
⚠️ Disclaimer: The information provided in this article is for educational purposes only and does not constitute medical advice. RevisionTown does not provide diagnosis, treatment, or medical recommendations. Always consult a qualified healthcare professional regarding any medical condition, symptoms, or concerns.
Read More – 🏥 Medical Disclaimer
1. Overview
What is Angina?
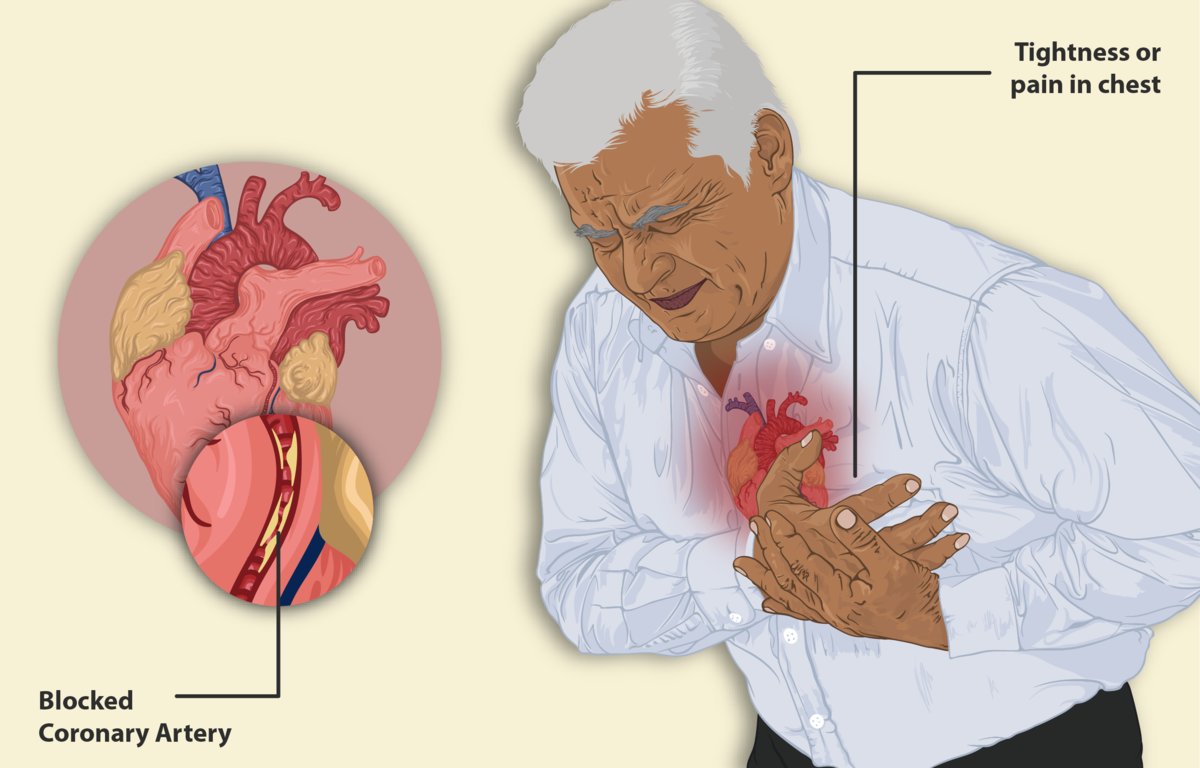
Angina pectoris, commonly known as angina, is a clinical syndrome characterized by discomfort or pain in the chest due to insufficient blood flow to the heart muscle (myocardium). This reduced blood flow results in inadequate oxygen supply to meet the metabolic demands of the heart, a condition known as myocardial ischemia. Angina is not a disease itself but rather a symptom of an underlying cardiac condition, most commonly coronary artery disease (CAD).
Affected Body Parts/Organs
While angina manifests primarily as chest discomfort, it fundamentally affects the cardiovascular system, specifically:
- The heart muscle (myocardium)
- Coronary arteries that supply blood to the heart
- The cardiac conduction system
- Potentially the autonomic nervous system that regulates cardiac function
The discomfort often radiates to other areas including the left arm, shoulders, neck, jaw, and upper back, reflecting the complex neural pathways of cardiac pain.
