
⚠️ Disclaimer: The information provided in this article is for educational purposes only and does not constitute medical advice. RevisionTown does not provide diagnosis, treatment, or medical recommendations. Always consult a qualified healthcare professional regarding any medical condition, symptoms, or concerns.
Read More – 🏥 Medical Disclaimer
What is high LDL cholesterol?
High LDL (low-density lipoprotein) cholesterol, often termed “bad cholesterol,” refers to elevated levels of LDL particles in the bloodstream beyond what is considered healthy. LDL cholesterol is one of several lipoproteins that transport cholesterol through the bloodstream. While cholesterol itself is essential for normal body functions—building cells, producing hormones, and aiding digestion—too much LDL cholesterol can lead to serious health complications.
LDL cholesterol becomes problematic when levels exceed recommended thresholds. For most adults, an LDL level below 100 mg/dL is considered optimal, while levels above 160 mg/dL are classified as high. However, target levels vary based on individual risk factors for cardiovascular disease.
Affected body parts/organs
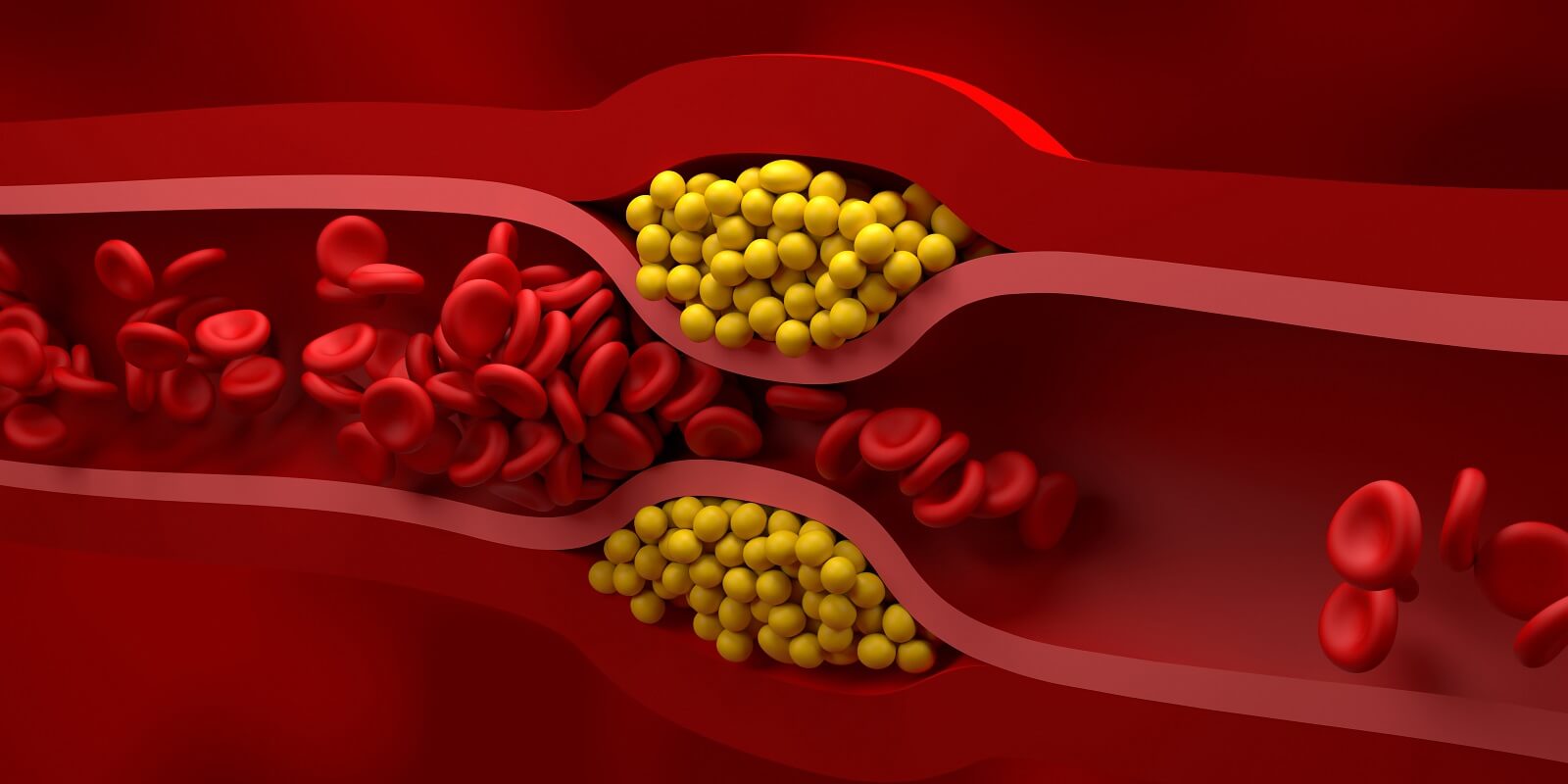
When LDL cholesterol levels are elevated, the primary affected systems are the cardiovascular and circulatory systems. Excess LDL cholesterol can accumulate in artery walls, forming plaque deposits in a process called atherosclerosis. This narrowing and hardening of arteries affects:
- Coronary arteries: Leading to coronary artery disease and potential heart attacks
- Cerebral arteries: Increasing risk of stroke
- Peripheral arteries: Causing peripheral artery disease, particularly in the legs
- Renal arteries: Potentially contributing to kidney disease
- Carotid arteries: Leading to carotid artery disease and heightened stroke risk
Prevalence and significance
High LDL cholesterol represents one of the most prevalent modifiable risk factors for cardiovascular disease worldwide. According to recent global data, approximately 4.4 million deaths per year are attributed to high LDL cholesterol, making it a significant public health concern.
