
⚠️ Disclaimer: The information provided in this article is for educational purposes only and does not constitute medical advice. RevisionTown does not provide diagnosis, treatment, or medical recommendations. Always consult a qualified healthcare professional regarding any medical condition, symptoms, or concerns.
Read More – 🏥 Medical Disclaimer
Comprehensive Report on Strep Throat
1. Overview
What is Strep Throat?
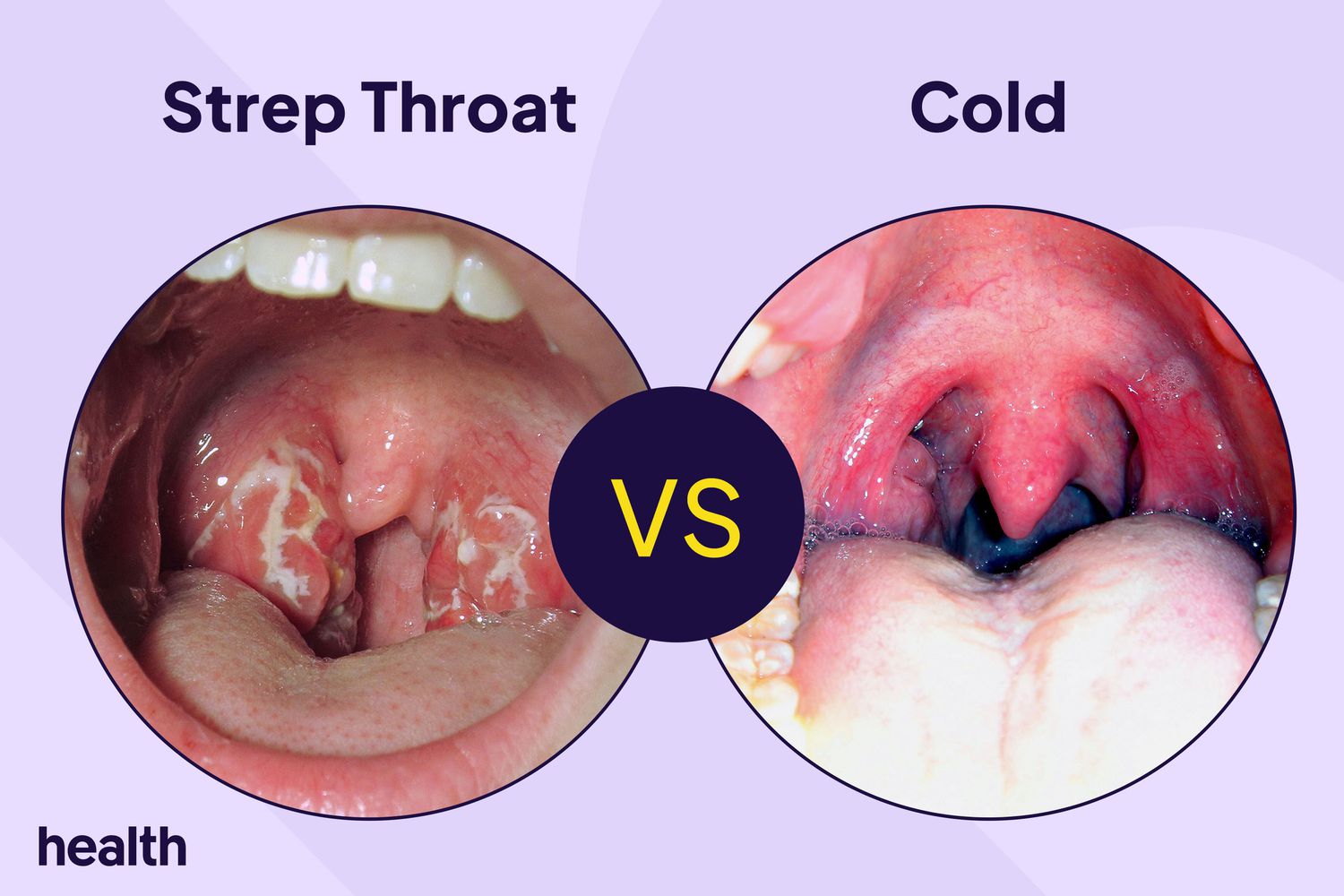
Strep throat (streptococcal pharyngitis) is an acute bacterial infection of the pharynx and tonsils caused by group A Streptococcus bacteria (Streptococcus pyogenes). It is characterized by inflammation of the throat and tonsils, resulting in pain, swelling, and distinctive clinical features that differentiate it from viral throat infections.
Detailed Definition
Strep throat is a bacterial infection that specifically targets the mucous membranes lining the pharynx, tonsils, and occasionally the larynx. Unlike viral pharyngitis, which accounts for the majority of sore throats, streptococcal pharyngitis is clinically significant due to its potential for triggering serious immune-mediated complications if left untreated. The infection develops when the pathogenic bacteria colonize the pharyngeal tissue, triggering an inflammatory response that produces the characteristic symptoms.
Affected Body Parts/Organs
The primary affected areas include:
- Pharynx: The middle part of the throat behind the mouth and nasal cavity
- Tonsils: Particularly the palatine tonsils, which often become enlarged and inflamed
- Lymph nodes: Cervical lymph nodes in the neck commonly become swollen
- Soft palate: May become inflamed and develop small red spots (petechiae)
- Uvula: Often becomes red and swollen
Secondary effects may manifest in other organ systems through immune-mediated processes, particularly in cases of untreated infections leading to complications.
Prevalence and Significance
Strep throat represents a significant global health burden with distinct epidemiological patterns:
Prevalence in children:
- 15-30% of sore throats in children aged 5-15 years
- Peak incidence occurs in late fall, winter, and early spring in temperate climates
- 10-15 million cases annually in the United States alone
Prevalence in adults:
- 5-10% of sore throats in adults
- Lower incidence compared to children due to acquired immunity and fewer exposures
- Approximately 1-3 million adult cases annually in the United States
Global burden:
- Estimated 616 million new cases worldwide annually
- Highest rates in developing countries and resource-limited settings
- Significant contributor to healthcare utilization and antibiotic prescriptions
Medical significance:
- Primary importance lies in preventing suppurative complications (abscesses) and non-suppurative sequelae (rheumatic fever, post-streptococcal glomerulonephritis)
- Responsible for approximately 30-40% of outpatient antibiotic prescriptions for children
- Economic impact through direct healthcare costs and indirect costs (school/work absences)
- Serves as a reservoir for invasive streptococcal disease in communities
Strep throat remains medically significant not merely due to its acute symptoms but primarily because of its potential to trigger serious autoimmune complications, particularly rheumatic fever, which can lead to permanent heart valve damage. This risk, though dramatically reduced in developed countries with access to antibiotics, continues to pose a substantial public health challenge in many parts of the world.
2. History & Discoveries
First Identification
The understanding of strep throat evolved gradually through several key historical developments:
Ancient observations: Clinical descriptions consistent with streptococcal pharyngitis appeared in ancient medical texts, though without understanding of the bacterial cause
1874: The Austrian surgeon Theodor Billroth first described chain-forming bacteria (“streptococci”) in cases of wound infections and erysipelas
1879: Louis Pasteur isolated streptococci from the blood of women with puerperal fever, establishing their role as pathogens
1884: Friedrich Fehleisen cultured streptococci from patients with erysipelas, fulfilling Koch’s postulates by reproducing the disease in human volunteers
1903-1907: The specific connection between streptococcal throat infections and rheumatic fever was first proposed by Ludwig Aschoff and Richard Geipel, who described the characteristic cardiac lesions (Aschoff nodules)
Key Historical Figures
Rebecca Lancefield (1895-1981): American microbiologist whose classification system for streptococci (1933) identified Group A Streptococcus as the primary human pathogen responsible for pharyngitis and other infections. Her serological typing system remains fundamental to understanding streptococcal epidemiology and pathogenesis.
Alvin Coburn: In the 1930s, conducted pivotal studies demonstrating the link between streptococcal pharyngitis and rheumatic fever, establishing the importance of treating strep throat to prevent this serious complication.
Charles H. Rammelkamp: Led studies at Warren Air Force Base in the 1950s that definitively established that penicillin treatment of streptococcal pharyngitis could prevent rheumatic fever, revolutionizing the approach to this common infection.