Prevalence and Significance
Angina affects approximately 112 million people worldwide, making it one of the most common cardiovascular conditions. In the United States alone, an estimated 10 million people have angina, with about 500,000 new cases diagnosed annually. The prevalence increases with age, affecting 5-8% of individuals over 55 years.
Angina significantly impacts quality of life and healthcare resources:
- It accounts for approximately 2% of all primary care consultations
- It’s a leading cause of emergency department visits
- It often precedes more serious cardiac events like myocardial infarction
- It serves as an important warning sign of underlying coronary artery disease
- It results in substantial economic burden through direct healthcare costs and lost productivity
2. History & Discoveries
First Identification
Symptoms resembling angina have been described in medical literature for thousands of years, dating back to ancient Egyptian papyri. However, the formal medical identification of angina pectoris is credited to British physician William Heberden, who provided the first clear clinical description in 1768 in his presentation to the Royal College of Physicians. Heberden coined the term “angina pectoris” (Latin for “strangling in the chest”) and described it as “a painful and most disagreeable sensation in the breast, which seems as if it would extinguish life if it were to increase or continue.”
Key Discoveries and Historical Figures
- William Heberden (1768): First clinical description and naming of angina pectoris
- Edward Jenner & Caleb Hillier Parry (1790s): Connected angina to coronary artery disease through post-mortem examinations
- Lauder Brunton (1867): Introduced amyl nitrite as the first effective treatment for angina
- William Murrell (1879): Pioneered the use of nitroglycerin (glyceryl trinitrate) for angina treatment
- James Herrick (1912): Distinguished angina from myocardial infarction (heart attack)
- Werner Forssmann (1929): Developed cardiac catheterization, enabling coronary angiography
- Mason Sones (1958): Refined selective coronary angiography, revolutionizing diagnosis
- René Favaloro (1967): Pioneered coronary artery bypass grafting (CABG)
- Andreas Grüntzig (1977): Performed the first percutaneous transluminal coronary angioplasty (PTCA)
- Julio Palmaz & Richard Schatz (1980s): Developed coronary stents
Evolution of Medical Understanding
The understanding of angina has evolved dramatically over centuries:
- Initially viewed as a mysterious chest ailment with no known cause
- Gradually recognized as a cardiac condition through post-mortem studies
- Connected to coronary artery disease in the 19th century
- Differentiated from heart attack in the early 20th century
- Recognition of different types (stable, unstable, variant) throughout the 20th century
- Understanding of microvascular angina in recent decades
- Modern comprehensive understanding incorporating biochemical, physiological, genetic, and environmental factors
- Recognition of sex differences in presentation and pathophysiology
- Evolution from primarily symptom management to prevention and treatment of underlying disease
3. Symptoms
Common Symptoms
- Chest discomfort: Often described as pressure, squeezing, heaviness, tightness, burning, or fullness rather than sharp pain
- Location: Typically behind the sternum (breastbone) or slightly to the left
- Radiation: May extend to shoulders, arms (especially left), neck, jaw, or back
- Duration: Usually lasts 2-10 minutes; rarely shorter than 30 seconds or longer than 30 minutes
- Accompanying symptoms: Shortness of breath, fatigue, sweating, nausea, dizziness
- Triggers: Typically brought on by physical exertion, emotional stress, cold weather, heavy meals, or smoking
Types of Angina and Their Symptoms
Stable Angina
- Predictable pattern of chest discomfort
- Triggered by specific activities or stressors
- Relieved by rest or nitroglycerin within minutes
- Consistent frequency, intensity, and duration over time
- Warning sign of underlying coronary artery disease but not an immediate emergency
Unstable Angina
- Occurs unpredictably, even at rest
- More severe, prolonged, or frequent than usual
- May not respond well to nitroglycerin
- Represents a significant escalation and medical emergency
- Warning of impending heart attack
Variant (Prinzmetal’s) Angina
- Occurs primarily at rest, often during sleep
- Caused by coronary artery spasm rather than blockage
- More common in younger patients and women
- May demonstrate cyclic pattern (same time each day)
- Often associated with ST-segment elevation on ECG during episodes
