
⚠️ Disclaimer: The information provided in this article is for educational purposes only and does not constitute medical advice. RevisionTown does not provide diagnosis, treatment, or medical recommendations. Always consult a qualified healthcare professional regarding any medical condition, symptoms, or concerns.
Read More – 🏥 Medical Disclaimer
What is Asbestosis?
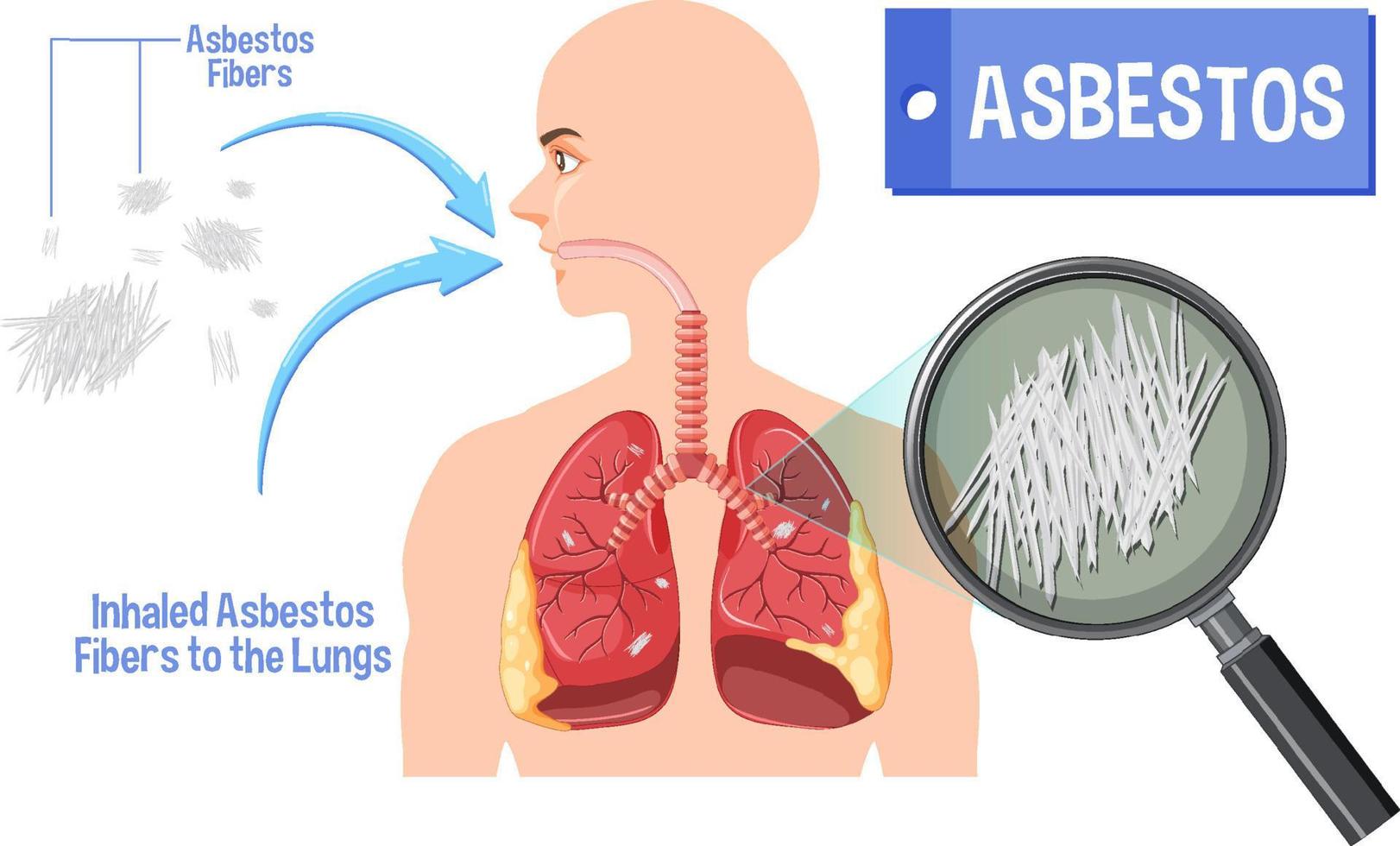
Asbestosis is a chronic, progressive pulmonary fibrosis (lung scarring) caused by the inhalation and retention of asbestos fibers in the lungs. It belongs to a group of diseases called pneumoconioses, which are lung diseases caused by the inhalation of dust particles. Asbestosis specifically results from prolonged exposure to asbestos fibers, leading to inflammation, scarring, and eventual impairment of lung function.
Definition and Pathophysiology
Asbestosis is defined as bilateral lower lobe pulmonary fibrosis resulting from the inhalation of asbestos fibers. The condition develops when asbestos fibers, typically longer than 5 micrometers, are inhaled and become permanently embedded in the alveolar tissue. These fibers trigger a chronic inflammatory response, leading to:
- Macrophage activation: Immune cells attempt to engulf the fibers but cannot break them down
- Cytokine release: Inflammatory mediators promote fibroblast proliferation
- Collagen deposition: Excessive collagen formation leads to progressive scarring
- Architectural distortion: Normal lung structure is replaced by fibrous tissue
Affected Body Parts and Organs
Primary Affected Area:
- Lungs: Lower lobes predominantly affected
- Pleura: Pleural plaques and thickening common
- Alveoli: Progressive fibrosis and destruction
- Interstitium: Thickening of the tissue between air sacs
Secondary Effects:
- Heart: Right heart strain (cor pulmonale) due to pulmonary hypertension
- Vascular system: Pulmonary circulation impairment
- Respiratory muscles: Increased work of breathing
Prevalence and Significance
Global Burden:
- Estimated cases: 200,000-400,000 people worldwide
- New diagnoses: 5,000-10,000 annually in developed countries
- Latency period: 15-40 years between exposure and disease manifestation
- Male predominance: 80-90% of cases (reflecting historical occupational patterns)
Public Health Significance:
- Preventable disease: Entirely caused by human-made exposure
- Economic burden: Billions in healthcare costs and compensation
- Legal implications: Major source of occupational litigation
- Environmental concern: Legacy contamination in buildings
- International health issue: Ongoing exposure in developing countries
Disease Classification
Severity Grades (ILO Classification):
- Category 1: Mild fibrosis, subtle changes
- Category 2: Moderate fibrosis, more obvious changes
- Category 3: Severe fibrosis, extensive lung involvement
Clinical Staging:
- Early: Asymptomatic with radiographic changes
- Moderate: Breathlessness on exertion, decreased function
- Advanced: Severe respiratory impairment, complications
2. History & Discoveries
Early Recognition and Documentation
Ancient Times to Industrial Revolution:
- Greek & Roman eras: Pliny the Elder noted lung problems in slaves mining asbestos
- 18th century: Industrial use of asbestos began
- Early 1900s: First reports of lung problems in asbestos workers
First Medical Recognition
Key Historical Milestones:
- 1900: Dr. H. Montague Murray documented first case in a young asbestos textile worker
- 1906: British Factory Inspector reported lung problems in asbestos workers
- 1924: Dr. W.E. Cooke coined the term “asbestosis” in British Medical Journal
- 1930: First comprehensive study by Dr. E.R.A. Merewether and Dr. C.W. Price
Major Discoveries and Breakthroughs
1930s-1950s: Recognition and Documentation
- 1930: Merewether-Price Report established dose-response relationship
- 1935: First compensation cases in the UK
- 1943: German studies linked asbestos to lung cancer
- 1955: Sir Richard Doll confirmed lung cancer-asbestos link
1960s-1980s: Comprehensive Understanding
- 1960: Irving Selikoff’s groundbreaking epidemiological studies
- 1965: Mesothelioma linked to asbestos exposure
- 1973: EPA begins regulating asbestos in the US
- 1989: Complete asbestos ban attempted in the US
Notable Researchers:
- Dr. Irving Selikoff: Pioneer in asbestos disease research
- Dr. E.R.A. Merewether: First systematic study of asbestosis
- Dr. J.C. Wagner: Described mesothelioma-asbestos relationship
- Dr. Richard Doll: Established carcinogenic evidence
Evolution of Medical Understanding
Pathophysiology Development:
- 1930s: Recognition of fibrotic process
- 1960s: Understanding of fiber types and their effects
- 1980s: Cellular and molecular mechanisms elucidated
- 2000s: Genetic factors and biomarkers identified
Regulatory Evolution:
- 1930s: First workplace exposure limits
- 1970s: Comprehensive occupational health regulations
- 1990s: International bans on asbestos use
- 2000s: Legacy exposure and remediation focus
Key Legislative and Medical Milestones
International Recognition:
- 1977: WHO recognizes asbestos as carcinogen
- 1998: EU bans all asbestos use
- 2019: WHO adds asbestos to essential medicines list for diagnosis
- Ongoing: Over 60 countries have banned asbestos
3. Symptoms
Asymptomatic Period
Silent Phase (15-40 years post-exposure):
- No symptoms despite ongoing pathological changes
- Gradual accumulation of fibers in lungs
- Early cellular inflammatory responses
- Radiographic changes may precede symptoms
Early Stage Symptoms
Initial Manifestations (Often Subtle):
Progressive Dyspnea (Shortness of Breath)
- Initially only on exertion
- Gradually worsens over time
- Most common early symptom (90% of patients)
Persistent Dry Cough
- Non-productive initially
- May become productive later
- Present in 60-70% of patients
Chest Tightness
- Feeling of constriction
- May worsen with activity
- Often described as “heaviness”
Fatigue and Exercise Intolerance
- Reduced stamina
- Easy exhaustion
- Decreased activity tolerance
Intermediate Stage Symptoms
Progressive Manifestations:
Worsening Dyspnea
- Breathlessness with minimal activity
- Eventually at rest
- Limits daily activities
Productive Cough
- Sputum production increases
- May contain blood (hemoptysis)
- Persistent and troublesome
Chest Pain
- Pleuritic in nature
- May be constant or intermittent
- Often bilateral
Finger Clubbing
- Enlargement of fingertips
- Curved nails
- Present in 40-60% of cases
Advanced Stage Symptoms
Severe Manifestations:
Severe Respiratory Distress
- Breathlessness at rest
- Orthopnea (breathing difficulty lying flat)
- Paroxysmal nocturnal dyspnea
Cyanosis
- Blue discoloration of lips, fingers
- Indicates severe oxygen deprivation
- Sign of respiratory failure
Right Heart Failure (Cor Pulmonale)
- Swelling of legs and ankles
- Abdominal distension
- Neck vein distension
Severe Exercise Limitation
- Unable to perform basic activities
- Requires assistance for daily tasks
- Wheelchair or bed-bound
Common vs. Rare Symptoms
Most Common Symptoms (>50% of patients):
- Progressive dyspnea (90%)
- Dry cough (70%)
- Fatigue (65%)
- Chest tightness (60%)
- Exercise intolerance (55%)
Moderately Common (25-50% of patients):
- Finger clubbing (40%)
- Chest pain (35%)
- Weight loss (30%)
- Night sweats (25%)
Rare Symptoms (<25% of patients):
- Hemoptysis (blood in sputum) (15%)
- Swallowing difficulties (10%)
- Hoarseness (5%)
- Recurrent respiratory infections (20%)
Symptom Progression Timeline
Typical Disease Course:
- Exposure period: Usually decades
- Latent period: 15-40 years (average 25-30 years)
- Early symptoms: Subtle, often attributed to aging
- Progressive phase: 5-15 years of worsening
- Advanced stage: Severe disability, complications
Factors Affecting Progression:
- Cumulative dose: Higher exposure = faster progression
- Fiber type: Amphibole asbestos more aggressive
- Individual susceptibility: Genetic and health factors
- Concurrent exposures: Smoking significantly worsens prognosis
- Age at exposure: Younger exposure may have worse outcomes
Symptom Variability
Individual Differences:
- Rate of progression: Varies significantly between patients
- Symptom severity: Not always correlated with radiographic changes
- Response to treatment: Individual variation in benefit
- Quality of life impact: Varies with adaptation and support
Complicating Factors:
- Smoking history: Accelerates decline
- Other lung diseases: COPD, silicosis may coexist
- Cardiovascular disease: Compounds symptoms
- Age-related changes: May mask or confound symptoms
4. Causes
Primary Environmental Cause
Asbestos Fiber Exposure: Asbestosis is exclusively caused by the inhalation of asbestos fibers. Asbestos is a group of six naturally occurring fibrous silicate minerals that were widely used in industry due to their unique properties.
