
⚠️ Disclaimer: The information provided in this article is for educational purposes only and does not constitute medical advice. RevisionTown does not provide diagnosis, treatment, or medical recommendations. Always consult a qualified healthcare professional regarding any medical condition, symptoms, or concerns.
Read More – 🏥 Medical Disclaimer
Comprehensive Report on Whooping Cough (Pertussis)
1. Overview
What is Whooping Cough?
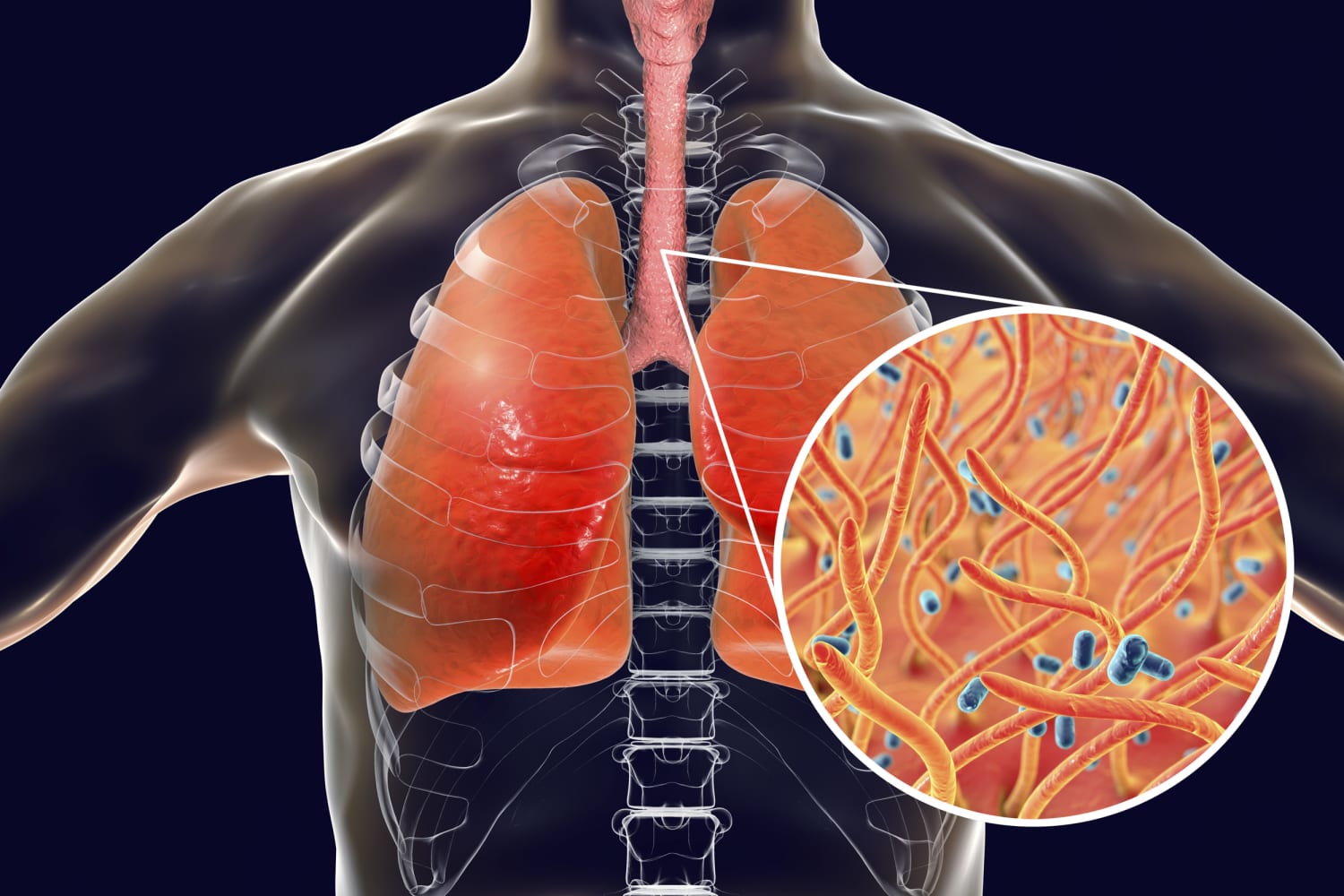
Whooping cough, clinically known as pertussis, is a highly contagious acute respiratory infection caused by the bacterium Bordetella pertussis. The disease is characterized by severe paroxysmal coughing episodes that typically end with a distinctive “whooping” sound when the patient rapidly inhales after a coughing fit. This characteristic sound is the origin of the common name “whooping cough,” though it may not be present in all cases, particularly in infants, adolescents, and adults.
Pertussis is classified as a notifiable disease in most countries due to its public health significance. Despite the availability of effective vaccines, it remains one of the leading causes of vaccine-preventable deaths worldwide, particularly in infants too young to be fully vaccinated.
Affected Body Parts/Organs
Whooping cough primarily affects the respiratory system, with specific impacts on:
- Respiratory Tract Epithelium: The bacteria attach specifically to the ciliated epithelial cells in the respiratory tract.
- Bronchi and Bronchioles: Inflammation and damage to these airways lead to the characteristic coughing.
- Trachea: Inflammation extends to the trachea, contributing to the coughing paroxysms.
- Lungs: Secondary complications can involve the lung parenchyma, particularly pneumonia.
- Systemic Effects: While primarily a respiratory infection, the toxins produced by B. pertussis can have systemic effects, potentially affecting:
- Cardiovascular system (in severe cases)
- Central nervous system (through hypoxia during coughing episodes or direct toxin effects)
- Immune system (via modulation of host immune responses)
Prevalence and Significance
Despite high global vaccination coverage, pertussis remains a significant public health concern:
- Global Burden: The World Health Organization (WHO) estimates 24.1 million cases of pertussis and about 160,700 deaths in children younger than 5 years annually, with the majority occurring in developing countries.
- Resurgence: Many developed countries have reported a resurgence of pertussis cases since the 1980s, even in highly vaccinated populations.
- Cyclical Pattern: Pertussis naturally demonstrates a cyclical pattern with peaks occurring every 3-5 years, even in vaccinated communities.
- Age Distribution Shift: In countries with established vaccination programs, the epidemiological pattern has shifted toward increased cases in adolescents and adults, who serve as reservoirs for transmission to vulnerable infants.
- Economic Impact: The estimated economic burden of pertussis exceeds $2 billion annually in direct and indirect costs in the United States alone.
- Vaccine Effectiveness Concerns: Waning immunity from acellular pertussis vaccines has contributed to ongoing transmission, even in highly vaccinated populations.
- Infant Mortality: Infants under 1 year, particularly those younger than 6 months, bear the greatest burden of mortality and serious complications.
Pertussis remains a global public health priority due to its significant morbidity and mortality, particularly in young infants, and the challenges of achieving and maintaining sufficient population immunity to prevent transmission.
2. History & Discoveries
Early Recognition and Description
The history of whooping cough spans several centuries, with progressively increasing understanding of the disease:
- First Clinical Descriptions: The earliest recognizable description of pertussis dates to 1578 when French physician Guillaume de Baillou (also known as Ballonius) documented an epidemic in Paris. He provided the first clear clinical description of the disease, though he did not name it.
- Term Origins: The term “pertussis” was first used by British physician Thomas Sydenham in 1670, derived from Latin “per” (intensive) and “tussis” (cough). The common name “whooping cough” emerged from the distinctive sound made when patients inhale after coughing paroxysms.
- Early Epidemics: By the 16th-18th centuries, whooping cough was recognized as a significant cause of childhood mortality throughout Europe, with documented epidemics occurring regularly.
- Initial Theories: Until the late 19th century, pertussis was variously attributed to miasmas, “bad air,” or unspecified contagions, reflecting the pre-germ theory understanding of disease.
Discovery of the Causative Agent
- Jules Bordet and Octave Gengou (1906): These Belgian scientists successfully isolated the causative bacterium, which they named Bordetella pertussis (initially called Haemophilus pertussis). This groundbreaking discovery occurred at the Pasteur Institute in Brussels.
- Culture Medium Development: Bordet and Gengou developed a special potato-glycerol-blood medium that was necessary to grow the fastidious bacteria, which was a significant technical achievement that enabled further research.
- Identification of Toxins: In the 1940s-1950s, researchers identified pertussis toxin, adenylate cyclase toxin, tracheal cytotoxin, and other virulence factors that explain the pathogenesis of the disease.
- Pearl Kendrick and Grace Eldering (1930s-1940s): These American public health researchers made substantial contributions to understanding pertussis epidemiology and developing the first effective vaccines.
Vaccine Development and Evolution
- First Whole-Cell Vaccine (1914): The first crude whole-cell pertussis vaccines were developed by Thorvald Madsen in Denmark, though with limited effectiveness.
- Improved Whole-Cell Vaccines (1940s): Pearl Kendrick and Grace Eldering developed and tested the first effective whole-cell pertussis vaccines in Michigan, USA.
