- Metabolic acidosis with urinary diversions
- Stomal complications (stenosis, herniation, prolapse)
- Post-radiation complications:
- Radiation cystitis (bladder inflammation)
- Proctitis (rectal inflammation)
- Small bowel strictures or obstructions
- Fistula formation
Disability and Fatality Rates
Functional Impairment
- 25-40% of bladder cancer survivors report moderate to severe urinary symptoms affecting daily life
- 30-50% experience sexual dysfunction following treatment
- 15-30% report chronic pelvic pain affecting activity levels
- Physical activity limitations reported by 40-60% of patients after cystectomy
- 20-30% require some form of assistance with daily activities after major treatment
Work and Productivity Impact
- Average time away from work: 3-6 months after major treatment
- 25-35% unable to return to previous employment after radical cystectomy
- Productivity loss estimated at $3.4 billion annually in the US alone
- Financial toxicity affects 30-50% of patients due to treatment costs and work disruption
Quality of Life Impact
- Significant impairment in overall quality of life, particularly with:
- External urinary diversions
- Advanced disease
- Multiple treatments for recurrence
- Psychological distress reported by 30-50% of patients
- Social isolation common due to concerns about urinary control
Mortality Data
Overall 5-year survival rates:
- All stages combined: Approximately 77%
- Non-muscle invasive (Stage 0-I): 88-98%
- Muscle invasive (Stage II): 63%
- Locally advanced (Stage III): 46%
- Metastatic (Stage IV): 15%
Annual mortality:
- Global: Approximately 213,000 deaths
- United States: About 17,000 deaths
- European Union: Approximately 52,000 deaths
Leading causes of death:
- Metastatic disease: 60-70%
- Treatment complications: 5-10%
- Comorbid conditions: 15-25%
Case fatality rate:
- Higher in developing countries (40-50%)
- Lower in developed countries (20-30%)
- Higher in women and racial minorities due to later-stage diagnosis
The complications of bladder cancer extend well beyond the primary disease, affecting multiple organ systems and significantly impacting quality of life. Early symptom recognition, prompt treatment, and comprehensive supportive care are essential to mitigate these complications and improve overall outcomes.
7. Diagnosis & Testing
Common Diagnostic Procedures
Initial Evaluation
Comprehensive history and physical examination:
- Detailed urinary symptom assessment
- Evaluation of risk factors
- Abdominal and pelvic examination
- Assessment of lymph nodes
- Digital rectal examination (men)
- Bimanual examination under anesthesia (if cystoscopy performed)
Urinalysis:
- Confirms presence of microscopic or gross hematuria
- Evaluates for infection or other urinary abnormalities
- First-line test when symptoms are present
Urine cytology:
- Examination of urine for cancer cells
- Higher sensitivity for high-grade tumors (70-90%)
- Lower sensitivity for low-grade tumors (30-50%)
- High specificity (>90%) when positive
- Often used in conjunction with cystoscopy
Endoscopic Procedures
Cystoscopy:
- Gold standard for diagnosis
- Direct visualization of the bladder interior using a flexible or rigid scope
- Can detect abnormalities not visible on imaging
- Allows for biopsy of suspicious areas
- Outpatient procedure usually performed under local anesthesia
- Enhanced techniques improve detection:
- Blue light/fluorescence cystoscopy
- Narrow band imaging
- Confocal laser endomicroscopy
Transurethral resection of bladder tumor (TURBT):
- Surgical procedure that serves both diagnostic and therapeutic purposes
- Removes visible tumor for pathological examination
- Assesses depth of invasion (staging)
- Performed under regional or general anesthesia
- Essential for accurate diagnosis and treatment planning
Medical Tests
Laboratory Tests
Complete blood count (CBC):
- May show anemia from chronic blood loss
- Elevated white blood cells may indicate infection
Comprehensive metabolic panel:
- Assesses kidney function (creatinine, BUN)
- Evaluates liver function
- Checks electrolyte balance
Urinary tumor markers:
- BTA (bladder tumor antigen) stat and TRAK:
- Sensitivity: 50-70%
- Specificity: 70-75%
- NMP22 (nuclear matrix protein 22):
- Sensitivity: 50-80%
- Specificity: 70-90%
- UroVysion FISH (fluorescence in situ hybridization):
- Detects chromosomal abnormalities
- Sensitivity: 70-86%
- Specificity: 65-85%
- ImmunoCyt/uCyt+:
- Sensitivity: 70-90%
- Specificity: 70-80%
- CxBladder:
- Measures expression of five mRNA markers
- Sensitivity: 82-91%
- Specificity: 85-91%
- BTA (bladder tumor antigen) stat and TRAK:
Imaging Studies
Computed Tomography (CT) Urography:
- Three-phase examination of the entire urinary tract
- Detects filling defects, wall thickening, and extravesical extension
- Evaluates upper urinary tract (kidneys, ureters)
- Assesses lymph nodes and potential metastatic sites
- Sensitivity: 85-95% for bladder tumors >5mm
- Limitations: Radiation exposure, contrast reactions
Magnetic Resonance Imaging (MRI):
- Provides excellent soft tissue contrast
- Better than CT for assessing depth of bladder wall invasion
- Multiparametric techniques improve accuracy
- Used when CT is contraindicated or for better local staging
- Sensitivity: 85-90% for muscle invasion
- Limitations: Cost, availability, contraindicated with certain implants
Ultrasound:
- Initial screening tool, especially in settings with limited resources
- Can detect larger tumors and assess hydronephrosis
- Non-invasive and no radiation exposure
- Sensitivity: 70-80% for tumors >5mm
- Limitations: Operator-dependent, less sensitive for small tumors
Intravenous Pyelogram (IVP):
- Less commonly used now, largely replaced by CT urography
- Shows filling defects in the bladder and upper tract
- Sensitivity: 60-70%
- Limitations: Less detailed, contrast reactions, radiation exposure
Additional Advanced Tests
Positron Emission Tomography (PET)/CT:
- Primarily used for evaluating metastatic disease
- Not routine for initial diagnosis
- Helps identify distant metastases not visible on conventional imaging
- Sensitivity: 80-90% for metastatic disease
- Limitations: Cost, false positives from inflammation
Bone scan:
- Used when bone metastases are suspected
- Indicated for patients with bone pain or elevated alkaline phosphatase
- Sensitivity: 80-95% for bone metastases
- Limitations: False positives from arthritis, trauma
Retrograde pyelography:
- Evaluates upper urinary tract when CT is inconclusive
- Direct contrast injection into ureters during cystoscopy
- Helpful for subtle ureteral abnormalities
Pathological Evaluation
Histopathological examination:
- Essential for definitive diagnosis
- Determines tumor type, grade, and stage
- Evaluates for presence of carcinoma in situ
- Assesses muscle invasion
Immunohistochemistry:
- Helps determine tumor subtype and origin
- Common markers include:
- GATA3, CK7, CK20, p63 (urothelial carcinoma)
- Uroplakin (urothelial differentiation)
- p53 (associated with aggressive disease)
- Ki-67 (proliferation marker)
Molecular testing:
- Increasingly used for prognostication and treatment planning