Types of Asbestos and Their Health Effects
Amphibole Asbestos (More Dangerous):
Crocidolite (Blue Asbestos)
- Most carcinogenic type
- Straight, needle-like fibers
- High biopersistence in lungs
Amosite (Brown Asbestos)
- Second most dangerous
- Straight fibers, moderate length
- Used in thermal insulation
Anthophyllite
- Less common
- Long, straight fibers
- Found in some vermiculite deposits
Tremolite
- Contaminant in other materials
- Highly pathogenic
- Found in some talc deposits
Actinolite
- Less common commercially
- Similar to tremolite
- Environmental exposure concern
Chrysotile Asbestos (Serpentine)
- White asbestos
- 90% of global asbestos use
- Curly, flexible fibers
- Still considered dangerous despite some debates
Biological Mechanisms
Fiber Characteristics Determining Toxicity:
Dimension
- Length > 5 micrometers more pathogenic
- Diameter < 3 micrometers more respirable
- Aspect ratio (length/diameter) important
Biopersistence
- Inability of lungs to clear fibers
- Amphiboles more persistent than chrysotile
- Determines long-term health effects
Surface Reactivity
- Chemical composition affects cell interaction
- Iron content influences toxicity
- Surface area determines inflammatory response
Pathogenic Process:
Inhalation and Deposition
- Fibers reach alveolar region
- Deposit based on aerodynamic properties
- Preferential lower lobe deposition
Cellular Response
- Alveolar macrophages attempt phagocytosis
- Frustrated phagocytosis (cannot digest fibers)
- Lysosomal damage and cell death
Inflammatory Cascade
- Release of inflammatory mediators
- Cytokine and growth factor production
- Recruitment of additional inflammatory cells
Fibrotic Response
- Fibroblast proliferation and activation
- Excessive collagen production
- Progressive scar tissue formation
Exposure Sources
Historical Industrial Uses:
- Construction materials: Insulation, roofing, flooring
- Textile industry: Fire-resistant fabrics
- Shipbuilding: Insulation, gaskets
- Automotive: Brake pads, clutches
- Manufacturing: Various industrial applications
Current Exposure Sources:
- Legacy materials: Older buildings and infrastructure
- Demolition and renovation: Disturbance of asbestos materials
- Natural deposits: Environmental exposure near deposits
- Imported products: Some countries still use asbestos
- Contaminated materials: Talc, vermiculite products
Dose-Response Relationship
Factors Determining Disease Development:
Cumulative Dose
- Total amount of fibers inhaled over time
- Measured in fiber-years or cumulative exposure
- Higher doses increase disease risk and severity
Exposure Duration
- Longer exposure periods increase risk
- Even brief but intense exposure can cause disease
- Intermittent exposure pattern matters
Exposure Intensity
- Concentration of fibers in air
- Peak exposures particularly dangerous
- Time-weighted average exposures
Genetic and Individual Susceptibility
Genetic Factors:
- HLA genes: Certain variants increase susceptibility
- Cytokine gene polymorphisms: Affect inflammatory response
- DNA repair genes: Influence cancer risk
- Antioxidant enzyme genes: Affect oxidative damage response
Individual Risk Factors:
- Age at exposure: Younger individuals may be more susceptible
- Gender: Males historically more exposed due to occupations
- Baseline lung function: Pre-existing conditions affect risk
- Immune system status: May influence disease development
No Safe Level of Exposure
Scientific Consensus:
- No threshold below which asbestos is safe
- Any exposure carries some risk
- Linear dose-response relationship at low levels
- Regulatory standards aim to minimize, not eliminate risk
Synergistic Effects:
- Smoking: Dramatically increases lung cancer risk
- Other dusts: Silica, coal dust may worsen effects
- Viral infections: May influence inflammatory response
- Air pollution: May compound respiratory effects
5. Risk Factors
Primary Occupational Risk Factors
Highest Risk Occupations (Historical and Current):
Construction Industry:
- Insulation workers: Highest historical risk
- Demolition workers: Current high-risk group
- Roofers and tillers: Asbestos roofing materials
- Plumbers and electricians: Pipe and wire insulation
- Maintenance workers: Often encounter unexpected asbestos
Manufacturing and Industrial:
- Shipyard workers: Peak risk 1940s-1970s
- Power plant workers: Boiler and turbine insulation
- Railroad workers: Locomotive insulation, brakes
- Steel workers: Protective clothing, insulation
- Textile workers: Asbestos fabric production
Mining:
- Asbestos miners: Direct extraction workers
- Vermiculite miners: Contaminated with asbestos
- Talc miners: Some deposits contain asbestos
- General miners: Potential contamination
Demographic Risk Factors
Age:
- Older adults: Most at risk due to historical exposure
- Peak diagnosis age: 60-80 years
- Latency period: 15-40 years post-exposure
- Younger workers: Now protected by regulations
Gender:
- Male predominance: 80-90% of cases
- Occupational patterns: Historically male-dominated industries
- Household exposure: Wives of asbestos workers
- Changing patterns: More women in construction/trades
Geographic Factors:
- Industrial regions: Higher historical exposure
- Shipyard communities: Concentrated risk areas
- Natural deposits: Environmental exposure zones
- Developing countries: Ongoing occupational exposure
Environmental Risk Factors
Community Exposure:
Proximity to Industry
- Asbestos mines and mills
- Manufacturing facilities
- Power plants using asbestos
- Distance from source affects risk
Natural Deposits
- Serpentine geological formations
- Erosion and weathering
- Recreational activities in affected areas
- Agricultural use of contaminated land
Legacy Contamination
- Older buildings and schools
- Vermiculite attic insulation
- Deteriorating asbestos materials
- Improper disposal sites
Household and Family Risk
Secondary Exposure:
- Take-home contamination: Fibers on clothing, tools
- Family members: Spouses and children at risk
- Washing clothes: Handling contaminated garments
- Home renovations: Disturbing asbestos materials
Household Products:
- Vermiculite insulation: Libby, Montana contamination
- Talc products: Historical contamination
- Imported goods: Some countries still use asbestos
- Decorative materials: Some imported tiles, paper
Lifestyle and Behavioral Factors
Smoking:
- Synergistic effect: Dramatically increases lung cancer risk
- Multiplicative interaction: Not just additive
- Cessation benefits: Reduces but doesn’t eliminate excess risk
- Prevalence: High smoking rates in exposed workers
Other Factors:
- Alcohol consumption: May affect immune response
- Nutrition: Antioxidant intake may influence risk
- Physical fitness: Better baseline health may help
- Stress levels: Chronic stress affects immune function
Genetic and Host Factors
Genetic Susceptibility:
HLA Associations
- HLA-DRB1 and HLA-DQB1 variants
- Affect immune response to asbestos
- Influence disease severity
Cytokine Gene Polymorphisms
- TNF-α gene variants
- IL-1β polymorphisms
- TGF-β gene variations
Metabolic Genes
- NAT2 acetylator status
- GSTT1/GSTM1 deletions
- CYP1A1 polymorphisms
Individual Susceptibility Factors:
- Clearance mechanisms: Lung’s ability to clear fibers
- Inflammatory response: Individual variation in inflammation
- Fibrotic tendency: Genetic predisposition to scarring
- DNA repair capacity: Ability to repair cellular damage
Medical Risk Factors
Pre-existing Conditions:
- Lung disease: COPD, asthma may worsen outcomes
- Autoimmune disorders: May affect inflammatory response
- Immune suppression: Medications or conditions
- Previous lung injury: May increase susceptibility
Medical Interventions:
- Radiation therapy: To chest may increase risk
- Certain medications: May affect fiber clearance
- Surgical history: Previous lung surgery
Protective Factors
Factors That May Reduce Risk:
- Early detection: May improve outcomes
- Smoking cessation: Reduces additional damage
- Regular exercise: Maintains lung function
- Good nutrition: Antioxidants may help
- Avoiding re-exposure: Critical for disease progression
Workplace Protections:
- Personal protective equipment: Properly fitted respirators
- Engineering controls: Ventilation, containment
- Work practices: Wet methods, proper procedures
- Medical surveillance: Regular health monitoring
Cumulative Risk Assessment
Quantitative Risk Models:
- Fiber-years exposure: Cumulative dose metric
- Exposure matrices: Job-specific risk estimates
- Epidemiological studies: Population-based risk data
- Individual risk calculators: Personalized assessment tools
Risk Stratification:
- High risk: Heavy occupational exposure
- Moderate risk: Moderate occupational or environmental
- Low risk: Brief or light exposure
- Background risk: General population exposure
6. Complications