Microvascular Angina
- Similar chest discomfort but caused by disease of the heart’s smallest blood vessels
- Often more diffuse or prolonged discomfort
- May be more resistant to standard treatments
- More common in women
- May present with more pronounced fatigue and shortness of breath
Symptom Progression
Angina symptoms typically evolve in the following ways:
- Initial presentation: Often mild discomfort during significant exertion only
- Early progression: Discomfort occurring at lower thresholds of activity
- Concerning changes: Increased frequency, severity, duration, or reduced response to medication
- Warning signs: New symptoms at rest, during sleep, or with minimal exertion
- Critical progression: Development of unstable angina patterns, representing critical narrowing or unstable plaque
4. Causes
Biological Causes
The fundamental cause of angina is an imbalance between myocardial oxygen supply and demand. The most common underlying biological causes include:
Primary Causes
- Atherosclerosis: Buildup of plaque (fatty deposits) in coronary arteries, narrowing the vessel lumen
- Coronary artery spasm: Temporary, sudden narrowing of a coronary artery
- Microvascular dysfunction: Abnormalities in the heart’s smallest blood vessels
- Inflammation: Vascular inflammation contributing to endothelial dysfunction
Secondary Causes
- Aortic stenosis: Narrowing of the aortic valve increasing cardiac workload
- Hypertrophic cardiomyopathy: Abnormal heart muscle thickening
- Severe anemia: Reduced oxygen-carrying capacity of blood
- Severe hypertension: Increased cardiac workload and oxygen demand
- Tachyarrhythmias: Rapid heart rhythms increasing oxygen demand
- Hyperthyroidism: Increased metabolic rate and cardiac demand
- Severe pulmonary hypertension: Right heart strain
- Carbon monoxide exposure: Reduced oxygen-carrying capacity
Genetic and Hereditary Factors
Genetic factors play a significant role in angina susceptibility:
- Familial hypercholesterolemia: Inherited disorder causing extremely high cholesterol levels
- Lipoprotein(a) variants: Genetic variations affecting this atherosclerosis-promoting lipoprotein
- Familial combined hyperlipidemia: Inherited disorder affecting multiple lipid types
- Genetic variants affecting:
- Vascular endothelial function
- Inflammatory responses
- Platelet aggregation
- Blood pressure regulation
- Glucose metabolism
- Inherited cardiomyopathies: Including hypertrophic and dilated forms
- Genetic variations in drug metabolism: Affecting response to anti-anginal medications
Known Triggers and Exposure Risks
Multiple factors can trigger angina episodes in susceptible individuals:
Physical Triggers
- Exertion: Physical activity increasing cardiac oxygen demand
- Temperature extremes: Especially cold exposure causing vasoconstriction
- Heavy meals: Diverting blood flow to digestive system and increasing cardiac work
- Sexual activity: Increasing heart rate and cardiac demand
Chemical Triggers
- Tobacco smoke: Both active and passive exposure
- Caffeine: Potentially increasing heart rate and blood pressure
- Alcohol: Especially binge drinking
- Recreational drugs: Particularly cocaine and amphetamines
- Air pollution: Especially particulate matter and nitrogen oxides
Physiological/Psychological Triggers
- Emotional stress: Releasing stress hormones that increase cardiac workload
- Anxiety and panic attacks: Increasing heart rate and blood pressure
- Sleep apnea episodes: Causing intermittent hypoxia
5. Risk Factors
Demographic Risk Factors
- Age: Risk increases significantly with advancing age
- Men: Risk rises notably after age 45
- Women: Risk increases after age 55 (post-menopause)
- Sex: Men have higher risk until women reach menopause, after which rates equalize
- Family history: Risk increases with first-degree relatives having premature heart disease (men under 55, women under 65)
- Ethnicity: Higher rates in South Asians, followed by Blacks, Whites, and Hispanics, with East Asians having generally lower rates
Lifestyle Risk Factors
- Tobacco use: Both active smoking and secondhand exposure significantly increase risk
- Diet: Diets high in saturated/trans fats, refined carbohydrates, sodium, and low in fruits, vegetables, fiber
- Physical inactivity: Sedentary lifestyle contributes to multiple cardiovascular risk factors
- Obesity: Particularly central/abdominal obesity
- Chronic stress: Persistent psychological stress adversely affects cardiovascular health
- Poor sleep: Insufficient or poor-quality sleep, especially with sleep apnea
- Excessive alcohol consumption: Beyond moderate intake (>1 drink/day for women, >2 for men)
