
⚠️ Disclaimer: The information provided in this article is for educational purposes only and does not constitute medical advice. RevisionTown does not provide diagnosis, treatment, or medical recommendations. Always consult a qualified healthcare professional regarding any medical condition, symptoms, or concerns.
Read More – 🏥 Medical Disclaimer
Comprehensive Report on Acid Reflux
1. Overview
What is Acid Reflux?
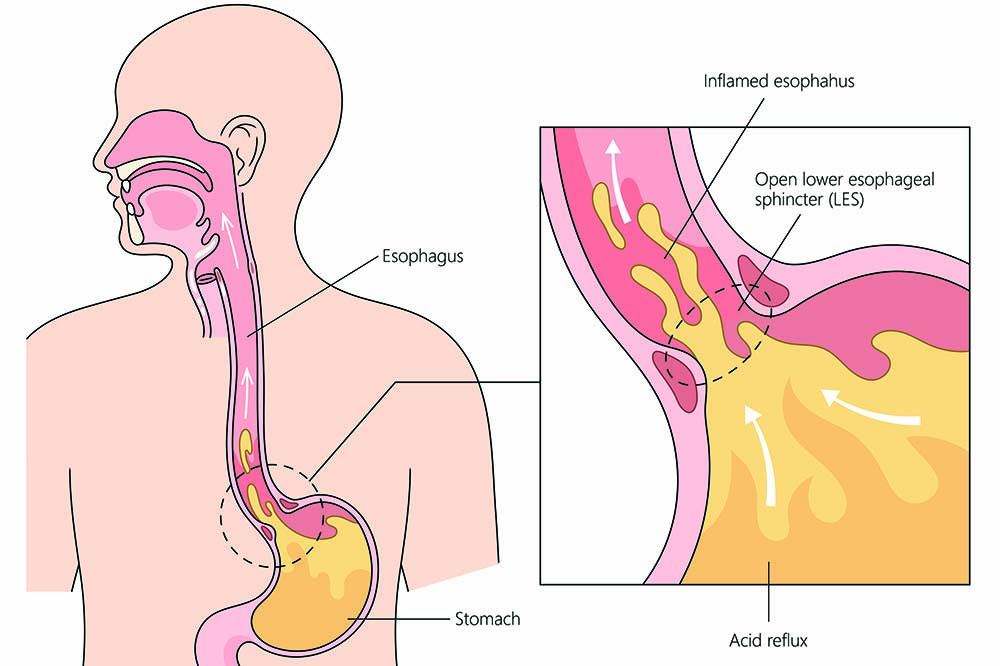
Acid reflux, medically known as gastroesophageal reflux disease (GERD), is a chronic digestive disorder characterized by the retrograde flow of stomach contents into the esophagus. This backflow occurs when the lower esophageal sphincter (LES), a ring-like muscle at the junction between the esophagus and stomach, becomes weak or relaxes inappropriately. While occasional acid reflux is common and not a cause for concern, persistent reflux can lead to inflammation, tissue damage, and various complications.
GERD exists on a spectrum of severity, from mild, intermittent symptoms to severe, daily episodes that significantly impact quality of life. The condition may be classified as:
- Non-erosive reflux disease (NERD): Symptoms are present without visible esophageal injury
- Erosive esophagitis: Inflammation and erosions are evident in the esophageal lining
- Complicated GERD: Characterized by strictures, Barrett’s esophagus, or esophageal adenocarcinoma
Affected Body Parts/Organs
Acid reflux primarily affects the digestive system, with several key structures involved:
- Esophagus: The muscular tube connecting the throat to the stomach, which can become inflamed, eroded, or structurally altered due to chronic acid exposure
- Lower Esophageal Sphincter (LES): The muscular valve between the esophagus and stomach that normally prevents backflow
- Diaphragm: The muscle separating the chest from the abdomen, which provides additional support to the LES
- Stomach: Produces the acidic contents that reflux upward
- Proximal Duodenum: The first part of the small intestine, which may contribute bile and digestive enzymes to refluxate
Secondary systems affected include:
- Respiratory System: Refluxed material can be aspirated into the lungs, causing inflammation or infection
- Oropharyngeal Structures: The throat, larynx, and mouth can be damaged by refluxed acid
- Dental Structures: Tooth enamel can be eroded by frequent acid exposure
Prevalence and Significance
Acid reflux represents one of the most common chronic digestive conditions worldwide:
- Global Prevalence: Approximately 8-33% of the population experiences GERD symptoms at least weekly, with significant geographical variations
- Western Countries: Prevalence ranges from 18-28%, with North America and Western Europe showing the highest rates
- Asia: Traditionally lower prevalence (5-10%), but rapidly increasing due to urbanization and Western dietary influences
- Gender Distribution: Generally equal between men and women, though certain complications show gender preferences
- Age Distribution: Prevalence increases with age, with peak onset between 45-64 years
The significance of GERD extends beyond symptom burden to include:
Economic Impact:
- Direct healthcare costs estimated at $8-10 billion annually in the United States alone
- Indirect costs due to decreased productivity and absenteeism exceed $75 billion globally
- Proton pump inhibitors (PPIs), the primary medication for GERD, account for more than $10 billion in annual pharmaceutical expenditures worldwide
Quality of Life Impact:
- GERD significantly impairs sleep, dietary enjoyment, social functioning, and work productivity
- Studies show quality of life impairment comparable to other chronic conditions like diabetes and heart failure
- 75% of patients report that symptoms affect their daily activities
Public Health Significance:
- GERD is the primary risk factor for esophageal adenocarcinoma, a cancer with rapidly increasing incidence in Western populations
- The condition represents one of the most common reasons for primary care visits and specialist referrals
- Self-medication for GERD symptoms contributes to potential medication interactions and adverse effects
The prevalence of GERD continues to rise globally, likely due to increasing obesity rates, dietary changes, aging populations, and improved diagnostic recognition, making this condition a priority for clinical care and research.
2. History & Discoveries
Early Recognition and Description
The symptoms of acid reflux have been recognized throughout medical history, though understanding of the underlying mechanism evolved gradually:
Ancient References:
- Egyptian medical papyri (circa 1550 BCE) described remedies for “heat in the chest,” possibly referring to heartburn
- Hippocrates (circa 400 BCE) noted the connection between certain foods and gastric discomfort rising to the chest
- Avicenna’s Canon of Medicine (1025 CE) described symptoms consistent with reflux and recommended elevation of the head during sleep
First Medical Descriptions:
- In 1618, Fabricius ab Aquapendente first described the anatomical anti-reflux mechanism at the gastroesophageal junction
- In 1732, German physician Georg Stahl provided one of the first clear descriptions of reflux disease as distinct from other gastric ailments
- In 1839, English physician William Brinton detailed “dyspeptic asthma,” recognizing the connection between digestive issues and respiratory symptoms
Key Historical Figures
- Philip Allison & Alan Johnstone (1943): First described hiatal hernia’s relationship to reflux symptoms
- Rudolf Nissen (1956): Developed the fundoplication surgical technique, the first effective surgical treatment for GERD
- Norman Barrett (1950): Described the condition now known as Barrett’s esophagus, a serious complication of chronic GERD
- Spencer Thorpe & André Robert (1960s): Established the role of acid in causing esophageal injury
- Rudolph Schindler (1932): Developed semi-flexible endoscopy, revolutionizing the ability to visualize GERD complications
- George Berci & M.E. Monie (1970s): Pioneered fiberoptic endoscopy, further advancing diagnostic capabilities
- George Sachs & A.L. Ganser (1977): Discovered the proton pump mechanism in gastric acid production, leading to PPI development
Major Discoveries and Breakthroughs
- 1940s-1950s: Recognition of hiatal hernia as a contributing factor to reflux
- 1956: Introduction of the Nissen fundoplication surgical procedure
- 1959: Bernstein acid perfusion test developed, establishing causality between acid and symptoms
- 1970s: Development of pH monitoring techniques for objective measurement of acid reflux
- 1976: Introduction of H2-receptor antagonists (H2RAs), the first effective pharmacological treatment for GERD
- 1980s:
- Development of proton pump inhibitors (PPIs), revolutionizing medical management
- Recognition of non-acid reflux and its clinical significance
- 1990s:
- Laparoscopic techniques for anti-reflux surgery introduced
- Identification of transient LES relaxations as a key mechanism in GERD
- 2000s:
- Introduction of impedance-pH monitoring to detect both acid and non-acid reflux
- Development of endoscopic anti-reflux procedures
- Recognition of the “acid pocket” concept
- 2010s:
- FDA approval of the LINX device, a magnetic sphincter augmentation system
- Elucidation of the role of the esophageal microbiome in GERD pathogenesis
- Development of potassium-competitive acid blockers (P-CABs) as alternatives to PPIs
Evolution of Medical Understanding
The conceptual understanding of GERD has evolved significantly:
Pre-1950s Era: Anatomical Focus
- GERD was primarily attributed to hiatal hernia
- Treatment focused on anatomical correction
- Limited understanding of physiological mechanisms
1950s-1970s: Acid-Centric Era
- Recognition that acid exposure is the primary cause of esophageal injury
- Development of acid suppression strategies
- Introduction of pH monitoring as the gold standard diagnostic tool
1980s-1990s: Motility Era
- Identification of LES pressure abnormalities and transient LES relaxations
- Recognition of esophageal dysmotility as a contributing factor
- Understanding of delayed gastric emptying as a risk factor
2000s-Present: Multifactorial Era
- Recognition of GERD as a complex disorder with multiple contributing factors
- Understanding of both acid and non-acid reflux components
- Appreciation of the esophageal microbiome’s role
- Recognition of genetic and environmental interactions
- Identification of different GERD phenotypes requiring personalized approaches
This evolution reflects a progression from a simplistic, single-cause view to a nuanced understanding of GERD as a multifactorial condition requiring individualized assessment and treatment approaches. Each era built upon previous knowledge while introducing new paradigms that expanded therapeutic options and improved patient outcomes.
3. Symptoms
Acid reflux presents with a wide spectrum of symptoms that can vary in severity, frequency, and presentation. Understanding the range of manifestations is crucial for proper diagnosis and management.
