
⚠️ Disclaimer: The information provided in this article is for educational purposes only and does not constitute medical advice. RevisionTown does not provide diagnosis, treatment, or medical recommendations. Always consult a qualified healthcare professional regarding any medical condition, symptoms, or concerns.
Read More – 🏥 Medical Disclaimer
What is Influenza Virus?
Influenza is a contagious respiratory illness caused by influenza viruses that infect the nose, throat, and sometimes the lungs. The disease ranges from mild to severe and can lead to hospitalization and death, particularly in vulnerable populations.
Concise Definition
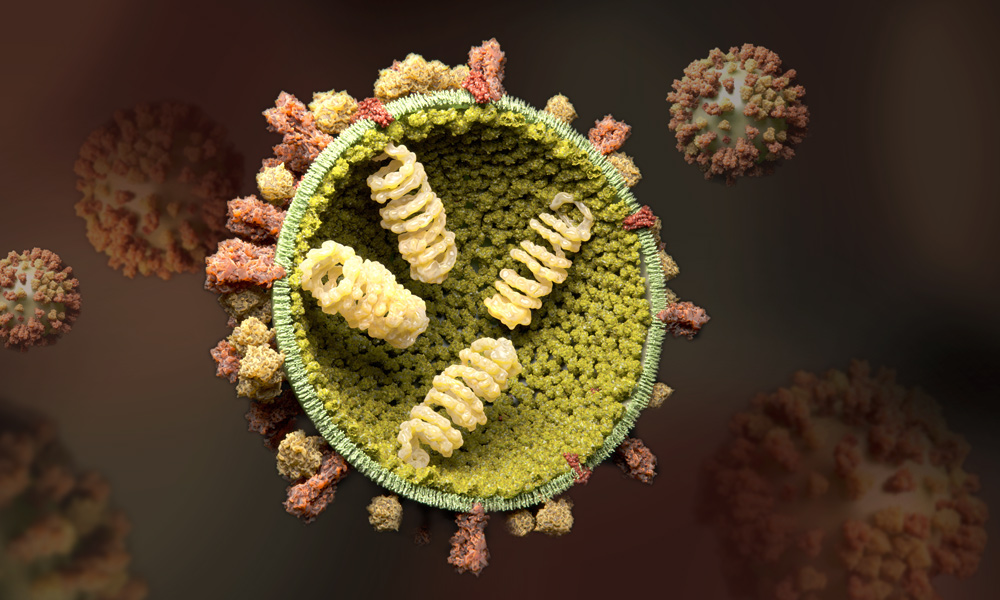
Influenza viruses are RNA viruses belonging to the Orthomyxoviridae family. There are four types of influenza viruses: A, B, C, and D. Influenza A and B viruses circulate and cause seasonal epidemics of disease in humans. Influenza A viruses are further classified into subtypes according to combinations of hemagglutinin (HA) and neuraminidase (NA) proteins on the virus surface.
Current Circulating Strains:
- Influenza A(H1N1)pdm09 (pandemic strain from 2009)
- Influenza A(H3N2)
- Influenza B/Victoria lineage
- Influenza B/Yamagata lineage (has not circulated since March 2020)
Affected Body Parts/Organs
Primary Targets:
- Respiratory System: Nose, throat, trachea, bronchi, and lungs
- Systemic Effects: Affects multiple organ systems through inflammatory responses
Secondary Complications Can Affect:
- Cardiovascular system (myocarditis, pericarditis)
- Central nervous system (encephalitis, seizures)
- Musculoskeletal system (myositis, rhabdomyolysis)
- Renal system (acute kidney injury)
Prevalence and Significance
Global Impact:
- Annual global burden: 3-5 million cases of severe illness
- Annual deaths: 290,000-650,000 respiratory deaths globally
- In the United States (2023-2024 season): 40 million illnesses, 18 million medical visits, 470,000 hospitalizations, and 28,000 deaths
- Economic burden: Billions of dollars in healthcare costs and lost productivity annually
Public Health Significance:
- Leading cause of vaccine-preventable death in the United States
- Major contributor to healthcare system strain during peak seasons
- Potential for pandemic emergence with novel strains
2. History & Discoveries
Timeline of Major Discoveries
1889-1893: Early Investigations
- First systematic studies of pandemic influenza
- Richard Pfeiffer identified Haemophilus influenzae (initially thought to be the causative agent)
- Establishment of bacteriological research methods
1918-1919 Pandemic: The Turning Point
- Most severe pandemic in recorded history
- Killed an estimated 50-100 million people worldwide
- Affected one-third of the global population (approximately 500 million people)
- Unique pattern: high mortality in healthy adults aged 20-40
1930s: Viral Discovery Era
- 1931: Richard E. Shope isolated swine influenza virus
- 1933: Wilson Smith, C.H. Andrewes, and P.P. Laidlaw at London’s National Institute for Medical Research isolated the first human influenza virus
- Recognition that influenza is caused by a virus, not bacteria
1940s-1950s: Vaccine Development
- 1942: First inactivated influenza vaccine developed by Thomas Francis and Jonas Salk
- 1947: Discovery that existing vaccines were ineffective against new strains
- 1948: WHO established the Worldwide Influenza Centre
- 1952: Creation of Global Influenza Surveillance and Response System (GISRS)
Modern Era Breakthroughs:
- 1957: Asian flu pandemic (H2N2)
- 1968: Hong Kong flu pandemic (H3N2)
- 2003: First live attenuated nasal spray vaccine licensed
- 2005: Complete genome sequencing of 1918 pandemic virus
- 2009: H1N1 pandemic emergence
- 2013: First recombinant DNA influenza vaccine approved
Major Scientific Breakthroughs
Virus Reconstruction (2005): Scientists successfully reconstructed the complete 1918 pandemic virus in CDC laboratories, providing crucial insights into pandemic virulence mechanisms and helping prepare for future pandemics.
