
⚠️ Disclaimer: The information provided in this article is for educational purposes only and does not constitute medical advice. RevisionTown does not provide diagnosis, treatment, or medical recommendations. Always consult a qualified healthcare professional regarding any medical condition, symptoms, or concerns.
Read More – 🏥 Medical Disclaimer
Comprehensive Report on Mesothelioma
1. Overview
What is Mesothelioma?
Mesothelioma is a rare, aggressive form of cancer that develops in the mesothelium, a thin layer of tissue that covers most internal organs. It is primarily caused by exposure to asbestos, with a long latency period typically ranging from 20 to 50 years between exposure and disease manifestation.
Affected Body Parts/Organs
Mesothelioma can affect several areas of the body:
- Pleural mesothelioma (75-80% of cases): Affects the pleura, the lining of the lungs
- Peritoneal mesothelioma (10-20% of cases): Affects the peritoneum, the lining of the abdominal cavity
- Pericardial mesothelioma (1-2% of cases): Affects the pericardium, the lining around the heart
- Testicular mesothelioma (<1% of cases): Affects the tunica vaginalis, the lining of the testicles
Prevalence and Significance
Mesothelioma is relatively rare, with approximately 2,500-3,000 new cases diagnosed annually in the United States and about 43,000 deaths worldwide each year. Despite its rarity, mesothelioma has significant social, medical, and legal implications due to its strong association with industrial asbestos exposure and its poor prognosis. The disease has become emblematic of occupational hazards and has prompted substantial regulatory changes across industries globally.
2. History & Discoveries
First Identification
Mesothelioma was first described in medical literature in 1767 by Joseph Lieutaud, the personal physician to King Louis XVI of France. However, it wasn’t recognized as a distinct clinical entity until the early 20th century.
Key Discoverers and Breakthroughs
- 1940s: First scientific papers suggesting a connection between asbestos exposure and cancer
- 1960: Dr. J. Christopher Wagner published a groundbreaking paper in the British Journal of Industrial Medicine establishing a clear link between asbestos exposure and mesothelioma in South African asbestos miners
- 1964: Dr. Irving J. Selikoff presented findings at the New York Academy of Sciences confirming high rates of asbestos-related diseases in insulation workers, bringing widespread attention to the health hazards of asbestos
- 1970s: Regulatory actions began in many countries to limit asbestos use
- 1982: First immunohistochemical markers for diagnosing mesothelioma were developed
Evolution of Medical Understanding
The understanding of mesothelioma has evolved significantly over time:
- Initially considered a variant of other cancers
- Recognized as a distinct cancer type by the mid-20th century
- Molecular and genetic understanding advanced dramatically in the 1990s and 2000s
- Recent advances in genomics have further characterized the molecular signatures of mesothelioma, revealing complex genetic alterations including mutations in BAP1, NF2, and CDKN2A genes
3. Symptoms
Early Symptoms
Early symptoms are often vague and may be mistaken for less serious conditions:
- Pleural mesothelioma:
- Persistent dry cough
- Shortness of breath (dyspnea)
- Chest pain or tightness
- Fatigue
- Peritoneal mesothelioma:
- Abdominal pain or swelling
- Feeling of fullness
- Changes in bowel habits
- Unexplained weight loss
- Pericardial mesothelioma:
- Chest pain
- Irregular heartbeat (arrhythmia)
- Heart murmur
- Shortness of breath when lying flat
Advanced-Stage Symptoms
As the disease progresses, symptoms become more severe:
- Severe pain in the affected area
- Significant weight loss
- Anemia
- Difficulty swallowing
- Respiratory complications including pleural effusion
- Bowel obstruction (in peritoneal cases)
- Cardiac tamponade (in pericardial cases)
- Night sweats and fever
- Hemoptysis (coughing up blood)
Symptom Progression
Symptoms typically follow this pattern:
- Initial vague, mild symptoms often attributed to other conditions
- Gradual worsening over months
- Rapid intensification once the disease reaches advanced stages
- Development of systemic symptoms reflecting general decline
- Terminal phase characterized by significant pain, cachexia, and organ dysfunction
The insidious onset and non-specific nature of early symptoms contribute to delayed diagnosis, with many patients diagnosed only after the disease has progressed to stages where treatment options are limited.