Early Symptoms vs. Advanced-Stage Symptoms
Early/Mild Symptoms:
- Heartburn: A burning sensation in the chest, often after eating, which may worsen when lying down or bending over
- Regurgitation: The sensation of stomach contents or sour liquid backing up into the throat or mouth
- Dyspepsia: Upper abdominal discomfort, bloating, or nausea
- Mild dysphagia: Occasional difficulty swallowing, particularly with solid foods
- Throat clearing: Frequent need to clear the throat
- Mild cough: Particularly after meals or while lying down
- Mild hoarseness: Especially in the morning
Advanced/Severe Symptoms:
- Persistent, intense heartburn: Unresponsive to over-the-counter medications
- Painful swallowing (odynophagia): Due to esophageal inflammation or ulceration
- Progressive dysphagia: Increasing difficulty swallowing that may progress from solids to liquids
- Chest pain: Can mimic cardiac pain, sometimes severe enough to prompt emergency evaluation
- Respiratory complications: Chronic cough, asthma exacerbations, recurrent pneumonia
- Severe laryngeal symptoms: Voice loss, chronic laryngitis, sensation of a lump in the throat (globus)
- Food impaction: Food becoming stuck in the esophagus due to strictures or inflammation
- Weight loss: Due to dietary limitations, dysphagia, or pain with eating
- Sleep disruption: Night-time reflux causing awakening, choking, or gasping
- Dental erosions: Visible damage to tooth enamel from acid exposure
Common vs. Rare Symptoms
Common Symptoms (Present in >20% of patients):
- Heartburn (80-90% of GERD patients)
- Regurgitation (54-70%)
- Epigastric discomfort (38-50%)
- Throat clearing (42%)
- Mild dysphagia (30-40%)
- Chronic cough (25-40%)
- Sleep disturbances (25-30%)
Less Common Symptoms (5-20% of patients):
- Hoarseness or voice changes
- Chest pain without heartburn
- Globus sensation (feeling of a lump in the throat)
- Excessive salivation (water brash)
- Nausea
- Halitosis (bad breath)
- Morning sore throat
Rare Symptoms (<5% of patients):
- Ear pain or recurrent otitis media
- Idiopathic pulmonary fibrosis
- Recurrent laryngospasm
- Vocal cord granulomas
- Subglottic stenosis
- Dental erosions as presenting symptom
- Recurrent sinusitis
Atypical Presentations
GERD can manifest with extraesophageal symptoms that may not be immediately recognized as related to reflux:
Respiratory manifestations:
- Chronic cough (particularly dry, nocturnal cough)
- Asthma or wheezing, especially adult-onset or nocturnal
- Recurrent bronchitis or pneumonia
- Pulmonary aspiration
Ear, nose, and throat manifestations:
- Chronic laryngitis
- Posterior laryngitis
- Voice fatigue or hoarseness
- Excessive throat mucus
- Chronic sinusitis
- Recurrent ear infections
Miscellaneous manifestations:
- Non-cardiac chest pain
- Sleep apnea exacerbation
- Chronic hiccups
- Globus pharyngeus
Symptom Progression Over Time
The natural history of GERD symptoms typically follows patterns that can be influenced by treatment, lifestyle modifications, and the development of complications:
Initial Presentation:
- Often begins with occasional postprandial heartburn
- Episodes may be triggered by specific foods, positions, or activities
- Symptoms typically resolve spontaneously or with over-the-counter remedies
- Symptom-free intervals between episodes
Progression Without Intervention:
- Increasing frequency of episodes (weekly to daily)
- Increasing severity and duration of symptoms
- Development of additional symptoms beyond heartburn
- Diminishing response to over-the-counter remedies
- Nighttime symptoms emerging, disrupting sleep
Advanced Progression:
- Daily symptoms affecting quality of life
- Emergence of dysphagia or odynophagia suggesting complications
- Development of extraesophageal manifestations
- Symptoms occurring despite dietary restrictions
- Incomplete response to standard medical therapy
Long-term Patterns:
- Persistent Pattern: Continuous symptoms with little variation over time (30% of patients)
- Progressive Pattern: Gradual worsening in frequency and severity (25%)
- Relapsing-Remitting Pattern: Periods of exacerbation alternating with symptom-free intervals (35%)
- Resolving Pattern: Initial symptoms that improve and eventually resolve (10%)
Factors Influencing Symptom Progression:
- Weight gain typically worsens symptoms
- Aging is associated with increasing symptom severity, particularly dysphagia
- Pregnancy often induces or exacerbates symptoms, with resolution post-partum
- Stress and anxiety are associated with symptom exacerbation
- Medication changes can impact symptom patterns
- Dietary changes can improve or worsen the symptom profile
Understanding the diverse symptom presentations of GERD is essential for proper diagnosis, especially since many patients present with atypical symptoms that may not immediately suggest a gastroesophageal etiology. Furthermore, symptom severity does not always correlate with the degree of esophageal damage, as some patients with severe esophagitis report minimal symptoms, while others with non-erosive disease experience substantial discomfort.
4. Causes
Acid reflux results from a complex interplay of anatomical, physiological, genetic, and environmental factors. Understanding these multifactorial causes is essential for effective management.
Biological Mechanisms
Primary Pathophysiological Mechanisms:
Lower Esophageal Sphincter (LES) Dysfunction:
- Hypotensive LES: Reduced resting pressure of the sphincter (<10 mmHg) allowing reflux during normal activities
- Transient LES Relaxations (TLESRs): Inappropriate spontaneous relaxations unrelated to swallowing, accounting for 50-80% of reflux episodes
- Anatomical Disruption: Hiatal hernia disrupting the gastroesophageal junction integrity
Esophageal Clearance Abnormalities:
- Impaired Peristalsis: Weak or ineffective esophageal contractions reducing acid clearance
- Reduced Salivation: Decreased neutralization of refluxed acid
- Gravity Effects: Supine position limiting the natural clearance mechanism
Gastric Factors:
- Delayed Gastric Emptying: Prolonged stomach distention promoting reflux
- Increased Gastric Acid Production: Heightening the damaging potential of refluxate
- Acid Pocket: Postprandial layering of highly acidic secretions at the gastroesophageal junction
Mucosal Defense Impairment:
- Reduced Epithelial Resistance: Decreased cellular junctions allowing acid penetration
- Impaired Tissue Recovery: Delayed healing after acid exposure
- Altered Mucus Production: Reduced protective barrier
Environmental Causes
Multiple environmental factors can trigger or exacerbate acid reflux:
Dietary Factors:
- Food Triggers: High-fat meals, chocolate, citrus, tomato-based products, spicy foods, coffee, carbonated beverages
- Meal Patterns: Large meals, late-night eating
- Alcohol Consumption: Particularly red wine, beer, and liquor
Behavioral Factors:
- Body Position: Recumbent position after meals, slouching
- Exercise: High-impact activities, abdominal straining, weight lifting
- Smoking: Both active and passive exposure
- Sleep Patterns: Inadequate sleep duration, sleep position
Medication-Induced Reflux:
- Smooth Muscle Relaxants: Calcium channel blockers, nitrates, theophylline
- Anti-Inflammatory Drugs: NSAIDs, corticosteroids
- Anticholinergics: Tricyclic antidepressants, antihistamines
- Hormonal Medications: Progesterone, estrogen
Physical Pressure Factors:
- Tight Clothing: Constrictive garments around the abdomen
- Occupational Positions: Bending, lifting, straining
- Obesity: Increased intra-abdominal pressure
- Pregnancy: Hormonal changes and physical pressure
Genetic and Hereditary Factors
Emerging research indicates substantial genetic contributions to GERD susceptibility:
Heritability Estimates:
- Twin studies indicate 30-45% heritability for GERD symptoms
- Family studies show 2-3 fold increased risk among first-degree relatives
- Monozygotic twins show 42% concordance versus 26% in dizygotic twins
Specific Genetic Associations:
- COL3A1 gene: Collagen synthesis affecting tissue integrity
- BARX1, FOXF1 genes: Involved in development of the gastroesophageal junction
- MHC/HLA complex genes: Influencing inflammatory responses
- GERD-specific loci: 25 genetic loci identified in genome-wide association studies
Inherited Conditions Associated with GERD:
- Ehlers-Danlos syndrome: Connective tissue disorder affecting sphincter function
- Scleroderma: Autoimmune condition causing esophageal dysmotility
- Cystic fibrosis: Associated with significant GERD in 35-82% of patients
- Congenital disorders: Esophageal atresia, tracheoesophageal fistula repair
Epigenetic Factors:
- DNA methylation patterns influenced by environmental exposures
- Altered gene expression affecting esophageal barrier function
- Inheritance of microbiome patterns affecting digestion
Known Triggers and Exposure Risks
Certain specific exposures can trigger or worsen acid reflux symptoms:
Immediate Triggers:
- Dietary: Coffee, chocolate, alcohol, acidic foods, peppermint, fatty meals
- Positional: Bending over, lying down after eating
- Pressure-Inducing: Coughing, vomiting, heavy lifting, straining
- Medications: NSAIDs, antibiotics, potassium supplements
Cumulative Exposure Risks:
- Chronic Tobacco Use: 1.35-1.7 fold increased risk
- Helicobacter pylori status: Complex relationship, with some evidence that eradication may unmask or worsen GERD
- Air Pollution: Emerging evidence for traffic-related pollution increasing risk
- Shift Work: Disruption of circadian rhythms affecting gastric acid secretion
Occupational Exposures:
- Physical Labor: Jobs requiring heavy lifting, bending, or straining
- Desk-Based Professions: Prolonged sitting and poor posture
- Occupational Stress: High-pressure environments
- Specific Industries: Construction, transportation, healthcare (shift work)
Psychosocial Factors:
- Psychological Stress: Alters gastric emptying and acid secretion
- Anxiety and Depression: 2-3 fold increased risk of symptoms
- Sleep Deprivation: Worsens both symptoms and esophageal acid exposure
- Traumatic Life Events: Associated with symptom onset or exacerbation
The multifactorial nature of acid reflux causation necessitates a comprehensive approach to management that addresses anatomical, physiological, genetic, and environmental factors. Individual patients typically have a unique combination of these causal factors, requiring personalized assessment and treatment strategies.
5. Risk Factors
Acid reflux risk factors encompass a wide range of demographic, lifestyle, medical, and genetic elements that increase an individual’s likelihood of developing the condition. Understanding these factors is essential for targeted prevention and management strategies.