In the United States, the CDC reports that approximately 11.3% of adults had high total cholesterol based on data from August 2021 to August 2023. Though awareness and treatment have improved over recent decades, hypercholesterolemia remains the most common yet poorly managed cardiovascular risk factor globally, with up to 75% of patients not reaching their target cholesterol levels.
The significance of high LDL cholesterol extends beyond its prevalence—it represents a modifiable risk factor that, when properly managed, can substantially reduce the risk of heart disease and stroke, the leading causes of death globally.
2. History & Discoveries
First identification of high LDL cholesterol
The history of cholesterol research begins in 1769 when François Poulletier de La Salle first identified solid cholesterol in gallstones. However, the connection between cholesterol and cardiovascular disease wasn’t established until much later. In 1913, Russian pathologist Nikolai Anichkov demonstrated that feeding rabbits with cholesterol caused atherosclerosis, laying the groundwork for what would later be called the “Lipid Hypothesis”—the concept that high blood cholesterol contributes to atherosclerosis and cardiovascular disease.
The differentiation between different types of cholesterol came decades later. In the 1950s and 1960s, physiologists identified the two major cholesterol-carrying lipoproteins: low-density lipoprotein (LDL) and high-density lipoprotein (HDL). This discovery was pivotal in understanding how cholesterol is transported through the bloodstream and how different lipoproteins affect cardiovascular health.
Key discoveries and breakthroughs
Several milestone discoveries have shaped our understanding of LDL cholesterol:
1929: The discovery of lipoproteins, the carriers of cholesterol in the bloodstream
1950s: John Gofman from Berkeley identified the spectrum of lipoproteins and their association with cardiovascular disease risk. His team classified lipoproteins based on their Svedberg flotation rates, establishing the foundation for modern lipoprotein classification (VLDL, IDL, LDL, and HDL)
1955: Doctors Richard Havel, Howard Eder, and Carl Bragdon developed the ultracentrifugation technique to isolate plasma lipoproteins
1972-1985: Michael Brown and Joseph Goldstein discovered the LDL receptor and how it regulates cholesterol metabolism. This groundbreaking research earned them the Nobel Prize in Physiology or Medicine in 1985
1973: Joe Goldstein, one of the founders of modern cholesterol research, genetically classified the types of cholesterol-carrying lipoproteins in the blood
1974: Goldstein and Brown identified the mechanism behind the inability to remove LDL in patients with familial hypercholesterolemia
1976: Japanese biochemist Akira Endo isolated HMG-CoA reductase inhibitor (later known as statins) from the fungal strain Penicillium Citrinum, leading to the first statin drug
1984: The Lipid Research Clinics Coronary Primary Prevention Trial provided the first robust evidence that lowering cholesterol levels could reduce coronary heart disease events
1994: The Scandinavian Simvastatin Survival Study (4S) demonstrated for the first time that statins reduced all-cause mortality
2003: Nabil Seidah discovered PCSK9, a protein that became the target for a new class of cholesterol-lowering drugs
2015: FDA approval of the first PCSK9 inhibitors (alirocumab and evolocumab), representing a significant advance in cholesterol management
Evolution of medical understanding
The understanding of LDL cholesterol and its role in cardiovascular disease has evolved considerably over time:
Early 20th Century: Cholesterol was identified in atherosclerotic plaques, suggesting its role in heart disease
Mid-20th Century: The distinction between “good” (HDL) and “bad” (LDL) cholesterol became clearer as researchers studied their different effects on cardiovascular health
1970s-1980s: The “cholesterol controversy” peaked as scientists debated whether high cholesterol truly caused heart disease and whether lowering it would provide benefits
1990s-2000s: Large clinical trials conclusively demonstrated that lowering LDL cholesterol, particularly with statins, reduced cardiovascular events and mortality
2000s-Present: Understanding has shifted toward a more nuanced view that considers not just total cholesterol but specific lipoprotein particles, their size, number, and functionality. The focus has expanded beyond LDL to include triglyceride-rich lipoproteins and lipoprotein(a)
Today’s understanding incorporates the concept that LDL cholesterol has a causal, cumulative effect on cardiovascular risk. Modern guidelines emphasize earlier intervention to prevent long-term exposure to elevated LDL levels and recognize the importance of personalized approaches to cholesterol management based on individual risk factors.
3. Symptoms
High LDL cholesterol itself typically doesn’t cause noticeable symptoms, which is why it’s often referred to as a “silent killer.” Most people discover they have high cholesterol only through blood tests. However, the complications that result from prolonged high LDL cholesterol can eventually produce symptoms.