Medical and Pre-existing Conditions
- Hypertension: Leading modifiable risk factor, damaging arterial walls
- Dyslipidemia: Abnormal lipid levels, particularly elevated LDL cholesterol and triglycerides, low HDL
- Diabetes mellitus: Accelerates atherosclerosis and often involves multiple comorbidities
- Metabolic syndrome: Cluster of conditions including abdominal obesity, hypertension, high blood sugar, and abnormal cholesterol
- Chronic kidney disease: Associated with accelerated cardiovascular disease
- Autoimmune conditions: Including rheumatoid arthritis, lupus, psoriasis
- Prior heart attack or stroke: Indicating established cardiovascular disease
- Peripheral artery disease: Indicating systemic atherosclerosis
- Chronic inflammatory conditions: Contributing to endothelial dysfunction and atherosclerosis
6. Complications
Immediate Complications
- Progression to unstable angina: Representing higher risk for acute events
- Acute myocardial infarction (heart attack): Complete blockage of coronary artery
- Sudden cardiac arrest: Particularly if major coronary arteries are involved
- Acute heart failure: If significant portion of heart muscle becomes ischemic
Long-term Complications
- Chronic ischemic heart disease: Ongoing coronary insufficiency
- Ischemic cardiomyopathy: Heart muscle damage from repeated or chronic ischemia
- Heart failure: Progressive cardiac dysfunction from cumulative damage
- Arrhythmias: Abnormal heart rhythms from damaged conduction tissue
- Refractory angina: Symptoms resistant to standard treatments
- Psychological effects: Including depression, anxiety, reduced quality of life
- Activity limitation: Restricted physical capacity and independence
- Job/role limitations: Inability to perform certain occupations or activities
Mortality and Disability Statistics
The prognosis for angina varies widely depending on severity, underlying coronary disease, comorbidities, and treatment:
Stable angina:
- Annual mortality rate: 1.2-2.4% per year
- Annual risk of non-fatal myocardial infarction: 0.6-2.7%
- 5-year survival rate: Approximately 85-93%
Unstable angina:
- 1-month mortality without treatment: 5-20%
- 1-year mortality with optimal treatment: 5-8%
- Significantly higher risk of progression to myocardial infarction
Disability impact:
- Approximately 30% of patients with chronic angina report significant limitations in daily activities
- 10-15% report inability to perform routine activities
- Major contributor to reduced work productivity and early retirement
- Significant impact on physical and emotional quality of life
7. Diagnosis & Testing
Clinical Evaluation
The diagnostic process begins with thorough clinical assessment:
- Detailed history: Character, location, radiation, duration, alleviating/aggravating factors
- Risk factor assessment: Age, family history, smoking, hypertension, diabetes, dyslipidemia
- Physical examination: Vital signs, cardiac auscultation, evidence of other vascular disease
- Symptom scoring systems: Canadian Cardiovascular Society (CCS) classification of angina severity
Non-invasive Testing
Multiple non-invasive tests help confirm diagnosis and assess severity:
Electrocardiographic Testing
- Resting ECG: May show ischemic changes or previous infarction
- Exercise stress test: ECG monitoring during standardized exercise protocol
- Holter monitoring: 24-48 hour continuous ECG recording
- Event monitoring: Longer-term recording activated during symptoms
Imaging Studies
- Echocardiography: Ultrasound imaging to assess heart structure and function
- Rest and stress (exercise or pharmacological)
- Can identify wall motion abnormalities during ischemia
- Nuclear perfusion imaging: Radiotracer studies showing blood flow
- Myocardial perfusion scintigraphy
- Positron emission tomography (PET)
- Cardiac computed tomography (CT):
- Coronary calcium scoring
- CT coronary angiography (CCTA)
- Cardiac magnetic resonance imaging (MRI):
- Functional assessment
- Stress perfusion imaging
- Tissue characterization
Invasive Testing
For definitive diagnosis or before interventions:
- Coronary angiography: Gold standard for defining coronary anatomy
- Identifies location and severity of coronary stenoses
- Guides revascularization decisions
- Fractional flow reserve (FFR): Measures pressure differences across stenoses
- Intravascular ultrasound (IVUS): Detailed imaging of vessel walls
- Optical coherence tomography (OCT): High-resolution imaging of coronary arteries
- Coronary flow reserve: Functional assessment of microcirculation
Laboratory Testing
Blood tests play supporting roles in diagnosis:
- Cardiac biomarkers: Troponin and other markers to rule out myocardial infarction
- Lipid profile: Total, LDL, HDL cholesterol, and triglycerides
- Glucose and HbA1c: For diabetes screening/management
- Renal function: Affects treatment options and prognosis
- Inflammatory markers: High-sensitivity C-reactive protein (hs-CRP)
- Thyroid function: To exclude hyperthyroidism
- Complete blood count: To rule out anemia
8. Treatment Options
Pharmacological Management
Multiple medication classes are used to treat angina:
Symptom Relief
- Nitrates:
- Short-acting (sublingual nitroglycerin): For acute episodes
- Long-acting (isosorbide mononitrate/dinitrate): For prevention
- Mechanism: Vasodilation improving myocardial oxygen supply/demand
- Beta-blockers (metoprolol, carvedilol, bisoprolol):
- Reduce heart rate and contractility
- Decrease myocardial oxygen demand
- First-line preventive therapy
- Calcium channel blockers:
- Dihydropyridines (amlodipine): Primarily vasodilators
- Non-dihydropyridines (diltiazem, verapamil): Reduce heart rate and contractility
- Particularly useful for vasospastic angina
- Ranolazine:
- Novel antianginal with unique mechanism
- Reduces sodium and calcium overload in cardiomyocytes
- Particularly useful in diabetes and when other medications inadequate
- Ivabradine:
- Selective If channel inhibitor reducing heart rate
- Used when beta-blockers contraindicated or poorly tolerated
Risk Reduction
- Antiplatelet agents:
- Aspirin: First-line for secondary prevention
- P2Y12 inhibitors (clopidogrel, ticagrelor): Added for high-risk patients
- Statins:
- Reduce atherosclerosis progression
- Plaque stabilization
- Anti-inflammatory effects
- ACE inhibitors/ARBs:
- Particularly for those with hypertension, diabetes, or heart failure
- Vascular protective effects
- PCSK9 inhibitors:
- For severe hypercholesterolemia despite statins
- Significant LDL reduction
Revascularization Procedures
For suitable patients with significant coronary obstruction:
Percutaneous Coronary Intervention (PCI)
- Coronary angioplasty: Balloon dilation of narrowed arteries
- Coronary stenting:
- Bare metal stents
- Drug-eluting stents
- Bioresorbable vascular scaffolds
- Atherectomy: Physical removal of plaque
Surgical Options
- Coronary artery bypass grafting (CABG):
- Using arterial grafts (internal mammary, radial)
- Or venous grafts (saphenous vein)
- Particularly for left main, three-vessel, or complex disease
- Minimally invasive direct coronary artery bypass (MIDCAB)
- Transmyocardial laser revascularization: For refractory angina with unsuitable anatomy
Alternative and Complementary Therapies
- Enhanced external counterpulsation (EECP): Non-invasive treatment improving collateral circulation
- Spinal cord stimulation: For refractory angina
- Acupuncture: Limited evidence for symptom improvement
- Cardiac rehabilitation programs: Structured exercise and lifestyle modification
Emerging Treatments and Clinical Trials
- Therapeutic angiogenesis: Stimulating new blood vessel growth
- Gene therapy (VEGF, FGF)
- Stem cell therapy
- Novel pharmacological agents:
- Sodium-glucose cotransporter-2 (SGLT2) inhibitors
- GLP-1 receptor agonists
- New classes of lipid-lowering drugs
- Mechanical devices:
- Coronary sinus reducers
- Novel stent designs
- Bioresorbable technologies
- Anti-inflammatory approaches:
- Targeted anti-cytokine therapies
- Colchicine for secondary prevention
9. Prevention & Precautionary Measures
Primary Prevention
Strategies to prevent angina development in at-risk individuals:
Lifestyle Modifications
- Dietary approaches:
- Mediterranean diet pattern
- DASH (Dietary Approaches to Stop Hypertension) diet
- Emphasizing fruits, vegetables, whole grains, lean proteins
- Limiting saturated/trans fats, refined carbohydrates, sodium
- Physical activity:
- 150+ minutes of moderate-intensity aerobic activity weekly
- Muscle-strengthening activities twice weekly
- Regular movement throughout the day
- Tobacco cessation:
- Complete abstinence from all tobacco products
- Avoidance of secondhand smoke exposure
- Weight management:
- Maintaining healthy BMI (18.5-24.9 kg/m²)
- Focus on waist circumference (<40 inches for men, <35 inches for women)
- Stress management:
- Regular relaxation practices
- Mindfulness meditation
- Adequate sleep (7-8 hours nightly)
Risk Factor Control
- Blood pressure management: Target <130/80 mmHg for most adults
- Lipid management:
- Primary target: LDL cholesterol
- Secondary targets: non-HDL cholesterol, triglycerides
- Diabetes control: Target HbA1c <7% for most adults
- Metabolic syndrome management: Addressing all components
Secondary Prevention