Edward Jenner: Though primarily known for smallpox vaccination, had earlier described the clinical features of “scarlatina” (scarlet fever, a form of streptococcal infection) in 1789.
Major Breakthroughs
1928-1941: Discovery of penicillin by Alexander Fleming and its subsequent clinical development provided the first effective treatment for streptococcal infections
1933: Rebecca Lancefield’s serological classification system for streptococci, identifying Group A as the major human pathogen
1950s: Rammelkamp’s Warren Air Force Base studies definitively established that penicillin treatment of strep throat prevents rheumatic fever
1930s-1950s: Elucidation of the relationship between streptococcal M proteins and virulence/immunity
1960s: Development of rapid antigen detection tests, allowing for quick diagnosis without waiting for culture results
1990s-2000s: Genomic sequencing of Streptococcus pyogenes, revealing virulence factors and the genetic basis of its pathogenicity
2002: Complete genome of Streptococcus pyogenes published, opening new avenues for understanding pathogenesis and potential vaccine development
Evolution of Medical Understanding
The conceptualization of strep throat has evolved dramatically over time:
Pre-bacteriological era (before 1880s): Throat infections were classified based on clinical appearance without understanding of microbial causes
Early bacteriological era (1880s-1920s): Recognition of streptococci as pathogens, but limited understanding of different species and types
Classification era (1920s-1940s): Lancefield’s work allowed differentiation of streptococcal types and correlation with specific clinical syndromes
Antibiotic era (1940s-1960s):
- Recognition that penicillin could effectively treat strep throat
- Understanding of the critical importance of treatment in preventing rheumatic fever
- Development of protocols for diagnosis and management
Immunological understanding (1960s-1980s):
- Elucidation of the molecular mimicry mechanism behind rheumatic fever
- Better understanding of the immune response to streptococcal antigens
- Recognition of the role of M proteins in virulence and immunity
Molecular era (1980s-present):
- Genomic analysis revealing virulence mechanisms
- Understanding of bacterial toxins and their effects
- Recognition of changing epidemiology and emerging resistance
- Development of more sensitive and specific diagnostic tests
Current understanding:
- Complex interplay between host factors, bacterial virulence, and environmental conditions
- Recognition of the long-term consequences of repeated infections
- Precision in differentiating viral from bacterial pharyngitis
- Population-based approaches to prevention in high-burden settings
This evolution reflects a transition from purely symptomatic recognition to deep molecular and immunological understanding of the pathogen-host interaction, guiding increasingly sophisticated approaches to diagnosis, treatment, and prevention.
3. Symptoms
Early Symptoms
The onset of strep throat is typically abrupt, with symptoms developing rapidly within 1-3 days of exposure to the bacteria. Early manifestations include:
Throat symptoms:
- Severe sore throat (often described as “razor blade” pain)
- Pain when swallowing (odynophagia)
- Redness and swelling of the tonsils and pharynx
- White or yellow patches of pus on the tonsils (exudates)
- Tiny red spots on the soft or hard palate (petechiae)
- Swollen, tender lymph nodes in the neck
Systemic symptoms:
- Sudden onset of high fever (typically 101-104°F/38.3-40°C)
- Headache
- Body aches and general malaise
- Loss of appetite
- Nausea (more common in children)
Distinctive features that help differentiate from viral pharyngitis:
- Absence of cough (typically)
- Absence of rhinorrhea (runny nose)
- Absence of conjunctivitis
- Presence of tonsillar exudates
- Tender anterior cervical lymphadenopathy
Later and Advanced Symptoms
If untreated, symptoms may progress to include:
- Intensification of throat pain, potentially severe enough to limit oral intake
- Persistent or increasing fever
- Development of scarlatiniform rash in some cases (scarlet fever):
- Fine, sandpaper-like red rash beginning on the chest and spreading to the extremities
- “Strawberry tongue” (white coating with red papillae, later becoming bright red)
- Circumoral pallor (paleness around the mouth)
- Pastia’s lines (linear petechiae in skin folds)
- Increased lymph node size and tenderness
- Difficulty opening the mouth (trismus) if peritonsillar inflammation develops
- Voice changes due to inflammation of surrounding structures
Common vs. Rare Symptoms
Common symptoms (present in >50% of cases):
- Sore throat
- Pain on swallowing
- Fever
- Headache
- Tonsillar enlargement and redness
- Tonsillar exudates
- Tender cervical lymph nodes
- Malaise and fatigue
Less common symptoms (10-50% of cases):
- Abdominal pain (particularly in children)
- Nausea or vomiting
- Palatal petechiae
- Body aches
- Loss of appetite
- Scarlatiniform rash (scarlet fever, in 10-20%)
Rare symptoms (<10% of cases):
- Hoarseness
- Cough (typically suggests alternative or concurrent diagnosis)
- Diarrhea
- Anterior neck swelling
- Streptococcal toxic shock syndrome (extremely rare)
Symptom Progression
The typical course of strep throat follows a characteristic pattern:
Day 1-2:
- Abrupt onset of sore throat and fever
- Development of systemic symptoms
- Redness of throat and tonsils becomes apparent
Day 2-4:
- Peak intensity of symptoms
- Development of exudates on tonsils
- Maximal pharyngeal inflammation
- Development of rash in cases of scarlet fever
Day 5-7 (untreated):
- Gradual resolution of fever in uncomplicated cases
- Persistent throat pain and lymphadenopathy
- Potential for local suppurative complications
Day 7-10 (untreated):
- Most symptoms begin to resolve spontaneously
- Risk period for development of peritonsillar abscess
Beyond 10 days (untreated):
- Resolution of acute symptoms in uncomplicated cases
- Risk period for post-streptococcal immune-mediated complications:
- Acute rheumatic fever (1-5 weeks after infection)
- Post-streptococcal glomerulonephritis (1-2 weeks after infection)
With appropriate antibiotic treatment:
- Rapid reduction in fever and systemic symptoms (usually within 24-48 hours)
- Decreased pharyngeal pain (typically within 2-3 days)
- Reduction in contagiousness (after 24 hours of antibiotics)
- Prevention of suppurative and non-suppurative complications
- Complete resolution typically within 5-7 days
The symptom complex and progression provide important diagnostic clues that help differentiate streptococcal pharyngitis from viral infections, which typically have a more gradual onset, milder pharyngeal findings, and prominent upper respiratory symptoms like cough and rhinorrhea.