Early symptoms
In the early stages of high LDL cholesterol:
- Typically asymptomatic: No noticeable symptoms directly attributable to high LDL levels
- Occasional yellowish deposits (xanthomas) may appear around the eyes or over tendons in individuals with very high cholesterol levels, particularly those with familial hypercholesterolemia
- Corneal arcus: A white or gray ring around the cornea of the eye may appear in younger adults with high cholesterol
Advanced-stage symptoms
As atherosclerosis progresses due to high LDL cholesterol, symptoms may develop related to the affected organs:
Coronary artery disease symptoms:
- Chest pain or angina
- Shortness of breath
- Fatigue during physical activity
- Heart palpitations
Carotid or cerebral artery disease symptoms:
- Transient ischemic attacks (mini-strokes)
- Stroke symptoms (weakness, numbness, speech difficulties)
- Memory problems or cognitive changes
Peripheral artery disease symptoms:
- Leg pain during walking (claudication)
- Numbness or weakness in the legs
- Poor wound healing in the extremities
- Cooler temperature in affected limbs
Symptom progression
The progression of symptoms related to high LDL cholesterol typically follows this pattern:
- Asymptomatic phase: Can last for decades as plaque slowly builds up
- Early vascular changes: Reduced blood flow that may cause subtle symptoms during exertion
- Significant blockage: More pronounced symptoms with less exertion
- Critical stenosis or rupture: Acute events such as heart attack or stroke
The insidious nature of high LDL cholesterol underscores the importance of regular cholesterol screening, as recommended by healthcare guidelines, particularly for those with family history, other cardiovascular risk factors, or starting at age 20 for general population screening.
4. Causes
Biological causes
Several biological mechanisms contribute to high LDL cholesterol:
Hepatic overproduction: The liver may produce excessive amounts of very low-density lipoprotein (VLDL), which eventually converts to LDL
Impaired LDL clearance: Reduced function or number of LDL receptors on liver cells can decrease the removal of LDL from circulation
Genetic mutations: Various genetic variants affect cholesterol metabolism, transport, and clearance
Hormonal influences: Changes in hormones, particularly thyroid hormones and estrogen, can affect LDL levels
Genetic and hereditary factors
Genetic factors play a significant role in determining LDL cholesterol levels:
Familial Hypercholesterolemia (FH): An inherited disorder that impairs the body’s ability to remove LDL cholesterol from the blood. It affects approximately 1 in 250 people worldwide, with 90% remaining undiagnosed. FH is caused by mutations in genes related to the LDL receptor (LDLR), apolipoprotein B (APOB), or proprotein convertase subtilisin/kexin type 9 (PCSK9)
Polygenic hypercholesterolemia: More common than FH, this condition results from the combined effect of multiple genetic variants that each have a small impact on cholesterol levels
Heritability: Research suggests that genetic factors account for approximately 40-60% of the variability in blood cholesterol levels between individuals
Environmental causes and triggers
Environmental and lifestyle factors significantly influence LDL cholesterol levels:
Diet: Consumption of foods high in saturated fats, trans fats, and cholesterol can raise LDL levels. These include:
- Red and processed meats
- Full-fat dairy products
- Fried foods
- Baked goods with trans fats
- Fast food
Physical inactivity: Sedentary lifestyle reduces HDL cholesterol and may indirectly increase LDL levels
Obesity: Excess body weight, particularly abdominal obesity, contributes to higher LDL cholesterol and triglyceride levels
Smoking: Tobacco use damages blood vessels, making them more likely to accumulate fatty deposits, and lowers HDL cholesterol
Alcohol consumption: Excessive alcohol intake can increase triglycerides and total cholesterol levels
Stress: Chronic stress may indirectly affect cholesterol levels through behavioral changes and physiological responses
Understanding these varied causes is essential for developing personalized prevention and treatment strategies, as addressing the specific underlying factors can lead to more effective management of high LDL cholesterol.
5. Risk Factors
Demographic factors
Various demographic factors influence the risk of developing high LDL cholesterol:
Age: LDL cholesterol levels typically rise with age. Men often see increases between ages 20-50, while women frequently experience rising levels after menopause
Sex: Before menopause, women generally have lower LDL levels than men of the same age. After menopause, women’s LDL levels tend to rise, eventually matching or exceeding those of their male counterparts
Race and ethnicity: Different racial and ethnic groups show varying patterns of cholesterol levels:
- African Americans typically have higher HDL and LDL cholesterol levels than white Americans
- Asian Americans are more likely to have higher LDL levels than other groups
- Hispanic populations often show distinctive patterns of dyslipidemia, with higher triglycerides and lower HDL
Lifestyle risk factors
Several modifiable lifestyle factors significantly influence LDL cholesterol levels:
Diet: Consuming foods high in saturated fats, trans fats, and cholesterol increases LDL levels
Physical inactivity: Sedentary lifestyle contributes to lower HDL and potentially higher LDL levels
Obesity: Body mass index (BMI) over 30 and especially abdominal obesity correlates with higher LDL cholesterol
Smoking: Tobacco use damages blood vessels and lowers HDL cholesterol
Alcohol consumption: Excessive alcohol intake can increase triglycerides and total cholesterol
Stress: Chronic psychological stress may contribute to higher cholesterol levels through various physiological mechanisms
Medical conditions affecting LDL levels
Several medical conditions can lead to or exacerbate high LDL cholesterol:
Diabetes mellitus: Both Type 1 and Type 2 diabetes alter lipid metabolism, often leading to higher LDL levels and increased risk of atherosclerosis
Hypothyroidism: Reduced thyroid function slows metabolism, including the breakdown of LDL cholesterol
Chronic kidney disease: CKD causes more rapid plaque buildup and dysfunctional lipid metabolism
Liver diseases: Conditions affecting liver function can impair cholesterol processing
Polycystic ovary syndrome (PCOS): Women with PCOS often have higher LDL and lower HDL levels
Lupus: Systemic lupus erythematosus is associated with higher levels of “bad cholesterol” and chronic inflammation
HIV/AIDS: Both the infection itself and some antiretroviral medications can raise cholesterol levels
Medication-related risk factors
Certain medications can adversely affect LDL cholesterol levels:
Corticosteroids: Prednisone and similar medications can raise LDL levels
Some diuretics: Certain water pills used for blood pressure can increase LDL
Retinoids: Used for skin conditions like acne
Some antiretroviral drugs: Particularly older HIV medications
Beta-blockers: Some types may raise triglycerides and lower HDL
Progestins: Found in some hormonal contraceptives
Anabolic steroids: Used illicitly or for specific medical conditions
Understanding these risk factors helps in identifying individuals who may benefit from earlier or more aggressive cholesterol screening and intervention strategies.