- Combined DTP Vaccine (1948): Combination of diphtheria, tetanus, and pertussis antigens into a single vaccine (DTP) greatly improved vaccination implementation.
- Acellular Pertussis Vaccines (1970s-1980s): Developed primarily in Japan and later adopted worldwide, these vaccines contain purified pertussis antigens rather than whole killed bacteria, resulting in fewer side effects.
- Adolescent and Adult Formulations (1990s-2000s): Development of Tdap vaccines with reduced antigen content for adolescent and adult boosters to address waning immunity.
- Maternal Immunization (2010s): Recognition of the effectiveness of vaccinating pregnant women to protect newborns through passive antibody transfer.
Evolution of Medical Understanding
- 1950s-1960s: Widespread implementation of whole-cell pertussis vaccines led to dramatic decreases in disease incidence in developed countries.
- 1970s-1980s: Safety concerns about whole-cell vaccines led to decreased vaccination rates in some countries and subsequent pertussis resurgence.
- 1990s: Transition to acellular pertussis vaccines in most developed countries to address safety concerns.
- 2000s-Present: Recognition of waning immunity with acellular vaccines and changing epidemiology of pertussis, with increased cases in adolescents and adults.
- Molecular Understanding: Advances in molecular biology have enabled detailed understanding of pertussis pathogenesis, including how the bacteria attach to respiratory epithelium, evade immune responses, and cause disease through various toxins.
- Transmission Dynamics: Improved understanding of transmission patterns, including the role of asymptomatic and mildly symptomatic carriers in disease spread.
- Genomic Evolution: Recent genomic studies have revealed changes in circulating B. pertussis strains, possibly in response to vaccine selection pressure, with potential implications for vaccine effectiveness.
The history of pertussis reflects the interplay between scientific discovery, public health interventions, and the adaptability of pathogens, with ongoing challenges in achieving optimal disease control despite significant advances in understanding and prevention.
3. Symptoms
Clinical Stages of Pertussis
Whooping cough typically progresses through three distinct clinical stages, each with characteristic symptoms:
1. Catarrhal Stage (Early Symptoms)
- Duration: 1-2 weeks
- Symptoms:
- Mild upper respiratory symptoms resembling the common cold
- Low-grade fever (usually minimal)
- Runny nose (rhinorrhea)
- Nasal congestion
- Mild, occasional cough
- Sneezing
- Tearing (lacrimation)
- Mild conjunctival injection (red eyes)
- Malaise and fatigue
- Significance: Highly contagious during this stage but often misdiagnosed as a common cold or viral upper respiratory infection
2. Paroxysmal Stage (Advanced Symptoms)
- Duration: 2-6 weeks, sometimes longer
- Characteristic Symptoms:
- Severe paroxysmal coughing fits (bursts of rapid, consecutive coughs)
- Post-tussive “whoop” (inspiratory gasp) in children >6 months
- Post-tussive vomiting or gagging
- Cyanosis (bluish discoloration) during coughing episodes
- Apnea (especially in infants)
- Exhaustion after coughing episodes
- Facial and conjunctival petechiae (small red spots) from coughing strain
- Subconjunctival hemorrhages
- Sweating episodes
- Distress and anxiety before coughing paroxysms
- Presentation Variations: The classic “whoop” may be absent in:
- Infants younger than 6 months (who may present with apnea instead)
- Adults and adolescents (who may have a persistent hacking cough)
- Previously vaccinated individuals (who often have milder disease)
3. Convalescent Stage
- Duration: Weeks to months (typically 2-3 weeks but can last up to 3 months)
- Symptoms:
- Gradual reduction in coughing severity and frequency
- Persistent cough that may worsen with respiratory infections
- Recovery of normal energy levels
- Susceptibility to other respiratory infections
- Resolution of paroxysms and whooping
Symptom Variations by Age Group
Infants (<1 year)
- Atypical presentations are common
- May not develop the characteristic “whoop”
- Apnea and cyanosis may be the primary presentations
- Short, shallow coughs rather than prolonged paroxysms
- Feeding difficulties and weight loss
- Gasping or gagging episodes
- Bradycardia (slow heart rate) during coughing episodes
- Higher risk of life-threatening complications
Young Children (1-10 years)
- Most likely to present with classic symptoms
- Pronounced “whoop” after coughing paroxysms
- Visible distress before coughing episodes
- Vomiting after coughing is common
- More prolonged recovery period
- May have characteristic ulcer on the frenulum from trauma during coughing
Adolescents and Adults
- Often unrecognized or misdiagnosed
- Persistent, prolonged cough (often >2 weeks)
- Often lack the characteristic “whoop”
- May have paroxysmal cough, especially at night
- Post-tussive vomiting less common than in children but still occurs
- Sleep disturbance due to coughing
- Rib fractures in severe cases
- Urinary incontinence during coughing (particularly in women)
Rare or Unusual Symptoms
- Neurological Symptoms:
- Seizures (usually from hypoxia during coughing episodes)
- Altered consciousness
- Encephalopathy (rare but serious)
- Severe Complications:
- Pneumothorax (collapsed lung)
- Subcutaneous emphysema (air under the skin)
- Inguinal or umbilical hernias from coughing strain
- Rectal prolapse (especially in infants)
- Atypical Presentations:
- “Silent pertussis” with minimal cough but persistent apnea (in young infants)
- Prolonged fever (suggests secondary infection)
- Hemoptysis (coughing up blood) in severe cases
Symptom Progression Over Time
- Week 1-2: Mild respiratory symptoms indistinguishable from common colds
- Week 3-8: Development and peak of paroxysmal coughing
- Paroxysms typically increase in frequency and severity over the first 1-2 weeks
- Peak symptom severity usually occurs 2-3 weeks after onset
- Gradually decreasing severity through weeks 4-6
- Weeks 8-12+: Convalescent phase with decreasing symptoms
- Persistent cough that can last for months in some cases
- Vulnerability to “cough triggers” (cold air, exercise, other respiratory infections)
- Recurrence of paroxysmal coughing with subsequent respiratory infections
The classic symptom progression described above represents typical cases, but the clinical course can vary significantly based on age, vaccination status, comorbidities, and timely initiation of appropriate antibiotic therapy.
4. Causes
Primary Causative Agent
Whooping cough is caused by infection with the bacterium Bordetella pertussis, a fastidious gram-negative coccobacillus that exclusively infects humans. It is a strictly human pathogen with no animal or environmental reservoir.
Bordetella Species Causing Pertussis-like Illness
- B. pertussis: Primary cause of classic whooping cough
- B. parapertussis: Causes a milder form of pertussis-like illness
- B. holmesii: Occasionally causes pertussis-like symptoms, particularly in immunocompromised patients
- B. bronchiseptica: Primarily an animal pathogen but rarely causes respiratory infections in humans
Pathophysiology and Disease Mechanism
Attachment and Colonization
- Initial Contact: B. pertussis enters the respiratory tract via aerosolized droplets.
- Adhesion Factors: Several bacterial adhesins facilitate attachment to ciliated epithelial cells:
- Filamentous hemagglutinin (FHA)
- Pertactin (PRN)
- Fimbriae (FIM)
- Pertussis toxin (PT)
- Colonization: Bacteria multiply on the ciliated epithelium of the respiratory tract but do not typically invade deeper tissues.
Toxin Production and Effects
B. pertussis produces several toxins that contribute to disease pathogenesis:
- Pertussis Toxin (PT):
- An A-B toxin that catalyzes ADP-ribosylation of G proteins
- Disrupts cellular signaling pathways
- Impairs immune cell responses
- Causes lymphocytosis (increased lymphocytes in blood)
- Enhances histamine sensitivity
- Adenylate Cyclase Toxin (ACT):
- Enters host cells and converts ATP to cyclic AMP
- Impairs neutrophil and macrophage function
- Inhibits phagocytosis and bacterial killing
- Promotes bacterial survival during early infection
- Tracheal Cytotoxin (TCT):
- Damages ciliated epithelial cells
- Causes cilia stasis and eventual death of ciliated cells
- Impairs mucociliary clearance
- Contributes to persistent cough
- Dermonecrotic Toxin (DNT):
- Activates small GTPases
- Causes vasoconstriction
- Role in clinical disease less clear than other toxins
- Lipopolysaccharide (LPS):
- Endotoxin in the bacterial cell wall
- Induces inflammatory responses
- Contributes to local respiratory inflammation
Disease Progression
- Epithelial Damage: Toxins damage ciliated epithelial cells, impairing mucociliary clearance.
- Mucus Accumulation: Damage to ciliated cells leads to accumulation of mucus and debris in airways.
- Inflammatory Response: Host inflammatory response to infection causes airway edema and additional damage.
- Cough Reflex Stimulation: Accumulated secretions and inflammation trigger the cough reflex.
