
⚠️ Disclaimer: The information provided in this article is for educational purposes only and does not constitute medical advice. RevisionTown does not provide diagnosis, treatment, or medical recommendations. Always consult a qualified healthcare professional regarding any medical condition, symptoms, or concerns.
Read More – 🏥 Medical Disclaimer
1. Overview
What is Ulcerative Colitis Treatment?
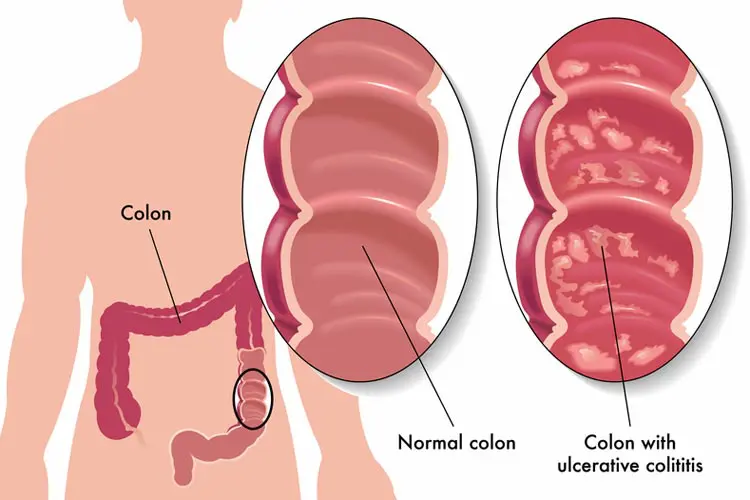
Ulcerative colitis (UC) treatment encompasses the medical, surgical, and lifestyle interventions used to manage ulcerative colitis—a chronic inflammatory bowel disease primarily affecting the colon and rectum. The treatment aims to control inflammation, alleviate symptoms, maintain remission, and prevent complications through a multimodal approach.
Definition & Affected Body Parts/Organs:
Definition: Ulcerative colitis treatment is the integrated approach designed to reduce inflammation in the colonic mucosa, ease gastrointestinal symptoms, and improve long-term outcomes for patients.
Affected Areas: The primary site of involvement is the colon and rectum. However, complications can involve other organ systems indirectly as a result of chronic inflammation and malabsorption.
Prevalence and Significance:
Global Impact: Ulcerative colitis is less common than its counterpart Crohn’s disease but remains a significant cause of morbidity among inflammatory bowel diseases. Prevalence rates vary by region, with higher rates observed in North America and Europe.
Clinical and Economic Significance: The condition contributes to a considerable healthcare burden due to its chronic nature, associated hospitalizations, and need for long-term therapy. Early intervention and appropriate treatment are critical to reducing complications and maintaining patients’ quality of life.
2. History & Discoveries
Initial Identification and Discovery:
Early Observations: The clinical characteristics of ulcerative colitis were first described in the 19th century as physicians began to differentiate various forms of colonic inflammation. However, it was during the mid-20th century that ulcerative colitis was distinctly classified from other inflammatory bowel diseases.
Pioneering Contributions: No single individual “discovered” ulcerative colitis treatment; rather, the evolution of its management is attributed to cumulative clinical observations and advancements in pathology, endoscopy, and immunology over several decades.
Major Discoveries and Breakthroughs:
Evolution of Diagnostic Tools: Early reliance on clinical history and rudimentary imaging was later complemented by colonoscopy and histopathology, enabling more precise diagnosis and monitoring of disease activity.
Therapeutic Milestones: The introduction of sulfasalazine in the mid-20th century marked a major shift. Later, the development of corticosteroids and immunomodulators (e.g., azathioprine, 6-mercaptopurine) further enhanced treatment efficacy. More recently, biologic agents (such as anti-TNF therapies) have revolutionized the management of moderate-to-severe cases.
Advances in Surgical Techniques: Surgical approaches have evolved from radical colectomy to more conservative, restorative procedures such as ileal pouch-anal anastomosis (IPAA), improving patient quality of life.
Evolution of Medical Understanding:
Medical insight into ulcerative colitis has moved from viewing the disease as a solely localized colonic disorder to understanding it as a complex, immune-mediated systemic condition. Advances in molecular biology, genetics, and immunology have refined treatment strategies and improved prognostic outcomes.
3. Symptoms
Early Symptoms vs. Advanced-Stage Symptoms:
Early Symptoms:
Mild to moderate abdominal discomfort or cramping
Frequent, sometimes urgent, bowel movements with mild bloody diarrhea
Tenesmus (a feeling of incomplete evacuation)
Low-grade fever or malaise in some cases
Advanced-Stage Symptoms:
Persistent and severe bloody diarrhea
Weight loss and significant fatigue
Abdominal pain that may become debilitating
Complications such as anemia, dehydration, or even signs of systemic infection
Common vs. Rare Symptoms:
Common Symptoms: Rectal bleeding, diarrhea, and urgency are the hallmarks of ulcerative colitis.
Less Common/Extraintestinal Manifestations: Some patients experience joint pain, skin lesions (erythema nodosum, pyoderma gangrenosum), and eye inflammation (uveitis).