Demographic Risk Factors
Age:
- Prevalence progression: Increases with age, peaking in the 60-70 year range
- Age-related changes:
- Decreased LES pressure (approximately 3-5 mmHg decline from ages 20 to 70)
- Reduced esophageal motility
- Increased prevalence of hiatal hernia (15% at age 30 vs. 60% at age 70)
- Special considerations: Different symptom presentation in elderly (less heartburn, more dysphagia and complications)
Gender:
- Overall prevalence: Generally similar between men and women
- Age-specific variations:
- Higher in males under 50 years (1.3:1 ratio)
- Equal or higher in females over 50 years, possibly related to post-menopausal changes
- Symptom differences: Women more likely to report extraesophageal symptoms
- Hormonal influences: Cyclic fluctuations related to menstrual cycle and significant impact during pregnancy
Race and Ethnicity:
- Prevalence patterns:
- Highest in Western populations (20-30%)
- Intermediate in South America and Middle East (15-20%)
- Lowest in East Asia, though rapidly increasing (5-17%)
- Genetic components: Differences in genetic predisposition between populations
- Cultural factors: Dietary habits, activity patterns, healthcare utilization
- Complication variations: Higher Barrett’s esophagus and esophageal adenocarcinoma rates in Caucasian populations
Geographic Factors:
- Western vs. Eastern patterns: Consistently higher rates in Western countries
- Urbanization impact: Rapidly increasing rates with urbanization (2-3 fold increase in urban vs. rural areas in developing countries)
- Latitude gradient: Some evidence for higher prevalence in northern latitudes
- Altitude effects: Mixed evidence, with some studies showing increased prevalence at higher altitudes
Lifestyle and Behavioral Risk Factors
Dietary Factors:
- High-risk dietary patterns:
- Western diet (high fat, processed foods)
- Fast food consumption (≥2 times/week increases risk by 30-50%)
- Large evening meals (especially within 3 hours of bedtime)
- Specific food triggers:
- Acidic foods (citrus, tomato products)
- Fatty foods (fried items, high-fat dairy)
- Spicy foods
- Chocolate (contains methylxanthines that reduce LES pressure)
- Mint (relaxes the LES)
- Beverages:
- Coffee (both caffeinated and decaffeinated)
- Carbonated drinks
- Alcohol (particularly white wine, beer, and liquor)
Body Weight and Composition:
- Obesity: One of the strongest risk factors
- BMI ≥30: 2-3 fold increased risk
- Central obesity particularly significant (waist circumference >94 cm in men, >80 cm in women)
- Weight fluctuations: Rapid weight gain increases risk
- Body fat distribution: Visceral fat more strongly associated than subcutaneous fat
- Mechanical effects: Increased intra-abdominal pressure
- Hormonal/inflammatory effects: Adipose tissue produces inflammatory cytokines affecting esophageal function
Physical Activity and Posture:
- Exercise patterns:
- Sedentary lifestyle increases risk (30-40% higher than active individuals)
- Certain high-intensity exercises may trigger symptoms
- Occupational posture:
- Prolonged sitting with forward lean
- Heavy lifting and straining
- Sleep position: Right-side and prone positions increase reflux episodes
Substance Use:
- Tobacco:
- Active smoking increases risk by 50-70%
- Dose-dependent relationship (>20 cigarettes/day: 2-fold risk increase)
- Mechanisms include reduced LES pressure, impaired esophageal clearance, reduced salivation
- Alcohol: Regular consumption (>7 drinks/week) increases risk by 25-40%
- Recreational drugs: Marijuana and cocaine associated with increased symptoms
Medical and Health-Related Risk Factors
Pre-existing Conditions:
- Gastrointestinal conditions:
- Hiatal hernia (strongest structural risk factor)
- Delayed gastric emptying
- Helicobacter pylori status (complex relationship)
- Previous gastric surgery
- Respiratory conditions:
- Asthma (bidirectional relationship with 40-60% overlap)
- COPD (2-3 fold increased risk)
- Obstructive sleep apnea (significantly increased nocturnal reflux)
- Neurological conditions:
- Cerebral palsy
- Parkinson’s disease
- Multiple sclerosis
- Connective tissue disorders:
- Scleroderma (80-90% have GERD)
- Ehlers-Danlos syndrome
- Marfan syndrome
Hormonal and Endocrine Factors:
- Diabetes mellitus: 25-40% increased risk, related to gastroparesis
- Pregnancy: 40-85% experience symptoms, particularly in third trimester
- Thyroid disorders: Both hypo- and hyperthyroidism can affect esophageal and gastric function
Medications:
- Direct irritants:
- NSAIDs
- Bisphosphonates
- Potassium supplements
- LES pressure reducers:
- Calcium channel blockers (30-50% increased risk)
- Nitrates
- Anticholinergics
- Benzodiazepines
- Others:
- Progesterone
- Opioids
- Theophylline
- Some antibiotics
Surgical History:
- Lung transplantation (65-75% develop GERD)
- Bariatric surgery (complex relationship – can improve or worsen)
- Anti-reflux surgery failure or recurrence
- Esophageal or gastric surgery
Environmental and Occupational Risk Factors
Occupational Factors:
- High-risk professions:
- Manual labor involving lifting and bending
- Professional singers and voice performers
- Long-haul truck drivers
- Healthcare workers (shift work)
- Workplace stress: High-stress environments increase risk by 30-40%
- Work schedule: Shift work, especially rotating shifts
- Environmental exposures: Dust, chemicals affecting respiratory function
Socioeconomic Factors:
- Education level: Mixed evidence, but some studies show inverse relationship
- Income: Lower income associated with higher prevalence in some populations
- Healthcare access: Affects diagnosis and management patterns
- Food environment: Food deserts limiting healthy dietary options
Air Quality and Climate:
- Air pollution (particulate matter) associated with increased symptoms
- Cold, dry air may exacerbate respiratory manifestations
- High altitude may affect pressure gradients and symptom expression
Psychosocial Factors:
- Psychological stress: Significant association with symptom severity
- Anxiety and depression: Bidirectional relationship with GERD
- Sleep quality: Poor sleep independently associated with increased symptoms
- Social support: Lower support associated with worse symptom perception
Understanding these diverse risk factors helps identify individuals at higher risk for developing GERD and informs targeted prevention and management strategies. Many of these factors are modifiable, offering opportunities for risk reduction through lifestyle changes, medication adjustments, and environmental modifications.
6. Complications
Chronic acid reflux can lead to a spectrum of complications ranging from quality of life impairment to life-threatening conditions. These complications primarily affect the esophagus but can extend to impact respiratory, oral, and systemic health.
Esophageal Complications
Erosive Esophagitis:
- Prevalence: Develops in 30-40% of untreated chronic GERD patients
- Pathophysiology: Acid-induced inflammation and erosion of esophageal mucosa
- Classification: Los Angeles Classification system grades severity from A (mild) to D (severe)
- Complications: Bleeding, ulceration, scarring
- Risk factors: Male gender, older age, hiatal hernia, obesity
- Long-term concerns: May progress to more severe complications if untreated
Esophageal Strictures:
- Prevalence: Occurs in 5-10% of long-standing GERD cases
- Mechanism: Chronic inflammation leads to fibrosis and narrowing of the esophageal lumen
- Presentation: Progressive dysphagia, initially for solids then advancing to liquids
- Location: Typically at the gastroesophageal junction or distal esophagus
- Treatment requirements: Often necessitates endoscopic dilation
- Recurrence rates: 30-40% within one year without adequate acid suppression
Barrett’s Esophagus:
- Definition: Metaplastic change from normal squamous epithelium to specialized intestinal columnar epithelium
- Prevalence: Develops in 5-15% of chronic GERD patients
- Risk profile: More common in Caucasian males, age >50, long-standing GERD (>5 years), obesity, smoking
- Significance: Precancerous condition with 0.1-0.5% annual risk of progression to adenocarcinoma
- Classification: Non-dysplastic, low-grade dysplasia, high-grade dysplasia
- Surveillance requirements: Regular endoscopic monitoring with biopsies
Esophageal Adenocarcinoma:
- Association: 5-10 fold increased risk in chronic GERD patients
- Annual incidence in Barrett’s esophagus: 0.1-0.5% per year
- Risk stratification: Highest in males with long-segment Barrett’s and dysplasia
- Incidence trends: One of the fastest-rising cancers in Western populations
- 5-year survival rate: 20% overall, 40-80% when detected early
- Prevention impact: Regular surveillance in high-risk individuals improves outcomes
Extraesophageal Complications
Respiratory Complications:
Chronic Cough:
- Prevalence in GERD: 25-40% of chronic cough cases
- Mechanism: Direct irritation or reflex-mediated bronchospasm
- Response to therapy: Variable, often requires prolonged treatment
Asthma:
- Bidirectional relationship: 50-80% of asthmatics have GERD; asthmatics have 1.5x increased risk of GERD
- Mechanism: Microaspiration, vagal reflex bronchospasm
- Impact: Harder-to-control asthma with more frequent exacerbations
- Response to GERD treatment: Improves symptoms in 30-50% of cases
Pulmonary Fibrosis:
- Association: 2-3 fold increased prevalence of GERD in idiopathic pulmonary fibrosis
- Hypothesis: Repeated microaspiration contributing to lung injury
- Impact: More rapid decline in lung function when GERD coexists
Aspiration Pneumonia:
- Risk: Particularly elevated in neurologically impaired patients
- Mortality impact: 30-40% increase in mortality when recurrent
- Prevention: Anti-reflux measures critical in high-risk patients
Ear, Nose, and Throat Complications:
Chronic Laryngitis:
- Prevalence: 10% of GERD patients develop laryngeal symptoms
- Findings: Posterior laryngeal inflammation, vocal cord edema
- Recovery: Often slow, requiring 3-6 months of intensive acid suppression
Dental Erosions:
- Mechanism: Acid exposure damaging tooth enamel
- Pattern: Typically affects the lingual and palatal surfaces of teeth
- Prevalence: 5-47% of GERD patients show dental erosions
- Irreversibility: Represents permanent loss of dental structure
Other ENT manifestations:
- Chronic sinusitis
- Recurrent otitis media
- Vocal cord granulomas or ulcers
- Globus pharyngeus (sensation of a lump in the throat)
- Halitosis
Systemic and Quality of Life Complications
Sleep Disturbances:
- Prevalence: 60-80% of GERD patients report sleep disruption
- Manifestations: Difficulty falling asleep, nighttime awakenings, poor sleep quality
- Mechanism: Nighttime reflux events, enhanced esophageal sensitivity during sleep
- Consequences: Daytime fatigue, reduced productivity, mood disturbances
- Bidirectional relationship: Sleep deprivation can worsen GERD symptoms
Psychological Impact:
- Anxiety and depression: 1.5-2 times more common in GERD patients
- Quality of life impairment: Comparable to other chronic diseases like diabetes and heart failure
- Social limitations: Dietary restrictions, avoidance of social activities
- Economic burden: Work absenteeism, reduced productivity, healthcare costs
Medication-Related Complications:
PPI-Related Concerns:
- Vitamin and mineral malabsorption (B12, magnesium, calcium, iron)
- Potential increased risk of bone fractures with long-term use
- Potential increased risk of C. difficile infection
- Potential kidney disease associations
- Interaction with other medications (e.g., clopidogrel)
Surgical Complications:
- Dysphagia (10-50% short-term, 5-10% long-term)
- Gas-bloat syndrome (inability to belch)
- Recurrent symptoms (10-30% at 5 years post-surgery)
- Surgical risks: bleeding, infection, perforation
Mortality and Disability Considerations
Direct Mortality Contributions:
- Esophageal adenocarcinoma: Approximately 16,000 deaths annually in the United States
- Aspiration pneumonia: Significant contributor in neurologically impaired patients
- Hemorrhagic complications: Rare but potentially fatal in severe erosive esophagitis
- Overall mortality impact: Modest increase in all-cause mortality (hazard ratio 1.2-1.4) in severe, untreated GERD
Disability Impact:
- Work productivity loss: 6-10 additional days of reduced productivity annually
- Activity limitation: 30-40% report limitations in daily activities
- Sleep-related impairment: Average 1.5 hours of sleep lost per night during flares
- Disability claims: GERD complications account for 1-2% of digestive disease-related disability claims
Long-term Progression and Natural History:
- Symptom evolution without treatment:
- 30-40% stable symptoms
- 30-50% progressive symptoms
- 10-20% developing complications
- 5-10% spontaneous improvement
- With standard treatment:
- 70-80% adequate symptom control
- 10-20% partial response
- 5-10% refractory symptoms
- 2-5% developing complications despite treatment
Risk Stratification for Complications:
- Highest risk profile:
- Caucasian males over 50
- Chronic symptoms >5 years
- Hiatal hernia >3 cm
- Obesity (BMI >30)
- Nocturnal symptoms
- Family history of Barrett’s or esophageal adenocarcinoma
- Moderate risk profile:
- Females with chronic symptoms
- Younger patients with severe symptoms
- Patients with partial response to therapy
- Lower risk profile:
- Young patients with intermittent symptoms
- Complete response to therapy
- No endoscopic evidence of damage
Understanding these complications is essential for appropriate risk stratification, monitoring, and therapeutic decision-making. While most patients with GERD will not develop serious complications, identifying those at higher risk allows for more aggressive management strategies to prevent long-term consequences.
7. Diagnosis & Testing
Accurate diagnosis of acid reflux requires systematic evaluation that may range from symptom assessment to specialized testing. The diagnostic approach typically follows a stepwise progression, balancing the need for accurate diagnosis against the invasiveness and cost of various tests.