- Paroxysmal Coughing: The characteristic coughing occurs as the body attempts to clear mucus from the airways.
- “Whooping” Sound: The rapid inspiration through narrowed glottis after coughing creates the characteristic sound.
Transmission Mechanisms
- Person-to-Person: Exclusively transmitted from human to human via respiratory droplets.
- Highly Contagious: Attack rates of 80-90% among susceptible household contacts.
- Incubation Period: Typically 7-10 days (range: 5-21 days).
- Contagious Period:
- Most contagious during the catarrhal (early) stage before severe coughing begins
- Contagiousness decreases substantially after 3 weeks of illness
- Antibiotic treatment reduces contagiousness to approximately 5 days after initiation
- Transmission Variables:
- Proximity and duration of contact with infected individuals
- Vaccination status of exposed individuals
- Timing of exposure relative to disease stage
- Environmental conditions (indoor, crowded settings increase risk)
Environmental Factors Influencing Spread
- Seasonal Patterns: In temperate climates, pertussis incidence typically peaks in summer and autumn months.
- Crowded Settings: Transmission is enhanced in:
- Schools and daycare centers
- Healthcare facilities
- Household settings
- Crowded urban environments
- Indoor Air Quality: Poor ventilation in indoor spaces increases transmission risk.
- Vaccination Coverage: Community-level vaccination rates significantly impact disease spread.
- Population Density: Higher population density correlates with increased transmission opportunities.
- Healthcare Access: Limited access to prompt diagnosis and treatment extends contagious periods.
Genetic and Hereditary Factors
Unlike some diseases, pertussis does not have strong direct genetic or hereditary components in terms of susceptibility. However, several genetic factors may influence infection risk, disease severity, and vaccine response:
Host Genetic Factors
- Immune System Genetic Variations:
- Toll-like receptor polymorphisms may affect recognition of bacterial components
- HLA variants influence adaptive immune responses to infection or vaccination
- Cytokine gene polymorphisms may affect inflammatory responses
- Genetic Immunodeficiencies: Primary immunodeficiency disorders increase susceptibility and severity.
- Twin Studies: Suggest some heritable component to vaccine response and antibody production.
Pathogen Genetic Factors
- Strain Variation: Genetic changes in circulating B. pertussis strains have been documented:
- Antigenic drift in key proteins (pertactin, pertussis toxin)
- Gene loss and genetic rearrangements
- Adaptations potentially influenced by vaccine selection pressure
- Vaccine Antigen Mismatch: Some circulating strains lack antigens contained in vaccines (e.g., pertactin-deficient strains).
The interplay between host and pathogen genetics represents an evolving area of research in understanding pertussis epidemiology and developing improved prevention strategies.
5. Risk Factors
Demographic Risk Factors
Age
- Infants (<1 year): Highest risk group, particularly those <6 months old who have not received the full primary vaccination series
- Young Children (1-4 years): Substantial risk, especially if under-vaccinated
- Adolescents (11-18 years): Increasing risk due to waning immunity from childhood vaccination
- Adults: Often unrecognized reservoir of infection, with increasing cases due to waning immunity
- Elderly: May have severe disease due to comorbidities and decreased immune function
Gender
- Generally Equal Risk: No significant gender predilection in pertussis susceptibility
- Possible Differences:
- Some studies suggest slightly higher incidence in females during adolescence and adulthood
- Pregnant women may have increased susceptibility due to immune system modulation
Geographic and Seasonal Factors
- Developing Countries: Higher burden due to lower vaccination coverage
- Urban vs. Rural: Generally higher incidence in urban settings due to population density
- Seasonal Variation: In temperate climates, peaks typically occur in summer and fall months
- Regional Outbreaks: Localized outbreaks occur even in highly vaccinated populations, particularly in schools and institutions
Vaccination Status
- Unvaccinated Individuals: 4-15 times higher risk compared to fully vaccinated persons
- Under-vaccinated Individuals: Those who haven’t completed the primary series have substantially increased risk
- Waning Immunity:
- Protection from acellular pertussis vaccine decreases substantially 2-4 years after last dose
- Whole-cell vaccine (still used in some countries) may provide longer-lasting protection
- Even fully vaccinated individuals become susceptible over time without boosters
- Time Since Last Dose: Risk increases with time elapsed since last pertussis-containing vaccine
- Vaccine Refusal Clusters: Geographic areas with high vaccine refusal rates experience more frequent and larger outbreaks
Exposure Factors
- Household Contacts: 80-90% attack rate among unvaccinated household contacts
- School/Daycare Exposure: High-risk settings for transmission
- Healthcare Settings: Both patients and healthcare workers at increased risk
- Crowded Living Conditions: Dormitories, military barracks, detention facilities
- Contact with Infants/Children: Increased exposure risk for parents, grandparents, childcare workers
- Healthcare Workers: Occupational exposure risk, particularly in pediatric and emergency settings
Pre-existing Health Conditions
- Immunodeficiency:
- Primary immunodeficiency disorders
- HIV/AIDS
- Immunosuppressive medications
- Transplant recipients
- Chronic Respiratory Conditions:
- Asthma
- COPD
- Cystic fibrosis
- Bronchiectasis
- Neurological Disorders:
- Conditions with impaired cough or swallow reflexes
- Neuromuscular disorders affecting respiratory function
- Pregnancy: Associated with more severe disease and complications
- Malnutrition: Impairs immune response and increases disease severity
- Concurrent Respiratory Infections: May increase susceptibility or disease severity
Social and Environmental Risk Factors
- Socioeconomic Status: Lower socioeconomic status associated with decreased vaccination rates and increased risk
- Healthcare Access: Limited access to preventive care and vaccination services
- Education Level: Lower parental education associated with decreased vaccination rates
- Cultural and Religious Factors: Certain cultural or religious beliefs may influence vaccination acceptance
- Vaccine Hesitancy: Growing concerns about vaccine safety have led to decreased vaccination rates in some communities
- Institutional Settings:
- Schools and universities
- Long-term care facilities
- Correctional facilities
- Military training centers
Risk Factors for Severe Disease and Complications
- Young Age: Infants <6 months at highest risk for severe complications and death
- Prematurity: Premature infants have higher risk for severe disease
- Low Birth Weight: Associated with more severe disease and complications
- Underlying Pulmonary Conditions: Increase risk of respiratory complications
- Malnutrition: Impairs immune response and recovery
- Immune Compromise: Results in prolonged or more severe illness
- Delayed Diagnosis and Treatment: Antibiotics are most effective when started early in the disease course
- Concomitant Infections: Particularly respiratory viral or bacterial co-infections
Understanding these risk factors helps in targeting prevention strategies, identifying high-risk individuals for prophylaxis, and implementing appropriate vaccination programs to protect the most vulnerable populations.