4. Causes
Biological Causes
Primary Pathogen:
- Streptococcus pyogenes (Group A Streptococcus or GAS) is the causative organism of strep throat
- Gram-positive, beta-hemolytic cocci that form chains when viewed under a microscope
- Possesses a cell wall composed of complex carbohydrates and proteins that contribute to virulence
- Multiple serotypes exist based on M protein differences (>200 identified M types)
Pathogenesis:
- Adhesion: Initial attachment to pharyngeal epithelium via bacterial surface proteins (lipoteichoic acid, fibronectin-binding proteins, M proteins)
- Colonization: Establishment of infection through biofilm formation and evasion of local immune defenses
- Invasion: Penetration of epithelial barriers using enzymes and toxins
- Inflammation: Robust host inflammatory response causing the classic symptoms
- Immune evasion: Various mechanisms allowing persistence despite host defenses
Virulence Factors:
- M protein: Surface protein that inhibits phagocytosis and facilitates adherence
- Capsule: Hyaluronic acid capsule that camouflages the bacteria from the immune system
- Streptolysins O and S: Hemolytic toxins that damage cell membranes
- Streptococcal pyrogenic exotoxins (SPEs): Superantigens that trigger massive immune activation (responsible for scarlet fever rash)
- Streptokinase: Enzyme that dissolves blood clots, promoting bacterial spread
- DNases: Enzymes that break down neutrophil extracellular traps
- Hyaluronidase: Enzyme that degrades connective tissue, facilitating spread
- C5a peptidase: Enzyme that impairs neutrophil recruitment
Transmission and Environmental Causes
Transmission Routes:
- Respiratory droplets: Primary mode of transmission through coughing, sneezing, or talking
- Direct contact: Close physical contact with infected individuals
- Fomites: Less commonly via shared objects (utensils, glasses) but possible
- Foodborne outbreaks: Rare but documented, particularly through improperly handled dairy products or food handlers who are carriers
Environmental Factors Promoting Transmission:
- Crowded settings: Schools, daycare centers, military barracks, and other close-quarter environments
- Seasonal patterns: Highest incidence during late fall, winter, and early spring in temperate climates
- Poor ventilation: Enclosed spaces with limited air circulation increase risk
- Household exposure: Family members have 25-50% risk of acquiring infection from an index case
- Socioeconomic factors: Overcrowded housing and limited access to healthcare increase risk
- Geographic factors: Increased prevalence in cooler, drier climates and during seasonal transitions
Genetic and Hereditary Factors
While strep throat itself is not inherited, several genetic factors influence susceptibility:
Host Genetic Factors:
- HLA associations: Certain Human Leukocyte Antigen (HLA) types, particularly HLA-DR4, are associated with increased susceptibility to streptococcal infections and complications
- B-cell alloantigens: D8/17 and 883 markers correlate with susceptibility to post-streptococcal rheumatic fever
- Mannose-binding lectin (MBL) polymorphisms: Affect innate immune response to GAS
- Toll-like receptor variations: Influence recognition of bacterial components and immune response
- Interleukin gene polymorphisms: Particularly IL-1, IL-6, and TNF-α, affecting inflammatory response
Familial Patterns:
- Shared susceptibility: Family studies show clustering of streptococcal infections
- Heritable immune response patterns: Similar antibody responses and T-cell reactivity patterns within families
- Familial rheumatic fever susceptibility: 2-3 fold increased risk in first-degree relatives
Known Triggers and Exposure Risks
Several factors have been identified that increase the risk of developing strep throat:
Individual Triggers:
- Recent exposure to someone with strep throat (highest risk factor)
- History of previous strep infections (altered immune response)
- Fatigue and stress (compromised immune function)
- Upper respiratory viral infections (impaired local immunity)
- Smoking (altered respiratory epithelium and mucociliary clearance)
Environmental Exposures:
- School or daycare attendance during outbreak periods
- Healthcare settings, particularly during respiratory infection seasons
- Household contacts with young, school-aged children
- Military training facilities and other congregate settings
- Winter sports and activities in enclosed spaces
Carrier States:
- Approximately 10-15% of school-aged children are asymptomatic carriers
- Carriage can persist for months and serve as a reservoir for infection
- Carriers generally pose lower transmission risk than symptomatic individuals
- The distinction between carriage and acute infection affects treatment decisions
The interplay between pathogen virulence factors, host genetic susceptibility, and environmental conditions determines whether exposure to the bacteria results in asymptomatic carriage, mild pharyngitis, or severe infection with complications. Understanding these factors guides preventive strategies and helps identify high-risk populations.
5. Risk Factors
Demographic Risk Factors
Several demographic characteristics influence the risk of developing strep throat:
Age:
- Children 5-15 years: Highest risk group, accounting for 30-40% of all cases
- Peak incidence occurs around ages 7-8
- 15-30% of sore throats in this age group are streptococcal
- Children <3 years: Relatively low risk of classic strep throat
- When infection occurs, often presents atypically
- Only 3-7% of sore throats in this age group are streptococcal
- Adolescents and young adults (15-24 years): Moderate risk
- 10-15% of sore throats in this population are streptococcal
- College students and military recruits show higher rates
- Adults >25 years: Declining risk with age
- 5-10% of sore throats in adults are streptococcal
- Risk continues to decrease with advancing age
- Older adults (>65 years): Very low risk
- <5% of sore throats in this population are streptococcal
- When present, may have atypical presentations
Gender:
- Generally equal distribution between males and females
- Slight female predominance noted in some studies (1.2:1)
- During puberty, girls may have slightly higher rates
Ethnic/Racial Factors:
- No consistent intrinsic racial or ethnic predisposition established
- Indigenous populations in Australia, New Zealand, and North America show higher rates
- Socioeconomic and healthcare access disparities likely explain observed differences
Environmental and Occupational Risk Factors
Environmental Factors:
- Seasonal patterns:
- Highest incidence during late fall, winter, and early spring in temperate climates
- Less pronounced seasonality in tropical regions
- Lowest incidence during summer months
- Geographic considerations:
- Higher rates in regions with distinct cold seasons
- Increased prevalence in areas with higher population density
- Endemic patterns in certain developing regions
Living Conditions:
- Household crowding: Increased risk with greater number of individuals per room
- Socioeconomic status: Higher rates in lower socioeconomic groups
- Urban vs. rural: Generally higher rates in urban settings
- Institutional settings: Increased risk in boarding schools, military barracks, prisons
Occupational Risk Factors:
- Healthcare workers: Particularly those in pediatrics, emergency medicine, and family practice
- Educators: Teachers and daycare workers have increased exposure risk
- Military personnel: Especially during basic training and in barracks settings
- Public-facing service workers: Increased exposure through frequent public contact
Lifestyle Risk Factors
Certain lifestyle factors and behaviors influence susceptibility:
Social Behavior:
- Close interpersonal contact: Hugging, kissing, sharing items
- Group activities: Team sports, choir, band, and other group activities
- Social gathering attendance: Parties, religious services, and other crowded events
Personal Habits:
- Hand hygiene practices: Poor hand washing increases risk
- Smoking: Both active and passive smoking increase susceptibility
- Sleep patterns: Inadequate sleep associated with increased susceptibility
- Stress levels: Chronic stress may impair immune function
Preventive Behaviors:
- Healthcare utilization: Delayed treatment of initial cases increases community spread
- Mask wearing: Reduced during respiratory illness season may increase exposure
- Vaccination status: Pneumococcal and influenza vaccines may reduce bacterial superinfections
Pre-existing Conditions and Genetic Factors
Medical Conditions:
- History of previous strep throat: Indicates either biological susceptibility or environmental exposure patterns
- Recurrent tonsillitis: May indicate predisposition or persistent carriage
- Immunocompromised states:
- HIV/AIDS
- Chemotherapy recipients
- Transplant patients on immunosuppressive therapy
- Primary immunodeficiency disorders
- Chronic medical conditions:
- Diabetes mellitus
- Chronic kidney disease
- Chronic obstructive pulmonary disease
Genetic Factors:
- Family history of rheumatic fever: Suggests genetic susceptibility to both initial infection and complications
- HLA types: Particularly HLA-DR4, associated with increased susceptibility
- Complement deficiencies: Particularly C3 and C4 components
- Mannose-binding lectin deficiency: Impairs innate immune response to streptococci
Anatomical Considerations:
- Tonsillar hypertrophy: Enlarged tonsils provide larger surface area for bacterial colonization
- Chronic adenoid hypertrophy: May serve as reservoir for bacteria
- Palatal abnormalities: Cleft palate repair and other variations may affect local defense mechanisms
Understanding these risk factors helps identify high-risk individuals, guide preventive strategies, and inform diagnostic approaches for different populations. This knowledge is particularly valuable in resource-limited settings where testing cannot be performed for all cases of pharyngitis.