Initial Clinical Evaluation
Symptom Assessment:
- Typical symptom pattern: Classic heartburn and regurgitation have a positive predictive value of 70-80% for GERD
- Symptom frequency and severity: Quantified using validated tools like the GERD-Q or Reflux Disease Questionnaire
- Symptom triggers: Relationship to meals, position, specific foods
- Alarm features requiring immediate investigation:
- Dysphagia or odynophagia
- Weight loss
- Anemia or evidence of bleeding
- Persistent vomiting
- Family history of upper GI malignancy
- Symptom onset after age 50
Physical Examination:
- Limited sensitivity for GERD diagnosis
- May reveal:
- Dental erosions
- Pharyngeal erythema
- Wheezing or respiratory findings in extraesophageal manifestations
- Abdominal obesity
- Signs of systemic conditions associated with GERD
Initial Diagnostic Approaches:
Empiric Therapy Trial:
- Often the first diagnostic step in patients with typical symptoms without alarm features
- PPI trial (4-8 weeks) with 70-80% sensitivity for GERD diagnosis
- Response supporting GERD diagnosis, non-response suggesting alternative diagnosis or refractory disease
- Limitations: May miss complications, less accurate for extraesophageal manifestations
Initial Laboratory Tests:
- Not diagnostic for GERD but may detect complications or alternative diagnoses
- Complete blood count to assess for anemia
- Basic metabolic panel to evaluate kidney function (relevant for medication choice)
- Liver function tests if hepatic symptoms present
- H. pylori testing in some cases
Endoscopic Evaluation
Upper Endoscopy (Esophagogastroduodenoscopy, EGD):
Indications:
- Presence of alarm symptoms
- Persistent symptoms despite empiric therapy
- High risk for Barrett’s esophagus
- Atypical symptoms requiring confirmation
- Consideration for anti-reflux surgery
Findings:
- Erosive esophagitis (classified by Los Angeles Classification: Grade A-D)
- Barrett’s esophagus
- Esophageal strictures or rings
- Hiatal hernia
- Alternative diagnoses (eosinophilic esophagitis, infectious esophagitis, malignancy)
Limitations:
- 50-70% of GERD patients have non-erosive reflux disease (NERD) with normal endoscopy
- Poor correlation between symptom severity and endoscopic findings
- Invasive procedure requiring sedation
Enhanced Endoscopic Techniques:
- Narrow Band Imaging (NBI): Enhances visualization of mucosal and vascular patterns
- Confocal Laser Endomicroscopy: Allows microscopic evaluation of esophageal mucosa
- Chromoendoscopy: Use of dyes to highlight mucosal abnormalities
- These techniques improve detection of Barrett’s esophagus and subtle mucosal changes
Biopsy Considerations:
Indications:
- Suspected Barrett’s esophagus
- Esophageal inflammation of unclear etiology
- Ruling out eosinophilic esophagitis
- Evaluation of esophageal strictures
Histopathological Findings in GERD:
- Basal cell hyperplasia
- Elongation of papillae
- Dilated intercellular spaces
- Inflammatory cell infiltration
- Absence of significant eosinophilia (which would suggest eosinophilic esophagitis)
Physiologic and Functional Testing
Ambulatory pH Monitoring:
Traditional Catheter-Based pH Monitoring:
- 24-hour measurement of esophageal acid exposure
- Parameters assessed: % time pH <4, number of reflux episodes, symptom correlation
- Normal values: Total acid exposure <4.2% of monitoring period
- Limitations: Catheter discomfort, altered behavior during testing
Wireless pH Monitoring (Bravo):
- Capsule attached to esophageal mucosa
- Extended monitoring (48-96 hours)
- Better tolerated than catheter-based systems
- Improved detection of day-to-day variability
- Limitations: Cost, rare complications (premature detachment, chest pain)
Combined Multichannel Intraluminal Impedance-pH Monitoring (MII-pH):
Functionality:
- Detects both acid and non-acid reflux events
- Distinguishes between liquid, gas, and mixed reflux
- Measures proximal extent of reflux
- Correlates symptoms with reflux events
Indications:
- Persistent symptoms despite PPI therapy
- Atypical symptoms with normal endoscopy
- Evaluation before anti-reflux surgery
- Suspected non-acid reflux
Key Metrics:
- Acid exposure time
- Number of reflux episodes (normal <80 per 24 hours)
- Symptom association probability (SAP)
- Symptom index (SI)
- Baseline impedance values
Esophageal Manometry:
- Purpose: Evaluates esophageal motor function and LES characteristics
- Findings in GERD:
- Hypotensive LES (<10 mmHg resting pressure)
- Ineffective esophageal motility
- Hiatal hernia detection
- Indications:
- Pre-surgical evaluation
- Dysphagia evaluation
- Distinguishing GERD from achalasia and other motility disorders
- Types:
- Conventional manometry
- High-resolution manometry with esophageal pressure topography
Barium Esophagogram/Upper GI Series:
- Utility:
- Evaluates structural abnormalities
- Assesses for hiatal hernia
- Identifies strictures and their length/diameter
- Can demonstrate reflux in real-time
- Limitations:
- Poor sensitivity for mild GERD
- Cannot detect mucosal changes
- Limited correlation with symptoms
- Best used for:
- Evaluating structural complications
- Assessing post-surgical anatomy
- Patients unable to tolerate endoscopy
Emerging and Specialized Diagnostic Methods
Hypopharyngeal Multichannel Intraluminal Impedance (HMII):
- Specialized probe positioned in the hypopharynx
- Detects proximal reflux events potentially causing extraesophageal symptoms
- Particularly useful in evaluating laryngopharyngeal reflux
Impedance Planimetry (EndoFLIP):
- Measures esophagogastric junction distensibility
- Provides functional assessment of the anti-reflux barrier
- Useful in evaluating efficacy of anti-reflux procedures
Pepsin Detection Tests:
- Salivary or respiratory fluid pepsin as biomarker for reflux
- Non-invasive option for detecting extraesophageal reflux
- Commercial kits available (Peptest)
- Limitations: standardization issues, timing dependency
Mucosal Impedance Testing:
- Direct measurement of esophageal mucosal integrity
- Can distinguish GERD from non-GERD causes of symptoms
- Emerging technology with promising diagnostic accuracy
Functional Lumen Imaging Probe (FLIP):
- Measures compliance and distensibility of the esophagus and LES
- Useful in evaluation of post-fundoplication dysphagia
- Emerging application in GERD diagnosis
Diagnostic Algorithms and Clinical Pathways
Algorithm for Typical Symptoms Without Alarm Features:
- Initial empiric PPI trial (4-8 weeks)
- If responsive, continue treatment and consider long-term management
- If non-responsive, proceed to endoscopy
- If endoscopy negative, consider pH or impedance-pH testing
- Treatment based on test results
Algorithm for Alarm Features or Age >50 with New Symptoms:
- Immediate endoscopy with appropriate biopsies
- Further testing based on endoscopic findings
- Treatment tailored to diagnosis and findings
Algorithm for Extraesophageal Symptoms:
- Evaluate and treat other more common causes first
- Consider empiric PPI trial (typically longer, 2-3 months)
- If non-responsive, consider MII-pH testing while on or off therapy
- Specialized testing (laryngoscopy, pulmonary function tests) as indicated
Pre-Surgical Evaluation Algorithm:
- Confirm GERD diagnosis with objective testing (endoscopy, pH study)
- Esophageal manometry to rule out motility disorders
- Consider additional tests (gastric emptying study, impedance planimetry)
- Multidisciplinary discussion for complex cases
The diagnostic approach to acid reflux requires balancing the risk-benefit ratio of various tests, considering the invasiveness, cost, and diagnostic yield in the context of each patient’s presentation. While empiric therapy remains a practical first-line approach for uncomplicated cases, objective testing is essential for atypical presentations, treatment failures, and pre-surgical evaluation.
8. Treatment Options
Management of acid reflux encompasses a spectrum of approaches, from lifestyle modifications to pharmaceutical interventions and surgical options. Treatment strategies should be individualized based on symptom severity, presence of complications, and patient preferences.
Lifestyle and Dietary Modifications
Dietary Adjustments:
Evidence-Based Recommendations:
- Weight loss for overweight/obese individuals (5-10% body weight reduction improves symptoms in 70-80% of patients)
- Meal timing (avoiding meals 2-3 hours before bedtime reduces nocturnal reflux by 40-50%)
- Small, frequent meals rather than large meals
- Moderate alcohol reduction (particularly spirits and wine)
Food Triggers with Strongest Evidence:
- High-fat foods (slow gastric emptying)
- Chocolate (reduces LES pressure via methylxanthines)
- Mint and peppermint (LES relaxation)
- Citrus and tomato products (direct irritation)
- Carbonated beverages (promote belching and reflux)
- Coffee (both caffeinated and decaffeinated)
Individualized Approach:
- Systematic elimination and reintroduction to identify personal triggers
- Food diary to correlate symptoms with specific foods
- Cultural and personal preferences considered in dietary planning
Positional and Behavioral Modifications:
Sleep Position:
- Left side sleeping (reduces reflux episodes by 15-20% compared to right side)
- Head-of-bed elevation (6-8 inches or 15-20 cm) reduces nocturnal reflux by 25-30%
- Specialized wedge pillows if bed elevation not feasible
Activity Considerations:
- Avoiding high-impact exercise immediately after meals
- Waiting 2 hours after eating before exercise
- Modified positions for yoga and strength training to reduce abdominal pressure
- Post-meal walking (10-15 minutes) to enhance gastric emptying
Other Behavioral Measures:
- Smoking cessation (improves LES function and reduces reflux events)
- Loose-fitting clothing around abdomen
- Stress reduction techniques (mindfulness, progressive muscle relaxation)
- Proper posture, especially while seated
Effectiveness of Lifestyle Measures:
- As sole therapy: Adequate for mild, intermittent symptoms in 20-30% of patients
- As adjunctive therapy: Enhances effectiveness of medical treatments by 15-25%
- Comparative effectiveness: Generally less effective than medications, but without side effects
- Long-term adherence: Key challenge, with declining compliance over time
Pharmaceutical Interventions
Antacids:
- Mechanism: Neutralize gastric acid
- Examples: Calcium carbonate, aluminum hydroxide, magnesium hydroxide
- Effectiveness: Rapid but short-term relief (1-2 hours)
- Best use: Mild, intermittent symptoms; breakthrough symptoms
- Limitations: Short duration, not effective for healing
- Side effects: Constipation (calcium/aluminum), diarrhea (magnesium)
H2-Receptor Antagonists (H2RAs):
- Mechanism: Block histamine receptors on gastric parietal cells
- Examples: Famotidine, cimetidine, ranitidine (now withdrawn), nizatidine
- Effectiveness: Reduces acid production by 60-70%
- Onset and duration: Effect within 30 minutes, lasts 6-12 hours
- Best use: Mild-moderate symptoms, maintenance after PPI therapy
- Limitations: Tolerance can develop within 2-4 weeks
- Side effects: Generally well-tolerated; rare headache, dizziness, confusion (elderly)
Proton Pump Inhibitors (PPIs):
- Mechanism: Irreversibly inhibit the H+/K+ ATPase pump in parietal cells
- Examples: Omeprazole, esomeprazole, pantoprazole, lansoprazole, dexlansoprazole, rabeprazole
- Effectiveness: Reduces acid production by 90-95%
- Onset: Full effect after 3-5 days of regular use
- Indications:
- Moderate to severe GERD
- Erosive esophagitis
- Barrett’s esophagus
- PPI-responsive extraesophageal syndromes
- Dosing considerations:
- Standard dose vs. double dose
- Once daily (typically 30-60 minutes before breakfast) vs. twice daily
- On-demand vs. continuous therapy
- Healing phase (8-12 weeks) followed by maintenance
- Long-term considerations:
- Safety concerns with prolonged use (bone fractures, C. difficile, pneumonia, vitamin/mineral deficiencies)
- Lowest effective dose for shortest necessary duration
- Periodic reassessment of continued need
- Deprescribing strategies for long-term users
Prokinetic Agents:
- Mechanism: Enhance gastric emptying and esophageal clearance
- Examples: Metoclopramide, domperidone (not FDA-approved in US), erythromycin
- Effectiveness: Modest benefit, primarily as adjunctive therapy
- Best use: Patients with documented delayed gastric emptying
- Limitations: Limited evidence as monotherapy for GERD
- Side effects: Extrapyramidal symptoms, tardive dyskinesia (metoclopramide), cardiac effects (domperidone)
Alginate-Based Formulations:
- Mechanism: Form raft that floats on gastric contents, physically blocking reflux
- Examples: Gaviscon, Gaviscon Advance
- Effectiveness: Superior to antacids, less effective than acid suppressants
- Best use: Mild symptoms, pregnancy, upright reflux
- Limitations: Multiple daily doses required
- Side effects: Minimal; occasional constipation
Baclofen:
- Mechanism: GABA-B agonist that reduces transient LES relaxations
- Effectiveness: Reduces reflux episodes by 40-60%
- Best use: Refractory regurgitation, volume reflux