Antiviral Development:
- Neuraminidase inhibitors (1990s-2000s): Oseltamivir, zanamivir, peramivir
- Cap-dependent endonuclease inhibitor (2018): Baloxavir marboxil – first new class of influenza antivirals in 20 years
Evolution of Medical Understanding
The understanding of influenza has evolved from a mysterious “epidemic disease” to a well-characterized viral infection with known transmission patterns, antigenic drift and shift mechanisms, and sophisticated surveillance systems. Modern research focuses on universal vaccines, improved antivirals, and pandemic preparedness.
3. Symptoms
Early Symptoms (First 24-48 hours)
Sudden Onset Characteristics:
- High fever (100°F/38°C or higher)
- Chills and sweats
- Headache
- Muscle aches and joint pain
- Extreme fatigue and weakness
- Dry cough (initially)
Advanced-Stage Symptoms (Days 3-7)
Respiratory Progression:
- Productive cough with phlegm
- Sore throat
- Runny or stuffy nose
- Chest discomfort
Systemic Symptoms:
- Continued high fever
- Severe body aches
- Persistent fatigue
- Nausea and vomiting (more common in children)
- Diarrhea (more common in children)
Common vs. Rare Symptoms
Common Symptoms (>70% of cases):
- Fever and chills
- Cough
- Body aches
- Fatigue
- Headache
- Sore throat
Less Common Symptoms (10-30% of cases):
- Gastrointestinal symptoms (nausea, vomiting, diarrhea)
- Runny nose
- Sneezing
Rare but Serious Symptoms (<5% of cases):
- Difficulty breathing or shortness of breath
- Chest pain or pressure
- Persistent dizziness
- Severe or persistent vomiting
- High fever lasting more than 3 days
Symptom Progression Timeline
Days 1-2: Sudden onset of fever, chills, and body aches Days 3-4: Peak symptoms with respiratory involvement Days 5-7: Gradual improvement in most patients Days 7-14: Complete recovery in uncomplicated cases
Complications typically emerge: Days 3-7 if they occur
4. Causes
Biological Causes
Viral Etiology:
- Primary Causative Agents: Influenza A and B viruses
- Viral Structure: Single-stranded, negative-sense RNA viruses with 8 gene segments
- Key Proteins: Hemagglutinin (HA) and Neuraminidase (NA) surface proteins determine subtype and infectivity
Antigenic Changes:
- Antigenic Drift: Gradual mutations leading to seasonal vaccine updates
- Antigenic Shift: Major changes potentially causing pandemics (influenza A only)
Environmental Causes and Transmission
Primary Transmission Routes:
- Respiratory droplets: When infected persons cough, sneeze, or talk
- Aerosol transmission: Fine particles remaining airborne
- Contact transmission: Touching contaminated surfaces then touching face
Environmental Factors Facilitating Spread:
- Cold, dry weather conditions
- Indoor crowding during winter months
- Poor ventilation systems
- Low humidity levels (below 40%)
Genetic and Hereditary Factors
Host Genetic Susceptibility:
- Variations in immune response genes (HLA types)
- Differences in innate immunity receptors
- Age-related immune system changes
- Pregnancy-related immune modifications
No Direct Hereditary Transmission: Influenza is not inherited but genetic factors influence individual susceptibility and disease severity.