For those already diagnosed with angina:
Self-Management Strategies
- Recognition of triggers: Understanding and avoiding personal triggers
- Activity pacing: Balancing activity and rest
- Medication adherence: Strict compliance with prescribed regimens
- Symptom diary: Tracking frequency, severity, and triggers
- Action plan: Clear protocol for managing episodes
- Nitroglycerin use: Proper carrying and administration technique
Cardiac Rehabilitation
- Structured exercise training
- Comprehensive education program
- Psychological support
- Risk factor modification
- Improves outcomes and quality of life
Regular Monitoring
- Scheduled follow-up with healthcare providers
- Periodic risk reassessment
- Medication adjustment as needed
- Consideration of progression to invasive management when appropriate
Preventive Screening
- Regular cardiovascular risk assessment
- Blood pressure monitoring
- Lipid screening
- Diabetes screening
- Assessment for other cardiovascular risk factors
- Consideration of advanced screening for high-risk individuals:
- Coronary calcium scoring
- Advanced lipid testing
- Inflammatory markers
10. Global & Regional Statistics
Global Prevalence
Angina affects approximately 112 million people worldwide, representing about 1.6% of the global population. The distribution varies significantly by region, economic development, and demographic factors:
- Global incidence: Approximately 3-4 million new cases annually
- Prevalence by development status:
- High-income countries: Stable or decreasing rates
- Low/middle-income countries: Rapidly increasing rates
- Age-standardized prevalence: Higher in Eastern Europe, Central Asia, Middle East, and North Africa
Regional Variations
Significant regional differences exist in angina prevalence:
North America
- United States: 10-12 million affected (3-4% of adults)
- Canada: Approximately 500,000 affected (1.9% of adults)
- Declining incidence due to improved preventive care
Europe
- Overall prevalence: 2-7% of adult population
- Higher rates in Eastern Europe (up to 7-8%)
- Lower rates in Mediterranean countries (2-3%)
- Significant north-south gradient correlating with cardiovascular risk profiles
Asia
- Dramatic regional variation:
- Eastern Asia: Traditionally lower rates (1-2%) but rapidly increasing
- South Asia: Higher rates (3-5%), particularly India and Pakistan
- Emergence of Western lifestyle patterns contributing to rising prevalence
- Japan: Lowest rates among developed nations (~1%)
Africa
- Limited epidemiological data
- Estimated prevalence: 1-3% in urban areas
- Rapidly increasing with urbanization and lifestyle changes
- Significant under-diagnosis in many regions
Australia/Oceania
- Australia: Similar to Western Europe (~2-3%)
- Pacific Islands: Emerging epidemic with rising obesity rates
Mortality and Economic Impact
- Global mortality: Coronary heart disease (including angina) causes approximately 9 million deaths annually
- Economic burden:
- Direct healthcare costs: $50-100 billion annually worldwide
- Indirect costs from lost productivity: $100-200 billion annually
- Highest economic impact in working-age populations in developing economies
- Healthcare utilization:
- Accounts for 2-3% of all primary care consultations globally
- Major contributor to emergency department visits
- Significant driver of cardiovascular procedure volumes
11. Recent Research & Future Prospects
Latest Research Advancements
Pathophysiological Insights
- Endothelial function: New understanding of the central role of endothelial dysfunction
- Inflammation: Recognition of inflammatory pathways in angina development
- Coronary microvascular dysfunction: Emerging recognition as a distinct entity
- Sex-based differences: Greater understanding of female-specific pathophysiology
Diagnostic Innovations
- Advanced imaging:
- Quantitative perfusion assessment with cardiac MRI
- Hybrid imaging techniques (PET/CT, PET/MRI)
- CT-derived fractional flow reserve (FFRCT)
- Biomarker development:
- Novel cardiac-specific markers of ischemia
- Genetic risk scores for personalized risk assessment
- Artificial intelligence applications:
- Automated ECG interpretation
- Image analysis for early detection
- Risk prediction models
Treatment Innovations
- Novel pharmacotherapy:
- Antianginal medications with unique mechanisms
- Targeted anti-inflammatory approaches
- Metabolism modulators
- Interventional advances:
- Biodegradable stents
- Drug-coated balloons
- Robotic-assisted procedures
- Regenerative approaches:
- Stem cell therapies to repair damaged heart tissue
- Gene therapy for angiogenesis
- Tissue engineering approaches
Ongoing Clinical Trials