4. Causes
Biological and Environmental Causes
The primary cause of mesothelioma is exposure to asbestos, accounting for approximately 80-90% of all cases. Asbestos refers to a group of naturally occurring silicate minerals with thin fibrous crystals. When these fibers are inhaled or ingested, they can become lodged in the mesothelium and cause inflammation, scarring, cellular damage, and eventually malignant transformation.
Types of asbestos associated with mesothelioma include:
- Amphibole asbestos (crocidolite, amosite): Considered more carcinogenic due to straight, needle-like fibers that more easily penetrate tissue
- Serpentine asbestos (chrysotile): More common but somewhat less carcinogenic, with curly fibers
Genetic and Hereditary Factors
While asbestos exposure is the predominant cause, genetic factors play important roles:
- BAP1 gene mutations: Individuals with germline mutations in the BAP1 tumor suppressor gene have increased susceptibility to mesothelioma and may develop the disease with minimal asbestos exposure
- Other genetic alterations: Mutations in NF2, CDKN2A, and TP53 genes are frequently observed in mesothelioma tumors
- Familial clustering: Some families show higher rates of mesothelioma, suggesting genetic predisposition
Other Known Triggers and Exposure Risks
- Radiation therapy: Prior radiation treatment for other cancers may increase risk
- Erionite exposure: A naturally occurring mineral fiber similar to asbestos, primarily in Turkey’s Cappadocia region
- Simian Virus 40 (SV40): A potential co-factor under investigation, possibly from contaminated polio vaccines in the 1950s-60s
- Carbon nanotubes: Some experimental evidence suggests certain engineered nanomaterials may have asbestos-like effects, though human evidence is lacking
- Chronic inflammation: May contribute to the malignant transformation of mesothelial cells
The latency period between asbestos exposure and mesothelioma development is exceptionally long, typically 20-50 years, making current cases often reflective of industrial practices from decades ago.
5. Risk Factors
Demographic Risk Factors
- Age: Primarily affects older adults (median age at diagnosis is 72)
- Gender: More common in men (75-80% of cases) due to occupational exposure patterns
- Race/Ethnicity: Generally similar across racial groups, though exposure opportunities may vary
Occupational Exposure
Highest risk occupations include:
- Asbestos miners and millers
- Insulation workers and installers
- Shipyard workers
- Construction workers (especially those involved in demolition)
- Automotive mechanics (particularly brake specialists)
- Power plant workers
- Firefighters
- Military personnel (particularly Navy veterans)
- Textile workers in facilities using asbestos
- Plumbers and pipefitters
Environmental Factors
- Residence near naturally occurring asbestos deposits
- Living near asbestos mines or factories
- Urban areas with deteriorating asbestos-containing buildings
- Proximity to sites of natural disasters or terrorist attacks that released asbestos (e.g., 9/11 World Trade Center collapse)
- Secondary exposure through contact with asbestos workers’ clothing or belongings
Impact of Pre-existing Conditions
- Prior respiratory disease: May increase susceptibility or complicate diagnosis
- Smoking: While not a direct cause of mesothelioma, smoking significantly increases the risk of lung cancer in asbestos-exposed individuals (synergistic effect)
- Compromised immune function: May increase susceptibility to asbestos-related cellular damage
Dose-Response Relationship
The risk increases with:
- Duration of exposure
- Intensity of exposure
- Cumulative exposure dose
- Type of asbestos (amphibole forms generally pose greater risk)
Despite clear risk factors, approximately 20% of mesothelioma patients have no identifiable history of asbestos exposure, suggesting either unrecognized exposure or alternative causative factors.