6. Complications
Immediate Complications
Strep throat can lead to several direct complications in the acute phase:
Suppurative (Abscess-Forming) Complications:
Peritonsillar abscess (quinsy):
- Collection of pus between the tonsil capsule and pharyngeal muscles
- Occurs in approximately 1-2% of untreated cases
- Characterized by severe throat pain, difficulty opening mouth (trismus), “hot potato” voice
- Requires drainage and antibiotics; hospitalization may be necessary
Retropharyngeal abscess:
- Infection of the deep space behind the pharynx
- More common in young children
- Presents with neck pain, stiff neck, difficulty swallowing, and respiratory distress
- Medical emergency requiring prompt surgical intervention
Parapharyngeal abscess:
- Infection of the lateral pharyngeal space
- Can lead to jugular vein thrombosis and septicemia if untreated
- Presents with severe neck pain, swelling, and systemic toxicity
- Requires IV antibiotics and often surgical drainage
Sinusitis and otitis media:
- Secondary bacterial spread to sinuses or middle ear
- Complicates approximately 5-10% of strep throat cases
- May require additional or extended antibiotic therapy
Cervical lymphadenitis:
- Severe infection of cervical lymph nodes
- Can progress to suppurative lymphadenitis requiring drainage
- More common in younger children
Systemic Acute Complications:
- Scarlet fever:
- Caused by erythrogenic toxin-producing strains
- Characterized by sandpaper-like rash, strawberry tongue, and desquamation
- Generally resolves without specific complications with appropriate antibiotic treatment
- Streptococcal toxic shock syndrome (rare complication):
- Severe systemic toxicity caused by toxin-producing strains
- Rapid onset of shock, organ failure, and tissue damage
- High mortality rate (30-70%) even with treatment
- Requires intensive care management
Delayed Non-Suppurative Complications
The most significant complications of strep throat are immunologically mediated and develop weeks after the acute infection:
Acute Rheumatic Fever (ARF):
- Incidence: 0.3-3% of untreated strep throat cases in susceptible individuals
- Timing: Typically develops 2-3 weeks after the acute infection
- Mechanism: Autoimmune response due to molecular mimicry between streptococcal M protein and human tissues
- Manifestations:
- Carditis (inflammation of the heart) in 50-70% of cases
- Migratory polyarthritis (primarily large joints)
- Sydenham’s chorea (neurological manifestation)
- Erythema marginatum (rash)
- Subcutaneous nodules
- Long-term impact: Permanent heart valve damage (rheumatic heart disease) in 30-45% of those with carditis
Post-Streptococcal Glomerulonephritis (PSGN):
- Incidence: 0.4-0.6% of untreated cases overall, higher with certain streptococcal strains
- Timing: Typically develops 1-2 weeks after pharyngeal infection (longer after skin infections)
- Mechanism: Immune complex deposition in kidney glomeruli
- Manifestations:
- Hematuria (blood in urine)
- Proteinuria
- Edema
- Hypertension
- Impaired kidney function
- Long-term impact: Generally good prognosis in children; 5-15% of adults may develop chronic kidney disease
Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal Infections (PANDAS):
- Controversy: Remains a debated entity in the medical community
- Proposed mechanism: Autoimmune response affecting the basal ganglia
- Manifestations:
- Sudden onset of obsessive-compulsive disorder
- Tic disorders
- Other neuropsychiatric symptoms
- Timing: Symptoms appear or worsen following streptococcal infection
- Long-term impact: Variable; some cases resolve, others have chronic symptoms
Long-Term Impact on Health
Repeated or severe streptococcal infections can have significant long-term consequences:
Rheumatic Heart Disease (RHD):
- Global burden: Affects 33 million people worldwide
- Mechanism: Result of cumulative valve damage from acute rheumatic fever
- Manifestations:
- Progressive valve stenosis or regurgitation
- Heart failure
- Atrial fibrillation
- Increased risk of endocarditis
- Outcomes: May require valve replacement; significant morbidity and mortality
Chronic Kidney Disease (CKD) from PSGN:
- Risk: Generally low risk in children (less than 1%)
- Higher risk populations: Adults and those with underlying kidney disease
- Manifestations:
- Hypertension
- Proteinuria
- Progressive decline in kidney function
Recurrent Streptococcal Infections:
- Frequency: True recurrence occurs in 10-15% of patients within one year
- Complications:
- Increased risk of suppurative complications
- Higher likelihood of developing non-suppurative sequelae
- Quality of life impact
- School/work absence
- Healthcare utilization burden
Tonsillectomy Consequences:
- Indication: Recurrent streptococcal tonsillitis may lead to tonsillectomy
- Secondary effects:
- Surgical risks
- Altered oropharyngeal microbiome
- Potential immunological impacts
Mortality and Disability Rates
The burden of strep throat-related mortality and disability varies widely by region and access to healthcare:
Direct Mortality (Acute Phase):
- Developed countries: Extremely rare, approaching zero
- Developing countries: Still rare but higher due to delayed treatment
- Causes:
- Airway obstruction from peritonsillar abscess
- Sepsis from invasive infection
- Toxic shock syndrome (mortality 30-70%)
Delayed Mortality (Complications):
- Rheumatic heart disease: 319,400 deaths annually worldwide
- Highest in Sub-Saharan Africa, South Asia, and Pacific Islands
- Rare in North America and Western Europe
- Post-streptococcal glomerulonephritis: Rarely directly fatal
- Regional variations: 95% of rheumatic fever/RHD deaths occur in developing countries
Disability:
- Global burden: Rheumatic heart disease accounts for 10.5 million disability-adjusted life years (DALYs) lost annually
- Economic impact: Substantial due to lost productivity and healthcare costs
- Inequities: Disproportionate burden in low- and middle-income countries
Current Trends:
- Developed countries: Dramatic decline in serious complications over past 70 years
- Developing countries: Continued high burden of rheumatic heart disease
- Global initiatives: Focus on prevention of rheumatic heart disease in high-burden regions
The stark contrast in complication rates between developed and developing regions highlights the importance of early diagnosis, appropriate antibiotic treatment, and secondary prophylaxis programs in preventing the most serious long-term consequences of this common infection.
7. Diagnosis & Testing
Clinical Evaluation
Accurate diagnosis of strep throat begins with a thorough clinical assessment:
History-Taking Elements:
- Sudden onset of sore throat
- Fever (typically ≥101°F/38.3°C)
- Absence of cough, runny nose, or conjunctivitis
- Exposure to confirmed cases
- Age of the patient (higher suspicion in school-aged children)
- Seasonal context (higher suspicion during winter/spring)
- History of previous strep infections or complications
Physical Examination Findings:
- Throat erythema (redness)
- Tonsillar enlargement
- Tonsillar exudates (white or yellow patches)
- Palatal petechiae (small red spots on the soft or hard palate)
- Tender anterior cervical lymphadenopathy
- Scarlatiniform rash if scarlet fever is present
- Assessment of hydration status and airway
Clinical Prediction Rules:
Centor Criteria (for adults):
- Fever
- Tonsillar exudates
- Tender anterior cervical lymphadenopathy
- Absence of cough
- One point for each criterion; higher scores increase likelihood of strep throat
Modified Centor/McIsaac Score (adds age criterion):
- Centor criteria plus age adjustments:
- Age 3-14 years: +1 point
- Age 15-44 years: 0 points
- Age ≥45 years: -1 point
- Score of ≤0: 1-2.5% risk of strep
- Score of 1-2: 5-17% risk of strep
- Score of 3-4: 38-63% risk of strep
- Centor criteria plus age adjustments:
FeverPAIN Score (used in some European guidelines):
- Fever
- Purulence (tonsillar exudates)
- Attends rapidly (within 3 days)
- Inflammation (severe tonsillitis)
- No cough or coryza
Limitations of Clinical Evaluation:
- Sensitivity of clinical judgment alone: 55-75%
- Specificity of clinical judgment alone: 60-80%
- Substantial overlap with viral pharyngitis symptoms
- Clinical criteria less reliable in children under 3 years
- Inter-observer variability in assessment
Laboratory Testing
Several testing options are available for confirming streptococcal pharyngitis:
Rapid Antigen Detection Test (RADT):
- Procedure: Throat swab processed with kit to detect streptococcal antigens
- Turnaround time: 5-10 minutes
- Sensitivity: 70-90% (varies by manufacturer and technique)
- Specificity: 95-100%
- Advantages:
- Immediate results
- Point-of-care testing
- High specificity (low false positive rate)
- Limitations:
- Moderate sensitivity (misses some cases)
- Technique-dependent
- Does not provide antibiotic susceptibility data
Throat Culture:
- Procedure: Throat swab plated on blood agar and incubated
- Turnaround time: 24-48 hours
- Sensitivity: 90-95% (reference standard)
- Specificity: 95-99%
- Advantages:
- High sensitivity and specificity
- Can detect antimicrobial resistance
- Can identify non-Group A streptococci
- Limitations:
- Delayed results
- Laboratory access required
- Higher cost
Molecular Tests:
- Procedure: Nucleic acid amplification tests (NAAT) like PCR
- Turnaround time: 15 minutes to several hours (depending on platform)
- Sensitivity: 93-99%
- Specificity: 97-99%
- Advantages:
- Rapid or same-day results
- Highest sensitivity among rapid tests
- Can detect multiple pathogens simultaneously in some formats
- Limitations:
- Higher cost
- Specialized equipment