6. Complications
Cardiovascular complications
The most serious complications of high LDL cholesterol involve the cardiovascular system:
Atherosclerosis: The fundamental pathological process where LDL cholesterol deposits in artery walls form plaques that narrow and harden the arteries
Coronary Artery Disease (CAD): Atherosclerosis in the coronary arteries reduces blood flow to the heart muscle, potentially leading to:
- Angina (chest pain)
- Myocardial infarction (heart attack)
- Heart failure
- Arrhythmias
Cerebrovascular Disease: Affects the blood vessels supplying the brain, resulting in:
- Transient ischemic attacks (TIAs or “mini-strokes”)
- Ischemic stroke
- Vascular dementia
Peripheral Artery Disease (PAD): Narrowing of arteries in the limbs, most commonly the legs, causing:
- Claudication (leg pain during walking)
- Critical limb ischemia
- Increased risk of infections and poor wound healing
- In severe cases, gangrene and amputation
Organ-specific complications
High LDL cholesterol can affect multiple organ systems beyond the heart and brain:
Kidney damage: Atherosclerosis in renal arteries can lead to reduced kidney function and renovascular hypertension
Eye problems: Cholesterol deposits can form in the eyes (arcus senilis), and atherosclerosis can affect retinal vessels
Digestive system: Reduced blood flow to intestines can cause mesenteric ischemia
Skin manifestations: Xanthomas (cholesterol deposits under the skin, especially around tendons) and xanthelasmas (yellowish cholesterol deposits around the eyes) can develop with severely elevated cholesterol
Long-term health impact
The cumulative impact of high LDL cholesterol on health includes:
Reduced life expectancy: High LDL cholesterol significantly increases mortality risk, particularly from cardiovascular causes
Disability: Cardiovascular events often lead to long-term disability, reduced mobility, and diminished quality of life
Cognitive decline: Cerebrovascular disease contributes to cognitive impairment and vascular dementia
Metabolic consequences: High LDL often clusters with other metabolic abnormalities (hypertension, insulin resistance, obesity) in what’s known as metabolic syndrome, compounding health risks
Fatality rates
The contribution of high LDL cholesterol to mortality is substantial:
- Globally, about 4.4 million deaths per year are attributed to high LDL cholesterol
- Approximately 2/3 of all cardiovascular disease deaths are linked to atherosclerotic cardiovascular disease
- Individuals with untreated familial hypercholesterolemia face a dramatically increased risk, with 50% of men experiencing fatal coronary events by age 60 and 30% of women by age 60
The good news is that these complications are largely preventable with appropriate cholesterol management. Each 38.7 mg/dL (1 mmol/L) reduction in LDL cholesterol is associated with approximately a 21% reduction in major cardiovascular events.