Exposure Risks and Triggers
High-Risk Exposures:
- Close contact with infected individuals (within 6 feet)
- Healthcare settings during influenza season
- Travel to areas with active influenza transmission
- Large gatherings during peak season
- Contact with contaminated surfaces
Occupational Risks:
- Healthcare workers
- Teachers and school staff
- Daycare providers
- Public transportation workers
- Military personnel in close quarters
5. Risk Factors
Age-Related Risk Factors
Highest Risk Groups:
- Children under 5 years (especially under 2 years)
- Adults 65 years and older
- Adults 50-64 years (intermediate risk)
Age-Specific Complications:
- Infants: Higher risk of severe disease and hospitalization
- Elderly: Highest mortality rates (68% of influenza deaths occur in those ≥65 years)
- Young adults: Lower risk but can develop severe disease during pandemics
Gender and Demographic Factors
Pregnancy:
- Increased risk of severe influenza and complications
- Higher hospitalization rates, especially in 2nd and 3rd trimesters
- Risk extends to 2 weeks postpartum
Gender Differences:
- Similar overall infection rates between males and females
- Pregnant women at significantly higher risk
- Some evidence of sex-based differences in immune responses
Occupational Risk Factors
High-Risk Occupations:
- Healthcare workers (3-4 times higher infection risk)
- Teachers and educational staff
- Childcare providers
- Emergency responders
- Military personnel
- Public transportation workers
Environmental and Lifestyle Factors
Increased Risk Factors:
- Living in crowded conditions
- Frequent travel, especially international
- Poor nutrition and physical fitness
- Inadequate sleep patterns
- High stress levels
- Smoking and alcohol abuse
Pre-existing Medical Conditions
Chronic Medical Conditions Increasing Risk:
- Pulmonary: Asthma, COPD, cystic fibrosis
- Cardiovascular: Heart disease, hypertension
- Metabolic: Diabetes, obesity (BMI ≥30)
- Renal: Chronic kidney disease
- Hepatic: Chronic liver disease
- Hematologic: Sickle cell disease, other blood disorders
- Neurologic: Seizure disorders, cerebral palsy, developmental disabilities
- Immunologic: HIV/AIDS, cancer, immunosuppressive medications
Immunocompromising Conditions:
- Cancer treatment (chemotherapy, radiation)
- Organ transplant recipients
- Chronic corticosteroid use
- Primary immunodeficiency disorders
6. Complications
Common Complications
Respiratory Complications:
- Primary viral pneumonia: Direct viral infection of lung tissue
- Secondary bacterial pneumonia: Most common serious complication
- Acute respiratory distress syndrome (ARDS): Severe cases
- Exacerbation of chronic conditions: Asthma, COPD
Secondary Bacterial Infections:
- Streptococcus pneumoniae (most common)
- Staphylococcus aureus (including MRSA)
- Haemophilus influenzae
Severe Complications
Cardiovascular:
- Myocarditis and pericarditis
- Acute myocardial infarction
- Stroke
Neurological:
- Encephalitis
- Febrile seizures (especially in children)
- Guillain-Barré syndrome (rare)
Multi-organ System:
- Sepsis and septic shock
- Multi-organ failure
- Acute kidney injury
- Rhabdomyolysis
Long-term Health Impact
Post-Influenza Complications:
- Prolonged fatigue and weakness
- Secondary bacterial infections
- Exacerbation of chronic conditions
- Increased risk of cardiovascular events in weeks following infection
Chronic Disease Impact:
- Worsening of underlying asthma or COPD
- Diabetic complications
- Increased hospitalizations for heart disease
Mortality and Disability Rates
Mortality Statistics (2023-2024 U.S. Season):
- Total Deaths: Approximately 28,000
- Pediatric Deaths: 724 estimated deaths in children <18 years
- Hospitalization Rate: 470,000 hospitalizations
- Case Fatality Rate: Varies by age and risk factors (0.1% overall, up to 5-10% in high-risk groups)
Age-Specific Mortality:
- Children <5 years: Higher hospitalization rates
- Adults 18-64 years: Moderate mortality risk
- Adults ≥65 years: Account for 68% of deaths despite being 8% of medical visits
Disability Impact:
- Temporary work disability: 3-7 days average
- School absenteeism: 5-10 days average
- Long-term disability: Rare but possible in severe cases with complications
7. Diagnosis & Testing
Overview of Testing Methods
Multiple diagnostic approaches are available for influenza detection, each with specific advantages, limitations, and appropriate clinical applications.