- FGFR3 mutation status
- p53 mutation analysis
- RNA expression profiling for molecular subtypes
- Genomic instability assessment
Early Detection Methods and Effectiveness
Screening Approaches and Effectiveness
General Population Screening:
- Not currently recommended due to:
- Relatively low incidence in general population
- High false positive rates
- Cost-effectiveness concerns
- Psychological impact of false positives
- May change as better biomarkers are developed
- Not currently recommended due to:
Risk-Based Screening:
- Recommended for high-risk individuals:
- Occupational exposure to known bladder carcinogens
- Heavy smokers (>30 pack-years)
- Patients with unexplained hematuria
- Patients with irritative urinary symptoms and risk factors
- Methods include:
- Annual urinalysis (sensitivity: 50-70%)
- Urine cytology (sensitivity: 40-90%, depending on tumor grade)
- Cystoscopy for highest-risk individuals
- Recommended for high-risk individuals:
Hematuria Evaluation:
- Most effective early detection approach
- American Urological Association recommends evaluation for:
- All patients with gross hematuria
- Adults >35 years with microscopic hematuria
- Risk-stratified approach based on risk factor profile
- Full evaluation includes:
- Cystoscopy
- Upper tract imaging
- Urine cytology
Early Detection Effectiveness
Stage at Diagnosis Impact:
- Non-muscle invasive: 5-year survival >90%
- Muscle invasive: 5-year survival 50-70%
- Locally advanced: 5-year survival 35-50%
- Metastatic: 5-year survival 5-15%
Hematuria Evaluation Effectiveness:
- Detects 90-95% of bladder cancers when properly performed
- Cost per cancer detected: $7,000-$10,000
- 12-18% of patients with gross hematuria are diagnosed with bladder cancer
- 2-5% of patients with microscopic hematuria are diagnosed with bladder cancer
Urinary Marker Limitations:
- All current markers have insufficient sensitivity as standalone tests
- False positives from:
- Urinary tract infections
- Stones
- Recent instrumentation
- Inflammatory conditions
- Complementary to, not replacements for, cystoscopy
Delayed Diagnosis Impact:
- Each month of delayed diagnosis increases risk of muscle-invasive disease by 1-3%
- Women experience 6-9 month longer delays in diagnosis on average
- Elderly patients (>80 years) experience 2-3 month longer delays
Future Directions in Early Detection
- Multi-marker panels: Combining complementary markers improves sensitivity
- Liquid biopsy approaches: Circulating tumor DNA in blood or urine
- Molecular urine tests: Gene expression and mutation analysis
- Artificial intelligence applications:
- Computer-aided detection during cystoscopy
- Pattern recognition in imaging studies
- Risk prediction models incorporating multiple variables
Early detection of bladder cancer remains challenging but critical for improved outcomes. While no perfect screening test exists, proper evaluation of urinary symptoms, particularly hematuria, provides the best opportunity for early diagnosis. Continued development of more sensitive and specific non-invasive tests holds promise for improving early detection in the future.
8. Treatment Options
Standard Treatment Protocols
Treatment approaches for bladder cancer are highly individualized based on stage, grade, and patient factors. The following represents standard treatment protocols by disease stage:
Non-Muscle Invasive Bladder Cancer (NMIBC) – Stage 0a, 0is, I
Initial Treatment:
- Transurethral resection of bladder tumor (TURBT)
- Complete removal of all visible tumors
- Deep resection to include muscularis propria layer
- Often followed by a re-resection in high-grade T1 tumors
- Transurethral resection of bladder tumor (TURBT)
Risk Stratification:
- Low Risk (solitary, small, low-grade Ta):
- Single immediate postoperative intravesical chemotherapy instillation
- Surveillance cystoscopy every 3-6 months initially
- Intermediate Risk (multiple or recurrent low-grade Ta):
- Induction intravesical therapy (typically 6 weekly treatments)
- Maintenance therapy for 6-12 months
- Surveillance cystoscopy every 3-4 months initially
- High Risk (T1, high-grade, CIS):
- BCG immunotherapy (induction and maintenance)
- Maintenance for 1-3 years
- Consideration of early cystectomy in highest-risk cases
- Surveillance cystoscopy every 3 months initially
- Low Risk (solitary, small, low-grade Ta):
Muscle Invasive Bladder Cancer (MIBC) – Stage II-III
Standard Approach:
- Radical cystectomy with pelvic lymph node dissection
- Removal of bladder, surrounding tissues, and regional lymph nodes
- Creation of urinary diversion (ileal conduit or neobladder)
- Neoadjuvant cisplatin-based chemotherapy
- Typically 3-4 cycles before surgery
- Improves overall survival by 5-8%
- Standard for eligible patients
- Adjuvant chemotherapy
- For patients who did not receive neoadjuvant treatment
- Based on pathological findings after surgery
- Radical cystectomy with pelvic lymph node dissection
Bladder Preservation Approach (selected cases):
- Maximal TURBT followed by
- Concurrent chemoradiation therapy
- Salvage cystectomy for incomplete response/recurrence
- Requires careful patient selection and multidisciplinary approach
Metastatic Bladder Cancer (Stage IV)
First-line Treatment:
- Cisplatin-based combination chemotherapy
- Gemcitabine plus cisplatin (GC)
- Dose-dense MVAC (methotrexate, vinblastine, doxorubicin, cisplatin)
- For cisplatin-ineligible patients:
- Carboplatin-based regimens
- Immune checkpoint inhibitors (pembrolizumab or atezolizumab)
- Cisplatin-based combination chemotherapy
Second-line Treatment:
- Immune checkpoint inhibitors
- Enfortumab vedotin (antibody-drug conjugate)
- Erdafitinib (for FGFR3-altered tumors)
- Clinical trials
Maintenance Therapy:
- Avelumab (anti-PD-L1) after first-line chemotherapy response
Medications
Intravesical Chemotherapy Agents
Mitomycin C:
- Used for immediate post-TURBT instillation
- Induction and maintenance therapy for intermediate-risk NMIBC
- Mechanism: DNA cross-linking agent
- Side effects: Chemical cystitis, allergic reactions, skin reactions
Gemcitabine:
- Alternative to mitomycin C
- Similar efficacy with potentially fewer side effects
- Mechanism: Nucleoside analog
- Side effects: Chemical cystitis, flu-like symptoms
Valrubicin:
- Approved for BCG-refractory carcinoma in situ
- Limited efficacy but option for patients ineligible for surgery
- Mechanism: Anthracycline that intercalates with DNA
- Side effects: Irritative voiding symptoms, hematuria
Docetaxel:
- Used in some combination protocols
- Mechanism: Microtubule inhibitor
- Side effects: Chemical cystitis, systemic absorption rare
Intravesical Immunotherapy
- Bacillus Calmette-Guérin (BCG):
- Live attenuated strain of Mycobacterium bovis
- Gold standard for high-risk NMIBC
- Mechanism: Induces local immune response against tumor cells
- Side effects: Cystitis, hematuria, flu-like symptoms, potential for BCG infection
- Schedule: Induction (6 weekly) followed by maintenance (3 weekly instillations at months 3, 6, 12, 18, 24, 30, 36)
Systemic Chemotherapy
Cisplatin-based combinations:
- Gemcitabine + Cisplatin (GC)
- MVAC (Methotrexate, Vinblastine, Doxorubicin, Cisplatin)
- Dose-dense MVAC with growth factor support
- Side effects: Nausea, vomiting, nephrotoxicity, neuropathy, myelosuppression
- Response rates: 40-60% in first-line setting
Carboplatin-based regimens:
- For cisplatin-ineligible patients
- Less effective than cisplatin
- Better tolerated in patients with renal impairment
- Side effects: Myelosuppression, nausea, fatigue
Immune Checkpoint Inhibitors
PD-1 Inhibitors:
- Pembrolizumab: Approved for BCG-unresponsive NMIBC, advanced/metastatic disease
- Nivolumab: Approved for advanced disease after platinum chemotherapy
- Mechanism: Blocks PD-1 receptor, enhancing T-cell activity against tumor
- Side effects: Fatigue, immune-related adverse events (colitis, pneumonitis, hepatitis, endocrinopathies)
PD-L1 Inhibitors:
- Atezolizumab: First-line for cisplatin-ineligible patients, second-line after platinum
- Avelumab: Maintenance therapy after response to first-line chemotherapy
- Durvalumab: Used in clinical trials, similar mechanism to other PD-L1 inhibitors
- Side effects: Similar to PD-1 inhibitors but potentially lower incidence
Targeted Therapies
Erdafitinib:
- FGFR inhibitor for metastatic disease with FGFR3 or FGFR2 genetic alterations
- First targeted therapy approved for bladder cancer
- Mechanism: Inhibits fibroblast growth factor receptor signaling
- Side effects: Hyperphosphatemia, stomatitis, diarrhea, hand-foot syndrome
Enfortumab vedotin:
- Antibody-drug conjugate targeting Nectin-4
- Approved for locally advanced or metastatic disease after platinum and immunotherapy
- Mechanism: Delivers microtubule-disrupting agent to tumor cells
- Side effects: Peripheral neuropathy, fatigue, rash, alopecia, hyperglycemia
Sacituzumab govitecan:
- Antibody-drug conjugate targeting Trop-2
- Used for metastatic disease after multiple prior therapies
- Mechanism: Delivers SN-38 (active metabolite of irinotecan) to tumor cells
- Side effects: Neutropenia, diarrhea, nausea, fatigue
Surgeries and Procedures
Non-Muscle Invasive Disease Procedures
Transurethral Resection of Bladder Tumor (TURBT):
- Primary treatment for diagnosis and management
- Complete removal of all visible tumor
- Techniques include monopolar or bipolar electrocautery
- Enhanced visualization methods (blue light, narrow band imaging)
- Re-TURBT often performed for high-grade T1 tumors
Office-based Procedures:
- Fulguration of small recurrences
- Cold-cup biopsy for surveillance
- Laser ablation of small tumors
Radical Surgical Approaches
Radical Cystectomy:
- Standard surgical treatment for MIBC
- Removal of entire bladder, proximal urethra, surrounding perivesical tissues
- In men: Removal of prostate and seminal vesicles
- In women: Often includes anterior vaginal wall, uterus, fallopian tubes, ovaries
- Extended lymph node dissection improves staging and outcomes
- Approaches:
- Open (traditional)
- Laparoscopic
- Robotic-assisted (increasingly common)
Partial Cystectomy:
- Removal of portion of bladder containing tumor
- Highly selective cases (solitary tumor in diverticulum or dome)
- Preserves bladder function
- Requires negative surgical margins
- Higher risk of recurrence compared to radical cystectomy
Urinary Diversion Options
Ileal Conduit:
- Most common diversion type
- Segment of ileum connected to ureters with stoma on abdominal wall
- External collection bag required
- Simpler procedure with fewer complications
- No learning curve for patient management
Orthotopic Neobladder:
- Creation of new bladder from intestinal segment
- Connected to native urethra for normal voiding
- Preserves body image
- Candidates must have negative urethral margins
- Potential complications: incontinence, retention, metabolic issues
Continent Cutaneous Diversion:
- Internal reservoir created from intestine
- Catheterizable channel to skin
- No external appliance needed
- Requires patient ability to catheterize
- Higher complication rate than other diversions
Bladder-Preserving Procedures
Trimodal Therapy:
- Maximal TURBT
- External beam radiation therapy
- Concurrent radiosensitizing chemotherapy
- 5-year bladder intact survival: 40-50%
- Requires careful patient selection and monitoring
Palliative Procedures:
- Urinary diversion without cystectomy
- Transurethral resection for bleeding control
- Nephrostomy tubes for upper tract obstruction
- Intravesical formalin or alum for intractable bleeding
Emerging Treatments and Clinical Trials
Immunotherapy Advances
Novel Checkpoint Inhibitors:
- CTLA-4 inhibitors in combination with PD-1/PD-L1 inhibitors
- Novel targets: TIM-3, LAG-3, TIGIT inhibitors
- Agonistic antibodies for costimulatory receptors (OX40, 4-1BB)
Cellular Therapies:
- Chimeric antigen receptor (CAR) T-cell therapy
- Tumor-infiltrating lymphocyte (TIL) therapy
- Natural killer (NK) cell approaches
- Cancer vaccines (personalized neoantigen vaccines)
Targeted Therapy Development
Next-generation FGFR Inhibitors:
- Improved selectivity and reduced toxicity
- Combinations with immunotherapy
- Strategies to overcome resistance mechanisms
Novel Antibody-Drug Conjugates:
- Targeting multiple tumor-associated antigens
- More potent cytotoxic payloads
- Improved linker technology
- Combinations with other treatment modalities
Other Molecular Targets:
- HER2-directed therapies for HER2+ tumors
- PARP inhibitors for DNA damage repair deficient tumors
- PI3K/AKT/mTOR pathway inhibitors
- Epigenetic modifiers (HDAC inhibitors, EZH2 inhibitors)
Novel Local Therapies
Viral Gene Therapy:
- Oncolytic viruses
- Intravesical delivery of immune-stimulating genes
- P53 gene replacement
Advanced Delivery Technologies:
- Nanoparticle-based drug delivery
- Sustained-release intravesical devices
- Thermosensitive gel formulations
- Electromotive drug administration (EMDA)
Novel Energy-based Therapies:
- Photodynamic therapy
- Radiofrequency ablation
- Cryotherapy
- High-intensity focused ultrasound (HIFU)
Precision Medicine Approaches
Molecular Subtyping:
- Treatment selection based on luminal, basal, or neural subtypes
- Immune infiltration patterns predicting immunotherapy response
- Consensus molecular classification systems emerging
Liquid Biopsy Applications:
- Circulating tumor DNA for treatment selection and monitoring
- Exosome analysis
- Circulating tumor cells
- Early detection of recurrence
Predictive Biomarkers:
- Tumor mutational burden
- DNA damage repair gene status
- RNA expression signatures
- Immune gene signatures
- FGFR alteration testing
Novel Combinations
- Dual checkpoint inhibition (anti-PD-1/PD-L1 plus anti-CTLA-4)
- Chemotherapy plus immunotherapy in various sequences
- FGFR inhibitors with immunotherapy
- Antibody-drug conjugates with checkpoint inhibitors
- Radiation therapy with immunotherapy (abscopal effect)
The landscape of bladder cancer treatment is rapidly evolving, with numerous clinical trials investigating innovative approaches. Patients should be encouraged to discuss clinical trial options with their healthcare team, as participation may provide access to promising new therapies before they become widely available.