6. Complications
Respiratory Complications
Direct Respiratory Complications
- Pneumonia: Most common severe complication
- Primary pertussis pneumonia from B. pertussis infection
- Secondary bacterial pneumonia (often Streptococcal or Staphylococcal)
- Occurs in 5-9% of all cases, higher in infants (20%)
- Atelectasis: Collapse of lung segments due to mucus plugging
- Bronchiectasis: Permanent dilation of bronchi from inflammation (rare but serious)
- Pneumothorax: Rupture of alveoli leading to air in pleural space from violent coughing
- Subcutaneous Emphysema: Air dissection into soft tissues from alveolar rupture
- Pneumomediastinum: Air in the mediastinum from respiratory tract rupture
- Respiratory Failure: Requires mechanical ventilation, occurs primarily in infants
Apnea and Breathing Abnormalities
- Apnea: Breathing stops, particularly dangerous in infants
- May be the presenting symptom in young infants
- Can occur without significant coughing in this age group
- Cyanosis: Blue discoloration during coughing paroxysms from oxygen deprivation
- Persistent Pulmonary Hypertension: Particularly in infants with severe disease
Neurological Complications
- Hypoxic Encephalopathy: Brain damage from oxygen deprivation during coughing or apnea
- Seizures: Occur in 1-2% of infants with pertussis
- May be due to hypoxia, toxin effects, or fever
- May lead to long-term neurological sequelae
- Pertussis Encephalopathy: Acute brain inflammation (rare but serious)
- Intracranial Hemorrhage: From increased pressure during coughing
- Subarachnoid Hemorrhage: Bleeding between the brain and surrounding membranes
- Subdural Hematoma: Blood collection between the brain and dura mater
- Long-term Neurological Sequelae: Including developmental delays and epilepsy
Physical Complications from Severe Coughing
- Rib Fractures: From violent coughing, more common in adults
- Abdominal Muscle Tears: From repeated forceful contractions
- Inguinal or Umbilical Hernias: Protrusion of intestine through weakened areas
- Rectal Prolapse: Protrusion of rectal tissue through the anus, more common in infants
- Conjunctival Hemorrhages: Bleeding in the eyes from increased pressure
- Epistaxis: Nosebleeds during coughing episodes
- Petechiae: Small red or purple spots from burst capillaries, typically on face and upper chest
- Ulcer of the Frenulum: In infants and young children from trauma against teeth during coughing
Metabolic and Systemic Complications
- Dehydration: From vomiting, decreased oral intake, and increased metabolic demands
- Malnutrition: Due to vomiting and increased caloric expenditure from coughing
- Weight Loss: Particularly concerning in infants and young children
- Metabolic Alkalosis: From repeated vomiting
- Urinary Incontinence: During coughing paroxysms, particularly in women
- Disrupted Sleep Patterns: Leading to fatigue and impaired quality of life
- Post-tussive Syncope: Fainting after coughing episodes due to changes in intrathoracic pressure
Long-term Sequelae
- Reactive Airway Disease: Increased risk of asthma-like symptoms for months to years
- Persistent Cough Syndrome: Cough lasting months after the acute infection resolves
- Bronchiectasis: Permanent airway damage (rare)
- Exercise Intolerance: Reduced lung function affecting physical activity
- Neurodevelopmental Abnormalities: Following severe neurological complications
- Post-Pertussis Syndrome: Recurrent episodes of paroxysmal coughing with subsequent respiratory infections
Complications in Special Populations
Infants (<1 year)
- Highest risk for severe complications and death
- Apnea and respiratory failure are major concerns
- Pulmonary hypertension more common
- Higher risk of seizures and encephalopathy
- Feeding difficulties leading to dehydration and malnutrition
Pregnant Women
- Increased risk of hospitalization
- Preterm labor
- Pregnancy loss
- Maternal complications from severe coughing (rib fractures, urinary incontinence)
Elderly and Those with Comorbidities
- Increased risk of pneumonia
- Sleep disruption leading to exacerbation of other conditions
- Rib fractures and associated complications
- Exacerbation of underlying cardiopulmonary conditions
Mortality Rates
- Overall Case Fatality Rate: <1% in developed countries
- Infant Mortality: Substantially higher
- Up to 1% in infants <6 months in developed countries
- Up to 4% in developing countries
70% of pertussis deaths occur in infants <1 year
- Risk Factors for Fatal Outcome:
- Age <3 months
- Prematurity
- Unvaccinated or incomplete vaccination
- Delayed antibiotic treatment
- Presence of pneumonia
- Presence of seizures or encephalopathy
- Pulmonary hypertension
- Leukocytosis >100,000 cells/μL
Disability and Quality of Life Impact
- Short-term Disability: Average duration of significant illness is 6-10 weeks
- School/Work Absence: Median 5-7 days, but can extend to weeks
- Sleep Disruption: Affects both patients and family members
- Economic Impact: Substantial from healthcare costs and lost productivity
- Psychological Impact: Anxiety about coughing episodes, sleep deprivation effects
Complications of pertussis are most serious in young infants but can affect individuals of all ages. Early recognition, prompt treatment, and appropriate supportive care are essential to reduce the risk of severe complications and long-term sequelae.
7. Diagnosis & Testing
Clinical Diagnosis
Case Definitions (CDC/WHO Criteria)
Clinical Case Definition: Cough illness lasting ≥2 weeks with at least one of:
- Paroxysmal coughing
- Inspiratory “whoop”
- Post-tussive vomiting
- Apnea (in infants)
Confirmed Case:
- Positive culture for B. pertussis, OR
- Positive PCR for B. pertussis, OR
- Clinical symptoms AND epidemiologic linkage to a laboratory-confirmed case
Probable Case:
- Meets clinical case definition but without laboratory confirmation or epidemiologic linkage
Clinical Evaluation
History:
- Duration and character of cough
- Presence of paroxysms, whoop, or post-tussive vomiting
- Vaccination status
- Age-specific manifestations
- Exposure to known or suspected cases
- Seasonality and local epidemiology
Physical Examination:
- Often normal between coughing episodes
- Observation of coughing paroxysms when possible
- Assessment for complications:
- Respiratory distress
- Cyanosis
- Neurological status
- Nutritional and hydration status
- Evidence of physical complications (petechiae, conjunctival hemorrhages)
Laboratory Testing
Direct Detection Methods
Polymerase Chain Reaction (PCR)
- Sensitivity: 80-95% within first 3 weeks of illness
- Specificity: 95-99%
- Advantages:
- Results available within hours
- Remains positive longer into course than culture
- Not affected by prior antibiotic therapy as significantly as culture
- Disadvantages:
- Cannot distinguish viable from non-viable organisms
- Potential for false positives due to contamination
- Optimal Timing: Within first 3 weeks of symptom onset
- Specimen Collection: Nasopharyngeal swab or aspirate
- Current Role: Now the gold standard for pertussis diagnosis in most developed countries
Bacterial Culture
- Sensitivity: 12-60% depending on timing, prior antibiotics, technical factors
- Specificity: Nearly 100% when properly performed
- Advantages:
- Definitive diagnosis
- Allows for antibiotic susceptibility testing
- Permits molecular typing for epidemiological studies
- Disadvantages:
- Time-consuming (takes 7-10 days)
- Significantly reduced sensitivity after antibiotics or >2 weeks of symptoms
- Requires special media (Regan-Lowe or Bordet-Gengou)
- Optimal Timing: Within first 2 weeks of symptom onset
- Specimen Collection: Nasopharyngeal swab or aspirate
- Current Role: Still important for antibiotic resistance monitoring and molecular epidemiology
Serological Testing
- IgG and IgA Antibodies to Pertussis Toxin (PT):
- Sensitivity: 80-90% in appropriate timing window
- Specificity: Variable depending on cutoff values and test methodology
- Advantages:
- Useful in later stages when PCR and culture sensitivity decline
- Helpful for diagnosis in patients presenting late in illness
- Disadvantages:
- Limited utility in recently vaccinated individuals
- Requires paired sera for definitive interpretation in some cases
- Single sample interpretation can be challenging
- Optimal Timing: At least 2 weeks after symptom onset
- Current Role: Useful for late diagnosis, epidemiological studies, vaccine efficacy evaluations
Direct Fluorescent Antibody (DFA) Testing
- Sensitivity: 10-50% (highly variable)
- Specificity: Variable, concerns about false positives
- Current Role: Largely replaced by PCR and culture due to poor diagnostic performance
Specimen Collection Techniques
Nasopharyngeal Swab:
- Flexible swab inserted through nostril to posterior nasopharynx
- Dacron or rayon swabs preferred (calcium alginate may inhibit PCR)
- Must reach nasopharynx for adequate sampling
- Less invasive than aspirate but slightly lower yield
Nasopharyngeal Aspirate/Wash:
- Instillation of small amount of sterile saline followed by aspiration
- Slightly higher yield than swabs
- More uncomfortable for patient
- Preferred for infants and young children when feasible
Oropharyngeal Specimens:
- Significantly lower yield than nasopharyngeal specimens
- Not recommended as primary specimen type
Additional Diagnostic Tests
Complete Blood Count (CBC)
- Characteristic Finding: Leukocytosis with absolute lymphocytosis
- Most prominent in infants and young children
- Often shows white blood cell counts of 15,000-100,000 cells/μL
- Extreme leukocytosis (>100,000 cells/μL) associated with poor prognosis in infants
- Utility: Supportive evidence but not diagnostic
- Limitations: Not specific to pertussis; may be normal in adolescents and adults
Chest Radiography
- Common Findings:
- Often normal despite severe cough
- Perihilar infiltrates or patchy atelectasis
- Pneumonic infiltrates if bacterial superinfection present
- Indications:
- Suspected pneumonia
- Respiratory distress
- Severe disease in infants
- Limitations: Not useful for pertussis diagnosis itself but helpful for identifying complications
Pulse Oximetry and Blood Gas Analysis
- Indications:
- Monitoring oxygen saturation during paroxysms
- Evaluation of severe cases, particularly in infants
- Assessment of respiratory failure
- Typical Findings:
- Desaturation during coughing episodes
- Normal values between episodes in uncomplicated cases
- Hypoxemia and hypercarbia in severe cases with respiratory compromise
Differential Diagnosis
- Other Bordetella Species:
- B. parapertussis
- B. holmesii
- B. bronchiseptica
- Viral Respiratory Infections:
- Respiratory syncytial virus (RSV)
- Adenovirus
- Influenza
- Parainfluenza
- Mycoplasma pneumoniae
- Chlamydia pneumoniae
- Tuberculosis
- Foreign Body Aspiration
- Allergic or Chemical Irritant Cough
- Gastroesophageal Reflux Disease (GERD)
- Cystic Fibrosis
- Asthma and Reactive Airway Disease
Early Detection Methods and Effectiveness
Clinical Recognition:
- Early recognition during catarrhal stage is challenging
- Awareness of local epidemiology and seasonal patterns
- Consideration of pertussis in all prolonged cough illnesses
- Higher index of suspicion in unvaccinated or partially vaccinated individuals
Surveillance Systems:
- Active surveillance in high-risk settings (schools, healthcare facilities)
- Mandatory reporting to public health authorities
- Contact tracing for known cases
Effectiveness of Early Detection:
- PCR testing early in disease course has highest yield
- Early detection allows for:
- Prompt antibiotic therapy (most effective if started in catarrhal stage)
- Implementation of isolation precautions
- Prophylaxis of high-risk contacts
- Reduced community transmission
- Decreased complication rates in diagnosed cases
Challenges in Early Detection:
- Non-specific early symptoms resembling common colds
- Variable clinical presentation across age groups
- Atypical presentation in previously vaccinated individuals
- Limited awareness among healthcare providers
- Logistical challenges in specimen collection and testing
Accurate and timely diagnosis of pertussis remains challenging due to its variable presentation and the limitations of available diagnostic tests. A combination of clinical assessment, laboratory testing, and epidemiological considerations provides the most reliable approach to diagnosis.