Rapid Diagnostic Tests (RIDTs)
Rapid Influenza Diagnostic Tests:
- Mechanism: Detect viral antigens in respiratory specimens
- Turnaround Time: 15 minutes or less
- Sensitivity: 50-70% (recently improved to ≥80% by FDA requirements)
- Specificity: 95-99%
- Clinical Use: Point-of-care testing in outpatient settings
- Limitations: High false-negative rates, especially during peak activity
Second-Generation RIDTs:
- Enhanced sensitivity with analyzer devices (Sofia, BD Veritor, Fujifilm)
- Improved performance but still inferior to molecular assays
Molecular Assays (Gold Standard)
Reverse Transcription-Polymerase Chain Reaction (RT-PCR):
- Sensitivity: 95-100%
- Specificity: 95-100%
- Turnaround Time: 45 minutes to several hours
- Capabilities: Can differentiate influenza A and B, identify subtypes
- Clinical Use: Preferred for hospitalized patients and definitive diagnosis
Rapid Molecular Assays:
- Turnaround Time: 15-30 minutes
- Sensitivity: 90-95%
- Specificity: Similar to RT-PCR
- Availability: Point-of-care testing increasingly available
- Advantage: Combines speed of RIDTs with accuracy of molecular testing
Specimen Collection Guidelines
Preferred Specimens:
- Nasopharyngeal swabs: Highest sensitivity
- Nasal swabs: Acceptable alternative
- Throat swabs: Lower sensitivity, not recommended alone
- Sputum: For hospitalized patients when available
Optimal Timing:
- Within 3-4 days of illness onset
- Earlier collection yields higher sensitivity
- Immunocompromised patients may shed virus longer
Diagnostic Algorithms
Outpatient Settings:
- Clinical assessment during influenza season
- Rapid molecular assay preferred over RIDT
- Negative RIDT should be confirmed with molecular assay during peak activity
Hospitalized Patients:
- RT-PCR or molecular assay required
- Results influence antiviral treatment decisions
- Infection control measures based on results
Institutional Outbreaks:
- Molecular confirmation required
- Contact tracing and prophylaxis decisions based on results
Testing Limitations and Considerations
False Negatives:
- More common with RIDTs (30-50% false negative rate)
- Late in illness course (>4 days)
- Poor specimen quality
- Low viral load patients
False Positives:
- Rare with high specificity tests
- More likely during low prevalence periods
- Cross-reactivity with other respiratory viruses (minimal with current assays)
Clinical Decision Making:
- Negative tests do not rule out influenza during peak season
- Positive RIDTs generally reliable
- Molecular assays provide most reliable results for clinical management
Emerging Diagnostic Technologies
Multiplex Assays:
- Detect multiple respiratory pathogens simultaneously
- Include influenza A/B, RSV, SARS-CoV-2, and other viruses
- Useful for differential diagnosis
Point-of-Care Advances:
- Improved sensitivity rapid molecular assays
- Integration with electronic health records
- Cost-effectiveness improvements
8. Treatment Options
Antiviral Medications
Neuraminidase Inhibitors:
Oseltamivir (Tamiflu®)
- Route: Oral
- Dosing: 75 mg twice daily for 5 days (adults)
- Mechanism: Blocks viral neuraminidase enzyme
- Effectiveness: Reduces illness duration by 1-3 days when started within 48 hours
- Special Uses: Preferred for pregnant women, children, hospitalized patients
Zanamivir (Relenza®)
- Route: Inhaled powder
- Dosing: 10 mg twice daily for 5 days
- Contraindications: Asthma, COPD (due to bronchospasm risk)
- Advantages: Minimal systemic absorption
Peramivir (Rapivab®)
- Route: Intravenous
- Dosing: Single 600 mg dose (adults)
- Use: Patients unable to take oral medications
- Duration: Single dose treatment
Cap-dependent Endonuclease Inhibitor:
- Baloxavir Marboxil (Xofluza®)
- Route: Oral, single dose
- Dosing: Weight-based (40-80 mg single dose)
- Mechanism: Inhibits viral RNA transcription
- Advantages: Single dose, faster viral clearance
- Effectiveness: Superior to placebo, similar clinical efficacy to oseltamivir
- Recent Evidence: Reduces household transmission by ~35%
Treatment Timing and Effectiveness
Optimal Treatment Window:
- Most effective when started within 48 hours of symptom onset
- Can be beneficial up to 4-5 days in hospitalized patients
- Earlier initiation provides greater benefit
Treatment Effectiveness:
- Symptom Duration: Reduced by 1-3 days
- Hospitalization: 40-60% reduction in risk when used appropriately
- Viral Shedding: Significantly reduced, especially with baloxavir
- Complications: Reduced incidence when treatment started early
Treatment Indications
Recommended for Treatment:
- Hospitalized patients with confirmed or suspected influenza
- Patients at high risk for complications
- Severe, complicated, or progressive illness
- Healthcare workers and residents of long-term care facilities
May Consider for Treatment:
- Otherwise healthy outpatients if treatment can be started within 48 hours
- Patients with prolonged illness beyond typical course
Supportive Care
Symptomatic Management:
- Fever/Pain: Acetaminophen, ibuprofen (avoid aspirin in children)
- Hydration: Increased fluid intake, electrolyte replacement if needed
- Rest: Adequate sleep and activity restriction