- May detect carrier state (non-acute infection)
Serological Tests:
- Antistreptolysin O (ASO) and Anti-DNase B antibody titers
- Not used for acute diagnosis but for confirming recent infection in suspected post-streptococcal complications
- Titers rise 2-3 weeks after infection and peak at 4-6 weeks
Testing Strategies and Guidelines
Major guidelines provide frameworks for when to test and treat:
Infectious Diseases Society of America (IDSA) Approach:
- Selective testing based on clinical features
- Testing recommended for patients with clinical features suggestive of GAS pharyngitis
- Negative RADT in children should be confirmed with throat culture
- Negative RADT in adults does not require backup culture
- No testing recommended for those with features suggesting viral etiology
American Academy of Pediatrics (AAP) Approach:
- Similar to IDSA guidelines
- Emphasizes confirmation of negative RADT with throat culture in children
- Recommends against testing in children <3 years unless specific risk factors present
European Approaches (vary by country):
- Some countries (UK, Netherlands) use clinical scoring without routine testing
- Others (France, Finland) employ routine testing strategies similar to US guidelines
- FeverPAIN or Centor scores often used to determine testing need
World Health Organization (WHO) Approach:
- Focus on resource-limited settings
- Clinical diagnosis without testing in high-prevalence areas
- Emphasis on identifying those at risk for rheumatic fever
Diagnostic Challenges and Emerging Methods
Distinguishing Carriers from Acute Infections:
- 5-15% of asymptomatic individuals (higher in children) carry Group A Streptococcus
- Testing during viral illness may detect carriage rather than causative infection
- Current tests cannot reliably distinguish carriers from acute infections
Special Populations:
- Infant and toddler testing: Atypical presentations make diagnosis challenging
- Immunocompromised patients: May have atypical presentations requiring lower threshold for testing
- Recurrent cases: Difficult to distinguish relapse from reinfection or carrier state
Emerging Diagnostic Methods:
- Multiplex PCR panels: Simultaneous detection of multiple respiratory pathogens
- Microbiome analysis: Understanding pharyngeal microbial communities in health and disease
- Mass spectrometry: Rapid bacterial identification
- Point-of-care molecular tests: Improving access to accurate rapid testing
- Smartphone-enabled diagnostics: Expanding testing capacity in resource-limited settings
Biomarkers:
- Procalcitonin: Shows promise for distinguishing bacterial from viral pharyngitis
- C-reactive protein (CRP): Moderately elevated in bacterial infections
- Interleukin-6: Potential marker for severe infections
- Combination biomarker panels: Research ongoing for improved discrimination
The trend in diagnosis is toward more accurate rapid testing with higher sensitivity and specificity, particularly point-of-care molecular methods that offer the speed of RADTs with accuracy approaching culture methods. However, clinical assessment remains fundamental, particularly in settings where testing resources are limited.
8. Treatment Options
Standard Treatment Protocols
Established guidelines provide clear recommendations for treating strep throat:
Antibiotic Therapy:
First-line treatment: Penicillin remains the gold standard
- Oral penicillin V:
- Children: 250mg 2-3 times daily for 10 days
- Adolescents/Adults: 500mg 2-3 times daily for 10 days
- Intramuscular benzathine penicillin G:
- <27kg: 600,000 units as single dose
- ≥27kg: 1.2 million units as single dose
- Advantages: 100% compliance, higher tissue levels
- Oral penicillin V:
Alternative for penicillin allergy (non-anaphylactic):
- First-generation cephalosporins (if no type I hypersensitivity)
- Cephalexin: 20mg/kg twice daily (max 500mg/dose) for 10 days
- Clindamycin:
- 7mg/kg 3 times daily (max 300mg/dose) for 10 days
- First-generation cephalosporins (if no type I hypersensitivity)
Alternative for penicillin allergy (anaphylactic):
- Macrolides (noting increased resistance rates in some regions):
- Azithromycin: 12mg/kg once daily (max 500mg) for 5 days
- Clarithromycin: 7.5mg/kg twice daily (max 250mg/dose) for 10 days
- Clindamycin (as above)
- Macrolides (noting increased resistance rates in some regions):
Duration controversies:
- Traditional recommendation: 10 days of therapy
- Shorter courses (5-7 days) with certain antibiotics (cephalosporins, azithromycin)
- Evidence suggests 10-day course superior for preventing rheumatic fever
Symptomatic Treatment:
- Pain management:
- Acetaminophen/paracetamol
- Ibuprofen or other NSAIDs
- Throat lozenges (for patients old enough to use safely)
- Salt water gargles
- Hydration: Encouraging adequate fluid intake
- Rest: Particularly during febrile period
- Soft diet: Avoiding irritating foods during acute phase
Treatment Guidelines by Organization:
Infectious Diseases Society of America (IDSA):
- Emphasizes penicillin as first-line therapy
- Recommends against routine use of azithromycin or broader-spectrum antibiotics
- Supports full 10-day treatment course
American Academy of Pediatrics (AAP):
- Aligns with IDSA guidelines
- Emphasizes importance of completing full course
- Addresses specific pediatric dosing considerations
World Health Organization (WHO):
- Focus on rheumatic fever prevention in endemic areas
- Emphasis on single-dose injectable therapy in high-risk populations
- Pragmatic approaches for resource-limited settings
Management Challenges and Special Situations
Recurrent Strep Throat:
- Definition: Generally ≥3 documented episodes within 6-12 months
- Approach:
- Distinguish between true recurrence and carrier state
- Consider throat culture for family members (household transmission)
- Extended antibiotic course for treatment failures
- Consider clindamycin or amoxicillin-clavulanate for suspected intracellular persistence
Carrier State Management:
- Indications for treating carriers:
- Family history of rheumatic fever
- Outbreaks of strep throat or invasive disease
- Family/community “ping-pong” infections
- Treatment regimens:
- Clindamycin: 7mg/kg 3 times daily (max 300mg/dose) for 10 days
- Rifampin plus penicillin
- Azithromycin: 12mg/kg once daily (max 500mg) for 5 days
Tonsillectomy Considerations:
- Potential indications:
- ≥7 documented episodes in one year
- ≥5 episodes per year for two consecutive years
- ≥3 episodes per year for three consecutive years
- With significant quality of life impact
- Effectiveness: Reduces frequency of strep throat but not all throat infections
- Risks vs. benefits: Individualized decision-making recommended
Special Populations:
- Pregnancy:
- Penicillin, amoxicillin, and cephalosporins remain first-line (Category B)
- Avoid tetracyclines and fluoroquinolones
- Limited data on newer macrolides
- Immunocompromised patients:
- Lower threshold for treatment
- May require longer courses or broader-spectrum agents
- Closer follow-up recommended
Emerging Treatments and Research Directions
Antibiotic Innovations:
- Narrow-spectrum agents: Targeting specific pathogens to reduce collateral damage to microbiome
- Novel delivery systems: Extended-release formulations to improve adherence
- Shorter treatment protocols: Evaluating efficacy of shorter courses with specific antibiotics
Non-Antibiotic Approaches:
- Bacteriophage therapy: Virus-based treatment targeting specific bacteria
- Probiotic interventions: Restoring healthy pharyngeal microbiome
- Immune modulators: Reducing inflammation while preserving immune clearance
- Anti-virulence strategies: Targeting bacterial toxins and virulence factors rather than killing bacteria
Prevention Research:
- Streptococcal vaccine development:
- M protein-based vaccines (30-valent vaccine in development)
- Non-M protein vaccines targeting conserved antigens
- Mucosal immunity approaches
- Passive immunization strategies:
- Monoclonal antibodies against virulence factors
- Engineered antibody fragments
Clinical Decision Support:
- Point-of-care algorithms: Integrating symptoms, biomarkers, and rapid test results
- Mobile health applications: Improving adherence and symptom monitoring
- Remote monitoring technologies: Ensuring treatment success and early detection of complications
Clinical Trials and Research
Several notable clinical trials and research initiatives are advancing strep throat management:
Active Clinical Trials:
- Vaccine trials: Phase I/II studies of multivalent M protein vaccines
- Treatment duration studies: Comparing 5 vs. 10-day regimens with various antibiotics
- Rapid diagnostic validation: Studies of newer molecular point-of-care tests
- Biomarker studies: Identifying predictors of complications and treatment response
Research Priorities:
- Developing effective Group A Streptococcus vaccines
- Improving diagnostic accuracy, particularly in resource-limited settings
- Understanding carriers and recurrent infections
- Addressing antimicrobial resistance
- Preventing rheumatic heart disease in high-burden regions
- Clarifying the pathophysiology of post-streptococcal immune-mediated complications
Implementation Research:
- Strategies to improve antibiotic stewardship
- Approaches to enhance treatment adherence
- Models for prevention in high-burden settings
- Cost-effective testing and treatment algorithms
The treatment landscape for strep throat continues to evolve, balancing the established efficacy of traditional approaches with innovations that promise improved outcomes, reduced complications, and enhanced antimicrobial stewardship in the face of growing global resistance concerns.