9. Prevention & Precautionary Measures
Primary Prevention Strategies
Tobacco Cessation and Prevention
- Smoking cessation reduces bladder cancer risk by 30-60% over time
- Risk decreases progressively with increased years since quitting
- After 25 years, risk approaches that of never-smokers
- Prevention of smoking initiation through education and policy
- Tobacco cessation programs should be integrated into healthcare systems
- Pharmacological support (nicotine replacement, varenicline, bupropion)
- Behavioral counseling increases success rates significantly
Occupational Exposure Reduction
- Implementation of safety standards in high-risk industries
- Engineering controls to reduce exposure:
- Closed systems
- Improved ventilation
- Automated processes to minimize handling
- Administrative controls:
- Job rotation to limit exposure time
- Worker education on proper handling
- Regular monitoring of exposure levels
- Personal protective equipment:
- Proper gloves, respirators, protective clothing
- Regular changing and cleaning protocols
- Regular medical surveillance for high-risk workers
- Early removal from exposure when symptoms develop
Environmental Protection Measures
- Drinking water safety:
- Regulation of arsenic levels in public water supplies
- Filtration systems for private wells in high-risk areas
- Alternative water sources in endemic areas
- Regular water quality testing
- Reduction of chlorination byproducts:
- Alternative disinfection methods
- Filtration of organic precursors
- Activated carbon filtration for home use
- Industrial waste regulation to prevent groundwater contamination
- Environmental monitoring in high-risk regions
Dietary and Lifestyle Modifications
- Adequate hydration (2-3 liters daily) dilutes urinary carcinogens
- Consumption of fruits and vegetables rich in antioxidants
- Reduction of processed meat intake
- Maintaining healthy weight (obesity linked to increased risk)
- Regular physical activity (associated with lower risk)
- Limited alcohol consumption
- Avoidance of unnecessary medications linked to bladder cancer:
- Pioglitazone (when alternatives exist)
- Cyclophosphamide (careful monitoring when required)
- Aristolochic acid-containing herbal preparations (should be avoided)
Lifestyle Changes for High-Risk Individuals
Hydration Optimization
- Increased fluid intake to ensure frequent bladder emptying
- Goal of pale yellow urine color
- Spread fluid intake throughout the day
- Reduced evening fluid intake if nocturia is problematic
- Consideration of mineral or filtered water in areas with high tap water contaminants
Dietary Recommendations
- Mediterranean diet pattern (associated with lower risk)
- Higher intake of cruciferous vegetables (broccoli, cauliflower, cabbage)
- Foods rich in antioxidants (berries, green tea, tomatoes)
- Reduction of charred or well-done meats
- Limitation of processed foods with nitrates/nitrites
- Adequate vitamin D and selenium intake
- Potential benefits of garlic, onions, and allium vegetables
Bladder Health Practices
- Regular and complete bladder emptying
- Treatment of chronic urinary conditions:
- Prompt treatment of urinary tract infections
- Management of chronic inflammation
- Treatment of urinary stones
- Avoidance of chronic urinary retention
- Pelvic floor strengthening when appropriate
- Limitation of bladder irritants (caffeine, alcohol, spicy foods) if symptomatic
Medical Surveillance
- More frequent urinalysis for high-risk individuals
- Lower threshold for evaluation of urinary symptoms
- Consideration of urine cytology screening for highest-risk populations
- Prompt reporting of any urinary changes, particularly hematuria
Preventive Screenings
Risk-Based Screening Approaches
- Not recommended for general population (insufficient evidence of benefit)
- Targeted screening for high-risk groups:
- Workers with significant carcinogen exposure
- Heavy smokers (>30 pack-years)
- Individuals with family history of bladder cancer
- Patients after treatment for bladder cancer (surveillance)
Screening Methods
Urinalysis for microscopic hematuria
- Limitations: Low sensitivity (30-50%)
- High false-positive rate from non-malignant causes
- Simple and inexpensive first test
Urine cytology
- Better specificity than urinalysis (>90%)
- Limited sensitivity for low-grade tumors (30-50%)
- Good sensitivity for high-grade tumors and CIS (70-90%)
- More expensive and requires cytopathology expertise
Urine-based biomarkers
- Currently not recommended for screening general population
- May have role in high-risk populations
- Examples: NMP22, BTA, UroVysion FISH, CxBladder
- Limitations: cost, variable performance, false positives
Imaging
- Not recommended for routine screening
- May be considered for highest-risk individuals
- Ultrasound most practical for screening purposes
- CT urography reserved for evaluation of hematuria or symptoms
Recommended Screening Intervals
- No consensus guidelines for asymptomatic high-risk individuals
- Expert opinion suggests:
- Annual urinalysis for moderate-risk individuals
- Annual urinalysis plus cytology for high-risk occupational exposure
- More frequent (every 6 months) for very high-risk individuals
- Immediate evaluation for any episode of gross hematuria
Secondary Prevention (Early Detection)
Hematuria Evaluation Protocol
All episodes of gross hematuria warrant full evaluation regardless of age
Microscopic hematuria evaluation recommendations:
- American Urological Association: Evaluation for ≥3 RBCs/HPF in adults ≥35 years
- More aggressive approach for high-risk individuals
- Risk-stratified approach gaining favor
Comprehensive evaluation includes:
- Upper tract imaging (CT urography preferred)
- Cystoscopy
- Urine cytology
- Evaluation completed even if bleeding resolves
Symptom Awareness Education
Public education about warning signs:
- Blood in urine (even once)
- Irritative voiding symptoms without infection
- Persistent urinary symptoms despite antibiotic treatment
- Information particularly targeting high-risk groups
Healthcare provider education:
- Avoiding attribution bias (especially in women)
- Appropriate evaluation of microhematuria
- Recognition that UTI symptoms without positive culture warrant evaluation
- Lower threshold for investigation in high-risk individuals
Special Considerations
For Bladder Cancer Survivors:
- Structured surveillance protocols based on risk stratification
- Lifelong monitoring required
- Continued lifestyle modifications to reduce recurrence risk
- Vigilance for upper tract tumors
For First-Degree Relatives:
- Higher vigilance for urinary symptoms
- Earlier evaluation of hematuria
- Consideration of baseline screening in families with early-onset cases
- Intensified preventive measures (smoking cessation, hydration)
The prevention of bladder cancer requires a multifaceted approach targeting modifiable risk factors, with particular emphasis on smoking cessation and occupational safety. While population-wide screening is not currently recommended, risk-stratified approaches to early detection hold promise for improving outcomes in high-risk populations. Education of both the public and healthcare providers about symptom recognition remains crucial for timely diagnosis.