Respiratory Complications
Progressive Pulmonary Fibrosis:
Restrictive Lung Disease
- Decreased lung capacity and compliance
- Impaired gas exchange
- Ventilation-perfusion mismatch
- Progressive nature with worsening over time
Respiratory Failure
- Type I: Hypoxemic (oxygen deficiency)
- Type II: Hypercapnic (CO₂ retention) in late stages
- Exercise-induced initially, then at rest
- May require supplemental oxygen or ventilation
Pneumothorax
- Spontaneous lung collapse
- Risk increased due to subpleural fibrosis
- Can be life-threatening
- May recur after treatment
Cardiovascular Complications
Pulmonary Hypertension:
- Secondary to lung fibrosis: Most common cause
- Progressive elevation: Worsens with disease progression
- Right heart strain: Increased workload on right ventricle
- Exercise limitation: Further reduces functional capacity
Cor Pulmonale (Right Heart Failure):
- Development timeline: Usually in advanced disease
- Clinical manifestations:
- Peripheral edema (swelling)
- Ascites (abdominal fluid)
- Jugular vein distension
- Hepatomegaly (enlarged liver)
- Prognosis: Significantly reduces life expectancy
Malignant Complications
Lung Cancer:
Increased Risk
- All cell types increased
- Bronchogenic carcinoma most common
- Dose-dependent relationship
- Latency period 20-40 years
Synergistic Effect with Smoking
- Multiplicative interaction (not additive)
- Asbestos + smoking = 50-80x increased risk
- Accounts for most lung cancers in asbestos workers
Mesothelioma:
Pleural Mesothelioma
- Most common type (80-90%)
- Primary pleural tumor
- Poor prognosis (median survival 12-18 months)
- Pathognomonic of asbestos exposure
Peritoneal Mesothelioma
- Rare but catastrophic
- Lower survival rates
- Associated with heavy exposure
Pericardial/Testicular Mesothelioma
- Extremely rare
- Very poor prognosis
- Limited treatment options
Pleural Complications
Pleural Plaques:
- Bilateral calcified deposits: Usually asymptomatic
- Marker of exposure: Not necessarily progressive
- Functional impact: Minimal in isolation
- Malignant potential: Generally considered benign
Diffuse Pleural Thickening:
- Progressive scarring: Can cause restriction
- Functional impairment: Reduced lung capacity
- Symptoms: Dyspnea, chest pain
- Treatment challenges: Surgery rarely beneficial
Pleural Effusion:
- Benign pleural effusion: Early sign sometimes
- Malignant effusion: Associated with mesothelioma
- Recurrent nature: May require repeated drainage
- Diagnostic challenge: Distinguishing benign from malignant
Functional Complications
Exercise Intolerance:
- Reduced exercise capacity: Progressive limitation
- Activities of daily living: Eventually affected
- Quality of life: Severely impacted
- Social isolation: Due to breathlessness
Sleep Disturbances:
- Sleep apnea: May develop secondarily
- Orthopnea: Difficulty breathing lying flat
- Night symptoms: Coughing, breathlessness
- Poor sleep quality: Affects overall health
Nutritional and Metabolic Complications
Weight Loss and Muscle Wasting:
- Chronic disease state: Increased metabolic demands
- Poor appetite: Due to chronic illness
- Reduced activity: Leads to muscle atrophy
- Nutritional deficiencies: Common in advanced disease
Osteoporosis:
- Reduced activity: Bone density loss
- Corticosteroid use: If prescribed for inflammation
- Malnutrition: Affects bone health
- Fall risk: Due to weakness and breathlessness
Psychological and Social Complications
Mental Health Effects:
Depression
- High prevalence (30-50%)
- Related to chronic illness
- Functional limitations
- Poor prognosis awareness
Anxiety
- Breathlessness-related panic
- Fear of progression
- Medical anxiety
- Social situations
Cognitive Effects
- Hypoxia-related changes
- Medication effects
- Chronic illness impact
- Reduced quality of life
Social Complications:
- Employment issues: Disability, discrimination
- Financial burden: Medical costs, lost income
- Relationship strain: Family stress, caregiver burden
- Social isolation: Activity limitations
Mortality and Disability
Mortality Statistics:
- Overall survival: Varies with disease severity
- Median survival: 10-20 years post-diagnosis
- Factors affecting survival:
- Age at diagnosis
- Disease severity
- Smoking status
- Complications
Disability Rates:
- Mild disability: Early disease, some limitation
- Moderate disability: Significant functional impairment
- Severe disability: Unable to work, minimal activity
- Total disability: Requires full-time care
Long-term Prognosis
Disease Progression:
- Relentless progression: Generally does not stabilize
- Variable rate: Individual differences
- Factors affecting progression:
- Continued exposure
- Smoking status
- Concurrent illnesses
- Treatment compliance
End-stage Complications:
- Respiratory failure: Ultimate cause of death
- Right heart failure: Cardiovascular collapse
- Pulmonary infections: Increased susceptibility
- Complicated pneumonias: May be fatal
Prevention of Complications
Medical Management:
- Regular monitoring: Pulmonary function tests
- Vaccination: Flu, pneumonia prevention
- Exercise programs: Maintain function
- Nutritional support: Prevent malnutrition
Complication-Specific Prevention:
- Smoking cessation: Reduces cancer risk
- Oxygen therapy: For hypoxemia
- Heart failure management: ACE inhibitors, diuretics
- Mental health support: Counseling, medication
7. Diagnosis & Testing
Clinical Assessment
Medical History:
Exposure History
- Detailed occupational history
- Duration and intensity of exposure
- Type of asbestos if known
- Personal protective equipment use
- Secondary exposure sources
Symptom Assessment
- Timeline of symptom development
- Progression pattern
- Impact on daily activities
- Associated symptoms
Social and Family History
- Smoking history (crucial)
- Family history of lung disease
- General health status
- Current medications
Physical Examination:
- Inspection: Chest wall movement, cyanosis, clubbing
- Palpation: Chest expansion, tactile fremitus
- Percussion: Dullness over affected areas
- Auscultation: Fine crackles (rales) in lower lungs
Pulmonary Function Testing
Spirometry:
Key Measurements
- FVC (Forced Vital Capacity): Reduced
- FEV₁ (Forced Expiratory Volume): May be normal initially
- FEV₁/FVC ratio: Usually normal or increased
- Restrictive pattern: Characteristic finding
Disease Progression Monitoring
- Serial measurements important
- Rate of decline varies
- Smoking may cause mixed pattern
Advanced Pulmonary Function Tests:
- Lung volumes: Total lung capacity (TLC) reduced
- Diffusion capacity (DLCO): Often first abnormality
- Compliance studies: Lung stiffness measurement
- Exercise testing: Assess functional capacity
Chest Imaging
Chest X-ray:
ILO Classification System
- Profusion: 0/0 to 3/3 scale
- Shape: Irregular (s, t, u) or rounded (p, q, r)
- Size: Small opacities classification
- Distribution: Usually bilateral lower zones
Radiographic Features
- Early changes: Subtle linear markings
- Progressive changes: Increased profusion
- Advanced disease: “Shaggy heart” sign
- Pleural changes: Plaques, thickening
High-Resolution Computed Tomography (HRCT):
Superior Sensitivity
- Detects early disease before chest X-ray
- Better definition of extent and pattern
- Differentiates from other pneumoconioses
HRCT Findings
- Subpleural curvilinear lines: Early finding
- Honeycomb pattern: End-stage disease
- Ground glass opacities: Active inflammation
- Traction bronchiectasis: Advanced fibrosis
Clinical Utility
- Diagnostic confirmation
- Disease monitoring
- Staging severity
- Detecting complications
Laboratory Tests
Blood Tests:
Routine Studies
- Complete blood count
- Comprehensive metabolic panel
- Liver function tests
- Inflammatory markers (ESR, CRP)
Specialized Biomarkers
- KL-6 (Krebs von den Lungen-6): Pneumocyte marker
- SP-A and SP-D: Surfactant proteins
- YKL-40: Inflammatory marker
- Osteopontin: Fibroblast activity marker
Arterial Blood Gas Analysis:
- Hypoxemia: Common finding
- A-a gradient: Usually elevated
- Exercise-induced changes: More sensitive
- CO₂ retention: Late finding
Bronchoscopy
Indications:
- Differential diagnosis: Rule out other conditions
- Bronchoalveolar lavage: Analyze cells and fibers
- Lung biopsy: Rarely needed for diagnosis
- Complication assessment: Investigate new symptoms
Findings:
- BAL cell count: Increased total cells
- Neutrophils: Often elevated
- Asbestos bodies: May be present
- Ferruginous bodies: Iron-coated fibers
Tissue Biopsy
Indications (Rare):
- Atypical presentation
- Rapid progression
- Suspected malignancy
- Uncertain diagnosis
Procedure Options:
- Transbronchial biopsy: Limited yield
- Video-assisted thoracoscopy: Better tissue samples
- Open lung biopsy: Rarely needed
Histological Features:
- Pulmonary fibrosis: Bilateral lower lobe
- Asbestos bodies: Pathognomonic when present