Numerous studies are investigating promising approaches:
Pharmacological Trials
- Novel antianginal agents targeting cardiac metabolism
- Anti-inflammatory therapies for coronary artery disease
- Selective sinus node inhibitors
- SGLT2 inhibitors for cardiovascular risk reduction
Interventional Trials
- Comparison of revascularization strategies in different patient subgroups
- Novel stent technologies
- Mechanical circulatory support during high-risk procedures
- Renal denervation for angina
Others
- Digital health interventions for angina management
- Precision medicine approaches based on genetic profiles
- Lifestyle and behavioral interventions
- Comprehensive cardiac rehabilitation models
Future Directions
The evolving landscape suggests several key directions:
Precision Medicine
- Genetic and biomarker-guided therapy selection
- Personalized risk prediction models
- Targeted therapies based on specific pathophysiological mechanisms
- Sex-specific diagnostic and treatment approaches
Technological Integration
- Remote monitoring technologies
- Wearable devices for early detection
- Digital therapeutics complementing traditional treatments
- Virtual cardiac rehabilitation programs
Preventive Focus
- Earlier intervention in at-risk populations
- Population-level approaches to risk factor modification
- Integration of social determinants of health
- Public health strategies addressing evolving lifestyle patterns
12. Interesting Facts & Lesser-Known Insights
Historical and Etymological Insights
- The term “angina pectoris” derives from the Latin “angere” (to strangle) and “pectus” (chest), vividly describing the sensation
- Historical treatments included bloodletting, leeches, and various herbal remedies
- William Heberden, who first described angina, never connected it to the heart, believing it was a primary chest disorder
- Nitroglycerin, a mainstay treatment, was initially developed as an explosive before its medical applications were discovered
Scientific Peculiarities
- “Warm-up angina” or “first-effort angina” describes the phenomenon where initial exertion causes angina, but continued activity at the same level may not
- “Walk-through angina” occurs when angina symptoms appear during initial exertion but disappear with continued effort
- Mental stress can induce myocardial ischemia even without significant coronary stenosis
- Silent ischemia (without pain) affects up to 75% of ischemic episodes in patients with coronary artery disease
- Diabetic patients are more likely to experience silent ischemia due to autonomic neuropathy
Myths and Misconceptions
- Myth: Only elderly people get angina Fact: While more common in older adults, angina can affect people of all ages, including young adults with risk factors or congenital conditions
- Myth: Angina always presents as left-sided chest pain Fact: Presentation varies widely – some experience primarily shortness of breath, fatigue, or discomfort in other locations
- Myth: Women don’t get angina as often as men Fact: Women have similar lifetime risk but often present differently and at older ages due to hormonal protection before menopause
- Myth: If an ECG is normal, there’s no coronary artery disease Fact: A resting ECG is often normal between angina episodes
- Myth: Angina always progresses to heart attack Fact: With proper management, many people with stable angina never experience a heart attack
Special Populations and Considerations
- High-altitude travelers: Reduced oxygen availability increases risk of angina at high altitudes
- Cold-weather athletes: Winter activities can trigger angina due to cold air exposure and physical exertion
- Performers/public speakers: Stress-induced ischemia can affect those with public-facing roles
- Post-menopausal women: Often experience more diffuse symptoms and microvascular disease
- Shift workers: Disrupted circadian rhythms contribute to higher cardiovascular risk
- Young athletes with anomalous coronary arteries: May experience exertional angina despite otherwise excellent health
Angina remains a critical cardiovascular condition that serves both as a symptom of underlying disease and a warning sign for more serious cardiac events. With advances in understanding, diagnosis, and treatment, the prognosis for patients with angina has improved dramatically in recent decades. However, the global burden continues to grow with aging populations and increasing prevalence of risk factors in developing regions. Continued research, improved preventive strategies, and novel therapeutic approaches offer hope for further reducing the impact of this common but serious condition.