7. Diagnosis & Testing
Standard diagnostic procedures
Diagnosing high LDL cholesterol primarily relies on blood tests. The standard diagnostic approach includes:
Lipid Profile: A comprehensive blood test that measures various lipid components:
- Total cholesterol
- LDL cholesterol
- HDL cholesterol
- Triglycerides
- Non-HDL cholesterol (calculated as total cholesterol minus HDL)
Fasting vs. Non-fasting: Traditionally, lipid profiles were performed after a 9-12 hour fast. However, current guidelines recognize that non-fasting lipid profiles are acceptable for initial screening, as LDL and total cholesterol vary only minimally with food intake. Fasting tests may still be preferred when triglycerides need to be precisely measured
Direct vs. Calculated LDL: While LDL can be directly measured, it’s often calculated using the Friedewald formula:
- LDL = Total Cholesterol – HDL – (Triglycerides/5)
- This formula becomes less accurate when triglycerides exceed 400 mg/dL
- Newer calculations like the Martin-Hopkins or Sampson-NIH formulas may provide better accuracy, especially with high triglycerides or low LDL levels
Specialized tests
Beyond standard lipid profiles, specialized tests can provide additional insights:
Advanced Lipoprotein Testing:
- LDL particle number (LDL-P)
- LDL particle size
- Apolipoprotein B (ApoB) levels, which reflect the total number of atherogenic particles
- Lipoprotein(a) [Lp(a)] measurement, a specialized form of LDL that significantly increases cardiovascular risk
Genetic Testing:
- DNA testing for familial hypercholesterolemia (FH) and other genetic dyslipidemias
- Tests may identify mutations in genes like LDLR, APOB, PCSK9, and others
Imaging Studies:
- Coronary calcium scoring to detect calcified atherosclerotic plaque
- Carotid ultrasound to assess plaque buildup in neck arteries
- Advanced imaging techniques like coronary CT angiography to visualize coronary arteries
Screening recommendations
Current guidelines for cholesterol screening vary slightly between organizations but generally recommend:
Initial Screening:
- Children: First test between ages 9-11, with earlier testing for those with family history of high cholesterol or premature heart disease
- Young adults (20-39 years): Every 5 years if no risk factors
- Adults 40-75 years: Every 1-5 years, depending on risk factors
More Frequent Monitoring:
- Individuals with established cardiovascular disease
- Those with diabetes
- People with familial hypercholesterolemia
- Individuals on cholesterol-lowering medications
- Anyone with other significant cardiovascular risk factors
Risk-Based Assessment:
- Modern approaches integrate LDL cholesterol values with other risk factors to calculate 10-year cardiovascular risk
- Tools like the ASCVD Risk Calculator help determine who might benefit most from intervention
Diagnostic thresholds
The interpretation of cholesterol levels has evolved toward a more personalized, risk-based approach, but general categories include:
LDL Cholesterol Levels:
- Optimal: Less than 100 mg/dL (2.6 mmol/L)
- Near optimal: 100-129 mg/dL (2.6-3.3 mmol/L)
- Borderline high: 130-159 mg/dL (3.4-4.1 mmol/L)
- High: 160-189 mg/dL (4.1-4.9 mmol/L)
- Very high: 190 mg/dL (4.9 mmol/L) or above
Target Levels based on risk:
- Very high-risk patients (established ASCVD, diabetes with target organ damage): <55 mg/dL (1.4 mmol/L)
- High-risk patients: <70 mg/dL (1.8 mmol/L)
- Moderate-risk patients: <100 mg/dL (2.6 mmol/L)
- Low-risk patients: <116 mg/dL (3.0 mmol/L)
Early and accurate diagnosis of high LDL cholesterol is critical for timely intervention to prevent the development of cardiovascular complications.
8. Treatment Options
Lifestyle modifications
Lifestyle changes form the foundation of cholesterol management for all patients:
Dietary Approach:
- Mediterranean diet or DASH (Dietary Approaches to Stop Hypertension) eating pattern
- Reduction of saturated fats to <7% of daily calories
- Elimination of trans fats
- Increased consumption of soluble fiber (10-25g/day)
- Inclusion of plant sterols/stanols (2g/day)
- Emphasis on fruits, vegetables, whole grains, legumes, and lean proteins
Physical Activity:
- 150+ minutes of moderate-intensity aerobic exercise weekly
- Muscle-strengthening activities at least 2 days per week
- Regular physical activity can increase HDL and improve LDL particle size
Weight Management:
- Even modest weight loss (5-10% of body weight) can significantly improve lipid profiles
- Maintaining a healthy BMI (18.5-24.9) is optimal for cholesterol management
Smoking Cessation:
- Quitting smoking improves HDL levels and reduces overall cardiovascular risk
Alcohol Moderation:
- Limiting alcohol to moderate levels (≤1 drink daily for women, ≤2 for men)
Pharmacological treatments
Several medication classes are used to treat high LDL cholesterol:
Statins (HMG-CoA Reductase Inhibitors):
- First-line therapy for most patients with elevated LDL
- Lower LDL by 20-60% depending on intensity
- Examples: atorvastatin, rosuvastatin, simvastatin, pravastatin
- Side effects may include muscle pain, liver enzyme elevation, and slightly increased diabetes risk
Ezetimibe:
- Blocks intestinal cholesterol absorption
- Lowers LDL by approximately 15-20%
- Often used in combination with statins
- Generally well-tolerated with minimal side effects
PCSK9 Inhibitors:
- Monoclonal antibodies that enhance LDL receptor recycling
- Can lower LDL by 50-70%
- Examples: evolocumab, alirocumab
- Administered by subcutaneous injection every 2-4 weeks
- High cost limits widespread use
Bempedoic Acid:
- Newer agent that inhibits cholesterol synthesis earlier in the pathway than statins
- Lowers LDL by approximately 15-25%
- May be useful for statin-intolerant patients
- Associated with fewer muscle-related side effects than statins
Bile Acid Sequestrants:
- Bind bile acids in the intestine, promoting LDL clearance
- Lower LDL by 15-30%
- Examples: cholestyramine, colesevelam
- Gastrointestinal side effects limit tolerability
Fibrates:
- Primarily reduce triglycerides but may modestly affect LDL
- Examples: fenofibrate, gemfibrozil
- Used mainly for mixed dyslipidemia
Niacin (Nicotinic Acid):
- Less commonly used due to side effects and limited evidence for cardiovascular benefit
- Can lower LDL by 10-20% at high doses
Emerging treatments
Several innovative approaches are in development or early clinical use:
Inclisiran:
- Small interfering RNA that inhibits PCSK9 production
- Requires only twice-yearly injections
- Provides sustained LDL reduction of approximately 50%
Evinacumab:
- Monoclonal antibody that inhibits angiopoietin-like protein 3 (ANGPTL3)
- Particularly effective for homozygous familial hypercholesterolemia
- Can reduce LDL by 30-50% in challenging cases
Gene Therapy:
- Approaches targeting genes involved in cholesterol metabolism
- Shows promise particularly for genetic dyslipidemias
RNA-based Therapies:
- Multiple agents targeting apolipoprotein B and other key proteins in development
Treatment protocols
Current treatment guidelines follow a risk-stratified approach:
Very High Risk (established ASCVD, FH with ASCVD, or diabetes with target organ damage):
- High-intensity statin therapy
- Target LDL reduction ≥50% from baseline
- Target LDL <55 mg/dL (<1.4 mmol/L)
- Consider combination therapy with ezetimibe and/or PCSK9 inhibitors if targets not achieved
High Risk (significant risk factors or FH without ASCVD):
- High-intensity statin therapy
- Target LDL reduction ≥50% from baseline
- Target LDL <70 mg/dL (<1.8 mmol/L)
- Consider adding non-statin therapies if needed
Moderate Risk:
- Moderate-intensity statin therapy
- Target LDL <100 mg/dL (<2.6 mmol/L)
Low Risk:
- Lifestyle modification
- Consider statin therapy if LDL persistently elevated despite lifestyle changes
Treatment decisions should always involve shared decision-making between patient and provider, considering individual preferences, tolerability, and overall health status.