- Collagen deposition: Progressive scarring
- Inflammatory infiltrates: Variable
Diagnostic Criteria
Standard Criteria (Helsinki Criteria 2014):
- Credible history of asbestos exposure
- Appropriate latency period (≥10 years)
- Bilateral lower lobe fibrosis on imaging
- Restrictive spirometry or reduced DLCO
- Exclusion of other causes
Supporting Evidence:
- Pleural plaques: Marker of exposure
- Asbestos bodies: In sputum or lung tissue
- Occupational history: Documented exposure
- Radiological progression: Over time
Differential Diagnosis
Conditions to Exclude:
Other Pneumoconioses
- Silicosis
- Coal worker’s pneumoconiosis
- Mixed dust pneumoconiosis
Idiopathic Pulmonary Fibrosis
- Similar symptoms and progression
- Different pattern on HRCT
- No exposure history
Connective Tissue Diseases
- Rheumatoid arthritis
- Scleroderma
- Sjögren’s syndrome
Drug-induced Lung Disease
- Chemotherapy agents
- Antibiotics
- Anti-inflammatory drugs
Early Detection and Screening
Surveillance Programs:
- High-risk occupations: Regular screening
- Chest X-ray frequency: Annual or biannual
- HRCT protocols: For early detection
- Pulmonary function: Serial testing
Screening Recommendations:
- Exposed workers: Regular health surveillance
- Family members: Consider screening
- Community exposure: Risk-based approach
- Cost-effectiveness: Debate continues
Modern Diagnostic Tools
Emerging Technologies:
- Exhaled breath analysis: Volatile organic compounds
- Serum biomarkers: Multiple protein panels
- Genetic testing: Susceptibility markers
- AI-assisted imaging: Computer-aided diagnosis
Future Developments:
- Molecular markers: Early disease detection
- Personalized medicine: Risk stratification
- Non-invasive monitoring: Continuous assessment
- Point-of-care testing: Rapid diagnosis
8. Treatment Options
Overview of Treatment Approach
Currently, there is no cure for asbestosis. Treatment is primarily supportive and symptomatic, focusing on:
- Symptom management
- Preventing disease progression
- Managing complications
- Improving quality of life
- Providing psychosocial support
Symptom Management
Respiratory Symptom Relief:
Oxygen Therapy
- Indications: Hypoxemia (PaO₂ <55 mmHg or O₂ sat <88%)
- Benefits: Improved exercise tolerance, better sleep
- Types: Continuous, nocturnal, or with exertion
- Monitoring: Regular assessment of oxygen needs
Bronchodilators
- Limited benefit: Unlike asthma or COPD
- Trial basis: May help in some patients
- Types: Short and long-acting beta-agonists
- Assessment: Monitor response carefully
Pulmonary Rehabilitation
- Exercise training: Improves functional capacity
- Education: Disease management, breathing techniques
- Nutritional counseling: Maintain optimal weight
- Psychosocial support: Address anxiety, depression
Anti-inflammatory and Antifibrotic Treatments
Corticosteroids:
- Limited evidence: Benefit unclear in stable disease
- Acute exacerbations: May help during rapid worsening
- Side effects: Significant with long-term use
- Monitoring: Careful risk-benefit assessment
Emerging Antifibrotic Agents:
Pirfenidone
- Mechanism: Antifibrotic and anti-inflammatory
- Evidence: Proven in IPF, trials in asbestosis
- Side effects: GI upset, photosensitivity
- Monitoring: Liver function, skin reactions
Nintedanib
- Mechanism: Tyrosine kinase inhibitor
- Evidence: Effective in IPF, potential in asbestosis
- Side effects: Diarrhea, liver toxicity
- Research: Ongoing trials in pneumoconioses
Management of Complications
Pulmonary Hypertension:
- Diagnosis: Right heart catheterization
- Treatment Options:
- Oxygen therapy: First-line approach
- Pulmonary vasodilators: Limited evidence
- Calcium channel blockers: Rarely effective
- PDE-5 inhibitors: Under investigation
Right Heart Failure (Cor Pulmonale):
- Diuretics: Manage fluid overload
- ACE inhibitors: May help some patients
- Digoxin: Limited role
- Oxygen: Essential for management
Respiratory Infections:
- Prevention: Vaccinations (influenza, pneumococcal)
- Early treatment: Prompt antibiotic therapy
- Pulmonary hygiene: Chest physiotherapy
- Monitoring: Watch for deterioration
Surgical Interventions
Lung Transplantation:
Candidate Selection
- Age typically <65-70 years
- End-stage disease
- No active malignancy
- Good functional status otherwise
Evaluation Process
- Comprehensive assessment
- Psychosocial evaluation
- Comorbidity assessment
- Support system evaluation
Outcomes
- 5-year survival: 50-60%
- Quality of life: Significantly improved
- Complications: Rejection, infection
- Immunosuppression: Lifelong requirement
Single vs. Bilateral Transplant:
- Single lung: Often sufficient for fibrotic disease
- Bilateral: May be preferred in younger patients
- Decision factors: Age, severity, wait times
Vaccination and Preventive Care
Recommended Vaccinations:
- Annual influenza: All patients
- Pneumococcal: PPSV23 and PCV13
- COVID-19: Complete series plus boosters
- Tdap: Every 10 years
Preventive Measures:
- Smoking cessation: Absolutely essential
- Avoid respiratory irritants: Pollution, chemicals
- Regular exercise: As tolerated
- Nutritional support: Maintain optimal nutrition
Palliative and End-of-Life Care
Palliative Care:
- Symptom management: Pain, dyspnea, anxiety
- Quality of life: Focus on comfort
- Advance directives: Early discussions
- Caregiver support: Family education and support
End-of-Life Considerations:
- Hospice care: When appropriate
- Comfort measures: Opioids for dyspnea
- Dignity: Respect patient wishes
- Bereavement support: For families
Emerging Treatments and Clinical Trials
Current Research Areas:
Antifibrotic Therapies
- Novel compounds: Beyond pirfenidone/nintedanib
- Combination therapies: Multiple mechanisms
- Targeted delivery: Lung-specific agents
Anti-inflammatory Approaches
- Selective inhibitors: Target specific pathways
- Immunomodulation: Regulatory T-cells
- Complement inhibition: Block inflammatory cascade
Cell-Based Therapies
- Mesenchymal stem cells: Anti-inflammatory effects
- Induced pluripotent stem cells: Regenerative potential
- Exosome therapy: Cell-free approaches
Gene Therapy
- Antifibrotic gene delivery: Direct to lungs
- microRNA modulation: Regulate fibrosis pathways
- CRISPR applications: Potential future therapy
Clinical Trial Considerations:
- Inclusion criteria: Disease stage, exposure history
- Outcome measures: Function, quality of life
- Trial design: Challenges in recruiting patients
- Regulatory approval: FDA/EMA considerations
Supportive Therapies
Nutritional Support:
- Caloric needs: May be increased
- Protein intake: Prevent muscle wasting
- Antioxidants: Vitamin C, E, selenium
- Weight management: Avoid obesity, malnutrition
Physical Therapy:
- Exercise prescription: Individualized programs
- Breathing techniques: Pursed lip breathing
- Chest percussion: Airway clearance
- Mobility aids: Oxygen carts, wheelchairs
Psychological Support:
- Counseling: Individual and family therapy
- Support groups: Peer connections
- Medication: Antidepressants if needed
- Coping strategies: Stress management
Monitoring and Follow-up
Regular Assessments:
- Clinical evaluation: Every 3-6 months
- Pulmonary function: Annual or semi-annual
- Chest imaging: Annual chest X-ray, periodic HRCT
- Oxygen saturation: Home monitoring
Specialist Referrals:
- Pulmonologist: Primary specialist care
- Cardiothoracic surgery: For transplant evaluation
- Oncology: For suspected malignancy
- Palliative care: For symptom management
Patient Education
Key Educational Points:
- Disease understanding: Natural history
- Symptom recognition: When to seek help
- Medication compliance: Importance of adherence
- Activity modification: Pace activities
- Emergency planning: Action plans for exacerbations
Resources:
- Patient organizations: Support and information
- Educational materials: Pamphlets, websites
- Smartphone apps: Symptom tracking
- Peer support: Patient mentorship programs
9. Prevention & Precautionary Measures
Primary Prevention (Exposure Prevention)
Regulatory Control Measures:
Asbestos Bans and Regulations
- Complete bans: Over 60 countries have banned asbestos
- Partial restrictions: Some countries limit specific uses
- Import restrictions: Control of asbestos-containing products
- Legacy management: Regulations for existing materials
Occupational Exposure Limits
- OSHA standard: 0.1 fibers/cm³ (8-hour TWA)
- Action level: 0.05 fibers/cm³ triggers medical surveillance
- ACGIH TLV: 0.01 fibers/cm³ (more protective)
- International variations: Different countries, different limits
Workplace Safety Measures:
Engineering Controls
- Ventilation systems: Local exhaust, general dilution
- Containment: Isolate work areas
- Wet methods: Suppress fiber release
- HEPA filtration: High-efficiency particulate air filters
Work Practice Controls
- Proper techniques: Training on safe procedures