10. Global & Regional Statistics
Incidence and Prevalence Rates Globally
Global Burden
- Approximately 573,000 new cases of bladder cancer diagnosed worldwide annually
- Ranks as the 10th most common cancer globally
- Accounts for about 3% of all new cancer diagnoses
- Male-to-female ratio of approximately 3:1 globally
- Prevalence of over 1.7 million people living with bladder cancer globally
- Age-standardized incidence rate (ASIR) of 5.7 per 100,000 population worldwide
Regional Incidence Variation
Highest Incidence Regions (age-standardized rates per 100,000):
- Southern Europe: 15.2 in men, 2.6 in women
- Western Europe: 14.7 in men, 3.2 in women
- North America: 13.0 in men, 3.3 in women
- Northern Africa (particularly Egypt): 19.0 in men, 4.0 in women
Moderate Incidence Regions:
- Eastern Europe: 11.8 in men, 2.2 in women
- Australia/New Zealand: 10.6 in men, 3.1 in women
- South America: 7.2 in men, 2.0 in women
- Central America: 4.9 in men, 1.7 in women
Lowest Incidence Regions:
- South-Central Asia: 2.6 in men, 0.7 in women
- Middle Africa: 2.8 in men, 1.1 in women
- Western Africa: 1.9 in men, 0.9 in women
- Eastern Africa: 3.2 in men, 1.5 in women
Histological Variations by Region
- Urothelial carcinoma predominates globally (>90% in developed countries)
- Squamous cell carcinoma more common in regions with schistosomiasis:
- 40% of bladder cancers in Egypt (improving with parasite control)
- 30-40% in parts of Sudan and Ethiopia
- 10-15% in other parts of Africa with endemic schistosomiasis
- Adenocarcinoma represents 0.5-2% globally, with similar distribution
Age Distribution
- Median age at diagnosis globally: 73 years
- More than 70% of cases diagnosed in patients >65 years
- Developing regions show slightly earlier median age at diagnosis (65-70 years)
- Childhood bladder cancer exceedingly rare globally (<0.1% of cases)
Mortality and Survival Rates
Global Mortality
- Approximately 213,000 deaths worldwide annually
- Ranks as the 13th leading cause of cancer death
- Male-to-female ratio for mortality approximately 3:1
- Age-standardized mortality rate of 1.9 per 100,000 population globally
Regional Mortality Rates (age-standardized per 100,000)
Highest Mortality Regions:
- Northern Africa: 7.6 in men, 1.8 in women
- Southern Europe: 5.2 in men, 1.0 in women
- Western Asia: 4.9 in men, 1.4 in women
- Central and Eastern Europe: 4.5 in men, 0.9 in women
Moderate Mortality Regions:
- North America: 3.0 in men, 0.8 in women
- Australia/New Zealand: 3.2 in men, 0.9 in women
- South America: 2.5 in men, 0.7 in women
Lowest Mortality Regions:
- Eastern Asia: 1.8 in men, 0.5 in women
- South-Central Asia: 1.4 in men, 0.4 in women
- South-Eastern Asia: 1.2 in men, 0.4 in women
Survival Rates by Region
5-year Relative Survival Rates:
- North America: 77% overall (ranges from 96% for in situ to 5% for distant disease)
- Western Europe: 70-75%
- Southern Europe: 65-70%
- Eastern Europe: 55-65%
- Australia/New Zealand: 74%
- Eastern Asia (Japan, South Korea): 65-70%
- China: 60-65%
- South America: 50-60%
- India: 40-50%
- Sub-Saharan Africa: 30-40%
Stage at Diagnosis by Region (influences survival):
- Developed regions:
- 50-60% non-muscle invasive
- 30% muscle-invasive
- 10-20% metastatic
- Developing regions:
- 30-40% non-muscle invasive
- 40-50% muscle-invasive
- 20-30% metastatic
- Developed regions:
Mortality-to-Incidence Ratio (MIR)
- Global average MIR: 0.33 (33 deaths per 100 cases)
- North America and Western Europe: 0.20-0.25
- Eastern Europe: 0.30-0.35
- Latin America: 0.35-0.40
- Southeast Asia: 0.40-0.45
- Africa: 0.50-0.60
- Higher MIR indicates poorer outcomes/healthcare access
Country-Specific Comparisons and Trends
Highest Incidence Countries (age-standardized rates per 100,000)
- Egypt: 19.0 in men, 4.0 in women (linked to schistosomiasis)
- Lebanon: 17.4 in men, 4.2 in women
- Belgium: 17.5 in men, 3.8 in women
- Spain: 17.2 in men, 3.0 in women
- Italy: 16.0 in men, 3.0 in women
- Denmark: 15.9 in men, 4.5 in women
- Greece: 15.7 in men, 2.5 in women
- Hungary: 15.1 in men, 3.7 in women
- United States: 13.0 in men, 3.3 in women
- Netherlands: 12.7 in men, 3.2 in women
Lowest Incidence Countries (age-standardized rates per 100,000)
- Uganda: 1.3 in men, 0.8 in women
- Niger: 1.4 in men, 0.6 in women
- Ghana: 1.6 in men, 0.7 in women
- Pakistan: 2.0 in men, 0.6 in women
- Indonesia: 2.4 in men, 0.5 in women
- India: 2.4 in men, 0.7 in women
- Nigeria: 2.5 in men, 0.9 in women
- Vietnam: 2.8 in men, 0.6 in women
- Bangladesh: 2.9 in men, 0.8 in women
- Philippines: 3.0 in men, 0.8 in women
Notable Country-Specific Patterns
Egypt: Transitioning from squamous cell (schistosomiasis-related) to urothelial carcinoma as parasite control improves; overall rates remain high due to smoking and other factors
United States:
- Declining incidence (−1.6% annually) due to smoking reduction
- Racial disparities: Higher incidence in White Americans but worse outcomes in African Americans
- Geographic hotspots in the Northeast and Great Lakes regions correlating with industrial areas
China:
- Rapidly increasing incidence (3-4% annually) with urbanization and increased smoking
- Significant exposure to industrial chemicals in manufacturing regions
- Arsenic in drinking water in some provinces
Japan:
- Stable or slightly declining rates
- Earlier detection than many countries
- High proportion of non-muscle invasive disease at diagnosis
United Kingdom:
- Increasing incidence in women (0.4% annually)
- Narrowing gender gap (related to changing smoking patterns)
- Significant geographic variation (higher in industrial North)
Temporal Trends
Developed Countries:
- Stable or slightly declining rates in men
- Increasing rates in women (narrowing gender gap)
- Improving survival rates (1-2% improvement per decade)
- Stage migration toward earlier diagnosis
Developing Countries:
- Rapidly increasing incidence with industrialization and tobacco use
- Demographic transition to aging populations increasing burden
- Improving diagnostic capabilities detecting more cases
- Mixed trends in countries with high schistosomiasis prevalence (decreasing parasite-related cases but increasing smoking-related cases)
Global Projections:
- Estimated 25% increase in global burden by 2040