6. Complications
Direct Complications
Mesothelioma leads to numerous serious complications:
Pleural Mesothelioma:
- Pleural effusions (fluid buildup around the lungs)
- Respiratory failure
- Atelectasis (lung collapse)
- Pneumonia
- Dysphagia (difficulty swallowing) from esophageal compression
- Horner’s syndrome from nerve involvement
- Superior vena cava syndrome
Peritoneal Mesothelioma:
- Ascites (fluid buildup in the abdomen)
- Bowel obstruction
- Nutritional deficiencies
- Hernias
- Abdominal adhesions
Pericardial Mesothelioma:
- Cardiac tamponade (fluid compression of the heart)
- Arrhythmias
- Congestive heart failure
- Constrictive pericarditis
Systemic Complications
- Cachexia (severe weight loss and muscle wasting)
- Paraneoplastic syndromes
- Thromboembolic events (DVT, pulmonary embolism)
- Hypercalcemia
- Anemia and other hematologic abnormalities
Treatment-Related Complications
- Surgical morbidity and mortality
- Radiation pneumonitis
- Chemotherapy side effects (myelosuppression, neuropathy, etc.)
- Immunotherapy-related adverse events
Long-Term Impact
Mesothelioma has profound long-term impacts on:
- Physical function: Progressive decline in respiratory or abdominal function
- Quality of life: Significant deterioration due to pain, fatigue, and psychological distress
- Financial status: Substantial economic burden from medical costs and lost income
- Family caregivers: High levels of distress and burden
Mortality Rates
Mesothelioma has a poor prognosis with:
- Median survival of 12-21 months for pleural mesothelioma
- Slightly better prognosis for peritoneal mesothelioma with specialized treatments
- 5-year survival rates of 5-10% overall, though significantly higher (40-50%) for patients who can undergo aggressive multimodal therapy with surgery
7. Diagnosis & Testing
Initial Assessment
- Comprehensive history (including occupational and environmental exposures)
- Physical examination
- Evaluation of presenting symptoms
Imaging Studies
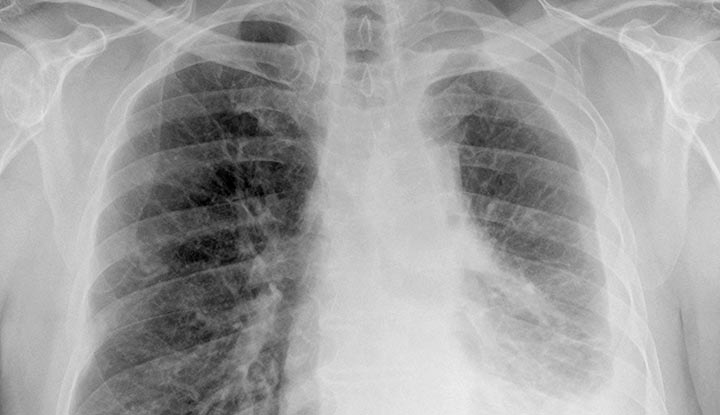
- Chest X-ray: Often shows pleural thickening, effusion, or masses (typically the first imaging study)
- CT scan: The primary imaging modality; shows extent of disease and can guide biopsy
- MRI: Provides better soft tissue contrast for evaluating local invasion
- PET-CT: Helps identify metabolically active tumors and distant metastases
- Ultrasound: Primarily used for guiding biopsies or evaluating effusions
Biomarkers and Blood Tests
- Soluble mesothelin-related peptides (SMRP): The most validated biomarker, elevated in 60-80% of patients
- Fibulin-3: Potentially useful for early detection
- Osteopontin: Elevated in mesothelioma but lacks specificity
- Routine laboratory tests: CBC, metabolic panel, inflammatory markers (often abnormal but not specific)
Pathological Diagnosis
- Cytology: Examination of fluid from effusions (sensitivity limited, 30-50%)
- Tissue biopsy: Essential for definitive diagnosis
- Fine-needle aspiration: Limited sample size, variable yield
- Core needle biopsy: Better yield than FNA but still limited
- Video-assisted thoracoscopic surgery (VATS): Gold standard for pleural mesothelioma
- Laparoscopy: Used for peritoneal mesothelioma
- Open surgical biopsy: Sometimes required for definitive diagnosis
Histopathological and Molecular Analysis
- Immunohistochemistry: Essential for differential diagnosis
- Positive markers: Calretinin, WT-1, D2-40, CK5/6, mesothelin
- Negative markers: CEA, TTF-1, Ber-EP4, MOC-31
- Histological subtypes:
- Epithelioid (60-70%, better prognosis)
- Sarcomatoid (10-20%, worse prognosis)
- Biphasic/mixed (20-30%, intermediate prognosis)
- Molecular testing: Increasingly important for targeted therapies and prognosis
- BAP1 immunohistochemistry
- CDKN2A FISH
- Next-generation sequencing panels
Staging
- TNM staging system: Evaluates tumor size/extent, lymph node involvement, and metastasis
- Functional assessment: Pulmonary function tests, cardiac stress tests, and performance status evaluation to determine treatment candidacy
Early detection remains challenging but is crucial for improving outcomes. Current research focuses on developing screening protocols for high-risk populations and more sensitive biomarkers for early diagnosis.