9. Prevention & Precautionary Measures
Primary Prevention Strategies
Several approaches can reduce the risk of acquiring strep throat:
Hygiene Measures:
- Hand hygiene: Regular washing with soap and water or alcohol-based sanitizers
- Respiratory etiquette: Covering coughs and sneezes with tissues or elbow
- Avoiding shared utensils and drinks: Particularly during known outbreaks
- Proper handling of tissues: Prompt disposal after use
- Regular cleaning of frequently touched surfaces: Especially in settings with children
Exposure Limitation:
- Avoiding close contact with infected individuals:
- Maintaining distance from people with confirmed strep throat
- Limiting exposure to individuals with sore throat symptoms
- Temporary avoidance of crowded settings during outbreak periods
- School and daycare exclusion policies:
- Infected individuals should remain home until 24 hours after starting antibiotics
- Some institutions require documented treatment before return
Environmental Measures:
- Adequate ventilation in schools, daycare centers, and workplaces
- Humidity control: Maintaining moderate humidity levels (40-60%)
- Reducing crowding in institutional settings
- Air filtration in high-risk environments
Lifestyle Factors:
- Adequate sleep: Maintaining healthy sleep patterns
- Stress management: Chronic stress can affect immune function
- Smoking cessation: Smoking damages respiratory defenses
- Proper nutrition: Supporting immune function
Secondary Prevention
For those who have had strep throat, preventing complications is crucial:
Prompt Diagnosis and Treatment:
- Early medical evaluation for symptoms suggestive of strep throat
- Appropriate antibiotic therapy:
- Timely initiation
- Correct medication selection
- Proper dosing
- Complete course adherence
- Treatment verification: Follow-up for persistent symptoms
Prevention of Recurrence:
- Identification and treatment of household carriers
- Replacement of personal items: Particularly toothbrushes after treatment initiation
- Enhanced preventive measures during high-risk seasons
Rheumatic Fever Prevention:
- Primary prophylaxis: Complete treatment of acute strep throat
- Secondary prophylaxis for those with history of rheumatic fever:
- Intramuscular benzathine penicillin G every 3-4 weeks
- Oral penicillin V twice daily
- Duration: Varies based on presence of carditis and severity:
- No carditis: Minimum 5 years or until age 21
- Carditis without residual heart disease: 10 years or until age 21
- Carditis with residual heart disease: At least 10 years and often lifelong
Vaccine Development
Though no vaccine is currently available, significant progress is being made:
Current Status:
- No licensed vaccine against Group A Streptococcus exists
- Several candidates in various stages of development
- Global health priority, particularly for rheumatic heart disease prevention
Vaccine Approaches:
- M protein-based vaccines:
- 30-valent vaccine in Phase I/II trials
- Coverage of most common disease-causing strains in North America and Europe
- Less coverage for strains in developing countries
- Conserved antigen vaccines:
- Targeting non-variable portions of M protein
- J8 peptide vaccine candidates
- Streptococcal C5a peptidase vaccines
- Combination approaches:
- Multiple antigens to broaden protection
- Targeting both colonization and virulence factors
Challenges in Development:
- Serotype diversity (>240 emm types identified)
- Regional variation in strain distribution
- Theoretical risk of autoimmune reactions
- Need for mucosal immunity
- Implementation challenges in resource-limited settings
Timeline and Prospects:
- Lead vaccine candidates in Phase I/II trials
- Earliest potential availability: 5-10 years
- Initial focus likely on high-burden populations
- Potential massive impact on rheumatic heart disease burden
Public Health Approaches
Comprehensive public health strategies are essential, particularly in high-burden regions:
Surveillance Systems:
- Outbreak monitoring: Early detection and response to clusters
- Antibiotic resistance tracking: Monitoring changes in susceptibility patterns
- Strain typing: Identifying particularly virulent strains
- Post-streptococcal disease registries: Tracking rheumatic fever and glomerulonephritis
Education Programs:
- Healthcare provider education:
- Appropriate testing strategies
- Judicious antibiotic prescribing
- Recognition of complications
- Community education:
- Symptom recognition
- Importance of treatment completion
- Transmission prevention measures
- School-based programs:
- Hand hygiene promotion
- Recognition of outbreaks
- Appropriate exclusion policies
Organized Prevention Programs:
- Rheumatic Heart Disease Prevention:
- School-based screening in endemic areas
- Register-based follow-up for secondary prophylaxis
- “RF ALL” program in New Zealand and Australia
- WHO global RHD action plan
- Integrated Management of Childhood Illness (IMCI):
- WHO/UNICEF approach incorporating strep throat recognition and management
- Standardized protocols for limited-resource settings
Policy Approaches:
- Antibiotic stewardship programs
- Healthcare access initiatives
- School health policies
- Housing policies to reduce overcrowding
- Water and sanitation improvements
The combination of individual preventive measures, appropriate treatment protocols, and comprehensive public health approaches offers the best strategy for reducing the burden of strep throat and its complications, particularly in vulnerable populations and high-burden regions. Future vaccination programs may dramatically change the landscape if successful candidates advance through development and implementation.
10. Global & Regional Statistics
Global Prevalence and Incidence
Strep throat represents a significant global disease burden with distinct epidemiological patterns:
Global Incidence:
- Estimated 616 million cases of strep throat annually worldwide
- Approximately 1.78 million new cases daily
- Accounts for 15-30% of all pharyngitis cases in children globally
- 5-15% of pharyngitis cases in adults worldwide
- Highest incidence during winter and early spring in temperate climates
- More consistent year-round incidence in tropical regions
Age Distribution:
- School-aged children (5-15 years): Peak incidence
- 25-30% of sore throats in this age group are streptococcal
- Annual incidence of approximately 15-20% in this population
- Preschool children (3-5 years): Moderate incidence
- 10-15% of sore throats are streptococcal
- Adults: Lower but significant incidence
- 5-10% of sore throats are streptococcal
- Annual incidence of approximately 2-4%
Healthcare Utilization:
- Estimated 15 million outpatient visits annually in the United States alone
- Accounts for 1-2% of all ambulatory care visits
- Responsible for 15-20% of antibiotic prescriptions for respiratory conditions
- Substantial economic impact through healthcare costs and lost productivity
Regional Variations
The epidemiology of strep throat and its sequelae varies significantly across regions:
High-Income Countries:
North America:
- Annual incidence: 15-20% in children, 2-4% in adults
- Dramatic decline in rheumatic fever rates (0.5-2 per 100,000)
- Low rheumatic heart disease prevalence (0.1-0.2 per 1,000)
- Seasonal peaks in late fall, winter, and early spring
- Higher rates in northern states compared to southern states
Western Europe:
- Similar patterns to North America
- Variations between northern countries (higher rates) and Mediterranean (lower rates)
- Very low rheumatic fever incidence (0.1-1 per 100,000)
- Less seasonal variation in Mediterranean countries
Australia and New Zealand:
- Moderate overall rates
- Significant disparities between indigenous and non-indigenous populations
- Indigenous populations have rates comparable to developing countries
- Focused public health initiatives addressing these disparities
Japan and South Korea:
- Lower rates than Western countries
- Highly sensitive detection and treatment systems
- Very low rheumatic fever incidence
Middle-Income Countries:
Eastern Europe and Russia:
- Moderate-to-high strep throat incidence
- Variable rheumatic fever rates (5-15 per 100,000)
- Fragmented surveillance systems
Latin America:
- Relatively high incidence (20-25% of sore throats)
- Rheumatic fever rates of 5-20 per 100,000
- Rheumatic heart disease prevalence of 1-5 per 1,000
- Successful RF prevention programs in some countries (Cuba, Costa Rica)
China:
- Lower reported rates than Western countries
- Significant urban-rural disparities
- Increasing attention to surveillance and prevention
Middle East and North Africa:
- Moderate-to-high incidence
- Rheumatic fever rates of 10-20 per 100,000 in some countries
- Limited comprehensive surveillance data
Low-Income Countries:
Sub-Saharan Africa:
- High incidence where measured