- Humidity: Humidified air for respiratory comfort
Respiratory Support:
- Oxygen therapy for hypoxemic patients
- Mechanical ventilation for severe respiratory failure
- ECMO for most severe cases
Chemoprophylaxis
Post-exposure Prophylaxis:
- Indications: High-risk individuals exposed to confirmed cases
- Timing: Within 48 hours of exposure
- Duration: 7 days after last exposure
- Agents: Oseltamivir, zanamivir, or single-dose baloxavir
Pre-exposure Prophylaxis:
- Indications: Institutional outbreaks, unvaccinated high-risk individuals
- Duration: Throughout outbreak period or influenza season
- Effectiveness: 70-90% efficacy in preventing illness
Emerging Treatments and Clinical Trials
Combination Therapies:
- Research into combination antiviral approaches
- Baloxavir plus neuraminidase inhibitor combinations
- Enhanced efficacy and resistance prevention
Novel Antiviral Targets:
- Polymerase complex inhibitors (pimodivir)
- Host-targeted therapies
- Broadly neutralizing antibodies
Monoclonal Antibodies:
- Emergency use authorizations for high-risk patients
- Targeted against specific influenza strains
- Potential for treatment and prevention
Future Directions:
- Universal influenza antivirals
- Resistance-proof treatment strategies
- Personalized medicine approaches based on viral and host genetics
9. Prevention & Precautionary Measures
Vaccination: Primary Prevention Strategy
Annual Influenza Vaccination:
- Recommendation: All persons ≥6 months of age annually
- Timing: Early fall, before influenza season begins
- Effectiveness: 40-60% when well-matched to circulating strains
- 2024-2025 Season: Trivalent vaccines containing A(H1N1), A(H3N2), and B/Victoria components
Vaccine Types Available:
Inactivated Influenza Vaccines (IIV)
- Standard-dose, high-dose, and adjuvanted formulations
- Approved for ages ≥6 months
- Most commonly used vaccine type
Live Attenuated Influenza Vaccine (LAIV)
- Nasal spray formulation (FluMist)
- Approved for ages 2-49 years (healthy individuals only)
- Self-administration option approved for 2025-2026 season
Recombinant Influenza Vaccines (RIV)
- Egg-free production
- Approved for ages ≥18 years
Special Populations:
- Pregnant Women: Inactivated vaccines recommended in any trimester
- Children 6 months-8 years: May need two doses in first vaccination season
- Adults ≥65 years: High-dose or adjuvanted vaccines preferred
- Egg Allergy: Recombinant or carefully administered standard vaccines
Non-Pharmaceutical Interventions
Personal Hygiene Measures:
- Hand Hygiene: Frequent handwashing with soap and water for ≥20 seconds
- Alcohol-based Sanitizers: When soap unavailable (≥60% alcohol content)
- Respiratory Etiquette: Cover coughs and sneezes with tissue or elbow
- Face Touching: Avoid touching eyes, nose, and mouth with unwashed hands
Physical Distancing:
- Maintain distance from sick individuals (≥6 feet when possible)
- Avoid crowded areas during peak influenza activity
- Stay home when ill to prevent transmission
Environmental Controls:
- Ventilation: Ensure adequate air circulation in indoor spaces
- Surface Disinfection: Regular cleaning of frequently touched surfaces
- Humidity Control: Maintain indoor humidity levels 40-60%
Workplace and Institutional Prevention
Healthcare Settings:
- Annual vaccination requirements for staff
- Isolation precautions for suspected/confirmed cases
- Personal protective equipment (PPE) protocols
- Visitor restrictions during outbreaks
Schools and Childcare:
- Exclude ill children until fever-free for 24 hours
- Promote hand hygiene and respiratory etiquette
- Environmental cleaning protocols
- Vaccination campaigns
Long-term Care Facilities:
- Comprehensive vaccination programs for residents and staff
- Outbreak response protocols
- Visitor screening and restrictions
- Antiviral prophylaxis during outbreaks
Lifestyle Modifications
Immune System Support:
- Adequate Sleep: 7-9 hours nightly for adults
- Regular Exercise: Moderate physical activity to boost immunity
- Healthy Diet: Balanced nutrition with adequate vitamins and minerals
- Stress Management: Chronic stress reduction techniques
Risk Reduction Behaviors:
- Smoking cessation (smoking increases influenza risk and complications)
- Moderate alcohol consumption
- Management of chronic diseases
- Regular medical care and preventive services
Travel Precautions
International Travel:
- Check destination influenza activity levels
- Ensure up-to-date vaccination
- Pack hand sanitizer and disinfecting wipes
- Consider antiviral prophylaxis for high-risk travelers
Air Travel Specific:
- Use hand sanitizer frequently
- Avoid touching face during travel
- Consider wearing masks in crowded areas
- Stay hydrated during flights
Community-Level Prevention
Public Health Surveillance:
- Monitor influenza activity levels
- Early detection of outbreaks
- Communication of current risk levels
Public Education Campaigns:
- Vaccination promotion
- Proper hygiene practices
- Recognition of symptoms
- When to seek medical care
Pandemic Preparedness:
- Stockpiling of antivirals and vaccines
- Healthcare system surge capacity planning