8. Treatment Options
Treatment Approach
Treatment for mesothelioma is typically multimodal and depends on:
- Type and stage of mesothelioma
- Patient’s overall health and performance status
- Patient preferences
- Available expertise and resources
Surgical Interventions
For Pleural Mesothelioma:
- Extrapleural pneumonectomy (EPP): Removal of the affected lung, pleura, diaphragm, and pericardium
- Pleurectomy/decortication (P/D): Removal of the pleura and visible tumor while preserving the lung
- Partial pleurectomy: Limited removal of pleura for symptom control
- Palliative procedures: Pleurodesis, indwelling pleural catheters for effusion management
For Peritoneal Mesothelioma:
- Cytoreductive surgery (CRS): Removal of visible tumors throughout the abdomen
- Hyperthermic intraperitoneal chemotherapy (HIPEC): Heated chemotherapy directly in the abdominal cavity following CRS
For Pericardial Mesothelioma:
- Pericardiectomy
- Window procedures
Radiation Therapy
- Adjuvant radiation: After surgery to reduce local recurrence
- Neoadjuvant radiation: Before surgery in some protocols
- Palliative radiation: For pain relief and symptom control
- Intensity-modulated radiation therapy (IMRT): More targeted to reduce damage to healthy tissue
- Proton beam therapy: Emerging option with potential for better tissue sparing
Chemotherapy
- First-line regimen: Cisplatin or carboplatin combined with pemetrexed (Alimta)
- Second-line options: Gemcitabine, vinorelbine, or re-challenge with first-line agents
- Maintenance therapy: Being investigated in clinical trials
- Intraoperative chemotherapy: For pleural and peritoneal disease
Immunotherapy
- Immune checkpoint inhibitors:
- Anti-PD-1 agents (pembrolizumab, nivolumab)
- Anti-CTLA-4 agents (ipilimumab)
- Combination immunotherapy: Multiple checkpoint inhibitors or with chemotherapy
- CAR-T cell therapy: In early clinical trials
- Dendritic cell vaccines: Experimental approaches
Targeted Therapies
- Antiangiogenic agents: Bevacizumab (approved in some countries as part of first-line treatment)
- Mesothelin-targeted agents: Anetumab ravtansine, SS1P
- BAP1 pathway inhibitors: Under investigation
- Arginine deprivation therapy: For ASS1-deficient tumors
- PARP inhibitors: For tumors with DNA repair deficiencies
Emerging Experimental Approaches
- Gene therapy: Targeting specific genetic alterations
- Photodynamic therapy: Light-activated agents for localized treatment
- Tumor treating fields (TTFields): Electric fields that disrupt cell division
- Cryoablation: Freezing of tumor tissues
- Oncolytic viruses: Engineered viruses that selectively kill cancer cells
Palliative Care
- Pain management
- Management of effusions
- Respiratory support
- Nutritional support
- Psychosocial care
Treatment outcomes vary widely, with peritoneal mesothelioma generally having a better response to aggressive treatment than pleural. The field is rapidly evolving, with numerous clinical trials exploring novel combinations and approaches.