- Prohibited practices: No dry sweeping, compressed air
- Waste disposal: Proper containerization and labeling
- Decontamination: Personnel and equipment cleaning
Personal Protective Equipment (PPE)
- Respirators: Half-face, full-face, powered air-purifying
- Fit testing: Ensure proper seal
- Protective clothing: Disposable suits, gloves, boots
- Eye protection: Safety glasses, goggles
Secondary Prevention (Early Detection)
Medical Surveillance Programs:
Pre-placement Examinations
- Baseline health assessment: Before exposure begins
- Chest X-ray: Reference for future comparison
- Pulmonary function tests: Establish baseline
- Medical history: Document prior exposures
Periodic Health Surveillance
- Annual examinations: For currently exposed workers
- Chest radiographs: ILO classification
- Respiratory questionnaire: Standardized symptom assessment
- Pulmonary function testing: Spirometry minimum
Post-exposure Surveillance
- Lifetime monitoring: For heavily exposed individuals
- Frequency: Risk-based intervals
- Early retirement: Medical removal protection
- Lung cancer screening: Consider CT screening
High-Risk Group Monitoring:
- Former asbestos workers: Continue surveillance
- Family members: Secondary exposure risk
- Community exposure: Environmental monitoring
- First responders: World Trade Center example
Personal Protection Strategies
For Working with Asbestos:
Respiratory Protection
- Minimum protection: N95 for short-term, low-level exposure
- Standard protection: P100 or equivalent
- High protection: Full-face respirator with P100 filters
- Highest protection: Supplied-air or SCSR systems
Protective Clothing
- Disposable suits: Tyvek or equivalent material
- Complete coverage: Head-to-toe protection
- Decontamination: Wet cleaning before removal
- Disposal: As asbestos waste
Work Practices
- Wet methods: Always use water sprays
- Minimal disturbance: Avoid unnecessary fiber release
- Proper cleanup: HEPA vacuuming, no sweeping
- Hand washing: Thorough cleaning after work
Safe Handling and Removal
Professional Abatement:
Licensed Contractors
- Certification required: State/federal licensing
- Training standards: 32-hour initial course
- Continuing education: Regular updates required
- Project notification: Regulatory agencies
Abatement Procedures
- Containment: Critical barriers, negative pressure
- Worker protection: Full protective equipment
- Waste handling: Double-bagging, proper labeling
- Air monitoring: During and after removal
Small-Scale Work:
- Professional recommendation: Even for minor work
- Homeowner guidance: When professional work not required
- Safety precautions: Minimal disturbance, wet methods
- Disposal requirements: Follow local regulations
Environmental Protection
Building Management:
Asbestos Surveys
- Pre-renovation/demolition: Required by law
- Building inspections: Regular assessment
- Materials sampling: Professional analysis
- Documentation: Maintain records
In-Place Management
- Encapsulation: Seal intact materials
- Enclosure: Physical barriers around materials
- Regular inspection: Monitor condition
- Maintenance protocols: Prevent disturbance
Community Protection:
- Zoning restrictions: Near natural deposits
- Air monitoring: Community exposure assessment
- Public education: Awareness programs
- Emergency response: Disaster planning
Home and Consumer Safety
Household Precautions:
Identifying Potential Asbestos
- Age of building: Pre-1980 most likely
- Common locations: Insulation, tiles, pipes
- Professional testing: When in doubt
- Assume presence: If unsure, treat as containing
Do-It-Yourself Guidelines
- Avoid disturbing: Leave intact if possible
- Small repairs only: Major work requires professionals
- Wet methods: Always use water
- Proper disposal: Follow local rules
Consumer Products
- Imported goods: Some may contain asbestos
- Vintage items: Older insulation, decorative materials
- Automotive parts: Some brake pads, gaskets
- Gardening materials: Some vermiculite products
Education and Training
Worker Training:
General Industry Training
- Awareness training: 2-hour minimum
- Operations and maintenance: 16-hour course
- Renovation/demolition: 32-hour course
- Refresher training: Annual requirements
Training Content
- Health effects: Disease risks
- Recognition: Where asbestos is found
- Work practices: Safe procedures
- Emergency procedures: Incident response
Public Education:
- School programs: Age-appropriate information
- Community workshops: Local exposure concerns
- Online resources: Government and NGO materials
- Healthcare provider training: Recognition and reporting
Regulatory Compliance
Key Regulations:
Occupational Safety
- OSHA standards: Construction and general industry
- EPA regulations: NESHAP, AHERA, TSCA
- State regulations: May be more stringent
- International standards: WHO, ILO guidelines
Environmental Protection
- Emission standards: Air quality protection
- Waste disposal: RCRA requirements
- Water protection: Clean Water Act provisions
- Emergency planning: SARA Title III
Compliance Assistance:
- Consultation programs: OSHA on-site help
- Training providers: Accredited courses
- Industry associations: Best practice guidance
- Legal compliance: Regular updates on changes
Special Considerations
Natural Asbestos Deposits:
- Geological surveys: Identify at-risk areas
- Land use restrictions: Limit development
- Dust control: Road paving, vegetation
- Public notification: Warning systems
Disaster Response:
- Emergency planning: Include asbestos considerations
- First responder protection: Proper equipment
- Debris management: Safe handling and disposal
- Community protection: Air monitoring, evacuation
Global Prevention Efforts
International Initiatives:
World Health Organization
- Global campaign: Elimination of asbestos-related diseases
- Technical guidelines: Prevention strategies
- Capacity building: Support for developing countries
- Monitoring systems: Global surveillance
International Labour Organization
- Convention 162: Safety in use of asbestos
- Technical standards: Workplace protection
- Training programs: Developing country support
- Research coordination: International collaboration
Challenges in Developing Countries:
- Continued use: Some countries still mine/use asbestos
- Limited resources: Inadequate protection measures
- Enforcement issues: Weak regulatory systems
- Technology transfer: Need for safer alternatives
Future Prevention Strategies
Research and Development:
- Safer substitutes: Continued development
- Detection methods: Better identification tools
- Exposure assessment: Improved monitoring
- Risk communication: More effective strategies
Policy Evolution:
- Global ban efforts: Push for universal prohibition
- Victim compensation: Fair and adequate systems
- Research funding: Support for prevention science
- International cooperation: Shared best practices
10. Global & Regional Statistics
Worldwide Disease Burden
Global Prevalence:
- Current cases: Estimated 200,000-400,000 people worldwide
- Annual new cases: 5,000-10,000 in developed countries
- Hidden burden: Likely underreported in developing nations
- Gender distribution: 80-90% male (historical occupational patterns)
Mortality Statistics:
- Annual deaths: Approximately 107,000-111,000 globally (2019 WHO data)
- Asbestos-related deaths:
- Lung cancer: ~60,000 deaths/year
- Mesothelioma: ~43,000 deaths/year
- Asbestosis: ~7,000 deaths/year
- Other: ~1,000 deaths/year
Regional Prevalence Patterns
Developed Countries (High Historical Exposure):
United States:
- Prevalence: Estimated 1.3-2.3 million exposed workers
- Annual cases: 2,000-3,000 new asbestosis diagnoses
- Latency period: Average 25-30 years
- Geographic distribution: Industrial centers, shipyards
European Union:
- Total burden: ~500,000 exposed workers still living
- Country variations: UK, Germany highest historical use
- Annual deaths: ~20,000 asbestos-related deaths
- Declining trend: Due to early bans (1980s-1990s)
United Kingdom:
- Historical peak exposure: 1960s-1980s
- Current annual deaths: ~5,000 (all asbestos diseases)
- Mesothelioma rates: Highest in the world
- Occupational groups: Shipbuilders, construction workers
Australia:
- Legacy of mining: Wittenoom mine caused epidemic
- Annual deaths: ~4,000 asbestos-related deaths
- Per capita rates: Among highest globally
- Compensation system: Extensive victim support
Japan:
- Industrial exposure peak: 1960s-1980s
- Annual deaths: ~10,000 asbestos-related deaths
- Geographic hotspots: Industrial ports, factories
- Recent recognition: Delayed acknowledgment of health risks
Developing Countries (Ongoing Exposure Risk)
Asia:
- China: World’s largest current asbestos consumer
- India: Significant ongoing use, limited regulation
- Southeast Asia: Growing industrial use
- Central Asia: Kazakhstan, Russia continue mining