- Largest increases projected in Africa and Asia
- Aging global population driving overall increase
- Improving survival expected to increase prevalence
The global landscape of bladder cancer shows significant geographic variation in incidence, mortality, and survival, reflecting differences in risk factors, healthcare access, and detection capabilities. While improvements in prevention, early detection, and treatment are yielding better outcomes in developed regions, the increasing burden in developing countries presents a significant global health challenge for the coming decades.
11. Recent Research & Future Prospects
Latest Advancements in Treatment and Research
Immunotherapy Refinements
Biomarker-Guided Immunotherapy:
- PD-L1 expression testing to guide treatment selection
- Tumor mutational burden as predictive marker
- Molecular subtyping to identify likely responders
- Interferon-gamma signature as response predictor
- Microbiome composition influencing efficacy
Novel Immunotherapy Combinations:
- Dual checkpoint inhibition showing improved response rates
- CTLA-4 inhibitors plus PD-1/PD-L1 inhibitors
- Chemotherapy plus immunotherapy demonstrating synergistic effects
- Radiation therapy with immunotherapy (abscopal effect)
- FGFR inhibitors with immunotherapy showing promise
Alternative Immunotherapy Approaches:
- Intravesical immune stimulants beyond BCG
- Recombinant IL-15 and IL-2 therapies
- Adoptive cell therapies (TILs, CAR-T)
- Personalized neoantigen vaccines
- Oncolytic viral therapies
Precision Oncology Applications
Comprehensive Genomic Profiling:
- Routine next-generation sequencing guiding treatment selection
- Liquid biopsy for non-invasive detection of actionable mutations
- Circulating tumor DNA for monitoring treatment response
- RNA expression profiling for molecular subtyping
- Integration of multi-omics data (genomics, transcriptomics, proteomics)
Expanded Targeted Therapy Options:
- Second-generation FGFR inhibitors with improved tolerability
- HER2-directed therapies for HER2-amplified tumors
- PARP inhibitors for DNA damage repair gene mutations
- PI3K/AKT/mTOR pathway inhibitors
- Epigenetic modifier drugs (HDAC inhibitors, EZH2 inhibitors)
Novel Antibody-Drug Conjugates (ADCs):
- Extended indications for enfortumab vedotin and sacituzumab govitecan
- Novel targets beyond Nectin-4 and Trop-2
- Improved linker technology and payload potency
- Bispecific antibody-drug conjugates
- Combination strategies with other treatment modalities
Surgical and Radiotherapy Innovations
Enhanced Surgical Approaches:
- Fluorescence-guided surgery improving complete resection rates
- Narrow band imaging for better tumor visualization
- Confocal laser endomicroscopy for real-time histological assessment
- Robotic surgery refinements for improved functional outcomes
- Novel urinary diversion techniques with reduced complications
Radiotherapy Advances:
- Adaptive radiotherapy with daily imaging
- Intensity-modulated radiotherapy reducing toxicity
- Hypofractionated protocols for shorter treatment courses
- MRI-guided radiotherapy for improved targeting
- Novel radiosensitizers enhancing efficacy
Organ Preservation Strategies:
- Refined patient selection criteria for bladder preservation
- Biomarkers predicting response to trimodality therapy
- Combination protocols with immunotherapy
- Partial cystectomy with sentinel lymph node mapping
- Focal therapy approaches for small tumors
Non-Invasive Diagnostics
Urine-Based Biomarkers:
- Multi-marker panels with improved sensitivity and specificity
- Methylation markers for early detection
- miRNA signatures for recurrence prediction
- Protein marker combinations (emerging commercial tests)
- Point-of-care testing platforms for rapid results
Imaging Advancements:
- Multiparametric MRI protocols specifically for bladder cancer
- Novel PET tracers beyond FDG (PSMA, FAPI)
- Artificial intelligence applications for image interpretation
- Molecular imaging targeting cancer-specific receptors
- Contrast-enhanced ultrasound techniques
Ongoing Studies and Future Medical Possibilities
Major Clinical Trial Directions
Immunotherapy Optimization Trials:
- Neoadjuvant immunotherapy before cystectomy
- Adjuvant immunotherapy after cystectomy
- Extended duration of maintenance therapy
- Treatment beyond progression protocols
- Rechallenge strategies after previous immunotherapy
BCG-Unresponsive Disease Solutions:
- Novel BCG strains and combinations
- Alternative intravesical immunotherapies
- Combination approaches (BCG plus other agents)
- Device-assisted drug delivery methods
- Gene therapy approaches
Metastatic Disease Trials:
- First-line immunotherapy plus chemotherapy combinations
- Novel sequencing approaches (switching therapy based on early response)
- Personalized therapy based on molecular profiling
- Maintenance strategies after initial response
- Oligometastatic disease-specific approaches
Quality of Life and Survivorship Studies:
- Patient-reported outcome measure development
- Sexual function preservation techniques
- Continence improvement strategies after neobladder
- Toxicity reduction approaches
- Psychosocial intervention effectiveness
Future Diagnostic Approaches
Liquid Biopsy Integration:
- Blood-based screening in high-risk populations
- Urine cell-free DNA analysis for surveillance
- Combination of genomic and proteomic markers
- Exosome analysis for early detection
- Prediction of treatment response and monitoring
Artificial Intelligence Applications:
- Computer-aided detection during cystoscopy
- Automated pathology interpretation
- Radiomic feature extraction from imaging
- Predictive modeling for recurrence and progression
- Treatment response algorithms
Point-of-Care Diagnostics:
- Smartphone-based microscopy for urine cytology
- Rapid biomarker testing platforms
- Home-based monitoring systems
- Continuous physiological monitoring
- Simplified molecular testing methods
Novel Therapeutic Paradigms
Metabolic Approaches:
- Targeting altered cancer metabolism
- Dietary modification to enhance treatment efficacy
- Microbiome manipulation to boost immunotherapy response
- Ketogenic diet trials as adjunctive therapy
- Metabolism-targeted small molecules
Immune Microenvironment Modulation:
- Therapies targeting immune-suppressive mechanisms
- Myeloid-derived suppressor cell inhibition
- T-regulatory cell modulation
- Cancer-associated fibroblast targeting
- Tumor-associated macrophage reprogramming
Synthetic Biology Applications:
- Engineered bacteria for tumor targeting
- CRISPR-based therapies
- Logic-gated cell therapies
- Biosensor integration
- Gene circuit-controlled therapeutic production
Potential Cures and Innovative Therapies
Emerging Cure Strategies for Non-Muscle Invasive Disease
Enhanced BCG Approaches:
- Genetically modified BCG expressing immune stimulants
- BCG combined with checkpoint inhibitors (ongoing trials showing 70-80% complete response in BCG-unresponsive disease)
- Recombinant BCG strains with improved efficacy
- Personalized BCG dosing and schedules
- Maintenance optimization to reduce recurrence
Novel Intravesical Therapies:
- Combination intravesical chemotherapy protocols
- Nanotechnology-based drug delivery systems
- Sustained-release devices for prolonged drug exposure
- Penetration enhancers to improve drug absorption
- Heat-activated targeted therapy
Precision Prevention of Progression:
- Molecular risk stratification for aggressive early intervention
- Targeted therapy for specific genetic alterations
- Immunotherapy in highest-risk patients
- Early radical therapy for selected genomic profiles
- Chemoprevention strategies for high-risk patients
Advanced Muscle-Invasive Disease Approaches
Curative-Intent Multimodal Therapy:
- Triplet therapy combinations showing promising results
- Chemotherapy + immunotherapy + radiotherapy
- Neoadjuvant immunochemotherapy followed by minimal invasive surgery
- Targeted therapy + immunotherapy + radiation
- Pathological complete response rates of 40-50% in ongoing trials
- Adaptive treatment based on early response assessment
- Organ preservation with equivalent survival to cystectomy
- Triplet therapy combinations showing promising results
Neoadjuvant Therapy Advancements:
- Biomarker-selected intense neoadjuvant protocols
- Circulating tumor DNA to guide treatment duration
- Treatment intensification for non-responders
- Pathological complete response rates approaching 50-60%
- Reduced-intensity surgery after exceptional response
Molecular Subtype-Directed Treatment:
- Luminal tumors: FGFR-targeted therapy
- Basal tumors: Intensified chemotherapy
- Luminal-infiltrated: Immunotherapy focus
- Neuronal subtype: Neuroendocrine-directed therapy
- p53-like: Alternative platinum agents
Metastatic Disease Breakthroughs
Long-term Remission Strategies:
- Oligometastatic disease: Aggressive local therapy plus systemic treatment
- Immune memory induction for durable response
- Novel combination immunotherapy showing durable responses in 25-30% of patients
- Maintenance strategies after initial response
- Depth of response as predictor of long-term outcome
Personalized Cellular Therapies:
- Tumor-infiltrating lymphocyte (TIL) therapy
- CAR-T targeting bladder cancer-specific antigens
- Natural killer (NK) cell therapy
- Dendritic cell vaccines
- Personalized neoantigen vaccines showing early promise
Integrated Systems Biology Approaches:
- Real-time treatment adaptation based on molecular changes
- Artificial intelligence-guided therapy selection
- Combination strategies targeting multiple cancer hallmarks
- Resistance mechanism prevention strategies
- Host factors (microbiome, immune status) optimization
The landscape of bladder cancer research is rapidly evolving, with unprecedented advancements in understanding the molecular basis of the disease and developing targeted therapeutic approaches. While a universal cure remains elusive, the emerging paradigm of precision oncology, combined with novel immunotherapeutic strategies and enhanced multimodal approaches, offers realistic hope for significantly improved outcomes across all disease stages in the coming decade.
12. Interesting Facts & Lesser-Known Insights
Uncommon Knowledge About Bladder Cancer Symptoms
Historical Perspectives and Cultural Aspects
- Ancient Egyptian papyri from around 1500 BCE described what was likely bladder cancer, including hematuria, now known as its most common symptom.
- Emperor Napoleon Bonaparte may have suffered from bladder cancer, with descriptions of his symptoms during his exile on St. Helena including intermittent hematuria and suprapubic pain.
- The association between occupation and bladder cancer symptoms was first made in 1895 when German surgeon Ludwig Rehn noticed high rates of bladder bleeding among dye workers.
- The term “painter’s disease” was used in the 18th and 19th centuries to describe urinary symptoms in artists exposed to carcinogenic pigments containing cadmium, leading to bladder cancer.
Symptom Peculiarities
- “Terminal hematuria” (blood appearing primarily at the end of urination) is more specific for bladder tumor location near the bladder neck, while “total hematuria” (blood throughout urination) suggests a different tumor location or cause.
- The color of hematuria can provide diagnostic clues: bright red often indicates lower tract bleeding (bladder), while darker “coca-cola” colored urine may suggest upper tract or older bleeding.
- Irritative bladder symptoms (frequency, urgency) without infection are more common in women with bladder cancer than men, contributing to delayed diagnosis as these symptoms are often attributed to cystitis.
- “Phantom cystitis” – recurrent symptoms of urinary tract infection with negative urine cultures – should raise suspicion for carcinoma in situ of the bladder.
- Environmental temperature changes can trigger or worsen symptoms in some patients with bladder cancer, particularly frequency and urgency.
Symptom Patterns and Associations
- Morning hematuria is more suggestive of bladder cancer, while hematuria throughout the day is more common with kidney stones or infection.
- Up to 10% of patients with bladder cancer experience referred pain to unusual locations, including the lower back, hip, or even heel due to nerve pathway connections.
- “Facetious hematuria” – the appearance of red urine without blood – can occur from foods (beets, rhubarb), medications (rifampin, phenazopyridine), or porphyria, sometimes leading to delayed investigation of true hematuria.