9. Prevention & Precautionary Measures
Primary Prevention
The cornerstone of mesothelioma prevention is eliminating or minimizing asbestos exposure:
Regulatory Measures:
- Complete bans on asbestos mining, manufacturing, and use (implemented in over 60 countries)
- Strict regulations for asbestos removal and handling
- Workplace exposure limits and monitoring requirements
- Mandatory safety protocols for high-risk industries
Occupational Safeguards:
- Engineering controls: Isolation, ventilation, dust suppression
- Administrative controls: Training, exposure time limits, work practices
- Personal protective equipment: Respirators, protective clothing, decontamination procedures
- Regular workplace air monitoring
- Medical surveillance for exposed workers
Environmental Controls:
- Safe removal and disposal of asbestos-containing materials
- Encapsulation of asbestos in buildings when removal isn’t feasible
- Public registries of buildings containing asbestos
- Proper management of naturally occurring asbestos sites
Public Education:
- Awareness programs about asbestos hazards
- Information resources for homeowners with asbestos-containing materials
- Training for DIY renovators to identify and avoid asbestos
Secondary Prevention
For those already exposed to asbestos:
Medical Surveillance:
- Regular chest X-rays or low-dose CT scans
- Pulmonary function tests
- Evaluation of biomarkers (under investigation)
Lifestyle Modifications:
- Smoking cessation (crucial, as smoking synergistically increases cancer risk with asbestos)
- Maintaining general health and immune function
- Prompt medical attention for respiratory symptoms
Preventive Interventions:
- No proven chemoprevention agents exist specifically for mesothelioma
- Research into anti-inflammatory and anti-oxidant approaches continues
Vaccine Development
Unlike some virus-associated cancers, there are no preventive vaccines for mesothelioma. However, therapeutic vaccines are under investigation as treatment options.
Cost-Effectiveness of Prevention
Economic analyses consistently demonstrate that prevention through asbestos bans and exposure controls is far more cost-effective than treatment of resulting diseases. The World Health Organization and International Labour Organization strongly advocate for global elimination of asbestos use as the only definitive preventive measure.
10. Global & Regional Statistics
Global Incidence and Prevalence
- Approximately 30,000-43,000 people die from mesothelioma worldwide each year
- Incidence varies dramatically by country, reflecting historical industrial asbestos use
- Global incidence is expected to peak at different times in different regions, based on when asbestos use was at its height and when/if it was banned
Regional Patterns
High-Incidence Regions:
- United Kingdom: Highest age-adjusted mortality rate globally (approximately 31 per million in males)
- Australia: Very high rates (30-40 per million in males) due to extensive mining and use
- Western Europe: Particularly Italy, Netherlands, and Belgium, with rates of 15-25 per million
- United States: Approximately 3,000 new cases annually, with rates of 10-15 per million in males
Emerging Concern Areas:
- Russia, China, India, and Brazil: Major current producers and users of asbestos
- Southeast Asia: Increasing industrialization with limited regulations
- Eastern Europe: Legacy of industrial use with inadequate controls
Special Concern Regions:
- Turkey (Cappadocia region): Extremely high rates due to environmental erionite exposure
- Libby, Montana (USA): Notable cluster related to vermiculite mining contaminated with asbestos
Mortality and Survival Rates
- Overall survival: Median survival of 12-21 months from diagnosis
- 5-year survival rate: 5-10% overall; varies significantly by type and stage
- Pleural: Generally 5-10% at 5 years
- Peritoneal: Up to 50% at 5 years with HIPEC/cytoreductive surgery
- Pericardial and testicular: Too rare for reliable statistics
- Mortality trends: Declining in some Western countries due to earlier asbestos bans; rising in countries with continued use
Temporal Trends
- Western countries: Peak incidence occurring now or recently passed
- Developing countries: Predicted to see rising rates over the next 2-3 decades
- Global burden: Estimated 9.9 million disability-adjusted life years (DALYs) annually
Economic Impact
- Healthcare costs: Estimated $1-2 billion annually in the US alone
- Compensation: Billions in legal settlements and workers’ compensation
- Productivity losses: Substantial due to premature mortality and disability
- Prevention costs: Estimated $150 billion for global asbestos removal and replacement
These statistics illustrate that mesothelioma remains a significant global health challenge with substantial geographic variation and economic impact. The disease burden is shifting from developed to developing countries as asbestos use continues in many parts of the world.