- Limitations: Not FDA-approved for GERD
- Side effects: Drowsiness, dizziness, fatigue
Combination Therapy Approaches:
- PPI + H2RA: H2RA at bedtime for nocturnal acid breakthrough
- PPI + Prokinetic: For patients with delayed gastric emptying
- PPI + Baclofen: For predominant regurgitation symptoms
- Effectiveness: 10-30% additional benefit versus PPI alone in selected patients
Endoscopic and Surgical Interventions
Surgical Approaches:
Laparoscopic Nissen Fundoplication:
- Procedure: 360° wrap of fundus around lower esophagus
- Effectiveness: 85-90% symptom improvement at 5 years
- Best candidates: Documented reflux, good response to PPI, normal motility
- Limitations: Side effects including dysphagia, gas-bloat syndrome
- Durability: 10-year success rates of 60-70%
Laparoscopic Partial Fundoplication:
- Types: Toupet (270° posterior), Dor (180-200° anterior)
- Advantages: Lower rates of dysphagia and gas-bloat
- Effectiveness: Slightly less effective for reflux control (80-85%)
- Best use: Patients with impaired esophageal motility
LINX Procedure:
- Mechanism: Magnetic beads placed around LES to augment pressure
- Effectiveness: 85% improvement in symptoms, 85% reduction in PPI use
- Advantages: Reversible, preserves gastric anatomy, shorter operative time
- Limitations: Contraindicated with MRI need, metal allergies
- Long-term data: Promising 5-year outcomes, limited 10-year data
Roux-en-Y Gastric Bypass:
- Dual benefit: Weight loss and anti-reflux mechanism
- Effectiveness for GERD: 80-90% symptom resolution
- Best candidates: Obese patients with GERD
- Limitations: More extensive surgery with higher initial risks
Endoscopic Therapies:
Transoral Incisionless Fundoplication (TIF):
- Procedure: Endoscopic partial fundoplication using EsophyX device
- Effectiveness: 70-80% improvement in symptoms
- Advantages: Outpatient procedure, faster recovery than surgery
- Limitations: Less effective for large hiatal hernias, limited long-term data
- Duration of effect: 3-year data shows maintained improvement in 60-70%
Medigus Ultrasonic Surgical Endostapler (MUSE):
- Procedure: Endoscopic stapling device creating anterior fundoplication
- Effectiveness: 65-75% reduction in symptoms and medication use
- Limitations: Limited availability, evolving long-term data
Stretta Procedure:
- Mechanism: Radiofrequency energy delivery to LES region
- Effectiveness: 60-70% improvement in symptoms
- Proposed benefits: Reduced TLESRs, enhanced barrier function
- Best candidates: Mild-moderate GERD without large hiatal hernia
- Limitations: Controversial long-term efficacy
Treatment Selection and Personalized Approaches
Initial Treatment Strategy by Severity:
Mild, Intermittent Symptoms:
- First line: Lifestyle modifications, on-demand antacids or H2RAs
- Second line: Low-dose PPI as needed
- Monitoring: Self-directed with follow-up as needed
Moderate Symptoms:
- First line: Daily PPI (standard dose) for 4-8 weeks plus lifestyle modifications
- Second line: Optimization of PPI timing, twice-daily dosing
- Maintenance: Step-down to lowest effective dose or intermittent therapy
- Monitoring: Clinical reassessment at 4-8 weeks
Severe Symptoms/Erosive Disease:
- First line: Daily PPI (standard or double dose) for 8-12 weeks
- Second line: Twice-daily PPI, consideration of adjunctive therapies
- Maintenance: Continued daily therapy with periodic attempts at dose reduction
- Monitoring: Endoscopic confirmation of healing for erosive disease
Special Population Considerations:
Pregnancy:
- First line: Lifestyle modifications, antacids
- Second line: Sucralfate, H2RAs (preferably famotidine)
- Third line: PPIs if benefits outweigh risks (best safety data for omeprazole)
- Avoidance of: Sodium bicarbonate, magnesium trisilicate
Elderly Patients:
- Consideration of drug interactions and comorbidities
- Monitoring for age-related side effects (confusion with H2RAs, fracture risk with PPIs)
- Deprescribing protocols to minimize long-term PPI exposure
- Higher threshold for invasive intervention due to operative risk
Extraesophageal Manifestations:
- Longer treatment trials (2-3 months minimum)
- Often requires higher PPI doses
- Consideration of twice-daily dosing
- Multidisciplinary approach with pulmonology or ENT
- pH/impedance testing to confirm GERD if initial response inadequate
Refractory GERD:
- Systematic evaluation of causes (compliance, timing, diagnosis)
- Objective testing (impedance-pH, endoscopy)
- Consideration of functional esophageal disorders
- Potential treatment options:
- Twice-daily PPI with optimized timing
- Addition of H2RA at bedtime
- Addition of baclofen for refractory regurgitation
- Consideration of surgery in confirmed reflux cases
The treatment landscape for acid reflux continues to evolve, with emphasis on tailored approaches based on individual patient characteristics, symptom patterns, and underlying pathophysiology. While acid suppression remains the cornerstone of medical therapy, recognition of the multifactorial nature of GERD has expanded treatment options to address specific patient needs and mechanisms of disease.
9. Prevention & Precautionary Measures
Preventing acid reflux and its complications involves a multifaceted approach targeting modifiable risk factors and implementing proactive strategies to minimize symptom occurrence and disease progression. This section explores comprehensive preventive approaches that can be tailored to individual risk profiles.
Primary Prevention Strategies
Weight Management:
- Target intervention: Maintaining healthy BMI (18.5-24.9 kg/m²)
- Evidence strength: Strong – each unit increase in BMI increases odds of GERD by approximately 10-15%
- Implementation approaches:
- Medical nutritional therapy with registered dietitian
- Caloric deficit of 500-750 kcal/day for gradual weight loss
- Combined dietary and physical activity interventions
- Regular monitoring and adjustment of strategies
- Effectiveness metrics: 5-10% weight loss improves symptoms in 70-80% of overweight GERD patients
Dietary Modifications:
Meal pattern optimization:
- Smaller, more frequent meals (5-6 smaller meals vs. 3 large meals)
- Avoiding late meals (>3 hours before bedtime)
- Slower eating pace to reduce air swallowing
- Regular meal timing to establish digestive rhythm
Food selection guidance:
- Reduced fat intake (especially saturated fats)
- Limited consumption of documented trigger foods
- Adequate fiber intake (25-30g daily)
- Anti-inflammatory food choices (fruits, vegetables, lean proteins, whole grains)
- Alkaline-forming foods as snacks between meals
Beverage considerations:
- Reduced carbonated beverage consumption
- Coffee limitation (both regular and decaffeinated)
- Alcohol moderation, particularly avoiding bedtime consumption
- Adequate water intake between rather than during meals
Positional and Behavioral Modifications:
Sleep positioning:
- Left side sleeping position
- Head-of-bed elevation (6-8 inches/15-20 cm)
- Special wedge pillows when bed elevation not possible
- Avoiding supine position after meals
Physical activity guidelines:
- Regular moderate exercise (150 minutes weekly)
- Low to moderate intensity activities preferential to high-intensity
- Exercise timing (2-3 hours after meals)
- Core-strengthening exercises to support diaphragmatic function
Stress management techniques:
- Mindfulness-based stress reduction
- Progressive muscle relaxation
- Guided imagery
- Regular sleep hygiene practices
- Cognitive behavioral approaches for anxiety related to symptoms
Avoiding Aggravating Factors:
Smoking cessation:
- Complete abstinence as goal
- Nicotine replacement therapy as bridge
- Reduced passive smoke exposure
- Includes avoidance of vaping and e-cigarettes
Medication review:
- Identification of medications that may trigger reflux
- Alternative options for essential medications
- Timing adjustments for unavoidable medications
- Taking medications in upright position with plenty of water
Clothing considerations:
- Avoiding tight belts and waistbands
- Loose-fitting clothing around midsection
- Elevated waistlines rather than constricting waistbands
Secondary Prevention: Managing Established GERD
Preventing Symptom Recurrence:
Maintenance therapy strategies:
- Continuous vs. on-demand medication approaches
- Step-down protocols (from PPI to H2RA)
- Lowest effective dose determination
- Regular reassessment of continued need
Combination approaches:
- Medication plus consistent lifestyle modifications
- Breakthrough symptom management plans
- Trigger avoidance with medication optimization
- Pre-emptive medication before anticipated triggers
Monitoring protocols:
- Symptom diaries or digital tracking
- Regular check-ins with healthcare providers
- Self-assessment of symptom patterns
- Quality of life impact evaluation
Preventing Complications:
Barrett’s esophagus surveillance:
- Risk-stratified endoscopic monitoring
- Frequency based on presence and grade of dysplasia
- Seattle protocol for systematic biopsy sampling
- Consideration of advanced imaging techniques
Esophagitis healing confirmation:
- Follow-up endoscopy for severe erosive disease
- Adequate duration of treatment before assessment
- Complete mucosal healing as endpoint
- Maintenance strategy to prevent recurrence
Stricture prevention:
- Aggressive acid suppression after dilation procedures
- Proactive treatment of recurrent dysphagia
- Anti-inflammatory approaches
- Adequate duration of therapy
Special Population Considerations
Pediatric Population:
Infant reflux management:
- Feeding modifications (smaller, more frequent feeds)
- Thickened feeds in selected cases
- Appropriate positioning after feeds
- Distinguishing physiologic reflux from GERD
Adolescent approach:
- Education about dietary triggers
- Weight management guidance
- Sleep position counseling
- Avoidance of smoking/vaping initiation
Pregnancy-Related Prevention:
First-line approaches:
- Small, frequent meals
- Avoiding late meals
- Head elevation during sleep
- Left-side sleeping position
Medication considerations:
- Antacids as first option (avoiding sodium bicarbonate)
- Sucralfate as non-absorbed option
- H2RAs (particularly famotidine) if needed
- PPIs reserved for severe, refractory cases
Elderly Population:
Polypharmacy considerations:
- Regular medication review
- Timing separation for interacting medications
- Alternatives to reflux-promoting medications when possible
Aspiration prevention:
- Upright position during and after meals
- Swallowing evaluation when indicated
- Thickened liquids if aspiration risk present
- Careful medication administration
Monitoring considerations:
- Atypical presentation awareness
- Vigilance for complications
- Nutrition status assessment
- Balance of symptom control and medication risks
Occupational Considerations:
- High-risk occupations:
Professional singers/voice performers:
- Pre-performance dietary restrictions
- Elevated upper body during sleep before performances
- Voice rest protocols with reflux flares
Shift workers:
- Consistent meal timing despite shifting schedule
- Avoiding eating within 3 hours of sleep period
- Sleep environment modification (elevated head)
- Light, non-triggering meals during night shifts
Physical laborers:
- Timing of more substantial meals during rest periods
- Core-strengthening to reduce abdominal strain
- Proper lifting techniques to minimize intra-abdominal pressure
- Hydration without carbonated beverages
Prevention Through Screening and Early Detection
Targeted Screening Approaches:
High-risk population identification:
- Chronic, longstanding GERD (>5 years)
- Multiple risk factors for Barrett’s esophagus
- Age >50, male gender, Caucasian race, central obesity
- Family history of esophageal adenocarcinoma or Barrett’s
Screening methodologies:
- Conventional endoscopy with targeted biopsies
- Emerging technologies:
- Cytosponge with TFF3 biomarker
- Transnasal endoscopy
- Non-endoscopic cell collection devices
Risk stratification tools:
- Michigan Barrett’s Esophagus Prediction Tool
- Prognostic models incorporating clinical and demographic factors
- Genetic testing for susceptibility variants
Early Intervention Strategies:
Barrett’s esophagus management:
- Intensive acid suppression (typically PPI)
- Consideration of aspirin or NSAIDs in selected cases
- Endoscopic eradication therapy for dysplasia
- Lifestyle modifications particularly important
Novel preventive approaches:
- Chemoprevention studies with aspirin, metformin
- Anti-inflammatory dietary patterns
- Microbiome modulation strategies
- Weight management programs specific to BE patients
The comprehensive approach to GERD prevention encompasses primary strategies to reduce risk and onset, secondary approaches to manage established disease and prevent recurrence, and targeted interventions for high-risk individuals to prevent serious complications. Given the multifactorial nature of GERD, combining multiple preventive strategies typically yields better results than single interventions, with an individualized approach based on specific risk factors and patient characteristics.