Progression Over Time:
Ulcerative colitis typically follows a relapsing–remitting course. Early stages may present with infrequent flare-ups that are manageable with medication, but over time, repeated inflammation may lead to mucosal damage, fibrosis, and an increased risk of colorectal cancer.
4. Causes
Biological and Environmental Causes:
Immunologic Dysfunction: Central to the pathogenesis is an abnormal immune response triggered by environmental antigens in genetically predisposed individuals.
Microbial Interactions: Dysbiosis—or an imbalance in the gut microbiota—has been implicated in perpetuating mucosal inflammation.
Genetic and Hereditary Factors:
Family studies demonstrate a genetic predisposition, with certain gene mutations (e.g., those related to immune regulation) increasing susceptibility. The genetics are complex and polygenic, involving interactions between multiple loci.
Known Triggers or Exposure Risks:
Environmental Triggers: Factors such as diet, stress, and smoking (though smoking has a more protective effect in ulcerative colitis compared to Crohn’s disease) may modulate disease activity.
Other Factors: Use of nonsteroidal anti-inflammatory drugs (NSAIDs) and certain infections may trigger exacerbations in susceptible individuals.
5. Risk Factors
Who is Most at Risk?
Age: Ulcerative colitis most commonly presents in young adults, though it can occur at any age.
Gender: The condition affects both genders relatively equally, with some regional variations reported.
Family History: A positive family history is a strong risk indicator.
Environmental, Occupational, and Genetic Factors:
Environmental: Lifestyle factors, including diet and stress, play a role. Urban living and industrialization have been associated with a higher prevalence.
Occupational: While no specific occupation has been conclusively linked, high-stress environments and sedentary lifestyles may contribute indirectly.
Pre-existing Conditions: Certain autoimmune disorders are more common in patients with ulcerative colitis.
6. Complications
Complications from Ulcerative Colitis:
Colonic Complications: Chronic inflammation increases the risk of colorectal cancer. Other complications include the development of strictures, perforations, and toxic megacolon.
Nutritional Deficiencies: Persistent diarrhea and malabsorption can lead to deficiencies in vitamins and minerals, such as iron and vitamin B12, and subsequent anemia.
Extraintestinal Manifestations: Long-term inflammation may trigger complications in joints, skin, eyes, and the liver (e.g., primary sclerosing cholangitis).
Long-Term Impact on Organs and Overall Health:
Continuous mucosal damage and inflammation compromise colon integrity and overall gastrointestinal function, which may significantly impact quality of life and overall health outcomes.
Potential Disability or Fatality Rates:
Although ulcerative colitis itself is rarely directly fatal, complications like toxic megacolon and colorectal cancer can increase mortality, particularly if the disease remains uncontrolled over many years.
7. Diagnosis & Testing
Common Diagnostic Procedures:
Clinical Examination: A detailed patient history with emphasis on symptom chronology and family history is fundamental.
Endoscopy: Colonoscopy remains the gold standard for diagnosis, allowing direct visualization of mucosal inflammation and obtaining biopsy samples for histopathologic confirmation.
Medical Tests:
Imaging: Techniques like CT or MRI may be employed to assess complications or extent of colonic involvement in severe cases.
Laboratory Studies: Blood tests (including complete blood count, inflammatory markers such as CRP, and liver function tests) aid in evaluating disease activity and ruling out other causes.
Biopsies: Histological examination confirms the diagnosis, revealing characteristic mucosal ulceration and inflammation.
Early Detection Methods and Their Effectiveness:
Advances in endoscopic techniques, including high-definition imaging and chromoendoscopy, have improved early detection and the ability to monitor disease progression. Regular surveillance is especially recommended in long-standing cases due to cancer risk.
8. Treatment Options
Standard Treatment Protocols:
Pharmacologic Therapies:
Aminosalicylates: Medications like mesalamine are often used as first-line agents in mild to moderate disease for their anti-inflammatory effects.
Corticosteroids: Employed during acute flare-ups to quickly reduce inflammation, though their long-term use is limited by side effects.
Immunomodulators: Agents such as azathioprine or 6-mercaptopurine help maintain remission in more severe cases.
Biologic Therapies: Anti-TNF agents (e.g., infliximab, adalimumab), as well as newer biologics targeting integrins or interleukin pathways, have broadened treatment options for refractory disease.
Surgical Interventions:
In patients who do not respond to medical therapy or who develop complications (like dysplasia or toxic megacolon), colectomy offers a curative option. Surgical approaches have evolved to balance complete disease removal with quality of life considerations, including restorative procedures such as ileal pouch-anal anastomosis (IPAA).
Emerging Treatments and Clinical Trials:
Targeted Biologics and Small Molecule Inhibitors: Ongoing research is focused on therapies that more precisely modulate the immune response and reduce systemic side effects.
Stem Cell and Regenerative Therapies: Early-phase clinical trials are exploring how cellular therapies might help repair damaged mucosa and restore normal immune function.
Microbiome Interventions: Fecal microbiota transplantation (FMT) and other approaches to restore gut microbial balance are being evaluated as complementary treatments.