- Communication systems for public health emergencies
- International cooperation and surveillance
10. Global & Regional Statistics
Global Disease Burden
Worldwide Impact (Annual Estimates):
- Total Cases: 1 billion infections globally
- Severe Illness: 3-5 million cases
- Deaths: 290,000-650,000 respiratory deaths
- Hospitalization: Several million annually
- Economic Impact: Billions in healthcare costs and lost productivity
Regional Variations:
- Seasonal patterns differ between Northern and Southern Hemispheres
- Tropical regions may have year-round circulation
- Pandemic potential remains global concern
United States Statistics
2023-2024 Influenza Season (Completed):
- Total Illnesses: 40 million
- Medical Visits: 18 million
- Hospitalizations: 470,000
- Deaths: 28,000 (including 724 pediatric deaths)
- Vaccine Coverage: Varied by age group (32-69%)
2024-2025 Season (Ongoing Preliminary Data):
- Season started with increased activity across all regions
- A(H3N2) viruses predominating (54.2% of subtyped viruses)
- A(H1N1)pdm09 comprising 44.3% of subtyped viruses
- 139.65 million vaccine doses distributed as of November 2024
Age-Specific Burden
Pediatric Impact:
- Children have highest infection rates
- 40.8% vaccination coverage (2024-2025 season)
- Significant school absenteeism during peak season
- Higher hospitalization rates in children <2 years
Adult Impact (18-64 years):
- Moderate disease burden
- Significant workplace productivity losses
- Vaccination coverage: 40.8% (similar to previous season)
Elderly Impact (≥65 years):
- Highest mortality rates (68% of total deaths)
- 50% of hospitalizations despite being minority of cases
- Highest vaccination coverage (69%)
- Greatest healthcare resource utilization
International Comparisons
Vaccine Effectiveness (2024-2025 Season):
- United States: 32-78% depending on age group and setting
- Canada: 54% overall effectiveness
- South America: 34.5% effectiveness (2024 Southern Hemisphere season)
- Global Variations: Effectiveness varies by strain circulation and vaccine match
Surveillance Systems:
- United States: FluSurv-NET covering ~9% of population
- Europe: European Centre for Disease Prevention and Control (ECDC)
- Global: WHO Global Influenza Surveillance and Response System (GISRS)
- Pandemic Preparedness: International Health Regulations coordination
Mortality Trends and Patterns
Historical Perspective:
- 1918 Pandemic: 50-100 million deaths worldwide
- 1957 Asian Flu: ~1.1 million deaths globally
- 1968 Hong Kong Flu: ~1 million deaths globally
- 2009 H1N1 Pandemic: 151,700-575,400 deaths globally (first year)
Current Mortality Patterns:
- Seasonal variation in death rates
- Higher mortality during A(H3N2) predominant seasons
- Excess mortality extends beyond laboratory-confirmed cases
- Cardiovascular and respiratory deaths increase during influenza seasons
Economic Impact
Healthcare Costs:
- United States: $10.4 billion in direct medical costs annually
- Hospitalizations: Account for largest portion of costs
- Outpatient Care: Significant but lower per-case costs
- Long-term Care: Additional costs from institutional outbreaks
Productivity Losses:
- Work absenteeism: 3-7 days average per case
- School closures during severe outbreaks
- Caregiving responsibilities for ill family members
- Reduced economic activity during peak seasons
Vaccination Coverage and Effectiveness
Global Vaccination Rates:
- Vary significantly by country and healthcare system
- High-income countries: Generally 40-75% coverage in recommended groups
- Low- and middle-income countries: Often <20% coverage
- WHO recommendation: Prioritize pregnant women, children <5, and adults ≥65
Effectiveness Variations:
- Annual variation based on vaccine-strain match
- Age-related differences in immune response
- Prior vaccination history effects
- Circulating strain characteristics
11. Recent Research & Future Prospects
Latest Antiviral Developments
Baloxavir Advances (2024-2025):
- New evidence shows 35% reduction in household transmission
- Demonstrated superior efficacy against influenza B compared to oseltamivir
- Real-world effectiveness studies confirming clinical trial results
- Combination therapy research with neuraminidase inhibitors
Next-Generation Antivirals:
- Pimodivir (VX-787): PB2 inhibitor showing promise in clinical trials
- Cap-dependent endonuclease inhibitors: Additional agents in development
- Host-targeted therapies: Targeting cellular pathways essential for viral replication
- Resistance-minimizing strategies: Combination approaches and novel targets
Universal Influenza Vaccine Research
Current Approaches:
- Conserved epitope targeting: Focus on stable viral regions across strains
- Broadly neutralizing antibodies: Targeting stem region of hemagglutinin
- T-cell based vaccines: Leveraging cellular immunity for broad protection
- Nanoparticle platforms: Improved antigen presentation and stability
Clinical Trial Progress:
- Phase I/II trials for several universal vaccine candidates
- Promising early results for broadly protective immunity
- Challenges remain in achieving adequate breadth and durability