10. Global & Regional Statistics
Acid reflux prevalence, impact, and management vary significantly across different regions worldwide, influenced by genetic factors, lifestyle patterns, dietary habits, healthcare access, and diagnostic approaches.
Global Incidence and Prevalence
Overall Global Burden:
- Worldwide prevalence: 8-33% of the global population experiences GERD symptoms at least weekly
- Total affected individuals: Approximately 1.03 billion people globally
- Trend analysis: 50% increase in prevalence over the past 20 years
- Gender distribution: Generally equal between men and women globally, with slight regional variations
- Age patterns: Increasing prevalence with age in most regions, with peak onset between 45-64 years
GERD Definition Considerations:
- Symptom-based prevalence: Higher when defined by presence of symptoms
- Endoscopic findings: Lower when defined by presence of esophagitis (30-40% of symptomatic patients)
- Combined criteria: Varies based on diagnostic approach and available healthcare resources
- Mild vs. severe disease: Approximately 37% of GERD patients have severe disease requiring daily medication
Prevalence by Major Regions:
North America:
- United States: 18-28% prevalence (60-90 million affected)
- Canada: 17-24% prevalence
- Mexico: 12-19% prevalence
- Regional trend: Stabilizing after decades of increase
Europe:
- Western Europe: 15-24% prevalence
- Northern Europe: 16-26% prevalence
- Southern Europe: 10-18% prevalence
- Eastern Europe: 12-15% prevalence
- Regional variation: Higher rates in Northwestern countries
Asia:
- East Asia (traditional): 5-8% prevalence
- East Asia (urbanized areas): 12-15% prevalence
- South Asia: 8-14% prevalence
- Middle East: 12-20% prevalence
- Regional trend: Rapidly increasing, particularly in urbanized areas
South America:
- Overall: 12-18% prevalence
- Southern cone: 16-23% prevalence
- Northern regions: 10-15% prevalence
- Regional pattern: Higher rates in more developed economies
Africa:
- North Africa: 14-20% prevalence
- Sub-Saharan Africa: 9-14% prevalence
- Regional challenges: Limited epidemiological data, likely underestimated
Australia/Oceania:
- Australia: 15-21% prevalence
- New Zealand: 17-22% prevalence
- Pacific Islands: Varied data, estimated 8-15% prevalence
Economic Impact by Region:
Healthcare Costs:
- North America: $15-20 billion annually
- European Union: €8-12 billion annually
- Asia-Pacific: $5-8 billion annually, rapidly increasing
- Global total: Estimated $50-65 billion in direct medical costs
Indirect Economic Burden:
- Productivity loss: $75-100 billion globally
- Absenteeism patterns: Average 2-5 workdays lost annually per patient
- Presenteeism impact: 10-30% reduced productivity while working with symptoms
Regional Variations in Disease Patterns
North American Patterns:
- Distinguishing features:
- Highest rates of obesity-associated GERD
- High PPI utilization (approximately 14-16% of adults)
- Highest rates of Barrett’s esophagus (5-6% of GERD patients)
- Growing pediatric GERD population
- Healthcare utilization:
- 4-5 million ambulatory visits annually for GERD
- Second most common chronic condition in outpatient setting
- High rates of over-the-counter treatment (35-40% self-medicating)
- Trends:
- Plateauing prevalence after decades of increase
- Rising concerns about PPI overuse
- Increasing utilization of surgical/endoscopic interventions
European Patterns:
- Regional variations:
- North-South gradient (higher in north)
- United Kingdom, Ireland, and Scandinavian countries with highest rates
- Mediterranean countries with lower rates despite increasing trends
- Treatment approaches:
- More conservative PPI prescribing than North America
- Greater emphasis on step-down therapy
- Earlier consideration of surgical options in some countries
- Healthcare system impacts:
- Significant national variation in management guidelines
- 2-8% of primary care consultations GERD-related
- Strong public health approaches in Northern Europe
Asian Patterns:
- Traditional vs. Changing Patterns:
- Historically low rates now rapidly increasing
- Urban-rural divide (urban areas 2-3x higher prevalence)
- Rising with adoption of Western dietary patterns
- Earlier age of onset in recent cohorts
- Phenotypic differences:
- Higher rates of non-erosive reflux disease (70-80% vs. 50-60% in West)
- Lower rates of Barrett’s esophagus (0.5-1.5% of GERD patients)
- More frequent dyspeptic symptoms accompanying reflux
- Common overlap with functional disorders
- Region-specific factors:
- H. pylori prevalence affecting GERD rates (inverse relationship)
- Tea consumption as both risk and protective factor (varies by type)
- Genetic differences in drug metabolism affecting treatment effectiveness
Middle Eastern Patterns:
- Prevalence characteristics:
- High rates comparable to Western countries (15-20%)
- Significant impact of dietary patterns during religious observances
- Higher rates of nocturnal symptoms reported
- Unique considerations:
- Impact of fasting and feast cycles (Ramadan effects)
- Higher rates of water pipe smoking affecting GERD
- Dietary pattern rich in potential triggers
- Distinctive tea consumption patterns
Latin American Patterns:
- Regional features:
- Significant country-to-country variation
- Higher rates in countries with greater “Western” dietary adoption
- Substantial indigenous population differences in prevalence
- Special considerations:
- High rates of H. pylori affecting GERD patterns
- Distinctive dietary triggers (spicy foods, specific fruits)
- Variable access to diagnostic and treatment resources
- Growing economic impact with industrialization
African Patterns:
- Data limitations:
- Sparse epidemiological studies
- Focus on urban populations with limited rural data
- Emerging recognition as healthcare priority
- Observed patterns:
- Lower reported rates than Western countries
- Higher prevalence in North Africa than Sub-Saharan regions
- Urbanization associated with increasing prevalence
- Potentially distinctive genetic and environmental factors
Complications and Mortality Statistics
Barrett’s Esophagus Prevalence:
- Global variation:
- North America: 5-6% of GERD patients
- Western Europe: 3-5% of GERD patients
- Eastern Europe: 2-3% of GERD patients
- East Asia: 0.5-1.5% of GERD patients
- Middle East: 1-2% of GERD patients
- Annual conversion to esophageal adenocarcinoma: 0.1-0.5% per year
- Risk modification: Lower progression rates with PPI use (30-40% reduction)
Esophageal Adenocarcinoma Incidence:
- Global annual cases: Approximately 52,000
- Regional variations:
- Highest: UK, Netherlands, Ireland, US (5-7 per 100,000)
- Intermediate: Australia, Germany, Canada (3-5 per 100,000)
- Low: Southern Europe, South America (1-3 per 100,000)
- Very low: East Asia, Africa (0.3-1 per 100,000)
- Temporal trends:
- 600% increase in Western countries over past 40 years
- Beginning to plateau in some regions
- Continuing increase in newly industrialized countries
- Survival statistics:
- Overall 5-year survival: 20%
- Stage I 5-year survival: 40-50%
- Stage IV 5-year survival: <5%
Other Complications by Region:
- Erosive Esophagitis:
- North America/Europe: 30-40% of GERD patients
- Asia: 15-30% of GERD patients
- More severe grades less common in Asian populations
- Strictures:
- Declining globally due to effective acid suppression
- Current prevalence: 1-2% of chronic GERD patients
- Regional variation primarily related to healthcare access
- Respiratory complications:
- Higher reporting in regions with advanced healthcare systems
- Likely global underdiagnosis of GERD-related asthma/cough
Treatment Patterns and Accessibility
Medication Utilization:
- PPI consumption per capita:
- Highest: United States, Iceland, Australia (>75 defined daily doses per 1000 inhabitants per day)
- High: Western Europe (40-75 defined daily doses per 1000 inhabitants per day)
- Moderate: Eastern Europe, East Asia, Latin America (20-40 defined daily doses per 1000 inhabitants per day)
- Low: Africa, South Asia (<20 defined daily doses per 1000 inhabitants per day)
- Over-the-counter availability:
- PPIs available without prescription in approximately 45% of countries
- H2RAs available over-the-counter in approximately 75% of countries
- Significant impact on utilization patterns and healthcare-seeking behavior
Surgical Intervention Rates:
- Anti-reflux procedures per 100,000 population:
- United States: 12-15 procedures
- Western Europe: 8-25 procedures (highest in Scandinavia)
- Australia/New Zealand: 10-14 procedures
- Latin America: 3-8 procedures
- Asia: 1-5 procedures
- Africa: <1 procedure
- Procedural trends:
- Declining traditional fundoplication in North America
- Increasing magnetic sphincter augmentation procedures
- Growing endoscopic therapies in high-resource settings
Healthcare Access Disparities:
- Endoscopy availability (per 100,000 population):
- High-income countries: 10-20 endoscopy units
- Middle-income countries: 2-10 endoscopy units
- Low-income countries: <2 endoscopy units
- Specialist availability (gastroenterologists per 100,000):
- North America: 3.5-4.0
- Western Europe: 2.5-3.8
- Eastern Europe: 1.5-2.5
- Latin America: 1.2-2.2
- Asia (variable): 0.5-3.0
- Africa: 0.1-0.5
- Medication affordability:
- PPI cost as percentage of daily wage (generic omeprazole):
- High-income: <5% of daily minimum wage
- Middle-income: 10-20% of daily minimum wage
- Low-income: Often >100% of daily minimum wage
- PPI cost as percentage of daily wage (generic omeprazole):
The global landscape of acid reflux shows remarkable variation in prevalence, presentation, complications, and management approaches. These differences reflect complex interactions between genetic predisposition, environmental exposures, healthcare system factors, and socioeconomic considerations. Understanding these regional patterns is essential for developing context-appropriate clinical guidelines, allocating healthcare resources, and designing public health interventions to address this common and impactful condition.
11. Recent Research & Future Prospects
The field of acid reflux research continues to evolve rapidly, with innovations spanning from basic science to clinical applications. This section explores cutting-edge developments and promising future directions that may transform GERD management.