8. Treatment Options
Antimicrobial Therapy
Primary Antibiotics
Macrolides (First-line therapy):
- Azithromycin:
- Preferred agent due to shorter course and better compliance
- Infants <6 months: 10 mg/kg/day for 5 days
- Everyone else: 500 mg on day 1, then 250 mg daily for days 2-5
- Clarithromycin:
- 15 mg/kg/day in two divided doses for 7 days (children)
- 500 mg twice daily for 7 days (adults)
- Erythromycin:
- 40-50 mg/kg/day in four divided doses for 14 days (children)
- 500 mg four times daily for 14 days (adults)
- Less preferred due to side effects and compliance issues
- Azithromycin:
Alternative Agents (for macrolide allergy or resistance):
- Trimethoprim-Sulfamethoxazole (TMP-SMX):
- Not for infants <2 months
- Children: 8 mg/kg/day (TMP component) in two divided doses for 14 days
- Adults: 160 mg TMP/800 mg SMX twice daily for 14 days
- Trimethoprim-Sulfamethoxazole (TMP-SMX):
Goals of Antibiotic Therapy
- Eradicate the organism and reduce infectiousness
- Shorten duration of communicability (from 21+ days to approximately 5 days)
- Reduce severity and duration of symptoms if given early
- Note: Antibiotics have minimal effect on the clinical course if started after 3 weeks of illness or during paroxysmal stage
Timing of Antibiotic Therapy
- Most effective when initiated during catarrhal stage
- Still recommended during paroxysmal stage to reduce transmission
- Not recommended after 3 weeks of illness unless needed to prevent transmission to high-risk contacts
Supportive Care
Respiratory Support
- Oxygen Therapy:
- For hypoxemia during paroxysms or with complications
- Continuous monitoring in severe cases
- Suction:
- Gentle nasopharyngeal suctioning to remove secretions
- Particularly important in infants
- Mechanical Ventilation:
- For respiratory failure or severe apnea
- Required in 10-20% of hospitalized infants
Nutritional and Fluid Support
- Hydration Maintenance:
- Oral fluids in mild cases
- Intravenous fluids if oral intake compromised
- Small, frequent feedings to minimize vomiting
- Nutritional Support:
- Nasogastric or nasojejunal feeding in severe cases
- Monitoring of weight and nutritional status
- Caloric supplementation as needed
Cough Management
- General Measures:
- Quiet environment
- Humidified air
- Avoidance of irritants (smoke, strong odors)
- Cough Suppressants:
- Generally not recommended
- Limited evidence for effectiveness
- May impair airway clearance
- Specific Therapies:
- Limited evidence supporting:
- Beta-2 agonists (only if bronchospasm present)
- Leukotriene modifiers
- Ipratropium bromide
- Limited evidence supporting:
Hospital-Based Treatment
Indications for Hospitalization
- Age-Based:
- Most infants <3 months
- Consideration for infants 3-6 months
- Clinical Severity:
- Severe paroxysms
- Cyanosis or apnea
- Respiratory distress or failure
- Difficulty feeding or severe vomiting
- Signs of neurological complications
- Laboratory Findings:
- Extreme leukocytosis (>30,000-50,000 cells/μL)
- Hypoxemia
- Radiographic evidence of pneumonia
- Social Factors:
- Inability to ensure adequate outpatient monitoring
- High-risk home situation
Intensive Care Considerations
- Indications for ICU Admission:
- Recurrent or prolonged apnea
- Respiratory failure requiring ventilation
- Pulmonary hypertension
- Seizures or encephalopathy
- Severe pneumonia
- Extreme leukocytosis (>100,000 cells/μL)
- Specialized Therapies in ICU:
- Mechanical ventilation strategies
- High-frequency oscillatory ventilation
- Extracorporeal membrane oxygenation (ECMO) in severe cases
- Nitric oxide for pulmonary hypertension
Adjunctive Therapies
Exchange Transfusion or Leukapheresis
- Indications:
- Extreme leukocytosis (>100,000 cells/μL)
- Particularly in young infants with respiratory distress
- Mechanism:
- Reduces leukocyte mass and pulmonary leukostasis
- May improve pulmonary hypertension
- Evidence:
- Case series and reports suggest benefit
- No randomized controlled trials
Corticosteroids
- Limited Evidence:
- Some small studies suggest potential benefit
- No definitive randomized controlled trials
- Possible Indications:
- Severe cases with respiratory distress
- Patients with bronchospasm
- Cautions:
- Risk of immunosuppression
- Limited evidence of benefit
Intravenous Immunoglobulin (IVIG)
- Theoretical Benefit:
- Neutralization of pertussis toxin
- Immunomodulatory effects
- Evidence:
- Limited to case reports and small series
- No conclusive evidence of efficacy
- Current Role:
- Considered experimental
- May be considered in critically ill infants
Special Populations
Neonates and Young Infants
- Antibiotic Considerations:
- Azithromycin preferred in infants <1 month
- Erythromycin associated with infantile hypertrophic pyloric stenosis risk
- Monitoring:
- Continuous cardiorespiratory monitoring
- Apnea monitoring for at least 24-48 hours after admission
- Frequent small feedings or alternative feeding methods
Pregnant Women
- Antibiotic Safety:
- Macrolides (preferably azithromycin) considered safe
- Avoid trimethoprim-sulfamethoxazole near term (risk of kernicterus)
- Supportive Care:
- Fetal monitoring in severe cases
- Oxygen therapy as needed
- Adequate hydration
- Prevention of vomiting to avoid preterm labor
Immunocompromised Patients
- Extended Antibiotic Courses:
- Longer duration may be considered
- Higher doses sometimes used
- Specialized Monitoring:
- More aggressive approach to complications
- Lower threshold for hospitalization
- Consideration of prophylactic antibiotics for high-risk exposures
Post-Exposure Prophylaxis
- Indications:
- Household contacts of pertussis cases
- High-risk contacts (infants, pregnant women, healthcare workers)
- Outbreak control in closed settings
- Recommended Agents:
- Same antibiotics and dosing as for treatment
- Typically 5-day course of azithromycin preferred
- Timing:
- Most effective if initiated within 21 days of exposure
- Limited benefit after 21 days except to protect high-risk contacts
Emerging Treatments and Clinical Trials
- Anti-Inflammatory Approaches:
- IL-1 receptor antagonists (anakinra) under investigation
- TNF-α inhibitors being studied
- Various cytokine modulators in preclinical research
- Monoclonal Antibodies:
- Humanized antibodies against pertussis toxin
- Animal studies show promising results
- Phase 1/2 clinical trials in process
- Novel Antibiotics:
- New macrolide derivatives with improved pharmacokinetics
- Targeted delivery systems for respiratory infections
- Alternative Adjunctive Therapies:
- Statins (for anti-inflammatory properties)
- Pulmonary surfactant administration
- Enhanced mucociliary clearance techniques
The treatment of pertussis remains primarily supportive, with antibiotics mainly effective for reducing transmission and potentially modifying disease course if given very early. Ongoing research focuses on better understanding the pathophysiology of severe disease and developing targeted interventions for the most vulnerable populations.