- Seasonal variation in bladder cancer diagnosis exists, with more cases diagnosed in winter months in some studies, potentially related to concentration of urine or delayed evaluation during summer vacation periods.
- “Symptomatic silence” – the absence of symptoms despite advanced disease – occurs in approximately 5-10% of bladder cancer cases, particularly in elderly patients with reduced bladder sensation.
Diagnostic Challenges
- Women experience an average diagnostic delay of 85 days longer than men after presenting with hematuria, contributing to more advanced stage at diagnosis.
- Microscopic hematuria is actually absent in about 15% of bladder cancer patients at the time of presentation, despite being considered a cardinal sign.
- Using dipstick tests alone without microscopic confirmation misses approximately 10% of significant hematuria due to false negatives.
- “Symptom clustering” – the specific combination of hematuria, urgency, and dysuria without fever – has been shown to have higher predictive value for bladder cancer than any symptom alone.
- Up to 30% of patients diagnosed with bladder cancer report having their symptoms initially attributed to benign causes by healthcare providers, resulting in diagnostic delays.
Myths and Misconceptions vs. Medical Facts
Myth: Blood in the urine is usually painful. Fact: Hematuria caused by bladder cancer is typically painless, which often leads patients to delay seeking medical attention. Pain with urination is more commonly associated with infection or inflammation.
Myth: A negative urinalysis rules out bladder cancer. Fact: Up to 15% of patients with bladder cancer may have normal urinalysis at presentation due to the intermittent nature of hematuria. Repeated testing and proper evaluation of symptoms is essential.
Myth: Most bladder cancers are detected at early stages due to obvious bleeding. Fact: Despite hematuria being a common early symptom, about 25% of bladder cancers are still diagnosed at advanced stages due to symptom misattribution, intermittent nature of bleeding, or lack of prompt evaluation.
Myth: Bladder cancer symptoms are similar in men and women. Fact: Women more commonly present with irritative symptoms (frequency, urgency, dysuria) rather than gross hematuria, contributing to the 60-90 day longer diagnostic delay compared to men.
Myth: Urinary tract infections and bladder cancer can be easily distinguished by symptoms. Fact: The symptoms can significantly overlap, and approximately 20% of patients diagnosed with bladder cancer were initially treated for presumed recurrent UTIs without proper evaluation.
Myth: Young people with hematuria don’t need evaluation for bladder cancer. Fact: While bladder cancer is less common in young adults, it can and does occur. Hematuria in any adult warrants proper evaluation regardless of age.
Myth: Smoking only increases risk but doesn’t affect how bladder cancer presents. Fact: Smoking-related bladder cancers often have different molecular profiles, and some studies suggest they may present with more aggressive symptoms and multifocal disease.
Myth: A single negative cystoscopy rules out bladder cancer as a cause of symptoms. Fact: Small or flat lesions like carcinoma in situ can be missed on conventional cystoscopy, and upper tract urothelial cancers may cause identical symptoms but aren’t visible during bladder examination.
Myth: Bladder cancer symptoms steadily worsen over time. Fact: Symptoms, particularly hematuria, are often intermittent with periods of complete resolution, which can falsely reassure patients and providers.
Myth: Men and women have similar outcomes when diagnosed at the same stage. Fact: Even when diagnosed at the same stage, women often have worse outcomes, which may relate to biological differences, including hormonal factors and differences in treatment response.
Impact on Specific Populations and Professions
Occupational Impact
Chemical Industry Workers:
- 30-50% higher incidence than general population
- Often present with symptoms at younger ages (50s vs. 70s)
- Higher rates of multiple tumors when diagnosed
- More aggressive variants in some studies
- Special screening programs recommended
Hairdressers and Barbers:
- 20-30% increased risk, particularly those working before 1980
- Often experience longer diagnostic delays due to attributing symptoms to standing-related urinary issues
- Female predominance in this occupational group changes typical demographics
- Earlier age at diagnosis (average 5-7 years earlier than general population)
Textile Workers:
- Historical high-risk group from dye exposures
- Symptom awareness programs have improved early detection
- Cultural barriers in textile-heavy regions (Southeast Asia) sometimes delay symptom reporting
- Industry-specific genetic polymorphisms may affect presentation
Truck Drivers and Transport Workers:
- Combination of diesel exposure and decreased urination frequency
- Often present with more advanced disease due to limited healthcare access
- Irregular schedules complicate symptom recognition
- Workplace constraints may delay seeking medical attention for urinary symptoms
Age-Specific Considerations
Young Adults with Bladder Cancer (under 40):
- Often experience significant diagnostic delays due to low suspicion
- Symptoms frequently attributed to benign causes
- Higher proportion of rare histological variants
- Greater impact on fertility and sexual function concerns
- More extensive genomic testing recommended
Elderly Patients (over 80):
- Often present with atypical symptoms (fatigue, weight loss without hematuria)
- Symptoms frequently attributed to aging or other conditions
- Decreased sensitivity to bladder filling leads to later presentation
- Multiple comorbidities mask specific symptoms
- Treatment modifications needed due to frailty
Gender-Specific Issues
Women with Bladder Cancer:
- 60-90 day longer diagnostic delay than men
- Symptoms often misattributed to gynecological causes
- Higher rates of advanced disease at diagnosis (40% vs. 30% in men)
- More frequent urologist referral delays
- Need for gender-specific symptom awareness campaigns
Men with Bladder Cancer:
- Symptoms sometimes confused with prostate conditions
- Cultural reluctance to discuss urinary symptoms
- Higher absolute numbers due to higher incidence
- Better overall survival stage-for-stage than women
Special Populations
Spinal Cord Injury Patients:
- Chronic catheterization increases risk by 4-5 times
- Symptoms masked by baseline urinary abnormalities
- Relies on screening rather than symptom recognition
- Higher rates of squamous cell variants
- Customized surveillance protocols needed
Organ Transplant Recipients:
- Immunosuppression increases bladder cancer risk
- Symptoms may be attributed to medication effects
- More rapid progression once symptoms develop
- Special screening protocols recommended
- Modified treatment approaches often required
Patients with Lynch Syndrome:
- 8x increased risk of upper tract urothelial cancer
- Need for awareness of urinary symptoms
- Cancer often develops at younger ages (40s-50s)
- Specialized surveillance protocols recommended
- Genetic counseling for family members
The understanding of bladder cancer symptoms continues to evolve, with increasing recognition of population-specific variations and the importance of prompt evaluation. Challenging common misconceptions and enhancing awareness of symptom patterns across different demographic groups remains crucial to improving early detection and outcomes.
This comprehensive report on bladder cancer symptoms provides a thorough overview of the current understanding of this condition. While extensive, it should be used for informational purposes and not as a substitute for professional medical advice. Any concerning symptoms should be promptly evaluated by healthcare professionals.