Africa:
- South Africa: Historical mining, ongoing exposure
- Nigeria: Increasing industrial use
- Limited surveillance: Under-recognition of disease
South America:
- Brazil: Major producer until recent bans
- Argentina: Continuing some use
- Chile: Historical mining exposure
Occupational Disease Patterns
Highest Risk Industries:
Shipbuilding Industry:
- Peak exposure: WWII through 1970s
- Workers affected: Millions globally
- Current legacy: Aging workforce with disease
- Geographic concentration: Major ports worldwide
Construction Industry:
- Asbestos cement: Widely used 1950s-1980s
- Renovation workers: Current highest risk
- Global variation: Depends on regulation timing
- Urban concentration: Major cities most affected
Asbestos Mining:
- Historical sites: Canada, South Africa, Australia
- Community exposure: Entire populations affected
- Environmental legacy: Ongoing contamination
- Current activity: Russia, Kazakhstan, China
Manufacturing:
- Friction products: Brake, clutch manufacturing
- Insulation: Power plants, refineries
- Textiles: Fire-resistant clothing
- Shipyard equipment: Gaskets, pipes
Mortality Trends by Region
North America:
- Peak deaths projected: 2015-2020
- Current trend: Plateau/slight decline
- Age-adjusted rates: Declining in younger cohorts
- Geographic variations: Industrial vs. rural areas
Europe:
- Earlier peak: Due to earlier bans
- Current status: Past peak in most countries
- East-West divide: Eastern Europe later peak
- Gender patterns: Male predominance changing
Asia-Pacific:
- Rising trends: Many countries still seeing increases
- Lagged epidemic: 10-20 years behind Western countries
- Urbanization effect: Cities more affected
- Economic factors: Industrial development correlation
Economic Impact
Global Economic Burden:
- Healthcare costs: $3-5 billion annually
- Litigation costs: $200+ billion (US alone)
- Compensation programs: $50+ billion globally
- Lost productivity: Immeasurable economic impact
Country-Specific Economic Data:
United States:
- Annual healthcare: $1.5-2 billion
- Legal settlements: $200+ billion to date
- Workers’ compensation: $20+ billion
- Economic losses: Incalculable productivity loss
European Union:
- Healthcare costs: €2-3 billion annually
- Compensation schemes: Vary by country
- Research investment: €100+ million annually
- Prevention costs: Billions in remediation
Australia:
- Compensation payouts: $AUD 1+ billion annually
- Healthcare burden: $AUD 500+ million
- Research funding: Significant government investment
- Legal costs: Substantial ongoing litigation
Surveillance and Reporting
Surveillance Systems:
National Registries:
- Finland: Comprehensive occupational disease registry
- Sweden: Long-standing surveillance system
- Australia: National mesothelioma registry
- UK: World-class surveillance infrastructure
International Coordination:
- WHO surveillance: Global health observatory
- ILO reporting: Occupational disease statistics
- Research networks: International collaboration
- Data standardization: Improving comparability
Challenges in Data Collection:
- Underreporting: Especially in developing countries
- Diagnostic challenges: Requires specialized expertise
- Long latency: Deaths decades after exposure
- Attribution issues: Multiple exposure sources
Demographic Patterns
Age Distribution:
- Peak age: 65-75 years at diagnosis
- Latency period: 15-40 years (average 25-30)
- Cohort effects: Birth year influences risk
- Future projections: Aging of exposed cohorts
Gender Patterns:
- Historical male dominance: 80-90% of cases
- Changing patterns: More women affected
- Secondary exposure: Household exposure increasing
- Occupational changes: Women entering traditional male jobs
Socioeconomic Factors:
- Blue-collar predominance: Manual laborers most affected
- Education correlation: Lower education = higher risk
- Income effects: Poverty limits access to care
- Geographic disparities: Rural vs. urban differences
Future Projections
Epidemic Timing:
- Developed countries: Peak passed or approaching
- Developing countries: Epidemic still building
- Time lag: 20-40 years from peak use to peak mortality
- Duration: Epidemics last 50-70 years
Projected Death Tolls:
- Global total: 5-10 million deaths by 2050
- Regional variations: Asia seeing largest increases
- Prevention impact: Bans reducing future burden
- Cohort effects: Generational differences in risk
Research and Policy Implications
Research Priorities:
- Treatment development: Urgent need for therapies
- Early detection: Biomarkers and screening
- Prevention focus: Exposure reduction strategies
- Global coordination: International research efforts
Policy Challenges:
- Global ban efforts: Still incomplete coverage
- Developing country support: Technical assistance needed
- Victim compensation: Fair and adequate systems
- Research funding: Sustained investment required
Special Populations
Veterans:
- Military exposure: Significant historical risk
- Navy personnel: Highest exposure levels
- VA recognition: Established disability benefits
- Research focus: Ongoing studies
Environmental Exposure:
- Community outbreaks: Near mining sites
- Natural deposits: Geological exposure areas
- Disaster exposure: 9/11, other catastrophes
- Family exposure: Secondary and environmental
Occupational Subgroups:
- First responders: Emergency workers at risk
- Teachers: School building exposure
- Maintenance workers: Often overlooked group
- Retirees: Aging workforce with delayed disease
11. Recent Research & Future Prospects
Latest Therapeutic Advances (2020-2024)
Antifibrotic Drug Development:
Pirfenidone in Pneumoconioses
- Mechanisms: Multiple antifibrotic pathways
- Clinical trials: PRAISE study in asbestosis
- Results: Modest benefit in slowing progression
- Side effects: Generally well-tolerated
- Future: Combination therapy studies planned
Nintedanib Research
- Mechanism: Tyrosine kinase inhibitor
- Pneumoconiosis trials: Ongoing studies
- Asbestosis applications: Early-phase research
- Challenges: Cost and side effect profile
Novel Antifibrotic Compounds
- PBI-4050: Multi-target antifibrotic agent
- FG-3019: Anti-connective tissue growth factor
- Pamrevlumab: PDGF receptor antibody
- Inhaled formulations: Direct lung delivery systems
Biomarker Discovery and Validation
Diagnostic Biomarkers:
Serum/Plasma Markers
- KL-6 (Krebs von den Lungen-6): Pneumocyte damage marker
- SP-A and SP-D: Surfactant proteins
- YKL-40: Chitinase-like protein
- Osteopontin: Fibroblast activation marker
Genetic Biomarkers
- MUC5B promoter variant: Associated with fibrosis risk
- TERT mutations: Telomerase and aging pathways
- FAM13A polymorphisms: COPD-asbestosis overlap
- HLA associations: Immune response variations
Exhaled Breath Analysis
- Volatile organic compounds: Metabolic fingerprints
- Fractional exhaled nitric oxide: Inflammation marker
- Breath condensate: Non-invasive sample collection
- Electronic nose technology: Pattern recognition
Prognostic Biomarkers:
- Progression predictors: Rate of decline markers
- Mortality risk: Survival prediction models
- Complication risk: Heart failure, cancer development
- Treatment response: Personalized therapy selection
Immunotherapy and Immunomodulation
Targeting Inflammatory Pathways:
Anti-TNF Therapy
- Etanercept studies: Limited efficacy shown
- Infliximab research: Ongoing investigations
- Safety concerns: Infection risk in lung disease
- Patient selection: Identifying responders
Interleukin Inhibition
- IL-1β blocking: Anakinra and canakinumab
- IL-13 antagonists: Lebrikizumab studies
- IL-17 inhibition: Secukinumab research
- Multi-cytokine approaches: Broad spectrum targeting
Complement System Modulation
- C5a receptor antagonists: Avacopan studies
- Alternative pathway inhibition: Factor D targeting
- Lectin pathway: Mannose-binding lectin modulation
- Systemic vs. local delivery: Route optimization
Cell-Based and Regenerative Therapies
Stem Cell Research:
Mesenchymal Stem Cells (MSCs)
- Mechanisms: Anti-inflammatory, antifibrotic
- Clinical trials: Phase I/II studies ongoing
- Delivery methods: IV, intratracheal, nebulized
- Cell sources: Bone marrow, adipose, umbilical cord
Induced Pluripotent Stem Cells (iPSCs)
- Personalized therapy: Patient-specific cells
- Lung organoids: Disease modeling platforms
- Differentiation protocols: Generating lung cells
- Safety considerations: Tumorigenicity concerns
Exosome Therapy
- Cell-free approach: Reduced safety concerns
- Paracrine effects: Growth factors, microRNAs
- Targeting strategies: Lung-specific delivery
- Manufacturing: Scalable production methods
Tissue Engineering:
- Bioengineered lungs: Scaffold-based approaches
- Decellularization: Using natural lung matrix
- 3D bioprinting: Creating lung tissue constructs
- Organoid development: Mini-lung models
Gene Therapy Approaches