9. Prevention & Precautionary Measures
Vaccination
Current Vaccine Types
- Whole-Cell Pertussis Vaccines (wP):
- Contain killed whole B. pertussis bacteria
- Higher rates of adverse reactions
- May provide longer-lasting immunity
- Still used in many developing countries
- Combined as DTwP (with diphtheria and tetanus toxoids)
- Acellular Pertussis Vaccines (aP):
- Contain purified B. pertussis antigens
- Fewer adverse reactions
- Components may include:
- Pertussis toxoid (inactivated PT)
- Filamentous hemagglutinin (FHA)
- Pertactin (PRN)
- Fimbriae types 2 and 3 (FIM)
- Combined as DTaP or Tdap (with diphtheria and tetanus)
Recommended Vaccination Schedules
- Infants and Children (CDC/WHO):
- Primary series: DTaP at 2, 4, and 6 months
- First booster: DTaP at 15-18 months
- Second booster: DTaP at 4-6 years
- Adolescents:
- Tdap booster at 11-12 years
- Single dose regardless of previous vaccination history
- Adults:
- One Tdap dose if not previously received
- During each pregnancy: Tdap between 27-36 weeks (preferably earlier in that window)
- Consider Tdap instead of Td for wound management if not previously received
- Special Populations:
- Healthcare workers: Tdap regardless of age
- Childcare providers: Tdap recommended
- Close contacts of infants: Tdap recommended (“cocooning strategy”)
Vaccine Effectiveness
- DTaP (Childhood Vaccine):
- 80-90% effective after 3-dose primary series
- Effectiveness wanes to approximately 70% by 5 years after last dose
- Protection against severe disease better than against mild disease
- Tdap (Adolescent/Adult Vaccine):
- Initially 70% effective
- Declines to about 30-40% effectiveness after 4 years
- Better at preventing severe disease than mild disease
- Maternal Vaccination:
- 91% effective at preventing pertussis in infants <2 months
- Transfer of maternal antibodies provides protection until infant vaccination begins
Infection Control Measures
Healthcare Settings
- Isolation Precautions:
- Droplet precautions for hospitalized patients
- Single room preferred
- Surgical mask for healthcare workers and visitors within 3 feet
- Continue until 5 days of appropriate antibiotic therapy completed
- Healthcare Worker Protection:
- Tdap vaccination for all healthcare workers
- Prompt identification and exclusion of symptomatic staff
- Post-exposure prophylaxis for exposed unvaccinated staff
- Environmental Controls:
- Standard disinfection procedures adequate
- B. pertussis does not survive long in environment
Community Settings
- School and Childcare:
- Exclusion of cases until 5 days of appropriate antibiotics completed
- Consideration of prophylaxis for high-risk contacts
- Verification of vaccination status during outbreaks
- Household Management:
- Treatment of all household members regardless of symptoms
- Particular attention to protecting vulnerable members (infants, pregnant women)
- Air Travel and Public Transportation:
- Cases should avoid travel while infectious
- Contact tracing may be considered for prolonged exposures
Public Health Strategies
Surveillance Systems
- Case Reporting:
- Mandatory reporting to public health authorities in most countries
- Active surveillance in high-risk settings
- Outbreak Detection:
- Recognition of increased case clusters
- Molecular typing to identify strain relationships
- Data Collection:
- Age distribution of cases
- Vaccination status
- Severity indicators
- Geographic clustering
Outbreak Control Measures
- Case Definition and Identification:
- Enhanced testing in outbreak settings
- Lower threshold for diagnosis
- Contact Tracing:
- Identification of close contacts
- Evaluation of high-risk contacts
- Consideration of prophylaxis
- Mass Prophylaxis:
- In specific settings (schools, healthcare facilities)
- Prioritization based on risk assessment
- Vaccination Campaigns:
- Catch-up vaccination for under-vaccinated populations
- Consideration of additional doses in certain situations
- Public Communications:
- Clear messaging about symptoms and when to seek care
- Vaccination reminders
- Prevention strategies
Preventive Antibiotics (Chemoprophylaxis)
- Indications:
- Household contacts of pertussis cases
- High-risk close contacts (infants, pregnant women in third trimester)
- In outbreak settings for defined groups
- Recommended Agents:
- Same antibiotics as for treatment (macrolides preferred)
- Azithromycin typically recommended for simplicity and compliance
- Timing:
- Most effective when administered within 21 days of exposure
- Limited benefit after 21 days except for high-risk contacts
- Effectiveness:
- Reduces secondary transmission by 80-90% when given promptly
- Less effective as time from exposure increases
Emerging Prevention Strategies
Novel Vaccine Approaches
- Live Attenuated Pertussis Vaccines:
- Intranasal delivery to stimulate mucosal immunity
- Potential for single-dose protection
- Currently in preclinical and early clinical trials
- Outer Membrane Vesicle Vaccines:
- Derived from B. pertussis membrane components
- May induce broader immune response
- Under investigation in animal models
- Recombinant Attenuated Vaccine Strains:
- Genetically modified for safety and immunogenicity
- Allow for intranasal administration
- Early stage development
- DNA Vaccines:
- Encoding key pertussis antigens
- Potential for cellular and humoral immunity
- Preclinical stage research
Maternal Immunization Optimization
- Timing Studies:
- Optimal gestational age for maximum antibody transfer
- Potential for repeat dosing in prolonged pregnancies
- Combined Strategies:
- Integration with other maternal vaccines
- Simplified administration platforms
Adjuvant Development
- Novel Adjuvants:
- To enhance and prolong immune response
- Targeting specific immune pathways
- Mucosal adjuvants for potential intranasal vaccines
- Controlled Release Systems:
- Prolonged antigen presentation
- Potential for single-dose regimens
Effectiveness of Prevention Strategies
- Vaccination Impact:
80% reduction in pertussis incidence in countries with sustained high coverage
95% reduction in pertussis mortality globally since widespread vaccination
- Greatest impact on infant mortality
- Maternal Immunization:
- 90% effective in preventing pertussis in infants too young for vaccination
- Most cost-effective strategy for preventing infant pertussis
- Cocooning Strategy:
- Vaccination of all household contacts and caregivers
- Moderate effectiveness (30-50% reduction in infant cases)
- Implementation challenges limit real-world effectiveness
- Antibiotic Prophylaxis:
- 80-90% effective in preventing secondary cases when given promptly
- Cost-effective when targeted to high-risk contacts
- Combined Approaches:
- Multilayered strategies most effective
- Integration of vaccination, prophylaxis, and isolation measures
Prevention of pertussis requires a multifaceted approach combining vaccination, prompt diagnosis and treatment of cases, appropriate antibiotic prophylaxis, and public health surveillance. Continued research into improved vaccines and prevention strategies is essential to address the resurgence of pertussis in many developed countries.
10. Global & Regional Statistics
Global Burden of Disease
- Estimated Global Cases (WHO): 24.1 million cases annually
- Annual Deaths: Approximately 160,700 deaths globally, primarily in children under 5 years
- Disease Burden: 13.8 million disability-adjusted life years (DALYs) lost
- Underreporting: Believed to be substantial, with actual burden likely 5-10 times higher than reported cases
- Vaccination Coverage: 86% global coverage for 3 doses of pertussis-containing vaccine (DTP3)
- Cyclical Pattern: 3-5 year epidemic cycles persist even in vaccinated populations
Regional Variations
North America
- United States:
- Reported cases: 15,000-50,000 annually with cyclical patterns
- Resurgence since the 1980s despite high vaccination coverage
- Peak in 2012: 48,277 cases (highest since 1955)
- Incidence: 4-15 cases per 100,000 population
- Mortality: <20 deaths annually, primarily in infants <3 months
- Changing epidemiology with increased adolescent and adult cases
- Canada:
- Similar patterns to the US
- Incidence: 2-10 cases per 100,000 population
- Regional outbreaks, particularly in areas with lower vaccination rates
Europe
- Western Europe:
- Incidence: 1-20 cases per 100,000 population
- Variations between countries related to vaccination policies
- Notable resurgence in countries that switched to acellular vaccines
- UK: Maternal vaccination program has reduced infant pertussis by >90%
- Eastern Europe:
- More variable reporting and surveillance
- Generally higher incidence than Western Europe
- Vaccination coverage more variable
Asia
- High-Income Countries (Japan, South Korea):
- Well-controlled with periodic outbreaks
- Japan: Early adopter of acellular pertussis vaccines
- South Korea: Low incidence with high vaccination coverage
- Southeast Asia:
- Estimated incidence: 10-40 per 100,000 population
- Significant underreporting
- Variable vaccination coverage
- South Asia:
- High burden, particularly in infants
- India: Estimated 200,000 cases and 60,000 deaths annually
- Limited surveillance systems
- Increasing but still suboptimal vaccination coverage
Africa
- Highest estimated burden: 7.8 million cases and 80,000 deaths annually
- Vaccination coverage: Range from 30-90% depending on country
- Surveillance: Limited in many countries
- Mortality rates: 3-5 times higher than global average
- Urban vs. rural: Higher reported incidence in urban areas, likely due to better detection
Latin America and Caribbean
- Improved control: Significant reductions since expanded vaccination programs
- Brazil: Largest burden in region, with periodic outbreaks
- Vaccination coverage: Generally high (>85% in most countries)
- Incidence: 1-5 cases per 100,000 in most countries
- Regional initiative: Focus on maternal vaccination improving infant protection
Oceania
- Australia: Experienced significant resurgence, peak in 2011
- Implemented maternal vaccination with good results
- Incidence: 50-170 cases per 100,000 during outbreak years
- New Zealand: Similar patterns to Australia
- Pacific Islands: Limited data, variable vaccination coverage
Mortality and Case-Fatality Rates
- Global Case-Fatality Rate: 0.1-4% depending on age and region
- Age Distribution of Deaths:
- Infants <1 year: 90% of all pertussis deaths
- Infants <3 months: Highest case-fatality rate (1-3% in developed countries, 4-8% in developing countries)