- Timeline: Potentially 5-10 years to licensure
Diagnostic Technology Advances
Point-of-Care Improvements:
- Enhanced sensitivity rapid molecular assays (>95% sensitivity)
- Multiplexed platforms detecting multiple respiratory pathogens
- Integration with electronic health records
- Cost reduction and increased accessibility
Emerging Technologies:
- CRISPR-based diagnostics: Ultra-sensitive detection methods
- Artificial intelligence: Enhanced result interpretation and prediction
- Wearable devices: Continuous monitoring for early detection
- Sequencing technologies: Real-time strain identification and characterization
Surveillance and Prediction Systems
Enhanced Global Surveillance:
- Real-time genomic sequencing networks
- Artificial intelligence for outbreak prediction
- Wastewater surveillance for community monitoring
- International data sharing improvements
Predictive Modeling:
- Machine learning for seasonal forecast accuracy
- Vaccine strain selection optimization
- Resource allocation planning
- Pandemic risk assessment tools
Vaccine Technology Innovations
mRNA Vaccines:
- Rapid development and deployment capabilities
- Improved strain matching potential
- Enhanced immune responses
- Clinical trials for seasonal and pandemic influenza
Adjuvant Developments:
- Next-generation immune enhancers
- Age-specific formulations
- Improved durability of protection
- Reduced dose requirements
Pandemic Preparedness Research
Zoonotic Surveillance:
- Enhanced monitoring of avian and swine influenza viruses
- Risk assessment for pandemic potential strains
- Pre-pandemic vaccine development (H5N1, H7N9)
- Rapid response protocols
Public Health Innovations:
- Digital contact tracing systems
- Community engagement strategies
- Risk communication optimization
- International cooperation frameworks
Host-Pathogen Interaction Studies
Genetic Susceptibility Research:
- Host genetic factors influencing disease severity
- Personalized medicine approaches
- Age-related immune changes
- Pregnancy-specific research
Immunological Advances:
- Understanding of protective immunity duration
- Cross-reactive immunity mechanisms
- Vaccine-induced vs. natural immunity
- Immune correlates of protection
Future Treatment Paradigms
Precision Medicine:
- Genetic testing to guide antiviral selection
- Viral sequencing for resistance testing
- Personalized vaccine recommendations
- Risk stratification algorithms
Combination Therapies:
- Antiviral combinations to prevent resistance
- Immunomodulatory approaches
- Prophylactic antibody treatments
- Therapeutic vaccines
Research Funding and Priorities
Major Research Initiatives:
- NIH/NIAID influenza research programs
- BARDA pandemic preparedness investments
- WHO research and development priorities
- Private-public partnerships
Priority Areas:
- Universal influenza vaccines
- Next-generation antivirals
- Improved diagnostic technologies
- Pandemic preparedness
- Pediatric and pregnancy-specific research
12. Interesting Facts & Lesser-Known Insights
Historical Curiosities
The “Spanish Flu” Misnomer: The 1918 pandemic was called “Spanish flu” not because it originated in Spain, but because Spain, being neutral in World War I, had no wartime censorship and freely reported the outbreak. The pandemic likely originated in Kansas, United States, and spread via military movements.
Viral vs. Bacterial Confusion: For over 30 years after the 1918 pandemic, scientists believed Haemophilus influenzae bacteria caused influenza. The viral nature wasn’t confirmed until 1933, highlighting how recent our understanding of respiratory viruses truly is.
The 1976 Swine Flu Vaccine Debacle: A mass vaccination campaign in the U.S. was launched after fears of a 1918-like pandemic. The pandemic never materialized, but the vaccine was associated with increased cases of Guillain-Barré syndrome, leading to public mistrust that persists today.
Surprising Scientific Facts
Virus Survival Outside the Body: Influenza virus can survive on hard surfaces for 24-48 hours, on tissues for 15 minutes, and on hands for only 5 minutes, yet hand-to-face transmission remains a major route of infection.
The Role of Humidity: Low indoor humidity (<40%) increases influenza transmission rates by up to 3-fold. This explains why heated indoor environments during winter create perfect conditions for seasonal outbreaks.
Pregnant Women’s Unique Risk: Pregnancy creates a perfect storm for severe influenza: altered immune system, increased oxygen demands, and mechanical changes from the growing fetus that compromise lung function, particularly in the 2nd and 3rd trimesters.
Myths vs. Medical Facts
Myth: “You can catch flu from the vaccine” Fact: Inactivated flu vaccines cannot cause influenza illness. The nasal spray vaccine contains weakened viruses that cannot cause flu in healthy people. Mild reactions are immune responses, not infections.
Myth: “Natural immunity is better than vaccine protection” Fact: While natural infection may provide broader immunity, the risks far outweigh benefits. Natural infection can cause severe complications and death, while vaccines provide safer protection with minimal risk.