9. Prevention & Precautionary Measures
Primary prevention strategies
Primary prevention focuses on preventing high LDL cholesterol before it develops:
Dietary Approach:
- Adopt a heart-healthy diet from early in life
- Emphasize fruits, vegetables, whole grains, legumes, and lean proteins
- Limit saturated fats to <7% of daily calories
- Avoid trans fats
- Consume foods rich in soluble fiber (oats, barley, legumes, fruits)
- Include plant sterols/stanols found in vegetable oils, nuts, seeds, and fortified foods
Regular Physical Activity:
- Establish exercise habits early in life
- Aim for at least 150 minutes of moderate-intensity activity weekly
- Include resistance training 2-3 times per week
- Reduce sedentary time throughout the day
Weight Management:
- Maintain a healthy body weight
- Focus on sustainable eating patterns rather than restrictive diets
- Address overweight/obesity early before metabolic complications develop
Avoid Tobacco Products:
- Never start smoking
- Avoid exposure to secondhand smoke
- Be aware that all forms of tobacco (including vaping) can negatively impact lipid profiles
Lifestyle modifications for prevention
Specific lifestyle changes that can help prevent high LDL cholesterol:
Specific Dietary Recommendations:
- Increase consumption of omega-3 fatty acids from sources like fatty fish, flaxseeds, and walnuts
- Use olive oil or canola oil as primary cooking oils
- Choose lean protein sources
- Limit processed foods and added sugars
- Consider plant-based eating patterns, which naturally reduce saturated fat intake
Stress Management:
- Practice regular stress-reduction techniques (meditation, yoga, deep breathing)
- Ensure adequate sleep (7-9 hours for adults)
- Maintain social connections and emotional well-being
Alcohol Consumption:
- If you drink alcohol, do so in moderation
- Limit to 1 drink daily for women and 2 for men at maximum
Regular Monitoring:
- Know your cholesterol numbers from early adulthood
- Track changes over time
- Identify trends before they become problematic
Preventive screening
Early detection through appropriate screening is essential:
General Population Screening:
- First screening between ages 9-11 years
- Repeat screening between ages 17-21
- Adults without risk factors: every 4-6 years
- Adults with risk factors: more frequent testing as recommended by healthcare provider
Enhanced Screening for High-Risk Individuals:
- Children with family history of high cholesterol or premature heart disease: screening as early as age 2
- Individuals with family history of familial hypercholesterolemia: early and more frequent screening
- Those with multiple cardiovascular risk factors: more frequent monitoring
- People with conditions that raise cardiovascular risk (diabetes, hypertension): annual lipid profiles
Public health approaches
Broader societal strategies can help prevent high LDL cholesterol:
Policy Measures:
- Regulations limiting trans fats in food supply
- Clear nutrition labeling requirements
- Public health campaigns raising awareness about cholesterol
- School-based nutrition and physical activity programs
Healthcare System Strategies:
- Integration of lipid screening into routine preventive care
- Implementation of guideline-based risk assessment tools
- Support for lifestyle modification programs
- Improved access to preventive care
Environmental Interventions:
- Creating walkable communities that encourage physical activity
- Increasing access to affordable healthy foods
- Workplace wellness programs
- Community-based heart health initiatives
Prevention of high LDL cholesterol requires a multi-faceted approach spanning individual, healthcare, and societal levels. The benefits extend beyond cholesterol management to overall cardiovascular and metabolic health.