- Regional Variations in Mortality:
- High-income countries: <0.5% case-fatality rate
- Low-income countries: 1-4% case-fatality rate
- Sub-Saharan Africa: Highest mortality burden
- Trends in Mortality:
- Global pertussis deaths declined 95% since 1980
- Stalled progress in some regions since 2010
- Maternal vaccination significantly reducing infant deaths where implemented
Epidemiological Trends
Temporal Patterns
- Natural Cyclic Pattern: 3-5 year epidemic cycles
- Seasonal Variation:
- Peak incidence in summer and fall in temperate regions
- Less pronounced seasonality in tropical regions
- Long-term Trends:
- Overall global decline since widespread vaccination
- Resurgence in many developed countries since 1980s
- Shifting age distribution toward adolescents and adults
Demographic Patterns
- Age Distribution Shift:
- Traditional pattern: Highest in children <5 years
- Current pattern in countries with established vaccination programs:
- Bimodal distribution with peaks in infants and adolescents/adults
- Increasing proportion of cases in 10-19 year age group
- Gender Distribution:
- Generally equal in children
- Slight female predominance in adolescents and adults
- Possibly related to childcare responsibilities and healthcare-seeking behavior
- Socioeconomic Factors:
- Higher reported incidence in higher socioeconomic groups in developed countries (likely due to better access to diagnosis)
- Higher true incidence and mortality in lower socioeconomic groups globally
Vaccination Impact
- Pre-Vaccine Era (1940s):
- United States: >200,000 cases and 9,000 deaths annually
- Global: Estimated 1.5 million deaths annually
- Post-Vaccine Introduction:
- 95% reduction in global incidence
- 99% reduction in mortality in developed countries
- Impact of Acellular Vaccine Transition:
- Initial maintenance of disease control
- Subsequent resurgence in many countries
- Attributed to shorter duration of protection
- Recent Maternal Vaccination Programs:
- UK: 91% reduction in infant pertussis cases
- USA: 78% reduction in pertussis among infants <2 months
- Australia: 85% reduction in infant hospitalizations
Outbreak Patterns
- School-Based Outbreaks:
- Common in middle and high schools
- Reflect waning immunity in adolescents
- Often first indicator of community-wide outbreaks
- Geographic Clustering:
- Often associated with vaccine refusal clusters
- Higher incidence in areas with philosophical exemptions to vaccination
- Notable Recent Outbreaks:
- California (2010, 2014): >9,000 and >11,000 cases respectively
- Washington State (2012): 5,000 cases
- United Kingdom (2012): 9,300 cases, 14 infant deaths
- Australia (2008-2011): 38,000 cases
The global burden of pertussis remains substantial despite decades of vaccination efforts, with significant regional variations in disease incidence, mortality, and control strategies. The changing epidemiology of pertussis, particularly in countries using acellular vaccines, presents ongoing challenges for disease control and prevention.
11. Recent Research & Future Prospects
Recent Research Advancements
Vaccine Effectiveness and Waning Immunity
- Duration of Protection Studies:
- Multiple large-scale epidemiological studies confirm waning protection from acellular pertussis vaccines
- Protection decreases to approximately 30-40% within 4 years after the final childhood dose
- Similar waning observed after adolescent and adult boosters
- Whole-cell vaccines may provide longer-lasting protection (7-10 years)
- Immune Response Characterization:
- Acellular vaccines primarily induce humoral (antibody) immunity
- Whole-cell vaccines stimulate both humoral and cell-mediated immunity
- Cell-mediated immunity appears important for long-term protection
- T-helper 17 (Th17) cell responses particularly relevant
- Transmission Studies:
- Baboon model demonstrates that acellular-vaccinated individuals can harbor and transmit bacteria despite being protected from disease
- Explains continued circulation in highly vaccinated populations
Molecular Epidemiology
- Genomic Evolution of B. pertussis:
- Whole genome sequencing reveals adaptation of circulating strains
- Antigenic drift away from vaccine strains
- Emergence of pertactin-deficient strains (PRN-negative)
- Potential vaccine-driven evolution
- Pertactin-Deficient Strains:
- Now predominant in many countries (60-90% of isolates)
- Appears to confer advantage in vaccinated populations
- No evidence of reduced virulence
- Modest impact on vaccine effectiveness
- Transmission Dynamics:
- Enhanced understanding of asymptomatic carriage
- Mathematical modeling of transmission in vaccinated populations
- Identification of key transmission settings and groups
Maternal Vaccination
- Optimization Research:
- Antibody kinetics during pregnancy
- Optimal timing studies (early third trimester appears best)
- Duration of infant protection (approximately 2-3 months)
- No evidence of blunting of infant immune responses to primary vaccination
- Implementation Studies:
- Barriers to uptake identified
- Healthcare provider recommendation most important factor
- Integration with prenatal care improves coverage
- Cost-effectiveness demonstrated across various healthcare systems
Diagnostic Advances
- Advanced Molecular Techniques:
- Multiplex PCR platforms for simultaneous detection of multiple respiratory pathogens
- Loop-mediated isothermal amplification (LAMP) for rapid, field-based testing
- Next-generation sequencing for outbreak investigation
- Point-of-Care Diagnostics:
- Rapid PCR systems with results in 30-60 minutes
- Developments in isothermal amplification techniques
- Microfluidic platforms for resource-limited settings
- Biomarker Research:
- Identification of host response markers that distinguish pertussis from other respiratory infections
- Potential for improved clinical algorithms
Ongoing Studies and Clinical Trials
Novel Vaccine Development
- Live Attenuated Nasal Vaccines:
- BPZE1: Genetically attenuated B. pertussis strain
- Phase 2 clinical trials showing promising immunogenicity
- Potential for single-dose, needle-free administration
- Aims to induce mucosal immunity and mimic natural infection
- Outer Membrane Vesicle Vaccines:
- Derived from B. pertussis membrane components
- Broader antigen presentation than current acellular vaccines
- Phase 1 trials underway
- Potential for improved duration of protection
- Adjuvanted Acellular Vaccines:
- Novel adjuvants to enhance Th1/Th17 responses
- TLR agonists to direct immune response
- Preclinical and early clinical studies
- Aim to combine safety of acellular vaccines with effectiveness of whole-cell vaccines
Treatment Innovations
- Monoclonal Antibody Therapy:
- Humanized antibodies targeting pertussis toxin
- Animal studies show protection when given post-exposure
- Potential for passive immunization of newborns
- Phase 1 safety trials in progress
- Anti-inflammatory Approaches:
- IL-1 receptor antagonists for severe infant cases
- TNF-α inhibitors under investigation
- Small clinical trials in severe infant pertussis
- Aim to reduce morbidity and mortality in critical cases
Epidemiological and Implementation Research
- Mixed Vaccine Schedules:
- Combining whole-cell and acellular vaccines
- Initial whole-cell doses followed by acellular boosters
- Studies in several countries evaluating immunogenicity and reactogenicity
- Potential for improved long-term protection
- Adult Vaccination Strategies:
- Periodic boosting studies (optimal intervals)
- Target group identification for cost-effective boosting
- Impact on transmission to vulnerable populations
- Implementation research in various healthcare systems
- Digital Health Applications:
- Smartphone-based cough analysis for screening
- Electronic immunization registries to improve coverage
- Outbreak prediction using artificial intelligence
- Surveillance system enhancements
Future Medical Possibilities
Next-Generation Vaccines
- Universal Pertussis Vaccines:
- Broader protection against multiple Bordetella species
- Coverage of antigenically divergent strains
- Potentially life-long protection
- 5-10 years from potential availability
- Novel Delivery Platforms:
- Microneedle patch delivery systems
- Thermostable formulations for resource-limited settings
- Extended-release depot formulations
- Single-dose regimens
- Combined Maternal-Infant Approaches:
- Optimized maternal vaccination plus enhanced infant schedules
- Potential for closing the immunity gap in early infancy
- Tailored to regional epidemiology
- Implementation research ongoing
Advanced Therapeutics
- Pathogen-Directed Therapies:
- Novel antibiotics specifically targeting B. pertussis
- Bacteriophage therapy
- Anti-virulence approaches targeting toxin production
- 5-15 years from potential clinical use
- Host-Directed Therapies:
- Modulation of excessive inflammatory responses
- Targeted immunotherapy for severe cases
- Biomarker-guided treatment protocols
- Potential for improving outcomes in infant cases
Prevention Systems
- Predictive Outbreak Models:
- Real-time surveillance with predictive analytics
- Integration of genomic, clinical, and epidemiological data
- Early warning systems for emerging strains
- Enhanced targeted response capabilities
- Precision Vaccination:
- Personalized vaccination schedules based on immune responses
- Genetic markers for vaccine response
- Tailored approaches for special populations
- Optimized community protection strategies
Barriers and Challenges
- Scientific Challenges:
- Incomplete understanding of correlates of protection
- Challenges in pertussis animal models
- Difficulty in studying transmission dynamics
- Limited knowledge of mucosal immunity
- Implementation Barriers:
- Vaccine hesitancy in some populations
- Resource limitations in low-income countries
- Healthcare provider education gaps
- Competing health priorities
- Economic Considerations:
- Cost constraints for novel vaccines
- Sustainability of vaccination programs
- Limited market incentives for new therapeutic development
- Resource allocation between prevention and treatment
The field of pertussis research continues to evolve, with significant advances in understanding the pathogen, host responses, and prevention strategies. Future prospects include improved vaccines with longer duration of protection, novel therapeutics for severe cases, and enhanced surveillance systems. However, substantial challenges remain in translating research advances into effective public health interventions globally.