9. Prevention & Precautionary Measures
Preventing Ulcerative Colitis and Its Exacerbations:
Primary Prevention: While the exact cause of ulcerative colitis remains multifactorial and not entirely preventable, lifestyle modifications—such as adopting a balanced, anti-inflammatory diet and managing stress—may mitigate risk.
Secondary Prevention: Early diagnosis and proactive treatment are key in preventing disease flares and complications. Regular monitoring via colonoscopy is recommended for long-term patients to screen for dysplasia and early cancer.
Lifestyle and Environmental Precautions:
Diet: Some patients benefit from diets low in processed foods and high in fiber; however, dietary recommendations should be individualized.
Stress Reduction and Physical Activity: Stress management techniques and regular exercise may help reduce flare frequency and improve overall well-being.
Vaccination and Preventive Screenings: Although no vaccine exists for ulcerative colitis, routine immunizations and screenings (including colonoscopic surveillance) are integral parts of comprehensive care.
10. Global & Regional Statistics
Incidence and Prevalence Rates Globally:
Global Overview: Ulcerative colitis is more prevalent in developed countries, with significant incidence reported in North America, Western Europe, and Australasia. Incidence is gradually increasing in developing countries, likely due to westernized lifestyle shifts.
Mortality and Survival Rates:
Outcomes: With effective medical and surgical management, most patients achieve a near-normal life expectancy. However, the risk of colorectal cancer in long-standing disease remains a vital concern.
Country-wise Comparison and Trends:
Variations exist between countries and regions, influenced largely by environmental factors, genetic predisposition, and access to healthcare. High-resource regions tend to have better outcomes due to early detection and advanced treatment modalities.
11. Recent Research & Future Prospects
Latest Advancements in Treatment and Research:
Innovative Drug Therapies: Novel biologics and small-molecule drugs are under investigation, aiming to target specific inflammatory pathways with greater precision.
Personalized Medicine: Genetic and biomarker studies are driving the development of individualized treatment approaches, improving the predictability of therapy response and minimizing adverse effects.
Ongoing Studies and Future Medical Possibilities:
Clinical Trials: New studies are underway assessing dual-acting drugs, combinations of immunomodulators with biologics, and non-pharmacologic interventions including microbiome restoration.
Potential Curative Approaches: Research into regenerative medicine, gene therapy, and stem cell applications holds promise for transformative advancements in ulcerative colitis management over the coming years.
12. Interesting Facts & Lesser-Known Insights
Uncommon Knowledge About Ulcerative Colitis Treatment:
Extraintestinal Manifestations: Beyond the colon, UC can be associated with arthritis, skin disorders, and ocular problems, underscoring the systemic impact of the condition.
Smoking Paradox: Unlike many diseases worsened by smoking, UC often shows a paradoxical improvement in smokers, although smoking is not advised due to its overall health risks and effects on other conditions.
Myths vs. Medical Facts: A common myth is that ulcerative colitis is solely diet-related. In reality, it is a complex interplay of genetic, environmental, and immunological factors.
Professional Impact: The chronic nature of ulcerative colitis can significantly affect work and social life, making tailored support systems and workplace accommodations an important aspect of overall care.
References
Overview: Information on definition, affected organs, and prevalence is based on clinical guidelines provided by the American Gastroenterological Association (AGA) and studies published in leading gastroenterology journals.
History & Discoveries: Historical perspectives and breakthroughs have been compiled from academic reviews and authoritative texts on inflammatory bowel disease.
Symptoms: Descriptions of symptom progression are corroborated by consensus documents and longitudinal studies on ulcerative colitis.
Causes: Insights on immunologic, genetic, and environmental factors are drawn from peer-reviewed articles in gastroenterology and immunology literature.
Risk Factors: Data are based on epidemiological studies and research from national registries and health organizations such as the CDC and WHO.
Complications: Information about complications and long-term impact comes from clinical outcome studies and systematic reviews.
Diagnosis & Testing: Diagnostic protocols follow recommendations of the AGA, supplemented by recent advances in endoscopic and imaging technologies.
Treatment Options: Treatment strategies are based on current clinical practice guidelines, meta-analyses, and emerging data from clinical trials.
Prevention & Precautionary Measures: Preventive strategies and lifestyle interventions reflect public health policies and guidelines from leading health institutions.
Global & Regional Statistics: Epidemiological statistics are sourced from international databases and registry studies.
Recent Research & Future Prospects: Future directions are informed by the latest clinical research updates and emerging trends published in specialty journals.
Interesting Facts & Lesser-Known Insights: Nuanced insights and myth debunking are taken from expert reviews and patient-oriented educational resources.
This detailed report outlines the multifaceted approach to ulcerative colitis treatment—from historical breakthroughs to the frontiers of modern therapeutic research. Maintaining an emphasis on early diagnosis, personalized treatment, and proactive management is vital in optimizing outcomes and improving patients’ quality of life. Stay focused, innovative, and informed as the evolving landscape of ulcerative colitis care continues to drive forward-thinking, evidence-based clinical practice.