10. Global & Regional Statistics
Global prevalence
High LDL cholesterol represents a significant global health challenge:
According to Global Burden of Disease data, high LDL cholesterol was responsible for approximately 4.4 million deaths worldwide in 2019, an increase from 3.0 million in 1990
The global prevalence of high total cholesterol (≥5.0 mmol/L or ≥190 mg/dL) was estimated at approximately 40% in adults by the World Health Organization
The total burden attributed to high LDL cholesterol is approximately 94.92 million disability-adjusted life years (DALYs) globally
Hypercholesterolemia remains the most common and poorly monitored cardiovascular risk factor, with estimates suggesting up to 75% of patients worldwide do not reach their target LDL levels
Regional variations
Significant geographic differences exist in cholesterol levels and related disease burden:
High-income Western countries: Have experienced decreasing levels of total and non-HDL cholesterol since the 1980s, largely due to improved awareness, screening, and treatment
East and Southeast Asia: Experiencing increasing trends in cholesterol levels, coinciding with rapid economic development and lifestyle changes
Eastern Europe and Central Asia: These regions have seen some of the highest age-standardized death rates attributed to high LDL cholesterol
Sub-Saharan Africa: Generally lower prevalence of high cholesterol but increasing with urbanization and dietary changes
North America: In the United States, approximately 11.3% of adults had high total cholesterol (≥240 mg/dL) during 2021-2023, according to CDC data, with prevalence varying by age, sex, and geographic location
Gender and age disparities
The impact of high LDL cholesterol shows important demographic patterns:
Gender differences:
- Age-standardized death rates from high LDL cholesterol are approximately 1.45 times higher in males compared to females
- Disability-adjusted life years are 1.70 times higher in males
- Interestingly, exposure to high LDL (measured by summary exposure value) is actually 1.10 times higher in females than males, suggesting that while women have higher exposure, men experience worse outcomes
Age patterns:
- LDL cholesterol levels typically increase with age in both sexes
- The burden of disease attributed to high LDL rises dramatically with advancing age
- The highest rates of death, disability, and exposure occur in the oldest age groups (95+ years)
- In the US, the prevalence of high total cholesterol is higher in middle-aged adults (40-59 years) compared to younger adults or those aged 60 and older
Socioeconomic factors
Social and economic determinants significantly influence cholesterol levels globally:
Socio-demographic Index (SDI) correlations:
- Countries with high SDI (socio-demographic index) have experienced declining rates of high cholesterol and related mortality
- Low and middle SDI countries show increasing trends in cholesterol-related disease burden
- This creates a shifting global epicenter of non-optimal cholesterol from high-income to lower and middle-income regions
Urban-rural differences:
- Urban populations typically show higher rates of elevated cholesterol than rural populations
- This pattern is particularly pronounced in rapidly developing economies
Access to healthcare:
- Significant disparities exist in access to cholesterol screening and treatment
- In high-income countries, approximately 60-80% of individuals with high cholesterol are aware of their condition, while awareness rates in low-income countries may be below 10%
These statistics highlight the dynamic nature of the global cholesterol landscape, with concurrent improvement in some regions and deterioration in others, emphasizing the need for tailored public health approaches based on regional needs and resources.
11. Recent Research & Future Prospects
Latest advancements in treatment
Recent years have witnessed significant innovations in LDL cholesterol management:
PCSK9 Inhibitors in Acute Settings: Recent trials like EVACS and EVOPACS demonstrated that administering PCSK9 inhibitors such as evolocumab within 24 hours of acute coronary syndrome significantly reduces LDL cholesterol within days, potentially improving outcomes for high-risk patients
Bempedoic Acid: Approved in 2020, this first-in-class adenosine triphosphate-citrate lyase (ACL) inhibitor provides a new option for statin-intolerant patients, lowering LDL by approximately 30% in monotherapy and showing cardiovascular benefits in recent outcomes trials
Inclisiran: This novel small interfering RNA therapy targets PCSK9 production in the liver, providing sustained LDL reduction with only twice-yearly injections, representing a potential breakthrough for treatment adherence
Fixed-Dose Combinations: The development of single-pill combinations, such as bempedoic acid with ezetimibe, simplifies treatment regimens and may improve adherence
Ongoing studies
Several promising research directions are currently being explored:
ANGPTL3 Inhibition: Evinacumab, which inhibits angiopoietin-like protein 3, shows remarkable efficacy in reducing LDL cholesterol in patients with homozygous familial hypercholesterolemia and is being studied in broader populations
Triglyceride-Rich Lipoprotein Targeting: Increasing focus on therapies that address triglyceride-rich lipoproteins, recognizing their contribution to cardiovascular risk, particularly in patients with diabetes and metabolic syndrome
Lipoprotein(a) Reduction: Novel therapies specifically targeting lipoprotein(a), including antisense oligonucleotides and small interfering RNAs, are in advanced clinical development
Combination Therapy Approaches: Studies are examining optimal combinations and sequences of lipid-lowering therapies to maximize benefit while minimizing side effects
Potential future therapies
Looking forward, several innovative approaches show promise:
Gene Editing Technologies: CRISPR-Cas9 and related technologies are being explored to correct genetic mutations causing familial hypercholesterolemia and other severe lipid disorders
mRNA-Based Therapies: Building on the success of mRNA vaccine platforms, similar approaches are being investigated for sustained production of proteins that lower LDL cholesterol
Selective PPAR Modulators: Next-generation peroxisome proliferator-activated receptor modulators with improved efficacy and safety profiles for managing complex dyslipidemia
Gut Microbiome Interventions: Emerging research suggests that modifying the intestinal microbiota may influence cholesterol metabolism, opening potential new therapeutic avenues
Nanomedicine Approaches: Advanced drug delivery systems using nanoparticles to target atherosclerotic plaques directly
Research trends and directions
Several key themes characterize current cholesterol research:
Earlier Intervention: Increasing evidence supports earlier initiation of lipid-lowering therapy to prevent cumulative exposure to elevated LDL levels, potentially altering the lifetime trajectory of atherosclerotic disease
Precision Medicine: Moving beyond simple LDL targets to personalized approaches based on genetic profiling, lipoprotein subfractions, and individual risk assessment
Inflammation and Cholesterol Interplay: Greater understanding of how inflammation and cholesterol metabolism interact in atherosclerosis development, potentially leading to dual-targeted therapies
Implementation Science: Research focused on improving real-world implementation of existing effective therapies, addressing the significant treatment gaps that persist globally
Technology Integration: Using digital health tools, artificial intelligence, and wearable devices to improve risk assessment, treatment adherence, and outcomes monitoring
The future of LDL cholesterol management appears promising, with multiple complementary approaches aimed at reducing the substantial global burden of atherosclerotic cardiovascular disease. The combination of innovative pharmacological approaches, genetic technologies, and improved implementation of evidence-based strategies offers hope for further reductions in cardiovascular morbidity and mortality.