12. Interesting Facts & Lesser-Known Insights
Historical Curiosities
- Ancient Names: Pertussis has been known by many colorful names throughout history:
- “Kink-cough” or “Kinkhoest” in Northern Europe
- “The 100-day cough” in China and Japan
- “Tussis Quintina” (fifth-day cough) in medieval texts
- “Hooping cough” in older English literature (referring to the whooping sound)
- “Chin cough” in some English regions
- Royal Victims: Several historical figures were affected by pertussis:
- Queen Anne’s son, William, Duke of Gloucester, died from complications of pertussis in 1700
- King Edward VII of England suffered from pertussis as a child
- The “Pertussis Waltz” was composed by Johann Strauss I during an epidemic that affected his family
- Historical Treatments: Before modern medicine, pertussis remedies included:
- Inhaling vapors from horse stables (the ammonia was thought to be therapeutic)
- Drinking donkey milk
- Wearing necklaces of peony root
- Spider webs mixed with honey
- Holding children near gas works for the sulfurous fumes
- Vaccine Development Drama: The whole-cell pertussis vaccine was developed during World War II by Pearl Kendrick and Grace Eldering, two female scientists who tested it on themselves before conducting the first controlled vaccine trial in the United States.
Biological Peculiarities
Host Specificity: B. pertussis is strictly a human pathogen with no animal reservoir or environmental persistence, unlike many other infectious diseases.
Bacterial Stealth Mechanisms: The bacteria have evolved remarkable mechanisms to evade immune detection:
- Adenylate cyclase toxin paralyzes immune cells upon contact
- Tracheal cytotoxin is actually fragments of the bacteria’s own cell wall that damage airway cells
- Pertussis toxin disables multiple immune signaling pathways simultaneously
Leucocytosis Extremes: Pertussis can cause white blood cell counts higher than almost any other condition, sometimes exceeding 100,000 cells/μL (normal range: 5,000-10,000 cells/μL).
Transmission Efficiency: A single person with pertussis can infect 12-17 susceptible individuals on average (R₀ of 12-17), making it more contagious than influenza, COVID-19, or polio.
Paradoxical Lung Findings: Despite severe coughing, physical examination of the lungs often reveals minimal abnormalities between coughing episodes.
Unusual Immunity Pattern: Unlike many infections, natural pertussis infection does not confer lifelong immunity; protection typically wanes after 7-20 years.
Unexpected Risk Factors
Birth Month Association: Some studies suggest that children born in autumn and winter months have slightly higher pertussis risk, possibly related to seasonal pathogen circulation at vulnerable ages.
Pet Ownership: Households with dogs may have slightly reduced pertussis risk, possibly due to exposure to cross-reactive Bordetella bronchiseptica (which causes kennel cough in dogs).
Vitamin D Status: Emerging research suggests vitamin D deficiency may be associated with increased pertussis severity and susceptibility.
Climate Change Impact: Altered seasonal patterns and population migrations due to climate change may influence pertussis transmission dynamics.
Microbiome Interactions: Preliminary research suggests that the composition of the nasopharyngeal microbiome may influence susceptibility to pertussis colonization.
Genetic Variations: Certain polymorphisms in toll-like receptor genes may increase susceptibility or severity of pertussis infection.
Occupational Patterns
Healthcare Worker Risk: Pertussis is an occupational hazard for healthcare workers, with attack rates 1.7-3.3 times higher than the general population during outbreaks.
Childcare Providers: Studies show childcare workers have 2-4 times higher pertussis risk than age-matched adults in other occupations.
Teachers: Elementary school teachers experience higher rates of pertussis, particularly during community outbreaks.
Wind Instrument Musicians: Professional wind instrument players have reported occupational difficulties following pertussis due to altered breathing control and lingering cough.
Public Speakers and Singers: These professionals often experience prolonged vocational impact from post-pertussis cough syndrome.
Emergency Service Workers: First responders may have increased exposure risk due to close contact with the public during respiratory emergencies.
Common Misconceptions
“Pertussis is a Mild Childhood Disease”: While often mild in adolescents and adults, pertussis remains life-threatening for infants, with case-fatality rates up to 1-3% in infants under 3 months.
“The ‘Whoop’ Is Always Present”: The characteristic whoop is absent in 30-50% of cases, particularly in adults, adolescents, partially immunized children, and young infants.
“Antibiotics Cure the Cough Quickly”: Once the paroxysmal stage begins, antibiotics have minimal effect on symptom duration, though they reduce infectiousness.
“One Vaccine Provides Lifelong Protection”: Unlike many vaccines, pertussis protection wanes relatively quickly, requiring boosters throughout life.
“Pertussis Is Rare in Vaccinated Communities”: Even highly vaccinated communities experience pertussis circulation, particularly with acellular vaccines which may prevent disease but not colonization.
“Adults Don’t Get Pertussis”: Adults account for a substantial proportion of cases, though often with atypical presentation and underdiagnosis.
“Pertussis Is Only Contagious During Coughing Episodes”: Infectiousness is actually highest during the early catarrhal stage before the characteristic cough develops.
Diet and Lifestyle Influences
Breastfeeding Protection: Exclusively breastfed infants have approximately 60% lower pertussis risk in the first 6 months of life.
Cough Triggers: Certain dietary elements can trigger coughing paroxysms during pertussis recovery:
- Cold beverages
- Citrus and acidic foods
- Spicy foods
- Carbonated drinks
Recovery Acceleration: Some nutritional factors may support faster recovery:
- Adequate hydration
- Small, frequent meals to prevent vomiting
- Honey (in children >1 year) for cough symptomatic relief
- Foods rich in vitamin A and C for respiratory epithelial health
Sleep Positioning: During recovery, slightly elevated head positioning may reduce nocturnal coughing episodes.
Air Quality: Indoor air pollution significantly worsens pertussis symptoms and may increase complication rates.
Demographic Nuances
Gender Differences in Adulthood: Adult women appear to have both higher incidence and longer duration of cough than men, possibly due to differences in healthcare-seeking behavior, exposure patterns, and possibly hormonal influences.
“Grandmother Effect”: Some researchers have proposed that post-reproductive women historically played a crucial role in pertussis immunity by acting as boosters for young mothers, providing indirect protection to infants.
Global Naming Patterns: The disease name in many languages references the number of coughs in typical paroxysms or the duration:
- “Cent jours toux” (hundred-day cough) in French
- “Keuchhusten” (barking cough) in German
- “Tos ferina” (wild/savage cough) in Spanish
- “Koklyush” (rooster-like cough) in Russian
Cyclical Immunity: Population-level immunity follows a cyclical pattern, with increased adult susceptibility approximately 30-40 years after large childhood epidemics.
Urban-Rural Differences: Urban areas typically experience earlier outbreak onset but rural areas often have higher per capita rates due to lower vaccination coverage in many regions.
Pandemic and Emerging Infection Insights
- COVID-19 Impact: The COVID-19 pandemic caused unprecedented decreases in pertussis cases worldwide due to:
- Social distancing and school closures
- Mask wearing
- Enhanced respiratory hygiene
- Reduced international travel
- These interventions demonstrated the feasibility of pertussis control through non-pharmaceutical interventions
- Post-Pandemic Concerns: Health authorities anticipate potentially larger pertussis outbreaks as COVID-19 restrictions lift due to:
- Missed vaccination appointments during the pandemic
- Reduced natural boosting from decreased circulation
- Waning immunity without exposure
- One Health Considerations: While B. pertussis is human-specific, related Bordetella species affect animals, creating a complex ecological and evolutionary network relevant to understanding pathogen adaptation.
These lesser-known facts and insights about pertussis highlight the complex and fascinating nature of this ancient disease, which continues to adapt and challenge medical science despite centuries of study and decades of vaccination efforts.
This comprehensive report provides a detailed overview of whooping cough (pertussis), from its basic definition to the latest research developments. The information presented aims to be accessible to both general readers and healthcare professionals while maintaining scientific accuracy.
Note: Medical information changes rapidly. Consult healthcare providers for personalized advice on pertussis prevention and management.