11. Recent Research & Future Prospects
Recent Advances in Research
Genomic and Molecular Insights:
- Comprehensive genomic analyses have revealed distinct molecular subtypes beyond histological classification
- Identification of key driver mutations (BAP1, NF2, CDKN2A, TP53) providing new therapeutic targets
- Discovery of specific gene expression signatures predicting treatment response
- Epigenetic alterations increasingly recognized as important in mesothelioma development
Immunotherapy Developments:
- FDA approval of ipilimumab-nivolumab combination for first-line treatment of unresectable pleural mesothelioma (October 2020)
- Emerging biomarkers to predict immunotherapy response (tumor mutational burden, PD-L1 expression, etc.)
- Novel checkpoint inhibitors targeting alternative immune pathways
- Approaches to overcome immunosuppressive tumor microenvironment
Improved Surgical Techniques:
- Minimally invasive approaches reducing morbidity
- Enhanced recovery after surgery (ERAS) protocols
- Intraoperative imaging for improved tumor visualization
- Computer-assisted surgical planning and navigation
Precision Medicine Approaches:
- Patient-derived organoids and xenografts for personalized treatment testing
- Circulating tumor DNA (ctDNA) for monitoring treatment response
- Artificial intelligence algorithms to predict outcomes based on clinical and molecular data
- Basket trials grouping patients by molecular alterations rather than cancer type
Current Clinical Trials
Novel Treatment Combinations:
- Immunotherapy with targeted agents
- Sequencing studies of surgery, radiation, and systemic therapy
- Maintenance strategies after initial disease control
Innovative Approaches:
- CAR-T cell therapy targeting mesothelin
- Tumor microenvironment modulators
- Microbiome-based interventions
- RNA interference therapeutics
Emerging Therapeutic Targets:
- Argininosuccinate synthetase 1 (ASS1) deficiency
- Linear ubiquitin chain assembly complex (LUBAC)
- EZH2 histone methyltransferase
- PARP in BAP1-mutated tumors
Future Prospects
Prevention and Screening:
- Development of blood-based screening tests for high-risk populations
- Global asbestos ban advocacy gaining momentum
- Improved protection for remediation workers
- Risk models incorporating genetic susceptibility markers
Therapeutic Horizons:
- Combination immunotherapy approaches showing promise
- Potential for curative treatment in peritoneal mesothelioma expanding
- Novel delivery systems for localized therapy
- Gene editing approaches to restore tumor suppressor function
Challenges Ahead:
- Addressing mesothelioma in developing countries
- Overcoming treatment resistance
- Expanding clinical trial access
- Balancing aggressive treatment with quality of life
- Addressing the anticipated global peak in cases
Promising Developments:
- Increasing survival rates for peritoneal mesothelioma with multimodal therapy (5-year survival now approaching 50%)
- Growing number of long-term survivors creating opportunity to study factors associated with extended survival
- International collaboration improving research quality and pace
- Patient advocacy driving increased research funding and awareness
The field of mesothelioma research has seen more advances in the past decade than in the previous century, offering genuine hope for improved outcomes. While a universal cure remains elusive, the prospect of transforming mesothelioma into a chronic, manageable disease represents a significant paradigm shift.