Latest Advancements in Understanding and Treatment
Pathophysiological Insights:
Microbiome Research:
- Esophageal Microbiome: Distinct patterns in GERD vs. healthy individuals
- Key findings: Reduced bacterial diversity and shift toward Gram-negative species in GERD
- Potential implications: Microbiome modulation as therapeutic target
- Current status: Multiple observational studies published; interventional trials beginning
- Example research: UCLA study demonstrating microbiome restoration with diet modification (2023)
Mucosal Integrity and Recovery:
- Discovery: Identification of specific proteins regulating tight junction integrity
- Clinical relevance: Explains variable symptom perception with similar acid exposure
- Therapeutic potential: Drugs targeting mucosal healing beyond acid suppression
- Biomarkers: Mucosal impedance as measure of epithelial integrity
- Recent development: Identification of key inflammatory pathways that delay healing (Fass et al., 2022)
Neuroinflammatory Mechanisms:
- Neuroimmune interactions: Cross-talk between immune cells and sensory nerves
- Visceral hypersensitivity: Central and peripheral sensitization mechanisms
- Biomarkers: Nerve growth factor, substance P, and specific cytokines
- Implications: Explains symptoms in non-erosive reflux disease
- Recent finding: Identification of microglial activation in chronic GERD models (Chen et al., 2023)
Diagnostic Innovations:
Non-Invasive Biomarkers:
- Salivary pepsin: High sensitivity for extraesophageal reflux
- Exhaled breath testing: Volatile organic compounds as GERD signature
- Genetic risk profiling: Multi-SNP panels for Barrett’s progression risk
- Clinical implementation: Point-of-care devices entering market
- Validation status: Large multi-center studies recently completed
Advanced Imaging Techniques:
- Confocal Laser Endomicroscopy: Real-time cellular visualization
- Volumetric Laser Endomicroscopy: Depth-resolved imaging of Barrett’s esophagus
- Advanced chromoendoscopy: Enhanced lesion detection in Barrett’s
- Artificial intelligence integration: Computer-aided detection of subtle changes
- Recent breakthrough: AI systems achieving >90% accuracy in dysplasia detection
Ambulatory Monitoring Refinements:
- Extended wireless pH monitoring: Up to 96 hours of data
- Miniaturized impedance-pH systems: Improved patient tolerance
- Oropharyngeal pH monitoring: Specialized detection of proximal reflux
- Smart algorithms: Automated analysis and interpretation
- Recent innovation: Smartphone-connected systems with patient symptom correlation
Therapeutic Developments:
Pharmacological Advances:
Potassium-Competitive Acid Blockers (P-CABs):
- Mechanism: Reversible potassium-competitive acid blockade
- Advantages: Rapid onset, meal-independent efficacy
- Examples: Vonoprazan, revaprazan, tegoprazan
- Current status: Approved in Asia, in late-phase trials in US/Europe
- Recent data: Superior healing of erosive esophagitis vs. PPIs
TLESR-Targeting Medications:
- Mechanism: Reducing transient lower esophageal sphincter relaxations
- Candidates: Improved GABA-B agonists, mGluR5 antagonists
- Advantage: Addressing mechanism beyond acid suppression
- Development status: Phase 2-3 trials
- Recent finding: Significantly reduced regurgitation symptoms
Esophageal Mucosal Protectants:
- Examples: Improved alginates, hyaluronic acid/chondroitin sulfate
- Mechanism: Physical protection and enhanced mucosal healing
- Target population: NERD patients, PPI partial responders
- Recent evidence: Effective as add-on therapy to acid suppression
Endoscopic Therapy Innovation:
Antireflux Mucosectomy (ARMS):
- Procedure: Endoscopic resection of gastroesophageal junction tissue
- Mechanism: Creates scar tissue barrier at cardia
- Evidence: 70-85% response rates in recent trials
- Advantage: Potentially accessible technique without special devices
- Current status: Spreading adoption with technique refinement
Endoscopic Plication Systems:
- Latest generation devices with improved durability
- Example: GERDx™ system with transmural plication
- Efficacy: 70-85% symptom improvement at 1 year
- Target: Patients with small/no hiatal hernia
- Recent data: 3-year results showing sustained benefits
Radiofrequency Energy Delivery:
- Refined Stretta procedure protocols
- Mechanism: Neurolysis and collagen remodeling
- Recent meta-analyses: Moderate efficacy for carefully selected patients
- Ongoing debate: Continued controversy over long-term effectiveness
- Recent development: Identification of optimal patient characteristics
Surgical Approach Refinements:
Magnetic Sphincter Augmentation (LINX) Evolution:
- Expanded indications to larger hiatal hernias
- Technical modifications for improved outcomes
- Long-term data: 85% effectiveness at 5+ years
- Recent innovation: MRI-compatible versions in development
- Cost-effectiveness: Recent studies showing comparable or superior to PPIs long-term
Electrical Stimulation Therapy:
- EndoStim system: Delivers electrical stimulation to LES
- Mechanism: Increases LES pressure while allowing normal relaxation
- Current status: Promising initial results, company restructuring delayed trials
- Recent development: New generation device with improved battery life
- Future direction: Personalized stimulation patterns based on impedance feedback
Robotic-Assisted Approaches:
- Enhanced precision for hiatal hernia repair
- Novel fundoplication techniques with reduced side effects
- Improved visualization and ergonomics
- Recent data: Potentially lower conversion rates and complications
- Cost-benefit: Ongoing evaluation of value proposition
Ongoing Studies and Research Directions
Major Clinical Trials:
Pharmacological Studies:
- PHALCON-NERD: Vonoprazan for non-erosive reflux disease
- RELIEF: Tegoprazan vs. esomeprazole for extraesophageal reflux symptoms
- HARMONY: Combination therapy with vonoprazan and prokinetics
- DELIVER: Dexlansoprazole in laryngopharyngeal reflux
- RESTORE: P-CABs for PPI-refractory GERD
Endoscopic and Surgical Trials:
- CALIBER: Comparative effectiveness of LINX vs. fundoplication
- RELIEF-TIF: Transoral incisionless fundoplication for extraesophageal reflux
- ARMOR: Antireflux mucosectomy randomized trial
- BIOME-GERD: Microbiome restoration post-antireflux surgery
- NERO: Neuromodulation for refractory symptoms
Diagnostic and Monitoring Studies:
- PREDICT-GERD: Multi-biomarker diagnostic algorithm validation
- INHIB-pH: Extended pH monitoring protocols
- DIGI-GERD: Digital health platform for GERD management
- PRECISE: Patient-reported outcomes correlation with objective measures
- AI-DETECT: Artificial intelligence for Barrett’s surveillance
Emerging Research Focus Areas:
Precision Medicine Applications:
- Genetic determinants of treatment response
- Metabolomic profiles predicting complications
- Personalized therapy algorithms based on pathophysiological phenotype
- Pharmacogenomic factors affecting medication metabolism
- Machine learning models integrating multiple data streams for personalized recommendations
Neurobiological Research:
- Central processing of esophageal stimuli via functional MRI
- Peripheral sensitization mechanisms and targeted therapies
- Brain-gut axis influence on symptom perception
- Autonomic nervous system dysregulation in GERD
- Neuromodulation approaches for symptom management
Regenerative Medicine:
- Stem cell therapies for esophageal epithelial repair
- Growth factor delivery to enhance mucosal healing
- Tissue engineering approaches for sphincter augmentation
- Extracellular matrix scaffolds for esophageal repair
- Gene therapy to restore barrier function proteins
Digital Health Integration:
- Remote patient monitoring platforms for GERD
- Smartphone-connected pH sensors for home monitoring
- AI-powered decision support for treatment selection
- Telehealth optimization for GERD management
- Digital therapeutic applications for behavioral modification
Future Prospects and Potential Breakthroughs
Short-Term Developments (1-3 Years):
P-CAB Availability:
- Global expansion of potassium-competitive acid blockers
- Expected advantages: Faster onset, meal-independence, potentially superior healing
- Impact: Paradigm shift in acid suppression therapy
- Challenges: Cost considerations, formulary adoption
- Prediction: Will capture 25-30% of PPI market within 3 years of approval
Enhanced Diagnostic Protocols:
- Implementation of combined impedance-pH testing as standard
- Widespread adoption of non-invasive biomarker testing
- Integration of multiple parameters into diagnostic algorithms
- AI-assisted interpretation of test results
- Prediction: Will reduce diagnostic delays by 40-50%
Optimization of Current Therapies:
- Refined patient selection criteria for endoscopic and surgical approaches
- Standardized protocols for extraesophageal reflux management
- Improved deprescribing strategies for long-term PPI users
- Enhanced combination therapies targeting multiple mechanisms
- Prediction: Will improve treatment satisfaction by 20-30%
Medium-Term Prospects (3-7 Years):
Microbiome-Targeted Therapies:
- Probiotics specifically designed for esophageal health
- Prebiotics supporting beneficial esophageal flora
- Postbiotic metabolites with anti-inflammatory properties
- Fecal microbiota transplantation protocols for selected patients
- Prediction: Will emerge as adjunctive therapy for 15-20% of patients
Advanced Endoscopic Solutions:
- Single-session, comprehensive endoscopic anti-reflux procedures
- Bioabsorbable sphincter augmentation devices
- Endoscopically delivered neuromodulation systems
- Tissue-engineered patches for mucosal repair
- Prediction: Will reduce need for traditional surgery by 30-40%
Novel Drug Targets:
- Esophageal pain-specific channel blockers
- Targeted anti-inflammatory agents for esophageal mucosa
- Compounds enhancing mucosal defense mechanisms
- Drugs modulating esophageal hypersensitivity
- Prediction: Will address refractory symptoms in 30-35% of non-responders
Long-Term Possibilities (7-15 Years):
- Transformative Approaches:
Bioengineered LES replacement:
- Tissue-engineered sphincter constructs
- Cellular therapy for sphincter regeneration
- Bioelectronic LES function restoration
- 3D-bioprinted sphincter components
- Prediction: First human applications within 10-12 years
Comprehensive Genetic Solutions:
- Gene therapy for heritable GERD components
- CRISPR-based correction of susceptibility variants
- Epigenetic modification to enhance mucosal resilience
- Precision genetic risk profiling from birth
- Prediction: Personalized genetic interventions by 2035-2040
Neurological Reimagining:
- Direct brain-computer interfaces for symptom control
- Vagal nerve stimulation protocols
- Targeted spinal cord modulation
- Peripheral nerve rewiring to restore normal function
- Prediction: Initial applications in severe, refractory cases within 15 years
Artificial Intelligence Integration:
- Continuous monitoring with implantable sensors
- Predictive modeling preventing symptom flares
- Automated medication adjustment
- Integrated management of multiple digestive disorders
- Prediction: Standard component of care by 2030-2035
The future of acid reflux management is likely to be characterized by increasingly personalized approaches based on specific pathophysiological mechanisms, enhanced by technological integration, and moving beyond acid suppression to address the multifactorial nature of the disease. While complete “cures” may remain elusive given the complex and often multifactorial nature of GERD, the combination of emerging therapies promises to dramatically improve quality of life and reduce complication rates for the millions affected worldwide.
12. Interesting Facts & Lesser-Known Insights
This section explores fascinating aspects of acid reflux that are not widely known, clarifies common misconceptions, and examines how the condition affects specific populations and professions.
Uncommon Knowledge About Acid Reflux
Historical and Evolutionary Perspectives:
Ancient Treatments: Egyptian papyri from 1550 BCE described treating “fire in the chest” (likely heartburn) with a mixture of mastic gum, milk, and honey. Remarkably, modern research has confirmed mastic gum’s acid-neutralizing properties.
Presidential Affliction: At least four U.S. presidents (John Adams, Theodore Roosevelt, Bill Clinton, and George W. Bush) suffered from documented GERD, suggesting the condition may be exacerbated by high-stress leadership positions.