Therapeutic Targets:
Antifibrotic Gene Delivery
- Decorin overexpression: Reduces collagen
- Fibroblast growth factor-10: Promotes repair
- Hepatocyte growth factor: Anti-inflammatory
- Interferon-γ: Regulates fibroblast activity
microRNA Modulation
- miR-29: Antifibrotic microRNA
- miR-21 inhibition: Reduces fibroblast activation
- miR-200 family: Epithelial-mesenchymal transition
- Delivery vehicles: Nanoparticles, liposomes
CRISPR/Cas9 Applications
- Gene editing: Correcting fibrosis genes
- Epigenetic modification: Reversing disease changes
- Safety challenges: Off-target effects
- Delivery hurdles: Getting to lung cells
Diagnostic Technology Advances
Artificial Intelligence and Machine Learning:
Image Analysis
- HRCT interpretation: Automated scoring
- Pattern recognition: Disease classification
- Progression tracking: Quantitative changes
- Radiologist assistance: Decision support systems
Predictive Modeling
- Disease progression: Individual risk assessment
- Treatment response: Therapy selection
- Prognosis: Survival prediction models
- Multi-omics integration: Comprehensive analysis
Advanced Imaging Techniques:
- Dual-energy CT: Better tissue characterization
- PET-CT imaging: Functional assessment
- MRI applications: Non-radiation alternatives
- Optical coherence tomography: Detailed airway imaging
Precision Medicine Initiatives
Personalized Treatment Approaches:
Genetic Profiling
- Pharmacogenomics: Drug metabolism variants
- Disease susceptibility: Risk stratification
- Treatment selection: Targeted therapies
- Companion diagnostics: Test-drug combinations
Phenotyping Studies
- Disease subtypes: Molecular classifications
- Endotypes: Biological pathway analysis
- Biomarker panels: Multi-marker approaches
- Clinical clusters: Symptom-based grouping
Implementation Challenges:
- Cost considerations: Economic barriers
- Healthcare integration: System adoption
- Regulatory approval: Companion diagnostic approval
- Physician education: Training requirements
Novel Drug Delivery Systems
Targeted Delivery:
Inhaled Therapeutics
- Nanoparticle formulations: Improved deposition
- Liposomal delivery: Sustained release
- Dry powder inhalers: Stable formulations
- Smart inhalers: Dose tracking technology
Intratracheal Administration
- Direct lung delivery: Bronchoscopic procedures
- Gel formulations: Prolonged residence time
- Cell-based delivery: Carrier cell systems
- Targeting ligands: Specific cell uptake
Nanotechnology Applications:
- Targeted nanoparticles: Lung-specific delivery
- Theranostic systems: Combined therapy/imaging
- Smart drug release: Triggered by disease signals
- Biocompatibility: Safety considerations
Prevention Research
Advanced Exposure Assessment:
Personal Monitoring
- Wearable sensors: Real-time exposure tracking
- Smart PPE: Integrated monitoring systems
- Environmental sensors: Area monitoring
- Data analytics: Exposure pattern analysis
Genetic Susceptibility Testing
- Risk stratification: High-risk identification
- Preventive strategies: Targeted interventions
- Ethical considerations: Privacy concerns
- Implementation: Workplace applications
Global Research Collaboration
International Initiatives:
Research Networks
- Global Alliance against Asbestos: Research coordination
- International Mesothelioma Study: Multi-country collaboration
- WHO research priorities: Global health focus
- Academic partnerships: University collaborations
Data Sharing Platforms
- Genomic databases: Shared genetic information
- Clinical trial networks: Coordinated studies
- Biobank initiatives: Sample sharing
- Harmonized protocols: Standardized approaches
Challenges and Barriers
Research Obstacles:
Funding Limitations
- Orphan disease status: Limited commercial interest
- Long-term studies: Expensive longitudinal research
- Public funding: Dependent on government support
- Industry investment: Limited pharmaceutical interest
Regulatory Challenges
- Approval pathways: Complex for fibrotic diseases
- Endpoint selection: Meaningful clinical measures
- Trial design: Challenges in recruitment
- International harmonization: Regulatory differences
Technical Barriers
- Disease complexity: Multiple pathways involved
- Animal models: Limited predictive value
- Biomarker validation: Expensive and time-consuming
- Patient heterogeneity: Variable disease progression
Future Directions (2025-2035)
Short-term Goals (5 years):
- Validation of existing antifibrotic agents
- Biomarker implementation in clinical practice
- Advanced imaging integration
- Precision medicine pilot programs
Medium-term Prospects (10 years):
- First-generation cell therapies approved
- Personalized treatment protocols
- AI-assisted diagnosis standard
- Novel drug combinations available
Long-term Vision (15+ years):
- Regenerative medicine applications
- Gene therapy approaches
- Prevention of disease progression
- Potential cure or significant life extension
Research Investment Needs
Priority Areas for Funding:
- Basic science research: Understanding mechanisms
- Translational studies: Bench to bedside
- Clinical trials: Testing new treatments
- Prevention research: Reducing future burden
- Implementation science: Translating research to practice
Global Coordination Needs:
- Standardized research protocols
- Shared databases and biobanks
- Regulatory harmonization
- Technology transfer to developing countries
Patient and Community Engagement
Research Participation:
- Patient advocacy groups: Research prioritization
- Clinical trial recruitment: Community engagement
- Data sharing: Patient-generated data
- Outcome measures: Patient-important endpoints
Education and Awareness:
- Research literacy: Understanding trial participation
- Hope and realism: Balancing expectations
- Support systems: During research participation
- Knowledge translation: Research to practice
12. Interesting Facts & Lesser-Known Insights
Historical Curiosities
Ancient and Medieval Awareness:
- Pliny the Elder (79 AD): Observed lung problems in slaves who wove asbestos
- Marco Polo: Described “salamander fur” (asbestos cloth) in China
- Medieval legend: Asbestos was thought to be salamander hair
- “Miracle mineral”: Called “mountain leather” by ancient Greeks
Industrial Revolution Mysteries:
- Secret ingredient: Early asbestos use was often proprietary
- Magic material: Marketed as fireproof miracle substance
- Royal connections: Queen Elizabeth I reportedly had asbestos tablecloth
- Military applications: Used in medieval siege defense
Unusual Properties and Applications
Remarkable Physical Properties:
- Heat resistance: Can withstand temperatures over 1,000°C
- Chemical inertness: Resistant to most acids and alkalis
- Tensile strength: Stronger than steel wire of same thickness
- Flexibility: Can be woven like cotton or wool
- Sound absorption: Excellent acoustic insulation properties
Bizarre Historical Uses:
- Funeral shrouds: Ancient Romans used for cremation cloth
- Stage curtains: Theaters used asbestos fire curtains
- Cooking pots: Some cultures made fireproof cookware
- Cigarette filters: Kent cigarettes used crocidolite (1952-1956)
- Snow on movie sets: Hollywood used asbestos for fake snow
Scientific Peculiarities
Fiber Characteristics:
- Microscopic size: 1,200 times thinner than human hair
- Aerodynamic properties: Can float in air for days
- Biopersistence: Fibers remain in lungs for decades
- Splitting tendency: One fiber can split into millions
- Magnetic properties: Some types are weakly magnetic
Biological Mysteries:
- Frustrated phagocytosis: Immune cells can’t digest fibers
- Selective toxicity: Different fiber types cause different diseases
- Latency paradox: Disease appears decades after exposure
- Threshold controversy: No scientifically established “safe” level
Geographic Anomalies
Natural Occurrence Hotspots:
- New Caledonia: 40% of island is serpentine rock containing asbestos
- Cyprus: Ancient asbestos mining sites still visible
- Quebec, Canada: Has world’s largest open-pit asbestos mine
- Ural Mountains: Extensive natural deposits
Environmental Exposures:
- Libby, Montana: Entire town contaminated by vermiculite mine
- Turkey’s “white death”: Villages built on asbestos-rich rock
- Australian ghost towns: Abandoned due to asbestos contamination
- Desert exposure: Natural erosion creates airborne fibers
Occupational Ironies
Protective Gear Made from Asbestos:
- Firefighter equipment: Suits and helmets contained asbestos
- Welding blankets: Made from asbestos fabric
- Industrial gloves: Heat-resistant asbestos gloves
- Rescue equipment: Ironically exposed those meant to save others
Industries with Unexpected Exposure:
- Tea processing: Asbestos in machinery insulation
- Breweries: Filtration systems used asbestos
- Hairdressing: Some hair dryers contained asbestos
- Jewelry making: Soldering boards made from asbestos