12. Interesting Facts & Lesser-Known Insights
Historical and Cultural Context
- Asbestos has been used for over 4,500 years, with evidence of its use in Finnish pottery dating to 2500 BCE
- Ancient Romans noted the “sickness of the lungs” in slaves who wove asbestos cloth
- Pliny the Elder described the use of asbestos cloth as funeral dress for kings and noted respiratory disease in asbestos miners
- The term “mesothelioma” derives from Greek: “meso” (middle) and “thelioma” (tumor)
Notable Cases
- Steve McQueen, American actor, died from mesothelioma in 1980 after exposure during his time in the Marines and as a race car driver
- Bernie Banton, Australian social justice advocate who fought for compensation for asbestos victims until his death from mesothelioma in 2007
- Admiral Elmo Zumwalt Jr., Chief of Naval Operations, died from mesothelioma related to asbestos exposure aboard Navy ships
Surprising Facts
- Mesothelioma has one of the longest latency periods of any disease, with cases developing up to 70 years after exposure
- Despite being banned in many countries, global asbestos production remains over 1.1 million tons annually
- Russia, China, Kazakhstan, and Brazil are the world’s largest asbestos producers today
- The World Trade Center collapse on 9/11 released hundreds of tons of asbestos into the air, raising concerns about future mesothelioma cases
- The U.S. military used asbestos extensively, resulting in veterans accounting for approximately 30% of all mesothelioma cases in the United States
Occupational Insights
- Shipyard workers from WWII experienced particularly high rates due to intensive asbestos use in naval vessels
- Family members of asbestos workers face elevated risk from “take-home” exposure on clothing and hair
- Teachers and school staff have developed mesothelioma from working in buildings with deteriorating asbestos insulation
- Automotive mechanics remain at risk from asbestos in older brake linings and clutches
Myths and Misconceptions
- Myth: Asbestos is banned in the United States Fact: Asbestos is regulated but not completely banned in the U.S.; it remains legal for use in certain products
- Myth: Only elderly men develop mesothelioma Fact: While most common in older men, mesothelioma can affect anyone exposed to asbestos, including young adults and children
- Myth: Brief or low-level asbestos exposure is safe Fact: No safe level of asbestos exposure has been established; even brief exposures can potentially cause disease
- Myth: Mesothelioma always develops in the lungs Fact: Mesothelioma develops in the mesothelium (the lining of organs), not in the organ tissue itself
- Myth: Smoking causes mesothelioma Fact: Unlike lung cancer, smoking does not cause mesothelioma, though it can worsen overall prognosis
Research Curiosities
- Certain populations appear resistant to mesothelioma despite heavy asbestos exposure, suggesting genetic protective factors
- Some studies suggest that higher fiber intake may reduce mesothelioma risk in exposed individuals
- The BAP1 cancer syndrome, discovered in 2011, creates susceptibility to mesothelioma even with minimal asbestos exposure
- Zeolite minerals, used in water filtration and pet litter, have chemical structures similar to asbestos and are being studied for potential health effects
- Environmental exposure to naturally occurring asbestos has created “mesothelioma villages” in Turkey, Greece, Corsica, and parts of China
These lesser-known facts highlight the complex history and ongoing challenges of mesothelioma, a disease that stands at the intersection of industrial history, occupational health, environmental exposure, and evolving medical science.
References and Further Reading
Medical Literature
- Carbone, M., et al. (2019). Mesothelioma: Scientific clues for prevention, diagnosis, and therapy. CA: A Cancer Journal for Clinicians, 69(5), 402-429.
- Yap, T. A., Aerts, J. G., Popat, S., & Fennell, D. A. (2017). Novel insights into mesothelioma biology and implications for therapy. Nature Reviews Cancer, 17(8), 475-488.
- Kindler, H. L., et al. (2018). Treatment of Malignant Pleural Mesothelioma: American Society of Clinical Oncology Clinical Practice Guideline. Journal of Clinical Oncology, 36(13), 1343-1373.
- Baas, P., et al. (2021). First-line nivolumab plus ipilimumab in unresectable malignant pleural mesothelioma (CheckMate 743): a multicentre, randomised, open-label, phase 3 trial. The Lancet, 397(10272), 375-386.
Organizations and Resources
- International Mesothelioma Interest Group (iMig): www.imig.org
- Mesothelioma Applied Research Foundation: www.curemeso.org
- International Ban Asbestos Secretariat: www.ibasecretariat.org
- World Health Organization – Elimination of Asbestos-Related Diseases: www.who.int/publications/i/item/WHO-SDE-OEH-06.03
Clinical Trial Information
- ClinicalTrials.gov (search term: mesothelioma)
- EU Clinical Trials Register
- International Clinical Trials Registry Platform (WHO)
This report represents a compilation of current medical knowledge as of October 2024. Readers are encouraged to consult healthcare professionals for personalized medical advice and to refer to the most recent studies as research in this field is rapidly evolving.