- Limited surveillance systems
- Rheumatic fever rates estimated at 13-86 per 100,000
- Rheumatic heart disease prevalence of 5-15 per 1,000
- Highest global burden of rheumatic heart disease
South Asia (India, Pakistan, Bangladesh):
- High strep throat incidence
- Rheumatic fever rates of 25-40 per 100,000
- Rheumatic heart disease prevalence of 4-10 per 1,000
- Significant urban-rural disparities
- Limited access to diagnostic testing and treatment
Pacific Islands:
- Extremely high rates of strep throat
- Highest global rates of rheumatic fever and rheumatic heart disease
- Rheumatic heart disease prevalence up to 33 per 1,000 in some islands
Mortality and Morbidity
The health impact of strep throat varies dramatically between direct effects and sequelae:
Direct Mortality from Acute Infection:
- High-income countries: Extremely rare, approaching zero
- Low-income countries: Still rare but higher due to limited access to care
- Causes of direct mortality:
- Airway obstruction from peritonsillar abscess
- Invasive infection leading to sepsis
- Streptococcal toxic shock syndrome (30-70% mortality)
Rheumatic Heart Disease Mortality:
- Estimated 319,400 deaths annually worldwide
- 95% of deaths occur in developing regions
- Regional annual mortality rates (per 100,000):
- Sub-Saharan Africa: 7-19
- South Asia: 2.5-8
- Pacific Islands: 9-15
- High-income countries: <0.1
Morbidity Burden:
- Rheumatic heart disease accounts for 10.5 million disability-adjusted life years (DALYs) annually
- Leading cause of cardiovascular mortality in children and young adults in developing countries
- Major cause of stroke and heart failure in young adults in endemic regions
- Significant economic impact through treatment costs and lost productivity
Trends and Changing Patterns
Several important epidemiological shifts have been observed:
Temporal Trends:
Developed countries:
- Dramatic decline in rheumatic fever incidence over 20th century
- Recent possible resurgence in some areas (intermittent outbreaks)
- Stable or slightly declining strep throat incidence
Developing countries:
- Evidence of declining rheumatic fever rates in some middle-income countries
- Persistently high rates in low-income settings
- Increased recognition due to improved surveillance
Antibiotic Resistance Patterns:
Macrolide resistance:
- Variable by region: 5-8% in US, 10-30% in Europe, >90% in certain Asian countries
- Cyclical patterns observed over time
- Critical monitoring issue for alternative treatment options
Penicillin: No documented resistance to date in Group A Streptococcus
Strain Variations:
- Certain emm types associated with higher virulence
- Geographic differences in prevalent strains
- Temporal shifts in dominant strains within regions
- Emergence of novel strains with altered virulence profiles
Impact of Public Health Initiatives:
- Substantial reductions in rheumatic fever where comprehensive programs implemented
- New Zealand reduced rheumatic fever by 40% through targeted program
- WHO Global Rheumatic Heart Disease Action Plan showing impact in pilot regions
- Success of register-based secondary prophylaxis programs
These global and regional patterns highlight the unequal distribution of disease burden and outcomes, with dramatic disparities between high-income and low-income settings. The stark contrast in complication rates emphasizes the critical importance of access to diagnosis and treatment, particularly in preventing the life-threatening and disabling sequelae of this common infection.
11. Recent Research & Future Prospects
Recent Scientific Advances
Significant progress has been made in understanding and managing strep throat:
Pathogen Biology:
- Genomic insights: Complete genome sequencing of multiple Group A Streptococcus strains
- Virulence factor characterization: Identification of novel toxins and immune evasion mechanisms
- Bacterial population dynamics: Understanding of strain diversity and evolution
- Host-pathogen interactions: Elucidation of molecular mechanisms of tissue invasion and persistence
- Biofilm formation: Recognition of role in recurrent infections and treatment failures
Immunological Advances:
- Pathogenesis of post-streptococcal sequelae: Improved understanding of molecular mimicry
- Immune response variations: Identification of genetic factors affecting host responses
- Microbiome interactions: Recognition of how pharyngeal microbiome influences susceptibility and outcomes
- Immune evasion mechanisms: Discovery of novel bacterial strategies for persistence
- Mucosal immunity: Better understanding of protective mechanisms at pharyngeal surfaces
Diagnostic Innovations:
- Point-of-care molecular testing: Development of rapid, highly sensitive nucleic acid amplification tests
- Multiplexed diagnostics: Systems detecting multiple respiratory pathogens simultaneously
- Biomarker identification: Discovery of host proteins that differentiate bacterial from viral infections
- Smartphone-based diagnostics: Technologies leveraging mobile devices for expanding access
- AI-assisted diagnosis: Algorithms to improve clinical decision-making
Treatment Advancements:
- Treatment duration optimization: Evidence supporting shorter courses for certain antibiotics
- Narrow-spectrum approaches: Targeted therapies minimizing collateral damage to microbiome
- Novel delivery systems: Long-acting formulations improving adherence
- Therapeutic monoclonal antibodies: Targeting specific virulence factors
- Phage therapy research: Virus-based approaches specific to streptococcal infections
Ongoing Research Initiatives
Several major research programs are advancing our understanding and management of strep throat:
Vaccine Development:
- StreptInCor vaccine: Based on conserved M protein epitopes; completed Phase I trials
- 30-valent M protein vaccine: In Phase I/II trials; targets common strains in developed countries
- J8-DT vaccine: Targeting conserved M protein region; in clinical development
- Non-M protein vaccines: Targeting conserved surface antigens like C5a peptidase
- Mucosal vaccine approaches: Targeting pharyngeal colonization via intranasal delivery
Diagnostics Research:
- Novel biomarker panels: Combining host and pathogen markers for improved accuracy
- Nanopore sequencing: Real-time bacterial identification and typing
- Breath analysis: Detection of volatile organic compounds associated with specific infections
- Mass spectrometry techniques: Rapid pathogen identification
- Digital health integration: Combining symptoms, biomarkers, and epidemiological data
Therapeutic Research:
- Anti-virulence approaches: Targeting bacterial toxins rather than bacterial growth
- Novel antibiotics: Development of new agents active against Group A Streptococcus
- Immune modulation: Approaches to enhance appropriate immune responses
- Microbiome manipulation: Probiotics and bacterial interference strategies
- Combination therapies: Synergistic approaches for difficult cases
Prevention Programs:
- Global RHD Action Plan: WHO-led initiative focused on rheumatic heart disease prevention
- School-based intervention trials: Evaluating comprehensive prevention approaches
- Primary prevention programs: Pragmatic approaches in high-burden settings
- Implementation science: Optimizing delivery of existing interventions
Future Treatment Possibilities
Several promising approaches may transform strep throat management:
Preventive Strategies:
- Universal or targeted vaccination: Would dramatically reduce incidence if successful
- Prophylactic probiotics: Manipulation of pharyngeal microbiome for colonization resistance
- Antiseptic throat sprays/lozenges: For use during high-risk exposures
- Monoclonal antibody prophylaxis: For high-risk individuals during outbreaks
Therapeutic Innovations:
- Precision antibiotics: Tailored based on specific strain characteristics
- Single-dose oral therapy: Improving adherence and outcomes
- Phage cocktails: Specifically targeting Group A Streptococcus
- CRISPR-based antimicrobials: Targeting essential bacterial genes
- Anti-biofilm agents: Addressing persistent and recurrent infections
- Combination rapid test/treatment kits: For home or community use
Management Approaches:
- Digital medicine programs: Remote monitoring for treatment adherence and outcomes
- Risk stratification algorithms: Tailoring treatment intensity to individual risk profiles
- Integration with telemedicine: Expanding access to expert care
- Population health management: Comprehensive approaches for high-risk communities
- Automated contact tracing: Using digital tools to identify and manage outbreaks
Future Research Directions
Several key knowledge gaps require further investigation:
Fundamental Questions:
- Carrier state biology: Why do some individuals asymptomatically carry Group A Streptococcus?