Myth: “Healthy people don’t need flu vaccines” Fact: Even healthy individuals can develop severe complications. Vaccination protects both the individual and the community through herd immunity, particularly protecting those who cannot be vaccinated.
Myth: “Antibiotics can treat the flu” Fact: Antibiotics only treat bacterial infections, not viral infections like influenza. Unnecessary antibiotic use contributes to antimicrobial resistance. Only antivirals can directly treat influenza.
Fascinating Biological Insights
The 8-Segment Shuffle: Influenza’s 8-segment RNA genome allows for “reassortment” when two different viruses infect the same cell, creating entirely new pandemic strains. This is how the 2009 H1N1 pandemic emerged.
Antigenic Sin: First exposure to influenza shapes lifelong immune responses through “imprinting.” People tend to have stronger protection against strains similar to their first infection, a phenomenon discovered in the 1960s.
The Cytokine Storm: The 1918 pandemic’s high mortality in healthy young adults was partly due to their robust immune systems creating deadly “cytokine storms”—excessive inflammatory responses that damaged lung tissue.
Impact on Specific Populations
Professional Athletes: Elite athletes may be at higher risk during intense training periods due to temporary immune suppression. The 2014 Sochi Olympics saw multiple influenza outbreaks among athletes.
Military Significance: Influenza has altered military history. The 1918 pandemic affected troop movements in WWI, and military populations remain high-risk due to crowded living conditions and global deployment.
Indigenous Populations: Isolated populations with no previous influenza exposure suffered devastating mortality rates during the 1918 pandemic, with some Arctic communities losing 85% of their population.
Modern Technology Intersections
AI and Drug Discovery: Artificial intelligence is now being used to predict viral evolution, design universal vaccines, and identify new antiviral compounds, potentially revolutionizing influenza prevention and treatment.
Social Media Surveillance: Public health agencies monitor social media posts to track influenza-like illness reports in real-time, providing earlier outbreak detection than traditional surveillance methods.
Climate Change Connections: Global warming may be altering influenza patterns, potentially extending seasons, changing geographic distribution, and affecting animal reservoirs that serve as sources for new pandemic strains.
Unusual Treatment History
Bloodletting and Mercury: Before modern medicine, influenza treatments included bloodletting, mercury compounds, and opium. These treatments often caused more harm than the disease itself.
Aspirin Toxicity in 1918: Many deaths during the 1918 pandemic may have been caused by aspirin poisoning. The newly available drug was given in extremely high doses (up to 30 grams daily), causing pulmonary edema.
Whiskey Prescriptions: During Prohibition in the United States, doctors could legally prescribe whiskey for influenza treatment, leading to a boom in “medicinal alcohol” prescriptions during flu seasons.
Economic and Social Curiosities
The $11 Billion Question: Annual U.S. productivity losses from influenza exceed direct healthcare costs, with businesses losing billions in sick days, reduced productivity, and workplace disruption.
School Closure Effectiveness: Closing schools during influenza outbreaks can reduce community transmission by 25-50%, but the economic impact on working parents often exceeds the public health benefits.
Vaccine Manufacturing Race: Each year’s vaccine production is essentially a global race against time, with strain selection occurring 6-8 months before the season, requiring predictions of viral evolution.
Future Fascinating Possibilities
Intranasal Universal Vaccines: Future vaccines delivered through nasal spray may provide better mucosal immunity and longer-lasting protection, potentially revolutionizing influenza prevention.
Seasonal Hibernation Patterns: Researchers are investigating whether influenza viruses have complex environmental reservoirs that could explain their mysterious summer survival and autumn emergence patterns.
Personalized Antiviral Selection: Future medicine may use rapid genetic testing to select the most effective antiviral for individual patients based on their genetic makeup and the viral strain’s characteristics.
Conclusion
Influenza virus remains one of humanity’s most persistent and adaptable adversaries. Despite over a century of research, seasonal epidemics continue to cause substantial morbidity and mortality globally, while the threat of pandemic emergence persists. The comprehensive understanding detailed in this report demonstrates both how much we have learned and how much remains unknown.
Recent advances in antiviral treatments, particularly the introduction of baloxavir marboxil, and improvements in vaccine technology offer hope for better disease management. However, the ultimate goal of a universal influenza vaccine remains elusive, requiring continued investment in research and international cooperation.
The COVID-19 pandemic has highlighted both the importance of respiratory virus preparedness and the power of rapid vaccine development. These lessons, combined with advancing technologies in diagnostics, surveillance, and treatment, position us better than ever to face future influenza challenges.
Success in controlling influenza will require continued vigilance in surveillance, sustained investment in research, effective public health policies, and most importantly, public trust and participation in prevention measures. The story of influenza is far from over, but our capacity to write its next chapters has never been stronger.