12. Interesting Facts & Lesser-Known Insights
Surprising cholesterol facts
Some intriguing aspects of LDL cholesterol that aren’t widely known:
Cholesterol’s Essential Roles: Despite its negative reputation, cholesterol is vital for human physiology—it forms cell membranes, serves as the precursor for steroid hormones and vitamin D, and facilitates nerve conduction
Dietary vs. Blood Cholesterol: Only about 20-25% of blood cholesterol comes from diet; the liver produces the majority (approximately 75-80%), which explains why dietary changes alone sometimes have limited impact on blood cholesterol levels
Cholesterol and the Brain: The brain contains about 25% of the body’s total cholesterol despite making up only about 2% of body weight, highlighting cholesterol’s crucial role in neurological function
Nobel Prize Connection: Cholesterol research has been recognized with at least 11 Nobel Prizes, including the 1985 award to Brown and Goldstein for their discovery of the LDL receptor
Statins from Mold: The first statin drug was discovered by Japanese biochemist Akira Endo while searching through thousands of fungi samples, eventually finding a compound in blue-green mold (Penicillium citrinum) that inhibited cholesterol synthesis
Myths and misconceptions
Several common misunderstandings persist about LDL cholesterol:
Myth: All cholesterol is bad Fact: Cholesterol is essential for life, and even LDL serves important physiological functions when in healthy ranges
Myth: Eggs should be avoided completely due to their cholesterol content Fact: Modern research suggests that dietary cholesterol has relatively minor effects on blood cholesterol for most people, and eggs can be part of a heart-healthy diet
Myth: Thin people don’t need to worry about cholesterol Fact: Even individuals with normal weight can have high LDL cholesterol due to genetic factors or poor diet quality
Myth: Children don’t need cholesterol screening Fact: Early screening is recommended for children, especially those with family history of high cholesterol or premature heart disease
Myth: Once you’re on cholesterol medication, lifestyle doesn’t matter Fact: Lifestyle measures remain important even when taking medication, often enhancing medication effects and reducing the dose required
Population-specific insights
Certain populations exhibit unique characteristics related to LDL cholesterol:
The French Paradox: Despite consuming diets relatively high in saturated fats, some regions in France traditionally had lower rates of heart disease, possibly due to other dietary factors (like red wine polyphenols) or lifestyle elements that modify cardiovascular risk
Tsimane People: This indigenous Bolivian population has been found to have the lowest recorded levels of coronary artery disease and remarkably low LDL cholesterol levels, attributed to their highly active lifestyle and unique diet
Familial Hypercholesterolemia Founder Effects: Certain populations, including Afrikaners in South Africa, French Canadians, and Lebanese Christians, have unusually high rates of specific FH mutations due to founder effects in relatively isolated populations
Sex Differences in Response: Women and men may respond differently to certain cholesterol-lowering therapies, with some evidence suggesting that women experience different patterns of benefit and side effects from statins
Unusual research findings
Some counterintuitive or surprising research observations:
Cholesterol Paradox in Heart Failure: Some studies have observed that higher cholesterol levels are associated with better outcomes in established heart failure—a finding that contrasts with cholesterol’s harmful effects in developing heart disease
Statins and Memory: Despite concerns about cognitive effects, large-scale research suggests statins may actually protect against dementia in some populations, highlighting the complex relationship between cholesterol and brain health
Morning vs. Evening Dosing: Some statins work better when taken in the evening because cholesterol synthesis peaks during night hours, while others are equally effective regardless of timing
Coffee’s Complex Effects: Unfiltered coffee (like French press or Turkish coffee) raises LDL cholesterol due to compounds called diterpenes, while filtered coffee doesn’t have this effect because paper filters remove these substances
Cholesterol and Infectious Disease: Some research suggests that LDL particles may play a role in immune defense, binding to and inactivating certain viruses and bacterial toxins—potentially explaining why extremely low cholesterol levels have been associated with increased infection risk in some studies
These fascinating aspects of LDL cholesterol research illustrate the complexity of lipid metabolism and its far-reaching implications for human health beyond the well-established connection to heart disease and stroke.