Diagnostic Curiosities
Unusual Presentations:
- Radiographic lag: Chest X-rays normal for years despite symptoms
- Unilateral disease: Rare cases affecting only one lung
- Rapid progression: Some cases worsen quickly after diagnosis
- Silent disease: Advanced disease with minimal symptoms
Diagnostic Challenges:
- Asbestos bodies: Only found in 50-80% of cases
- False negatives: Early disease often missed on X-rays
- Mimicry: Can look like other lung diseases
- Reader variability: Different radiologists, different interpretations
Legal and Social Phenomena
Litigation Extremes:
- Longest-running cases: Some lawsuits span decades
- Largest settlements: Billions paid to single plaintiffs
- Forum shopping: Plaintiffs seek favorable jurisdictions
- Corporate bankruptcy: Entire companies dissolved due to asbestos liability
Cultural Impact:
- “Mesothelioma commercials”: Ubiquitous TV advertising
- Support groups: Strong online communities formed
- Advocacy movements: Patient-driven research initiatives
- Media attention: Regular documentary and news coverage
Technological Surprises
Modern Unexpected Uses:
- Space industry: Still used in some specialized applications
- Brake pads: Some developing countries still use asbestos
- Gaskets: High-temperature applications in some industries
- Roofing materials: Still manufactured in some countries
Detection Technology:
- Electron microscopy: Required for fiber identification
- Phase contrast: Original detection method
- Transmission methods: See-through fiber identification
- Polarized light: Distinguishes asbestos from other fibers
Medical Mysteries
Unexplained Phenomena:
- Gender differences: Men and women develop different disease patterns
- Ethnic variations: Some populations more susceptible
- Family clusters: Genetic factors influence susceptibility
- Protective factors: Some heavy exposures don’t develop disease
Treatment Paradoxes:
- Anti-inflammatories: May sometimes worsen fibrosis
- Oxygen therapy: Can be both helpful and harmful
- Exercise: Beneficial despite breathing difficulties
- Smoking cessation: Benefits even after disease development
Economic Oddities
Market Contradictions:
- Continued mining: Some countries increase production while others ban
- Price fluctuations: Dramatic swings based on regulations
- Black markets: Illegal trade in banned countries
- Substitution costs: Safer alternatives often more expensive
Insurance Anomalies:
- Prediction failures: Insurers underestimated liability
- Long-tail risk: Claims appear decades after policies end
- Global coverage: Some insurers cover claims worldwide
- Reinsurance crisis: Multiple insurance company failures
Research Surprises
Unexpected Findings:
- Protective genes: Some people genetically resistant
- Beneficial bacteria: Lung microbiome affects disease progression
- Antioxidant paradox: Some antioxidants worsen outcomes
- Exercise benefits: Movement helps despite breathing difficulties
Scientific Controversies:
- Threshold debates: Safe exposure level arguments continue
- Chrysotile controversy: “White asbestos” safety claims
- Animal model limitations: Differences from human disease
- Biomarker challenges: Few reliable blood tests available
Future Predictions
Surprising Developments Expected:
- Nanotechnology solutions: Microscopic removal of fibers
- Genetic therapy: Modifying immune response to fibers
- Bacterial treatments: Using microbes to break down fibers
- Regenerative medicine: Growing new lung tissue
Social Changes:
- Younger demographics: More women and younger patients
- Global shift: Disease burden moving to developing countries
- Technology integration: Smart devices monitoring exposure
- Lifestyle factors: Exercise and nutrition becoming more important
Myths vs. Reality
Common Misconceptions:
Myth: “Short exposure can’t cause disease” Reality: Even brief exposure can lead to disease
Myth: “Only workers get asbestos disease” Reality: Family members and community exposure occurs
Myth: “White asbestos is safe” Reality: All types of asbestos are dangerous
Myth: “If you don’t have symptoms, you’re fine” Reality: Disease can be asymptomatic for decades
Myth: “Asbestos disease is curable” Reality: No cure exists, only supportive treatment
Professional Misconceptions:
- Some doctors still underestimate exposure risks
- Radiologists may miss early disease changes
- Insurance companies often deny claims incorrectly
- Employers sometimes downplay exposure risks
Global Variations
Cultural Differences:
- Compensation systems: Wide variation in victim support
- Medical recognition: Some countries resist acknowledging disease
- Prevention efforts: Dramatic differences in protection measures
- Research investment: Varies greatly by country
Language and Communication:
- Multiple names: Different terms for asbestos diseases
- Translation challenges: Technical terms vary by language
- Patient education: Cultural barriers to understanding
- Medical communication: Explaining complex concepts globally
The Human Element
Patient Stories:
- Delayed recognition: Years of misdiagnosis common
- Family impact: Disease affects entire families
- Courage and advocacy: Patients driving research forward
- Quality of life: Finding meaning despite illness
Healthcare Heroes:
- Pioneering doctors: Early recognizers of disease
- Dedicated researchers: Scientists working without profit motive
- Compassionate nurses: Providing comfort and care
- Legal advocates: Fighting for patient rights
Environmental Surprises
Natural Phenomena:
- Geological formations: Asbestos creates beautiful landscapes
- Wildlife effects: Animals also develop asbestos-related disease
- Plant interactions: Some plants can absorb asbestos fibers
- Weather patterns: Wind and rain affect fiber distribution
Cleanup Challenges:
- Contaminated soil: Difficult to completely remove
- Water contamination: Fibers can pollute water supplies
- Air persistence: Fibers remain airborne for extended periods
- Disposal dilemmas: Safe disposal remains challenging
Conclusion
Asbestosis represents one of the most significant preventable occupational health disasters in human history, serving as a stark reminder of the importance of prioritizing worker and public health over industrial profits. From its ancient recognition by Pliny the Elder to the modern global epidemic affecting hundreds of thousands, asbestosis exemplifies how commercial interests can tragically override scientific evidence and human welfare.
The disease’s unique pathophysiology—irreversible pulmonary fibrosis caused by virtually indestructible mineral fibers—makes prevention the only truly effective intervention. While current treatment remains supportive rather than curative, emerging research in antifibrotic agents, cell therapy, and precision medicine offers hope for improved management and potentially disease modification.
The global burden continues to evolve, with developed countries experiencing the delayed consequences of peak asbestos use decades ago, while developing nations face ongoing exposure risks. The latency period of 15-40 years means that even with complete global bans, new cases will continue to emerge for decades, making continued vigilance in diagnosis, treatment, and support essential.
Perhaps most importantly, asbestosis serves as a powerful case study in occupational health, demonstrating how early recognition of health hazards, proper regulation, and effective prevention measures can dramatically reduce disease burden. The lessons learned from the asbestos epidemic continue to inform modern approaches to evaluating and managing occupational and environmental health risks.
For healthcare providers, maintaining awareness of exposure histories and the disease’s varied presentations remains crucial for timely diagnosis. For policymakers, the asbestos experience underscores the importance of applying the precautionary principle when evaluating potentially hazardous materials. For affected individuals and families, understanding the disease’s trajectory and available support systems can help navigate the challenging journey of living with asbestosis.
As we move forward, continued research investment, global cooperation in prevention efforts, and support for affected individuals will be essential to minimize the ongoing impact of this entirely preventable disease. The ultimate goal remains a world where no one develops asbestosis—a goal achievable through sustained commitment to public health, worker protection, and environmental safety.
This comprehensive report reflects the current understanding of asbestosis based on medical literature available through October 2024. Clinical decisions should always be made in consultation with qualified healthcare professionals familiar with the patient’s specific circumstances and current medical guidelines.