- Host susceptibility factors: What genetic and environmental factors determine who develops complications?
- Strain virulence determinants: Which bacterial factors predict invasive disease or sequelae?
- Microbiome interactions: How do other pharyngeal bacteria influence Group A Streptococcus behavior?
- Immune memory: Why doesn’t natural infection provide lasting immunity?
Translational Research Priorities:
- Vaccine development: Overcoming challenges of strain diversity and safety concerns
- Rapid diagnostic optimization: Improving accuracy, accessibility, and cost-effectiveness
- Novel therapeutic targets: Identifying bacterial vulnerabilities for new treatments
- Biomarkers for complications: Predicting who will develop rheumatic fever or glomerulonephritis
- Prevention strategies: Determining most effective approaches for different settings
Implementation Research Needs:
- Healthcare delivery models: Optimizing testing and treatment strategies for different resources
- Antibiotic stewardship: Balancing appropriate treatment with resistance concerns
- Public health approaches: Developing sustainable prevention programs
- Health disparities: Addressing inequities in disease burden and outcomes
- Cost-effectiveness analyses: Guiding resource allocation for greatest impact
The future management of strep throat will likely involve a multi-faceted approach combining improved diagnostics, targeted therapies, and preventive strategies including vaccination. Advances in these areas promise to reduce both the acute burden of disease and the devastating long-term complications that continue to affect millions worldwide, particularly in resource-limited settings.
12. Interesting Facts & Lesser-Known Insights
Surprising Historical Facts
The history of strep throat contains fascinating elements often overlooked:
Historical Significance:
- Royal impact: Queen Anne of Great Britain (1665-1714) lost 17 of her 18 children, with several deaths attributed to what were likely streptococcal infections
- Military influence: Rheumatic fever outbreaks significantly impacted military readiness in both World Wars, leading to major research initiatives
- Scarlet fever fear: In the 19th century, scarlet fever (a form of strep throat with characteristic rash) was feared similar to how polio was in the 20th century
- Children’s literature: The death of Beth in “Little Women” is attributed to complications of scarlet fever, reflecting its historical lethality
Scientific Milestones:
- Early biological warfare: In 1941, military researchers at Camp Detrick investigated streptococci as potential biological weapons before abandoning the approach
- Rebecca Lancefield’s work: Her classification system was developed using streptococci grown in broth made from meat obtained from a local butcher
- Penicillin discovery: While Fleming discovered penicillin in 1928, its first clinical use for streptococcal infections didn’t occur until 1941
- Tragic experiment: In 1924, the Viennese pathologist Ernst Löwenstein purposely infected children with streptococci to study rheumatic fever, an experiment that would be considered deeply unethical today
Unexpected Connections:
- Disease decline mystery: Scarlet fever and rheumatic fever began declining in incidence before antibiotics were introduced, for reasons still not fully understood
- Puerperal fever link: The same organism causing strep throat was responsible for childbed fever, which killed thousands of women before Semmelweis discovered its contagious nature
- Centuries-old descriptions: Hippocrates described what was likely streptococcal pharyngitis around 400 BCE
- Dual discovery: Streptococci were independently identified by Louis Pasteur and Robert Koch in the same year (1879), working with different clinical conditions
Common Misconceptions
Several persistent myths surround strep throat:
Myth: Strep throat always presents with white spots on the tonsils. Fact: While tonsillar exudates are common, up to 30% of confirmed strep throat cases do not have visible exudates.
Myth: You can diagnose strep throat just by looking at the throat. Fact: Clinical examination alone has only 50-70% sensitivity and specificity; laboratory confirmation is necessary for accurate diagnosis.
Myth: All sore throats should be treated with antibiotics to “be safe.” Fact: 70-85% of sore throats are viral and do not benefit from antibiotics; unnecessary treatment contributes to antibiotic resistance.
Myth: Once you feel better, you can stop taking the prescribed antibiotics. Fact: Completing the full course of antibiotics is essential to prevent complications and reduce the risk of rheumatic fever.
Myth: Strep throat always causes fever. Fact: While fever is common, approximately 15-20% of confirmed strep throat cases occur without significant fever.
Myth: Adults don’t get strep throat. Fact: Though less common than in children, adults account for approximately 5-15% of all strep throat cases.
Myth: Natural remedies like honey and lemon are as effective as antibiotics for strep throat. Fact: While these may provide symptomatic relief, they do not kill the bacteria or prevent complications.
Myth: You must throw away your toothbrush after having strep throat. Fact: While changing toothbrushes is often recommended, studies have not conclusively proven this reduces recurrence rates.
Myth: Strep throat always causes a rash. Fact: The characteristic rash (scarlet fever) only occurs in 10-20% of cases when the infecting strain produces erythrogenic toxin.
Myth: You can’t get strep throat twice. Fact: Previous infection provides only type-specific immunity; with over 240 different M types, repeated infections are common.
Unusual Scientific Insights
Research has uncovered some remarkable aspects of strep throat:
Biological Peculiarities:
- Human-specific pathogen: Group A Streptococcus naturally infects only humans, with no animal reservoir
- Molecular mimicry: The M protein of Group A Streptococcus contains sections that resemble human heart valve tissue, explaining autoimmune complications
- Unique hyaluronic acid capsule: Identical to human connective tissue, providing “molecular camouflage” from the immune system
- Seasonal strains: Different emm types predominate in different seasons, with certain strains more common in winter vs. spring
- Superantigen production: Some strains produce toxins that activate up to 20% of all T-cells (compared to 0.01% in normal immune responses)
Epidemiological Curiosities:
- Family susceptibility: Having a family member with strep throat increases your risk 2-4 times
- Classroom spread: When cases occur in schools, the risk to classmates increases 3-5 times
- Occupational patterns: Elementary school teachers have 2-3 times higher rates than secondary school teachers
- Age-related immunity: Adults who live with children have better immunity and lower rates than adults who don’t
- Meteorological correlations: Some studies show associations between strep throat outbreaks and specific weather patterns
Clinical Observations:
- Rapid response: Fever typically resolves within 24 hours of starting antibiotics, faster than almost any other bacterial infection
- Taste changes: Up to 30% of patients report a metallic taste or altered taste perception during infection
- Palatal petechiae pattern: The distribution of small red spots on the palate is often distinctive for strep vs. viral causes
- Abdominal predominance: In children under 6, abdominal pain may be more prominent than sore throat
- Post-streptococcal psychiatric symptoms: Beyond PANDAS, various neuropsychiatric symptoms can occur following infection
Impact on Specific Populations
Strep throat affects various groups in unique ways:
Professional Singers and Performers:
- Higher awareness and concern about pharyngeal infections
- Potentially career-threatening when chronic or recurrent
- Often receive more aggressive treatment approaches
- May use prophylactic strategies during high-risk periods
- Economic impact through canceled performances
Indigenous Populations:
- Dramatically higher rates of rheumatic fever and rheumatic heart disease
- In Australian Aboriginal communities, rates 20-40 times higher than non-Aboriginal populations
- Similar disparities in Native American, Māori, and Pacific Islander populations
- Complex factors including housing, healthcare access, and genetic susceptibility
- Target of specialized public health initiatives
Immunocompromised Individuals:
- May present with atypical features
- Higher risk of invasive disease and complications
- Potentially longer treatment courses required
- Higher threshold for prophylactic strategies
- May have impaired response to future vaccine candidates
Military Personnel:
- Historical significance in military medicine
- Crowded conditions in training facilities facilitate transmission
- Surveillance systems for early outbreak detection
- Standardized treatment protocols
- Subject of major military medical research initiatives
Competitive Athletes:
- Special concerns about cardiac involvement
- Specific return-to-play guidelines after infection
- Team outbreaks can significantly impact competitions
- Testing protocols during tournament play
- Concerns about performance impact of symptoms and treatment
These fascinating aspects of strep throat illustrate that even a common condition harbors surprising complexity and historical significance. From molecular mimicry to population-specific impacts, the full story of this ancient pathogen continues to unfold through ongoing research and clinical observation.
This comprehensive report provides an in-depth examination of strep throat, integrating historical context, current clinical practice, and future directions. While Group A Streptococcus infections remain common worldwide, continued advances in diagnosis, treatment, and prevention promise to reduce both the immediate burden of disease and its potentially devastating long-term complications.