Evolutionary Theory: Some researchers propose that acid reflux may be partially a consequence of human evolution to an upright posture, which repositioned the esophageal-gastric junction in a way that makes it more vulnerable to reflux compared to quadrupedal animals.
Victorian Diagnosis: In the 19th century, GERD symptoms were often diagnosed as “nervous dyspepsia” and treated with odd remedies including strychnine, arsenic, and electrical stimulation of the abdomen.
Physiological Curiosities:
The Acid Pocket: After meals, a layer of highly acidic gastric juice (pH 1-2) forms at the top of the stomach contents, directly below the esophageal opening, creating an “acid pocket” that is particularly likely to reflux. This phenomenon wasn’t discovered until the early 2000s.
Left-Side Sleeping: Sleeping on the left side reduces reflux episodes by 71% compared to the right side. This is due to the anatomical position of the stomach and esophagus, which places the junction higher than the pool of acid when lying on the left.
Saliva Superpowers: Human saliva can neutralize refluxed acid with its natural bicarbonate content and stimulate esophageal clearance. A single swallow can normalize esophageal pH from acidic (pH 4) to neutral (pH 7) within 7-10 seconds.
The Air Swallowing Connection: The average person swallows 2,000-3,000 times daily and inadvertently swallows about 20-30 cubic inches of air in the process. In GERD patients, this volume can be 2-3 times higher and contribute to reflux events.
Belching Physiology: A single belch releases about 10-30 mL of gas from the stomach and can trigger reflux. GERD patients tend to belch 2-3 times more frequently than healthy individuals (60-80 times daily vs. 25-30 times).
Clinical Pearls:
Midnight Acid Surge: Around 2-3 AM, the body naturally produces more stomach acid, explaining why nighttime reflux can be particularly problematic. This corresponds with the lowest point of prostaglandin production, which normally protects the stomach lining.
Post-Exercise Window: The risk of reflux is highest during the first 30-45 minutes after exercise, not during the activity itself, due to transient changes in pressure gradients across the gastroesophageal junction.
Silent Reflux Reality: Up to 20% of patients with significant esophageal acid exposure have no heartburn or typical symptoms, instead presenting with “silent reflux” manifestations like chronic cough or hoarseness.
The Rebound Phenomenon: Approximately 40-60% of patients experience acid hypersecretion (rebound) when stopping PPI therapy after extended use, which can be mistaken for return of GERD rather than a medication withdrawal effect.
Hiccup Connection: Chronic hiccups can be both a cause and consequence of GERD, creating a vicious cycle where each exacerbates the other. Treating the reflux resolves hiccups in about 35% of chronic cases.
Myths and Misconceptions vs. Medical Facts
Myth: Acid reflux is just a nuisance, not a serious medical condition. Fact: Chronic GERD can lead to significant complications including Barrett’s esophagus, strictures, and esophageal adenocarcinoma, which has increased 700% in incidence over the past four decades.
Myth: Milk is an effective remedy for heartburn. Fact: While milk may temporarily buffer stomach acid, it stimulates acid production within 30-60 minutes due to its calcium and protein content, potentially worsening symptoms.
Myth: Acid reflux only affects the esophagus. Fact: GERD can impact multiple body systems, including the respiratory system (asthma, chronic cough), ears, nose and throat (laryngitis, sinusitis), oral health (dental erosions), and even sleep quality.
Myth: More stomach acid means more reflux. Fact: GERD is primarily caused by anatomical and functional issues with the esophageal sphincter and esophageal clearance mechanisms, not excessive acid production. In fact, some GERD patients have normal or even low acid production.
Myth: Heartburn during pregnancy means your baby will be born with a full head of hair. Fact: This old wives’ tale has no scientific basis. Pregnancy-related reflux is caused by hormonal changes and physical pressure from the growing uterus, not fetal hair development.
Myth: GERD is an inevitable part of aging. Fact: While prevalence increases with age, reflux is not a normal part of aging. Age-related changes that can contribute to GERD (weakened LES, delayed gastric emptying) can often be addressed with appropriate interventions.
Myth: Drinking water with meals dilutes stomach acid and worsens digestion. Fact: Moderate water consumption with meals does not significantly impact digestion and may actually help neutralize and clear acid from the esophagus if reflux occurs.
Myth: Once you start taking PPIs, you’ll need them for life. Fact: Many patients can successfully discontinue PPIs after healing with properly managed step-down approaches. Even long-term users can often reduce dosage or switch to on-demand therapy.
Myth: Spicy foods cause stomach ulcers and should be avoided with GERD. Fact: Ulcers are primarily caused by H. pylori infection or NSAID use, not spicy foods. While spicy foods may trigger reflux symptoms in some individuals, they don’t damage the stomach or cause ulcers directly.
Myth: GERD symptoms that aren’t relieved by PPIs must be something else. Fact: 30-40% of GERD patients have an incomplete response to PPIs. This may be due to non-acid reflux, delayed gastric emptying, visceral hypersensitivity, or other mechanisms that PPIs don’t address.
Impact on Specific Populations and Professions
Occupational Impacts:
Professional Singers and Voice Performers:
- Prevalence: 55-70% report GERD symptoms, much higher than general population
- Unique manifestations: Voice changes, throat clearing, vocal fatigue
- Performance impact: Acid exposure can cause vocal cord edema and mucosal thickening, affecting voice quality
- Career consequences: Can limit performance ability and longevity
- Management challenges: Balance between pre-performance fasting, medication timing, and energy needs
- Specialized approaches: Custom protocols for performance days, including timing of meals and medications
Shift Workers:
- Prevalence: 25-30% higher than day workers
- Contributing factors: Disrupted circadian rhythms affecting gastric acid secretion patterns
- Severity: Often more severe symptoms due to irregular eating patterns and sleep disruption
- Special challenges: Difficulty maintaining consistent mealtimes and sleep positions
- Industry-specific risk: Highest in healthcare, transportation, and manufacturing sectors
- Management approach: Modified meal scheduling, timed acid suppression therapy
Professional Athletes:
- High-risk sports: Running, cycling, weightlifting, high-intensity training
- Mechanism: Increased intra-abdominal pressure during exertion
- Performance impact: Can limit training intensity and competition performance
- Nutritional challenge: Balancing caloric needs with reflux management
- Medication considerations: Timing around competition, doping regulations
- Prevention strategies: Pre-event nutrition protocols, specialized hydration approaches
Commercial Drivers:
- Prevalence: 34-40% report regular GERD symptoms
- Risk factors: Sedentary position, irregular meals, limited food choices
- Safety concerns: Sleep disruption, medication side effects, pain distraction
- Economic impact: Lost work days and medical certification concerns
- Management challenges: Limited access to healthy food options, restricted medication timing
- Specialized approaches: Vehicle modifications, route planning for meal access
Age-Specific Considerations:
Pediatric GERD:
- Distinctive features: More common respiratory manifestations (cough, wheezing)
- Developmental impacts: Can affect feeding, weight gain, and sleep patterns
- Diagnostic challenges: Limited ability to describe symptoms in young children
- Long-term concerns: Potential esophageal damage during critical growth periods
- Treatment differences: More conservative medication approaches due to developing systems
- Natural history: Often improves with physical development, particularly after age 12-18 months
Elderly Patients:
- Symptom variations: Often less heartburn but more regurgitation, dysphagia, and respiratory symptoms
- Comorbidity interactions: Complicated by multiple medications and conditions
- Complication risks: Higher risk of severe esophagitis and Barrett’s esophagus
- Medication considerations: Altered drug metabolism, increased risk of medication interactions
- Nutritional impacts: Can contribute to malnutrition and weight loss
- Quality of life effect: Significant impact on independence and activity levels
Special Populations:
Pregnant Women:
- Prevalence: 40-85% experience GERD symptoms during pregnancy
- Trimester pattern: Usually worst in third trimester
- Mechanisms: Combination of hormonal effects (progesterone relaxes LES) and physical pressure
- Management challenges: Medication safety concerns, limited positioning options
- Postpartum resolution: Symptoms typically resolve within 4-6 weeks after delivery
- Long-term impact: Possibly higher lifetime risk of GERD after multiple pregnancies
Post-Bariatric Surgery Patients:
- Complex relationship: Can improve or worsen GERD depending on procedure type
- Procedure-specific risks: Sleeve gastrectomy may worsen GERD (35-63% new-onset)
- Protection effect: Roux-en-Y gastric bypass typically improves or resolves GERD (75-80%)
- Anatomical challenges: Altered surgical anatomy complicates both diagnosis and treatment
- Nutritional factors: Post-surgical diet modifications may inadvertently trigger symptoms
- Monitoring importance: Regular assessment essential due to changing anatomy and weight
Patients with Connective Tissue Disorders:
- Prevalence: Up to 80% in scleroderma, 30-40% in Ehlers-Danlos syndrome
- Mechanism: Weakened tissue support structures and impaired esophageal motility
- Severity: Often more severe and refractory to standard treatments
- Complication risk: Higher rates of Barrett’s esophagus and strictures
- Treatment challenges: Often require higher medication doses and earlier surgical consideration
- Management approach: Multidisciplinary care coordinating rheumatological and gastroenterological expertise
Pulmonary Disease Patients:
- Bidirectional relationship: GERD can worsen asthma, COPD, pulmonary fibrosis; respiratory conditions can exacerbate GERD
- Symptom overlap: Cough, shortness of breath can be attributed to either condition
- Medication interactions: Respiratory medications (theophylline, beta-agonists) can worsen GERD
- Treatment impact: GERD control can improve pulmonary function and reduce exacerbations
- Diagnostic complexity: Often requires specialized testing to clarify relationship
- Integrated management: Coordinated care between pulmonology and gastroenterology critical
The complex and multifaceted nature of acid reflux extends far beyond simple heartburn, affecting diverse aspects of human physiology, daily life, and specific populations in unique ways. Understanding these nuances helps debunk common misconceptions and enables more personalized and effective management strategies for this ubiquitous condition.
Conclusion
Acid reflux or GERD represents a significant global health challenge affecting millions of individuals across all demographics. As this comprehensive report has highlighted, the condition is far more complex than just occasional heartburn, involving intricate physiological mechanisms, diverse symptom presentations, and potential for serious complications if left untreated.
The medical understanding of GERD has evolved substantially over the past century, from rudimentary descriptions of symptoms to sophisticated comprehension of its multifactorial pathophysiology. This evolution continues today, with emerging research into genetic factors, microbiome influences, and neuroinflammatory components offering new insights into why some individuals develop GERD and how it can be most effectively managed.
From a therapeutic perspective, treatment approaches have progressed from simple antacids to targeted pharmacological, endoscopic, and surgical interventions. The current management paradigm emphasizes individualized care based on symptom patterns, underlying mechanisms, and patient preferences. Looking forward, innovative approaches including novel pharmaceuticals, advanced endoscopic techniques, and potentially transformative bioengineered solutions promise to further expand the therapeutic armamentarium.
Prevention and early intervention remain crucial strategies, with lifestyle modifications forming the foundation of both primary prevention and adjunctive treatment. The significant geographical variations in GERD prevalence highlight the influence of environmental and lifestyle factors, offering opportunities for targeted public health interventions.
For patients living with GERD, understanding the condition’s true nature—beyond the myths and misconceptions—enables more effective self-management and informed healthcare decisions. For healthcare providers, recognizing the diverse manifestations, population-specific considerations, and emerging treatment options facilitates optimal care delivery.
As research continues to advance our understanding of this common yet complex condition, the future holds promise for more effective, personalized, and potentially curative approaches to acid reflux management, reducing its global burden and improving quality of life for the millions affected worldwide.

